 M. B. Borg
M. B. Borg M. Battaglia
M. Battaglia M. Invernizzi
M. Invernizzi A. Baricich
A. Baricich
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Rehabil. Sci. , 23 December 2024
Sec. Rehabilitation for Musculoskeletal Conditions
Volume 5 - 2024 | https://doi.org/10.3389/fresc.2024.1506279
Osteoporotic vertebral fractures (OVFs) significantly impair the quality of life in older adults. Spinal orthoses are commonly used, but their effectiveness is debated. Thus, we aimed to evaluate the impact of different spinal orthoses on pain, functionality, and quality of life in patients with OVFs. A review of PubMed, Scopus, PEDro, and Cochrane Library was conducted, covering studies from 2000 to 2024. Studies assessing spinal orthoses’ effects on pain, functionality, and quality of life in adults with OVFs were included. Ten studies involving 970 participants were included. Several studies reported significant improvements in pain, functionality, and quality of life with spinal orthoses. Dynamic hyperextension orthoses, such as Spinomed® and Spinfast®, showed potential benefits, particularly in enhancing trunk muscle strength. In conclusion, spinal orthoses may help manage pain and improve functionality and quality of life in OVFs. However, further high-quality trials are needed to confirm their efficacy.
Osteoporotic vertebral fractures (OVFs) are a common and debilitating consequence of osteoporosis, a systemic skeletal disease characterized by low bone mass and microarchitectural deterioration of bone tissue (1).
OVFs are associated with substantial morbidity and mortality, significantly impacting patients' quality of life (2). The pathophysiology of OVFs involves a complex interplay of factors, including decreased bone density, altered bone microarchitecture, and increased bone fragility (3). Clinically, OVFs often present with acute back pain, progressive deformity, loss of height, and disability. Current treatment strategies for OVFs aim to manage pain, prevent further fractures, and improve function and quality of life. These approaches include pharmacological therapies, surgical treatments, physical therapies, lifestyle modifications, and the use of orthotic devices (4, 5). Among these, spinal orthoses have gained particular attention for their potential to provide external support, reduce pain, and enhance functional status in patients with stable fractures and no neurological impairments (6).
There are various types of spinal orthoses, which can be either custom-made or prefabricated. They can be categorized based on the area of the spine they support, or on their specific properties. In this mini-review, the following types of spinal orthoses for osteoporotic fragility vertebral fractures were considered (7):
1. Rigid Orthosis: rigid orthoses are spinal braces made from hard materials such as plastic or metal, designed to provide maximal support and immobilization to the spine. These devices restrict movement in multiple planes, reducing the load on the vertebral bodies and promoting spinal alignment. They are typically prescribed for acute traumatic fractures or post-surgical stabilization. They provide strong immobilization and protection against further injury. However, they could also lead to discomfort, potential muscle atrophy due to limited movement, and challenges in adherence to long-term use (8).
2. Soft Orthosis: soft orthoses, also known as flexible braces, are constructed from elastic or foam materials, offering support with greater flexibility compared to rigid orthoses. They allow for some spinal movement while providing moderate support and compression. These are often used for less severe fractures or for patients requiring prolonged use, where comfort is a priority. Advantages include greater comfort and ease of use, less impacting muscle function. However, disadvantages include reduced support and immobilization, which may be insufficient for more severe fractures.
3. Dynamic Orthosis: dynamic orthoses, such as the Spinfast® and the Spinomed® braces, are designed to encourage muscle activation and posture correction through biofeedback mechanisms. These braces are more flexible and adjust to the patient's movement, promoting active engagement of the back muscles during daily activities. They are often indicated for chronic management, focusing on improving functionality and reducing pain over time. Advantages include the potential for improving muscle strength and posture, with less discomfort than rigid braces. Disadvantages include a potentially lower degree of stabilization compared to rigid orthoses, and the need for patient compliance and correct usage to achieve therapeutic benefits.
Spinal orthoses, including rigid, soft, or dynamic braces, are commonly employed to manage of OVFs. However, the efficacy of these devices remains a topic of ongoing debate, with studies reporting mixed results (6, 9, 10). Some evidence suggests that dynamic orthoses may offer significant benefits for patients with sub-acute OVFs. Yet, very low-quality evidence indicates no significant differences in outcomes when comparing dynamic, rigid, and soft braces in the management of acute fractures (11). Consequently, a recent systematic review concluded that, due to the variability in study quality and the limitations of previous research, a general recommendation for the use of spinal orthoses in treating osteoporotic vertebral fractures is not feasible, as no clear evidence supports the superiority of any specific orthosis (12).
