 Zonglin Wen
Zonglin Wen Ruoyun Lyu
Ruoyun Lyu Wei Wang1
Wei Wang1 Lingjun Kong
Lingjun Kong
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
STUDY PROTOCOL article
Front. Rehabil. Sci. , 25 August 2023
Sec. Rehabilitation for Musculoskeletal Conditions
Volume 4 - 2023 | https://doi.org/10.3389/fresc.2023.1165548
Background: Chronic ankle instability (CAI) is a common sports injury disease and characterized by limited mobility, perceived instability and muscle weakness, combined treatment of hip-knee-ankle is a common rehabilitation method. Tuina, as a traditional Chinese manual therapy, is usually used for CAI, but many of them only focus on the local ankle joint rather than the combination of hip and knee joint. Therefore, we have designed a randomized controlled trial (RCT) to investigate the effects of Tuina base on the concept of hip-knee-ankle conjugation on the stability and balance of lower limbs and ankle function in patients with CAI.
Methods: We have designed a randomized controlled trial. A total of 72 participants with CAI will be randomly divided into functional training groups and hip-knee-ankle Tuina combined with functional training group in a 1:1 ratio. Participants in control group will receive 8 sessions of functional training (30 min per session, twice a week for 4 weeks). Participants in intervention group will receive 8 sessions of Tuina combined with functional training (twice a week for 4 weeks). The primary outcomes include the Y-Balance Test (YBT) and Cumberland Ankle Instability Tool (CAIT). The Secondary outcomes include the Foot and Ankle Ability Measure (FAAM) and ankle range of motion (ROM). The outcome assessments will be conducted before the first intervention and after the last intervention.
Discussion: The aim of this study is to explore a safe and effective manipulation program and serve as reference for clinical treatment of CAI and expect to provide the necessary theoretical and practical support to our future research.
Clinical Trial Registration: Chinese Clinical Trail Registry ChiCTR2300068274.
Ankle sprains are one of the most common recurrent injury disease in sports, according to statistics, ankle sprains account for 15% of all sports injuries (1), and over 40% of ankle sprains go on to develop chronic symptoms (2). Studies (3) have shown that the patients who suffer from ankle sprains are prone to ankle sprain again due to the lack of awareness and the failure of timely, effective treatment. Recurrent ankle sprains are one of the main causes of chronic ankle instability (CAI). CAI is associated with functional changes such as proprioception, neuromuscular control, muscle strength, and postural control. Another study shows that CAI (4) is deficient in strength and dynamic postural control of hip and knee extensors. Inappropriate joint biomechanics is the main risk factor of osteoarthritis (5). However, rehabilitation exercises enhancing the strength of the hip and knee muscles may have a positive effect on improving dynamic postural control.
The knee and ankle are adjacent joints. The flexion and extension of the two joints are closely related. The flexion and extension of the knee can reduce the unnecessary movement of ankle to protect the lower limb joints. Meanwhile, individuals with chronic ankle instability have insufficient ankle plantar flexion torque, which may result in insufficient knee flexor and extensor torque, as well as deficient neuromuscular adaptation of the knee (6). In addition, altering foot progression angle in both toe-in and toe-out directions significantly affects the external knee joint moments in patients with medial knee osteoarthritis (7). The external knee joint moments is a surrogate indicator of knee joint load distribution during walking (8), which is closely related to the progression of knee medial compartment osteoarthritis (9, 10). On the other hand, the hip joint is also an important joint to maintain the stability of human posture. Multiple studies (11–14) have shown that repetitive ankle injuries lead to decreased isometric strength of hip adductor and abductor muscles, while proximal neuromuscular injuries may exacerbate dynamic postural control deficits in people with ankle injuries and further affect central regulation of motor control, which ultimately lead to widespread lower limb neuromuscular injuries. Patients with ankle injury have delayed activation of the hip extensor during hip extension, which may be related to the afferent disturbance of the proximal limb muscles caused by the dysfunction of mechanoreceptor afferents in the distal injured ankle (15). Therefore, in the treatment of ankle injuries, the combined treatment of hip and knee joint should also be paid sufficient attention.
