 Peter Gaumond
Peter Gaumond Lindsey Ann Martin
Lindsey Ann Martin Brett T. Hagman
Brett T. Hagman Mary J. Davis1†
Mary J. Davis1†
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Public Health , 10 April 2025
Sec. Substance Use Disorders and Behavioral Addictions
Volume 13 - 2025 | https://doi.org/10.3389/fpubh.2025.1585533
This article is part of the Research Topic Innovations in Recovery Science: Pathways, Policies, and Platforms that Promote Thriving After Addiction View all 14 articles
In 2024, the Office of National Drug Control Policy (ONDCP) convened an interagency working group (IWG) comprised of 30 federal agencies to identify federal recovery research gaps and opportunities on recovery from substance use disorder (SUD). This article outlines the process undertaken to identify these research opportunities and describes four core research topic areas and three cross-cutting themes and provides the rationale for their selection. It also identifies potential pathways for recovery research, including evaluation and data collection activities, and discusses challenges and potential opportunities for recovery research.
Research on SUD recovery has grown rapidly over the past few years. Nonetheless, recovery science lags far behind science on topics such as the treatment of substance use disorder and addiction-related pharmacotherapies. Moreover, research has tended to focus on specialty treatment populations, which represent a relatively small subset of individuals who have resolved alcohol or other drug (AOD) problems. Among individuals who reported having resolved an AOD problem, Kelly and colleagues found that 27.6 percent had received specialty treatment while 21.8 percent had received recovery support, and 45.1 percent had participated in mutual aid groups (1). Similarly, in 2023, while an estimated 54.2 million U.S. individuals age 12 and over needed SUD treatment, less than one quarter (12.8 million) of these individuals received treatment (2). A significant portion of individuals experiencing AOD problems report natural recovery, the resolution of an AOD problem without treatment, mutual aid, or other services or supports. To more fully understand the addiction, recovery, and remission processes, research needs to be broadened to include those for whom the trajectory to recovery or remission does not include formal treatment.
The 2022 National Drug Control Strategy (NDCS) noted the need for “targeted, actionable research to guide policy and resource allocation decisions in the recovery domain” and called for the establishment of an interagency workgroup (IWG) to advance such an effort, directing federal agencies to: (1) summarize the current scientific knowledge of the recovery process and recovery support services (RSS); (2) catalog current federally-funded research and evaluation efforts germane to these topics; and (3) identify key areas where additional research is needed. While the NDCS called on 16 federal agencies to participate in the IWG, a total of 30, including six components of the Department of Health and Human Services, participated. Supplementary material 2 provides a list of participating federal agencies.
To establish a baseline of current knowledge, ONDCP staff consulted with IWG participants and compiled existing literature reviews and research publications. IWG participants gathered information on recent, current, and planned federally supported research, evaluation, and data collection efforts as well as services, billing and other program data. In addition, participating agencies were canvassed to identify recovery-related research, evaluation, and data collection activities in which they were not currently engaged, but which were possible under agencies’ statutory authorities (See Supplementary material 1 for the table used to collect information on activities within agencies’ purview and scope, whether they are currently engaged in them or not). Following a review and discussion of the current agency efforts and of the scientific knowledge base, IWG participants developed a list of research opportunity areas. To be considered a research opportunity, research topics need to represent an underdeveloped area of research.
IWG participants identified seven research opportunity areas, including four core research topics and three cross-cutting themes. The core topics were recovery support services (RSS); organization and financing of systems and services; recovery and remission trajectories and intervention points; and recovery measure validation. The three cross-cutting themes were: role of people with lived and living experience (PWLLE) of SUD in policy, systems, services and research; ecosystems (i.e., multilevel approaches to research); and stigma.
Figure 1 depicts the working group’s process for identifying the recovery research opportunity areas.
