
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Rehabil. Sci. , 01 February 2024
Sec. Rehabilitation for Musculoskeletal Conditions
Volume 5 - 2024 | https://doi.org/10.3389/fresc.2024.1318951
 Felipe Alves Machado1*†
Felipe Alves Machado1*† Gustavo J. Almeida2,†
Gustavo J. Almeida2,† André Luiz Maia do Vale1,†
André Luiz Maia do Vale1,† Alexandre Lima de Araújo Ribeiro1,†Graziella França Bernardelli Cipriano3,†
Alexandre Lima de Araújo Ribeiro1,†Graziella França Bernardelli Cipriano3,† Gerson Cipriano Junior3,†Wagner Rodrigues Martins4,†
Gerson Cipriano Junior3,†Wagner Rodrigues Martins4,†
Background: Osteoarthritis (OA) is the most common and prevalent musculoskeletal disease associated with population aging, negatively impacting function and quality of life. A consequence of knee OA is quadriceps muscle weakness. Musculoskeletal rehabilitation using low load exercises, associated with Blood Flow Restriction (BFR) may be a useful alternative to high load exercises when those cannot be tolerated. Several systematic reviews have reported inconclusive results due to discrepancies in study findings, heterogeneity of results, evaluated time points, and research questions explored.
Objective: To perform an overview of systematic reviews with meta-analyses, synthesizing the most recent evidence on the effects of muscle strength training with BFR for knee OA.
Methodology: Systematic reviews that include primary controlled and randomized clinical trials will be considered for inclusion. Articles will be considered only if they present a clear and reproducible methodological structure, and when they clearly demonstrate that a critical analysis of the evidence was carried out using instrumented analysis. Narrative reviews, other types of review, overviews of systematic reviews, and diagnostic, prognostic and economic evaluation studies will be excluded. Studies must include adults aged 40 years and older with a diagnosis of knee OA. Two authors will perform an electronic search with guidance from an experienced librarian. The following databases will be searched: PubMed via MEDLINE, Embase, CENTRAL (Cochrane Central Register of Controlled Trials), PEDro, Cumulative Index to Nursing and Allied Health Literature (CINAHL) via EBSCO host, Web of Science, and the gray literature. The search strategy used in the databases will follow the acronym PICOS (population, intervention, comparison, outcome, and study design). Screening (i.e., titles and abstracts) of studies identified by the search strategy will be selected using Rayyan (http://rayyan.qcri.org). The quality assessment will be performed using the “Assessment of Multiple Systematic Reviews” (AMSTAR-2) tool.
Systematic Review Registration: PROSPERO, CRD42022367209.
Knee osteoarthritis (OA) is a very common and prevalent musculoskeletal chronic degenerative joint disease characterized by pain, swelling, stiffness, bone crepitus, atrophy, and muscle weakness (1), causing alterations in the cartilage metabolism and synovial inflammation, with consequent cartilage deterioration, joint space narrowing, osteophyte formation, subchondral bone sclerosis, and cystic formations (2, 3). It is estimated that OA affects approximately 250 million adults worldwide, with a prevalence correlated to the aging of the population, negatively impacting the function and quality of life of these individuals (4, 5), in addition to burdening the health system with significant costs.
These symptoms and activity limitations have been associated with non-modifiable risk factors, such as age and the female sex, in addition to modifiable factors, such as obesity, low level of physical activity, joint overload, muscle imbalance in the knee joint, and reduced weight and muscle strength in the lower limbs (6–8).
Quadriceps weakness is a characteristic finding of patients with knee OA, especially in older people, due to sarcopenia, affecting physical function through decreased strength and muscle mass (9), vascular function (10), and bone mineral density (11) that occur in aging. This muscle deficit becomes a biomechanical factor that can significantly contribute to the incidence of symptoms of knee OA and the progressive loss of joint cartilage (12–14). Several studies report that individuals with knee OA present with quadriceps muscle weakness (14–20). One study revealed that adequate quadriceps muscle strength prevents the incidence of symptom development in knee OA (13) resulting in functional improvement and decreasing the incidence and/or progression of the disease (21). Therefore, quadriceps strengthening and hypertrophy is considered as a first-line therapy (22, 23), making resistance training a common practice in OA management (23–25).
For the conditioning and muscle development of healthy people, the American College of Sports Medicine recommends a minimum of resistance training loads of 60%–70% of one repetition maximum (1RM) for strength gains, and 70%–85% of 1RM for muscle hypertrophy (26). However, training with these high loads may not be possible or may even be deleterious in individuals with knee OA.
Resistance training with low loads failed to stimulate muscle hypertrophy to the magnitude observed in resistance training with high loads after a period of 6 (27) or 8 (28) weeks, with a frequency of 3 weekly sessions. Strength adaptations were maximized with high load training (27, 28) and muscle cross-sectional area comparisons suggested that the hypertrophy and strength gains seen with low-load training are not as great as those achieved with high load training (29). However, the clinical perspective of musculoskeletal rehabilitation using low loads could be a useful strategy in situations where training using high loads are not feasible, especially in older people with knee OA (30).