In 2021, the Academy of Orthopedics Physical Therapy of the American Physical Therapy Association (APTA) issued the clinical practice guide “Ankle stability and movement coordination impairments: lateral ankle ligament sprains revision 2021”. The guideline recommends manipulative therapy as one of the main treatments for ankle injuries. Tuina, as a traditional Chinese manual therapy, is often used to improve pain, range of motion, and tissue extensibility (16). According to traditional Chinese medicine, Tuina technique, such as Rotating-Traction-Poking manipulation and Rubbing-Traction-Kneading manipulation and so on, can activate blood and remove stasis, relieve swelling and pain (17), and achieve the purpose of releasing soft tissue spasm, restoring joint alignment, improving ankle function and promoting rehabilitation (18–21). There are also some evidence to suggest that manual therapy can improve ankle dorsiflexion range of motion or dynamic postural control in patients with CAI (22, 23). However, in the treatment of CAI, many clinicians only focus on the local ankle joint rather than the combination of hip and knee joint.
Traditional Chinese medicine is highly affected by the concept of viewing things of Chinese classical philosophy, the concept of holism permeates through all the fields in traditional Chinese medicine, including physiology, pathology, diagnosis, syndrome differentiation and treatment. Traditional Chinese medicine believes that the human body is an organic whole, including hip-knee-ankle. In the treatment of CAI, it suggests that we should focus overall rather than only focus on the local to achieve better therapeutic effect. As an important part of traditional Chinese medicine, the concept of holism is also the principle of Tuina therapy.
The guideline also suggests that functional training is an important part of the treatment of ankle injuries (24), such as proprioceptive training, balance training and muscle strength training and so on. Many studies (25–28) have shown that functional training can enhance ankle stability, improve balance ability, reduce the risk of re-injury, promote the rehabilitation of ankle injury and help patients return to normal life and work as soon as possible.
Therefore, based on the concept of hip-knee-ankle conjugation, the objective of this randomized controlled trial (RCT) is to investigate the effects of 4-weeks Tuina on stability and balance of lower limbs, ankle function and ankle range of motion (ROM) of CAI patients to explore a new manipulation program for the treatment of ankle injuries.
To investigate the effects of Tuina on stability and balance of lower limbs, ankle function and ankle range of motion (ROM) on CAI patients and explore a new manipulation program for the treatment of ankle injuries.
This study is a randomized controlled trial (RCT) designed to confirm the clinical efficacy of Tuina therapy base on the concept of hip-knee-ankle conjugation in CAI. Seventy-two participants with CAI will be randomly assigned into intervention group and control group with the ratio of 1:1.
(1) According to the position statement of the International Ankle Consortium criteria (29).
(2) Participants have a history of at least one severe ankle sprain in the 12 months prior to join in this study, with pain, swelling and other symptoms on the affected side, which resulted in at least one day of inability to function normally.
(3) Two or more episodes of ankle loss of control and/or sprain and/or instability within 6 months.
(4) Cumberland Ankle Instability Tool (CAIT) scores less or equal than 27.
(5) Age 18–60 years old, male or female.
(1) Cardiovascular, hepatic, renal, hematopoietic, and other serious primary diseases or mental disorders.
(2) Pregnant or lactating women who cannot complete the radiology examination.
(3) Patients with rheumatism/rheumatoid arthritis, osteoporosis, gout and other serious bone and joint diseases.
(4) Those patients who could not correctly understand and fill in various scales related to the study.
(1) The condition deteriorates, or more serious complications occur.
(2) Serious adverse reactions occurred.
(1) Participants do not follow the original treatment plan (poor compliance).
(2) Participants receive other treatments without investigator's permission during the intervention period.
(3) Participants withdrew from the trial due to their own factors.
Patients with CAI will be recruited from Tuina Department of Shuguang Hospital affiliated to Shanghai University of Traditional Chinese Medicine. The main recruitment method will be advertising on social media, such as WeChat and Weibo, which is like WhatsApp and Twitter. The poster will also be displayed in hospital.
The intensity of Tuina treatment should not be too large and the duration of treatment should not be excessive. Participants will be reminded to be careful during the test. Participants with aggravation of pain or other serious complications after the Tuina treatment will be referred to an orthopedist or surgeon to receive other form of treatment.
We will explain the details of our study to the participants before they join our study. The frequency of treatment is twice a week for 4 weeks.
