 Ting Yang
Ting Yang Guoyan Zheng1
Guoyan Zheng1 Shuzhi Peng
Shuzhi Peng
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 18 March 2025
Sec. Aging and Public Health
Volume 13 - 2025 | https://doi.org/10.3389/fpubh.2025.1547425
Objective: To explore the relationship between sleep quality and mild cognitive impairment in older adult patients with multimorbidity.
Methods: The general data of older adult patients with chronic diseases were collected, and the sleep quality and mild cognitive impairment (MCI) of older adult patients with multimorbidity were investigated by questionnaire. Logistic regression model and restricted cubic spline (RCS) model were used to analyze the correlation between sleep quality and MCI in older adult patients with multimorbidity.
Results: There are 902 valid samples in this study, of which 333 (36.9%) have MCI. The number of chronic diseases ranges from 2 to 6, and the number of types of medication ranges from 0 to 7. The score of PSQI is 2–18, with an average score of 11.13. MoCA score range is 7–30. The MoCA score of MCI patients is lower than that of Non-MCI patients. In all three models, PSQI score is significantly correlated with MCI. The results of the segmented regression analysis show that: the inflection point of MCI’s PSQI scoring relationship is 12. RCS result display: with the increase of PSQI score, the OR increases between PSQI score and MCI, when PSQI score reaches 12, OR is significantly higher than 1.
Conclusion: Sleep quality is an important influencing factor of MCI, and there is a threshold effect in the above association. According to this correlation, health professionals can take measures to improve the sleep quality of older adult patients with multimorbidity to reduce the occurrence of MCI.
In 2020, the total number of older adult people aged 60 and above in Chinese mainland will be 264 million, accounting for 18.7% of the total population (1). With the aggravation of population aging, the number of older adult patients with chronic diseases has also increased year by year, and the coexistence of two or more chronic diseases is more common. There are many older adult patients with multimorbidity in China who have Mild cognitive impairment (MCI) and sleep disorders (2). Investigation shows that about 50–60% of the older adult in China complain about poor sleep. The prevalence of MCI in the older adult over 60 years old is estimated to be 15.5% (3). Most patients regard MCI symptoms and sleep problems as a normal aging process. Because of insufficient understanding of the disease, they usually refuse to see a doctor.
Multimorbidity means that a person has two or more chronic health problems at the same time (4). MCI means that the decline of cognitive ability is greater than the expected degree of individual age and education level, but it has no obvious influence on daily life activities (5). Due to the decline of physical function, the older adult with multimorbidity have changed their sleep structure and circadian rhythm, which makes them more likely to cause sleep quality decline and even sleep disorders (6). In recent years, it is considered that sleep is a controllable risk factor for MCI (7). Sleep changes may be a valuable sign of early MCI (8).
At present, many studies have found that the decline of sleep quality and the occurrence and development of MCI are vicious cycles (9). It is difficult for older adult patients with multimorbidity to have a good and deep sleep when they have symptoms related to diseases (10). Sleep problems can lead to or aggravate the occurrence and development of MCI, and even develop into Alzheimer’s disease (11). Therefore, it is of great practical significance to deeply understand the sleep situation of older adult patients with multimorbidity, and to give targeted prevention and early intervention, so as to reduce the influence of MCI on the development of chronic diseases of the older adult and alleviate the medical burden brought by the rapid increase of social medical needs of older adult patients.
In recent years, there have been many studies on the relationship between sleep problems and cognitive dysfunction in older adult patients with chronic diseases, but there are few studies on the relationship between sleep problems and MCI in older adult patients with multimorbidity. Therefore, in our study, we use Pittsburgh Sleep Quality ScaleI (PSQI) and Montreal Cognitive Assessment Scale (MoCA) to evaluate the sleep quality and MCI of older adult patients with multimorbidity. To study the potential correlation between sleep quality and MCI in order to control the development of MCI into Alzheimer’s disease by controlling sleep quality. In the past, researchers liked to study the sleep problems and cognitive dysfunction of older adult patients with chronic diseases separately, and included them as classified variables in the model analysis (12–15). This will lose some information as a continuous variable. At present, there is little research on the relationship between PSQI score as a continuous variable and MCI risk. In this study, the sleep quality and MCI of older adult patients with chronic diseases in Shanghai and Sichuan were investigated, and the survey data were analyzed to explore the relationship between PSQI score and MCI through RCS model.
