 Wen-yuan Wang
Wen-yuan Wang Tao Zhang
Tao Zhang
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 28 March 2025
Sec. Health Economics
Volume 13 - 2025 | https://doi.org/10.3389/fpubh.2025.1546542
Objectives: Tracheobronchial foreign body aspiration (TFBA) constitutes a life-threatening pediatric emergency with substantial clinical and public health implications. While current research prioritizes diagnostic and therapeutic strategies for TFBA, limited attention has been paid to its socioeconomic consequences. This study focuses on Gansu Province, a representative underdeveloped region in China, to systematically assess both direct medical costs (surgical interventions and hospitalization) and broader socioeconomic impacts of pediatric TFBA management. The findings aim to inform evidence-based healthcare policies for childhood emergencies in resource-limited settings.
Methods: Using Gansu Provincial statistical data, we analyzed the economic burden of 951 pediatric tracheobronchial foreign body cases (2017–2021) meeting inclusion criteria at a provincial tertiary hospital’s respiratory department.
Results: (1) Urban–rural disparities in economic burden: The average annual total income of rural households was significantly lower than that of urban households (p < 0.01). The proportion of hospitalization costs relative to income in rural areas reached 36.31 ± 4.43%, 3.1 times that of urban households (11.91 ± 2.14%, p < 0.001). Rural minority-concentrated regions bore the heaviest burden (48.06%), while urban Han-majority regions had the lowest burden (9.29%). No significant urban–rural difference in surgical costs (P>0.05). (2) Regional heterogeneity in economic burden: Hospitalization costs in underdeveloped minority-concentrated rural areas reached 13,323¥ (8% higher than the rural average), yet their income (27,678¥) was 33% below the average. Their cost-to-income ratio (48.06%) was 3.2 times that of their urban counterparts (15.21%). In developed Han-majority regions, despite comparable hospitalization costs (11,872 ¥ vs. 12,339 ¥), the higher income (42% above average) resulted in the lowest cost-to-income ratio (21.52%).
Conclusion: TFBA poses a critical global health challenge with disproportionate impacts on children aged 1–3 years and significant economic burden on families, especially in underdeveloped minority-concentrated rural areas. This study highlights severe urban–rural disparities in economic burdens.
Tracheobronchial foreign body aspiration (TFBA) remains a significant pediatric emergency and global public health issue, particularly in children under 3 years old. It is associated with high morbidity, preventable mortality, and substantial economic burdens, primarily due to delayed diagnosis and complications such as airway obstruction or recurrent infections (1, 2). Previous research has shown that TFBA accounts for 7.9–18.1% of accidental injuries in children aged 0–14 years in China and 80% in children aged 1–3 years (3). TFBA are the third most common cause of death due to unintentional injury in children aged <1 year in the USA, where they have been reported to occur in 0.43 per 100,000 children aged <5 years (4). In recent years, the global incidence rate has not changed significantly. When compared to 1990, global incidence of TFBA in children under 5 years old decreased in 2019, but an increasing trend in the incidence rate of TFBA was observed from 2014 to 2019 (5). The diagnosis and differential diagnosis of TFBA remain clinically challenging due to non-specific or overlapping symptoms. A subset of cases is initially misdiagnosed as chronic pulmonary infections or wheezing disorders, causing patients to undergo multiple ineffective treatments and delayed interventions. In severe cases, complications such as airway necrosis or abscess formation may necessitate invasive procedures (e.g., thoracotomy), further exacerbating the risks of missed or incorrect diagnoses (6). These diagnostic pitfalls not only compromise clinical outcomes but also impose significant socioeconomic burdens on families and healthcare systems.
Current research on pediatric TFBA predominantly emphasizes diagnostic and therapeutic advancements, with scant attention paid to its socioeconomic burden, including healthcare expenditures and systemic costs. To address this gap, this study focuses on Gansu Province, a region with notable socioeconomic disparities, and retrospectively analyzes clinical data from children with TFBA treated at our institution over the past 5 \years. By quantifying direct medical costs (e.g., surgical and hospitalization expenses) and evaluating the financial strain on affected families, this investigation aims to delineate the broader economic impact of TFBA. These findings will serve as an evidence-based foundation for formulating targeted prevention strategies and optimizing public health resource allocation.