In this group, we will divide the functional training into two parts.
(1) Balance training
Squat with eyes closed: participants will squat and stand up slowly with eyes closed. At the beginning, they can support the wall or help objects, gradually increase the amplitude and reduce dependence. During each session, they need to perform three sets of ten repetitions.
Balance board training: participants will stand on the balance board with both feet, maintain balance and slightly rock from side to side. At the beginning, they can support the wall or help objects, and the difficulty can gradually increase. During each session, they need to perform three sets of ten repetitions.
(2) Resistance training
During each session, participants will use the resistance band to complete the resistance training in four directions of ankle motion (plantar flexion, dorsiflexion, inversion and eversion) which perform 3 sets of 10 repetitions.
In this group, the treatment scheme is based on the control group, and we will add the Tuina therapy base on the concept of hip-knee-ankle conjugation which is shown below. We will establish a scientific and normative, standardization work process, execute operation procedures and quality standards seriously. All treatment will be performed by the registered Tuina doctors, who have the qualification of clinicians and have been engaged in clinical work of tuina for more than 5 years. All of them graduated from the major of Tuina, and they will be trained and assessed with the standard operating procedures (SOP) of tuina manipulation in this study. Each session of Tuina treatment lasts about 30 min.
First, participants will lie in a supine position, with legs straight and relax. The doctor will hold the ankle with both hands, place the thumb on the patient's lateral or medial malleolus suture and press, while the other four fingers fix, rotate and shake the foot for several times. The ankle is pulled outward and downward with both thumbs. Then, keep kneading and twirling on the ankle relax tendons and activate collaterals and promote recovery. Finally, rub the ankle and taken heat transmission as the degree.
Second, participants keep lying in a supine position, the doctor will relax the soft tissues of the groin, thigh, knee and lower leg in turn, including quadriceps femoris, tibialis anterior muscle and soft tissues around the patella and so on. According to the actual situation, the knee adjustment manipulation techniques in sitting or supine position will be performed when necessary.
Third, participants transform in a prone position, the doctor will relax the muscles of the buttocks, thighs and calves in turn, including gluteus maximus, gluteus medius, piriformis, biceps femoris and gastrocnemius and so on. The manipulation should not be too heavy. Take the feeling of acid, swelling and numbness as degree. According to the actual situation, the hip joint adjustment manipulation techniques will be performed when necessary.
The first primary outcome measure is the stability and balance of lower limbs evaluated by the Y-Balance Test (YBT). Y-Balance Test is a clinical instrument base on star excursion balance test (SEBT) which is commonly used for assesses dynamic stability and neuromuscular control of the lower extremity, and studies have proofed its reliability (30). The YBT will be assessed before and after Tuina treatment.
Before the YBT, participants will be instructed to learn the correct stretch technique and allowed four practice trials in each direction, with three consecutive test trials in each direction during testing. The order of the directions is random. Composite scores and two-sided differences will be calculated at the end of the test. The calculation formula is shown below. If the composite score is less than 95%, it indicates poor joint stability, and there may be a high risk of injury to the support leg, a lower score indicates a higher risk of injury. If bilateral difference is greater than 5%, it suggests a large difference in strength or balance between the left and right support legs, a higher difference indicates a higher risk. Studies have shown that patients with an anterior right/left reach distance difference greater than 4 cm would be 2.5 times more likely to sustain a lower extremity injury (31).
Notes: a1, b1, c1, a2, b2 and c2 represent the farthest distance of the left/right foot extended in the three directions respectively. L represents the length of the leg.
The second primary outcome measure is self-assessment of ankle instability evaluated by Cumberland Ankle Instability Tool (CAIT). CAIT is an easy and understandable valid tool for the assessment of chronic ankle instability (32), and it can differentiate the stable and unstable ankle (33). Participants will rate their left and right ankles separately. Each question is assigned a different score based on the number of options. The maximum unilateral ankle score is 30. Participants with a unilateral ankle score equal or less than 27 are considered unstable on that side of the ankle and the range above it are considered stable (33).
