 Wenli Yang
Wenli Yang Zubing Xiang1*
Zubing Xiang1* Haoyuan Zheng
Haoyuan Zheng
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 26 February 2025
Sec. Children and Health
Volume 13 - 2025 | https://doi.org/10.3389/fpubh.2025.1540968
Introduction: The physical and mental health of adolescents is a crucial cornerstone for social development. Therefore, this study aimed to examine whether family socioeconomic status made a difference in Chinese teenage mental and physical health and to disentangle the mediating role of parental involvement in youth sports in the process in which family socioeconomic status influenced adolescent health.
Methods: A quantitative analysis used a sample of approximately 11,000 adolescents from Chinese middle schools. The research employed structural equation modelling (SEM) to explore the relationships among family socioeconomic status, parental involvement in youth sports, and adolescent mental and physical health.
Results: The findings indicated that both family socioeconomic status and parental involvement in youth sports significantly positively predict levels of adolescents’ physical health and mental health. Further analysis revealed that parental involvement in youth sports mediated the relationship between family socioeconomic status and adolescent health.
Discussion: It is evident that parental involvement in youth sports plays a crucial role in adolescent mental and physical health. Regardless of family socioeconomic status, parents should actively engage in sports activities with their children, which is not only an important way to promote adolescents’ health but also a manifestation of realizing health equity.
Family socioeconomic status (SES) is a significant factor influencing adolescents’ physical and mental health, demonstrating an important relationship with adolescent health (1, 2). As one of the most crucial social determinants of health, low SES is considered the greatest threat to health by the World Health Organization (3). SES is associated with a wide array of health, cognitive, and socioemotional outcomes in children, with effects beginning before birth and continuing into adulthood (2). Adolescents from different family socioeconomic status often exhibit varying characteristics, among which there exist commonalities. Young adults and middle-aged adults in poverty are multi-morbid compared to their wealthier peers. There is a significant negative association between measures of SES and BMI (4). In a meta-analysis, youth with lower socioeconomic status had greater psychopathology and SES was more strongly related to behavior problems than depression or anxiety (5, 6). Parents, as the primary caregivers of most adolescents, play a vital role in their development. Parents from different socioeconomic backgrounds demonstrate varying attitudes toward their children’s lifestyle and education (7). Children’s wellbeing is positively associated with socioeconomic status (8), so low-SES students may experience more threat, more health problems, more negative emotions (9) Parental involvement can make up for parents’ scarcity of economic and social capital and promote children to participate in more sports activities and help improve their overall health (10).
Adolescence is a critical period of rapid physical and psychological development, where parental accompaniment is an important determinant for ensuring adolescents’ mental health (11). Tangible supportive behaviors by parents, including co-participation and transportation, could positively influence PA levels of their offspring (12) and then promote the health-related physical fitness of adolescents (13). Among different types of parental support behaviors, participating in sports activities with children is particularly effective in promoting adolescents’ engagement in physical exercise (12, 14), which in turn enhances their overall health (15–17).