Blood flow restriction (BFR) therapy has been shown to be a useful alternative to high load resistance training to improve muscle function in individuals with knee OA. BFR therapy uses inflated cuffs in the proximal region of the thigh, with occlusion pressure between 40% and 90% of the maximum, and low loads around 30% of 1 RM that can produce significant gains in muscle hypertrophy and strength (31–34). Furthermore, with regard to hypertrophy, training with BFR has shown responses comparable to those found in resistance training with high loads (35).
The physiological adaptations of muscle strength (36), and vascular (37) and pulmonary systems (38) have been reported with low-intensity aerobic exercise with BFR. Therefore, from a mechanical point of view, the hypothesis is that, in an ischemic and hypoxic environment generated by partial vascular occlusion, high levels of stress are generated along with the mechanical tension associated with exercise. Both metabolic stress and mechanical strain are described as “primary hypertrophy factors” (39) and speculated to activate other mechanisms for muscle development. These proposed mechanisms include: a systemic increase in hormone production (40, 41), healing cell stimulation (42), production of reactive oxygen species (43, 44), intramuscular anabolic/anti-catabolic signaling (45–47), and increased recruitment of fast-twitch fibers (48–50) that promote muscle tissue development.
With regard to the safety of applying BFR during exercise, in relation to hemodynamic disorders and ischemic reperfusion injury, a systematic review with meta-analysis states that with correct implementation, this technique does not present a greater risk than traditional exercise modes that do not use BFR (30, 50).
To date, a series of systematic reviews and meta-analyses (51–53) have been published investigating the evidence on the effect of muscle strength training with BFR for knee OA. These systematic reviews used various clinical outcomes, such as pain, stiffness, muscle strength and hypertrophy, functionality, mobility, and balance. However, due to discrepancies across study findings, heterogeneity of results, time points assessed, and research questions explored, these systematic reviews have reported inconclusive or contradictory results.
The purpose of this overview is to describe and assess the methodological quality of the current body of systematic reviews with meta-analyses. We will synthesize the best available evidence on the effects of muscle strength training with BFR in patients with knee OA, critically and systematically (see Data synthesis and reporting). This overview will examine the strengths and limitations of current evidence and discuss the applicability to clinical practice and recommendations for future research.
This is an overview of systematic reviews following the recommendations of the Cochrane Handbook (54). As per the Handbook, the unit of searching, inclusion and data extraction is the systematic review, thus we will follow their guidelines. The protocol was written using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocol (PRISMA-P) (55) see Supplementary Material/Appendix 1, and is registered with PROSPERO (CRD42022367209).
All authors contributed to devising the search strategies for each database using a combination of subject headings and free-text keywords. Two authors (FAM and GJA) will perform the electronic search guided by a librarian with experience in database search: PubMed via MEDLINE, Excerpta Medica Database (EMBASE), CENTRAL (Cochrane Central Register of Controlled Trials), PEDro, Cumulative Index to Nursing and Allied Health Literature (CINAHL) via EBSCO host, Web of Science, Epistemonikos and gray literature via ProQuest (Brazilian Digital Library of Theses and Dissertations), and Global ETD Search (Networked Digital Library of Theses and Dissertations).
The search strategy used in all databases will follow the acronym PICOS (Participants, Interventions, Comparison, Outcome and Study Design) using standardized MeSH (Medical Subject Headings) keywords from the MeSH Database of the “National Library of Medicine” and the Boolean operators AND, OR and NOT to combine keywords for addition, alternation, or negation between terms.
To meet our objective, we will search for relevant articles combining the following terms presented in Table 1. No date or language restrictions will be applied to the initial search.
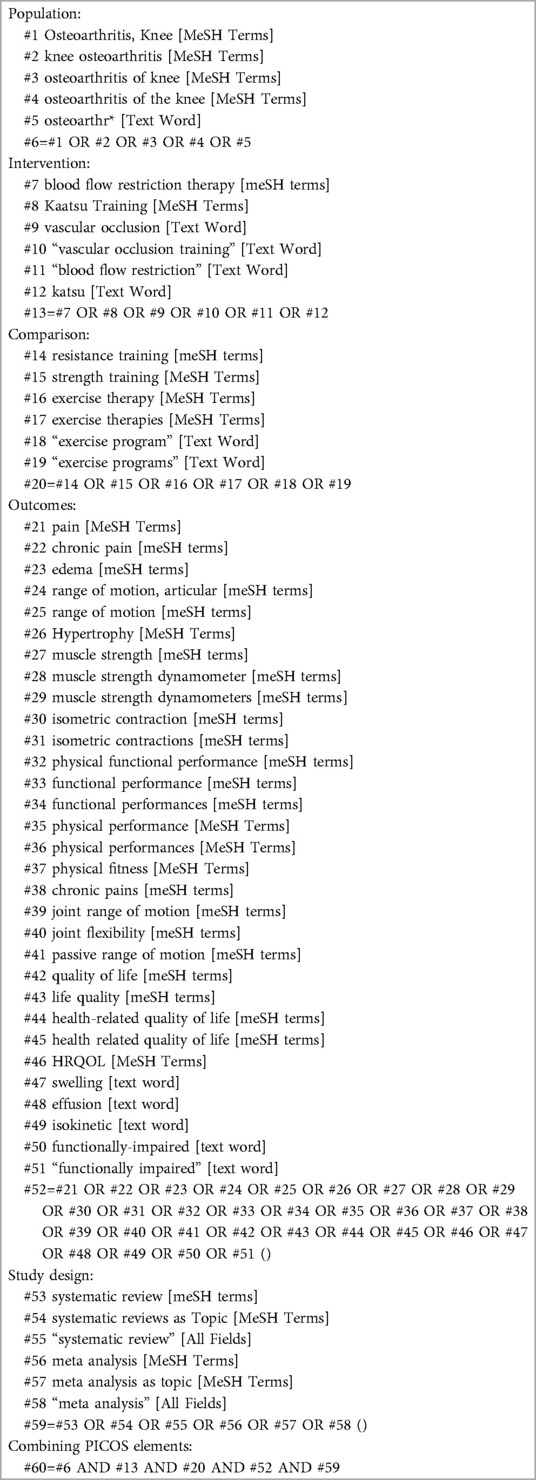
Table 1. Example of search strategy for pubMed via MEDLINE.