This study received ethical approval from the Institutional Review Board of our hospital. We retrospectively analyzed 951 pediatric patients with TFBA admitted to our center in Gansu Province between January 2017 and December 2021, adhering to established diagnostic criteria for foreign body aspiration. The cohort comprised 638 males (67.09%) and 313 females (32.91%), demonstrating male predominance (ratio 2.04:1). Geographic distribution revealed 664 rural cases (69.82%) versus 287 urban cases (30.18%), with a rural/urban ratio of 2.31:1. Exclusion criteria comprised endogenous airway foreign bodies, respiratory tract malformations, and comorbidities including cerebral palsy, congenital heart disease, or genetic metabolic disorders.
The economic burden of disease, a comprehensive metric introduced by the World Bank and the World Health Organization (WHO) in 1993, quantifies the health and socioeconomic impact of diseases through epidemiological and economic dimensions. The burden of disease (BOD) refers to the loss and impact on population health and social economy caused by a disease, disability, and premature death, including the epidemiological burden and economic burden of the disease (7, 8). The economic burden of disease comprises three components: direct costs (medical and non-medical expenditures during treatment), indirect costs (productivity losses due to illness), and intangible costs (non-monetizable psychosocial impacts). Direct costs encompass hospitalization fees, surgical expenses, and ancillary costs (e.g., transportation and accommodation for caregivers). Indirect costs primarily reflect productivity losses among caregivers, particularly in pediatric cases requiring prolonged family care. Intangible costs include psychological distress (e.g., caregiver anxiety) and reduced quality of life, which are challenging to quantify (9, 10).
In this study, we focus exclusively on direct medical costs (hospitalization and surgery expenses) for tracheobronchial foreign body (TFBA) management, excluding indirect expenditures (e.g., lost wages) and intangible burdens. Economic data were derived from the Gansu Statistical Yearbook (2017–2021) (11), including urban and rural household income statistics across the province to contextualize the financial impact relative to regional socioeconomic profiles.
IBM SPSS Statistics 22 was used for data processing. Data were analyzed using IBM SPSS Statistics 22. Categorical variables were described as frequencies and percentages (%), with intergroup comparisons by χ2-test. Continuous variables were expressed as mean ± standard deviation (SD). Normality was assessed via the Kolmogorov–Smirnov test. For data conforming to a normal distribution, the t-test was used for comparison between two groups, and ANOVA was used for comparison among multiple groups. For data not conforming to a normal distribution, non-parametric tests were used. p < 0.05 was considered statistically significant, and p-value <0.01 as highly significant.
Gansu Province administers 14 prefecture-level divisions (12 cities and 2 autonomous prefectures) with 87 county-level administrative units. This study encompassed 951 pediatric TFBA cases from 72 counties across all municipal and autonomous prefectural jurisdictions, covering 82.76% of the province’s county-level administrative units.
Over the past 5 years (2017–2021), rural households in Gansu Province demonstrated a progressive increase in mean annual total income (33,603¥), while maintaining stable medical expenditure patterns: Surgical costs averaged 7,778¥, representing 23.02% of household income, with interannual variation peaking at 28.66% in 2018, dipping to 18.90% in 2021. Hospitalization costs averaged 12,244¥, representing 36.31% of household income, showing notable annual fluctuations ranging from 42.94% (2018) to 30.81% (2021). Detailed data are presented in Table 1.

Table 1. Urban–rural disparities in economic burden (¥).