Socioeconomic status (SES) is a comprehensive sociological concept. Mueller and Parcel (18) defined it as the relative position of individuals or families in the social hierarchy, based on the acquisition or control of wealth, prestige, and power. This conceptual framework which laid the foundation for further research guides this paper to conduct an in-depth exploration of how SES shapes individuals’ life trajectories and impacts on people’s well-being. Findings from research have shown that disparities in SES, as a manifestation of social inequality, significantly influence individuals’ health lifestyle choices, leading to profound effects on their health status (19). According to The social causation hypothesis, individual health that is related to socially determined structural factors means that an individual’s position within the social structure determines their health outcomes, for example, those with lower SES typically experience poorer health (20). The impact of SES extends throughout the life cycle, with socioeconomic inequality resulting in differences in health behaviors and physical health status (21). Max Weber’s classical theoretical framework posits that class, status, and power collectively form an individual’s social position (18). Class is primarily determined by economic factors, status corresponds to an individual’s social prestige and represents the degree of social and cultural support one can access, and power is related to political background (22). Weber’s social stratification research provides profound theoretical insights into understanding SES through the three dimensions. These elements interact to delineate an individual’s position within the social structure, thereby influencing their access to health resources and health outcomes. SES is an important reference for measuring an individual’s position, and researchers usually quantify SES using income, occupation, and educational attainment as indicators (2, 4). Due to children’s and adolescents’ absence from the labor market, the SES of their families or parents serves as the primary basis for assessing childhood and adulthood socioeconomic position (23). This underscores the significance of family background about the children and adolescents’ health. For a long time, SES has been viewed as a fundamental factor of disease and health (24, 25). Empirical research consistently confirms the positive influence of family SES on adolescents’ physical health (26) and mental health (27). Adolescents from low SES backgrounds are at a higher risk of depression (28–30) and tend to report poorer self-evaluated health (31, 32).
The specific parenting behavior of “parental involvement in youth sports,” which refers to the frequency with which adolescents participate in sports activities with their parents, is intrinsically linked to family socioeconomic status (SES). According to ecological systems theory, the impact of external forces (such as parental SES) on children is mediated through parenting processes (33). Parental involvement in youth sports, as a kind of practice within the parenting process, is a vital means by which parents fulfil their roles. It allows parents to directly engage in their children’s daily lives and foster parent–child interaction through sports activities. While existing researches broadly address the concept of parental involvement and explore its relationship with SES, studies directly focusing on parental involvement in youth sports remain limited. Most research employs the broader view of parental involvement to analyze social issues related to adolescents.
Currently, there is still some debate over the specific concept of parental involvement. Based on social capital and social closure theories, Coleman (34) systematically categorized parental involvement as family internal involvement and external involvement. This classification has gained widespread application due to its operability in empirical research. Coleman further noted that parental involvement is a comprehensive reflection of family and community social capital, affecting children’s development. The differences in the intergenerational transmission of SES often manifest in the quantity and quality of parental involvement. Parental involvement in youth sports, as a form of internal family participation, directly involves communication and interaction between parents and children. It is also influenced by SES. Parents’ decisions regarding which activities their children participate in and what material and cultural resources are available to them are typically determined by their SES (35, 36). Low SES may limit families’ opportunities to engage in physical activities due to a lack of transportation and financial resources (37). What’s more, the greater levels of cultural capital possessed by parents with high SES can effectively promote their children’s positive development (38–40) and engagement in extracurricular sports activities, as a way to accumulate cultural capital, may facilitate children’s future socioeconomic success (41). Parents with high SES may have a better understanding of the health benefits associated with physical activity (42) and thus they may be more inclined to participate in sports activities with their children.
Furthermore, some researchers have found that family SES can influence parents’ emotions, behaviors and parenting style (7, 43, 44). Parents with low-SES are more likely to have less psychological well-being compared to those from middle or high-SES backgrounds, which significantly predicts a low level of parental emotional warmth (45). This may lead to a lack of parental involvement in youth sports among adolescents from low SES families.
Parental involvement in youth sports is a unique link to the parenting process and its importance becomes more apparent. Multiple studies indicated that parental involvement in youth sports not only positively influences adolescents’ weight management but also has profound effects on their psychological well being. Niemeier et al. (46) conducted a systematic review and meta-analysis revealing that parental participation in weight-related health interventions significantly reduced the body mass index (BMI) of children and adolescents, and then this underscored the notable effectiveness of parental involvement in youth sports for adolescents’ weight control and obesity prevention. Additionally, research by Babkes and Weiss (47) highlighted that parental involvement in youth sports could elicit more positive psychosocial responses in children. The positive correlation between parental involvement in youth sports and adolescents’ levels of physical activity (PA) has also been substantiated (48). Verloigne et al. (49) found in their systematic review that family correlates with adolescents’ energy balance-related behaviors, and parental involvement in youth sports is identified as the most important, positive correlates of physical activity.