From July 2024 to September 2024, older adult patients with chronic diseases were collected in hospitals in Sichuan and Shanghai. The study included both inpatients and outpatients. Inclusion criteria: ①Age ≥ 60 years old; ② Adapting to multimorbidity (two or more coexisting diseases, including but not limited to hypertension, diabetes, cardiovascular disease, chronic obstructive pulmonary disease (COPD), and arthritis); Exclusion criteria: ① Age < 60 years old; ② Severe mental disorders; ③ Severe visual and hearing impairment; ④Diseases of central nervous system (e.g., stroke, Parkinson’s disease). All participants knew the purpose of the survey and signed an agreement authorizing the collection of data.
General information questionnaire was used to investigate and test the basic characteristics of participants, such as sex, age, BMI, marital status, education attendance and so on. Sleep quality was evaluated by Pittsburgh Sleep Quality Index (PSQI). PSQI can evaluate the sleep quality of patients within 1 month, including the overall score and seven component scores (16). The component items are as follows: subjective sleep quality, sleep latency, sleep duration, sleep efficiency, sleep disorders, use of sleep drugs and daytime dysfunction (17). The score range of each part is 0–3, with a perfect score of 21. The higher the score, the worse the sleep quality (18). Cognitive function was assessed by Montreal cognitive assessment (MoCA) (19). The main scoring items of MoCA scale include naming, attention, language, abstraction, delayed recall, orientation, visual space and executive function (20). Divide normal and MCI with 26 as the demarcation value, score ≥ 26 is Non-MCI, and MCI means score < 26 (21).
A questionnaire survey was conducted in Sichuan and Shanghai from June 2024 to July 2024. Investigators have received unified training. In order to ensure that investigators describe and explain the contents of the investigation in the same way, all our investigators are the same group of uniformly trained personnel. The sample size was determined using sociological research methods and calculated using the following formula: n = p × z2 × (1 – p)/e2, where prefers to the overall proportion, z refers to the confdence coefcient, and e refers to the allowable error (22). If p = 0.8, the maximum variance could obtain a relatively conservative sample size. At the same time, the allowable error of 5–10% and the placing interval of 95% were selected in this survey, the calculated available sample size should be at least 683. See Figure 1 for the sample collection flow chart.