In summary, despite the widespread use of spinal orthoses for osteoporotic vertebral fractures (OVFs), there is no clear consensus on their effectiveness in key outcomes such as pain relief, functional improvement, and quality of life. Previous reviews have explored these devices, but a thorough evaluation comparing different types of orthoses is still missing. This mini-review addresses this gap by assessing the efficacy of various orthoses in managing pain, enhancing functionality, and improving quality of life in OVF patients, aiming to identify any orthosis that demonstrates superior efficacy and to inform clinical practice and future research efforts.
Two investigators independently performed a systematic search in PubMed/MEDLINE, Scopus, PEDro, and the Cochrane Library (PROSPERO registration number CRD42024573116), focusing on studies published from 2000 onwards in English and involving human participants. This time frame was chosen to prioritize research on contemporary spinal orthoses, as technological advancements render older models less relevant. The search employed Medical Subject Headings (MeSH) and keywords based on the Population, Intervention, Comparator, and Outcome (PICO) framework. The eligibility criteria were as follows: adults aged 18 years or older with osteoporotic vertebral fractures (Population), studies investigating the use of spinal orthoses (Intervention), studies comparing different types of spinal orthoses, comparing a spinal orthosis to no intervention, or studies with no comparator (Comparator), and outcomes related to pain, functionality (e.g., back extensor strength and gait), and quality of life (Outcomes). Experimental studies, including randomized controlled trials (RCTs), cohort studies, case-control studies, and prospective studies, were included, regardless of the presence of a control group. Non-experimental designs, observational studies, reviews, and studies not reporting the relevant outcomes were excluded. After removing duplicates, the investigators independently reviewed titles and abstracts, resolving discrepancies through discussion or, if needed, consultation with a third reviewer. Full texts of the selected studies were then evaluated, and reference lists were scanned for additional relevant studies. The final search was completed on July 25th, 2024, with any remaining disagreements settled by a third author.
The search string used was: [(osteoporosis OR osteoporotic OR fragility) AND fracture] AND (brace OR bracing OR orthosis) AND (pain OR functionality OR quality of life).
Each full-text document underwent a thorough evaluation for eligibility, conducted independently by two investigators. Data extraction was performed using a pre-designed data extraction form. The extracted data included: year of publication, authors, country, population characteristics, type of spinal orthosis used, modality and duration of orthosis use (hours per day and total length of use), comparator if applicable, and outcome measures (pain, functionality, and quality of life). The collected data were recorded in an Excel spreadsheet for subsequent analysis. Any discrepancies in data extraction were resolved through discussion between the two investigators, or by consulting a third investigator if necessary. This process was carried out manually, without the use of automated tools.
The study findings were integrated using a narrative method, which was necessitated by the heterogeneity in both methodology (including study design and outcomes) and clinical aspects (such as participant and intervention characteristics).
The risk of bias for included studies was assessed using the Cochrane Risk of Bias 2 (RoB 2) tool for randomized trials and the Risk Of Bias In Non-Randomized Studies of Interventions (ROBINS-I) tool for non-randomized studies. Two independent investigators conducted the evaluations, and any disagreements were resolved through discussion or by consulting a third investigator. Each domain of the RoB 2 and ROBINS-I tools was assessed, including random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective outcome reporting, and other potential sources of bias.
A total of 473 records were identified through database searches. After removing duplicates, 267 studies underwent eligibility screening based on titles and abstracts, resulting in the exclusion of 255 records. Twelve studies proceeded to full-text review, but one report was not retrieved, and another was excluded due to its observational design. Thus, ten studies met the inclusion criteria for this mini-review: de Sire et al. (13), Hettchen et al. (14), Kato et al. (15), Kim et al. (16), Li et al. (17), Meccariello et al. (18), Murata et al. (19), Pfeifer et al. (20, 21), and Valentin et al. (22).
The studies included in this review were published between 2004 and 2024 and were conducted in various countries, including Japan (n = 3), Germany (n = 3), Italy (n = 2), Korea (n = 1), and Denmark (n = 1). The study designs varied, encompassing prospective studies (n = 3), randomized controlled trials (RCTs) (n = 3), prospective comparative studies (n = 1), prospective cohort studies (n = 2), and experimental follow-ups (n = 1).
Sample sizes ranged from 13 to 284 participants, with a total of 970 participants (68%–100% female), and the mean age was 72 years. Time since osteoporotic vertebral fracture ranged from less than 3 days to more than 6 months, with one study including patients up to 17 years post-fracture. Overall, fracture levels spanned from T1 to L5.
