 Ingeborg Farver-Vestergaard
Ingeborg Farver-Vestergaard Eleonora Volpato
Eleonora Volpato Henrik Hansen
Henrik Hansen Liz Steed
Liz Steed
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
EDITORIAL article
Front. Rehabil. Sci. , 12 February 2025
Sec. Pulmonary Rehabilitation
Volume 6 - 2025 | https://doi.org/10.3389/fresc.2025.1562337
This article is part of the Research Topic Psychosocial Issues and Interventions in Pulmonary Rehabilitation View all 8 articles
Editorial on the Research Topic
Psychosocial issues and interventions in pulmonary rehabilitation
Pulmonary rehabilitation is a cornerstone of care for individuals with chronic respiratory disease as it offers a structured approach to alleviate symptoms and improve physical function and quality of life (1–3). However, its effectiveness is deeply intertwined with a myriad of psychosocial and behavioural factors (4). In the context of chronic disease, rehabilitation programmes must encompass meaningful psychosocial interventions, that facilitate patient engagement in activities that contribute to maintaining their quality of life (5, 6). These efforts are most successful if they address the disease-related fear, psychological distress, fatigue and social isolation that respiratory conditions cause (7, 8). Understanding how such interventions can best be integrated into pulmonary rehabilitation to provide the optimal opportunity for holistic care based on the biopsychosocial approach to medicine, is important to guide practice.
A collection of articles in Frontiers of Rehabilitation Sciences addresses the psychosocial dimensions of pulmonary rehabilitation and highlights interventions that improve patient outcomes by addressing the interplay of psychological social and behavioural factors. To guide the discussion, we have organised these dimensions into four key themes:
1. Pulmonary rehabilitation as a dynamic, ongoing process
2. The role of psychosocial factors in symptom perception and management
3. Timing and tailoring of interventions to meet patient needs
4. Improving communication between patients and healthcare professionals
In the sections that follow, we consider each theme based on key findings from the featured articles. Finally, we identify potential implications for clinical practice and propose future directions for research and intervention development.
A unifying theme across the articles is the recognition of pulmonary rehabilitation as a continuous process rather than a finite program. Chronic respiratory diseases follow varied trajectories, requiring flexible approaches (9). For example, chronic obstructive pulmonary disease (COPD), as studied by Gronhaug et al., Farver-Vestergaard et al., Kaasgaard et al., involves a gradual decline punctuated by acute exacerbations. In contrast, lung cancer, as examined by Kaasgaard et al., often presents a more rapid and terminal progression. Meanwhile, lung transplant recipients, as explored by Song et al., face an intense post-transplant phase in which rehabilitation is crucial for recovery. These distinct trajectories underscore the need for multidisciplinary and adaptive care models that address shared and condition-specific challenges, such as breathlessness as studied by Pavy et al.
The studies in this collection underscore the significant role of psychological and social factors in shaping patients’ experience of their symptoms and their ability to manage them. Pavy et al.'s narrative review of nine experimental studies, in which breathlessness was induced in healthy individuals, demonstrates how unpredictable episodes of breathlessness can amplify fear and distress, thereby increasing the overall burden of these episodes. On the other hand, the predictability of such episodes has been shown to be associated with lower levels of distress. Similarly, Farver-Vestergaard et al.'s prospective study of individuals with COPD participating in a community-based pulmonary rehabilitation program emphasises how disease-specific anxiety management strategies, such as planning, problem solving and acceptance of physical symptoms, can be integrated into pulmonary rehabilitation activities and interactions with healthcare professionals and peers.
Another key theme is tailored interventions to address unique patient needs leading to better engagement and outcomes. For example, Kaasgaard et al. demonstrate that disease-specific rehabilitation programmes for patients with non-small cell lung cancer were associated with higher attendance rates and perceived relevance compared to generalised programs. Another study by Kaasgaard et al. indicates that self-reported activity levels and quality of life scores 5 years after initial PR were positively related to initial completion of the programme, regardless of whether patients had attended conventional physical exercise training or standardised group singing as the training modality.
The cross-sectional study by Song et al. identifies two distinct subgroups among stable lung transplant recipients up to 3 years post-transplantation: those with a high quality of life and those with a low quality of life. Their results indicate the importance of timely rehabilitation attention for the low quality of life-group, which was characterised by single lung transplantation, hospital readmission due to infection, low levels of optimism and mindfulness, and high levels of negative emotions. Identifying such characteristics could be facilitated by patient-reported outcome measures, as demonstrated in the study by Gronhaug et al., which will be discussed in the following section.
Effective rehabilitation depends on healthcare professionals understanding and addressing the unique needs and challenges of patients. In order to achieve this, communication between the patient and healthcare professional is essential, as the impact of symptoms and psychosocial issues cannot be objectively measured. Gronhaug et al. demonstrate how integrating patient-reported outcome measures (PROMs) into clinical practice facilitates meaningful dialogue and uncovers overlooked psychosocial challenges, enabling more personalised rehabilitation strategies.
This collection advances our understanding of not only the content but also the approach to integrating psychosocial dimensions into pulmonary rehabilitation. Throughout, the importance of personalisation and multidisciplinary, patient-centred approaches is underscored. Table 1 summarises key findings from each theme listed in this editorial along with potential clinical implications and future directions.
