
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Public Health , 19 March 2025
Sec. Disaster and Emergency Medicine
Volume 13 - 2025 | https://doi.org/10.3389/fpubh.2025.1543150
 Hannah Richter1Marlieke Schneider2†Johanna Eisenberger2Nastaran Jafari1Hannah Haumann3†
Hannah Richter1Marlieke Schneider2†Johanna Eisenberger2Nastaran Jafari1Hannah Haumann3† David Häske1*†
David Häske1*†Background: The COVID-19 pandemic has had an unprecedented impact on healthcare systems worldwide. Emergency medical services (EMS) frequently served as the sole point of contact for individuals in need of assistance or emergency support. This study aimed to map the impact of the pandemic on emergency calls and EMS operations.
Methods: A systematic literature search was conducted in the electronic databases Pubmed and Web of Science. A hand search supplemented the search. Published articles in English or German dealing with frequencies, diagnoses, and factors influencing emergency calls and EMS use were included. Studies on cardio-pulmonary resuscitation were not included.
Results: The initial search yielded 3,359 articles, of which 3,187 were screened by title/abstracts, and 120 full-text articles were analyzed. Fifty articles were then included. Fourteen articles reported the number of emergency calls, 30 on the number of EMS operations, and six on both outcomes. The articles were mostly published in 2020 (n = 18) or 2021 (n = 29) and dealt with the situation of EMS during the COVID-19 pandemic in 13 European countries and 11 non-European countries. However, the quantitative data on changes in emergency calls show considerable variation (standard deviation of 31.3% with a mean of 0.0%, minimum: −50.0% to maximum: 121.0%). The quantitative data on changes in EMS operations show a more significant overall decrease (mean: −12.2%, standard deviation: 24.7%, minimum: −72% to maximum: 56%).
Conclusions: The heterogeneity of the studies is considerable; overall, there appears to have been a decline in emergency calls, particularly EMS operations. Clear patterns, e.g., by region, cannot be identified.
Review protocol registration: The review protocol is registered in the Open Science Framework: https://osf.io/8urq9.
The novel coronavirus SARS-CoV-2 (COVID-19) detected at the end of 2019 has had extreme consequences worldwide. On March 11 2020, the World Health Organization declared COVID-19 a global pandemic (1). In many countries, public life was severely restricted after that. Public events were canceled, schools and universities were closed, and “Stay-at-Home Restrictions” and “lockdowns” were implemented (2–4). Where possible, employees were sent to home office to reduce infection rates in workplaces (3).
To date, numerous studies have examined the Impact of COVID-19 on a variety of areas, such as the education system (5, 6), the economy (7, 8), and the healthcare system (9, 10). The COVID-19 pandemic tested healthcare systems worldwide and significantly impacted the functionality and utilization of healthcare and emergency medical services (EMS) (1). Studies almost universally reported declining healthcare utilization for diseases other than COVID-19, and it is noteworthy that this trend was observed for both routine and emergency services (10). Many countries experienced a decrease in patient contacts, but also the planned suspension of elective procedures and a consecutive redistribution of clinical staff to relieve colleagues in intensive care units and COVID-19-associated patient care, which led to a disruption in care (1).
Prehospital emergency medical services (EMS) deserve special attention in the healthcare sector. These EMS providers treat and transport patients for various indications, usually without prior knowledge of the patients. Numerous country-specific studies have documented this phenomenon by examining the impact of the coronavirus disease 2019 (COVID-19) pandemic EMS. However, to the best of our knowledge, no comprehensive overview exists. This review will analyze the impact of the pandemic on the number of emergency calls and EMS operations, and specific diagnoses will break both down.
Given the considerable heterogeneity of the expected publications, we conducted a scoping review on the frequency of EMS calls and EMS operations during the COVID-19 pandemic. This work adheres to the methodological framework of Arksey and O'Malley and the PRISMA Statement Extension for Scoping Reviews (PRISMA-ScR) (11, 12). The study protocol is registered in the Open Science Framework: https://osf.io/8urq9.
The present study has included published articles in English or German examining the frequency, type of diagnoses, and factors influencing ambulance operations and emergency calls (Table 1). These influencing factors may include demographic characteristics (e.g., age, gender, socioeconomic status), temporal patterns (e.g., seasonal or diurnal variations), geographic influences (e.g., countries, continents), and system-level variables, among others.
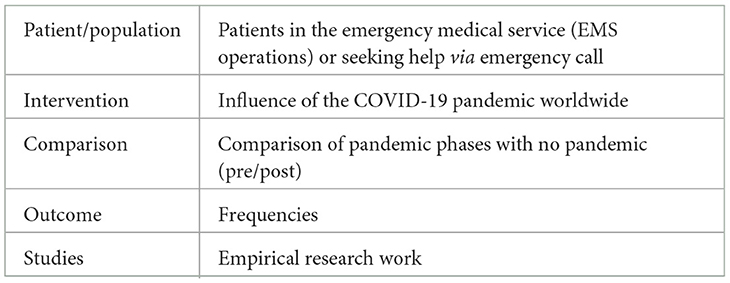
Table 1. PICOS-Schema.
Studies focusing primarily on cardiopulmonary resuscitation (CPR) were excluded from consideration due to their unique clinical and operational considerations, which are the focus of a separate review. The inclusion criteria were chosen to ensure a comprehensive understanding of the broader landscape of EMS interventions and emergency call dynamics. Analyzing the frequency and type of EMS calls and the factors that influence these events aims to identify patterns and potential areas for system improvement. The exclusion of studies dealing with CPR is justified by their highly specialized nature, which often involves different research methods, patient populations, and outcome measures than general EMS interventions.
We conducted a systematic literature search in the electronic databases Pubmed and Web of Science using the following search terms and filters: (“Emergency Medical Services” [Mesh] AND “SARS-CoV-2” [Mesh]) OR (“Emergency Medical Services” [Mesh] AND “COVID-19” [Mesh]) and (“EMS” OR “Emergency Medical Service” OR “ambulance” OR “Prehospital”) AND (“COVID-19” OR “SARS-CoV-2”). A hand search supplemented the search. The searches took place between June and December 2021. The date of the most recent search was September 16, 2021.
The literature search resulted in a total of 3,359 articles. After removing duplicates, 3,187 articles were screened by titles and abstracts. Based on title and abstract, 3,067 were excluded, and 120 full-text articles were retrieved and assessed for eligibility. The full-text screening resulted in the exclusion of 70 studies for the following reasons: 46 reported other outcomes (e.g., out-of-hospital cardiac arrest), relevant information was missing in 10 studies, 6 were duplicates that were not identified in advance because they were published in different languages, 2 reported the impact of the COVID-19 pandemic on another setting like hospitals. There was no full-text for two articles; one was published in another language. Finally, 50 articles were included in this scoping review. Figure 1 shows the complete study selection process in a PRISMA flow chart.

Figure 1. PRISMA flow chart for the study selection process.
The indexed publications were reviewed independently by two reviewers using Rayyan software to check titles and abstracts [Qatar Computing Research Institute (Data Analytics), Doha, Qatar] (13). Any discrepancies between the reviewers at any stage of the selection process were resolved through discussion or by a third reviewer. The full text of selected citations was reviewed in detail. Reasons for excluding literature in the complete text analysis phase were recorded.
Data extraction was done using a standardized data abstraction table developed for this scoping review. The table included relevant information on study characteristics (year of publication, outcomes, country, and study population), detailed information on study periods, and described changes in EMS calls and operations. All patients included in the studies were considered. Based on an initial literature search and our own experience, additional subgroup analyses from the studies on the following diagnoses were included in the table: cardiac emergencies, respiratory diseases, traumata, mental health conditions, and intoxications. The percentage changes presented in the studies are included in the table. If absolute values were given, percentage changes were calculated. If a percentage change was neither shown nor could be calculated, the only information included in the table was whether an increase, a decrease, or no change was observed. Two reviewers carried out data extraction. Ambiguities and uncertainties were discussed with a third reviewer.