The studies included in the present mini-review reported high heterogeneity in the type of intervention and comparator offered. The most frequent intervention proposed was dynamic orthosis which figured in 6 studies (Spinomed® in 5 studies and Spinfast® in 1 study), then rigid thoracolumbosacral orthosis (TLSO) in 3 studies, and soft lumbar orthosis in 2 studies.
Daily orthosis use varied from 15 min to 24 h per day, with total treatment durations ranging from 3 weeks to 12 months (mean: 13.5 weeks).
Detailed studies' characteristics and intervention data can be found in Table 1.
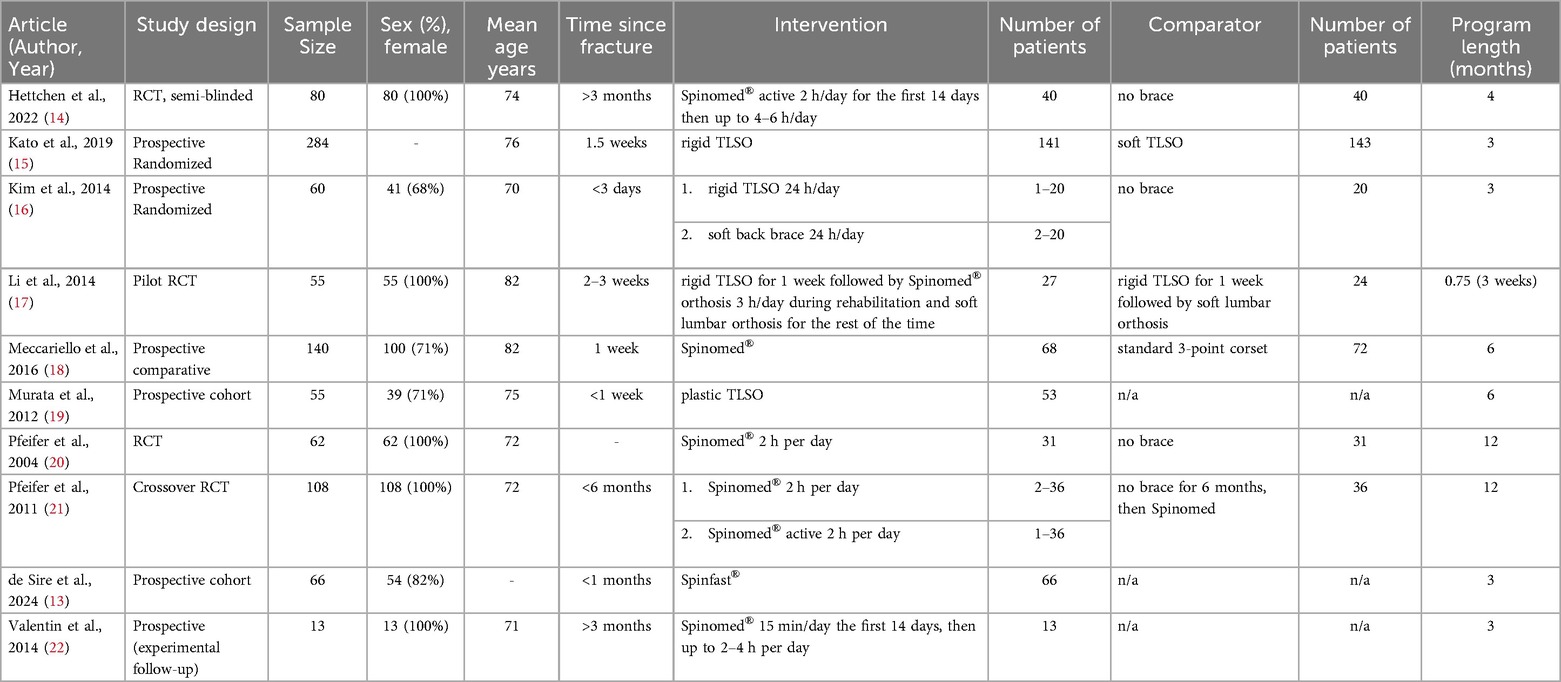
Table 1. Studies’ characteristics and interventions.
The key findings from the current review are detailed in Table 2. Below, the findings for each type of orthosis are presented:
1. Rigid Orthoses: Rigid orthoses were particularly effective in stabilizing vertebral fractures and preventing spinal deformities during early recovery. Murata et al. found that TLSO braces promoted effective fracture healing, with 88.7% of fractures settled within 6 months, and enabled early mobilization (19). Similarly, Kato et al. demonstrated superior spinal deformity prevention by rigid braces at 12 weeks, although their effectiveness in reducing pain and improving functionality was comparable to soft braces at 48 weeks (15). Despite their stabilizing properties, the long-term benefits of rigid orthoses in terms of pain relief or quality of life were limited.