High levels of PA have been widely proven to have comprehensive positive impacts on adolescents’ health, including reduced risk of cardiovascular diseases and improved physical fitness (50). Further research by Ghekiere et al. (51) involving 919 Australian children aged 10–12 showed that parental accompaniment when walking or cycling was significantly positively associated with the frequency of children’s walking or cycling trips each week. Furusa et al. (52) found that parents can influence children’s enjoyment of their sporting experience through parents’ active engagement with their child in sports. These findings suggested that parental involvement in youth sports not only directly encouraged children’s participation in physical activities but also laid a solid foundation for long-term health.
In summary, family socioeconomic status is related to adolescents’ physical health and mental health, and also has an important influence on parental involvement in youth sports. Parental involvement in youth sports has a positive impact on improving adolescents’ physical and mental health. Currently, research on parental involvement in youth sports is still limited, and there are few studies that explore the relationship among family socioeconomic status, parental involvement in youth sports, and health together. This study utilizes data from the China Education Panel Survey (CEPS) to examine the relationships among adolescents’ family socioeconomic status, parental involvement in youth sports, and levels of adolescents’ physical health and mental health, aiming to further clarify the role of parental involvement in youth sports in the process by which family socioeconomic status influences adolescent health. Therefore, this study proposes the following hypotheses:
H1: Family socioeconomic status has a positive impact on different dimensions of adolescent health.
H2: Parental involvement in youth sports is a mediating variable linking family socioeconomic status and adolescent health; family socioeconomic status promotes adolescent health by increasing parental involvement in youth sports.
This study utilizes data from the baseline survey of the China Education Panel Survey (CEPS) conducted in 2013–2014. The survey was designed and implemented by the National Survey Research Center (NSRC) at Renmin University of China. It is the first large-scale, nationally representative tracking survey project in China that starts from the junior high school stage. In 2013, the CEPS adopted a stratified, multi-stage probability proportional to size (PPS) sampling method. A total of 112 schools and 438 classes were surveyed nationwide, with all students in the selected classes included in the sample. The baseline survey collected data from approximately 20,000 samples. The CEPS database contains relevant information on students’ gender, family socioeconomic status, self-reported physical health, psychological health test items, and parental involvement in physical activities with their children, which are essential for addressing the core questions of this research. After deleting samples with missing values and outliers related to the core variables, a sample of 11,003 students was retained for empirical analysis.
The CEPS questionnaire includes three items to measure adolescents’ physical health: “How would you rate your current overall health? Very poor, Poor, Average, Good, Excellent; How would you rate your child’s current health? Very poor, Poor, Average, Good, Excellent; Compared to your peers, how do you rate your current health? Significantly unhealthy, Less unhealthy, Average, Healthier, Significantly healthy.” The values of 1–5 were assigned to the responses, of which 1 represented the poorest and 5 represented the best. Physical health was measured by the three questions. Lundberg et al. conducted a reliability test for self-evaluated health, validating self-evaluated health against a range of other health issues and then self-evaluated health demonstrated good overall reliability (53). Previous studies suggested that self-evaluated health is a subjective report indicator with high reliability (54, 55). We measured adolescents’ physical health using the question: “How would you rate your current overall health?” Additionally, upon examining the sample data, we identified cases where self-rated health and parent-rated health showed significant discrepancies. To accurately reflect the true health status of the respondents and identify potential outliers in the differences between self-assessment and parental assessment, we calculated the Z-scores of these differences. Among the 12,138 samples, a total of 1,135 observations had Z-scores exceeding ±2 standard deviations and were flagged as outliers, as illustrated in Figure 1. Sensitivity analysis confirmed that excluding these outliers did not significantly alter our main results.