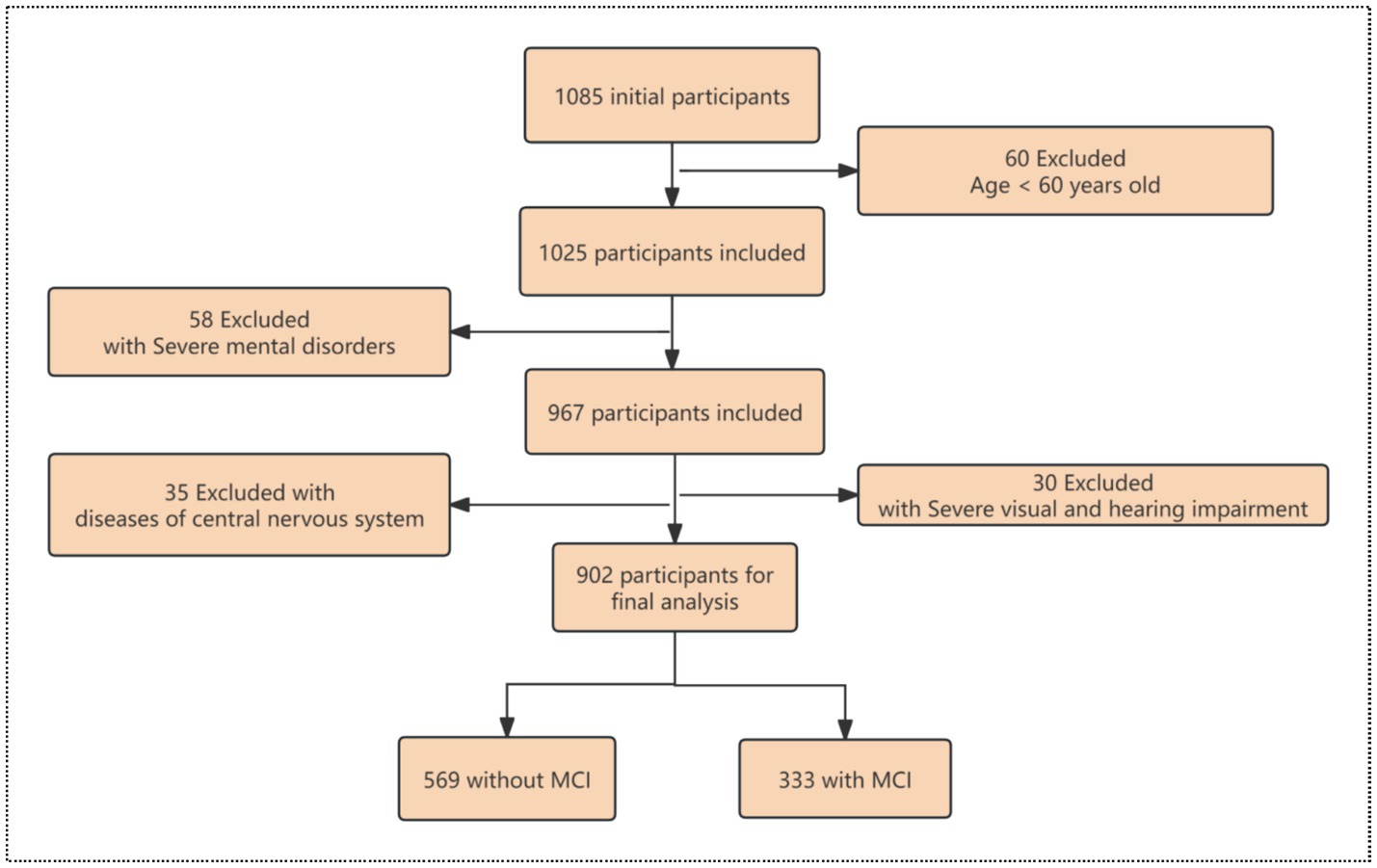
Figure 1. The flow chart of sample collection.
Participants were divided into two groups according to whether they had MCI. All continuous variables were tested for normality using the Shapiro–Wilk test. Variables that did not meet the normality assumption were log-transformed. For weighted feature description, continuous variables were presented as means ± standard error (SE) and categorical variables were presented by percentage (%) (23). The difference of baseline variables was tested by t test and chi-square test. Using logistic regression model, the odds ratio (OR) and 95% confidence interval (CI) of the correlation between Sleep quality and MCI were discussed. Model 1, no covariate was adjusted. Model 2 was adjusted for sex, age, BMI, marital status, education attainment, living conditions, social contact, exercise, smoking, drinking. Model 3 added number of chronic diseases, number of types of medication, PSQI score, subjective sleep quality, sleep latency, sleep duration, sleep efficiency, sleep disorders, use of sleep drugs and daytime dysfunction in model 2. RCS is used to explore nonlinear problems (24). In addition, we also conducted subgroup analysis to investigate whether this association was changed by social demography, disease-related conditions or lifestyle characteristics in the fully adjusted model (25). Then a two-segment linear regression model is established to calculate the turning point. All statistical analysis was carried out by R 4.3.3 software, and p-values<0.05 was considered to be statistically significant.
There are 902 valid samples in this study, of which 333 (36.9%) have MCI. The age range of all participants is 60–91 years old, with an average age of 67.76 years old. There are more men than women with MCI, and there are more people with low education than those with high education. Among the related factors of diseases, the number of chronic diseases ranges from 2 to 6, and the number of types of medication ranges from 0 to 7. The score of PSQI is 2–18, with an average score of 11.13. The scores of seven components of sleep quality and the occurrence of MCI were analyzed by t test, and it was found that there was significant difference between each component and the occurrence of MCI. MoCA score range is 7–30. The MoCA score of MCI patients is lower than that of Non-MCI patients (See Table 1 for details).