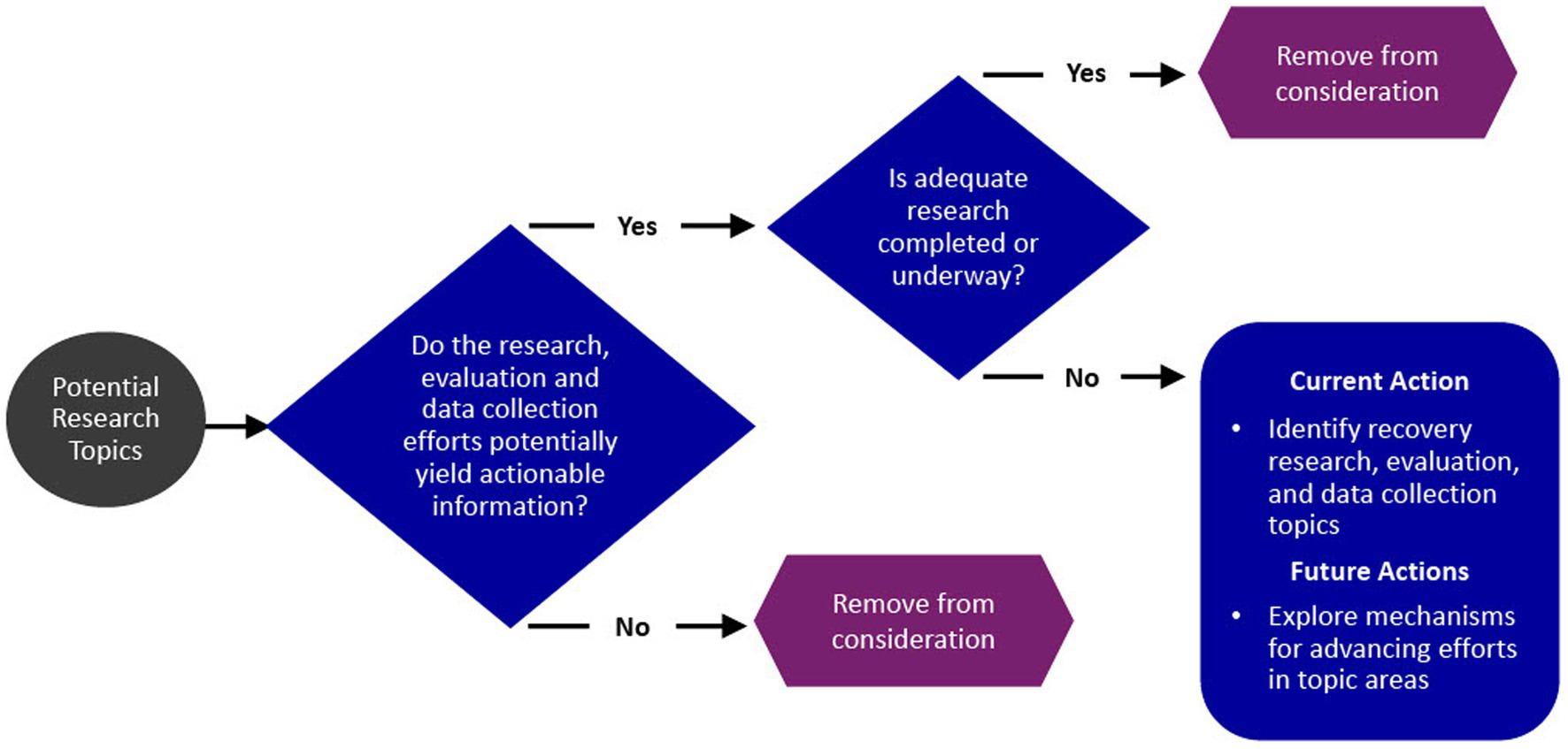
Figure 1. Federal recovery research interagency working group process.
In the following section we describe the scope of the identified research opportunities and provide the rationale for their selection. Most participating federal agencies reported research, evaluation, and data collection activities focused on recovery support services (n = 25). This was followed by fewer agency activities related to organization and financing of systems/services (n = 13), recovery and remission trajectories and intervention points (n = 6), and measure validation (n = 4). In terms of cross-cutting themes, agencies reported fewer activities related to the role of people with lived and living experience in SUD (n = 6), ecosystems (n = 2), and stigma (n = 5). In Table 1, we provide a list of sample topics/questions by research area.