2. Soft Orthoses: Soft orthoses showed notable efficacy in reducing pain and enhancing mobility in patients with mild to moderate conditions. Li et al. reported significant pain reduction and improved mobility with soft lumbar orthoses, achieving comparable outcomes to rigid braces (17). Kim et al. observed that no-brace, soft-brace, and rigid-brace groups showed similar improvements in pain and functional scores over time, suggesting equivalent long-term recovery benefits (16). The lightweight design of soft orthoses promotes better compliance, making them a favorable choice for extended use.
3. Dynamic Orthoses: Dynamic orthoses, including Spinomed® and Spinfast®, consistently outperformed other types across multiple outcomes, particularly for long-term rehabilitation. Meccariello et al. showed that dynamic orthoses provided greater pain reduction, improved functionality, and fewer complications compared to three-point orthoses (18). Pfeifer et al. documented that Spinomed® improved back extensor strength (up to 73%), posture, and quality of life while reducing pain by 38% and enhancing daily living functionality (20, 21). Valentin et al. reported that Spinomed® III increased back extensor strength by 50%, reduced back pain by 33%, and showed borderline significant improvements in physical functioning (22). Hettchen et al. found that Spinomed active® reduced back pain by 37%, improved kyphosis angle, and enhanced trunk strength and functional performance (e.g., improved chair-rise test results) (14). Similarly, De Sire et al. highlighted that Spinfast® significantly improved pain intensity, physical functioning, and quality of life within 3 months (13).
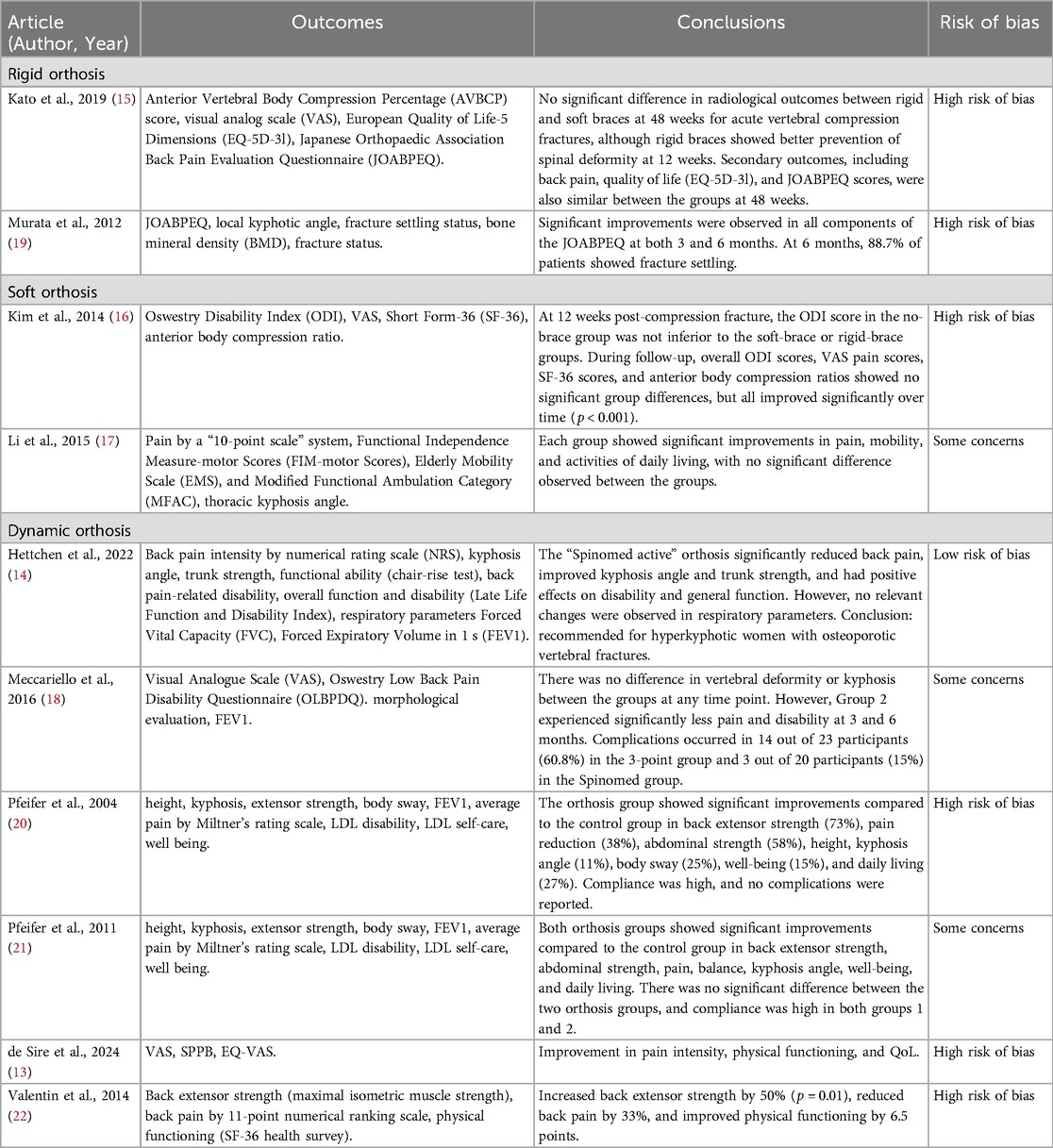
Table 2. Studies’ outcomes and conclusions.
