 Yuanping Zhao
Yuanping Zhao Hong Xie2*
Hong Xie2* Jianan Li
Jianan Li
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Rehabil. Sci. , 22 April 2024
Sec. Disability, Rehabilitation, and Inclusion
Volume 5 - 2024 | https://doi.org/10.3389/fresc.2024.1384698
Background: In the previous research, the Disability Assessment Scale based on ICF had been constructed for LTC insurance in China. To apply this scale in further studies, it is essential to establish assessment standards for disability levels.
Objective: To establish standardized disability classification criteria and identify the disability statuses and levels in older people.
Methods: This is a cross-sectional study, in which 1,610 older individuals in 15 long-term care institutions in China were assessed by the disability assessment scale based on ICF. Cluster analysis was used for classification of the disability levels. Mean (SD) and median (IQR) were used to describe the scores for each item and each dimension.
Results: The total scores of the disability assessment scale were classified into six disability levels. The overall disability level of the 1,610 participants was moderate-to-severe. The disability in the dimension of “self-care ability and activity” was the most obvious and severe.
Conclusion: The Disability Assessment Scale is capable of identifying disability statuses and levels of older people, and it can serve as a valuable tool for investigating the disabilities among old people and for conducting cross-national comparisons of disability levels.
The phenomenon of global population aging has been rapidly accelerating in recent years, which brings huge social and medical problems. The global population aged 65 or above was estimated at 761 million in 2021, and is projected to double by 2050, reaching approximately 1.6 billion (1). By the end of 2023, China, as the most populous country in the world, had a quarter of the global older population, which reached 217 million and accounted for 15.4% of the total population (2). As the health gradually declines with age, the number of older people with disability is gradually increasing; the number of disabled older people has now reached 40.63 million in China (3). The out-of-pocket expenses for long-term care services among disabled older people are substantial, posing unprecedented challenges to China. In response to this issue, the Chinese government implemented long-term care (LTC) insurance in 15 cities in 2016 (4). An appropriate assessment tool is the foundation for determining the correspondence between physical conditions and care services required, and could pave the way for improved LTC services (5).
Worldwide, the Barthel Index is the most widely used tool for assessing disabilities in older people (6), while there are still various assessment tools being utilized in different countries, such as the International Resident Assessment Instrument (Inter RAI) in the US (7), “Questionnaire for Identification of Nursing Care” in Japan (8), the Aged Care Funding Instrument (ACFI) in Australia (9) and the National Assessment Standard (known as the NBA) in Germany (10). However, there are several limitations in these disability assessment tools. Firstly, the Barthel Index simply applies the activities of daily living to the disability assessment of older people, lacking of comprehensive evaluation on multiple dimensions. Secondly, some of the tools contain disease diagnosis and medical treatments that not directly related to functioning or disability. Thirdly, some assessment tools, such as Inter RAI, contain excessively complex items, leading to cumbersome evaluations. Furthermore, the differences of LTC insurance policies across different countries renders these assessment tools insufficiently rigorous and applicable for direct use in disability assessment in China.
The International Classification of Functioning, Disability, and Health (ICF) is a classification of health and functioning framework (11, 12). In the ICF, functioning and disability are viewed as a complex interaction between an individual's health condition and the contextual factors of the environment, as well as personal factors (13). In the preliminary research, our team had constructed a disability assessment scale for long-term care insurance based on ICF, which showed a good level of reliability and validity (14). A scientific disability level classification standard is required for applying the disability assessment tool in China. The study aims to scientifically classify the disability levels of disabled older people with this disability assessment scale and describe the disability characteristics of the elders. After collecting disability data on older people in China, LTC service levels and contents can be reasonably distributed, and the relevant information can facilitate the development of LTC insurance standards, helping alleviate the burden of the aging population effectively.