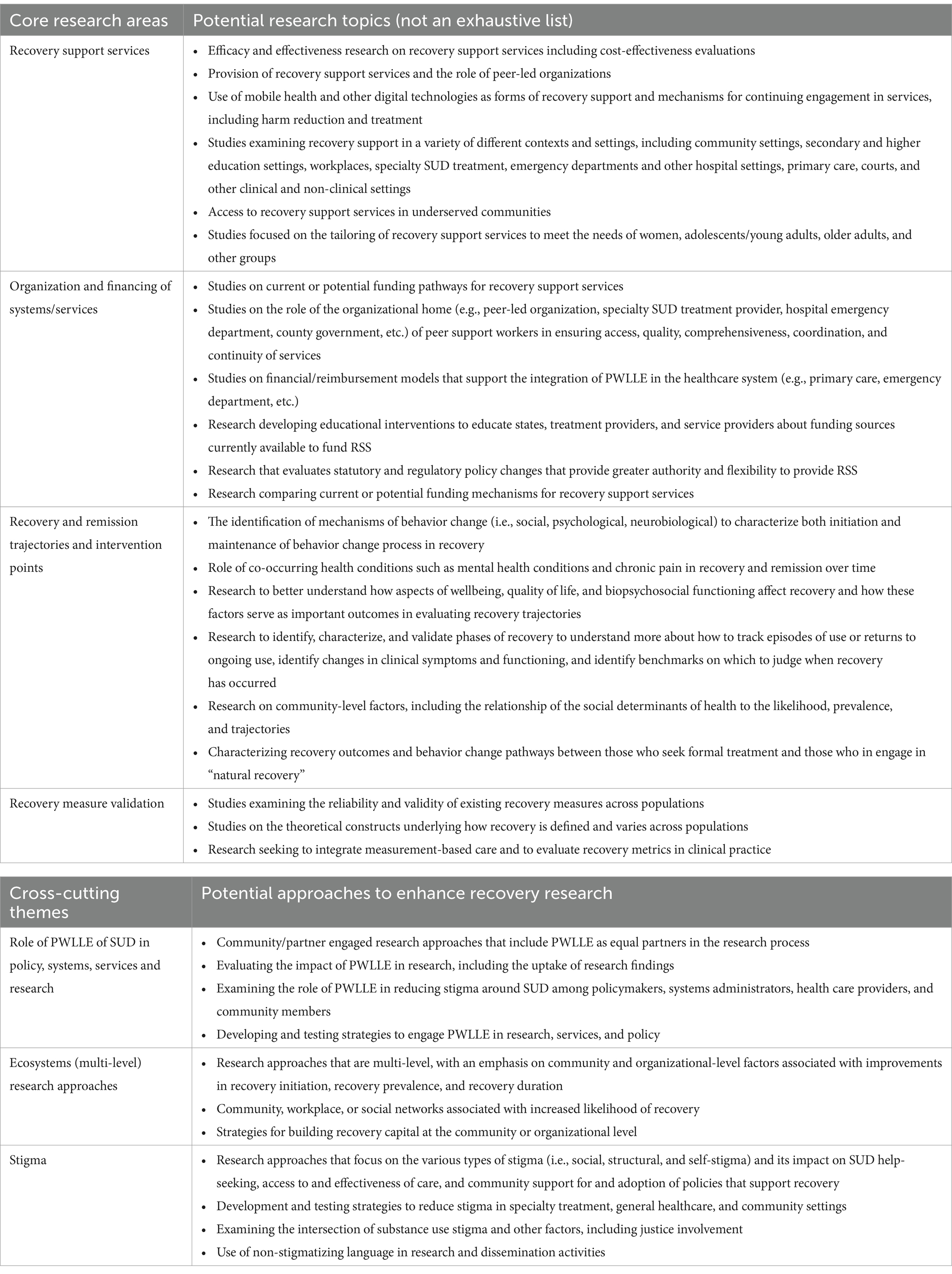
Table 1. Recovery research opportunity areas.