The results identified by the search strategy in the databases will be exported and saved into the Rayyan platform (http://rayyan.qcri.org), where two independent and blind reviewers (FAM and GJA) will perform the initial removal of duplicate and non-relevant papers based on the abstracts and titles. A full text will be acquired for those that meet the inclusion criteria. It is important to note that evidence from primary studies will not be considered. At the end of screening in Ryyan, blinding of reviewers will be opened and disagreements in study selection will be resolved by consensus among the initial reviewers and, if necessary, decided by a third reviewer (WRM). The full text documents will then be examined for eligibility. In addition, the reference lists of the selected reviews will be consulted to find possible additional systematic reviews. The anticipated study screening process is shown in Figure 1 and Supplementary Material/Appendix 2.
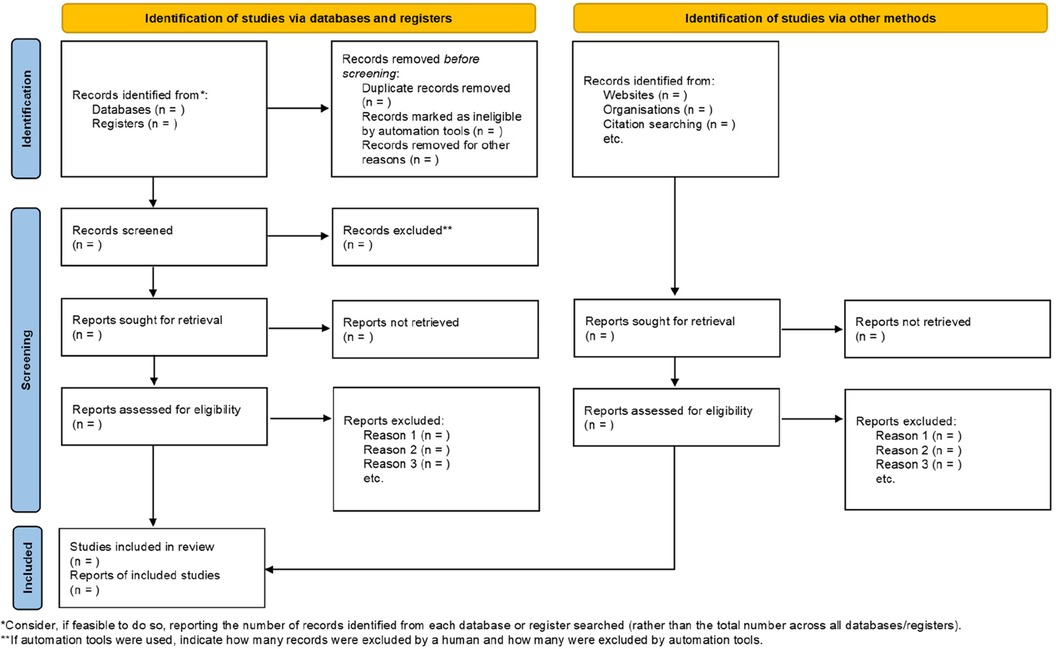
Figure 1. Schematic for PRISMA 2020 flow diagram of the screening process—identification of studies via databases, registers and other methods.
Systematic reviews of studies such as controlled and randomized clinical trials will be included. Articles will be deemed to be systematic reviews if they present a clear and reproducible methodological structure. Also, they must clearly demonstrate that a critical analysis of the evidence was conducted, made available through instrumented analysis [i.e., search strategy, risk of bias, and certainty of evidence and the strength of recommendations via “Grading of Recommendations Assessment, Development and Evaluation” (GRADE)]. Narrative reviews, other types of reviews, and other overviews of systematic reviews will be excluded. Diagnostic, prognosis, and economic evaluation studies will also be excluded.
Studies will be selected that include patients over 40 years based on cartilage lesions in arthroscopy, magnetic resonance imaging evidence of cartilage or meniscus damage, and/or bone marrow lesions of the subchondral bone, symptoms (clinical examination—joint line tenderness and/or crepitus, knee pain without any recent trauma associated with joint stiffness), the presence of clinical risk factors (e.g., family history of OA, metabolic syndrome, malalignment and/or leg length discrepancy), patient reported outcomes [i.e., Knee Injury and Osteoarthritis Outcome score (KOOS) for defining pain and functional limitation], and Kellgren-Lawrence grade 0–1 (56–58).