Urban households in Gansu Province experienced a steady rise in mean annual total income (95,043¥, 2017–2021), with surgical and hospitalization costs maintaining relative stability. Surgical costs averaged 7,688¥, accounting for 8.18% of household income, peaking at 11.16% in 2018 and declining to 6.63% in 2021. Hospitalization costs averaged 11,176¥ (11.91% of household income), ranging from 15.38% in 2018 to 10.04% in 2021. Detailed data are presented in Table 1.
Comparative analysis revealed statistically significant disparities between urban and rural households. The mean annual total income of urban families consistently exceeded that of rural counterparts across all study years (p < 0.01). While no significant intergroup difference was observed in surgical costs (P>0.05), rural areas demonstrated substantially higher hospitalization expenditures (p < 0.05). Notably, rural households bore disproportionately greater financial burdens, as evidenced by significantly elevated hospitalization-to-income ratios compared to urban populations (p < 0.05).
To investigate the regional heterogeneity of economic burden associated with pediatric TFBA, this study implemented a multidimensional classification framework for Gansu Province’s 14 prefecture-level divisions. The categorization criteria integrated three key regional characteristics: economic development gradients (stratified by per capita GDP rankings), ethnic distribution patterns (measured through minority population concentration indices), industrial structural profiles (classified by dominant economic sectors). Four distinct regional typologies were subsequently identified, enabling systematic analysis of healthcare expenditure patterns. The economic burden of different regions in rural and urban areas was analyzed, with the results as shown in Table 2. Hospitalization costs and total family income are the average values from 2017 to 2021, all economic metrics were derived from the Gansu Statistical Yearbook (2017–2021 edition).
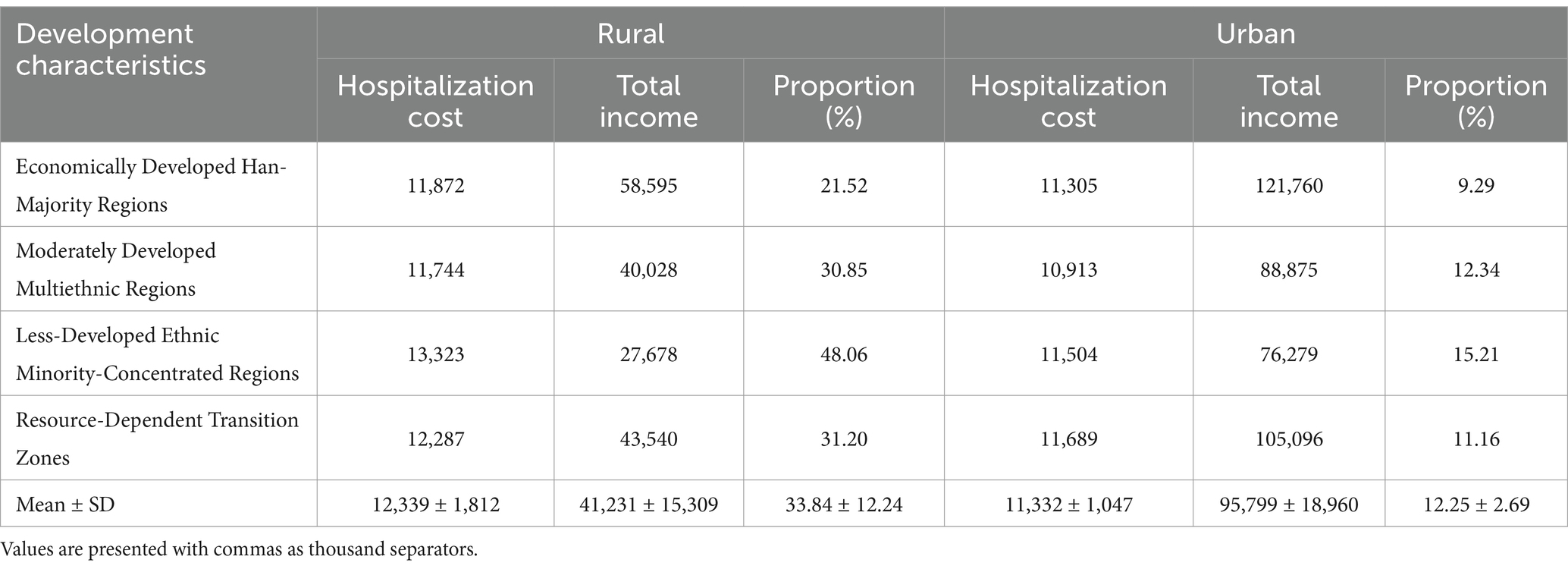
Table 2. Economic burden in different regions.