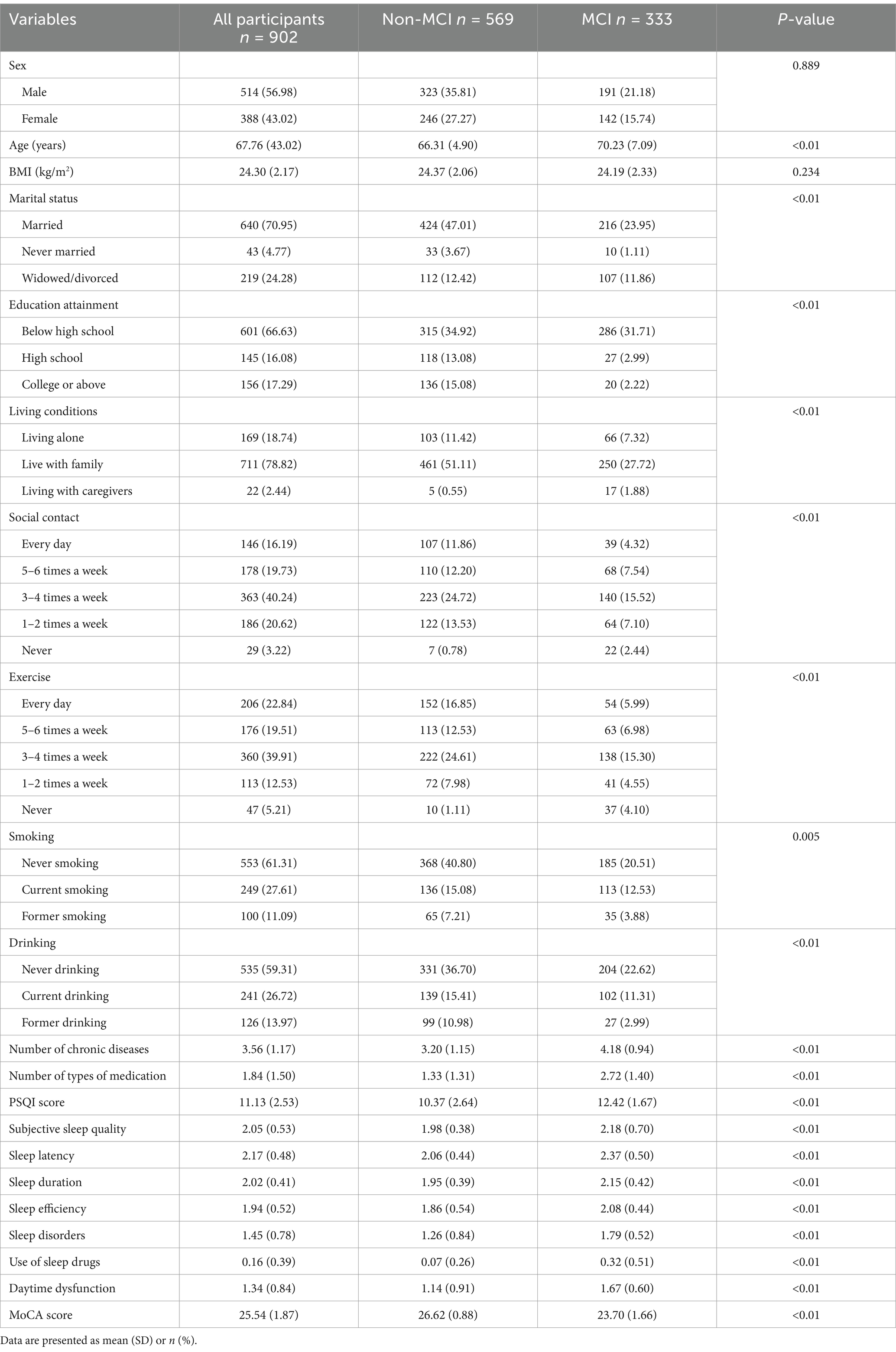
Table 1. Demographic characteristics and disease-related factors of the study population.
In all three models, PSQI score is significantly correlated with MCI (see Table 2 for details). Considering the significant relationship between PSQI score and MCI, we conducted a piecewise regression analysis (see Table 3 for details). The inflection point of MCI’s PSQI scoring relationship is 12. On this basis, we adopt a cubic spline model based on model 3 (see Figure 2). With the increase of PSQI score, the OR of correlation between PSQI score and MCI increases. When PSQI score reaches 12, OR is significantly higher than 1.
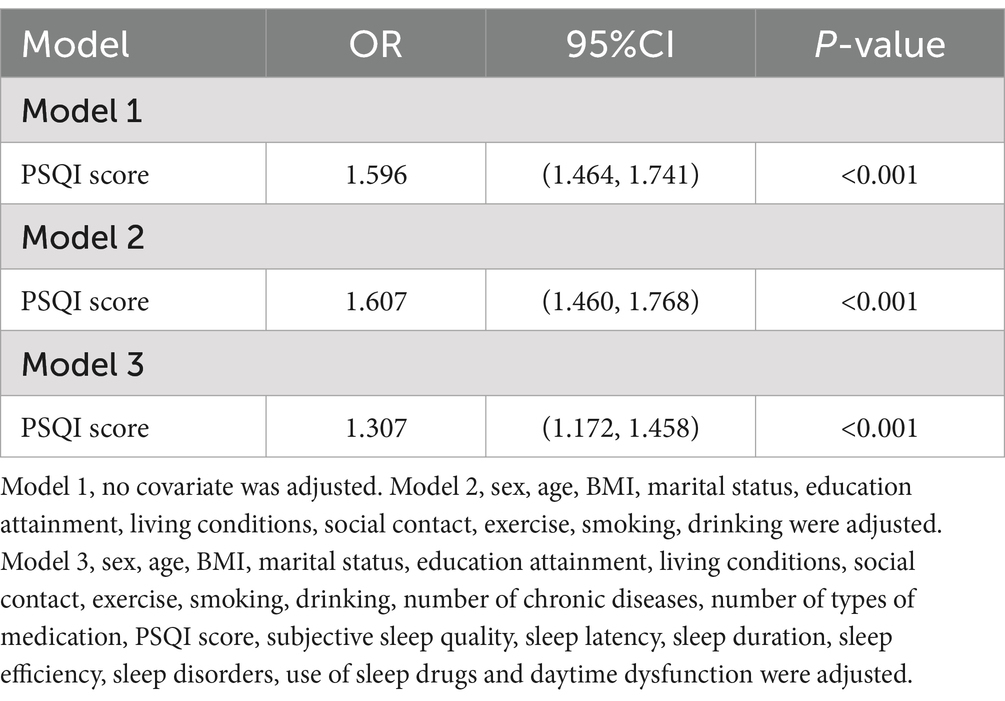
Table 2. Logistic regression results of associations between sleep quality and MCI.
