 Maurice Douryang
Maurice Douryang Lervasen Pillay2
Lervasen Pillay2 Calogero Foti
Calogero Foti
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
OPINION article
Front. Rehabil. Sci. , 16 July 2024
Sec. Strengthening Rehabilitation in Health Systems
Volume 5 - 2024 | https://doi.org/10.3389/fresc.2024.1442626
Rehabilitation 2030 is a World Health Organization (WHO) concept for the development of a new initiative and vision on rehabilitation. This has stemmed from the profound unmet need for access to rehabilitation services and research, also in the field of primary healthcare, for a range of disabling acute, acute-on-chronic, and chronic conditions worldwide (1). As part of Universal Health Coverage (UHC), rehabilitation is a key component of the healthcare system. Prioritising rehabilitation will reduce the burden of disability. The WHO aims to goad world leaders and stakeholders to strengthen their healthcare systems to provide high-quality rehabilitation services. The aims of the WHO initiative are being partially realised in many regions of the world, and most health-related issues involve rehabilitation. In Africa, the increase in the incidence of disability is alarming due to (1) traffic and workplace accidents, (2) complications of medical interventions, (3) natural disasters and conflicts, (4) poor access to education, (5) communicable diseases (e.g., malaria, poliomyelitis, and leprosy), and (6) non-communicable diseases (e.g., diabetes, hypertension, and cancer). This begs the question about the effectiveness of the present role of rehabilitation in Africa. Is Africa adequately prepared with qualified rehabilitation professionals and is there access to resources to achieve the WHO's rehabilitation action goals by 2030? To answer these questions, we need to identify African-specific challenges and should aim to address them.
Disability is defined as a difficulty or inability to perform various activities in physical or mental functional domains. Examples of these are impairments in seeing, hearing, mobilising, memory, concentration, muscular strength, pain perception, self-care or communication, and problems such as anxiety and depression (1–4). However, these disability-related concepts are still poorly understood on the African continent. The reasons for this are not clear and may be attributed to different views on disability resulting from the cultural and social differences of various countries. An example of such differences can be found in the recent COVID-19 pandemic. Many African countries did not include rehabilitation in their COVID-19 management protocols even at a later stage as the evidence evolved (5). This was possibly due to the low primary care practitioner-to-patient ratio on the continent. Little attention was focused on the consequences of infection (e.g., post-COVID-19 fatigue, postpulmonary infection rehabilitation). Different countries in Africa have different healthcare approaches depending on the prevailing healthcare needs of the communities and access to resources.
In Cameroon, only three categories of disability are recognised: (1) physical, (2) mental, and (3) multiple disabilities, but these are not specified. Chad has specified visual and hearing disabilities for those categories of disability adopted by Cameroon. Disability always poses challenges of acceptance, adaptation, integration, and/or participation in Africa (4). This poor understanding of the condition imposes a burden on African communities and acts as a barrier to improve access to physical and mental rehabilitation.
Several African countries lack appropriate screening policies for disabilities among infants and children (e.g., cerebral palsy, congenital abnormalities) (6). This may be due to disability being perceived by many communities on the African continent as a curse, a manifestation of the forbidden, or an expression of punishment to the family or community (4). These African cultural concepts further burden those with disabilities and make them approach rehabilitation through traditional cultural methods rather than modern medical practices. However, as societies are increasingly exposed to a more Western-like healthcare system, they realise the value of rehabilitation.
This change in thinking will allow healthcare rehabilitation approaches to work in tandem with traditional approaches with a better likelihood of achieving the rehabilitation goals, as envisioned by the WHO, by 2030.
Education is a key strategy for advancing quality rehabilitation services worldwide. However, there is a paucity of physical and rehabilitation medicine curricula within the academic environment of the majority of African countries (4). Despite this fact, some universities and institutions do offer qualifications in fields such as physiotherapy, speech therapy, biokinetics, occupational therapy, orthotics/prosthetics, and psychology (3, 4). But these programs are limited in Africa. Undergraduate medical training curriculums leave clinicians underprepared in efficiently prescribing exercise-based rehabilitation. A healthcare practitioner interested in rehabilitation training will need to attend some courses or pursue postgraduate qualifications to develop exercise prescription skills. The present level of training focuses only on the prescription of common medications and not on lifestyle changes.
Therefore, it will be crucial and imperative to adapt healthcare practitioner training to include the use of exercise and rehabilitation as a primary and secondary prevention and treatment tool in Africa and promote the development of rehabilitation and movement sciences.
Rehabilitation research is limited in Africa compared with other regions in the world. Research performed on other continents with different resource availabilities and accesses cannot be duplicated in all countries of the African continent because of the heterogeneity of professionals available and resources that can be accessed. There needs to be an African solution for an African problem—which will be more conducive to evidence-based practice implementation and dissemination on the African continent. Africa has obstacles not identified by other types of research in other countries (4). Some parts of Africa have barriers to including technology in rehabilitation. These include, amongst others, (1) education on its use and the significance of its findings, (2) cost factors for access, (3) affordable access to the internet, and (4) socio-cultural effects. Benefits may be had in developing an African Rehabilitation Council for all African countries. Strategically teaming with international collaborators would prove advantageous to the continent in terms of sharing knowledge.