For the figures that show the frequencies of call-outs or emergency calls, the relative frequencies in terms of increase or decrease were presented in bar charts, as well as the mean change in the respective diagnostic groups and the 95% confidence interval in the further figure.
Table 2 shows the study characteristics, including study outcomes, year of publication, country of origin, and study population. Of the 50 articles included, 14 reported the number of EMS calls, 30 reported the number of EMS operations, and six reported both outcomes (Figures 2, 3). The articles were mostly published in 2020 (n = 18) or 2021 (n = 29) and covered the situation of EMS services during the COVID-19 pandemic in 13 European countries and ten non-European countries. Countries most frequently represented among the included studies were the USA (n = 9), Germany (n = 7) and Italy (n = 6) (Figure 4). Most studies reported the number of EMS calls or operations for all patients. Two articles are limited to specific age groups (14, 15), and eight are limited to specific stroke diagnoses (16–23). In some studies, in addition to analyses of all patients, additional subgroup analyses were conducted (Supplementary material). The study periods varied between the included articles (Supplementary material). Most studies reported the first months of the COVID-19 pandemic, which often included a lockdown. Others reported more extended periods, e.g., about a year. Most articles compared the number of EMS calls or operations with those from the corresponding period in the previous year(s). Others compared to the months before the outbreak of the COVID-19 pandemic or reported variations in the months of the pandemic. Some studies compared several periods.
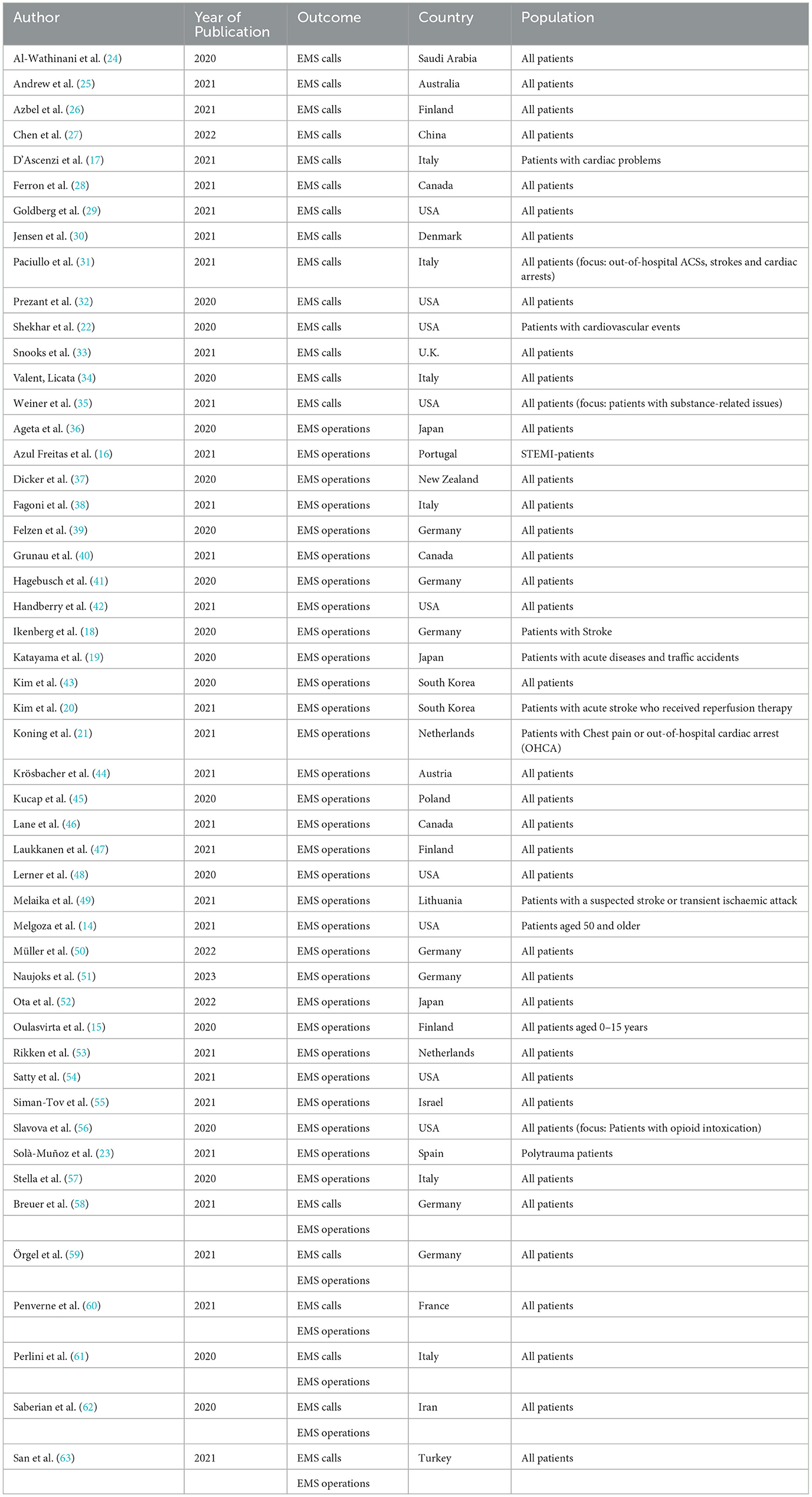
Table 2. Study characteristics.
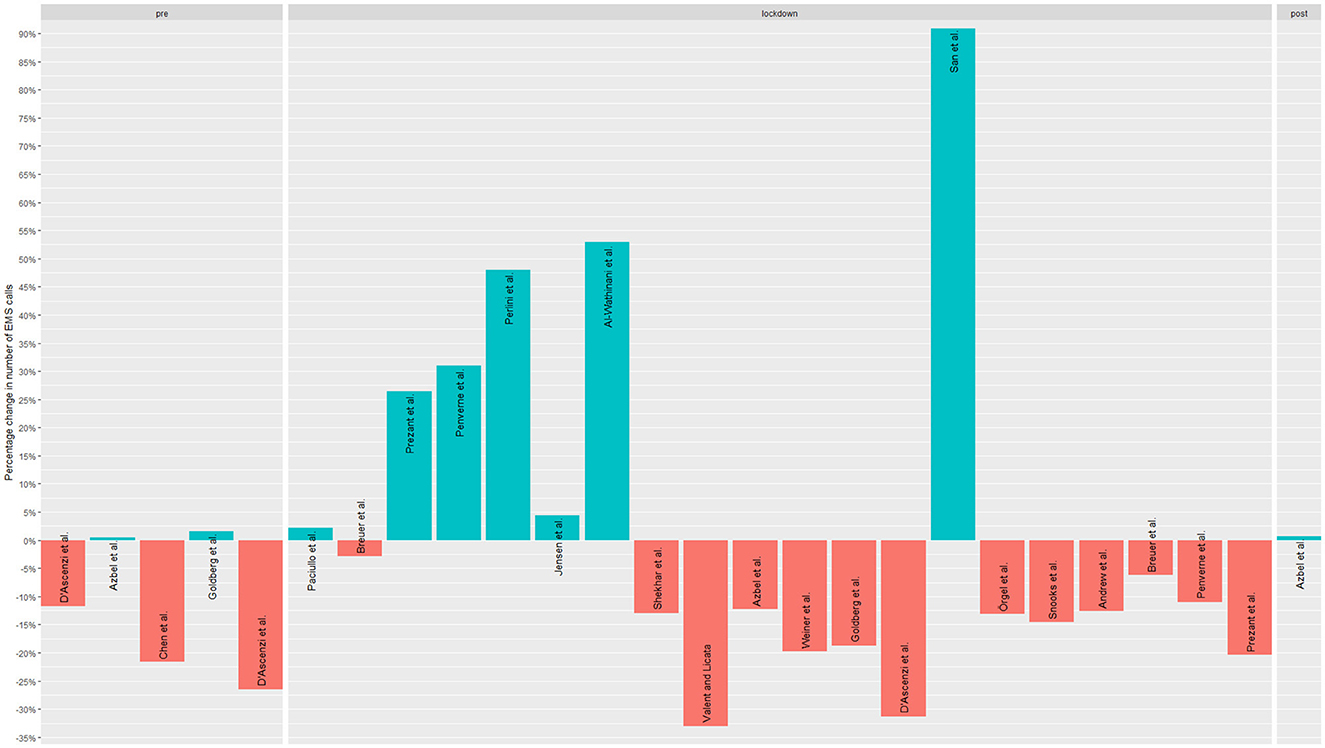
Figure 2. Studies' reported changes regarding EMS calls.