Ankle function will be assessed by Foot and Ankle Ability Measure (FAAM). The FAAM is also a patient-completed rating scale consisting of a daily activities subscale (21 rated items) and a physical activity subscale (7 rated items) with response options on a 5-point Likert scale (4 to 0, respectively), which has been demonstrated reliable, to evaluate postural control and muscle strength in patients with CAI (34).
Ankle range of motion (ROM) will be assessed by limb goniometer. Ankle plantar flexion/dorsiflexion, varus and valgus range of motion will be measured, the method of measurement is shown below, and the angle of activity will be measured and recorded by the researcher.
(1) Ankle dorsiflexion range of motion: participants will move their weight forward, squat on one leg, land on their heels, and flex their knees to the maximum. The angle between the lower leg and the ground will be measured when the ankle is dorsiflexed to the maximum range of motion.
(2) Ankle plantarflexion range of motion: participants will move their weight back, squat on one leg, land on the balls of their feet, and extend their knees to the maximum extent. The angle between the lower leg and the ground will be measured when the ankle is plantarflexed to the maximum range of motion.
(3) Range of motion of ankle inversion and eversion: participants will move their weight to the left and right sides, squat on one leg, land on the balls of their feet, and maximize inversion and eversion their ankle. The angle between the lower leg and the ground will be measured when the ankle inversion and eversion to the maximum range of motion.
The participants will be randomly divided into functional training group (control group) and hip-knee-ankle Tuina group (intervention group), the allocation ratio of the two groups is 1:1. Sample size calculation is based on the Y-Balance Test (the primary outcome), the sample size formula for comparison of means between two groups in a randomized controlled trial is used to perform the sample size calculation. With the test levels set at α = 0.05 (2-sided), β = 0.1, according to the relevant literature at home and abroad (31, 35), the maximum acceptable right/left reach distance difference was 4 cm. The standard deviation of the comprehensive score of Y-Balance test in the pre-experimental observation was 4.95. It is substituted into the sample size calculation formula, n = 32.15. Considering a 10% dropout rate, and take the integer n = 36, so we will include 36 participants for each group, the total number of participants is 72.
We will use Statistical Package for the Social Sciences (SPSS) Ver.25.0 (IBM Inc, New York, USA) and manual assistance to complete randomization, the method is shown below.
Before the study, a randomization specialist, who will not join other part of this trial, will be set up, and the specialist will use SPSS Ver.25.0 to generate a set of random numbers according to the numbers 1–72. After that, the numbers will be sorted according to the order of random number from small to large, 72 numbers will be randomly divided into the intervention group and the control group, and the numbers and corresponding groups will be sent to the researchers. When the appropriate participants are recruited, the researchers will enter the form and number it according to the order of enrollment, and determined the group of the current case according to the grouping generated by the randomization specialist. The lists of the two groups are sorted into tables and sent to the doctor, who are informed of the treatment plan for each group in advance, in order to reduce unnecessary communication between researchers and randomization specialist in the grouping process, and avoid the influence of researchers' subjective will on the grouping as much as possible. The participants and the doctor will not be blinded because of specialization of Tuina. However, the data analysis and efficacy assessment will be performed by the research assistant, who will not join other part of this trial, and blinded in order to decrease analysis bias.
We will collect the baseline data before the study. The primary and secondary outcomes will be assessed at baseline and 4 weeks (at the end of the intervention). The researcher will collect the data in the case report form (CRF) after obtaining signed consent from the participants. To protect the privacy of the participants, we will use codes and initials instead of their personal information. After data uploading and confirming, only statistician can access to the data.
The principle of Intention-To-Treat (ITT) analysis and Per-Protocol (PP) analysis will be followed in the process of statistical analysis. The Last Observation Carried Forward Analysis (LOCF) rule will be applied for missing data in ITT analysis. All the statistical analysis will be performed using SPSS Ver.25.0 with a significance level of 0.05.
First, the different baseline characteristics of the two groups will be described, data will be presented as mean or median with standard deviation or interquartile range for continuous variables and as frequency distributions for categorical variables. Moreover, the histograms, boxes and other representations will also be considered for the graphic analysis of corresponding data. Two-sample t-test for quantitative data or Chi-square test for qualitative data will be performed as homogeneity test, and the covariance analysis will also be performed if an adjustment is needed for a baseline characteristic.
