
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 26 March 2025
Sec. Environmental Health and Exposome
Volume 13 - 2025 | https://doi.org/10.3389/fpubh.2025.1546842
This article is part of the Research Topic Impact of Environmental Factors on the Health of Children and Older Adults View all 9 articles
 Min-Ming Li1,2†
Min-Ming Li1,2† Xian-Ting Jiao2,3†
Xian-Ting Jiao2,3† Jing Zhang1†Zhen-Yan Gao2Jia Cao2,4Jun-Xia Liu2Yu-Lin Yang1*
Jing Zhang1†Zhen-Yan Gao2Jia Cao2,4Jun-Xia Liu2Yu-Lin Yang1* Chong-Huai Yan2*
Chong-Huai Yan2*Aims: To evaluate the prevalence and risk factors of elevated blood lead levels (EBLL) among the pediatric population in China.
Methods: Questionnaire investigation about Lead exposure information, venous blood samples collection and BLL detection are conducted. A total of 32,543 subjects aged 0–6 years old (from 1 month old to under 7 years old) were recruited from May 2013 to March 2015 in 15 provinces of China.
Results: The overall weighted prevalence of EBLL which is defined as BLL ≥ 50 μg/L in this study is 4.1%, as for different geographical regions, with lowest prevalence in the western region of China, lowest prevalence in Shaanxi province and highest in Hebei province. In 0–3-Year-old children, female weighted prevalence of EBLL (4.0%) is higher than male (2.4%), while in 3–6-Year-old children, male (8.3%) is higher than female (6.3%). Bad hygienic habits, some kind of custom, using folk prescriptions, living on the ground floor, poor drinking water quality, indoor air pollution and passive smoking exposure remain risk factors of EBLL (BLL ≥ 50 μg/L) of 0–6-year-old (from 1 month old to under 7 years old) children in China, after adjustment of gender, age, geographical region, annual household income, educational background and occupation of the parents and caregivers.
Conclusion: This study reveals the prevalence and risk factors for EBLL (BLL ≥ 50 μg/L) in 0–6-Year-old Children of China. We hope this study will help public health education and inform policy for preventing and eradicating children’s lead poisoning in China.
Lead naturally occurs in the earth’s crust and has been used in industry, paint, gasoline, construction, pottery, folk medicines, and herbal remedies for centuries. Lead is pervasively present in the environment, slowly impacting health from early childhood and throughout life (1). When lead is absorbed in different ways, it enters the body, attaches to soft tissue, easily assimilated into the nervous system (2). Lead poisoning causes toxicity in several organ systems, such as central nervous system impairment what needed special attention, mainly manifested as impairing neurological development, reducing intelligence quotient, and generating negative behavior (3, 4). The adverse effects of childhood lead exposure have been well-documented, such as learning issues (5), behavior problems (6, 7), worsened cognition (8, 9), and the like (10–12). Even blood lead levels less than 50 μg/L are associated with irreversible neurocognitive and behavioral development impairments in infants and children who are more susceptible to lead toxicity (13, 14).
Lead poisoning has been recognized for centuries for its extensive application and environmental persistence (1, 13); however, lead exposure is still a critical public health problem globally, especially in developing countries (15), as poverty may lead to significant ongoing exposures (16).
As a developing country, China has experienced dramatic industrial and economic growth over the past decades, becoming one of the largest lead producers and consumers worldwide. Different sources of children lead exposure are reported in different countries affected by the economic, social and cultural levels. Children still face risks of lead exposure from coal burning, petroleum fuel consumption, e-waste recycling piles (17–19), ore and metal processing, lead-containing folk remedies (20–22), and poor living environment (19, 23–26).
In 2006 public guideline for the prevention of high BLLs and lead poisoning in children issued by the Ministry of Health in China stated that high blood lead syndrome in children should be recognized if the venous blood lead level reaches 100–199 μg/L two consecutive times. Furthermore, lead poisoning in children should be diagnosed if venous blood lead level is ≥200 μg/L two consecutive times (27). Since leaded gasoline was prohibited in 2000 in China, the children BLLs and the prevalence of lead poisoning have dramatically declined over the past 20 years (28, 29). However, the American Centers for Disease Control reports that there is no acceptable level of lead in the human body and that even minimal levels of lead can cause neurological damage to children (30). The Council of State and Territorial Epidemiologists’(CSTE) blood lead reference value is 3.5 μg/dL which is used to identify adults and children whose blood lead levels are higher than the 97.5th percentile of adults and children nationwide (30). Considering sensitivity to lead toxicity in children’s neurocognitive and behavioral development, even BLLs less than 50 μg/L, we defined BLL ≥ 50 μg/L as EBLL in this study, referring to acceptable children’s blood lead levels in 2012 by the American Centers for Disease Control.
For the lack of national epidemiological investigation of blood lead levels and Pb exposure risk factors of 0–6-Year-old children (from 1 month old to under 7 years old) in China, we conduct this national population-based cross-sectional survey. This study explores the prevalence of EBLL, defined as BLL ≥ 50 μg/L, and the risk factors of EBLL. We aim to reveal the epidemiological characteristics of EBLL and provide a theoretical basis for targeted preventive measures of lead exposure for children.
The study population is selected using a multi-stage stratified cluster random sampling technique. The survey methods and sampling details have been published elsewhere (31). The sampling steps are as follows: First, every five provinces were selected from Eastern China, Central China and Western China by the simple random sampling (SRS) method. According to the classification by the National Bureau of Statistics, Shanghai, Jiangsu, Hebei, Guangdong, and Fujian are categorized as eastern regions; Shanxi, Henan, Hunan, Jilin, and Hubei as central regions; and Shaanxi, Yunnan, Qinghai, Guangxi, Xinjiang as western regions. Second, within each selected province, a probabilistic proportional to size (PPS) sampling method was used to choose districts of major cities, medium and small cities and towns/villages of rural areas based on the population. According to the “China Small and Medium City Development Report (63)” and the “Regulations on the Statistical Division of Urban and Rural Areas,” cities with a resident population of over 1 million are classified as major cities, while those with a resident population of 1 million or less are categorized as small and medium-sized cities. Areas outside these designated urban regions are defined as rural areas. Third, children from 1 to 2 neighborhoods chosen by the SRS method within each selected district/village were investigated.
The study uses a multi-stage stratified cluster random sampling method. The formula is used to calculate the sample size for each stratification, in which as for 95% CI, Z sets to 1.96, p as expected prevalence rate set to 6%, based on the results of we previous meta-analysis that the pool lead poisoning rate of Chinese population aged 0–18 years old was 5.3% and the pool lead poisoning rate of children was from 4.7 to 9.5% of different age groups under 7 years old (excluding newborn) (29). The allowable error d setting to 2% is applied here. Design effect is applied when considering representativeness of 15 provinces of three regions (i.e., Eastern China, Central China, Western China), rural and urban areas (i.e., major cities, medium and small cities and rural areas), gender (i.e., male and female) and age (i.e., 0–36 months and 36–84 months) which are the stratified analysis factors. Consequently, this calculation resulted in a sample size of 24,390 Taking response rate of 90% into account, the final sample size was targeted at 27100. At last, there were over 30,000 samples collected.
The survey is strictly quality-controlled. All investigators undertaken by experienced medical professional, are well trained by project team to ensure using standardized questionnaire instructions, standard sample collection, preservation and transportation. Each questionnaire undergoes double scanning and entry, with 10% of the questionnaires being reviewed by the project quality control officers. We obtain sociodemographic information (gender, date of birth, nationality, education level, occupation, and annual family income), self-reported behavior tendencies (smoking, physical activity, hand-to-mouth activity, and washing hands before eating), and living environment for estimating potential lead exposure (folk prescriptions for treatment, customs and habits leading to potential lead exposure, industry around the house, and house location). We obtain the information through face-to-face interviews using a questionnaire of mostly closed-ended questions. We survey Uyghur participants jointly with a Uyghur language translator using a questionnaire translated into Uyghur language. The participants’ confidentiality and privacy are assured. After completion of the interview, anthropometric measurements and blood samples are obtained.
A trained nurse drew 3 milliliters of venous blood into a vacuum blood tube. EDTA (Na2) is used as an anticoagulant, and samples were stored at 4°C. Refrigerated batches of 100 tubes are sent in a box of ice to the central laboratory at the local site and stored at −20°C before measurement. Blood sample collection is performed in a clean room, far from pollution sources. Children are required to clean their hands with soap before blood collection. Blood lead concentration is measured using an atomic absorption spectrometry-graphite furnace (PerkinElmer Company, 900Z, United States). Quality control is performed using a sample test. The laboratory protocol includes daily calibration with five standards (1–50 μg/L; agreement <5%) and standard reference materials (Contox, Kaulson Laboratories, Inc., NJ, United States) to ensure the accuracy of the assay. The method’s limit of detection (LOD) is 1 ug/dL for BLL. No sample has a BLL less than the LOD. All plastic tubes used for blood lead tests are washed thoroughly, soaked with dilute nitric acid, rinsed with deionized water, and dried before use.