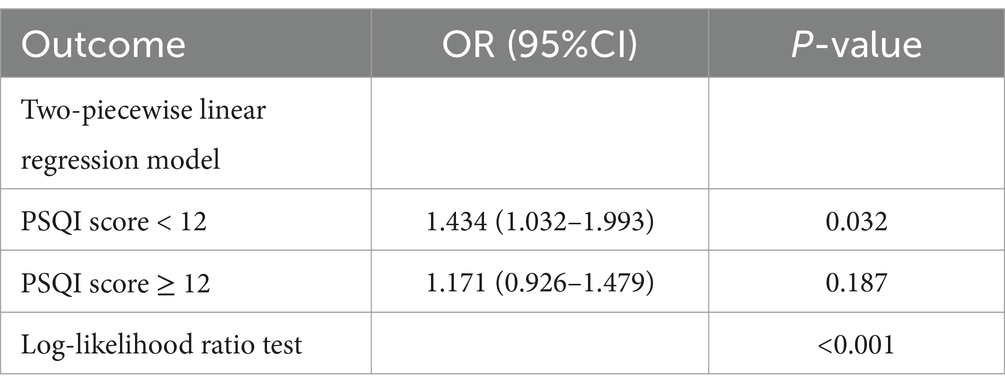
Table 3. Threshold effect analysis between sleep quality and MCI.
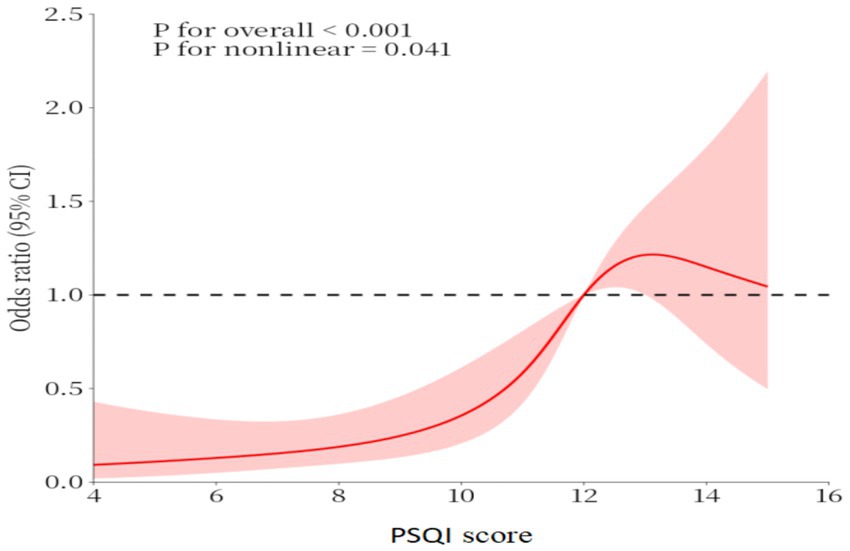
Figure 2. The dose–response relationship between PSQI score and MCI.
A total of 902 older adult patients with multimorbidity were included in this study. The age range of all participants was 60–91 years, with an average age of 67.76 years. The number of chronic diseases ranged from 2 to 6 with an average of 3.56. The possible reasons are as follows: the pathological states of various chronic diseases in the older adult will affect each other, and the interweaving of various chronic diseases will lead to the aggravation of brain ischemia and hypoxia and form a vicious circle (26).