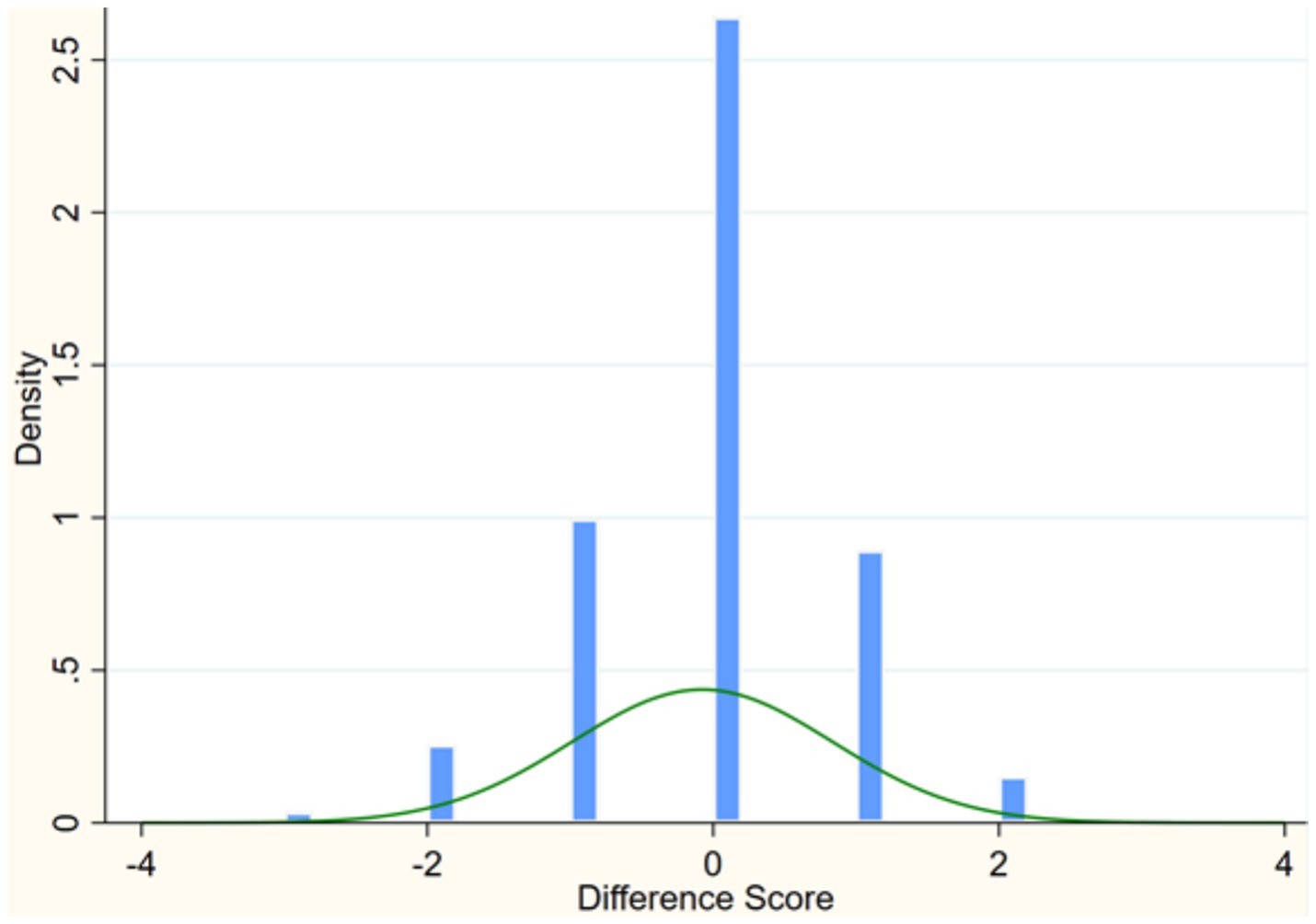
Figure 1. Discrepancies between self-rated health and parent-rated health.