The quality of the included studies was assessed using the Cochrane RoB2 tool for randomized trials and the ROBINS-I tool for non-randomized studies, overall judgments are reported in Table 2. Randomized trials showed varying levels of bias, with some at low risk and others at higher risk, particularly in deviations from intended interventions. As a result, these studies had some concerns regarding bias, and conclusions should be interpreted with caution. For non-randomized studies, risks ranged from low to serious, particularly due to confounding.
Overall, while the studies provide valuable insights, their limited quality requires cautious interpretation and further research is needed to confirm the findings.
The included studies, moreover, varied significantly in their approaches to monitoring confounders, particularly the use of analgesics. Some studies, such as Hettchen et al. (14) and Kato et al. (15), systematically tracked analgesic use over time, either through regular follow-up assessments or questionnaires, and reported no significant differences between groups. Others, including Pfeifer et al. (20, 21) and Valentin et al. (22), provided baseline data on analgesic consumption but did not monitor changes during the study period, limiting the ability to interpret their impact on outcomes. De Sire et al. (13) reported detailed data on pain medications, highlighting variability among participants but acknowledged the lack of systematic screening for other potential confounders. Conversely, studies such as Kim et al. (16), Li et al. (17), Meccariello et al. (18), and Murata et al. (19) did not address the use of analgesics or confounders related to pain management, presenting a gap in methodological rigor. These inconsistencies underscore the need for standardized protocols to account for confounding factors in future research.
This mini-review revealed that while spinal orthoses, including rigid, soft, and dynamic types, generally improved pain, functional outcomes, and quality of life in patients with osteoporotic vertebral fractures, no single orthosis consistently outperformed others across all measures.
More in detail, our investigation revealed several key insights into the efficacy of different spinal orthoses for managing pain, improving functionality, and enhancing quality of life in patients with osteoporotic vertebral fractures. Across the studies, no significant differences were observed between rigid and soft braces in terms of pain relief, functional improvement, or quality of life, although rigid braces were more effective in preventing spinal deformity in the short term, 12 weeks. However, long-term radiological outcomes at 48 weeks were similar between the two types of braces (15). Moreover, Murata et al. supports the role of rigid orthoses, such as the plastic TLSO, in providing critical biomechanical support and facilitating early mobilization, though it is noted that such benefits may not always translate into significantly better long-term outcomes compared to softer or dynamic options (19). Interestingly, the absence of a brace did not result in inferior clinical outcomes when compared to either soft or rigid braces, with all groups showing comparable improvements in pain and functionality over time (16). This indicates that while rigid braces may offer short-term benefits in preventing deformity and providing biomechanical support, their overall impact on pain relief and functional improvement is comparable to that of soft braces. Thus, the choice between rigid and soft braces may depend more on patient-specific factors and preferences rather than on significant differences in clinical effectiveness. The systematic review published by Newman et al. in 2016 reported that rigid orthoses were associated with higher complication rates compared to softer alternatives (6). This suggests that while rigid braces might offer certain benefits, they may come with increased risks and complications. Soft braces, in contrast, often present fewer complications and may provide a comparable level of clinical benefit without the added risk, making them a potentially safer choice for managing these stable fractures.