This cross-sectional observational study investigated older people living in 15 insurance-designated LTC institutions (including both nursing and community homecare sections) in China from April 2018 to May 2018. Using stratified sampling method, 8 pilot cities were selected considering the distribution of pilot cities in eastern, western, southern and northern China in which 2 pilot cities were randomly selected respectively. One to two representative institutions (with necessary facilities and adequate occupancy rate) were selected from each city. This study used stratified sampling to select older people from self-care and disabled areas in each institution.
Older people were included in the study based on the following well-defined inclusion criteria: (1) aged ≥60 years; (2) resided in nursing institutions or community homecare; (3) provided informed consent. The exclusion criteria comprised inability to participate due to diseases or personal reasons. A total of 1,699 older individuals were given questionnaires and 1,610 questionnaires were returned and valid. The response rate was 94.76% and the effectiveness rate was 100%.
The Disability Assessment Scale consists of two parts: (1) General information section, including basic information such as gender and age; (2) Disability Assessment Scale section, which consists of 20 items in ICF. The score for each item is based on the Numerical Rating Scale (NRS) to determine the disability level, which ranges from 0 to 10. The higher the item scores, the more severe the disability is. Based on this, we divided the continuous scores (0–10 points) for each item into 5 levels: 0 (no problem), 1–3 (mild problem), 4–6 (moderate problem), 7–9 (severe problem), and 10 (complete problem). Specific evaluation rules for each level of each item were designed detailedly. The final score was calculated by adding up each item on the scale, which was higher in the higher level of disability in individual cases.
In the preliminary research, the Disability Assessment Scale showed good reliability and validity (14). The 20 items in the Disability Assessment Scale were divided into three dimensions: self-care ability and activity (11 items), emotion and spirit (4 items), and cognition and perception (5 items). The Cronbach's coefficient and split-half reliability of the scale were 0.969 and 0.877. The calibration validity of the scale and SF-12 were good (rPCS = −0.596, rMCS = −0.332, p < 0.001).
The older people were evaluated in the institutions by specially trained assessors. And then assessors filled in the Disability Assessment Scale on designed app. Researchers were responsible for data review and extraction.
SPSS 20.0 was used for data analysis. Mean [standard deviation (SD)] and median [interquartile range (IQR)] were used to describe the scores for each item and each dimension. Cluster analysis was used for classification of the disability levels.
A total of 1,610 older individuals were assessed. Their ages ranged from 60 to 105 years, with a mean age of 81.5 (58.71) years. Other characteristics were shown as in Table 1.
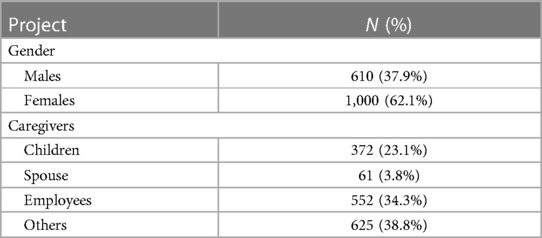
Table 1. Sample characteristics (n = 1,610).
The mean (SD) of the Disability Assessment Scale was 108.49 (54.32), the median (IQR) of the Disability Assessment Scale was 115 (60,157), and the average of the mean (SD) per item was 5.42 (2.72). It can be summarized that the overall disability level of the 1,610 older individuals was moderate–to-severe. From the perspective of the mean per item of dimensions and the sequence, the three dimensions were sorted in order as follows (from more severe to less severe): self-care ability and activity (mean per item was 5.97), emotion and spirit (mean per item was 5.00), and cognition and perception (mean per item was 4.64) (Table 2). From the perspective of the mean score of item and the sequence, the serious degrees of disability existed in “b455 Activity endurance” (7.03), “d510 Washing oneself” (6.78), “d520 Caring for one's body parts” (6.78), “d230 Daily routine” (6.57), “d450 Walking” (6.40) and “d455 Non-walking movement” (6.13), while the minor degrees of disability were “b525 Defecation” (4.82), “b280 Pain” (4.53), “d550 Eating” (4.19), “b210 Vision” (4.11) and “b230 Hearing” (4.00) (Table 3).