The CEPS questionnaire set mental health scale, consisting of five items: “In the past seven days, did you have the following feelings: sadness, depression, unhappiness, a sense of life being meaningless and grief?” The values of 1–5 were assigned to “Always, Often, Sometimes, Seldom and Never” respectively. Mental health was measured by the five questions. The reliability coefficient (a) for the mental health scale was 0.85, and it has been employed in studies regarding the mental health of Chinese adolescents (56). The summary description of the dependent variables is provided in Table 1.
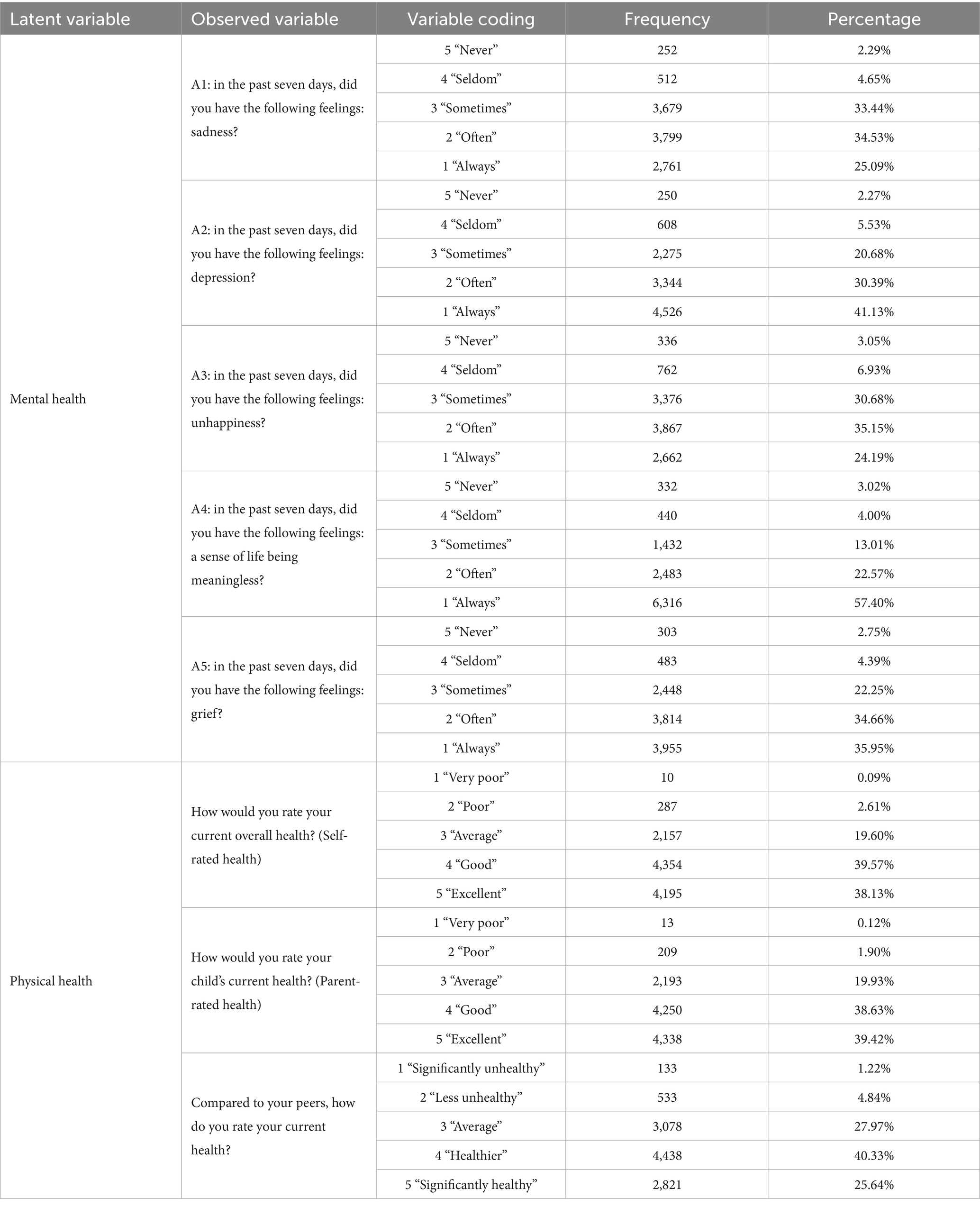
Table 1. The descriptive statistics of the dependent variables.