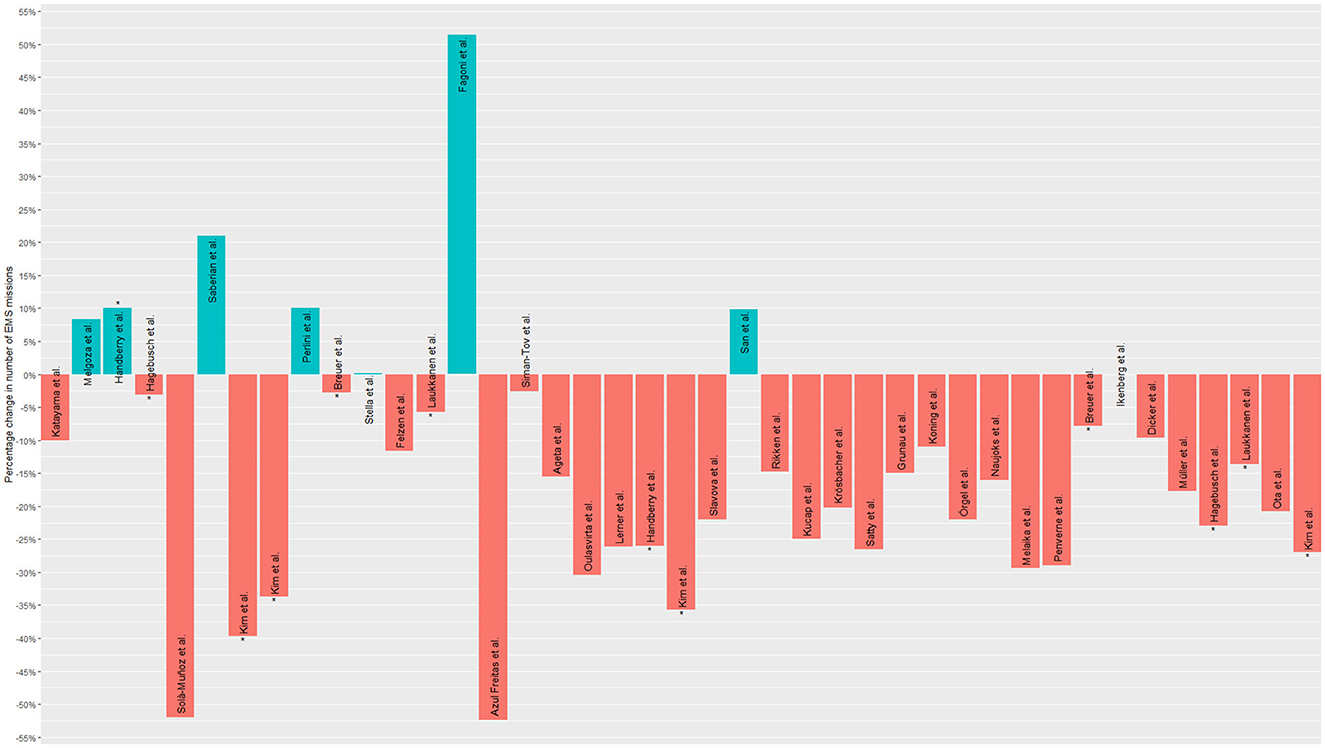
Figure 3. Studies' reported changes regarding EMS operations. In the graph, those studies that appear more than once (because they compared different periods) are marked with an asterisk (*).
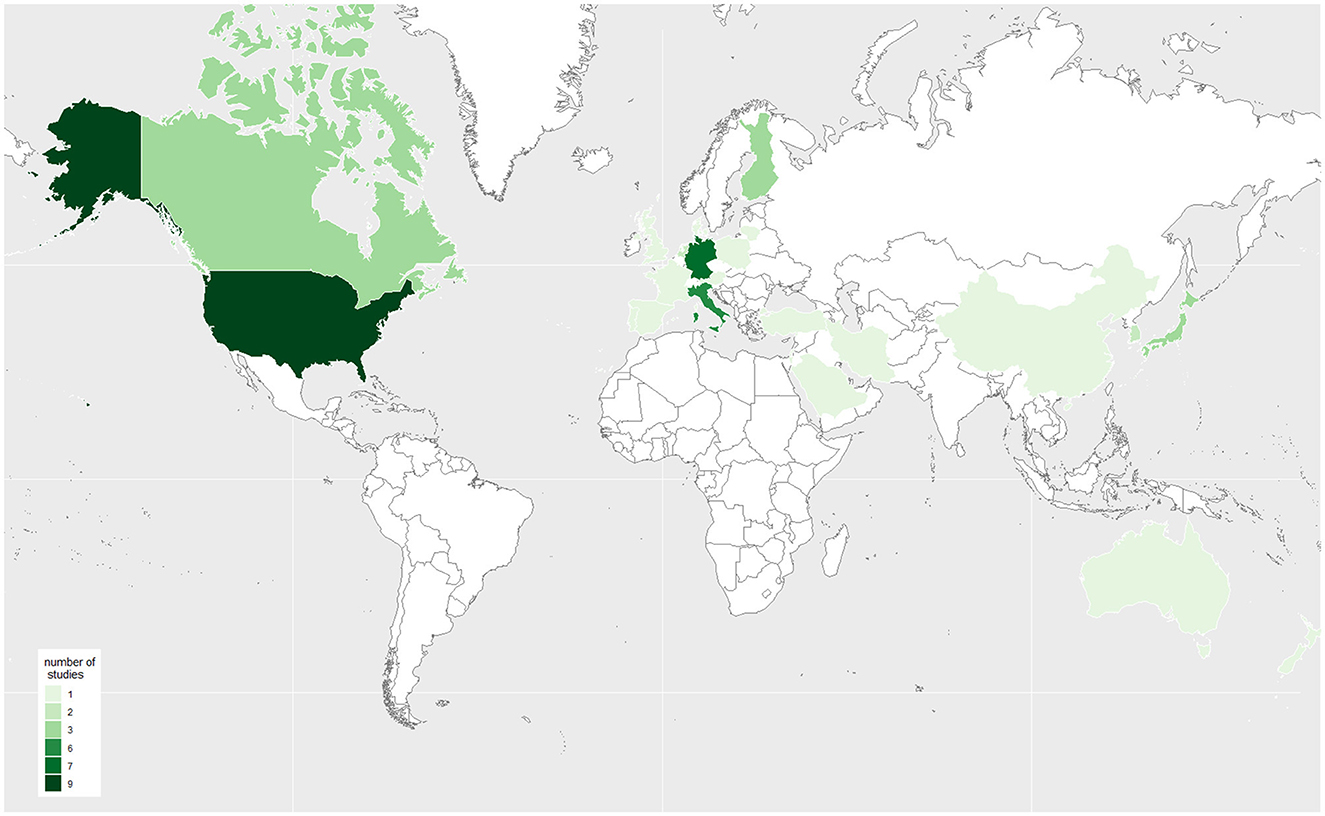
Figure 4. Origin of the included studies (the darker the color the more studies included).