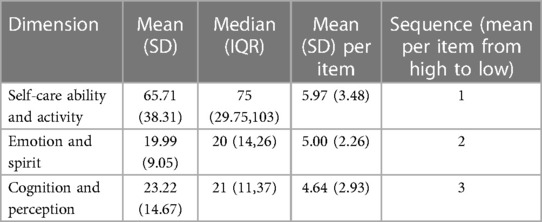
Table 2. Dimension-related results (n = 1,610).
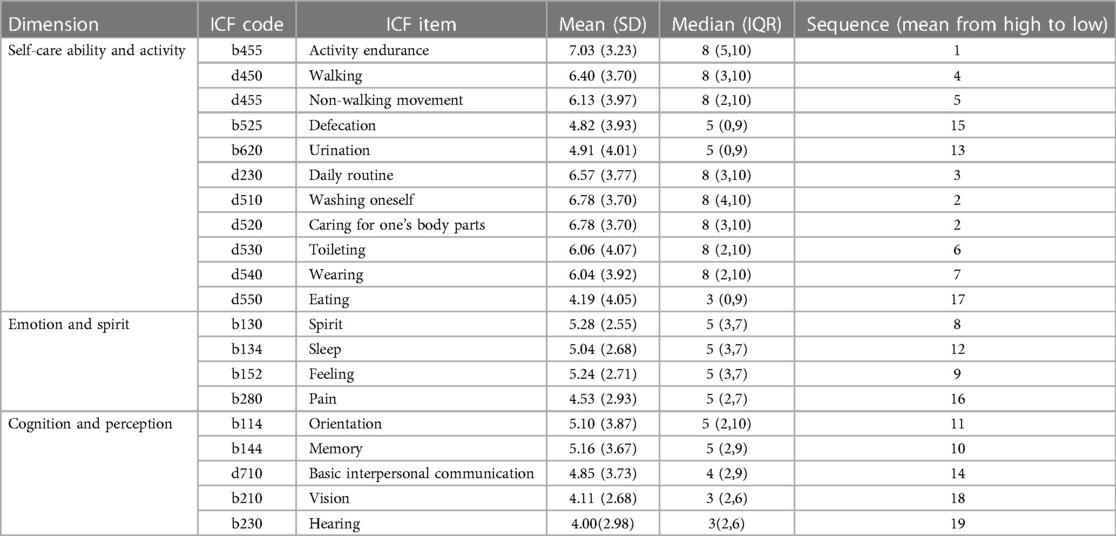
Table 3. Item-related results (n = 1,610).
Clustering analysis (15) was carried out on the total score of the Disability Assessment Scale. A cluster tree diagram was cut out using the 2.5 distance between classes. In our study, total disability scores were divided into five levels: level I (scores of 0–42), level II (scores of 43–92), level III (scores of 93–124), level IV (scores of 125–148), and level V (scores of 149–200), which were designated as mild, moderate, moderate-to–severe, severe, and complete disability, with a score of 0 indicting total self-care.
The number and proportion of older people in different disability levels are shown in Table 4, with the largest number in level Ⅴ and the smallest number in level 0. Dimension and item scores for each disability level are shown in Tables 5, 6. As shown in Tables 5, 6, we can clearly see the differences in each dimension and item score by disability level. From level Ⅰ to level Ⅴ, the per item score of each dimension and score of each item gradually increased, indicating that as the disability level increases, the disability degree of each dimension and item in disabled elders gradually became more severe. Comparing different dimensions, in the mild and moderate disabilities, the most severe disability was reflected in the emotion and spirit aspects. While in the moderate-to-severe and more severe disabilities, the degree of disability in terms of self-care ability and activity was the most severe. Similarly, we can identify differences in the characteristics of disability items at a certain level of disability, as well as differences in disability items among individuals at different levels of disability.

Table 4. Number and proportion of older people in different disability levels (n = 1,610).

Table 5. Dimension scores for different disability levels [mean (SD); median (IQR), n = 1,610].