Recovery support services (RSS) are non-clinical services that help individuals initiate and sustain recovery from SUD. They can be offered in conjunction with treatment or other clinical services or separately, through entities such as recovery community centers, recovery residences, recovery community organizations, recovery high schools, collegiate recovery programs, and other organizations. The majority of RSS are offered by PWLLE, or “peers.” RSS provided by PWLLE are known as peer recovery support services (PRSS). During the final decade of the 20th century, PRSS began to be embedded in clinical service systems and grew to be recognized as a separate form of community-based services and support infrastructure. This was due, in no small measure, to the Recovery Community Services Program, a Substance Abuse and Mental Health Services Administration (SAMHSA) grant program that continues to this day. The Recovery Community Services Program has played a key role in the development of recovery community organizations and recovery community centers nationally. Recovery housing, which had spread nationally by the middle of the 20th century (3), is the most studied form of peer recovery support services. Research on other forms, including recovery coaching, collegiate recovery programs, recovery high schools (3), and recovery community organizations (4) is emerging, but is far less developed. The role and impact of mutual aid groups, such as Alcoholics Anonymous, Narcotics Anonymous, and SMART Recovery, is an additional gap area.
While there is growing evidence that PRSS can be critical to initiating and maintaining recovery from SUD (5–7), organizational and financing barriers remain. For example, a recent study found that peer support services covered by Medicaid were underutilized by people with opioid use disorder (8). PRSS are typically funded through federal, state, and local sources, including Medicaid; Substance Use Prevention, Treatment, and Recovery Services Block Grant; state general revenue; federal discretionary grants; and drug courts. Private health insurance, local fundraising efforts, and philanthropies also play a role. PRSS do not have dedicated federal funding streams such as those provided for primary prevention and treatment. Because PRSS are often offered by non-traditional providers, states, local governments, and private insurers may not be accustomed to purchasing services from such entities and may not have standards in place for doing so. Multi-state public and private payers may also be impeded by inconsistencies in peer certification criteria and differing regulatory requirements across states. Questions remain about the best approaches for integrating PRSS and clinical services and how they may build community-level recovery capital in a manner that reaches non-treatment populations.
The recovery domain is anchored in SAMHSA’s working definition of recovery as “a process of change through which individuals improve their health and wellness, live a self-directed life, and strive to reach their full potential.” Under this definition, recovery has four major dimensions: health, home, purpose, and community (9). Recovery is viewed through a strengths-based lens with a focus on improvements in health, social functioning, and quality of life. Importantly, multiple stakeholders note the heterogeneity of recovery pathways, arguing that a range of potential intervention points will need to be identified, studied and validated. For example, in the development of the National Institute on Alcohol Abuse and Alcoholism definition of recovery, recovery stakeholders identified and acknowledged that recovery involves multiple domains and is often marked by the fulfillment of basic needs, enhancements in social support and spiritualty, and improvements in physical and mental health, quality of life, and other dimensions of wellbeing (10). In addition, participants in a recent National Institutes of Health HEAL Initiative recovery workshop also noted how individual recovery trajectories and narratives vary widely, and how the recovery journey can be impacted by challenges such as lack of employment and treatment access (11). From a research perspective, recovery from SUD is commonly characterized as a process of initiation and maintenance of health behavior change that can include periods of remission and recurrence (12, 13). Understanding the heterogenous behavior change pathways and trajectories of recovery from SUD is critical for characterizing phases of recovery and identifying important intervention points for initiating and/or sustaining recovery and better informing federal policies that support the recovery process.
Recovery measure validation was not initially identified as a core research opportunity area given the range of validated recovery capital and quality of life measures, such as the Brief Assessment of Recovery Capital or BARC-10, and other relevant validated measures. However, additional reliability and validity testing is needed to better understand contextual variations of recovery capital (14). Addiction recovery stakeholders and researchers clearly acknowledge that wellbeing and biopsychosocial functioning constructs are considered integral in defining recovery. Additional research needs to address how best to operationalize these constructs, identify threshold values to mark clinically meaningful progress, and identify the constructs that are most integral to success in recovery from an alcohol or other drug use disorder (10, 11). More research is also needed to support recovery-focused measurement-based care, a process that utilizes standardized, valid, repeated measurements to track an individual’s progress over time (15).