The articles reporting quantitative data on changes in emergency calls demonstrate a mean change of 0.0%. However, considerable variation exists, with a standard deviation of 31.3% (minimum: −50.0% to maximum: 121.0%). Of the 20 articles that reported changes regarding EMS calls, nine reported a decrease (17, 22, 25, 27, 28, 33–35, 59), varying from −4.62% (22) to −33.02% (34) (Supplementary material). They presented the situation in Australia (25), China (27), Italy (17, 34), Canada (28), Germany (59), the USA (22, 35) and U.K. (33). An increase in EMS calls was observed in six studies, varying from +2.14% (31) to +90.9% (63) (Supplementary material). An increase of +347% (62) represented a substantial outlier value. An increase was reported in Saudi Arabia (24), Denmark (30), Italy (31, 61), Iran (62) and Turkey (63). Five studies reported mixed trends in the number of emergency calls in Finland (26), Germany (58), the USA (29, 32), and France (60), depending on the study period.
EMS calls on cardiac emergencies, respiratory diseases, trauma, mental health conditions, and intoxication were considered (Supplementary material). Eleven studies examined changes in EMS calls for cardiac emergencies (17, 22, 24, 25, 27–29, 31, 32, 34, 60). Five studies reported increased calls for cardiac emergencies, three reported a decrease, and three had mixed trends. Changes in EMS calls for respiratory diseases were examined in six studies (28, 29, 32, 34, 35, 60). Four articles reported an increase, and two articles reported a decrease. Six studies reported changes for traumata (24, 26, 28, 32, 34, 60), five of which observed a decrease, and one article reported mixed trends depending on a specific diagnosis. Changes in EMS calls for mental health conditions are the subject of three articles (25, 28, 32). Two reported an increase, and one a decrease. Three studies reported changes in intoxication (28, 35, 60); one stated an increase and two a decrease.
The articles that reported quantitative data on changes in EMS operations indicated an overall mean decrease of −12.2%, with a standard deviation of 24.7% (minimum: −72% to maximum: 56%) (Figure 5). Overall, 36 studies included changes in EMS operations (Supplementary material). Of these, 27 studies reported a decrease in EMS operations during the COVID-19 pandemic (15, 16, 19–21, 23, 36, 37, 39–41, 43–56, 58–60), varying from −2.6% (55) to −52.4% (16) (Supplementary material). Countries for which a decrease was reported were Japan (19, 36, 52), Portugal (16), Germany (39, 41, 50, 51, 58, 59), New Zealand (37), South Korea (20, 43), the Netherlands (21, 53), Austria (44), Canada (40), Poland (45), Finland (15, 47), the USA (48, 54, 56), Lithuania (49), France (60), Israel (55) and Spain (23). An increase in EMS operations was reported in six studies (14, 38, 46, 61–63), varying from +8.32% (14) to +51.5% (38) and representing the situation in Italy (38, 61), the USA (14), Canada (46), Iran (62) and Turkey (63). Two studies (Germany (18) and Italy (57) stated no changes in EMS operation frequencies. One study from the USA reported mixed trends depending on the study period.
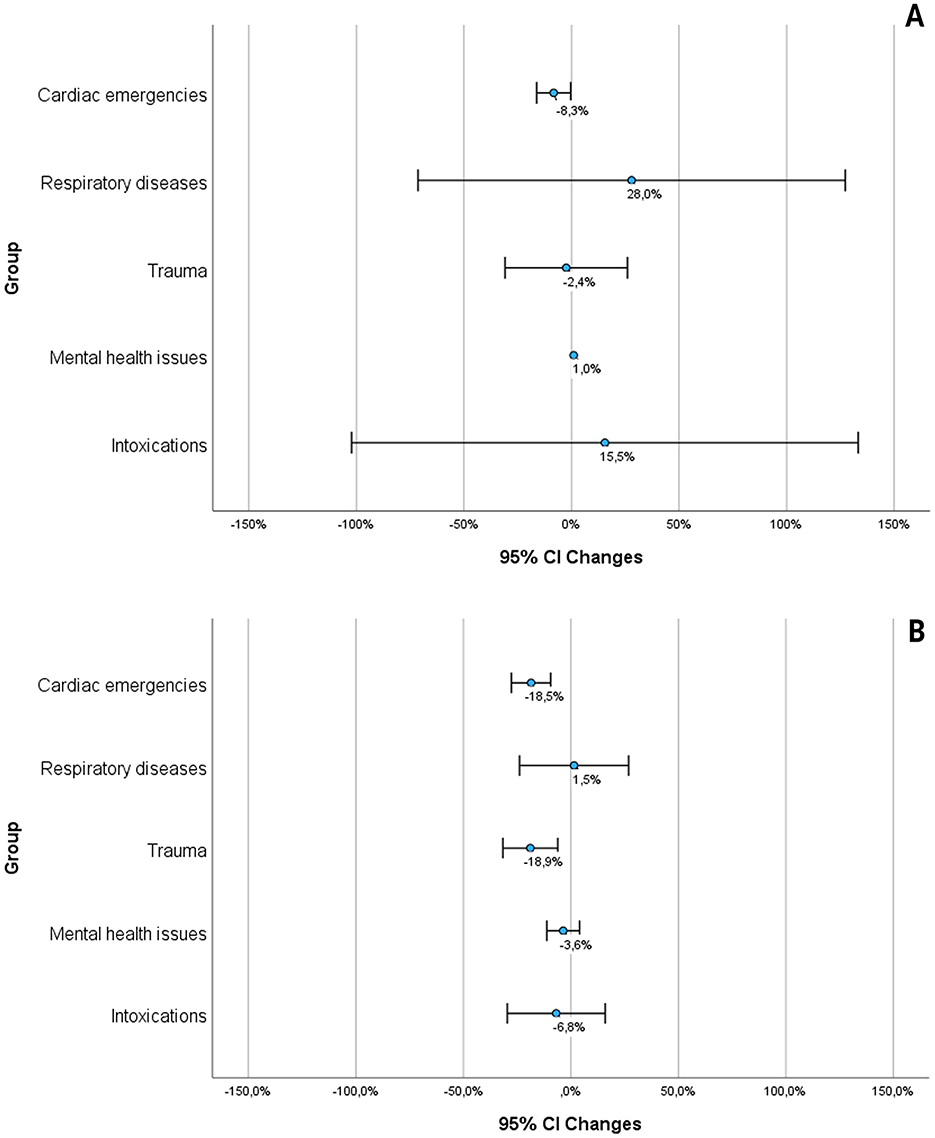
Figure 5. The figures show the graphical summary (mean and 95%-confidence interval) of the studies that reported quantitative data. (A) Shows the emergency calls, (B) shows the EMS operations, based on the sources: (16, 18, 20, 21, 37, 40, 44, 45, 49, 51, 54, 55, 57, 60, 63).
EMS operations on cardiac emergencies, respiratory diseases, traumata, mental health conditions, and intoxication were considered (Supplementary material). Fourteen studies reported changes in EMS operations for cardiac emergencies (16, 18, 20, 21, 37, 40, 45, 49, 51, 54, 55, 57, 60, 63). One study reported an increase, nine reported a decrease, and three reported mixed trends depending on the specific diagnosis. In addition, one article reports no change. Nine studies examined changes in EMS operations for respiratory diseases (37, 38, 40, 44, 45, 50, 54, 55, 57). Six of them reported an increase, and three of them a decrease. Thirteen studies reported changes in traumata (15, 19, 23, 26, 37, 40, 44, 45, 48, 51, 54, 55, 57). One study stated an increase and ten studies stated a decrease of EMS operations for traumata. Two studies reported mixed trends depending on the specific diagnosis. Six studies reported changes in mental health conditions (37, 40, 45, 51, 54, 55); four reported an increase, and two a decrease. Five studies included changes in EMS operations for intoxication (37, 51, 54–56). Two described an increase, and three, a decrease in EMS operations.