The independent variable, Family Socioeconomic Status, was a latent variable in this study, typically measured by indicators such as parental occupation, education level, and family income (57). However, some researchers argued that measuring family income was difficult in the context of Chinese households and suggested that it can be omitted, as occupation and education level adequately reflected a family’s socioeconomic status (58). Furthermore, the CEPS database lacked objective and direct information regarding family economic conditions (e.g., annual income, annual expenditure). The CEPS questionnaire included questions related to parental education level and occupation, specifically: “What does your mother do for work?” and “What does your father do for work?” as well as the educational levels of the student’s father and mother. Therefore, this study used the father’s occupation, mother’s occupation, father’s education level, and mother’s education level as observed variables to measure family socioeconomic status. The basic description of the independent variables was presented in Table 2.
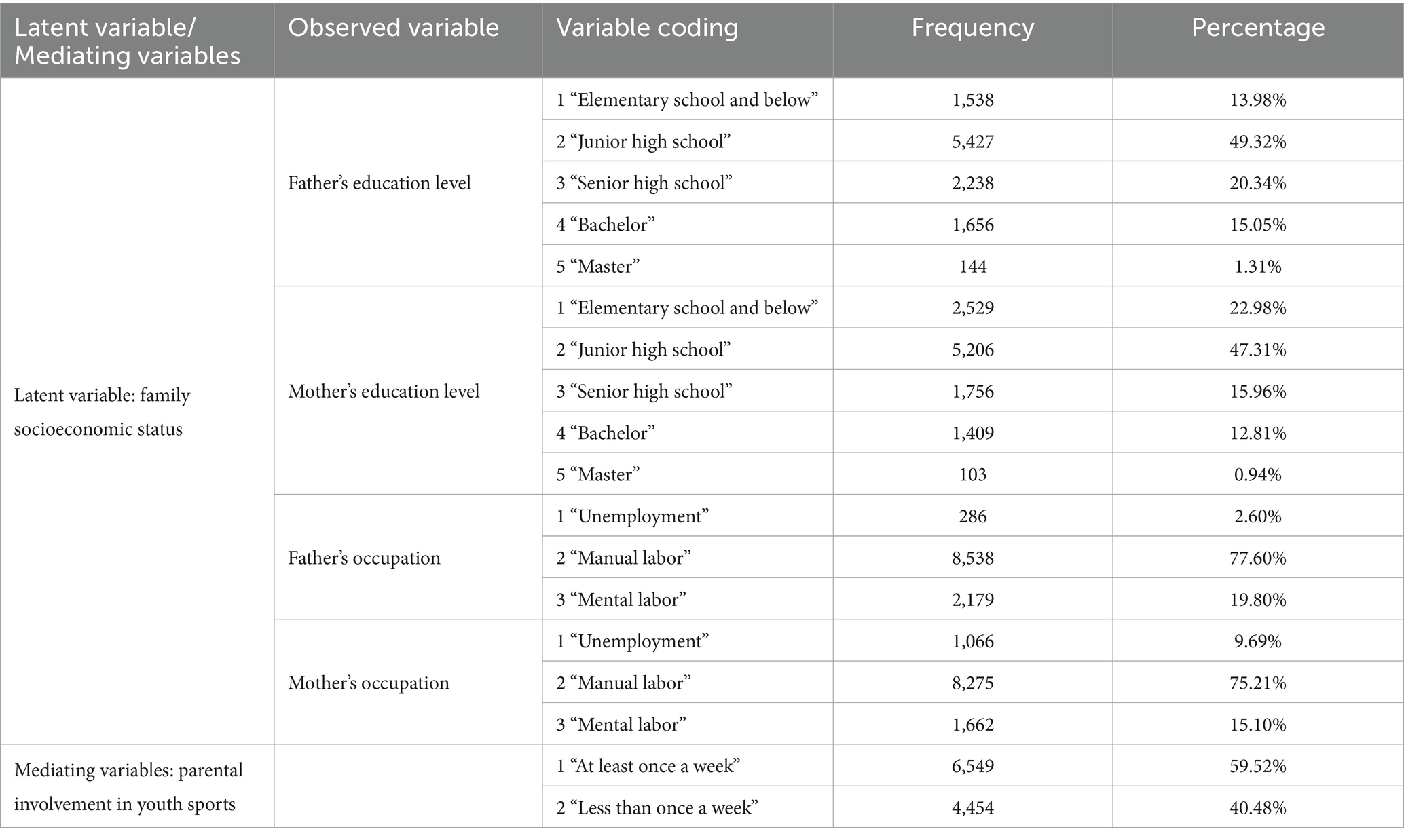
Table 2. The descriptive statistics of the independent variables and mediating variables.
The occupation variable was reclassified and reassigned based on existing research, categorizing occupations as follows: (1) Unemployment: including joblessness and layoff; (2) Manual labor: including farmers, skilled workers, drivers, general employees, and self-employed individuals; (3) Mental labor: including leaders and staff of government agencies and public institutions, senior and mid-level leaders in enterprises/companies, teachers, engineers, doctors, and lawyers, with values assigned sequentially from 1 to 3.
Based on their academic qualifications, parents’ education levels were categorized into five levels: elementary school and below, junior high school, senior high school, bachelor, master and above, with values assigned sequentially from 1 to 5.