In this study, the total score of PSQI should be used as the overall evaluation of sleep quality. Our study found that PSQI score is positively correlated with the OR of MCI. The score of MCI group is significantly higher than that of non-MCI group. After adjusting the related confounding factors, it is still found that the PSQI score is high, and the risk of MCI in older adult patients with multimorbidity is higher. This is consistent with the research results of McKinnon et al. (27). Some studies have pointed out that the increase of serum cortisol and corticotropin-releasing hormone is related to the decline of cognitive ability (28). However, the levels of serum cortisol and corticotropin-releasing hormone increased in the older adult population with decreased sleep quality (29).
Mayer et al. (7) used PSQI to evaluate sleep quality and analyze the relationship between sleep disorder and MCI. However, in their study, the PSQI score was divided into five groups, which were divided into sleep disorder group and normal sleep group. In our research, PSQI is regarded as a continuous variable, and the RCS model is adopted. It is found that the score of PSQI has a threshold, and subgroup analysis further confirms these results. When PSQI score reaches 12, OR is significantly higher than 1. This shows that when the PSQI score is higher than 12, it is the risk factor for cognitive decline. Higher threshold may reflect the compounded effects of multimorbidity on sleep quality and cognitive function. The lack of association in patients with severe sleep disorders (PSQI≥12) may be due to ceiling effects or the presence of other confounding factors that were not fully accounted for in the analysis.
Sleep is a changeable risk factor. Based on the results of this study, it is found that the problem of sleep quality should be taken into account when formulating intervention measures for MCI in the older adult with multimorbidity. Keeping good sleep behavior, reducing sleep latency, improving sleep efficiency and improving daytime sleepiness may be one of the measures to prevent MCI in the older adult with multimorbidity or delay the development of MCI into dementia.
Previous studies mostly discussed the relationship between sleep quality and MCI by classified variables, or the linear relationship between PSQI score and MoCA score, which limited the comprehensive interpretation of the relationship between PSQI and MCI abnormal illness (9, 27, 30), while the RCS model is a kind of nonlinear regression model, which can capture the nonlinear relationship between independent variables and dependent variables more flexibly and has good explanatory power (24). MCI is a reversible or potentially reversible clinical syndrome (31). Early identification and effective intervention are helpful to reverse the occurrence of MCI.
The sample size of this study is 902 cases, which cannot represent all the older adult people with comorbidity, and more centers and larger samples are needed in the future. Although the inclusion of exclusion criteria and statistical models controlled some confounding factors, the results were still influenced by unmeasured or not excluded interference factors, and related factors will be further strictly controlled in future research. This study is a cross-sectional study. Prospective cohort study is needed to further clarify the causal relationship between sleep quality and MCI in older adult with multimorbidity.
Our study found that there is a nonlinear correlation between PSQI score and MCI in the older adult with multimorbidity after adjusting for potential confounding factors. Sleep quality is an important influencing factor of MCI, and there is a threshold effect in the above association. According to this correlation, health professionals can take measures to improve the sleep quality of older adult patients with multimorbidity to reduce the occurrence of MCI. In addition, the evidence of this study also encourages older adult patients with multimorbidity to evaluate their sleep quality and reduce the occurrence of MCI.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
The studies involving humans were approved by the Ethics Review Committee of the Shanghai University of Medicine and Health Sciences (No.2023-hxxm-01-612401197903300537). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
TY: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. GZ: Data curation, Investigation, Methodology, Supervision, Writing – review & editing. SP: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declare that no Gen AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
MCI, Mild Cognitive Impairment; RCS, Restricted Cubic Spline; PSQI, Pittsburgh Sleep Quality Scale; MoCA, Montreal Cognitive Assessment Scale; BMI, Body Mass Index; SE, standard error; OR, Odds Ratio; CI, Confidence Intervals.