The study is approved by Ethics Committee of Xinhua Hospital affiliated with Shanghai Jiao Tong University School of Medicine (XHEC-C-2013-008). Signed consent forms are collected from the guardians of all children who participated in the study.
Data weighting is used as a statistical technique to adjust survey data to represent the target population. The design weight for adjusting the probability of being sampled for each individual unit of the smallest survey unit is computed by multiplying the sampling weight of each stage. As describing in study design section of this article, we applied three sampling steps and stratified sampling which divided the sample into subgroups as below: different provinces, urban areas and rural areas, different genders and different age groups. The formula is applied. N in formula is the total population, Nh represents the number of people in layer h of the population, n is the sample population, nh represents the population of layer h in the sample. We adjust the design weight using the no-answer factor, which is the reciprocal of the response rate. Given the known stratification structure of the population (such as urban and rural areas, age, gender, etc.), the sample is re-stratified and the weights of each stratum are adjusted to match the overall proportion. Population information refers to the data from The Sixth National Population Census of China in 2010. In this survey, the post-stratification weights were adjusted according to age and gender stratification.
Sample characteristics are summarized using descriptive statistics (n, mean, median, p25, p75). A threshold of 50 μg/L for BLLs is used to categorize BLLs into two groups. The socioeconomic status, residence characteristics, and potential risk factors for lead exposure among children are compared between different BLL groups. A logistic regression analysis is performed to estimate odds ratios (OR), 95% confidence intervals (CI), and p-values. IBM SPSS version 22 is used for statistical analysis. Statistical significance is set at a p-value of 0.05 (two-tailed test).
This population-based cross-sectional study is conducted to examine the prevalence and associated risk factors of EBLL (BLL ≥ 50 μg/L) among Chinese children aged 0–6 years old (from 1 month old to under 7 years old), and their blood samples are also obtained. We finally recruited 32,543 0–6-year-old children (from 1 month old to under 7 years old) from 15 provinces of China from May 2013 to March 2015 with 16,997 (52.2%) males and 15,546 (47.8%) females.
The weighted prevalence with BLL ≥50 μg/L (EBLL) in 0–6-year-old children (from 1 month old to under 7 years old) is 4.1%. There is significant difference of prevalence among different geographical regions of China with 2.7% in the western region much lower than the other two regions in China.
Considering geographic factor, children in rural areas of eastern (12.4%) and western (7.4%) regions have higher prevalence of EBLL than urban areas, while children in urban areas of middle or small-sized city in central region (7.4%) have higher prevalence of EBLL.
And prevalence of EBLL differs significantly by province, with the lowest in Shaanxi province (0.5%) and highest in Hebei province (18.5%) (Figure 1). There is significant difference in children EBLL prevalence of urban areas in major cities (1.8%), urban areas in medium and small cities (7.2%) and in rural areas (8.5%). However, there are significant differences in prevalence among different districts in some provinces. In Qinghai, highest prevalence of urban areas in major city (21.9%) and in middle or small-sized city (16.2%) are observed. In Hebei, highest prevalence of rural areas (41%) is observed (Table 1).
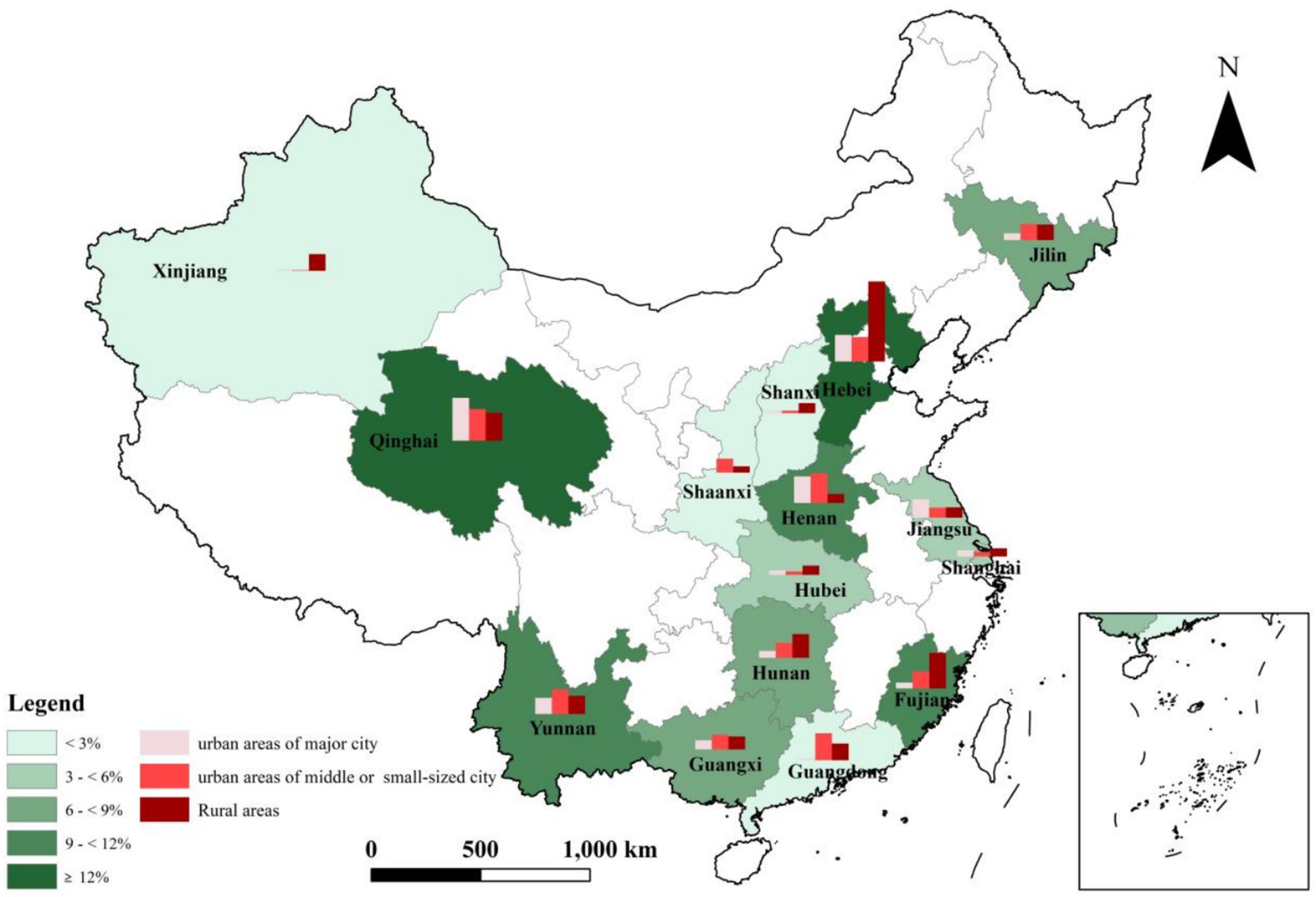
Figure 1. Distribution and EBLL prevalence in 0–6-year-old children of fifteen provinces in China.