Second, the analyses will focus on whether statistically better treatment outcomes could be achieved in the intervention group. p Values less than 0.05 were considered statistically significant and tests were 2-sided.
Third, safety analysis will be performed using the Chi-square test or Fisher's exact test based on the frequency and percentage of all recorded adverse events between two groups.
The Flow chart is detailed in Appendix I below.
Holism is one of the characteristics of traditional Chinese medicine, during the process of diagnosing disease and treatment, how to apply the holistic concept and syndrome differentiation is one of the most important problems in clinical treatment. In the treatment of CAI, Tuina therapy is one of the common and effective treatment methods, and it can also combine the treatment of hip-knee-ankle in a good way, so we have designed a clinical trial for the application of Tuina in the treatment of chronic ankle instability. The aim of this study is to investigate the effects of Tuina based on the concept of hip-knee-ankle conjugation in patients with chronic ankle instability. The stability and balance of lower limbs will be assessed by Y-Balance Test and CAIT scores. The ankle function will be assessed by FAAM scores and ankle range of motion test. The study will attempt to explore the effect of hip-knee-ankle treatment on chronic ankle instability and provide evidence of the effects of Tuina in patients with CAI.
Decreased balance and impaired precise joint movement control are the main consequences of CAI, and recurrent ankle sprain is one of the important causes of this disease. These symptoms ultimately degrade the quality of life and athletic ability of patients with CAI. Although there are previous studies on hip-knee-ankle conjugate theory, they are most applied in the treatment of knee osteoarthritis. This study focus on the effect of hip-knee-ankle conjugate theory on the treatment of CAI, in order to explore how to improve the stability and balance of lower limbs and ankle function by using manipulation and improve the quality of life and motor ability of the patients with CAI.
Although the aim of this trial is to explore the effect of Tuina on ankle injuries and address the limitations of previous studies, this study also has its own limitations. First, because it is impossible to blind the doctor and participants, it is difficult to design a double-blinded RCT. To minimize the risk of detection bias, we have a randomization specialist, he will divide the participants into two groups randomly prior to the study, the assessors and analyst will be blinded to the group assignment in this study. Second, due to lack of precision instruments, lower limb stability, balance ability and ankle range of motion can only be assessed manually, which inevitably leads to certain errors.
In summary, we have designed a randomized controlled clinical trial to explore a safe and effective manipulation program to serve as reference for clinical treatment of ankle injuries. We also expect that this study can help our future research to provide the necessary theoretical and practical support.
The version number of this protocol is 2.0, dated on 10 January 2023. Participants will be recruited between March 2023 and June 2024. Study completion is expected to be October 2024.
The studies involving human participants were reviewed and approved by IRB of Shuguang Hospital afiliated with Shanghai University of Traditional Chinese Medicine (Approved number of ethic committee: 2022-1226-163-01). The patients/participants provided their written informed consent to participate in this study.
ZW is the director of the study who will plan and manage this study, and developed the manuscript. RL is the co-director of the study, contributed to the protocol development, provided clinical expertise, and developed the manuscript. WW, XH, YY, KZ contributed to design the first draft of this study. JW and LK contributed to revise and edit the protocol necessary for the performance of this study. All authors contributed to the article and approved the submitted version.
This trial is funded by Traditional Chinese Medicine research project of Shanghai Health Commission (No. 2022QN091) and Shanghai Three Year Action Plan for the Development of Traditional Chinese Medicine (Shanghai Traditional Chinese Medicine School Inheritance Project) (NO. ZYSNXD CC HPGC JD 001). The funder did not have a role in the study design, collection, management, analysis, interpretation of data, manuscript writing, or decision making for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Doherty C, Delahunt E, Caulfield B, Hertel J, Ryan J, Bleakley C. The incidence and prevalence of ankle sprain injury: a systematic review and meta-analysis of prospective epidemiological studies. Sports Med. (2014) 44(1):123–40. doi: 10.1007/s40279-013-0102-5
2. Mugno AT, Constant D. Recurrent ankle sprain. Treasure Island (FL): StatPearls Publishing (2022).
3. Delahunt E, Bleakley CM, Bossard DS, Caulfield BM, Docherty CL, Doherty C, et al. Clinical assessment of acute lateral ankle sprain injuries (ROAST): 2019 consensus statement and recommendations of the international ankle consortium. Br J Sports Med. (2018) 52(20):1304–10. doi: 10.1136/bjsports-2017-098885
4. Kang C, Qingliang W, Ye Z, Lan T, Ke X, Yanhong M. A study on hip and knee muscle strength and dynamic posture control in patients with chronic ankle instability. China Rehabil. (2022) 37(06):363–6.