Significant disparities in hospitalization cost-to-income ratios were observed across rural regions, ranging from 21.52% in Economically Developed Han-Majority Regions to 48.06% in Less-Developed Ethnic Minority-Concentrated Regions. Less-Developed Ethnic Minority-Concentrated Regions exhibited the most severe financial burden, with hospitalization costs averaging 13,323¥ (8% higher than the provincial rural mean), despite household incomes (27,678¥) 33% below the rural average. Economically Developed Han-Majority Regions demonstrated optimal economic resilience, combining the lowest cost ratio (21.52%) with incomes (58,595¥) 42% above rural averages, despite comparable hospitalization costs (11,872¥ vs. 12,339¥). Resource-Dependent Transition Zones showed intermediate burdens (31.20%), while Moderately Developed Multiethnic Regions reached 30.85%, exceeding urban counterparts by 2.4-fold (12.25 ± 2.69%). Full metrics are systematically compared in Table 2.
The urban economic burden analysis revealed hospitalization cost-to-income ratios ranging from 9.29% in Economically Developed Han-Majority Regions to 15.21% in Less-Developed Ethnic Minority-Concentrated Regions. Key urban–rural disparities included: Income Inequality: Urban households demonstrated 2.3-fold higher incomes than rural counterparts (95,799 ± 18,960¥ vs. 41,231 ± 15,309¥; p < 0.001). Cost Burden Gradient: Rural hospitalization costs consumed 33.84 ± 12.24% of household income – 2.8-fold higher than urban averages (12.25 ± 2.69%; p < 0.001). Less-Developed Ethnic Minority-Concentrated Regions: Despite lower absolute costs (11,504¥ vs. rural 13,323¥), Less-Developed Ethnic Minority-Concentrated Regions exhibited the highest urban burden (15.21%) due to depressed incomes (76,279¥ vs. urban mean 95,799¥). Detailed metrics are stratified by region in Table 2.
Unlike ordinary respiratory infections, pediatric TFBA cases require mandatory surgical intervention, incurring substantially higher hospitalization expenses. Diagnostic delays and misdiagnoses, particularly when resulting in extended foreign body retention due to missed identification or delayed clinical intervention, exacerbate clinical complexity, leading to escalated therapeutic costs and disproportionate family financial strain (12). This study systematically evaluates the economic burden of clinically confirmed TFBA cases. While healthcare-related economic burdens manifest multidimensionally, our analysis focuses on quantifiable direct medical costs: surgical expenditures and hospitalization fees. Given that surgical costs constitute the predominant financial component in foreign body management, these are subjected to dedicated stratified analysis.
Our study reveals significant disparities in the economic burden of pediatric TFBA between urban and rural areas in Gansu Province, reflecting broader socioeconomic inequities. Rural households face disproportionate financial strain, with an average annual total income (33,603¥) representing only 35.3% of urban households’ income (95,043¥), while rural hospitalization costs consume 36.31% of total family income—3.1 times the urban rate (11.91%, p < 0.001). Surgical costs account for nearly a quarter (23.02%) of rural household income, compared to <10% in urban areas. This disparity stems from three compounding factors, income disparity: A 2.8-fold urban–rural income gap (urban 95,043¥ vs. rural 33,603¥); Healthcare cost differentials: rural hospitalization costs exceed urban levels by 9.6% (12,244¥ vs. 11,176¥). Cumulative effects of diagnostic delays: rural cases exhibit wider annual fluctuations in hospitalization cost-to-income ratios (30.81–42.94% vs. urban 10.04–15.38%), likely due to delayed referrals and higher complication rates prolonging hospital stays (13, 14). The inverse relationship between regional economic development and healthcare affordability highlights systemic vulnerabilities in rural healthcare systems. Lower incomes exacerbate these disparities: despite earning 2.8 times less, rural households shoulder significantly higher hospitalization and surgical expenditures (p < 0.05). Diagnostic delays and limited access to timely interventions likely amplify clinical complexity, driving cost escalation in underserved areas (15).