In addition, the intervention needs to have been performed using strength training with vascular occlusion as a tool during the rehabilitation process. We will exclude studies in which intervention was applied to athletes and/or patients in the postoperative period.
Data extraction will include characteristics of the populations included in each eligible systematic review. This information will be discussed and interpreted accordingly.
We will include systematic reviews that used resistance training with BFR for the quadriceps muscles in open kinetic chain exercises (i.e., leg extension) and closed kinetic chain exercises (i.e., leg press, squat, or semi-squat) in individuals with knee OA. Studies with a weekly frequency of 2 or more treatment sessions for at least 4 weeks will be selected.
The primary outcomes of interest are self-reported pain, knee function, muscle strength, and hypertrophy measured in the short and medium term. When applicable, these results will be summarized according to the type of BFR intervention (e.g., exercise-based rehabilitation programs with BFR using high or low intensity), assessment time point and duration of follow-up (i.e., 4, 6, or 8 weeks after intervention).
Secondary outcomes will include the design of the rehabilitation programs using BFR; details on specific patient populations examined in each included review; rate of adverse events associated with the intervention; and effect of intervention on other outcome domains, such as range of motion and health-related quality of life, when reported.
Data extraction and analysis will be conducted in accordance with the guidelines of the Cochrane Handbook of Systematic Reviews of Interventions. The full texts of included reviews will be retrieved. Two review authors (FAM and GJA) will independently extract descriptive and outcome data from each included review. A third review author (WRM) will arbitrate if discrepancies cannot be resolved by consensus. A bespoke data extraction form will be designed, tested, and used to record review features, including the purpose and rationale, types and numbers of studies included in the review, population(s), intervention(s), comparator(s), results (including beneficial and harmful effects, and reported adverse events), whether or not a meta-analysis was performed and the date of the last search, and methods for evaluating the quality of the studies. In case we include more than one review containing the same studies, we will examine the review question of each article, the comparisons explored, the date of the final search and key aspects of methodological quality (e.g., types of studies included and assessment of risk of bias) and will list the individual studies included in each review. This approach will enable identification of studies included in one review, and not in the other. Using this data, we will determine which of the reviews to include to contribute data to the results, based on the review with most current search strategy that included the most recent trials.
It is possible that the systematic reviews included address a similar research question and the primary studies are the same, so we will take this factor into account in the data analysis. If we find overlapping systematic reviews, we will follow the Cochrane Handbook recommendations to include all non-overlapping systematic reviews and, for a group of overlapping reviews, the most recent, highest quality, most relevant or most comprehensive systematic review will be included (59). Thus, we will avoid double counting of data by ensuring that the findings of each primary study are extracted separately. A citation matrix will be constructed to visually demonstrate the amount of overlapping and the “corrected covered area” will be calculated indicating the degree of overlapping in the overview.
Two reviewers (FAM and GJA) will independently assess the quality of the reports and the methodological quality of the included reviews using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist (60) and the Assessment of Multiple Systematic Reviews (AMSTAR-2) tool (61), respectively. We will report the PRISMA quality ratio (number of items reported/27 checklist items *100%). The AMSTAR-2 contains 16 items that assess the methodology used in a systematic review. Each item is scored as yes, no, partially yes, and not applicable/NA. There is no total score. The presence of failures and weaknesses translates into general confidence in the results of the systematic review. Overall confidence is rated as “critically low”, “low”, “moderate”, or “high”. Based on AMSTAR-2 scores, the quality of the systematic reviews will be classified as high methodological quality (score of 8–11), as medium quality (score of 4–7), and as low quality (score of 0–3) (61).
Data will be presented as a narrative synthesis, with textual commentary supplemented with the use of summary tables and figures to enhance clarity of reporting (62). We will document primary and secondary outcomes of each intervention comparison from the included reviews, as well as the number of studies and number of participants included in each comparison. Data (when reported in the review) will be described as mean difference (or standardized mean difference), 95% confidence intervals, and I2 statistic for heterogeneity (63). We will synthesize key information pertaining to the quality of evidence, and documented eligibility criteria, study characteristics, and the primary outcome of each review. Flow diagrams will be used to summarize the study selection process. Finally, reasons for excluding reviews will be described.
Depending on the amount of information provided by the reviews and number of participants included, we plan to analyze key functional outcomes according to patient characteristics (e.g., age and sex) and intensity of intervention (i.e., BFR associated with high vs. low intensity resistance training).
The findings of this overview of systematic reviews on the effects of BFR in patients with knee OA will potentially have implications for clinical practice, research, and the future development and/or updating of guidelines. Our results are intended to provide greater clarity and synthesis of the available evidence on this intervention technique and its effectiveness to improve symptom-related and functional outcomes in this population. Such information is likely to impact existing and planned resource allocation in the clinical setting, inform the direction of future research, including randomized controlled trials on the effectiveness of BFR training, and support guideline recommendations. The conclusions in this overview will highlight outcomes that demonstrate clear benefits and those for which there is no clear evidence. If sufficient data are available, our findings may also add clarity to the “dose” of the BFR intervention (i.e., type, intensity of exercise load, intensity of vascular occlusion pressure, and duration), as well as circumstances under which any adverse events or harm were reported as a consequence of the intervention.