1. Zhang, R, Sun, L, Jia, A, Wang, S, Guo, Q, Wang, Y, et al. Effect of heatwaves on mortality of Alzheimer's disease and other dementias among elderly aged 60 years and above in China, 2013-2020: a population-based study. Lancet Reg Health West Pac. (2024) 52:101217. doi: 10.1016/j.lanwpc.2024.101217
2. Miller, MA. The role of sleep and sleep disorders in the development, diagnosis, and management of neurocognitive disorders. Front Neurol. (2015) 6:224. doi: 10.3389/fneur.2015.00224
3. Yang, Y, Xiao, M, Leng, L, Jiang, S, Feng, L, Pan, G, et al. A systematic review and meta-analysis of the prevalence and correlation of mild cognitive impairment in sarcopenia. J Cachexia Sarcopenia Muscle. (2023) 14:45–56. doi: 10.1002/jcsm.13143
4. Skou, ST, Mair, FS, Fortin, M, Guthrie, B, Nunes, BP, Miranda, JJ, et al. Multimorbidity. Nat Rev Dis Primers. (2022) 8:48. doi: 10.1038/s41572-022-00376-4
5. Abramowitz, A, and Weber, M. Management of MCI in the outpatient setting. Curr Psychiatry Rep. (2024) 26:413–21. doi: 10.1007/s11920-024-01514-3
6. Wood, H. Diabetes could hasten MCI-to-AD conversion. Nat Rev Neurol. (2024) 20:456. doi: 10.1038/s41582-024-00996-2
7. Mayer, G, Frohnhofen, H, Jokisch, M, Hermann, DM, and Gronewold, J. Associations of sleep disorders with all-cause MCI/dementia and different types of dementia - clinical evidence, potential pathomechanisms and treatment options: a narrative review. Front Neurosci. (2024) 18:1372326. doi: 10.3389/fnins.2024.1372326
8. Cogné, É, Postuma, RB, Chasles, MJ, De Roy, J, Montplaisir, J, Pelletier, A, et al. Montreal cognitive assessment and the clock drawing test to identify MCI and predict dementia in isolated REM sleep behavior disorder. Neurology. (2024) 102:e208020. doi: 10.1212/WNL.0000000000208020
9. Rao, RV, Subramaniam, KG, Gregory, J, Bredesen, AL, Coward, C, Okada, S, et al. Rationale for a multi-factorial approach for the reversal of cognitive decline in Alzheimer's disease and MCI: a review. Int J Mol Sci. (2023) 24:1659. doi: 10.3390/ijms24021659
10. Teverovsky, EG, Gildengers, A, Ran, X, Jacobsen, E, Chang, CCH, and Ganguli, M. Benzodiazepine use and risk of incident MCI and dementia in a community sample. Int Psychogeriatr. (2024) 36:142–8. doi: 10.1017/S1041610223000455
11. Pak, VM, Onen, SH, Bliwise, DL, Kutner, NG, Russell, KL, and Onen, F. Sleep disturbances in MCI and AD: neuroinflammation as a possible mediating pathway. Front Aging Neurosci. (2020) 12:69. doi: 10.3389/fnagi.2020.00069
12. Deyang, T, Baig, MAI, Dolkar, P, Hediyal, TA, Rathipriya, AG, Bhaskaran, M, et al. Sleep apnoea, gut dysbiosis and cognitive dysfunction. FEBS J. (2024) 291:2519–44. doi: 10.1111/febs.16960
13. Wang, J, Tian, Y, Qin, C, Meng, L, Feng, R, Xu, S, et al. Impaired glymphatic drainage underlying obstructive sleep apnea is associated with cognitive dysfunction. J Neurol. (2023) 270:2204–16. doi: 10.1007/s00415-022-11530-z
14. Zhou, L, Kong, J, Li, X, and Ren, Q. Sex differences in the effects of sleep disorders on cognitive dysfunction. Neurosci Biobehav Rev. (2023) 146:105067. doi: 10.1016/j.neubiorev.2023.105067
15. Yin, C, Zhang, M, Jin, S, Zhou, Y, Ding, L, Lv, Q, et al. Mechanism of Salvia miltiorrhiza Bunge extract to alleviate chronic sleep deprivation-induced cognitive dysfunction in rats. Phytomedicine. (2024) 130:155725. doi: 10.1016/j.phymed.2024.155725
16. Zitser, J, Allen, IE, Falgàs, N, Le, MM, Neylan, TC, Kramer, JH, et al. Pittsburgh sleep quality index (PSQI) responses are modulated by total sleep time and wake after sleep onset in healthy older adults. PLoS One. (2022) 17:e270095. doi: 10.1371/journal.pone.0270095
17. Jerković, A, Mikac, U, Matijaca, M, Košta, V, Ćurković Katić, A, Dolić, K, et al. Psychometric properties of the Pittsburgh sleep quality index (PSQI) in patients with multiple sclerosis: factor structure, reliability, correlates, and discrimination. J Clin Med. (2022) 11:2037. doi: 10.3390/jcm11072037