Regional analysis based on a multidimensional classification framework (economic development, ethnic distribution, and industrial structure) reveals that underdeveloped ethnic minority-concentrated regions endure a dual burden of “low income-high expenditure”: Rural hospitalization costs (¥13,323) exceed the provincial rural average by 8%, while household income (¥27,678) falls 33% below the mean, yielding a cost-to-income ratio of 48.06%—3.2 times higher than urban counterparts. In contrast, economically developed Han-majority regions demonstrate economic resilience: despite comparable hospitalization costs (¥11,872 vs. provincial average ¥12,339), their household income (¥58,595, 42% above rural averages) reduces the cost-to-income ratio to 21.52%.
This “burden inversion” phenomenon stems from cultural-cognitive disparities, healthcare resource mismatches, environmental exposures. Cultural-cognitive disparities: the interplay between economic development and cultural-cognitive factors critically shapes health outcomes. In economically underdeveloped ethnic minority regions, limited health literacy and entrenched traditional medical practices hinder timely recognition and management of foreign body aspiration (FBA) (16). Healthcare resource mismatches: Medical staff in primary hospitals have limited ability to identify foreign bodies, high misdiagnosis rate at first diagnosis, and low bronchoscope allocation rate, which leads to multiple levels of referral to specialized hospitals and delays in treatment time. Environmental exposures: Geographical disparities further amplify risks, rural agricultural communities exhibit higher exposure to plant-based foreign bodies (e.g., sunflower seeds, peanuts), particularly during harvest seasons when children lack adequate supervision, parental risk awareness remains suboptimal (17). Globally, children in low-and middle-income countries face amplified TFBA risks due to overlapping vulnerabilities: socioeconomic deprivation, limited healthcare access, and insufficient risk awareness. These systemic inequities transform a preventable condition into a cascade of medical and financial crises, demanding culturally tailored prevention strategies and resource redistribution (18).
TFBA imposes catastrophic health expenditures across both urban and rural households, with hospitalization costs consuming a substantial proportion of family income—particularly in socioeconomically disadvantaged minority-concentrated regions. To address this inequity, a multi-tiered intervention strategy is imperative: (1) Targeted Medical Subsidy Mechanisms, the concentration of high hospital costs in low-income areas highlights a vicious cycle in which poverty increases health spending and further exacerbates economic disadvantage, and targeted health subsidies are recommended. (2) Strengthening Primary Care Diagnostic Capacity, portable bronchoscopes were provided in county-level hospitals to strengthen the ability of grassroots children’s respiratory doctors to identify, diagnose and deal with children’s TFBA in emergencies. (3) Building a health education system: Foreign body prevention is more important than treatment, and primary health care training and public awareness campaigns should be strengthened (18).
This study has several limitations that warrant consideration. First, although our institution pioneered bronchoscopic interventions in the province and manages the majority of TFBA cases, recent advancements in endoscopic techniques have enabled municipal hospitals to initiate similar services. Consequently, our single-center data may not fully represent provincial epidemiological patterns, further multi-center, large-sample studies are needed. Second, the economic analysis focused solely on direct medical costs, excluding indirect expenditures such as caregiver lost wages, transportation, and accommodation expenses. Therefore, the overall economic burden caused by TFBA is more than this. Third, our use of regional average household incomes rather than individual family-level data may obscure socioeconomic heterogeneity, making the assessment of family economic burden not objective enough. In addition, it is difficult to obtain the intangible costs caused by the spiritual burden of grief, anxiety, and inconvenience of children and their caregivers in actual research, and these indirect economic losses may have a significant impact on the total costs, which need to be further investigated in future research.