This review demonstrates the global impact of the coronavirus disease 2019 (COVID-19) pandemic on emergency medical services (EMS). We analyzed the number of emergency calls EMS operations and how these relate to specific diagnoses. Emergency calls showed no discernible trend, unlike in EMS operations, where frequencies decreased overall. This trend was also observed in the diagnoses of cardiac emergencies, traumata, and mental health conditions. On the other hand, respiratory diseases showed an increasing trend in EMS operations. EMS calls did not show a clear trend regarding specific diagnoses. However, considering the substantial data, heterogeneity results should be interpreted carefully. Data heterogeneity is caused by the pandemic's dynamic progression, resulting in variations in reported time intervals, study populations, and corresponding EMS systems.
While EMS operations decreased overall, studies from individual countries show increased EMS operations. So in Italy (+51.5% and +10%) (38, 61), an increase was reported from Iran (+21%) (62), an increase in Turkey (+9.8%) (63), an increase in California among older Latinos (+8.3%) (14), and an increase in Canada (+61%) (46). Apart from the different periods reported, it is challenging to identify geographical or structural correlations. A wide range of influences, such as the structure of the health care system, socio-demographic factors, and health policy decisions during the pandemic, need to be discussed.
The most significant effect, reported in almost all studies, might be caused by fear of getting infected with COVID-19 (14, 18, 21, 28, 51). This fear might have prevented people from seeking medical treatment (21, 27, 28, 61), for example, in hospitals (17–19, 21, 27, 29, 35, 40, 44, 45, 48, 51, 54–57, 59, 61). Aspects stimulating this fear were public information strategies (17, 55) with general recommendations to avoid hospitalization in case of non-emergency diseases (27, 47). However, it is also discussed that patients do not want to burden the healthcare system further (19, 21, 29, 40, 44, 46, 54), perhaps reinforced by media coverage from regions dramatically affected (40) and campaigns to thank healthcare providers (19). On the other hand, it is discussed that people were frightened by the media coverage, panicked, and called the emergency services to get information (63). Studies, when reported, classify differently from urgent or differently severely ill or injured patients. However, the proportion of non-life-threatening and, therefore, possibly “non-urgent bagatelle missions” has decreased by 58% in some cases (39).
The lockdown, with its social restrictions, also significantly impacted the number of EMS calls and operations. The closure of schools and workplaces, bars and nightclubs, and increased hygiene practices prevented many community-acquired illnesses (37). In addition, our scoping review demonstrates that patients with different diagnoses used the EMS more or less frequently during the COVID-19 pandemic. However, considering the results within the broader context of the general frequency of EMS calls and operations, along with their variations, is imperative. The periods examined in the individual studies included in this review were presented with significant heterogeneity. Nevertheless, when frequencies were previously available, the impression could be confirmed that the COVID-19 pandemic is the cause of the substantial fluctuations, as external literature also suggests (17, 37, 45, 47, 64).
Most of the studies included investigated cardiac emergencies in the broader sense during the COVID-19 pandemic. These included suspected diagnoses such as chest pain, myocardial infarction, cardiac arrest, stroke, and cerebral ischemia (Supplementary material). There is no clear trend in the emergency calls in the included studies, but the data indicate a decline in the number of emergency operations.
Changes in the utilization of EMS for cardiac emergencies and strokes have been described even in life-threatening health emergencies (18, 21, 22, 28, 33, 42, 46, 47, 49, 55, 63) leading to delayed response times or alerts to the emergency medical services (29, 42, 47, 55, 63). On the other hand, it was discussed whether the public recommendations on using emergency numbers led to increased EMS operations, particularly in the case of COVID-19 symptoms. The initial objective of this strategy was to prevent an undue burden on the emergency services, but it led to a delay in alerts and, therefore, in treatment. (20). However, it has been suggested that sudden professional and personal isolation also led to lifestyle changes (e.g., increased nicotine consumption and poorer medication adherence) in the home environment, which may be a further cause of the increase in cardiac emergencies and strokes (51). In contrast, decreased cardiovascular emergencies were explained by less intense physical activity, better air quality, and lower physiological and work-related stress in conjunction with COVID-19 measures, which could reduce the risk of acute myocardial infarction and stress-related cardiac events (21).
COVID-19 is a systemic disease, so symptoms and the severity of a COVID-19 infection vary depending on the virus type. In addition to fever, respiratory symptoms such as respiratory distress and shortness of breath predominated. Therefore, many studies have examined the trends of EMS calls and operations for respiratory diseases, and there has been an increase. Increased operations caused by breathlessness were related to increased alertness of the population to these symptoms (14, 44). Reduced respiratory diseases have been linked to various factors like decreased social contact, decreased transmission of airborne illnesses (37), and improved air quality during the lockdown (37).
Trauma-related incidents have declined sharply. There are many reasons for the decline in injuries and accidents, which are well explained. Traffic volumes fell sharply worldwide during the COVID-19 pandemic, accompanied by a significant decline in road deaths worldwide and reduced road fatalities (65). This is attributed to the general reduction in mobility, especially car traffic (23, 28, 37, 44, 45, 48, 52, 54, 55, 62), as the included studies also show, which is well explained by “stay at home” slogans (52, 54, 62, 63), the expansion of flexible working hours (63), home office jobs, and reduced commuter flow (51) l. However, road traffic accidents and trauma generally decreased (66, 67). Reasons for this decrease in EMS calls and operations due to traumata, in general, were related to the closure of nightclubs and bars (26, 37), an inability to socialize (37), canceled sports events and practices (26, 54), reduced risky recreational activities (48) and injury-prone locations (55).
Studies examining EMS calls and operations due to mental health conditions showed a slight trend toward an increase. The increase in mental health conditions was associated with the restriction in social contacts and social isolation (37, 47), the fear of (1) Being infected with COVID-19 (37, 47), (2) losing family and friends through COVID-19 (37), and (3) losing one's job and therefore facing financial difficulties (37)—all possibly resulting in depression and anxiety (55). Psychosocial stress has also been discussed as a cause of an increase in domestic violence (23, 41, 51). Prison releases result in individuals abruptly reentering society, mainly without a care plan for people with opioid use disorder (56), and changes in the illicit drug market due to the social distancing measures (56). Other studies report an increase in psychosocial emergencies and higher suicide rates without providing a socio-spatial context (68, 69). A group that was reported to be severely affected by the restrictions due to COVID-19 were those using substances or those in recovery (28, 35, 42). Reasons discussed to explain this were social isolation, a lack of social support, stress, and particularly the interruption of (1) regular primary health care (28, 56), (2) medication supply for people with opioid use disorder, and (3) recovery support services (42). Concerning intoxication, no clear trend has been shown in the included studies.
The principal challenge is the lack of comparability among the included studies due to differences in the reported study periods, the study populations and countries, and the corresponding EMS systems and contexts of comparison. Furthermore, the influence of the pandemic should be acknowledged not only in terms of emergency calls and operations but also in the treatment time for patients and the time required for ambulances to become operational due to hygiene protocols, which were not included in the review.
Since only articles in German and English were included, developments in other language countries could not be considered if studies were published in the national language. In addition, several other publications emerged during the research, but these were not included after the research period.