We plan to strictly follow the approach outlined by the Cochrane Collaboration to undertake an overview of systematic reviews (64). We will note when included systematic reviews are out of date and identify any relevant new studies that have been published after the date of the last reported systematic review search. However, we will not formally consider recent articles not included in previous systematic reviews. We are not planning to undertake a new systematic review within our general framework (64). Our discussion will focus on the current state of evidence related to BFR in patients with knee OA based on systematic reviews.
The proposed overview will summarize the current knowledge about the role of BFR therapy in patients with knee OA along with the strength of evidence from outcomes reported in the included systematic reviews. This overview will provide the clinicians and researchers with some level of certainty on the effects of BFR therapy on several outcomes in individuals with knee OA. Furthermore, the overview may shed light on future directions for systematic reviews and possibly new research studies.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
FM: Conceptualization, Investigation, Methodology, Writing – review & editing. GA: Conceptualization, Investigation, Methodology, Writing – review & editing. AV: Conceptualization, Formal Analysis, Methodology, Writing – original draft. AR: Conceptualization, Formal Analysis, Methodology, Writing – original draft. GFB-C: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Supervision, Validation, Visualization, Writing – original draft. G-CJ: Conceptualization, Formal Analysis, Investigation, Methodology, Supervision, Validation, Visualization, Writing – review & editing. WM: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article.
We received financial support from the Decanate of Research and Innovation (DPI) and Graduate Studies (DPG) of the University of Brasília (UnB) through Public Notice DPI/DPG n° 01/2022.
For the publication of this protocol, we received financial support from the Decanate of Research and Innovation (DPI) and Graduate Studies (DPG) of the University of Brasília (UnB) through Public Notice DPI/DPG n° 01/2022, which aims to stimulate, through payment of financial assistance to researchers, the execution of scientific, technological and innovation research projects, with the participation of professors and active administrative technicians from the permanent staff of the University of Brasília, which results in the production of scientific articles in journals that charge a publication fee. The opinions expressed are those of the author(s).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fresc.2024.1318951/full#supplementary-material
2. Duarte VS de, Santos ML dos, Rodrigues KA de, Ramires JB, Arêas GPT, Borges GF. Exercícios físicos e osteoartrose: uma revisão sistemática. Fisioter em Mov. (2013) 26(1):193–202. doi: 10.1590/S0103-51502013000100022
3. Martel-Pelletier J, Boileau C, Pelletier J-P, Roughley PJ. Cartilage in normal and osteoarthritis conditions. Best Pract Res Clin Rheumatol. (2008) 22(2):351–84. doi: 10.1016/j.berh.2008.02.001
4. Papalia R, Zampogna B, Torre G, Lanotte A, Vasta S, Albo E, et al. Sarcopenia and its relationship with osteoarthritis: risk factor or direct consequence? Musculoskelet Surg. (2014) 98(1):9–14. doi: 10.1007/s12306-014-0311-6
5. Vos T, Flaxman AD, Naghavi M, Lozano R, Michaud C, Ezzati M, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: a systematic analysis for the global burden of disease study 2010. Lancet. (2012) 380(9859):2163–96. doi: 10.1016/S0140-6736(12)61729-2
6. Cheon Y-H, Kim H-O, Suh YS, Kim MG, Yoo W-H, Kim RB, et al. Relationship between decreased lower extremity muscle mass and knee pain severity in both the general population and patients with knee osteoarthritis: findings from the KNHANES V 1-2. PLoS One. (2017) 12(3):e0173036. doi: 10.1371/journal.pone.0173036 (Mischak H, editor).28296926
7. Ruhdorfer A, Wirth W, Eckstein F. Association of knee pain with a reduction in thigh muscle strength—a cross-sectional analysis including 4553 osteoarthritis initiative participants. Osteoarthr Cartil. (2017) 25(5):658–66. doi: 10.1016/j.joca.2016.10.026
8. Glass NA, Torner JC, Frey Law LA, Wang K, Yang T, Nevitt MC, et al. The relationship between quadriceps muscle weakness and worsening of knee pain in the MOST cohort: a 5-year longitudinal study. Osteoarthr Cartil. (2013) 21(9):1154–9. doi: 10.1016/j.joca.2013.05.016