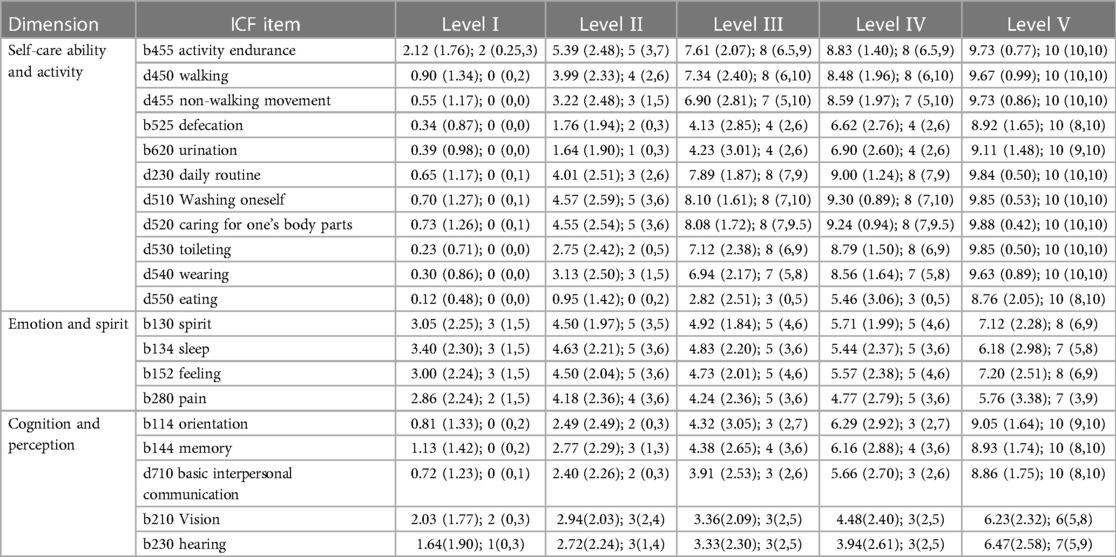
Table 6. Items scores for different disability levels (mean (SD); median (IQR), n = 1,610).
The issue of population aging is a universal challenge confronting all nations and regions. However, due to the different characteristics of national regimes and policies, there is a lack of an effective tool to measure the disability level of older people among different countries and regions. This study developed the Disability Assessment Scale based on the theoretical ICF classification system, encompassing two advantages. On one hand, the ICF is a health and function classification system that uses an international standardized language code, and it can be recognized and applied throughout the world (16). In this way, our tool is a cross-nation, cross-regional and cross-cultural assessment tool which may be used to measure and compare disability levels among different countries. On one other hand, as ICF can be used across all diseases and health problems, our tool can reflect different clinical outcomes by differences of disability levels. And the results can be used as the basis for an integrated model of medicine, rehabilitation and nursing.
In this study, 20 items were selected from the ICF, covering the disabilities of the human body in the eight functional areas of active ability: self-care ability, sleep and mental status, emotion, pain, interpersonal communication, social, cognitive and sensory ability. These areas are comprehensive and essential, and may be considered an ICF core set for disabled older people. In addition, we categorized the 20 ICF items into three dimensions, each of which can be used as an assessment combination for evaluating a specific aspect of disability. ICF researchers (17) recommend using an NRS to assess the problem severity for each ICF item. The meanings represented by both extremes of the NRS scores, namely 0 and 10, are universally applicable (and similar to the meanings of 0 and 10, respectively, in the Numeric Pain Rating Scale), so an NRS can be used for all ICF items and easily understood by assessors.
Based on Disability Assessment Scale scores, we can understand the physical and mental conditions of older people. According to the overall assessment data, the disability of older people was mainly reflected in issues with self-care ability and activity. The decline of motor function is more pronounced in older individuals with disabilities, and more attention should be paid to the maintenance and training of integral motor system in disability intervention. This highlights the key points of LTC. LTC services should focus more on the comprehensive care of older people, while giving consideration to their cognitive perception regarding rehabilitation and emotional and psychological comfort.