PWLLE bring experience and perspective to research, helping ensure that study designs are well-tailored to targeted communities. Additionally, when leading research or taking part in community-level data collection, PWLLE can overcome common barriers to participation, including trust of the researchers. For this reason, federal agencies have taken significant steps to engage PWLLE in the planning, implementation and dissemination of research. The NIH HEAL Initiative’s Patient and Community Engagement Resources webpage is one example. Working groups and panels comprised of PWLLE provide another example of how federal agencies engage people affected by SUD in their response efforts. There is a critical need to increase the number of researchers with lived experience leading federally supported research. This brings an important perspective to research design, can foster greater trust between the research team and community partners, and can lead to greater acceptability and sustainability of studied evidence-based interventions (16). Engagement of PWLLE in the development of programs that impact them has been limited. Future work could follow the model adopted by Health Canada that includes a PWLLE Council and extensive involvement of PWLLE in research through the Canadian Research Initiative in Substance Misuse (CRISM).
People with SUD and those in recovery are embedded in and interact with multiple ecosystems. These include family, neighborhood, community, school, work, and faith groups. They also include formal systems, such as specialty SUD treatment, broader health care systems, and the child welfare and criminal justice systems. Recovery is a long-term process that may be initiated during treatment (one ecosystem), but will continue afterward, taking place primarily in the community (a second ecosystem). Ecosystems are themselves an important topic of research. A Recovery Ready Ecosystem Model and a Recovery Ready Community Framework (17) have been proposed to identify gaps in community infrastructure. Additionally, research utilizing a county-level recovery ecosystem index (REI) found that counties’ overdose death rates were inversely related to their REI score (18). A UK-based hub-and-spoke model designed to raise awareness of recovery and visibility of people in recovery may hold promise for building recovery infrastructure at the community level. Under this model, a non-profit organization operated three hubs offering an enriched array of services and supported and proactively built spoke networks through contracts, informal agreements, and ongoing outreach and engagement of key community partners. The spokes were built upon long-term relationships with individuals and communities and rely to a significant degree on volunteerism (19).
Stigma is pervasive, creating barriers to employment and housing, and is associated with reluctance to dispense buprenorphine among pharmacists (20), disruption of interpersonal relationships, harms to physical and mental health, and reduced help-seeking (21). The IWG highlighted the need for more intersectional research approaches that incorporate stigma as a critical factor that accounted for to more fully understand and support the recovery process. This includes research on the use of stigmatizing language about SUD and related topics, which remains prevalent in media, among health professionals, and elsewhere. Stigmatizing language is associated with greater attribution of blame to individuals for having an AOD disorder and with increased support for punitive responses (22).
While there is a need for additional recovery research, it must be balanced with other opportunities in addiction research. Because federal agencies identify research gaps independently, and have varying processes and timelines for doing so, there is a need for cross-agency coordination to advance recovery research. This will require alignment of processes with differing timelines and components across agencies. Similarly, agency resources for evaluating their own programs are limited and there may be statutory evaluation requirements that must be prioritized over other efforts. Data collection on recovery, whether in relation to annual surveys, services, epidemiological efforts, or programs, needs to be consistent from year-to-year. New elements or changes in survey questions or data elements must be weighed against the need to ensure comparability of annual data.
This mini-review article serves to mark progress made to date by the IWG. It may not be inclusive of all recovery research interests, including evaluation and data collection efforts that were launched after the completion of the IWG’s activities. In addition, research gaps may shift over time, affecting the research needed. Additional research is needed to improve our understanding of RSS, identify effective strategies for financing and organizing recovery-oriented systems of care, map the diverse pathways from SUD to recovery or remission, and validate recovery measures. Importantly, this research should strongly encourage the inclusion of PWLLE, utilize multi-level approaches assessing factors impacting recovery outcomes, and address stigma. This article offers a pathway forward for the growing field of recovery science to inform critical policy and resource allocation decisions with the goal of increasing the rates at which recovery and remission from SUD are initiated and sustained.