On the other hand, studies on dynamic braces, such as those by Hettchen et al. (14), Pfeifer et al. (20, 21), Valentin et al. (22), and De Sire et al. (13), present a more favorable picture for dynamic orthoses. Li et al. (17) and Meccariello et al. (18) investigated the general efficacy of dynamic orthoses and found that they contribute to significant improvements in pain reduction and functional mobility, with Meccariello et al. indicating superior outcomes in pain and disability reduction compared to three-point orthoses, and Li et al. showing that Spinomed® and soft lumbar orthoses demonstrated similar efficacy in pain reduction and functional mobility gains during the subacute stage (17). Pfeifer's et al. studies on the Spinomed® dynamic brace demonstrated notable improvements in back extensor strength, kyphosis angle, and quality of life, with minimal adverse effects, supporting its use as an effective non-pharmacological treatment (20, 21). Similarly, the Spinomed® III orthosis was effective in enhancing back extensor strength and reducing pain, with borderline significant improvements in physical functioning (22). Moreover, Hettchen et al. stated that the Spinomed® active orthosis significantly reduced back pain intensity and kyphosis angle while improving trunk strength and disability outcomes in hyperkyphotic women with vertebral fractures older than 3 months. Although respiratory function did not improve, the findings highlight orthosis as an effective option for addressing chronic back pain and related physical limitations in this population (14). However, as noted by Pieroh et al., the positive results associated with Spinomed® have been challenged by concerns about study quality and potential biases, indicating that while Spinomed shows potential, further high-quality research is necessary to confirm its effectiveness and address issues related to reproducibility (12). Finally, Spinfast® dynamic spinal orthosis, a more recent development, has demonstrated improvements in pain management, physical functioning, and quality of life in older patients with vertebral fragility fractures, according to De Sire et al. (13).
These findings collectively suggest that while different spinal orthoses offer varying degrees of benefit, dynamic braces such as the Spinomed® and Spinfast® offer promising non-pharmacologic options for managing osteoporotic vertebral fractures. This orthosis appears to address some limitations of previous models and provides promising results. Nonetheless, both Spinomed® and Spinfast® should be evaluated with careful consideration of their respective evidence bases. The existing studies suggest benefits from dynamic braces, but additional well-designed research is needed to establish their definitive role and to ensure that these benefits are consistently reproducible across diverse patient populations.
Our nuanced results are in line with previous reviews. Pieroh et al. noted a preference for soft or dynamic orthoses over rigid braces. Even though, despite some studies showing potential benefits, the highest-quality research indicated that patients treated without an orthosis had comparable outcomes to those using one. This highlights the limited and mixed evidence supporting the routine use of spinal orthoses (12). In contrast, Kweh et al. provided moderate-quality evidence supporting spinal orthoses for improving vertebral stability and functional outcomes in elderly patients (23). Similarly, Goodwin et al. highlighted the inconsistent evidence for orthotic devices and taping, noting that while Spinomed® showed some benefits, the overall quality of studies was limited (10).
In addition, Newman et al. conducted a systematic review whose key findings showed some promising results for subacute and longer-term rehabilitation. Specifically, semirigid thoracolumbar orthoses (TLO) and weighted kypho-orthoses (WKO) demonstrated potential benefits in improving strength, pain, posture, and balance (6). Rzewuska et al. et al. found low to moderate evidence supporting spinal orthoses for medium-term pain relief and disability reduction, which resonates with our findings on dynamic braces. However, this review also pointed out the overall low-quality evidence for conservative treatments, including orthoses, and the need for better-designed studies (9).
Lastly, Sanchez-Pinto-Pinto et al. demonstrated that dynamic hyperextension braces significantly reduced thoracic kyphosis and improved back extensor strength and quality of life, aligning with our results on the effectiveness of dynamic braces in improving these outcomes (24).
Overall, the findings suggest that while dynamic orthoses like Spinomed® and Spinfast® show promise in improving patients' outcomes, the comparative effectiveness of different orthotic types remains a subject of ongoing research. Moreover, the above-mentioned reviews collectively call for larger, more rigorous studies to better determine the efficacy of orthoses and to explore their role within comprehensive rehabilitation programs. The current evidence suggests that while spinal orthoses may offer some benefits, especially in specific contexts like subacute rehabilitation, their overall effectiveness and the risk of complications warrant cautious interpretation and further investigation.