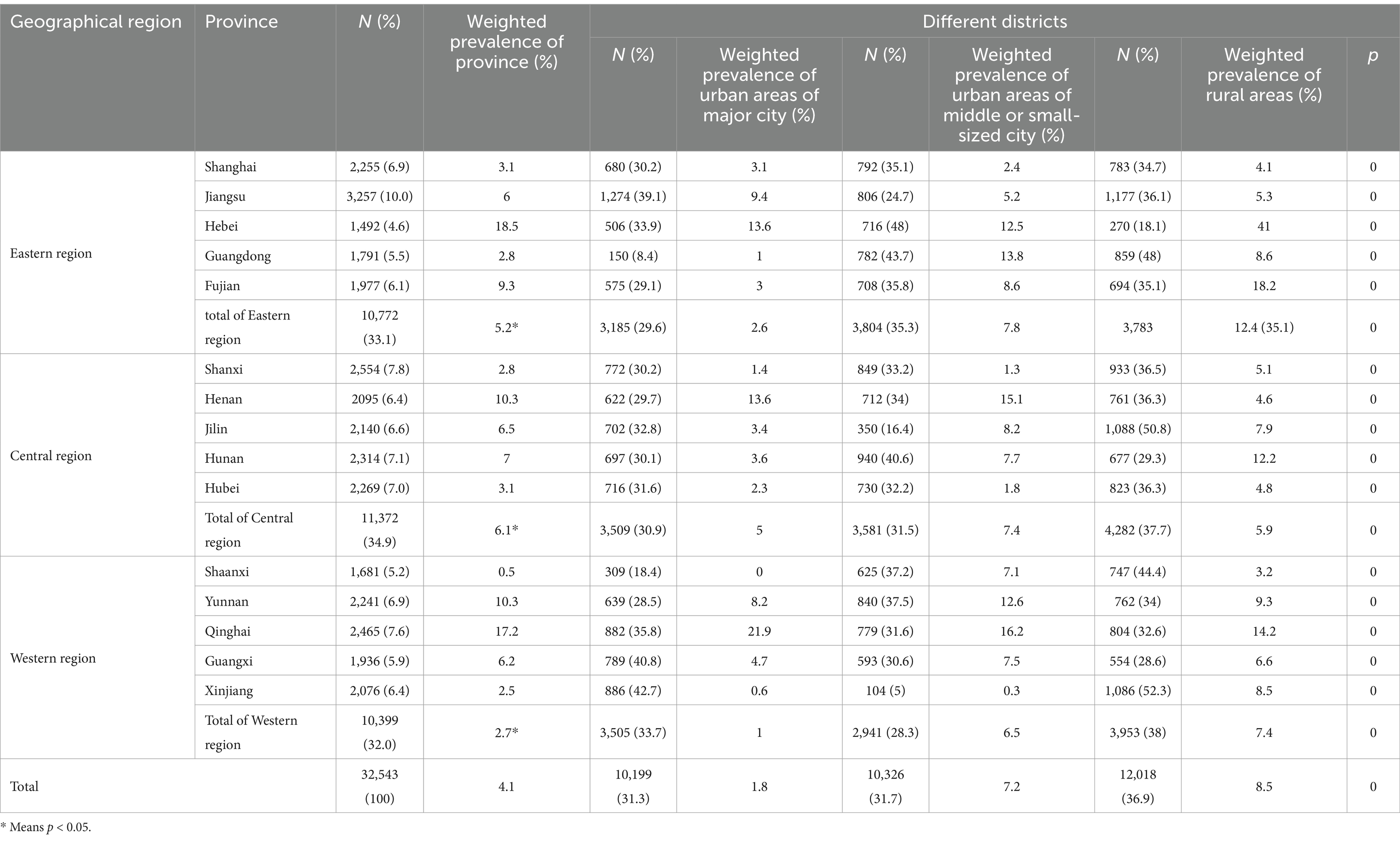
Table 1. The EBLL prevalence of children in different geographical regions of China.
The weighted prevalence of children with BLL ≥50 μg/L (EBLL) is higher in female (4.9%) than in male (3.7%). However, the situation varies among different age groups.
In 0–3-Year-old children, female weighted prevalence of EBLL (4.0%) is higher than male (2.4%), while in 3–6-Year-old children, male (8.3%) is higher than female (6.3%). Among different areas, female EBLL weighted prevalence in urban area of major cities (3.5%) is higher, while male EBLL weighted prevalence in urban area of middle or small-sized city (8.7%) and in rural areas (10.4%) are higher (Table 2; Figure 2).
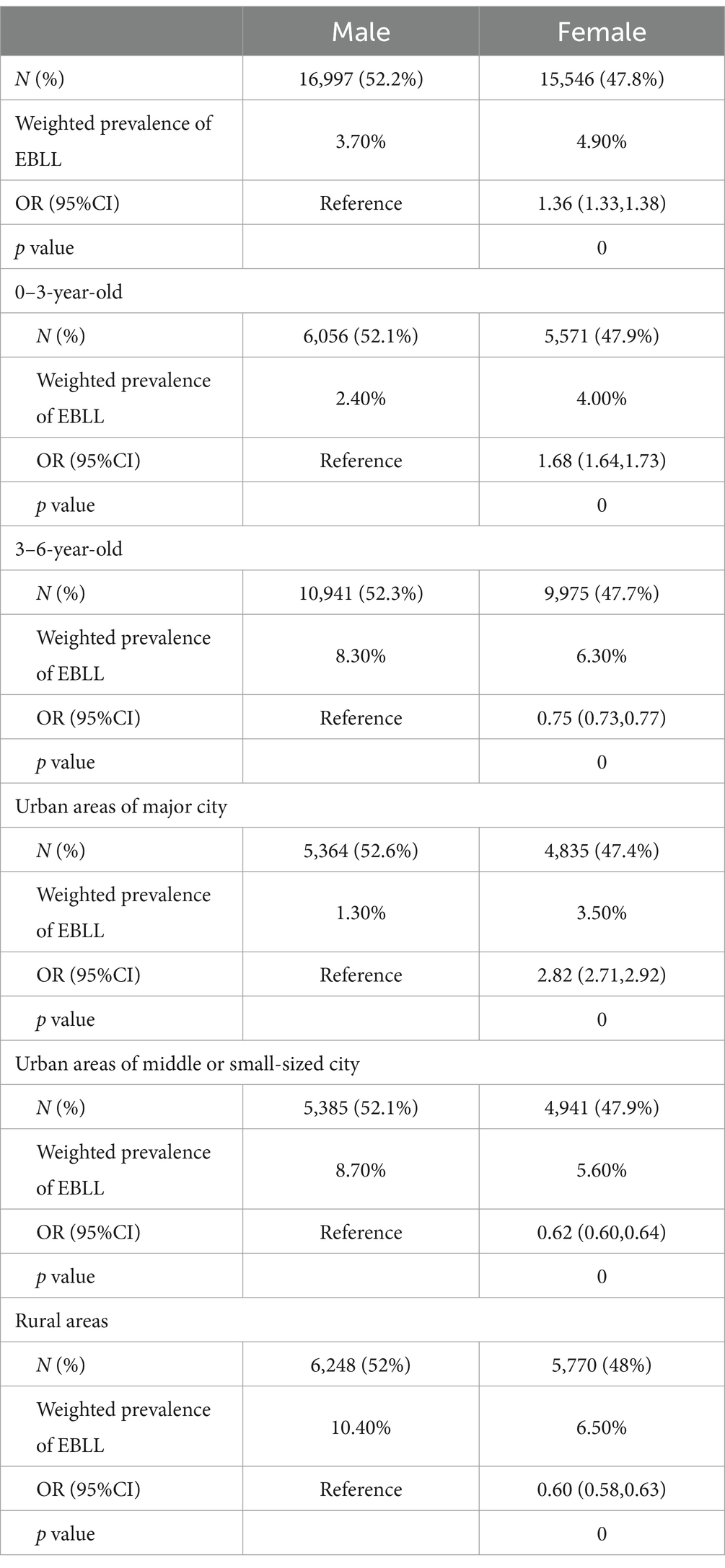
Table 2. EBLL prevalence of children with different ages and genders in China.
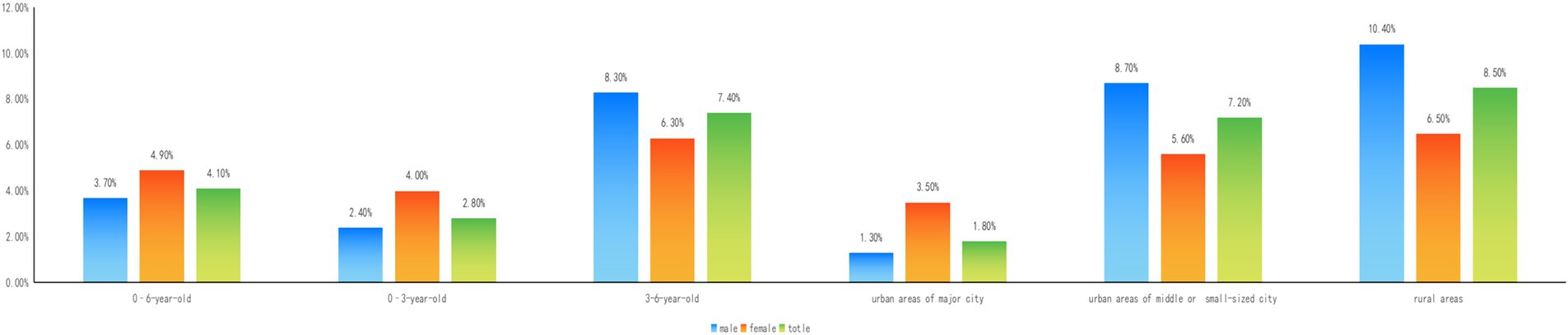
Figure 2. EBLL prevalence of children with different ages and genders in China.
Table 3 shows the EBLL (BLL ≥50 μg/L) proportion of 0–6-year-old (from 1 month old to under 7 years old) children in China by demographic characteristics. A specific population of mothers with low educational levels (ORilliterate = 6.43, ORprimary school = 4.55, ORmiddle school = 3.46, ORhigh school = 2.47), fathers (ORilliterate = 8.28, ORprimary school = 6.99, ORmiddle school = 4.86, ORhigh school = 3.57), primary caregivers (ORilliterate = 2.71, ORprimary school = 1.93, ORmiddle school = 1.76) refering to the person who lived with the child and was mainly responsible for the child’s daily living arrangements, mother’s occupation worker (OR = 1.53) or peasantry (OR = 1.31), father’s (ORworker = 1.24, ORpeasantry = 1.25), primary caregivers’ (ORworker = 1.19, ORpeasantry = 1.23), low economic income (OR <50,000 yuan = 3.3, OR50,000–250,000 yuan = 2.11) is at risk of EBLL compared to other groups.