Advances in technology, such as in the fields of artificial intelligence and telemedicine, appear to offer potential opportunities to bridge rehabilitation gaps and enable good strategies for expanding assisted and remote rehabilitation. However, the reliance of these technologies on internet connectivity may prove to be a challenge in some countries in Africa.
For these reasons, Africa needs to embrace technological innovation to advance rehabilitation by mobilising the necessary resources. Developing a disability map to identify areas that require rehabilitative services may help in implementing strategies.
High-quality rehabilitation services are costly due to the cost of treatments, the use of equipment, and the time spent on the rehabilitation process (3). While the majority of the African population face the challenge of extreme poverty and are devising ways and means to overcome this challenge almost on a daily basis, they do not pay attention to their medical expenses (including rehabilitation expenses), and as a result, these tend to be neglected (7).
Survivors from conflicts or other medical-related issues are often left with long-term disability. This adds to further medical costs and economic strain on families and communities. These financial challenges may be the reasons why the issue of rehabilitation is approached in traditional cultural ways rather than from a medical perspective.
The leadership and governance of the national healthcare systems of African countries focus on financing disease treatment via medication only when healthcare system infrastructure and the development of disease prevention strategies are overlooked (8). However, prevention should be one of the main ways to tackle non-communicable diseases and rehabilitation should be done after one contracts a communicable disease. These are of particular value in a low-income country where there is healthcare resource limitation. Health insurance is a luxury for many Africans. Contrastingly on other continents, strategies have been formulated for providing health cover for all without any discrimination (7). With most Africans either employed in the informal economic sector or unemployed, it would be imperative to include the costs of the different aspects of rehabilitation if individual governments intend providing health insurance, which will help further increase the relevance of Universal Health Care. A discussion on how to overcome existing financial barriers and expand health insurance coverage for all on the African continent is beyond the scope of this article, but any discussion that deals with the aforementioned points and helps improve access to appropriate rehabilitation measures for the population will always be useful at any given time.
Therefore, community-based rehabilitation programs can be developed for different conditions prevailing in this country, but they need to be supplemented by effective governance, available resources, expertise, and community participation.
Non-communicable diseases in Africa highlight shortcomings in health systems both at a social and at a welfare level (8). Physical activity is an appropriate (9), cost-effective, and evidence-based strategy to prevent and manage chronic diseases and promote health. Healthcare professionals involved in this field should be encouraged to join and develop effective nationally led systems and must be supported through policy so that these strategies could become effective.
With the 10-point call to action statement that we have suggested in Table 1, we are confident that countries in Africa can improve the response to disabilities and undertake appropriate rehabilitation.
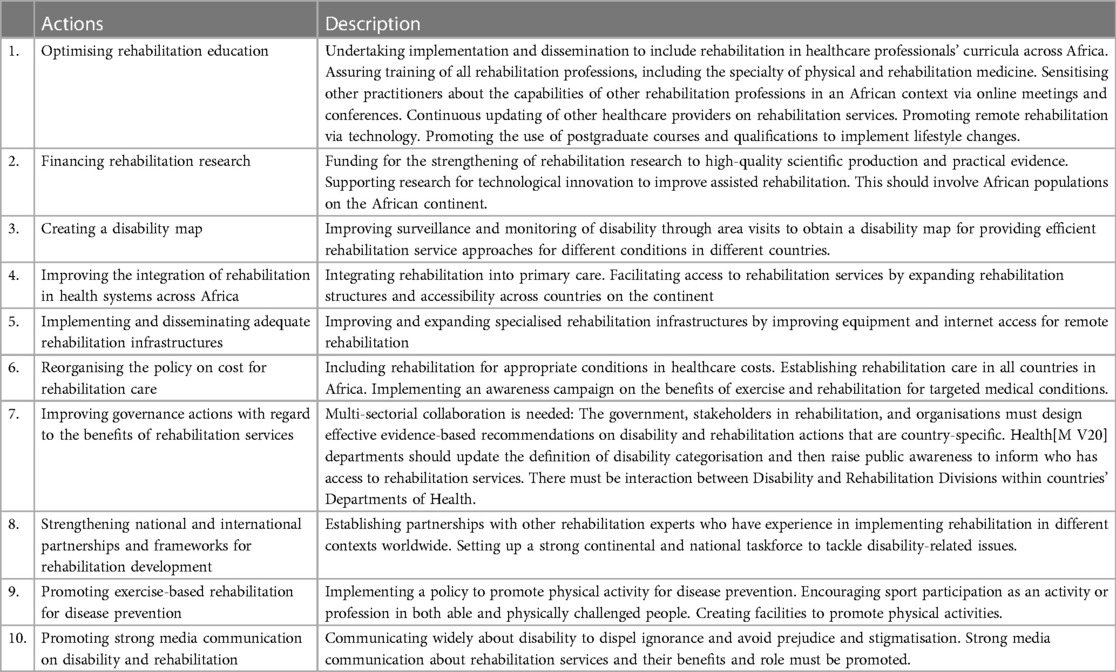
Table 1 Ten key strategic actions for Africa to achieve the WHO Rehabilitation 2030 goals.