Clustering has the advantages of not determining the number of clusters beforehand, flexibly controlling the clustering granularity, and clearly expressing the hierarchical relationship between classes. By the clustering method, the older people were divided into six disability levels based on Disability Assessment Scale scores. From level Ⅰ to Ⅴ, the mean score of each dimension and item gradually increased, which showed the feasibility of the disability level classification. Also, we can identify the disability characteristics of individuals with different levels of disability and provide targeted interventions to prevent and delay the progression of disability. In level Ⅰ and level Ⅱ, we should pay attention to the care of emotion and spirit. While in the level Ⅲ and above, we should pay more attention to the care of self-care ability and activity.
By comparing tools for the assessment and classification of LTC for older people in other countries, we can conclude that each country has a slightly different classification method based on their tool's characteristics and the country's social security levels. There are three classification methods. The first method, which is used in Japan and the US, involves a rating system software where the assessment results are entered and it can display the disability level simultaneously. For example, Japan's Department for LTC Insurance (8) designed a rating system software to identify the level of care requirements based on “Questionnaire for the Identification of Nursing Care”. The care requirements are divided in to three levels: self-reliant, support required (type 1 or 2) and care required (type 1, 2, 3, 4, 5). The second method, which is used in Germany, is to add up the total scores of each dimension, taking into account the weight of each dimension. Germany (10) weights each dimension of NBA as follows: dimension 1 accounts for 10%, dimension 2 and 3 account for 15%, dimension 4 accounts for 40%, dimension 5 accounts for 20%, and dimension 6 accounts for 15%. According to the total score, the older people are divided into five levels of disability: 15–29, 30–49, 50–59, 60–89 and ≥90, which are designated independent level 1–5 respectively. The third method, which is used in Australia, is to combine the results of each dimension to obtain the disability level of older people without weighting. Australia (9) designed each dimension of ACFI so it can be divided into H, M, and L according to the total score for the items of each dimension. The combination of the three levels in three dimensions divide disabled old people into a high or low care level. The classification method of the Disability Assessment Scale in this study belongs to the second category and does not consider the weight of each dimension, which makes it more direct and time-efficient when determining disability levels.
The ICF-based Disability Assessment Scale can be used as a screening tool for older people in China. It is well known that China has a large number of older people and a poor level of social security. The tool was designed with a simple structure to facilitate basic screening of functional levels in older people in China, aiming to optimize the allocation of LTC resources in a more rational and efficient manner. Based on the Disability Assessment Scale, the next step is to design a more detailed assessment tool. In previous surveys of the disability in China, such as the Chinese Urban and Rural Older People Tracking Survey, Chinese Follow-Up Investigation on Influential Factors of Longevity and Health, Chinese Health and Old-Age Care Survey, and the Seventh National Population Census, the assessments were solely focused on the performance of activities of daily living (18). In contrast, the Disability Assessment Scale in this study is more comprehensive and standardized, making it more practical for conducting large-scale investigations.
Also, the ICF-based tool may be used to assess disability across national populations. It is well known that the International Classification of Diseases (ICD) (19) is the international unified disease classification method published by the WHO. The ICD standardizes disease names and helps to make disease information as widely shared as possible in order to reflect countries’ health situations. After issuing the ICD, the WHO issued the ICF as the international unified functioning classification system. The ICF and ICD are the two major health classification systems published by the WHO. The ICD can only reflect the classification of etiological diagnoses such as disease and injury, but these diseases may increase the risk of disability after clinical treatment, causing additional expenses that cannot be compensated by medical insurance. The ICF can be used to reflect post-acute and convalescent disability and it promotes the linkage of medical care and LTC, the medical maintenance and the realization of an integrated health strategy. Due to health conditions, older people may be sent to different care institutions, such as hospitals, nursing homes and convalescent homes where elders may face repeat assessments. Using the Disability Assessment Scale, the information can be accessed with the agreement of individuals, and a people-centered care system will be promoted.