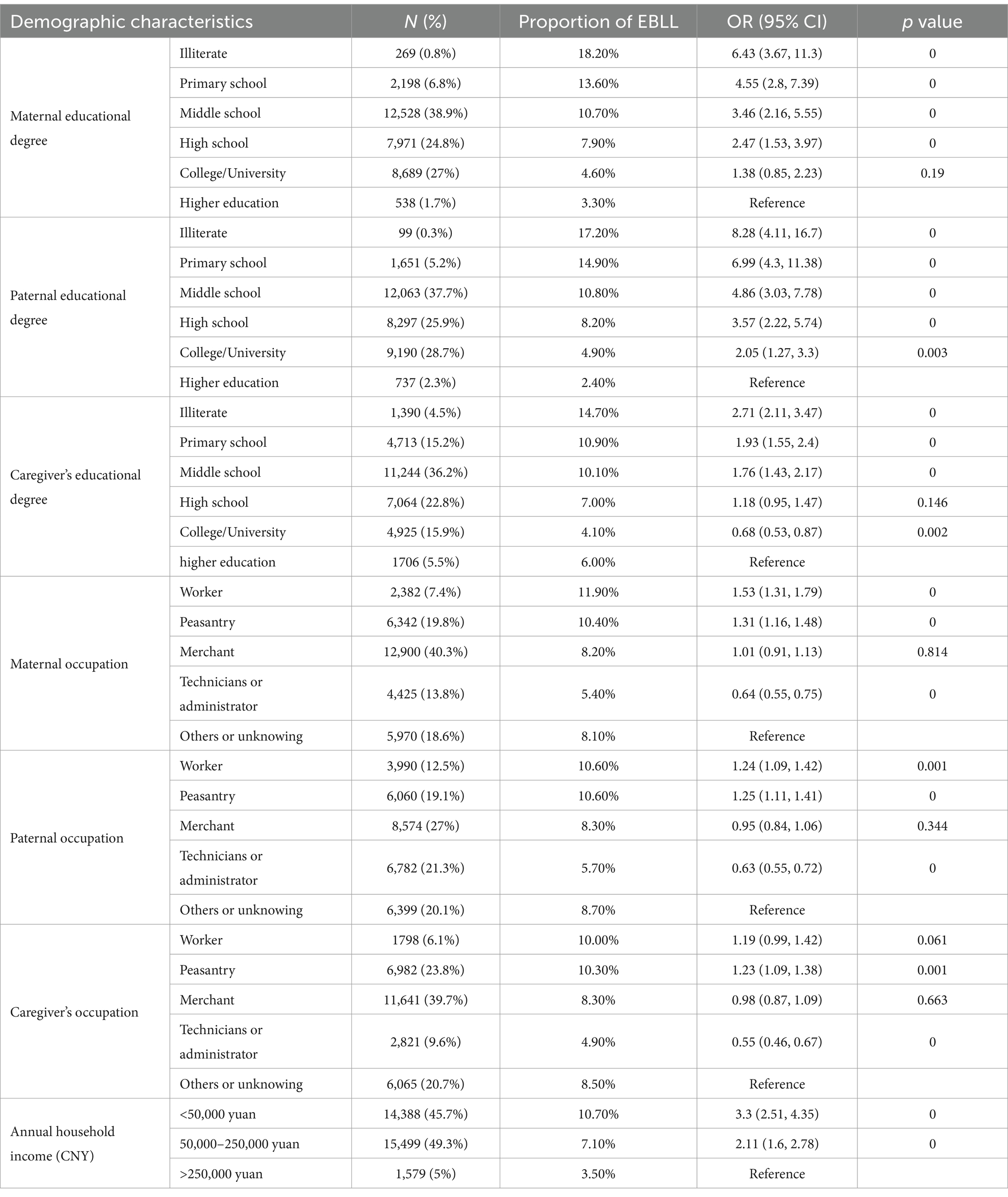
Table 3. Proportion of EBLL in children by demographic characteristics.
Information on children’s behavioral habits is also collected, including taking nutritional supplements, health habits, local customs, taking traditional Chinese medicine or folk prescriptions, and drinking water. Logistic regression analysis shows that risk factors of EBLL include unfrequently nail trimming (OR = 1.23, 1.35), sometimes/frequently hand-to-mouth activity (OR = 1.20, 1.39), frequently playing with dirt (OR = 1.37), contacting or burning tinfoil paper 3 times or more per year (OR = 1.24, 2.17), applying lead tetroxide (OR = 1.61), sometimes/frequent using traditional dinnerware such as tin pots (OR = 1.47, 1.85), using tap water, surface water, ground water (OR = 1.15, 1.60, 2.10). In contrast, protection factors include sometimes/frequently taking Zinc (OR = 0.75, 0.73), Iron (OR = 0.90, 0.83), Calcium (OR = 0.74, 0.61), Vitamin D supplements (OR = 0.72, 0.61), sometimes/frequently washing hands using soap or hand sanitizer before meals (OR = 0.76, 0.61).
After adjustment of gender, age, geographical region, annual household income, educational background and occupation of the parents and caregivers, risk factors concerning children’s behavior habits of EBLL include unfrequently nail trimming (OR = 1.14, 1.24), sometimes/frequently hand-to-mouth activity (OR = 1.23, 1.42), sometimes/frequently playing with dirt (OR = 1.12, 1.15), contacting or burning tinfoil paper 3 times or more per year (OR = 1.27, 1.96), applying lead tetroxide (OR = 1.56), sometimes/frequent using traditional dinnerware such as tin pots (OR = 1.34, 1.68), using folk prescriptions (OR = 1.23), using ground water (OR = 1.52). At the same time, sometimes/frequently taking Calcium (OR = 0.88, 0.82), Vitamin D supplements (OR = 0.86, 0.81), sometimes/frequently washing hands using soap or hand sanitizer before meals (OR = 0.87, 0.79) are protection factors (Table 4).
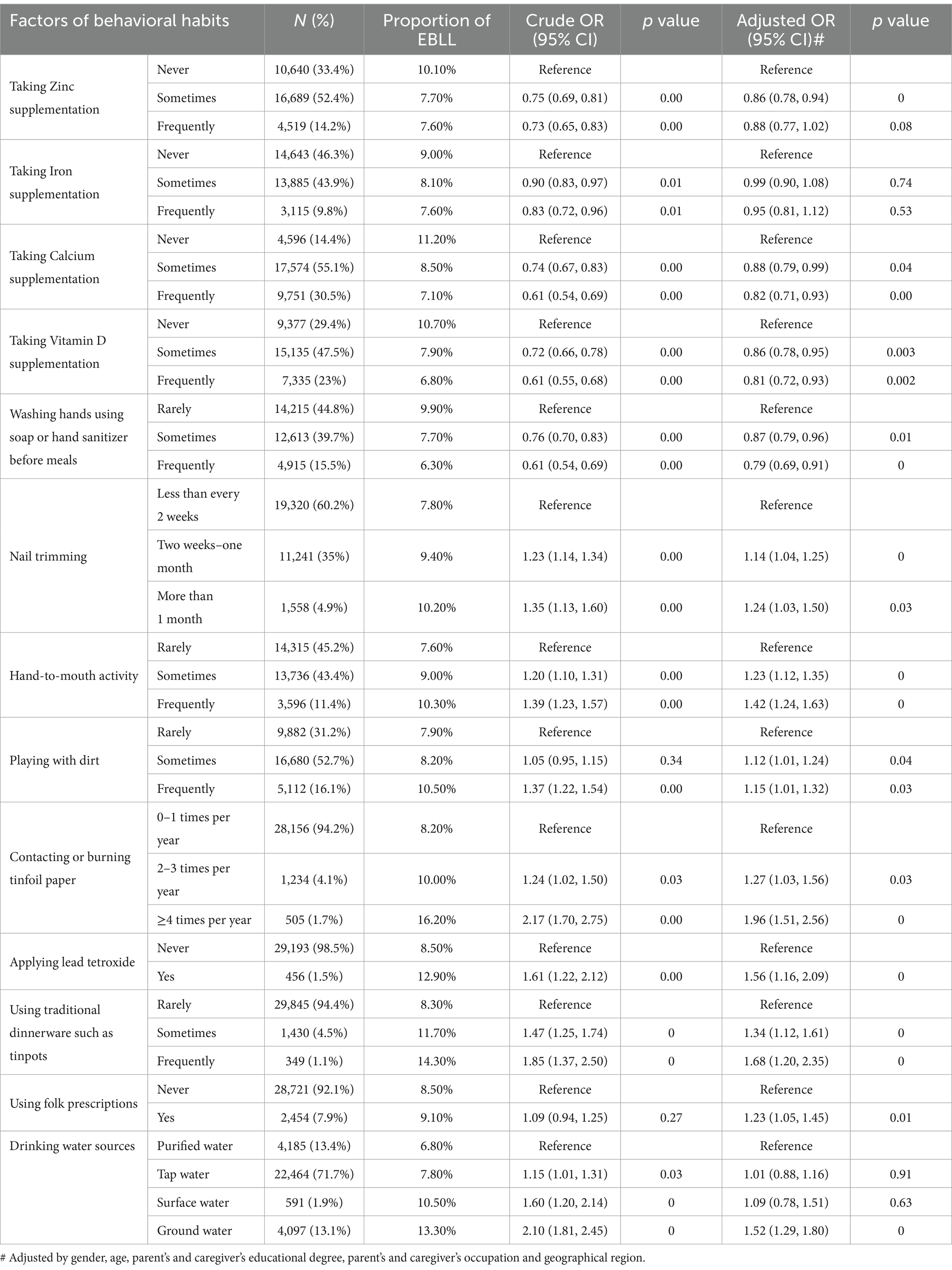
Table 4. Risk factors of children’s behavior habits associated with EBLL.