9. Lang T, Streeper T, Cawthon P, Baldwin K, Taaffe DR, Harris TB. Sarcopenia: etiology, clinical consequences, intervention, and assessment. Osteoporos Int. (2010) 21(4):543–59. doi: 10.1007/s00198-009-1059-y
10. Dinenno FA, Jones PP, Seals DR, Tanaka H. Limb blood flow and vascular conductance are reduced with age in healthy humans. Circulation. (1999) 100(2):164–70. doi: 10.1161/01.CIR.100.2.164
11. Blain H, Vuillemin A, Teissier A, Hanesse B, Guillemin F, Jeandel C. Influence of muscle strength and body weight and composition on regional bone mineral density in healthy women aged 60 years and over. Gerontology. (2001) 47(4):207–12. doi: 10.1159/000052800
12. Segal NA, Glass NA, Torner J, Yang M, Felson DT, Sharma L, et al. Quadriceps weakness predicts risk for knee joint space narrowing in women in the MOST cohort. Osteoarthr Cartil. (2010) 18(6):769–75. doi: 10.1016/j.joca.2010.02.002
13. Segal NA, Torner JC, Felson D, Niu J, Sharma L, Lewis CE, et al. Effect of thigh strength on incident radiographic and symptomatic knee osteoarthritis in a longitudinal cohort. Arthritis Rheum. (2009) 61(9):1210–7. doi: 10.1002/art.24541
14. Segal NA, Glass NA, Felson DT, Hurley M, Yang M, Nevitt M, et al. Effect of quadriceps strength and proprioception on risk for knee osteoarthritis. Med Sci Sport Exerc. (2010) 42(11):2081–8. doi: 10.1249/MSS.0b013e3181dd902e
15. Baker KR, Xu L, Zhang Y, Nevitt M, Niu J, Aliabadi P, et al. Quadriceps weakness and its relationship to tibiofemoral and patellofemoral knee osteoarthritis in Chinese: the Beijing osteoarthritis study. Arthritis Rheum. (2004) 50(6):1815–21. doi: 10.1002/art.20261
16. Brandt KD, Heilman DK, Slemenda C, Katz BP, Mazzuca S, Braunstein EM, et al. A comparison of lower extremity muscle strength, obesity, and depression scores in elderly subjects with knee pain with and without radiographic evidence of knee osteoarthritis. J Rheumatol. (2000) 27(8):1937–46. Available at: http://www.ncbi.nlm.nih.gov/pubmed/1095533610955336
17. Lewek MD, Rudolph KS, Snyder-Mackler L. Quadriceps femoris muscle weakness and activation failure in patients with symptomatic knee osteoarthritis. J Orthop Res. (2004) 22(1):110–5. doi: 10.1016/S0736-0266(03)00154-2
18. Palmieri-Smith RM, Thomas AC, Karvonen-Gutierrez C, Sowers MF. Isometric quadriceps strength in women with mild, moderate, and severe knee osteoarthritis. Am J Phys Med Rehabil. (2010) 89(7):541–8. doi: 10.1097/PHM.0b013e3181ddd5c3
19. Fisher NM, Pendergast DR. Reduced muscle function in patients with osteoarthritis. Scand J Rehabil Med. (1997) 29(4):213–21. Available at: http://www.ncbi.nlm.nih.gov/pubmed/94280559428055
20. Petterson SC, Barrance P, Buchanan T, Binder-Macleod S, Snyder-Mackler L. Mechanisms underlying quadriceps weakness in knee osteoarthritis. Med Sci Sport Exerc. (2008) 40(3):422–7. doi: 10.1249/MSS.0b013e31815ef285
21. McAlindon TE, Bannuru RR, Sullivan MC, Arden NK, Berenbaum F, Bierma-Zeinstra SM, et al. OARSI guidelines for the non-surgical management of knee osteoarthritis. Osteoarthr Cartil. (2014) 22(3):363–88. doi: 10.1016/j.joca.2014.01.003
22. Roddy E, Doherty M. Changing life-styles and osteoarthritis: what is the evidence? Best Pract Res Clin Rheumatol. (2006) 20(1):81–97. doi: 10.1016/j.berh.2005.09.006
23. Ferraz RB, Gualano B, Rodrigues R, Kurimori CO, Fuller R, Lima FR, et al. Benefits of resistance training with blood flow restriction in knee osteoarthritis. Med Sci Sports Exerc. (2018) 50(5):897–905. doi: 10.1249/MSS.0000000000001530
24. Topp R, Woolley S, Hornyak J, Khuder S, Kahaleh B. The effect of dynamic versus isometric resistance training on pain and functioning among adults with osteoarthritis of the knee. Arch Phys Med Rehabil. (2002) 83(9):1187–95. doi: 10.1053/apmr.2002.33988
25. Huang M-H, Lin Y-S, Yang R-C, Lee C-L. A comparison of various therapeutic exercises on the functional status of patients with knee osteoarthritis. Semin Arthritis Rheum. (2003) 32(6):398–406. doi: 10.1053/sarh.2003.50021
26. Progression models in resistance training for healthy adults. Med Sci Sport Exerc. (2009) 41(3):687–708. doi: 10.1249/MSS.0b013e3181915670
27. Ogasawara R, Loenneke JP, Thiebaud RS, Abe T. Low-Load bench press training to fatigue results in muscle hypertrophy similar to high-load bench press training. Int J Clin Med. (2013) 04(02):114–21. doi: 10.4236/ijcm.2013.42022
28. Schoenfeld BJ, Peterson MD, Ogborn D, Contreras B, Sonmez GT. Effects of low- vs. High-load resistance training on muscle strength and hypertrophy in well-trained men. J Strength Cond Res. (2015) 29(10):2954–63. doi: 10.1519/JSC.0000000000000958