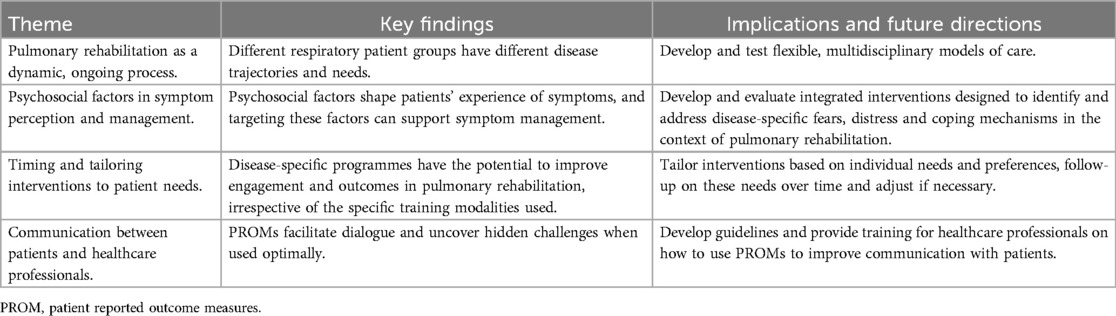
Table 1. Key findings from the themes listed in the article collection.
There are several areas that merit further exploration. First, current knowledge of biopsychosocial mechanisms is typically based on cross-sectional studies or studies with relatively short follow-up periods. As chronic respiratory diseases often develop over several years, longitudinal research is needed to capture the evolution of these factors over time. Second, the impact of respiratory disease extends to family carers, who often face unique emotional and practical challenges. It is likely that the role and burden of carers in chronic respiratory disease deviate from carer burden in other diseases, such as cancer, for which relatively more research is available. Third, distinguishing between disease-related psychosocial challenges and comorbid mental disorders in respiratory disease is complex. Further research is needed to develop accurate assessment methods and implement effective stepped-care intervention strategies.
As respiratory diseases continue to pose significant global health challenges, addressing psychosocial issues at referral to and during pulmonary rehabilitation is essential. This research topic highlights and inspires the potential for pulmonary rehabilitation interventions that are as multidimensional and dynamic as the patients they serve.
IF-V: Writing – original draft, Writing – review & editing. EV: Writing – review & editing. HH: Writing – review & editing. LS: Writing – review & editing.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for prevention, diagnosis and management of COPD: 2023 report. Global Initiative for Chronic Obstructive Lung Disease (2023). Available online at: https://goldcopd.org/2023-gold-report-2/ (Accessed February 06, 2025).
2. Troosters T, Blondeel A, Janssens W, Demeyer H. The past, present and future of pulmonary rehabilitation. Respirology. (2019) 24:830–7. doi: 10.1111/resp.13517
3. Spruit MA, Singh SJ, Garvey C, Zu Wallack R, Nici L, Rochester , et al. An official American Thoracic Society/European Respiratory Society statement: key concepts and advances in pulmonary rehabilitation. Am J Respir Crit Care Med. (2013) 188:e13–64. doi: 10.1164/rccm.201309-1634ST
4. Holland A, Dal Corso S, Spruit MA. Pulmonary Rehabilitation (ERS Monograph). Sheffield: European Respiratory Society (2021).
5. Lenferink A, Lee AL. Education and self-management. In: Holland AE, Dal Corso S, Spruit MA, editors. Pulmonary Rehabilitation (ERS Monograph). Sheffield: European Respiratory Society (2021). p. 00–116.
6. Farver-Vestergaard I, Johannesen G, Beek L ter. Occupational therapy, nutritional modulation and psychological support. In: Holland A, Dal Corso S, Spruit M, editors. Pulmonary Rehabilitation. Sheffield: European Respiratory Society (2021). pp. 83–98.
7. Carl J, Schultz K, Janssens T, von Leupoldt A, Pfeifer K, Geidl W. The “can do, do do” concept in individuals with chronic obstructive pulmonary disease: an exploration of psychological mechanisms. Respir Res. (2021) 22:1–10. doi: 10.1186/s12931-021-01854-1
8. von Leupoldt A. Treating anxious expectations can improve dyspnoea in patients with COPD. Eur Respir J. (2017) 50:1701352. doi: 10.1183/13993003.01352-2017
Keywords: chronic respiratory disease, behaviour change, psychological distress, holistic care, breathlessness
Citation: Farver-Vestergaard I, Volpato E, Hansen H and Steed L (2025) Editorial: Psychosocial issues and interventions in pulmonary rehabilitation. Front. Rehabil. Sci. 6:1562337. doi: 10.3389/fresc.2025.1562337
Received: 17 January 2025; Accepted: 3 February 2025;
Published: 12 February 2025.
Edited by:
Enrico M. Clini, University of Modena and Reggio Emilia, ItalyReviewed by:
Mara Paneroni, Scientific Clinical Institute Maugeri (ICS Maugeri), ItalyCopyright: © 2025 Farver-Vestergaard, Volpato, Hansen and Steed. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ingeborg Farver-Vestergaard, aW5nZWJvcmcuZmFydmVyQHJzeWQuZGs=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.