Logistic regression analysis shows that risk factors of children’s living environment associated with EBLL include living on the ground floor/The 2nd–3rd floor (OR = 1.93, 1.32), never/sometimes disusing first section of over night water (OR = 1.54, 1.35), frequently/sometimes passive smoking (OR = 1.32, 1.15), using coal or coal products/wood straw for cooking fuel (OR = 1.87, 1.41), using coal or coal products/wood straw for heating fuel (OR = 2.00, 1.55), none/chimney/window ventilated (OR = 1.60, 1.40, 1.28). There is no difference among houses of different distance to main road.
After adjustment of gender, age, geographical region, annual household income, educational background and occupation of the parents and caregivers, living on the ground floor (OR = 1.25), never/sometimes disusing first section of over night water (OR = 1.19, 1.16), frequently/sometimes passive smoking (OR = 1.24, 1.13), using coal or coal products for cocking fuel (OR = 1.50), using coal or coal products for heating fuel (OR = 1.68) remain risk factors of EBLL of 0–6-year-old children (Table 5).
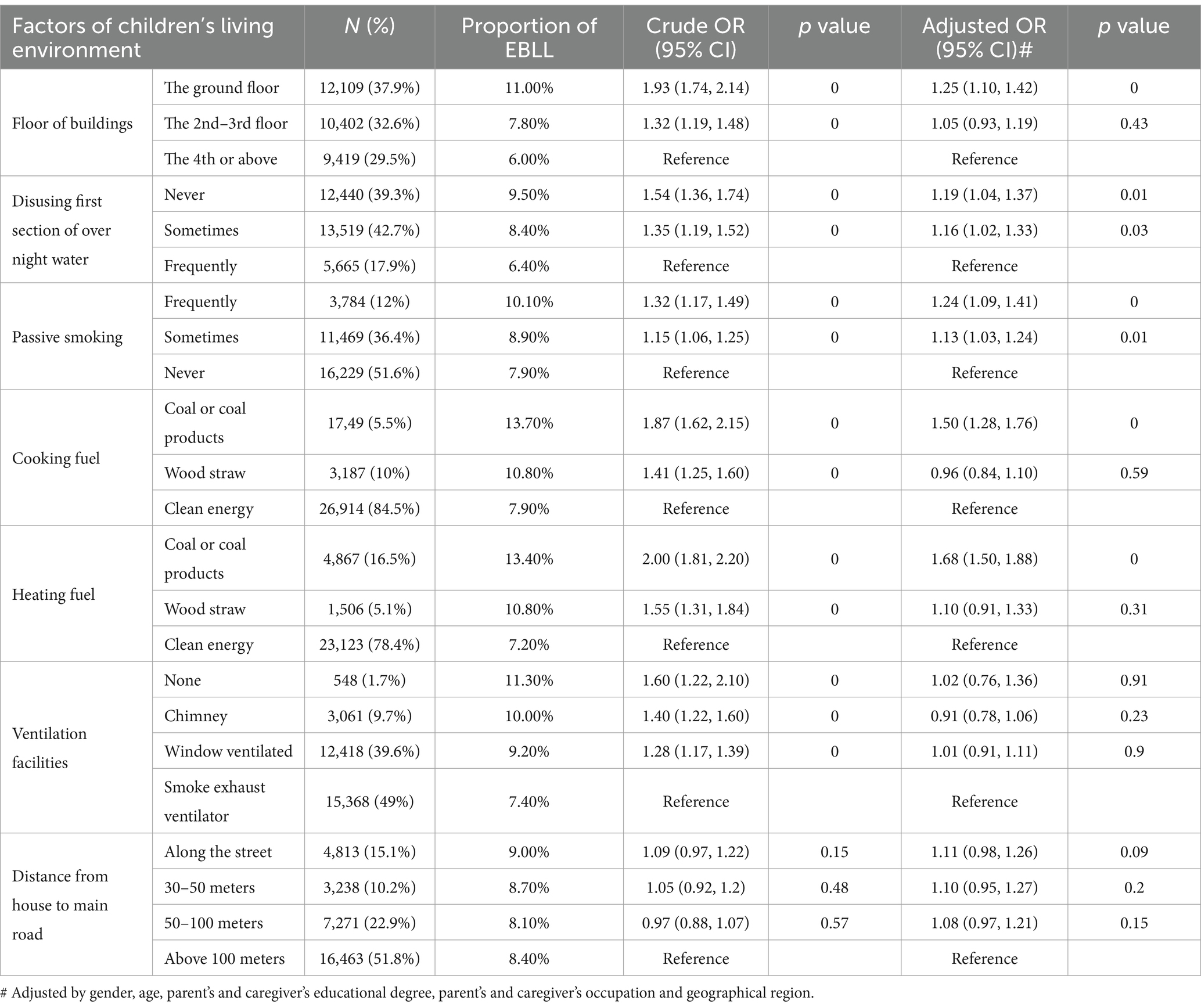
Table 5. Risk factors of children’s living environment associated with EBLL.
Phasing out leaded petrol in 2000 and a series of environmental protection measures have dramatically decreased children’s BLL and the prevalence of lead poisoning in China over the past 20 years (28, 29); however, the CDC (2022) reported that there is no acceptable level of lead in the human body and that minimal lead levels can cause neurological damage to children (30). Lead exposure remains an important public health problem in China because of its extensive use in the manufacturing industry with rapid economic growth (20). This study assesses the prevalence and risk factors of EBLL in 0–6-year-old children in China. This group has more susceptibility to lead exposure for frequent hand-to-mouth activity and higher sensitivity to lead toxicity due to an immature nervous system.
The prevalence of EBLL, defined in this study as BLL ≥ 50 μg/L, among 0–6-year-old children in China is 4.1%. The Council of State and Territorial Epidemiologists’ (CSTE) blood lead reference value is 35 μg/L in the United States. This value is used to identify adults and children whose blood lead levels are higher than the 97.5th percentile of adults and children nationwide (32, 33).
This study explores the prevalence of EBLL in different geographic regions of China. The weighted prevalence of EBLL in the central region is much higher than the other two regions in China, which is consistent with the result that the pool rate of lead poisoning in China’s central region is higher than those in eastern and western regions as previous research showed (29). This change might be interpreted as the western region gradually reducing pollution industries with increasing awareness of environmental protection (34). The increasing support for primary medical and health care in western China from the central and local governments also contributes to the improving of children’s health. However, among provinces of western region, the children prevalence of EBLL in Qinghai Province is at a high level, especially the prevalence of EBLL in urban areas of major city (21.9%) and in urban areas of middle or small-sized city (16.2%), which both ranked first in their respective categories. The investigation sites of children in urban areas in Qinghai province are located in Xining City, Delingha and Geermu City, where coal resources are abundant, and the proportion of manufacturing and mining industries is rising year by year. Delingha and Geermu City belong to Mongolian and Tibetan Autonomous Region, where multi-ethnic population lives together. Environment pollution caused by industrial development, different national cultures and living habits bring a great challenge of the improvement of children’s living environment and health habits in such areas. Those results in the study suggest that we should pay more attention to monitoring children’s blood lead levels and strengthening health education in areas with different national culture and rapid industrial development.
This survey reveals the prevalence of children EBLL of rural areas in China is much higher than of urban areas, which suggests that children in rural areas is at high risk of lead exposure. Considering geographic factor, children in rural areas of eastern and western regions is at high risk of EBLL, while children in urban areas of middle or small-sized city in central region should be pay more attention of possible lead exposure.
Some studies reveal the association between controlling environmental lead pollution in the atmosphere and considerable and sustained reduction of a population’s blood lead level (16, 35). We found that prevalence of EBLL differed significantly by province with the highest in Hebei province (18.5%), which dominated by industry with proportion accounts for 53.5%, especially the iron and steel industry as the first pillar industry in Hebei Province in 2011. Among different districts, weighted prevalence of EBLL in rural area of Hebei province, where mineral resources such as coal and coal bed methane were abundant, is high up to 41.0%. This result suggests that we should pay attention to screening the blood lead levels of children in mineral rich areas.