TFBA remains a critical yet preventable global pediatric health challenge, disproportionately affecting children aged 1–3 years. As a time-sensitive iatrogenic crisis, TFBA causes acute respiratory compromise and chronic complications including obstructive pneumonia atelectasis, mortality in delayed diagnoses, and a heavier financial burden. This study systematically reveals the urban–rural disparities and regional heterogeneity in the economic burden of TFBA among children in Gansu Province, highlighting the structural incongruities between healthcare resource allocation and imbalanced socioeconomic development in China’s underdeveloped regions. Our findings reinforce three essential pillars for TFBA management, first, early intervention imperative—intervention within 24 h significantly reduces both complication risks and treatment costs. Second, socioeconomic equity focus—rural minority communities exhibit catastrophic health expenditure rates than urban counterparts, necessitating targeted medical subsidy programs. Third and foremost, prevention as cost-effective strategy, majority of cases can be prevented through measures such as caregiver education and toy safety regulations. In essence, preemptive public health measures outweigh reactive clinical management in averting this avoidable childhood trauma.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
This project was approved by the Medical Ethics Committee of our hospital. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin. Written informed consent was obtained from the individual(s), and minor(s)’ legal guardian/next of kin, for the publication of any potentially identifiable images or data included in this article.
W-yW: Conceptualization, Data curation, Funding acquisition, Methodology, Writing – original draft, Writing – review & editing. TZ: Investigation, Methodology, Writing – original draft. W-YL: Data curation, Formal analysis, Validation, Writing – review & editing. S-YW: Formal analysis, Software, Validation, Writing – original draft. Q-JZ: Conceptualization, Investigation, Methodology, Writing – original draft. Y-JW: Writing – review & editing.
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by the Gansu Provincial Joint Research Fund General Project (24JRRA936).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declare that no Gen AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Brkic, F, Umihanic, S, Altumbabic, H, Ramas, A, Salkic, A, Umihanic, S, et al. Death as a consequence of foreign body aspiration in children. Med Arch. (2018) 72:220–3. doi: 10.5455/medarh.2018.72.220-223
2. Lluna, J, Olabarri, M, Domènech, A, Rubio, B, Yagüe, F, Benítez, MT, et al. Recommendations for the prevention of foreign body aspiration. An Pediatr (Barc). (2017) 86:50.e1–6. doi: 10.1016/j.anpedi.2016.04.013
3. Subspecialty Group of Pediatrics Society of Otorhinolaryngology Head and Neck Surgery Chinese Medical Association. Experts consensus on diagnosis and treatment of tracheobronchial foreign bodies in children. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. (2018) 53:325–38. doi: 10.3760/cma.j.issn.1673-0860.2018.05.002
4. Moola, A, Verwey, C, Mabaso, T, Mopeli, K, Withers, A, Loveland, J, et al. Tracheobronchial foreign body aspiration in children in Soweto, South Africa: a retrospective descriptive study. Afr J Thorac Crit Care Med. (2024) 30:e1145. doi: 10.7196/AJTCCM.2024.v30i2.1145
5. Wu, Y, Zhang, X, Lin, Z, Ding, C, Wu, Y, Chen, Y, et al. Changes in the global burden of foreign body aspiration among under-5 children from 1990 to 2019. Front Pediatr. (2023) 11:1235308. doi: 10.3389/fped.2023.1235308