This scoping review shows that COVID-19 significantly impacted EMS calls and operations worldwide. While some studies report increased EMS calls and others decreased, a clear trend toward reduced EMS operations is evident. Specific patient groups used emergency services differently during the pandemic, influenced by social restrictions, lockdowns, and lifestyle changes. These findings highlight the need for improved preparedness for future crises.
Hospital studies reveal high workloads and increased mortality, yet a critical gap remains: EMS data are rarely linked to hospital outcomes, limiting insights into patient trajectories. A standardized “minimum emergency data set” or core data points should be established globally to improve emergency care and crisis response. This would enable better data interoperability within EMS and between EMS and hospitals, supporting more informed decision-making. Given global differences in healthcare systems and data protection laws, adaptable frameworks are essential to facilitate secure data exchange.
Despite these challenges, EMS demonstrated agility and adaptability. Although managing infectious patients is not routine for EMS, they quickly adjusted protocols, stocked protective equipment, and adapted faster than other healthcare providers.
However, the immense burden on EMS personnel must not be overlooked. Beyond traditional roles, they contributed significantly through COVID-19 testing, vaccine delivery, increased sanitation, extended response times, patient education, and covering for isolated colleagues. Their dedication ensured continuity of emergency care despite extreme strain.
For future health crises, enhancing data interoperability, strengthening EMS-hospital collaboration, and supporting EMS personnel are key to ensuring resilience, optimizing resources, and maintaining high-quality emergency care.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
HR: Formal analysis, Investigation, Writing – original draft, Writing – review & editing. MS: Formal analysis, Investigation, Methodology, Validation, Writing – review & editing. JE: Data curation, Formal analysis, Methodology, Validation, Visualization, Writing – review & editing. NJ: Data curation, Resources, Visualization, Writing – review & editing. HH: Conceptualization, Funding acquisition, Investigation, Project administration, Resources, Writing – review & editing. DH: Conceptualization, Formal analysis, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
The author(s) declare that financial support was received for the research and/or publication of this article. This research project was funded by the Forum Health Location Baden-Württemberg, Ministry of Science, Research and the Arts Baden-Württemberg, Germany.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
The author(s) declare that no Gen AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1543150/full#supplementary-material
1. World Health Organization. Pulse Survey on Continuity of Essential Health Services During the COVID-19 Pandemic (2020). Available online at: https://iris.who.int/bitstream/handle/10665/334048/WHO-2019-nCoV-EHS_continuity-survey-2020.1-eng.pdf?sequence=1 (accessed on 14 June 2024).
2. Sandford A. Coronavirus: Half of Humanity Now on Lockdown as 90 Countries Call for Confinement. Available online at: https://www.euronews.com/2020/04/02/coronavirus-in-europe-spain-s-death-toll-hits-10-000-after-record-950-new-deaths-in-24-hou (accessed on 14 June 2024).
3. Mathieu E, Ritchie H, Rodés-Guirao L, Appel C, Gavrilov D, Giattino C, et al. COVID-19: School and Workplace Closures Available online at: https://ourworldindata.org/covid-school-workplace-closures (accessed on 14 June 2024).
4. Mathieu E, Ritchie H, Rodés-Guirao L, Appel C, Gavrilov D, Giattino C, et al. COVID-19: Stay-at-Home Restrictions. Available online at: https://ourworldindata.org/covid-stay-home-restrictions (accessed on 14 June 2024).
5. Marinoni G, Van't Land H, Jensen T. The impact of COVID-19 on higher education around the world IAU global survey report. (2020). Paris: International Association of Universities.
6. Tadesse S, Muluye W. The impact of COVID-19 pandemic on education system in developing countries: a review. Open J Soc Sci. (2020) 08:159–70. doi: 10.4236/jss.2020.810011
7. Naseer S, Khalid S, Parveen S, Abbass K, Song H, Achim MV. COVID-19 outbreak: impact on global economy. Front Public Health. (2022) 10:1009393. doi: 10.3389/fpubh.2022.1009393
8. Ibn-Mohammed T, Mustapha KB, Godsell J, Adamu Z, Babatunde KA, Akintade DD, et al. A critical analysis of the impacts of COVID-19 on the global economy and ecosystems and opportunities for circular economy strategies. Resour Conserv Recycl. (2021) 164:105169. doi: 10.1016/j.resconrec.2020.105169
9. Moynihan R, Sanders S, Michaleff ZA, Scott AM, Clark J, To EJ, et al. Impact of COVID-19 pandemic on utilisation of healthcare services: a systematic review. BMJ Open. (2021) 11:e045343. doi: 10.1136/bmjopen-2020-045343
10. Roy CM, Bollman EB, Carson LM, Northrop AJ, Jackson EF, Moresky RT. Assessing the indirect effects of COVID-19 on healthcare delivery, utilization and health outcomes: a scoping review. Eur J Public Health. (2021) 31:634–40. doi: 10.1093/eurpub/ckab047
11. Arksey H, O'Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. (2005) 8:19–32. doi: 10.1080/1364557032000119616
12. Tricco AC, Lillie E, Zarin W, O'Brien KK, Colquhoun H, Levac D, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. (2018) 169:467–73. doi: 10.7326/M18-0850
13. Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan-a web and mobile app for systematic reviews. Syst Rev. (2016) 5:210. doi: 10.1186/s13643-016-0384-4
14. Melgoza E, Beltrán-Sánchez H, Bustamante AV. Emergency medical service use among latinos aged 50 and older in California Counties, Except Los Angeles, During the Early COVID-19 pandemic period. Front Public Health (2021) 9:660289. doi: 10.3389/fpubh.2021.660289
15. Oulasvirta J, Pirneskoski J, Harve-Rytsälä H, Lääperi M, Kuitunen M, Kuisma M, et al. Paediatric prehospital emergencies and restrictions during the COVID-19 pandemic: a population-based study. BMJ Paediatr Open (2020) 4:e000808. doi: 10.1136/bmjpo-2020-000808
16. Azul Freitas A, Baptista R, Gonçalves V, Ferreira C, Milner J, Lourenço C, et al. Impact of SARS-CoV-2 pandemic on ST-elevation myocardial infarction admissions and outcomes in a Portuguese primary percutaneous coronary intervention center: preliminary Data. Revista portuguesa de cardiologia orgao oficial da Sociedade Portuguesa de Cardiologia. (2021) 40:465–71. doi: 10.1016/j.repc.2020.10.012
17. D'Ascenzi F, Cameli M, Forni S, Gemmi F, Szasz C, Di Fabrizio V, et al. Reduction of emergency calls and hospitalizations for cardiac causes: effects of COVID-19 pandemic and lockdown in Tuscany region. Front Cardiovasc Med. (2021) 8:625569. doi: 10.3389/fcvm.2021.625569