In the field of disability assessment, the international community used to focus more on the decline of physical function when evaluating disability in elders, which was particular evident in the assessment of the Barthel index. In recent years, researchers have gradually focused on various aspects of disability such as cognitive function, contributing to the development of comprehensive assessment tools. The decline in physical function among older individuals is more obvious and receive more social attention, while the cognitive decline such as Alzheimer's disease is initially coming into people's mind. The weight of physical and cognitive functions should be continuously adjusted according to national conditions, changes in the spectrum of diseases, and other complex factors.
The Disability Assessment Scale can describe the overall level of disability among older people, and long-term care insurance can provide protection for some disabilities based on their disability levels. However, specific populations, such as elders with only cognitive disability but good physical function, may not be covered by long-term care insurance. Therefore, special attention needs to be paid to this group. One possible solution is to build an additional pathway for dementia assessment to evaluate cognitive function, which can come to an additional score as a supplementary assessment. If the elders failed to be evaluated as severe or complete disability in the first-round assessment, they can be also considered as severely dementia elders with severe problems both in “b114 Orientation” and “b144 Memory” (score ≥7 points). The limitation of the research is that the existing data cannot verify the rationality of grouping. Therefore, we are collecting data on care services of disabilities in current research and the rationality of grouping disabilities will be verified through the different burden of care needed.
In this study, the sampling method and sample size represent study limitations. In a future study, we need to conduct stratified and phased sampling, using stratification variables such as the number of beds in each LTC institution and the urban characteristics of the cities where the LTC institutions are located.
In this study, the Disability Assessment Scale developed based on the ICF is capable of identifying the disability status and classifying the level of disability in older individuals. Based on the assessment scores of the tool, the LTC insurance funds and other resources in China can be reasonably distributed. At the same time, the tool is internationally standardized and simple, and can therefore be used for large-scale disability investigations in China and comparisons of older persons’ disability levels between countries.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding authors.
The studies involving humans were approved by the biomedical ethics committee of Peking University (no. IRB00001052-18047). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
YZ: Writing – original draft. HX: Writing – original draft, Writing – review & editing. KW: Writing – review & editing, Data curation, Investigation. SL: Validation, Writing – review & editing. JY: Resources, Writing – review & editing. JL: Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article.
This study was supported by Research project of the Medical Security Professional Committee of the Chinese Society of Social Security, sponsored by Taikang Pension Insurance Co., Ltd. (Y2017003) and Beijing Social Science Foundation Project (15SHA006).
This paper is the result of research directed by the Medical Security Professional Committee of the Chinese Society of Social Security. The authors wish to acknowledge the sponsorship of Taikang Pension & Insurance Co., Ltd. The authors also wish to thank the 15 LTC institutions for their support in the implementation of the project.
The authors declare that this study received funding from Taikang Pension Insurance Co., Ltd. The funder had the following involvement in the study: data collection.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. United Nations Department of Economic and Social Affairs. World Social Report 2023 (2023). (updated June). doi: 10.18356/9789210019682
2. National Bureau of Statistics. Statistical Bulletin on National Economic and Social Development of the People’s Republic of China in 2023 (2024). Available online at: https://www.stats.gov.cn/sj/zxfb/202402/t20240228_1947915.html (updated February 29).
3. Ministry of Civil Affairs. Results of the Fourth Sampling Survey on the Living Conditions of Older People in Urban and Rural Areas in China (2016). Available online at: http://www.mca.gov.cn/article/xw/mzyw/201610/20161015001974.shtml (updated October 9).
4. Ministry of Human Resources and Social Security of the People’s Republic of China. Guidance of the General Office of the Ministry of Human Resources and Social Security on the Pilot of Long-Term Care Insurance System (2016). Available online at: https://www.gov.cn/xinwen/2016-07/08/content_5089283.htm (updated June 27)
5. Fengyue L, Junko O. Financing elderly people’s long-term care needs: evidence from China. Int J Health Plann Manage. (2018) 33:479–88. doi: 10.1002/hpm.2488
6. Li Q, Li CH, Yue SM. Comparison and reflection on pilot schemes of long-term care insurance system—based on comparative analysis of 15 pilot areas nationwide. J Shandong Agric Univ Soc Sci Ed. (2018) 20:23–30. CNKI:SUN:SDND.0.2018-02-004
7. Centers for Medicare and Medicaid Service. MDS 3.0 for Nursing Homes and Swing Bed Providers (2015). Available online at: https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/NursingHomeQualityInits/NHQIMDS30.html (updated June 3)
8. Residence Hiroshi. What is the Certification for Long-Term Care. Tokyo: Hitotsubashi Publishing Co., Ltd (2004). p. 23–36.