In this study, we observed weighted prevalence of children with BLL ≥50 μg/L (EBLL) is higher in female than in male, which seems inconsistent with previous results with higher proportion of BLL ≥50 μg/L in male than in female (31). However, in consideration of multi-stage sampling method of the survey, the proportion does not represent prevalence. In order to make the sample better reflect the overall characteristics, weighting issue should be taken into account when prevalence is mainly discussed in this paper. Though boys has higher BLLs compared to girls as previous results, the prevalence of girls with BLL ≥50 μg/L is higher. When subgroups are discussed, the situation varies among different age groups and area groups. In 0–3-Year-old children, female weighted prevalence of EBLL is higher than male, while in 3–6-Year-old children, male is higher than female. Also, in major city districts, female weighted prevalence of EBLL is higher than male, while in middle or small-sized city districts and in rural areas, the situation is on the contrary. The same phenomenon has been reported about age-dependent manner of EBLL prevalence increasing with age growth (36). In this survey, EBLL prevalence is higher in 3–6-year-old children, and BLL is also higher compared to 0–3-year-old children which published in our previous article (31). More boys’ bad habits and outdoor activity in 3–6-year-old children or in rural areas are likely to increase the risk of lead exposure (18, 35, 37).
As far as demographic characteristics are concerned, this study shows that mothers with low educational levels, fathers, caregivers, low socioeconomic family income and mother’s occupation worker or peasantry, fathers, caregivers seemed to have a higher prevalence of EBLL. However, the trends of both BLL and EBLL prevalence increased significantly in an age-dependent manner was not observed in this study, which was needed further research and exploration. As for family socioeconomic status, parents or caregivers with higher educational levels are better aware of avoiding lead exposure and promoting children’s good hygiene habits, reducing opportunities for children suffering from lead poisoning (26). Children living in poverty are more likely to reside in older houses with lead-based paint and lead-containing plumbing and have a higher likelihood of having nutritional imbalances such as iron deficiency (38).
This study examined risk factors related to children’s behavioral tendency toward EBLL. The results show that unfrequently nail trimming, sometimes/frequently hand-to-mouth activity, sometimes/frequently playing with dirt were the risk factors of EBLL, as previous research has shown (39–43).
In this study we also explored local traditional custom and folk prescription impacting on EBLL incidence. We found that contacting or burning tinfoil paper 3 times or more per year, sometimes/frequent using traditional dinnerware such as tin pots, applying lead tetroxide, using folk prescriptions were risk factors of children EBLL. Local customs and traditions (such as contacting or burning tinfoil paper several times or using tin pots as dinnerware) might be related to lead exposure. Tinfoil paper is a complex of tin and lead with a surface layer of metal-containing lead. According to local customs in East China, during funerals, people often fold or burn tinfoil paper at home, and lead on the surface layer releases polluting indoor air, which might result in lead exposure (44). Another study showed that tinfoil paper manufacture in family workshops seriously impacts the BLLs of operators and their family members (45). We also found that tin pots, a traditional vessel containing lead, may cause EBLL if children use them (46). Traditional Chinese medicine believes that the rational use of lead can treat various difficult and complicated diseases, but modern traditional Chinese medicine rarely uses it. Lead poisoning caused by lead containing drugs often comes from folk remedies. Lead tetroxide (chemical formula Pb3O4) is popular in some remote rural areas of southern China (47) for treating skin diseases, such as prickly heat and eczema; it is typically applied on children’s necks, armpits, and groin areas. A case report covered that a 3-year-old boy with BLL 303 μg/L and his 6-month-old sister with BLL 385 μg/L had used lead tetroxide instead of baby power (21). An investigation of approximately 222 children living in a Chinese rural area showed that lead-containing powder use is significantly associated with EBLL (47). Other folk remedies that are significantly correlated with higher BLL are also reported, such as folk remedies for treating epilepsy (48–50). Although the medicinal value of lead was recorded in the earliest Chinese pharmacological works, Shennong Classic of Materia Medica, for example, adding minerals such as lead to enhance the stability, sustainability, efficacy and storability of herbal medicines, modern Chinese medicine rarely used lead. Many studies revealed that the use of lead-containing herbs or lead-containing preparations mostly originated from folk remedies and long-term use of such lead-containing drugs may suffer from high risk of elevated blood lead levels or even lead poisoning (22, 45, 47, 51).
Furthermore, this study found that decentralized water supply was one of the risk factors for increased blood lead levels in children. In rural areas of China, decentralized water supply projects primarily utilized shallow well, mostly by household construction and management, and with the lack of water quality testing and monitoring. The findings show that the ground water with a non-central water supply was unsafe for lead exposure. Contamination of soil, water (groundwater and surface water), sediment, and air with hazardous and toxic compounds is one of the most severe and challenging problems that the industrialized world faces (52). A cross-sectional survey in Pakistan was conducted using water samples from drinking water sources. Of the 216 ground and surface water samples collected, 86% had lead levels higher than the World Health Organization’s maximum acceptable concentration of 10 ppb. The mean lead concentration in groundwater was 146 ppb, significantly higher than in surface water, with a lead concentration of 77.1 ppb (53).
Previous studies also found that elevated lead concentration in water often occurs due to corrosive water effects on pipeline materials, such as plumbing, coating, solder, pipes, pipe joints, and fittings (54). That might partially explain the result in this study that never/sometimes disusing first section of over night water might increase risk of EBLL.
This study also discussed children’s living environmental risk factors associated with EBLL. Lead pollution mainly comes from dust and sediment on the ground or suspended in the air. These are released by industrial metal smelting, mining enterprises, and related industrial and manufacturing industries, such as battery manufacturing, printing, mechanical manufacturing, and shipbuilding (18, 55). The results of a meta-analysis show that the corrected pooled lead poisoning rates of populations living around mining areas (70%) and industrial areas (57.5%) are much higher than those in urban areas (9.6%), suburban areas (23.6%), and rural areas (23.8%) (29). The total suspended lead particle counts in ambient air and lead concentrations are ten times higher than in the upper air above the ground where children breathe (40).
Our investigation suggested that the parents’ occupational exposure to lead is a risk factor for EBLL among children. Lead dust from parents’ surfaces and work clothing can be digested or inhaled by children at home (37). Parents may also carry the lead from the workplace to home in their clothing.
We find that living on the ground might increase the EBLL risk due to contacting dust, soil, or smoke. Lead in the air and the soil can enter the room of lower floors more easily than on higher floors, which leads to a higher rate of EBLL occurrence. A study tested that reducing 1,000 ppm or more lead in soil accessible to children would decrease at least 30 μg in BLLs. The results demonstrated that lead-contaminated soil or dust contributes to the lead burden in children (56).
We also verify that passive smoking as a risk factor is associated with EBLL, which is similar to the result of a previous study (37). Cigarettes contain heavy metals, such as cadmium and lead, and second-hand smoking exposure can increase the level of lead in children’s blood (26, 57, 58). It is estimated that 72% of non-smokers, including 180 million children under the age of 15, who live in China are exposed to second-hand smoke (59, 60).
This study also focuses on the impact of indoor air pollution from coal burning on children EBLL. During the coal combustion process, various atmospheric pollutants can be generated, including the heavy metal element lead, which is highly volatile. The result revealed the harmfulness of indoor cooking and heating fueled by coal or coal products. Therefore, coal which is commonly used as indoor fuel in northern China, is not recommended as a household fuel to avoid lead exposure.
Unlike previous research results, we did not find an increase in the prevalence of EBLL with a decrease in the distance between the residence and the main road. Local researches in China have found that after the implementation of unleaded gasoline, automobile exhaust is no longer the main source of atmospheric lead pollution. Lead pollution in road dust is mainly controlled by coal combustion emissions and non-ferrous metallurgical emissions (61, 62). Thus, the distance between the residence and the main road is not a risk factor of EBLL in China.
The strength of this study is its reporting prevalence of EBLL in Chinese children aged 0–6 years (from 1 month old to under 7 years old) in a large sample size and exploring risk factors for children lead exposure, especially in areas of traditional Chinese customs and the use of folk remedies. These issues have been rarely addressed in previous studies. Nonetheless, this study has some limitations. While adequate for assessing the BLLs of most Chinese children aged 0–6 years, the sample size may not be sufficient to reflect the extent of overall risk associated with lead exposure. Furthermore, this study did not directly measure the lead level of pollution sauces, such as the atmosphere, drinking water, soil, house dust, diet, and others in the children’s proximate environment. Moreover, as a cross-sectional study, the data reflect children’s lead exposure over the study period.
This study reveals the prevalence and risk factors for EBLL (BLL ≥ 50 μg/L) in 0–6-year-old children (from 1 month old to under 7 years old) in China. The pediatric population with high-risk factors should be given attention of lifestyle habits and living environment of lead exposure. This study also indicates that lead poisoning in children is preventable by removing high-risk factors and promoting protective factors. We hope this study will help public health education and inform policy for preventing and eradicating lead poisoning in China.
The data are available from the corresponding author on reasonable request.