This mini-review has several limitations to consider. The included studies exhibited significant heterogeneity in study design, participant characteristics, types of orthoses, and outcome measures. Methodological quality varied, with some studies lacking blinding or randomization, potentially introducing bias. Inconsistent follow-up periods limited the assessment of long-term efficacy and safety. Additionally, the management of confounders, particularly related to pain medications, varied considerably across studies. While some studies systematically monitored and reported the use of analgesics and other pharmacological interventions, others provided only baseline data or no information at all. This inconsistency limits the ability to fully account for the potential impact of pain medications on the reported outcomes. There is also a risk of publication bias, as studies with negative results may be underrepresented, and the review's restriction to English-language studies could lead to language bias. These factors highlight the need for more rigorous randomized controlled trials with standardized measures and longer follow-up periods to better evaluate the efficacy of spinal orthoses for osteoporotic vertebral fractures.
In conclusion, the choice of spinal orthosis should be tailored to individual patient needs, considering fracture characteristics and the specific advantages and limitations of each orthotic type. While spinal orthoses can help manage pain and improve function in osteoporotic vertebral fractures (OVFs), the variability in study designs and outcomes prevents definitive conclusions. Soft orthoses appear non-inferior to rigid braces, which may carry higher complication risks, while dynamic hyperextension orthoses like Spinomed® and Spinfast® show promise in enhancing trunk muscle strength and functionality. However, further high-quality randomized trials are needed to solidify these findings and guide clinical practice.
MBB: Conceptualization, Data curation, Investigation, Methodology, Writing – original draft, Writing – review & editing. MB: Data curation, Formal Analysis, Methodology, Writing – original draft. MI: Supervision, Validation, Writing – review & editing. AB: Conceptualization, Formal Analysis, Supervision, Validation, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. NIH Consensus Development Panel on Osteoporosis Prevention, Diagnosis, and Therapy. Osteoporosis prevention, diagnosis, and therapy. J Am Med Assoc. (2001) 285(6):785–95. doi: 10.1001/jama.285.6.785
2. Borgström F, Karlsson L, Ortsäter G, Norton N, Halbout P, Cooper C, et al. Fragility fractures in Europe: burden, management and opportunities. Arch Osteoporos. (2020) 15(1):59. doi: 10.1007/s11657-020-0706-y
3. Seeman E. Pathogenesis of bone fragility in women and men. Lancet. (2002) 359(9320):1841–50. doi: 10.1016/S0140-6736(02)08706-8
4. Kanis JA, Cooper C, Rizzoli R, Reginster JY, Scientific Advisory Board of the European Society for Clinical and Economic Aspects of Osteoporosis (ESCEO) and the Committees of Scientific Advisors and National Societies of the International Osteoporosis Foundation (IOF). European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos Int. (2019) 30(1):3–44. doi: 10.1007/s00198-018-4704-5
5. Kutsal FY, Ergin Ergani GO. Vertebral compression fractures: still an unpredictable aspect of osteoporosis. Turk J Med Sci. (2021) 51(2):393–9. doi: 10.3906/sag-2005-315
6. Newman M, Minns Lowe C, Barker K. Spinal orthoses for vertebral osteoporosis and osteoporotic vertebral fracture: a systematic review. Arch Phys Med Rehabil. (2016) 97(6):1013–25. doi: 10.1016/j.apmr.2015.10.108
7. Varma S, Tsang K, Peck G. Thoraco-lumbar-sacral orthoses in older people: a narrative literature review. Injury. (2023) 54(10):110986. doi: 10.1016/j.injury.2023.110986
8. McAviney J, Mee J, Fazalbhoy A, Du Plessis J, Brown BT. A systematic literature review of spinal brace/orthosis treatment for adults with scoliosis between 1967 and 2018: clinical outcomes and harms data. BMC Musculoskelet Disord. (2020) 21(1):87. doi: 10.1186/s12891-020-3095-x
9. Rzewuska M, Ferreira M, McLachlan AJ, Machado GC, Maher CG. The efficacy of conservative treatment of osteoporotic compression fractures on acute pain relief: a systematic review with meta-analysis. Eur Spine J. (2015) 24(4):702–14. doi: 10.1007/s00586-015-3821-5
10. Goodwin VA, Hall AJ, Rogers E, Bethel A. Orthotics and taping in the management of vertebral fractures in people with osteoporosis: a systematic review. BMJ Open. (2016) 6(5):e010657. doi: 10.1136/bmjopen-2015-010657