PG: Conceptualization, Investigation, Visualization, Writing – original draft, Writing – review & editing. LM: Conceptualization, Investigation, Visualization, Writing – original draft, Writing – review & editing. BH: Conceptualization, Investigation, Visualization, Writing – original draft, Writing – review & editing. MD: Conceptualization, Investigation, Project administration, Resources, Writing – review & editing.
The author(s) declare that no financial support was received for the research and/or publication of this article.
The authors would like to thank the members of the interagency recovery working group, which included representatives from the Departments of Health and Human Services, Defense, Justice, Labor, Education, Housing and Urban Development, and the Veterans Administration, for their time and expertise that led to the development of this manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declare that no Gen AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The views and opinions expressed in this manuscript are those of the authors only and do not necessarily represent the views, official policy or position of the Office of National Drug Control Policy or of the U.S. Department of Health and Human Services or any of its affiliated institutions or agencies.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1585533/full#supplementary-material
ONDCP, Office of National Drug Control Strategy; IWG, interagency working group; SUD, substance use disorder; AOD, alcohol or other drug; NDCS, National Drug Control Strategy; RSS, recovery support services; PWLLE, people with lived and living experience; PRSS, peer recovery support services; SAMHSA, Substance Abuse and Mental Health Services Administration; REI, recovery ecosystem index.
1. Kelly, JF, Bergman, B, Hoeppner, BB, Vilsaint, C, and White, WL. Prevalence and pathways of recovery from drug and alcohol problems in the United States population: implications for practice, research, and policy. Drug Alcohol Depend. (2017) 181:162–9. doi: 10.1016/j.drugalcdep.2017.09.028
2. Substance Abuse and Mental Health Services Administration. Key substance use and mental health indicators in the United States: results from the 2023 National Survey on drug use and health. Rockville, MD: U.S. Department of Health and Human Services (2024) HHS Publication No. PEP24-07-021, NSDUH Series H-59). Available online at: https://www.samhsa.gov/data/report/2023-nsduh-annual-national-report.
3. Jason, LA, Salomon-Amend, M, Guerrero, M, Bobak, T, O’Brien, J, and Soto-Nevarez, A. The emergence, role, and impact of recovery support services. Alcohol Res. (2021) 41:9. doi: 10.35946/arcr.v41.1.04
4. Kelly, JF, Fallah-Sohy, N, Cristello, J, Stout, RL, Jason, LA, and Hoeppner, BB. Recovery community centers: characteristics of new attendees and longitudinal investigation of the predictors and effects of participation. J Subst Abus Treat. (2021) 124:108287. doi: 10.1016/j.jsat.2021.108287
5. Treitler, P, Crystal, S, Cantor, J, Chakravarty, S, Kline, A, Morton, C, et al. Emergency department peer support program and patient outcomes after opioid overdose. JAMA Netw Open. (2024) 7:e243614-E. doi: 10.1001/jamanetworkopen.2024.3614
6. Eddie, D, Hoffman, L, Vilsaint, C, Abry, A, Bergman, B, Hoeppner, B, et al. Lived experience in new models of Care for Substance use Disorder: a systematic review of peer recovery support services and recovery coaching. Front Psychol. (2019) 10:1052. doi: 10.3389/fpsyg.2019.01052
7. Reif, S, Braude, L, Lyman, DR, Dougherty, RH, Daniels, AS, Ghose, SS, et al. Peer recovery support for individuals with substance use disorders: assessing the evidence. Psychiatr Serv. (2014) 65:853–61. doi: 10.1176/appi.ps.201400047
8. Bao, Y, Zhang, H, Hutchings, K, Harris, RA, Calderbank, T, and Schackman, BR. Medicaid-covered peer support services used by enrollees with opioid use disorder. JAMA Netw Open. (2024) 7:e2420737-e. doi: 10.1001/jamanetworkopen.2024.20737
9. Substance Abuse and Mental Health Services Administration. SAMHSA’s working definition of recovery. U.S. Department of Health and Human Services. SAMHSA: Rockville, MD (2010).