5. Saxby DJ, Lloyd DG. Osteoarthritis year in review 2016: mechanics. Osteoarthr Cartil. (2017) 25(2):190–8. doi: 10.1016/j.joca.2016.09.023
6. Gribble PA, Robinson RH. An examination of ankle, knee, and hip torque production in individuals with chronic ankle instability. J Strength Cond Res. (2009) 23(2):395–400. doi: 10.1519/JSC.0b013e31818efbb2
7. Simic M, Wrigley TV, Hinman RS, Hunt MA, Bennell KL. Altering foot progression angle in people with medial knee osteoarthritis: the effects of varying toe-in and toe-out angles are mediated by pain and malalignment. Osteoarthr Cartil. (2013) 21(9):1272–80. doi: 10.1016/j.joca.2013.06.001
8. Hunt MA, Birmingham TB, Giffin JR, Jenkyn TR. Associations among knee adduction moment, frontal plane ground reaction force, and lever arm during walking in patients with knee osteoarthritis. J Biomech. (2006) 39(12):2213–20. doi: 10.1016/j.jbiomech.2005.07.002
9. Miyazaki T, Wada M, Kawahara H, Sato M, Baba H, Shimada S. Dynamic load at baseline can predict radiographic disease progression in medial compartment knee osteoarthritis. Ann Rheum Dis. (2002) 61(7):617–22. doi: 10.1136/ard.61.7.617
10. Chang AH, Moisio KC, Chmiel JS, Eckstein F, Guermazi A, Prasad PV, et al. External knee adduction and flexion moments during gait and medial tibiofemoral disease progression in knee osteoarthritis. Osteoarthr Cartil. (2015) 23(7):1099–106. doi: 10.1016/j.joca.2015.02.005
11. McCann RS, Crossett ID, Terada M, Kosik KB, Bolding BA, Gribble PA. Hip strength and star excursion balance test deficits of patients with chronic ankle instability. J Sci Med Sport. (2017) 20(11):992–6. doi: 10.1016/j.jsams.2017.05.005
12. McCann RS, Bolding BA, Terada M, Kosik KB, Crossett ID, Gribble PA. Isometric hip strength and dynamic stability of individuals with chronic ankle instability. J Athl Train. (2018) 53(7):672–8. doi: 10.4085/1062-6050-238-17
13. Ward S, Pearce AJ, Pietrosimone B, Bennell K, Clark R, Bryant AL. Neuromuscular deficits after peripheral joint injury: a neurophysiological hypothesis. Muscle Nerve. (2015) 51(3):327–32. doi: 10.1002/mus.24463
14. Webster KA, Gribble PA. A comparison of electromyography of gluteus medius and maximus in subjects with and without chronic ankle instability during two functional exercises. Phys Ther Sport. (2013) 14(1):17–22. doi: 10.1016/j.ptsp.2012.02.002
15. Khalaj N, Vicenzino B, Heales LJ, Smith MD. Is chronic ankle instability associated with impaired muscle strength? Ankle, knee and hip muscle strength in individuals with chronic ankle instability: a systematic review with meta-analysis. Br J Sports Med. (2020) 54(14):839–47. doi: 10.1136/bjsports-2018-100070
16. Walsh BM, Bain KA, Gribble PA, Hoch MC. Exercise-based rehabilitation and manual therapy compared with exercise-based rehabilitation alone in the treatment of chronic ankle instability: a critically appraised topic. J Sport Rehabil. (2020) 29(5):684–8. doi: 10.1123/jsr.2019-0337
17. Linlin F, Rui C. Biomechanical analysis of manipulation for ankle sprain. Chinese Manipulation Rehabil Med. (2021) 12(07):61–3.
18. Yiying Y. Study on the mechanism of rotating-traction-poking manipulation in the treatment of lateral ankle sprain based on the theory of “gu zheng jin rou”. China Acad Chinese Med Sci. (2019).