11. Jin YZ, Lee JH. Effect of brace to osteoporotic vertebral fracture: a meta-analysis. J Korean Med Sci. (2016) 31(10):1641–9. doi: 10.3346/jkms.2016.31.10.1641
12. Pieroh P, Spiegl UJA, Völker A, Märdian S, von der Höh NH, Osterhoff G, et al. Spinal orthoses in the treatment of osteoporotic thoracolumbar vertebral fractures in the elderly: a systematic review with quantitative quality assessment, glob. Spine J. (2023) 13(1_suppl):59S–72. doi: 10.1177/21925682221130048
13. de Sire A, Lippi L, Calafiore D, Marotta N, Mezian K, Chiaramonte R, et al. Dynamic spinal orthoses self-reported effects in patients with back pain due to vertebral fragility fractures: a multi-center prospective cohort study. J Back Musculoskelet Rehabil. (2024) 37(4):929–41. doi: 10.3233/BMR-230177
14. Hettchen M, Willert S, von Stengel S, Kohl M, Kemmler W. Effects of the “spinomed active” orthosis on chronic back pain in kyphotic women with osteoporotic vertebral fractures three months and older: a randomized controlled study. Front Pain Res. (2022) 3:1038269. doi: 10.3389/fpain.2022.1038269
15. Kato T, Inose H, Ichimura S, Tokuhashi Y, Nakamura H, Hoshino M, et al. Comparison of rigid and soft-brace treatments for acute osteoporotic vertebral compression fracture: a prospective, randomized, multicenter study. J Clin Med. (2019) 8(2):198. doi: 10.3390/jcm8020198
16. Kim H-J, Yi JM, Cho HG, Chang BS, Lee CK, Kim JH, et al. Comparative study of the treatment outcomes of osteoporotic compression fractures without neurologic injury using a rigid brace, a soft brace, and no brace: a prospective randomized controlled non-inferiority trial. J Bone Joint Surg Am. (2014) 96(23):1959–66. doi: 10.2106/JBJS.N.00187
17. Li M, Law SW, Cheng J, Kee HM, Wong MS. A comparison study on the efficacy of SpinoMed® and soft lumbar orthosis for osteoporotic vertebral fracture. Prosthet Orthot Int. (2015) 39(4):270–6. doi: 10.1177/0309364614528204
18. Meccariello L, Muzii VF, Falzarano G, Medici A, Carta S, Fortina M, et al. Dynamic corset versus three-point brace in the treatment of osteoporotic compression fractures of the thoracic and lumbar spine: a prospective, comparative study. Aging Clin Exp Res. (2017) 29(3):443–9. doi: 10.1007/s40520-016-0602-x
19. Murata K, Watanabe G, Kawaguchi S, Kanaya K, Horigome K, Yajima H, et al. Union rates and prognostic variables of osteoporotic vertebral fractures treated with a rigid external support. J Neurosurg Spine. (2012) 17(5):469–75. doi: 10.3171/2012.7.SPINE122
20. Pfeifer M, Begerow B, Minne HW. Effects of a new spinal orthosis on posture, trunk strength, and quality of life in women with postmenopausal osteoporosis: a randomized trial. Am J Phys Med Rehabil. (2004) 83(3):177–86. doi: 10.1097/01.PHM.0000113403.16617.93
21. Pfeifer M, Kohlwey L, Begerow B, Minne HW. Effects of two newly developed spinal orthoses on trunk muscle strength, posture, and quality-of-life in women with postmenopausal osteoporosis: a randomized trial. Am J Phys Med Rehabil. (2011) 90(10):805–15. doi: 10.1097/PHM.0b013e31821f6df3
22. Valentin GH, Pedersen LN, Maribo T. Wearing an active spinal orthosis improves back extensor strength in women with osteoporotic vertebral fractures. Prosthet Orthot Int. (2014) 38(3):232–8. doi: 10.1177/0309364613497393
23. Kweh BTS, Lee HQ, Tan T, Rutges J, Marion T, Tew KS, et al. The role of spinal orthoses in osteoporotic vertebral fractures of the elderly population (age 60 years or older): systematic review. Global Spine J. (2021) 11(6):975–87. doi: 10.1177/2192568220948036
Keywords: osteoporotic vertebral fractures (OVFs), spinal orthoses, pain management, functional improvement, quality of life
Citation: Borg MB, Battaglia M, Invernizzi M and Baricich A (2024) Efficacy of different spinal orthoses for pain management, functional improvement, and quality of life in osteoporotic vertebral fractures: a mini review. Front. Rehabil. Sci. 5:1506279. doi: 10.3389/fresc.2024.1506279
Received: 4 October 2024; Accepted: 9 December 2024;
Published: 23 December 2024.
Edited by:
Fan Gao, University of Kentucky, United StatesReviewed by:
Wolfgang Kemmler, Institute of Radiology University Hospital Erlangen, GermanyCopyright: © 2024 Borg, Battaglia, Invernizzi and Baricich. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: M. B. Borg, MjAwMDQwOThAc3R1ZGVudGkudW5pdXBvLml0
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.