10. Hagman, BT, Falk, D, Litten, R, and Koob, GF. Defining recovery from alcohol use disorder: development of an NIAAA research definition. Am J Psychiatry. (2022) 179:807–13. doi: 10.1176/appi.ajp.21090963
11. National Institutes of Health. Lived/living experience session NIH HEAL Initiative Workshop: (2024).
12. Kwasnicka, D, Dombrowski, SU, White, M, and Sniehotta, F. Theoretical explanations for maintenance of behaviour change: a systematic review of behaviour theories. Health Psychol Rev. (2016) 10:277–96. doi: 10.1080/17437199.2016.1151372
13. Voils, CI, Gierisch, JM, Yancy, WS Jr, Sandelowski, M, Smith, R, Bolton, J, et al. Differentiating behavior initiation and maintenance: theoretical framework and proof of concept. Health Educ Behav. (2014) 41:325–36. doi: 10.1177/1090198113515242
14. Bunaciu, A, Bliuc, A-M, Best, D, Hennessy, EA, Belanger, MJ, and Benwell, CSY. Measuring recovery capital for people recovering from alcohol and drug addiction: a systematic review. Addict Res Theory. (2024) 32:225–36. doi: 10.1080/16066359.2023.2245323
15. Hallgren, KA, Cohn, EB, Ries, RK, and Atkins, DC. Delivering remote measurement-based care in community addiction treatment: engagement and usability over a 6-month clinical pilot. Front Psych. (2022) 13:840409. doi: 10.3389/fpsyt.2022.840409
16. Cioffi, C, Hibbard, P, Hagaman, A, Tillson, M, and Vest, N. Perspectives of researchers with lived experience in implementation science research: opportunities to close the research-to-practice gap in substance use systems of care. Implement Res Pract. (2023) 4:26334895231180635. doi: 10.1177/26334895231180635
17. Ashford, RD, Brown, AM, Ryding, R, and Curtis, B. Building recovery ready communities: the recovery ready ecosystem model and community framework. Addict Res Theory. (2020) 28:1–11. doi: 10.1080/16066359.2019.1571191
18. Wahlquist, AE, Mathis, SM, Hunt Trull, L, Toitole, KK, Howard, A, Fletcher, E, et al. Associations between drug overdose mortality and recovery ecosystems in the United States: a county-level analysis using a novel index. Subst Use Addict Jo. (2024) 46:238–46. doi: 10.1177/29767342241262125
19. Best, D, Higham, D, Pickersgill, G, Higham, K, Hancock, R, and Critchlow, T. Building recovery capital through community engagement: a hub and spoke model for peer-based recovery support Services in England. Alcohol Treat Q. (2021) 39:3–15. doi: 10.1080/07347324.2020.1787119
20. Light, AE, Green, TC, Freeman, PR, Zadeh, PS, Burns, AL, and Hill, LG. Relationships between stigma, risk tolerance, and buprenorphine dispensing intentions among community-based pharmacists: results from a National Sample. Subst Use Addict J. (2024) 45:211–21. doi: 10.1177/29767342231215178
21. Krendl, AC, and Perry, BL. Stigma toward substance dependence: causes, consequences, and potential interventions. Psychol Sci Public Interest. (2023) 24:90–126. doi: 10.1177/15291006231198193
Keywords: recovery, remission, substance use disorder, recovery capital, peer recovery support services
Citation: Gaumond P, Martin LA, Hagman BT and Davis MJ (2025) Substance use disorder recovery research opportunities: perspectives from a federal interagency workgroup. Front. Public Health. 13:1585533. doi: 10.3389/fpubh.2025.1585533
Edited by:
Kenneth Blum, Western University of Health Sciences, United StatesReviewed by:
Lisa Saldana, Chestnut Health Systems - Lighthouse Institute, United StatesCopyright © 2025 Gaumond, Martin, Hagman and Davis. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Peter Gaumond, R2VyYXJkX1AuX0dhdW1vbmRAb25kY3AuZW9wLmdvdg==
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.