18. De Gennaro, N, Poliseno, M, Dargenio, A, Balena, F, Fiordelisi, D, Spada, V, et al. Pittsburgh sleep quality index (PSQI) changes in virologically suppressed people living with HIVSwitching to long-acting cabotegravir and rilpivirine. Biomedicines. (2024) 12:1995. doi: 10.3390/biomedicines12091995
19. Lorenzo-Mora, AM, López-Sobaler, AM, Bermejo, LM, González-Rodríguez, LG, Cuadrado-Soto, E, Peral-Suárez, Á, et al. Association between mineral intake and cognition evaluated by Montreal cognitive assessment (MoCA): a cross-sectional study. Nutrients. (2023) 15:4505. doi: 10.3390/nu15214505
20. Danquah, MO, Yan, E, Lee, JW, Philip, K, Saripella, A, Alhamdah, Y, et al. The utility of the Montreal cognitive assessment (MoCA) in detecting cognitive impairment in surgical populations - a systematic review and meta-analysis. J Clin Anesth. (2024) 97:111551. doi: 10.1016/j.jclinane.2024.111551
21. Mascarenhas, FL, Sheppard, DP, and Chaytor, NS. MoCA Intraindividual cognitive variability in older adults with type 1 diabetes. Alzheimer Dis Assoc Disord. (2023) 37:152–5. doi: 10.1097/WAD.0000000000000534
22. Andrade, C. Sample size and its importance in research. Indian J Psychol Med. (2020) 42:102–3. doi: 10.4103/IJPSYM.IJPSYM_504_19
23. Maia, IS, Kawano-Dourado, L, Damiani, LP, Fitzgerald, M, Lewis, RJ, and Cavalcanti, AB. Update in statistical analysis plan of the RENOVATE trial. Crit Care Resusc. (2023) 25:113–4. doi: 10.1016/j.ccrj.2023.06.008
24. Li, Z, Zhu, Y, Zhang, W, and Mu, W. Rcs signal transduction system in Escherichia coli: composition, related functions, regulatory mechanism, and applications. Microbiol Res. (2024) 285:127783. doi: 10.1016/j.micres.2024.127783
25. You, Y, Chen, Y, Zhang, Q, Yan, N, Ning, Y, and Cao, Q. Muscle quality index is associated with trouble sleeping: a cross-sectional population based study. BMC Public Health. (2023) 23:489. doi: 10.1186/s12889-023-15411-6
26. Larvin, H, Kang, J, Aggarwal, VR, Pavitt, S, and Wu, J. Systemic multimorbidity clusters in people with periodontitis. J Dent Res. (2022) 101:1335–42. doi: 10.1177/00220345221098910
27. McKinnon, AC, Beath, AP, and Naismith, SL. Relationships between sleep quality, depressive symptoms and MCI diagnosis: a path analysis. J Affect Disord. (2019) 256:26–32. doi: 10.1016/j.jad.2019.05.045
28. Sroykham, W, and Wongsawat, Y. Effects of brain activity, morning salivary cortisol, and emotion regulation on cognitive impairment in elderly people. Medicine (Baltimore). (2019) 98:e16114. doi: 10.1097/MD.0000000000016114
29. Dressle, RJ, Feige, B, Spiegelhalder, K, Schmucker, C, Benz, F, Mey, NC, et al. HPA axis activity in patients with chronic insomnia: a systematic review and meta-analysis of case-control studies. Sleep Med Rev. (2022) 62:101588. doi: 10.1016/j.smrv.2022.101588
30. Yoon, E, Bae, S, and Park, H. Gait speed and sleep duration is associated with increased risk of MCI in older community-dwelling adults. Int J Environ Res Public Health. (2022) 19:7625. doi: 10.3390/ijerph19137625
31. Arevalo-Rodriguez, I, Smailagic, N, Roqué-Figuls, M, Ciapponi, A, Sanchez-Perez, E, Giannakou, A, et al. Mini-mental state examination (MMSE) for the early detection of dementia in people with mild cognitive impairment (MCI). Cochrane Database Syst Rev. (2021) 7:CD10783. doi: 10.1002/14651858.CD010783.pub3
Keywords: multimorbidity, RCS, sleep quality, MCI, PSQI
Citation: Yang T, Zheng G and Peng S (2025) Association between sleep quality and MCI in older adult patients with multimorbidity. Front. Public Health. 13:1547425. doi: 10.3389/fpubh.2025.1547425
Edited by:
Vahid Rashedi, University of Social Welfare and Rehabilitation Sciences, IranReviewed by:
Yang Li, Tongji University, ChinaCopyright © 2025 Yang, Zheng and Peng. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shuzhi Peng, cHN6MTk5NDkyMUAxNjMuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.