6. China Maternal and Child Health Association Minimally invasive Branch children interventional respiratory disease committee, Bronchoscopy collaboration Group, Respiratory Group, Pediatric Branch, Chinese Medical Association. National Health Commission Talent Exchange Service Center Pediatric Respiratory Endoscopy Technology Project Expert Group, Chinese Medical Doctor Association Pediatric Physician Branch Endoscopy Professional Committee, Chinese Medical Doctor Association Endoscopy Physician Branch Pediatric Respiratory Endoscopy Professional Committee, et al. Expert consensus on pediatric airway foreign body respiratory intervention diagnosis and treatment in China. Chin J Pract Pediatr. (2018) 33:1392–402. doi: 10.3760/cma.j.issn.2095-428X.2018.18.008
7. Hu, SL. Study on disease burden (part 1)[J]. Health Econ Res. (2005) 5:22–7. doi: 10.3969/j.issn.1004-7778.2005.05.011
8. Pengwei, C, Na, L, and Zhaojun, D. Research Progress on economic burden of disease. Chin J Prevent Med. (2016) 17:612–6. doi: 10.16506/j.1009-6639.2016.08.012
9. Jo, C. Cost-of-illness studies: concepts, scopes, and methods. Clin Mol Hepatol. (2014) 20:327–37. doi: 10.3350/cmh.2014.20.4.327
10. Rochmah, TN, Rahmawati, IT, Dahlui, M, Budiarto, W, and Bilqis, N. Economic burden of stroke disease: a systematic review. Int J Environ Res Public Health. (2021) 18:7552. doi: 10.3390/ijerph18147552
11. Gansu Provincial Bureau of Statistics. Gansu Statistical Yearbook [EB/OL]. Available online at: http://tjj.gansu.gov.cn/tjj/c109464/info_disp.shtml.
12. Foltran, F, Ballali, S, Rodriguez, H, (Sebastian) van As, AB, Passali, D, Gulati, A, et al. Inhaled foreign bodies in children: a global perspective on their epidemiological, clinical, and preventive aspects. Pediatr Pulmonol. (2013) 48:344–51. doi: 10.1002/ppul.22701
13. Yu, Z, Hongchen, D, Guitao, L, Guoshun, M, Xiaying, C, Ying, Z, et al. Analysis of clinical correlated factors in delayed diagnosis of pediatric tracheobronchial foreign bodies. J Clin Pulmonary Med. (2022) 27:1692–169, 1701. doi: 10.3969/j.issn.1009-6663.2022.11.013
14. Liu, B, Ding, F, An, Y, Li, Y, Pan, Z, Wang, G, et al. Occult foreign body aspirations in pediatric patients: 20-years of experience. BMC Pulm Med. (2020) 20:320. doi: 10.1186/s12890-020-01356-8
15. Kaushal, D, Goyal, A, Soni, K, Choudhury, B, Nair, NP, Kumar, P, et al. Challenges in management of tracheobronchial foreign bodies with delayed presentation: an institutional experience. Int Arch Otorhinolaryngol. (2022) 26:e005–9. doi: 10.1055/s-0040-1718964
16. Gan, W, Xiao, N, Feng, Y, Zhou, D, Hu, J, Liu, S, et al. Clinical analysis of tracheobronchial foreign body aspiration in children: a focus on external and intrinsic factors. BMC Surg. (2021) 21:108. doi: 10.1186/s12893-021-01089-3
17. Ding, L, Su, S, Chen, C, Yao, H, and Xiao, L. Tracheobronchial foreign bodies in children: experience from 1,328 patients in China. Front Pediatr. (2022) 10:873182. doi: 10.3389/fped.2022.873182
Keywords: economic burden, children, tracheobronchial foreign body, foreign body inhalation, urban–rural difference
Citation: Wang W-y, Zhang T, Li W-Y, Wang S-Y, Zhao Q-J and Wang Y-J (2025) Economic burden analysis of pediatric tracheobronchial foreign body. Front. Public Health. 13:1546542. doi: 10.3389/fpubh.2025.1546542
Edited by:
Michael Ekubu Otim, Dubai Medical University, United Arab EmiratesReviewed by:
Burak Tander, Acıbadem University, TürkiyeCopyright © 2025 Wang, Zhang, Li, Wang, Zhao and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yong-Jun Wang, OTM5ODI2NjM2QHFxLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.