9. Australian Government Department of Health. Aged Care Funding Instrument (ACFI) Reports (2019). Available online at: https://agedcare.health.gov.au/tools-and-resources/aged-care-funding-instrument-acfi-reports (updated March 7)
10. Büscher A, Wingenfeld K, Schaeffer D. Determining eligibility for long-term care-lessons from Germany. Int J Integr Care. (2011) 11:e019. doi: 10.5334/IJIC.584
11. Johansen T, Kvaal AM, Konráðsdóttir ÁD. Developing and implementing ICF-based tools for occupational rehabilitation supporting the communication and return to work process between sickness absentees, clinical team and job centre contacts. Front Rehabilit Sci. (2022) 3:830067. doi: 10.3389/fresc.2022.830067
12. Afghah T, Alfakir R, Meis M, van Leeuwen L, Kramer SE, Hammady M, et al. The development of a self rated ICF-based questionnaire (HEAR-COMMAND tool) to evaluate hearing, communication, and conversation disability: multinational experts’ and patients’ perspectives. Front Rehabilit Sci. (2022) 3:1005525. doi: 10.3389/fresc.2022.1005525
13. World Health Organization. International Classification of Functioning, Disability and Health. Geneva: World Health Organization (2018). Available online at: http://www.who.int/icf (updated March 2).
14. Li J, Qiu H, Zhang X, Jin J, Zhao Y, Yan J, et al. Validation of a disability assessment tool based on the international classification of functioning, disability, and health in the Chinese context. Front Rehabilit Sci. (2022) 3:855502. doi: 10.3389/fresc.2022.855502
15. Sun ZQ, Wang L. Comprehensive Evaluation Method and its Medical Application. Beijing: People’s Health Publishing House (2014).
16. Leonardi M, Lee H, Kostanjsek N, Fornari A, Raggi A, Martinuzzi A, et al. 20 years of ICF—international classification of functioning, disability and health: uses and applications around the world. Int J Environ Res Public Health. (2022) 19:11321. doi: 10.3390/ijerph191811321
17. Liu S, Reinhardt JD, Zhang X, Ehrmann C, Cai W, Prodinger B, et al. System-wide clinical assessment of functioning based on the international classification of functioning, disability and health in China: interrater reliability, convergent, known group, and predictive validity of the ICF generic-6. Arch Phys Med Rehabil. (2019) 100:1450–7. doi: 10.1016/j.apmr.2018.11.014
18. Xiaoyu M, Ping T. Research progress in disability assessment tools in China. Chin J Mult Organ Dis Elderly. (2023) 22:218–21. doi: 10.11915/j.issn.1671-5403.2023.03.045
Keywords: international classification of functioning, disability and health, long-term care, disability assessment tool, disability level, classification
Citation: Zhao Y, Xie H, Wang K, Liu S, Yan J and Li J (2024) Application of the international classification of functioning, disability, and health to disability assessment for older people in China. Front. Rehabil. Sci. 5:1384698. doi: 10.3389/fresc.2024.1384698
Received: 10 February 2024; Accepted: 3 April 2024;
Published: 22 April 2024.
Edited by:
Brendan McCormack, The University of Sydney, AustraliaReviewed by:
Alessandro Giustini, Chair of Master In Robotic Rehabilitation—University San Raffaele, Italy© 2024 Zhao, Xie, Wang, Liu, Yan and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hong Xie eGg2OTU5QDE2My5jb20= Jianan Li bGlqaWFuYW5AY2FybS5vcmcuY24=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.