19. Chunyu G, Hao C, Zhiyi L, Zhaojun C, Weiguo Z, Honglei D, et al. Effects ofshaking-pulling-poking manipulation on relieving pain and swelling in patients with acute lateral ankle sprains. Beijing J Tradit Chinese Med. (2015) 34(01):3–6.
20. Jinghua G, Zhiyi L, Hao C, Hua S, Chunyu G, Honglei D. The observation of shake-stamp-pull technique in improving the efficacy of acute lateral ankle sprain dysfunction. Chinese J Tradit Med Traumatol Orthop. (2013) 21(12):14–6.
21. Chunyu G, Jinghua G, QingFu W, Hao C, Hua S, Chengwei W, et al. Clinical study on the treatment of acute lateral ankle sprain by technique of shaking, drawing and stabbing. Chinese J Tradit Med Traumatol Orthop. (2015) 23(01):10–3.
22. Kosik KB, Gribble PA. The effect of joint mobilization on dynamic postural control in patients with chronic ankle instability: a critically appraised topic. J Sport Rehabil. (2018) 27(1):103–8. doi: 10.1123/jsr.2016-0074
23. Hoch MC, Andreatta RD, Mullineaux DR, English RA, Medina McKeon JM, Mattacola CG, et al. Two-week joint mobilization intervention improves self-reported function, range of motion, and dynamic balance in those with chronic ankle instability. J Orthop Res. (2012) 30(11):1798–804. doi: 10.1002/jor.22150
24. Martin RL, Davenport TE, Fraser JJ, Sawdon-Bea J, Carcia CR, Carroll LA, et al. Ankle stability and movement coordination impairments: lateral ankle ligament sprains revision 2021. J Orthop Sports Phys Ther. (2021) 51(4):Cpg1–80. doi: 10.2519/jospt.2021.0302
25. Doherty C, Bleakley C, Delahunt E, Holden S. Treatment and prevention of acute and recurrent ankle sprain: an overview of systematic reviews with meta-analysis. Br J Sports Med. (2017) 51(2):113–25. doi: 10.1136/bjsports-2016-096178
26. Bellows R, Wong CK. The effect of bracing and balance training on ankle sprain incidence among athletes: a systematic review with meta-analysis. Int J Sports Phys Ther. (2018) 13(3):379–88. doi: 10.26603/ijspt20180379
27. Vuurberg G, Hoorntje A, Wink LM, van der Doelen BFW, van denBekerom MP, Dekker R, et al. Diagnosis, treatment and prevention of ankle sprains: update of an evidence-based clinical guideline. Br J Sports Med. (2018) 52(15):956. doi: 10.1136/bjsports-2017-098106
28. Leppänen M, Aaltonen S, Parkkari J, Heinonen A, Kujala UM. Interventions to prevent sports related injuries: a systematic review and meta-analysis of randomised controlled trials. Sports Med. (2014) 44(4):473–86. doi: 10.1007/s40279-013-0136-8
29. Gribble PA, Delahunt E, Bleakley CM, Caulfield B, Docherty CL, Fong DT, et al. Selection criteria for patients with chronic ankle instability in controlled research: a position statement of the international ankle consortium. J Athl Train. (2014) 49(1):121–7. doi: 10.4085/1062-6050-49.1.14