18. Ikenberg B, Hemmer B, Dommasch M, Kanz K-G, Wunderlich S, Knier B. Code stroke patient referral by emergency medical services during the public COVID-19 pandemic lockdown. J Stroke Cerebrovasc Dis Off J Nat Stroke Assoc. (2020) 29:105175. doi: 10.1016/j.jstrokecerebrovasdis.2020.105175
19. Katayama Y, Kiyohara K, Kitamura T, Hayashida S, Shimazu T. Influence of the COVID-19 pandemic on an emergency medical service system: a population-based, descriptive study in Osaka, Japan. Acute Med Surg. (2020) 7:e534. doi: 10.1002/ams2.534
20. Kim YD, Nam HS, Sohn SI, Park H, Hong JH, Kim GS, et al. Care process of recanalization therapy for acute stroke during the COVID-19 outbreak in South Korea. J Clin Neurol (Seoul, Korea) (2021) 17:63–9. doi: 10.3988/jcn.2021.17.1.63
21. Koning ER de, Boogers MJ, Bosch J, Visser M de, Schalij MJ, Beeres SLMA. Emergency medical services evaluations for chest pain during first COVID-19 lockdown in Hollands-Midden, the Netherlands. Neth Heart J (2021) 29:224–9. doi: 10.1007/s12471-021-01545-y
22. Shekhar AC, Effiong A, Ruskin KJ, Blumen I, Mann NC, Narula J. COVID-19 and the Prehospital Incidence of Acute Cardiovascular Events (from the Nationwide US EMS). Am J Cardiol. (2020) 134:152–3. doi: 10.1016/j.amjcard.2020.08.003
23. Solà-Muñoz S, Yuguero O, Azeli Y, Roig G, Prieto-Arruñada JA, Español J, et al. Impact on polytrauma patient prehospital care during the first wave of the COVID-19 pandemic: a cross-sectional study. Eur J Trauma Emerg Surg. (2021) 47:1351–8. doi: 10.1007/s00068-021-01748-3
24. Al-Wathinani A, Hertelendy AJ, Alhurishi S, Mobrad A, Alhazmi R, Altuwaijri M, et al. Increased Emergency Calls during the COVID-19 Pandemic in Saudi Arabia: a National Retrospective Study. Healthcare (2020) 9:14. doi: 10.3390/healthcare9010014
25. Andrew E, Nehme Z, Stephenson M, Walker T, Smith K. The Impact of the COVID-19 Pandemic on Demand for Emergency Ambulances in Victoria, Australia. Prehosp Emerg Care. (2021) 16:1–7. doi: 10.1080/10903127.2021.1944409
26. Azbel M, Heinänen M, Lääperi M, Kuisma M. Effects of the COVID-19 pandemic on trauma-related emergency medical service calls: a retrospective cohort study. BMC Emerg Med. (2021) 21:102. doi: 10.1186/s12873-021-00495-3
27. Chen J, Cheng Y-R, Fu X-Y, Wang C-Y, Wen W, Ni J, et al. Exploring the impact of the COVID-19 epidemic on the medical emergency calls and calls for cardiovascular diseases in Hangzhou, China. Irish J Med Sci. (2022) 191:563–7. doi: 10.1007/s11845-021-02644-w
28. Ferron R, Agarwal G, Cooper R, Munkley D. The effect of COVID-19 on emergency medical service call volumes and patient acuity: a cross-sectional study in Niagara, Ontario. BMC Emerg Med. (2021) 21:39. doi: 10.1186/s12873-021-00431-5
29. Goldberg SA, Cash RE, Peters G, Weiner SG, Greenough PG, Seethala R. The impact of COVID-19 on statewide EMS use for cardiac emergencies and stroke in Massachusetts. J Am Coll Emerg Physicians Open. (2021) 2:e12351. doi: 10.1002/emp2.12351
30. Jensen T, Holgersen MG, Jespersen MS, Blomberg SN, Folke F, Lippert F, et al. Strategies to handle increased demand in the COVID-19 crisis: a coronavirus EMS support track and a web-based self-triage system. Prehosp Emerg Care. (2021) 25:28–38. doi: 10.1080/10903127.2020.1817212
31. Paciullo F, Giannandrea D, Gianfredi V, Borgognoni F, Verdecchia P, L'Angiocola PD, et al. Epidemiology of emergency calls for time-dependent acute illnesses during COVID-19 outbreak in Umbria region (Italy). Ann Ig. (2021) 33:198–200. doi: 10.7416/ai.2020.2392
32. Prezant DJ, Lancet EA, Zeig-Owens R, Lai PH, Appel D, Webber MP, et al. System impacts of the COVID-19 pandemic on New York City's emergency medical services. J Am Coll Emerg Physicians Open. (2020) 1:1205–13. doi: 10.1002/emp2.12301
33. Snooks H, Watkins AJ, Bell F, Brady M, Carson-Stevens A, Duncan E, et al. Call volume, triage outcomes, and protocols during the first wave of the COVID-19 pandemic in the United Kingdom: results of a national survey. J Am Coll Emerg Physicians Open. (2021) 2:e12492. doi: 10.1002/emp2.12492
34. Valent F, Licata S. Emergency medical services calls during Italy's COVID-19 Lockdown. Ann Emerg Med. (2020) 76:812–4. doi: 10.1016/j.annemergmed.2020.06.036
35. Weiner SG, Cash RE, Hendricks M, El Ibrahimi S, Baker O, Seethala RR, et al. Ambulance calls for substance-related issues before and after COVID-19. Prehosp Emerg Care. (2021) 25:768–76. doi: 10.1080/10903127.2020.1845420
36. Ageta K, Naito H, Yorifuji T, Obara T, Nojima T, Yamada T, et al. Delay in emergency medical service transportation responsiveness during the COVID-19 pandemic in a minimally affected region. Acta medica Okayama. (2020) 74:513–20.
37. Dicker B, Swain A, Todd VF, Tunnage B, McConachy E, Drake H, et al. Changes in demand for emergency ambulances during a nationwide lockdown that resulted in elimination of COVID-19: an observational study from New Zealand. BMJ Open. (2020) 10:e044726. doi: 10.1136/bmjopen-2020-044726
38. Fagoni N, Perone G, Villa GF, Celi S, Bera P, Sechi GM, et al. The lombardy emergency medical system faced with COVID-19: the impact of out-of-hospital outbreak. Prehosp Emerg Care. (2021) 25:1–7. doi: 10.1080/10903127.2020.1824051
39. Felzen M, Brockert A-K, Beckers S, Follmann A, Rossaint R, Schröder H. Einfluss der COVID-19-Pandemie auf die prähospitale Notfall- und Telenotfallmedizin—eine vergleichende Kohortenanalyse. Der Notarzt. (2020) 36:271–7. doi: 10.1055/a-1211-2484
40. Grunau B, Helmer J, Lee S, Acker J, Deakin J, Armour R, et al. Decrease in emergency medical services utilization during early stages of the COVID-19 pandemic in British Columbia. CJEM. (2021) 23:237–41. doi: 10.1007/s43678-020-00062-y
41. Hagebusch P, Naujoks F, Rouchi H, Schindelin I, Schweigkofler U. Decline in emergency medical service missions during the COVID-19 pandemic: results from the fifth largest city in Germany. Intern Emerg Med. (2020) 15:1609–11. doi: 10.1007/s11739-020-02482-1
42. Handberry M, Bull-Otterson L, Dai M, Mann NC, Chaney E, Ratto J, et al. Changes in Emergency Medical Services Before and During the COVID-19 Pandemic in the United States, January 2018-December 2020. Clin Infect Dis. (2021) 73:S84–91. doi: 10.1093/cid/ciab373
43. Kim HS, Jang TC, Kim GM, Lee SH, Ko SH, Seo YW. Impact of the coronavirus disease 2019 outbreak on the transportation of patients requiring emergency care. Medicine. (2020) 99:e23446. doi: 10.1097/MD.0000000000023446
44. Krösbacher A, Kaiser H, Holleis S, Schinnerl A, Neumayr A, Baubin M. Evaluierung der Maßnahmen zur Reduktion von Notarzteinsätzen in Tirol während der COVID-19-Pandemie. Der Anaesthesist. (2021) 70:655–61. doi: 10.1007/s00101-021-00915-w