The development of rehabilitation care is challenging worldwide. Africa has additional complex contextual barriers to the implementation and expansion of rehabilitation. These include a lack of educational programs, limitation of rehabilitation integration in healthcare systems, poverty, difficulties in accessing rehabilitation in primary care, misperception of disability and rehabilitation, lack of a disability map, limited research funding, poor or absent policies, and poor government support. To significantly contribute to the future of rehabilitation as expected by the WHO, Africa needs to take concrete actions such as those suggested in our proposed 10-point Action Plan.
MD: Conceptualization, Investigation, Writing – original draft, Writing – review & editing. LP: Writing – review & editing, Investigation, Writing – original draft. NM: Writing – review & editing, Investigation, Writing – original draft. CF: Conceptualization, Writing – original draft, Writing – review & editing.
The authors declare that no financial support was received for the research, authorship, and/or publication of this article.
We would like to thank Carlotte Kiekens, MD, FEBPRM, for her suitable revision of the manuscript.
NM is the executive director of NtombiSport.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. World Health Organization. The Need to Scale up Rehabilitation. No. WHO/NMH/NVI/17.1. World Health Organization (2017). Available online at: https://ap–ps.who.int/iris/bitstream/handle/10665/331210/WHO-NMH-NVI-17.1-eng.pdf. (Accessed April 08, 2024).
2. Taylor R, Zwisler AD, Uddin J. Global health-care systems must prioritise rehabilitation. Lancet (London, England). (2021) 396(10267):1946–7. doi: 10.1016/S0140-6736(20)32533-2
3. Seijas V, Kiekens C, Gimigliano F. Advancing the world health assembly’s landmark resolution on strengthening rehabilitation in health systems: unlocking the future of rehabilitation. Eur J Phys Rehabil Med. (2023) 59(4):447–451. doi: 10.23736/S1973-9087.23.08160-1
4. Cannata G, Douryang M, Ljoka C, Giordani L, Monticone M, Foti C. The burden of disability in Africa and Cameroon: a call for optimizing the education in physical and rehabilitation medicine. Front Rehabil Sci. (2022) 3:873362. doi: 10.3389/fresc.2022.873362
5. Tessema SK, Nkengasong JN. Understanding COVID-19 in Africa. Nat Rev Immunol. (2021) 21(8):469–470. doi: 10.1038/s41577-021-00579-y
6. Donald KA, Samia P, Kakooza-Mwesige A, Bearden D. Pediatric cerebral palsy in Africa: a systematic review. Semin Pediatr Neurol. (2014) 21:30–5. doi: 10.1016/j.spen.2014.01.001
7. Kibu OD, Kepgang E, Sinsai R, Conner A, Asahngwa C, Ngwa W, et al. Barriers and motivations for health insurance subscription among health-care users in Cameroon. J Surg Res. (2024) 293:158–167. doi: 10.1016/j.jss.2023.09.010
8. Douryang M, Tsafack Nanfosso KJ, Bouba Y. Physical activity for health promotion and disease prevention in Africa and Cameroon: a call to action. J Phys Act Health. (2023) 20(8):680–682. doi: 10.1123/jpah.2023-0172
9. Ar H. ACSM’s Guidelines for Exercise Testing and Prescription. 11th edn. American College of Sport Medicine (2024). Available online at: https://www.acsm.org/education-resources/books/guidelines-exercise-testing-prescription (Accessed May 12, 2024).
Keywords: WHO, rehabilitation 2030, health system, African region, strengthening
Citation: Douryang M, Pillay L, Mkumbuzi NS and Foti C (2024) The World Health Organization's Rehabilitation 2030 vision: an African perspective. Front. Rehabil. Sci. 5:1442626. doi: 10.3389/fresc.2024.1442626
Received: 2 June 2024; Accepted: 26 June 2024;
Published: 16 July 2024.
Edited by:
Christina-Anastasia Rapidi, General Hospital of Athens G. Genimatas, GreeceReviewed by:
Sara Laxe, Hospital Clinic of Barcelona, Spain© 2024 Douryang, Pillay, Mkumbuzi and Foti. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maurice Douryang, bWF1cmljZS5kb3VyeWFuZ0B1bml2LWRzY2hhbmcub3Jn
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.