The studies involving humans were approved by Ethics Committee of Xinhua Hospital affiliated with Shanghai Jiao Tong University School of Medicine (XHEC-C-2013-008). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
M-ML: Data curation, Formal analysis, Investigation, Methodology, Project administration, Validation, Writing – original draft, Writing – review & editing. X-TJ: Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Visualization, Writing – original draft, Writing – review & editing. JZ: Formal analysis, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. Z-YG: Data curation, Methodology, Project administration, Software, Supervision, Writing – review & editing. JC: Data curation, Methodology, Project administration, Supervision, Writing – review & editing. J-XL: Methodology, Supervision, Writing – review & editing. Y-LY: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – review & editing. C-HY: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – review & editing.
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by the National Basic Research Program of China (“973” Program, 2012CB525001), the National Natural Science Foundation of China (No. 81773411).
We thank the children and their parents for participating in this project, as well as all others who contributed to this study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declare that no Gen AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Warniment, C, Tsang, K, and Galazka, SS. Lead poisoning in children. Am Fam Physician. (2010) 81:751–7.
2. Aaron, HJ. Lead poisoning in children: a preventable disease[D] Antioch University (2024). https://aura.antioch.edu/etds/1047
4. Brewer, GJ, and Prasad, AS eds. Essential and toxic trace elements and vitamins in human health Academic Press (2020).
5. Hong, SB, Im, MH, Kim, JW, Park, EJ, Shin, MS, Kim, BN, et al. Environmental lead exposure and attention deficit/hyperactivity disorder symptom domains in a community sample of south Korean school-age children. Environ Health Perspect. (2015) 123:271–6. doi: 10.1289/ehp.1307420
6. Liu, J, Liu, X, Wang, W, McCauley, L, Pinto-Martin, J, Wang, Y, et al. Blood lead concentrations and children’s behavioral and emotional problems: a cohort study. JAMA Pediatr. (2014) 168:737–45. doi: 10.1001/jamapediatrics.2014.332
7. Taylor, MP, Forbes, MK, Opeskin, B, Parr, N, and Lanphear, BP. The relationship between atmospheric lead emissions and aggressive crime: an ecological study. Environ Health. (2016) 15:1–10. doi: 10.1186/s12940-016-0122-3
8. Weuve, J, Press, DZ, Grodstein, F, Wright, RO, Hu, H, and Weisskopf, MG. Cumulative exposure to lead and cognition in persons with Parkinson's disease. Mov Disord. (2013) 28:176–82. doi: 10.1002/mds.25247
9. Bihaqi, SW, Bahmani, A, Subaiea, GM, and Zawia, NH. Infantile exposure to lead and late-age cognitive decline: relevance to AD. Alzheimers Dement. (2014) 10:187–95. doi: 10.1016/j.jalz.2013.02.012
10. Kopp, SJ, Barron, JT, and Tow, JP. Cardiovascular actions of lead and relationship to hypertension: a review. Environ Health Perspect. (1988) 78:91–9. doi: 10.1289/ehp.887891
11. Campbell, JR, Rosier, RN, Novotny, L, and Puzas, JE. The association between environmental lead exposure and bone density in children. Environ Health Perspect. (2004) 112:1200–3. doi: 10.1289/ehp.6555
12. Hou, S, Yuan, L, Jin, P, Ding, B, Qin, N, Li, L, et al. A clinical study of the effects of lead poisoning on the intelligence and neurobehavioral abilities of children. Theor Biol Med Model. (2013) 10:1–9. doi: 10.1186/1742-4682-10-13
13. Wani, AL, Ara, A, and Usmani, JA. Lead toxicity: a review. Interdiscip Toxicol. (2015) 8:55–64. doi: 10.1515/intox-2015-0009
14. Caravanos, J, Carrelli, J, Dowling, R, Pavilonis, B, Ericson, B, and Fuller, R. Burden of disease resulting from lead exposure at toxic waste sites in Argentina, Mexico and Uruguay. Environ Health. (2016) 15:1–9. doi: 10.1186/s12940-016-0151-y
15. Lin, S, Wang, X, Yu, ITS, Tang, W, Miao, J, Li, J, et al. Environmental lead pollution and elevated blood lead levels among children in a rural area of China. Am J Public Health. (2011) 101:834–41. doi: 10.2105/AJPH.2010.193656
16. Jones, AL. Emerging aspects of assessing lead poisoning in childhood. Emerg Health Threats J. (2009) 2:7080. doi: 10.3402/ehtj.v2i0.7080
17. Cai, T, Luo, W, Ruan, D, Wu, YJ, Fox, DA, and Chen, J. The history, status, gaps, and future directions of neurotoxicology in China. Environ Health Perspect. (2016) 124:722–32. doi: 10.1289/ehp.1409566
18. Guo, P, Xu, X, Huang, B, Sun, D, Zhang, J, Chen, X, et al. Blood lead levels and associated factors among children in Guiyu of China: a population-based study. PLoS One. (2014) 9:e105470. doi: 10.1371/journal.pone.0105470
19. Nuwayhid, I, Nabulsi, M, Muwakkit, S, Kouzi, S, Salem, G, Mikati, M, et al. Blood lead concentrations in 1–3 year old Lebanese children: a cross-sectional study. Environ Health. (2003) 2:1–9. doi: 10.1186/1476-069X-2-5
20. Yan, C, Xu, J, and Shen, X. Childhood lead poisoning in China: challenges and opportunities. Environ Health Perspect. (2013) 121:A294–5. doi: 10.1289/ehp.1307558
21. Lin, G, Wu, F, Yan, C, Li, K, and Liu, XY. Childhood lead poisoning associated with traditional Chinese medicine: a case report and the subsequent lead source inquiry. Clin Chim Acta. (2012) 413:1156–9. doi: 10.1016/j.cca.2012.03.010
22. Ying, X, Xu, J, Markowitz, M, and Yan, CH. Pediatric lead poisoning from folk prescription for treating epilepsy. Clin Chim Acta. (2016) 461:130–4. doi: 10.1016/j.cca.2016.07.024
23. Cao, J, Li, M, Wang, Y, Yu, G, and Yan, C. Environmental lead exposure among preschool children in Shanghai, China: blood lead levels and risk factors. PLoS One. (2014) 9:e113297. doi: 10.1371/journal.pone.0113297
24. Hui-fen, LIN, Fu-yun, MA, Jin-bin, LUO, and Da, SHI. Lead hazard investigation of tin foil processing in family workshops. J Environ Occup Med. (2010) 27:754–5.
25. Brink, LA, Talbott, EO, Marsh, GM, Sharma, R, Benson, S, Wu, WC, et al. Revisiting nonresidential environmental exposures and childhood lead poisoning in the US: findings from Kansas, 2000–2005. J Environ Public Health. (2016) 2016:1–8. doi: 10.1155/2016/8791686
26. Li, Y, Qin, J, Wei, X, Li, C, Wang, J, Jiang, M, et al. The risk factors of child lead poisoning in China: a meta-analysis. Int J Environ Res Public Health. (2016) 13:296. doi: 10.3390/ijerph13030296
27. Ministry of Health of the People's Republic of China. Guidelines for the prevention of Hyperleademia and Lead poisoning in children. (2006). doi: 10.3969/j.issn.1671-878X.2006.04.001 (in Chinese).
28. Li, M, Cao, J, Xu, J, Cai, SZ, Shen, XM, and Yan, CH. The national trend of blood lead levels among Chinese children aged 0–18 years old, 1990–2012. Environ Int. (2014) 71:109–17. doi: 10.1016/j.envint.2014.06.005
29. Li, M, Cao, J, Gao, Z, Shen, XM, and Yan, CH. The trend of lead poisoning rate in Chinese population aged 0–18 years old: a meta-analysis. BMC Public Health. (2015) 15:1–12. doi: 10.1186/s12889-015-2103-9
30. Ruckart, PZ, Jones, RL, Courtney, JG, LeBlanc, TL, Jackson, W, Karwowski, MP, et al. Update of the blood Lead reference value – United States, 2021. MMWR. (2021) 70:1509–12. doi: 10.15585/mmwr.mm7043a4
31. Li, MM, Gao, ZY, Dong, CY, Wu, MQ, Yan, J, Cao, J, et al. Contemporary blood lead levels of children aged 0–84 months in China: a national cross-sectional study. Environ Int. (2020) 134:105288. doi: 10.1016/j.envint.2019.105288
32. CDC. National Notifiable Diseases Surveillance System (NNDSS), Lead, elevated blood lead level. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention (2023).