29. Schoenfeld BJ, Wilson JM, Lowery RP, Krieger JW. Muscular adaptations in low- versus high-load resistance training: a meta-analysis. Eur J Sport Sci. (2016) 16(1):1–10. doi: 10.1080/17461391.2014.989922
30. Hughes L, Paton B, Rosenblatt B, Gissane C, Patterson SD. Blood flow restriction training in clinical musculoskeletal rehabilitation: a systematic review and meta-analysis. Br J Sports Med. (2017) 51(13):1003–11. doi: 10.1136/bjsports-2016-097071
31. Burgomaster KA, Moore DR, Schofield LM, Phillips SM, Sale DG, Gibala MJ. Resistance training with vascular occlusion: metabolic adaptations in human muscle. Med Sci Sport Exerc. (2003) 35(7):1203–8. doi: 10.1249/01.MSS.0000074458.71025.71
32. Abe T, Kawamoto K, Yasuda T, Kearns CF, Midorikawa T, Sato Y. Eight days KAATSU-resistance training improved sprint but not jump performance in collegiate male track and field athletes. Int J KAATSU Train Res. (2005) 1(1):19–23. doi: 10.3806/ijktr.1.19
33. Loenneke JP, Kim D, Fahs CA, Thiebaud RS, Abe T, Larson RD, et al. Effects of exercise with and without different degrees of blood flow restriction on torque and muscle activation. Muscle Nerve. (2015) 51(5):713–21. doi: 10.1002/mus.24448
34. Takarada Y, Tsuruta T, Ishii N. Cooperative effects of exercise and occlusive stimuli on muscular function in low-intensity resistance exercise with moderate vascular occlusion. Jpn J Physiol. (2004) 54(6):585–92. doi: 10.2170/jjphysiol.54.585
35. Loenneke JP, Wilson JM, Marín PJ, Zourdos MC, Bemben MG. Low intensity blood flow restriction training: a meta-analysis. Eur J Appl Physiol. (2012) 112(5):1849–59. doi: 10.1007/s00421-011-2167-x
36. Abe T, Fujita S, Nakajima T, Sakamaki M, Ozaki H, Ogasawara R, et al. Effects of low-intensity cycle training with restricted leg blood flow on thigh muscle volume and VO2MAX in young men. J Sports Sci Med. (2010) 9(3):452–8. Available at: http://www.ncbi.nlm.nih.gov/pubmed/2414964024149640
37. Ozaki H, Miyachi M, Nakajima T, Abe T. Effects of 10 weeks walk training with leg blood flow reduction on carotid arterial compliance and muscle size in the elderly adults. Angiology. (2011) 62(1):81–6. doi: 10.1177/0003319710375942
38. Ozaki H, Sakamaki M, Yasuda T, Fujita S, Ogasawara R, Sugaya M, et al. Increases in thigh muscle volume and strength by walk training with leg blood flow reduction in older participants. J Gerontol Ser A Biol Sci Med Sci. (2011) 66A(3):257–63. doi: 10.1093/gerona/glq182
39. Pearson SJ, Hussain SR. A review on the mechanisms of blood-flow restriction resistance training-induced muscle hypertrophy. Sport Med. (2015) 45(2):187–200. doi: 10.1007/s40279-014-0264-9
40. Takarada Y, Nakamura Y, Aruga S, Onda T, Miyazaki S, Ishii N. Rapid increase in plasma growth hormone after low-intensity resistance exercise with vascular occlusion. J Appl Physiol. (2000) 88(1):61–5. doi: 10.1152/jappl.2000.88.1.61
41. Reeves GV, Kraemer RR, Hollander DB, Clavier J, Thomas C, Francois M, et al. Comparison of hormone responses following light resistance exercise with partial vascular occlusion and moderately difficult resistance exercise without occlusion. J Appl Physiol. (2006) 101(6):1616–22. doi: 10.1152/japplphysiol.00440.2006
42. Loenneke JP, Fahs CA, Rossow LM, Abe T, Bemben MG. The anabolic benefits of venous blood flow restriction training may be induced by muscle cell swelling. Med Hypotheses. (2012) 78(1):151–4. doi: 10.1016/j.mehy.2011.10.014
43. Kawada S, Ishii N. Skeletal muscle hypertrophy after chronic restriction of venous blood flow in rats. Med Sci Sport Exerc. (2005) 37(7):1144–50. doi: 10.1249/01.mss.0000170097.59514.bb
44. Pope ZK, Willardson JM, Schoenfeld BJ. Exercise and blood flow restriction. J Strength Cond Res. (2013) 27(10):2914–26. doi: 10.1519/JSC.0b013e3182874721
45. Fujita S, Abe T, Drummond MJ, Cadenas JG, Dreyer HC, Sato Y, et al. Blood flow restriction during low-intensity resistance exercise increases S6K1 phosphorylation and muscle protein synthesis. J Appl Physiol. (2007) 103(3):903–10. doi: 10.1152/japplphysiol.00195.2007
46. Fry CS, Glynn EL, Drummond MJ, Timmerman KL, Fujita S, Abe T, et al. Blood flow restriction exercise stimulates mTORC1 signaling and muscle protein synthesis in older men. J Appl Physiol. (2010) 108(5):1199–209. doi: 10.1152/japplphysiol.01266.2009
47. Laurentino GC, Ugrinowitsch C, Roschel H, Aoki MS, Soares AG, Neves M, et al. Strength training with blood flow restriction diminishes myostatin gene expression. Med Sci Sport Exerc. (2012) 44(3):406–12. doi: 10.1249/MSS.0b013e318233b4bc
48. Takarada Y, Sato Y, Ishii N. Effects of resistance exercise combined with vascular occlusion on muscle function in athletes. Eur J Appl Physiol. (2002) 86(4):308–14. doi: 10.1007/s00421-001-0561-5