30. Nelson S, Wilson CS, Becker J. Kinematic and kinetic predictors of Y-balance test performance. Int J Sports Phys Ther. (2021) 16(2):371–80. doi: 10.26603/001c.21492
31. Plisky PJ, Rauh MJ, Kaminski TW, Underwood FB. Star excursion balance test as a predictor of lower extremity injury in high school basketball players. J Orthop Sports Phys Ther. (2006) 36(12):911–9. doi: 10.2519/jospt.2006.2244
32. Hiller CE, Refshauge KM, Bundy AC, Herbert RD, Kilbreath SL. The cumberland ankle instability tool: a report of validity and reliability testing. Arch Phys Med Rehabil. (2006) 87(9):1235–41. doi: 10.1016/j.apmr.2006.05.022
33. Khan B, Ikram M, Rehman SSU, Un Nisa Z. Urdu translation and cross-cultural validation of cumberland ankle instability tool (CAIT). BMC Musculoskelet Disord. (2022) 23(1):443. doi: 10.1186/s12891-022-05408-4
34. Goulart Neto AM, Maffulli N, Migliorini F, de Menezes FS, Okubo R. Validation of foot and ankle ability measure (FAAM) and the foot and ankle outcome score (FAOS) in individuals with chronic ankle instability: a cross-sectional observational study. J Orthop Surg Res. (2022) 17(1):38. doi: 10.1186/s13018-022-02925-9
35. Ness BM, Taylor AL, Haberl MD, Reuteman PF, Borgert AJ. Clinical observation and analysis of movement quality during performance on the star excursion balance test. Int J Sports Phys Ther. (2015) 10(2):168–77.25883865
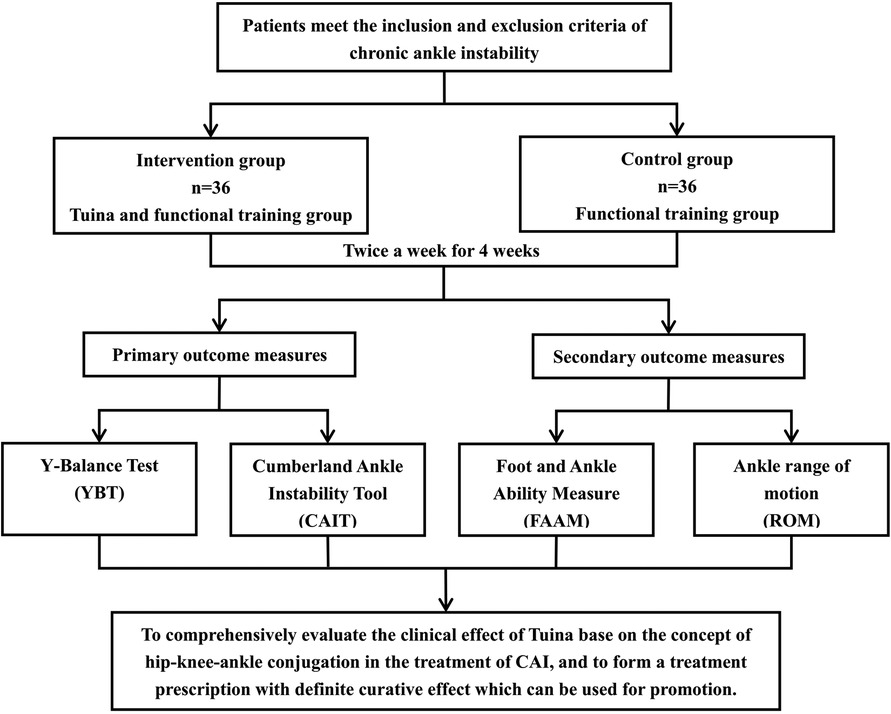
Appendix Figure 1. Flow Chart
Keywords: chronic ankle instability, tuina, hip-knee-ankle conjugation, clinical trial, functional training, physical therapy
Citation: Wen Z, Lyu R, Wang W, Hua X, Yu Y, Zeng K, Kong L and Wang J (2023) The effect of Tuina based on the concept of hip-knee-ankle conjugation in patients with chronic ankle instability: study protocol for a randomized controlled trial. Front. Rehabil. Sci. 4:1165548. doi: 10.3389/fresc.2023.1165548
Received: 14 February 2023; Accepted: 7 August 2023;
Published: 25 August 2023.
Edited by:
Feng Yang, Georgia State University, United StatesReviewed by:
Zhifeng Liu, Beijing University of Chinese Medicine, China© 2023 Wen, Lyu, Wang, Hua, Yu, Zeng, Kong and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lingjun Kong Y2h1bnlvbmcwMUAxNjMuY29t JianWei Wang d2FuZzM2MzAxQDE2My5jb20=
†These authors share first authorship
Abbreviations RCT, randomized controlled trial; CAI, chronic ankle instability; CAIT, cumberland ankle instability tool; YBT, Y-balance test; SEBT, star excursion balance test; FAAM, foot and ankle ability measure; ROM, range of motion; CRF, case report form.
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.