45. Kucap M, Nadolny K, Ładny JR, Zyśko D, Gałazkowski R, Gasior M, et al. Retrospective analysis of interventions performed by emergency medical teams in poland before and during the SARS-CoV-2 Pandemic. Wiadomosci lekarskie (Warsaw, Poland 1960). (2020) 73:1659–62. doi: 10.36740/WLek202008113
46. Lane DJ, Blanchard IE, Buick JE, Shaw M, McRae AD. Changes in presentation, presenting severity and disposition among patients accessing emergency services during the first months of the COVID-19 pandemic in Calgary, Alberta: a descriptive study. CMAJ Open. (2021) 9:E592–601. doi: 10.9778/cmajo.20200313
47. Laukkanen L, Lahtinen S, Liisanantti J, Kaakinen T, Ehrola A, Raatiniemi L. Early impact of the COVID-19 pandemic and social restrictions on ambulance missions. Eur J Public Health. (2021) 31:1090–5. doi: 10.1093/eurpub/ckab065
48. Lerner EB, Newgard CD, Mann NC. Effect of the coronavirus disease 2019 (COVID-19) pandemic on the U.S. emergency medical services system: a preliminary report. Acad Emerg Med. (2020) 27:693–9. doi: 10.1111/acem.14051
49. Melaika K Sveikata L Wiśniewski A Jaxybayeva A Ekkert A JatuŽis D . Changes in prehospital stroke care and stroke mimic patterns during the COVID-19 lockdown. Int J Environ Res Public Health. (2021) 18:2150. doi: 10.3390/ijerph18042150
50. Müller F, Hummers E, Jablonka A, Schmidt T, Noack EM. Auswirkung des COVID-19-Lockdowns auf Rettungseinsätze. Notfall & rettungsmedizin. (2022) 25:341–7. doi: 10.1007/s10049-021-00873-1
51. Naujoks F, Schweigkofler U, Lenz W, Blau J, Brune I, Lischke V, et al. Veränderungen der rettungsdienstlichen Einsatzzahlen in einer Metropolregion während der ersten COVID-19-Pandemie-bedingten Kontaktbeschränkungsphase. Notfall & rettungsmedizin. (2023) 26:30–8. doi: 10.1007/s10049-021-00875-z
52. Ota S, Jitsuiki K, Muramatsu K-I, Kushida Y, Nagasawa H, Yasuda K, et al. Analysis of the dispatch of physician staffed-helicopters in the COVID-19 pandemic. Am J Emerg Med. (2022) 54:306–8. doi: 10.1016/j.ajem.2021.05.018
53. Rikken QG, Mikdad S, Mota MT, Leeuw MA de, Schober P, Schwarte LA, et al. Operational experience of the Dutch helicopter emergency medical services (HEMS) during the initial phase of the COVID-19 pandemic: jeopardy on the prehospital care system? Eur J Trauma Emerg Surg. (2021) 47:703–11. doi: 10.1007/s00068-020-01569-w
54. Satty T, Ramgopal S, Elmer J, Mosesso VN, Martin-Gill C. EMS responses and non-transports during the COVID-19 pandemic. Am J Emerg Med. (2021) 42:1–8. doi: 10.1016/j.ajem.2020.12.078
55. Siman-Tov M, Strugo R, Podolsky T, Blushtein O. An assessment of treatment, transport, and refusal incidence in a National EMS's routine work during COVID-19. Am J Emerg Med. (2021) 44:45–9. doi: 10.1016/j.ajem.2021.01.051
56. Slavova S, Rock P, Bush HM, Quesinberry D, Walsh SL. Signal of increased opioid overdose during COVID-19 from emergency medical services data. Drug Alcohol Depend. (2020) 214:108176. doi: 10.1016/j.drugalcdep.2020.108176
57. Stella F, Alexopoulos C, Scquizzato T, Zorzi A. Impact of the COVID-19 outbreak on emergency medical system missions and emergency department visits in the Venice area. Eur J Emerg Med. (2020) 27:298–300. doi: 10.1097/MEJ.0000000000000724
58. Breuer F, Brettschneider P, Pommerenke C, Poloczek S, Dahmen J. Notrufe und gemeldete Hauptbeschwerden während der COVID-19-Pandemie in der Leitstelle der Berliner Feuerwehr. Der Notarzt. (2021) 37:158–66. doi: 10.1055/a-1403-3347
59. Örgel M, Gogol M, Graulich T, Omar M, Ranker A, Böttcher C, et al. A retrospective analysis of the initial effect of COVID-19 on German prehospital care during lockdown in Germany. Open Access Emerg Med OAEM. (2021) 13:97–105. doi: 10.2147/OAEM.S289070
60. Penverne Y, Jenvrin J, Montassier E. EMS Dispatch Center Activity during the COVID-19 Containment. (2021). 2 p. doi: 10.1016/j.ajem.2020.07.083
61. Perlini S, Canevari F, Cortesi S, Sgromo V, Brancaglione A, Contri E, et al. Emergency Department and Out-of-Hospital Emergency System (112-AREU 118) integrated response to Coronavirus Disease 2019 in a Northern Italy centre. Intern Emerg Med. (2020) 15:825–33. doi: 10.1007/s11739-020-02390-4
62. Saberian P, Conovaloff JL, Vahidi E, Hasani-Sharamin P, Kolivand P-H. How the COVID-19 epidemic affected prehospital emergency medical services in Tehran, Iran. Western J Emerg Med Integr Emerg Care Popul Health. (2020) 21:110–6. doi: 10.5811/westjem.2020.8.48679
63. San I, Usul E, Bekgöz B, Korkut S. Effects of COVID-19 Pandemic on emergency medical services. Int J Clin Pract. (2021) 75:e13885. doi: 10.1111/ijcp.13885
64. Herr D, Bhatia S, Breuer F, Poloczek S, Pommerenke C, Dahmen J. Increasing emergency number utilisation is not driven by low-acuity calls: an observational study of 1.5 million emergency calls (2018–2021) from Berlin. BMC Med. (2023) 21:184. doi: 10.1186/s12916-023-02879-7
65. Yasin YJ, Grivna M, Abu-Zidan FM. Global impact of COVID-19 pandemic on road traffic collisions. World J Emerg Surg. (2021) 16:51. doi: 10.1186/s13017-021-00395-8
66. Stirparo G, Ristagno G, Bellini L, Bonora R, Pagliosa A, Migliari M, et al. Changes to the major trauma pre-hospital emergency medical system network before and during the 2019 COVID-19 Pandemic. J Clin Med. (2022) 11:6748. doi: 10.3390/jcm11226748
67. Driessen ML, van Ditshuizen JC, Waalwijk JF, van den Bunt G, IJpma FF, Reininga IH, et al. Impact of the SARS-CoV-2 pandemic on trauma care: a nationwide observational study. Eur J Trauma Emerg Surg. (2022) 48:2999–3009. doi: 10.1007/s00068-022-01891-5
68. Kippe YD, Adam M, Finck A, Moran JK, Schouler-Ocak M, Bermpohl F, et al. Suicidality in psychiatric emergency department situations during the first and the second wave of COVID-19 pandemic. Eur Arch Psychiatry Clin Neurosci. (2023) 273:311–23. doi: 10.1007/s00406-022-01486-6
Keywords: emergency medical services, emergency medicine, EMS, emergency calls, emergency operations, COVID-19, coronavirus, SARS-CoV-2
Citation: Richter H, Schneider M, Eisenberger J, Jafari N, Haumann H and Häske D (2025) Impact of the COVID-19 pandemic on prehospital emergency medical service: a scoping review. Front. Public Health 13:1543150. doi: 10.3389/fpubh.2025.1543150
Received: 10 December 2024; Accepted: 24 February 2025;
Published: 19 March 2025.
Edited by:
Andrea Brambilla, Polytechnic University of Milan, ItalyReviewed by:
Isabella Nuvolari-Duodo, Fondazione Politecnico di Milano, ItalyCopyright © 2025 Richter, Schneider, Eisenberger, Jafari, Haumann and Häske. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: David Häske, ZGF2aWQuaGFlc2tlQG1lZC51bmktdHVlYmluZ2VuLmRl
†ORCID: Marlieke Schneider orcid.org/0000-0002-7395-3932
Hannah Haumann orcid.org/0009-0006-5876-2878
David Häske orcid.org/0000-0001-5190-3937
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.