49. Yasuda T, Loenneke J, Ogasawara R, Abe T. Influence of continuous or intermittent blood flow restriction on muscle activation during low-intensity multiple sets of resistance exercise. Acta Physiol Hung. (2013) 100(4):419–26. doi: 10.1556/APhysiol.100.2013.4.6
50. Loenneke JP, Wilson JM, Wilson GJ, Pujol TJ, Bemben MG. Potential safety issues with blood flow restriction training. Scand J Med Sci Sports. (2011) 21(4):510–8. doi: 10.1111/j.1600-0838.2010.01290.x
51. Grantham B, Korakakis V, O’Sullivan K. Does blood flow restriction training enhance clinical outcomes in knee osteoarthritis: a systematic review and meta-analysis. Phys Ther Sport. (2021) 49:37–49. doi: 10.1016/j.ptsp.2021.01.014
52. Cuyul-Vásquez I, Leiva-Sepúlveda A, Catalán-Medalla O, Araya-Quintanilla F, Gutiérrez-Espinoza H. The addition of blood flow restriction to resistance exercise in individuals with knee pain: a systematic review and meta-analysis. Brazilian J Phys Ther. (2020) 24(6):465–78. doi: 10.1016/j.bjpt.2020.03.001
53. Ferlito JV, Pecce SAP, Oselame L, De Marchi T. The blood flow restriction training effect in knee osteoarthritis people: a systematic review and meta-analysis. Clin Rehabil. (2020) 34(11):1378–90. doi: 10.1177/0269215520943650
54. Cumpston M, Li T, Page MJ, Chandler J, Welch VA, Higgins JP, et al. Updated guidance for trusted systematic reviews: a new edition of the cochrane handbook for systematic reviews of interventions. Cochrane Database Syst Rev. (2019). doi: 10.1002/14651858.ED000142
55. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Br Med J. (2021) n71. doi: 10.1136/bmj.n71
56. Migliore A, Scirè CA, Carmona L, Beaumont GH, Bizzi E, Branco J, et al. The challenge of the definition of early symptomatic knee osteoarthritis: a proposal of criteria and red flags from an international initiative promoted by the Italian society for rheumatology. Rheumatol Int. (2017) 37(8):1227–36. doi: 10.1007/s00296-017-3700-y
57. Luyten FP, Denti M, Filardo G, Kon E, Engebretsen L. Definition and classification of early osteoarthritis of the knee. Knee surgery, Sport Traumatol Arthrosc. (2012) 20(3):401–6. doi: 10.1007/s00167-011-1743-2
58. Mahmoudian A, Lohmander LS, Jafari H, Luyten FP. Towards classification criteria for early-stage knee osteoarthritis: a population-based study to enrich for progressors. Semin Arthritis Rheum. (2021) 51(1):285–91. doi: 10.1016/j.semarthrit.2020.11.002
59. Pollock M, Fernandes RM, Becker LA, Pieper D, Hartling L. Chapter V: overviews of reviews. In: Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. editors. Cochrane Handbook for Systematic Reviews of Interventions Version 63 (updated February 2022). (2022). Available at: from: www.training.cochrane.org/handbook
60. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JPA, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med. (2009) 6(7):e1000100. doi: 10.1371/journal.pmed.1000100
61. Shea BJ, Reeves BC, Wells G, Thuku M, Hamel C, Moran J, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. Br Med J. (2017) j4008. doi: 10.1136/bmj.j4008
62. Smith V, Devane D, Begley CM, Clarke M. Methodology in conducting a systematic review of systematic reviews of healthcare interventions. BMC Med Res Methodol. (2011) 11(1):15. doi: 10.1186/1471-2288-11-15
Keywords: osteoarthritis, knee, blood flow restriction therapy, Kaatsu Training, resistance training, overview, systematic review
Citation: Machado FA, Almeida GJ, do Vale ALM, Ribeiro ALdA, Cipriano GFB, Cipriano Junior G and Martins WR (2024) Effects of blood flow restriction therapy in patients with knee osteoarthritis: protocol for an overview of systematic reviews. Front. Rehabil. Sci. 5:1318951. doi: 10.3389/fresc.2024.1318951
Received: 11 October 2023; Accepted: 15 January 2024;
Published: 1 February 2024.
Edited by:
Damiano Pizzol, Cigna, ItalyReviewed by:
Dalila Scaturro, University of Palermo, Italy© 2024 Machado, Almeida, do Vale, Ribeiro, Cipriano, Cipriano Junior and Martins. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Felipe Alves Machado ZmVsaXBldW5pZmVzcEBob3RtYWlsLmNvbQ==
†ORCID Felipe Alves Machado orcid.org/0000-0003-3765-7244 Gustavo J. Almeida orcid.org/0000-0003-4041-2651 André Luiz Maia do Vale orcid.org/0000-0002-7125-6295 Alexandre Lima de Araújo Ribeiro orcid.org/0000-0001-5266-4499 Graziella França Bernardelli Cipriano orcid.org/0000-0001-9560-6520 Gerson Cipriano Junior orcid.org/0000-0001-6323-7003 Wagner Rodrigues Martins orcid.org/0000-0002-0709-7373
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.