33. Council of State and Territorial Epidemiologists (CSTE). Public health reporting and national notification for elevated blood lead levels. Atlanta, GA: (2022). Available from: https://cdn.ymaws.com/www.cste.org/resource/resmgr/ps/ps2022/22-EH-01_lead_in_blood.pdf
34. Wang, Y, and Shen, N. Environmental regulation and environmental productivity: the case of China. Renew Sust Energ Rev. (2016) 62:758–66. doi: 10.1016/j.rser.2016.05.048
35. Qiu, J, Wang, K, Wu, X, Xiao, Z, Lu, X, Zhu, Y, et al. Blood lead levels in children aged 0–6 years old in Hunan Province, China from 2009–2013. PLoS One. (2015) 10:e0122710. doi: 10.1371/journal.pone.0122710
36. Lu, W, Zhen, LI, Huang, SX, Chuang, DU, Hong, WA, He, LP, et al. A systematic assessment of blood lead level in children and associated risk factors in China. Biomed Environ Sci. (2015) 28:616–9. doi: 10.3967/bes2015.086
37. Liu, J, Ai, Y, McCauley, L, Pinto-Martin, J, Yan, C, Shen, X, et al. Blood lead levels and associated sociodemographic factors among preschool children in the south eastern region of China. Paediatr Perinat Epidemiol. (2012) 26:61–9. doi: 10.1111/j.1365-3016.2011.01234.x
38. Hauptman, M, Bruccoleri, R, and Woolf, AD. An update on childhood lead poisoning. Clin Pediatr Emerg Med. (2017) 18:181–92. doi: 10.1016/j.cpem.2017.07.010
39. Ko, S, Schaefer, PD, Vicario, CM, and Binns, HJfor the Safer Yards Project. Relationships of video assessments of touching and mouthing behaviors during outdoor play in urban residential yards to parental perceptions of child behaviors and blood lead levels. J Expo Sci Environ Epidemiol. (2007) 17:47–57. doi: 10.1038/sj.jes.7500519
40. Xu, J, Sheng, L, Yan, Z, and Hong, L. Blood lead and cadmium levels in children: a study conducted in Changchun, Jilin Province, China. Paediatr Child Health. (2014) 19:73–6. doi: 10.1093/pch/19.2.73
41. Kennedy, C, Lordo, R, Sucosky, MS, Boehm, R, and Brown, MJ. Primary prevention of lead poisoning in children: a cross-sectional study to evaluate state specific lead-based paint risk reduction laws in preventing lead poisoning in children. Environ Health. (2014) 13:1–10. doi: 10.1186/1476-069X-13-93
42. Curtis, V, and Cairncross, S. Effect of washing hands with soap on diarrhoea risk in the community: a systematic review. Lancet Infect Dis. (2003) 3:275–81. doi: 10.1016/S1473-3099(03)00606-6
43. Luby, SP, Agboatwalla, M, Feikin, DR, Painter, J, Billhimer, W, Altaf, A, et al. Effect of handwashing on child health: a randomised controlled trial. Lancet. (2005) 366:225–33. doi: 10.1016/S0140-6736(05)66912-7
44. Wang, H, Han, XP, and Hu, WM. Investigation on current lead hazard status in a family tin-foil processing workshop. China Occup Med. (2008) 4:47.
45. Lin, CG, Schaider, LA, Brabander, DJ, and Woolf, AD. Pediatric lead exposure from imported Indian spices and cultural powders. Pediatrics. (2010) 125:e828–35. doi: 10.1542/peds.2009-1396
46. Cima, F. Tin: environmental pollution and health effects. Encycl Environ Health. (2011) 10:351–9. doi: 10.1016/B978-0-444-52272-6.00645-0
47. Lin, SH, Wang, XR, Yu, ITS, Tang, WNJ, Li, J, and Liu, BOY. Lead powder use for skin care and elevated blood lead level among children in a Chinese rural area. J Expo Sci Environ Epidemiol. (2012) 22:198–203. doi: 10.1038/jes.2011.46
48. Breeher, L, Mikulski, MA, Czeczok, T, Leinenkugel, K, and Fuortes, LJ. A cluster of lead poisoning among consumers of Ayurvedic medicine. Int J Occup Environ Health. (2015) 21:303–7. doi: 10.1179/2049396715Y.0000000009
49. Chui, SH, Wong, YH, Chio, HI, Fong, MY, Chiu, YM, Szeto, YT, et al. Study of heavy metal poisoning in frequent users of Chinese medicines in Hong Kong and Macau. Phytother Res. (2013) 27:859–63. doi: 10.1002/ptr.4816
50. Mitra, AK, Ahua, E, and Saha, PK. Prevalence of and risk factors for lead poisoning in young children in Bangladesh. J Health Popul Nutr. (2012) 30:404–9. doi: 10.3329/jhpn.v30i4.13292
51. Nagarajan, S, Sivaji, K, Krishnaswamy, S, Pemiah, B, Rajan, KS, Krishnan, UM, et al. Safety and toxicity issues associated with lead-based traditional herbo-metallic preparations. J Ethnopharmacol. (2014) 151:1–11. doi: 10.1016/j.jep.2013.10.037
52. Zouboulis, AI, Moussas, PA, and Nriagu, E. Groundwater and soil pollution: bioremediation. Encycl Environ Health. (2011). doi: 10.1016/B978-0-444-52272-6.00035-0
53. Ul Haq, N, Arain, MA, Badar, N, Rasheed, M, and Haque, Z. Drinking water: a major source of lead exposure in Karachi, Pakistan. East Mediterr Health J. (2011) 17:882–6. doi: 10.26719/2011.17.11.882
54. Pfadenhauer, LM, Burns, J, Rohwer, A, and Rehfuess, EA. A protocol for a systematic review of the effectiveness of interventions to reduce exposure to lead through consumer products and drinking water. Syst Rev. (2014) 3:1–13. doi: 10.1186/2046-4053-3-36
55. Lanphear, BP, Lowry, JA, Ahdoot, S, Baum, CR, Bernstein, AS, Bole, A, et al. Prevention of childhood lead toxicity. Pediatrics. (2016) 138:e20161493. doi: 10.1542/peds.2016-1493
56. Weitzman, M, Aschengrau, A, Bellinger, D, Jones, R, Hamlin, JS, and Beiser, A. Lead-contaminated soil abatement and urban children's blood lead levels. JAMA. (1993) 269:1647–54. doi: 10.1001/jama.1993.03500130061033
57. Friedman, LS, Lukyanova, OM, Kundiev, YI, Shkiryak-Nizhnyk, ZA, Chislovska, NV, Mucha, A, et al. Predictors of elevated blood lead levels among 3-year-old Ukrainian children: a nested case-control study. Environ Res. (2005) 99:235–42. doi: 10.1016/j.envres.2004.12.006
58. Apostolou, A, Garcia-Esquinas, E, Fadrowski, JJ, McLain, RN, P, Weaver, VM, and Navas-Acien, A. Secondhand tobacco smoke: a source of lead exposure in US children and adolescents. Am J Public Health. (2012) 102:714–22. doi: 10.2105/AJPH.2011.300161
59. Liu, Y, and Chen, L. New medical data and leadership on tobacco control in China. Lancet. (2011) 377:1218–20. doi: 10.1016/S0140-6736(10)61391-8
60. Hsia, J, Yang, GH, Li, Q, Xiao, L, Yang, Y, Wu, YW, et al. Methodology of the global adult tobacco survey in China, 2010. Biomed Environ Sci. (2010) 23:445–50. doi: 10.1016/S0895-3988(11)60005-6
61. Mukai, H, Tanaka, A, Fujii, T, Zeng, Y, Hong, Y, Tang, J, et al. Regional characteristics of sulfur and lead isotope ratios in the atmosphere at several Chinese urban sites. Environ Sci Technol. (2001) 35:1064–71. doi: 10.1021/es001399u
62. Chen, J, Tan, M, Li, Y, Zhang, Y, Lu, W, Tong, Y, et al. A lead isotope record of Shanghai atmospheric lead emissions in total suspended particles during the period of phasing out of leaded gasoline. Atmos Environ. (2005) 39:1245–53. doi: 10.1016/j.atmosenv.2004.10.041
63. Economic Development Committee of Small and Medium-sized Cities of China Urban Economics Association, The Compilation Committee on the Report on the Development of Small and Medium-sized Cities in China. Annual report on development of small and medium-sized cities in China. (2010), [M]. Beijing: Social Sciences Academic Press. (in Chinese).
Keywords: children, elevated blood lead levels, prevalence, risk factors, China
Citation: Li M-M, Jiao X-T, Zhang J, Gao Z-Y, Cao J, Liu J-X, Yang Y-L and Yan C-H (2025) Prevalence and risk factors of elevated blood lead levels in 0-6-year-old children: a national cross-sectional study in China. Front. Public Health. 13:1546842. doi: 10.3389/fpubh.2025.1546842
Edited by:
Xin Long, Chongqing Institute of Green and Intelligent Technology (CAS), ChinaReviewed by:
Niti B. Jadeja, University of Virginia, United StatesCopyright © 2025 Li, Jiao, Zhang, Gao, Cao, Liu, Yang and Yan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yu-Lin Yang, eWFuZ3l1bGluQHNobWNoYy5jbg==; Chong-Huai Yan, eWFuY2hvbmdodWFpQHhpbmh1YW1lZC5jb20uY24=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.