Parental Involvement in Youth Sports was measured by the question: “Frequency of doing the following activities with your parents – exercising.” The responses included six options: “1 = never”; “2 = once a year”; “3 = once every six months”; “4 = once a month”; “5 = once a week”; “6 = more than once a week.” In this study, the options “once a week” and “more than once a week” were combined and revalued as “at least once a week” (assigned a value of 2), while the other options are combined and revalued as “less than once a week” (assigned a value of 1). The basic description of the control variables was presented in Table 2.
To validate the research hypotheses proposed in this study, we employed structural equation modeling (SEM) using Stata 16.0 statistical software. SEM is a statistical method for exploring the relationships and structures between theories and concepts, integrating ideas and techniques from factor analysis, path analysis, and multiple linear regression analysis. This study utilized two sets of structural equation models: the baseline model and the mediation model. First, the baseline model established a direct path effect between family socioeconomic status and adolescent health to test Hypothesis 1. Second, the mediation model added the mediating variable of parental involvement in youth sports to the baseline model, examining the path effects among family socioeconomic status, parental involvement in youth sports, and adolescent health to test Hypothesis 2. The theoretical model for this study was constructed based on existing literature and the research hypotheses. The theoretical framework of the study was illustrated in Figure 2.

Figure 2. Theoretical model. The arrows represent the impact paths.
Additionally, a model deemed satisfactory should meet a set of criteria. A standardized root mean square residual (SRMR) value of 0.000 indicates a perfect model-data fit, while a value below 0.08 was considered acceptable. Regarding parsimony correction indices, the root meant square error of approximation (RMSEA) is viewed as an “approximate error” index. An RMSEA estimate and its corresponding 90% confidence interval below 0.10 suggested a good model-data fit. For comparative fit indices, the comparative fit index (CFI) ranged from 0.000 to 1.000, with values closer to 1.000 indicating a better model-data fit (59).
Since the ML estimator is unbiased and consistent under large sample conditions and was the most commonly used estimation method in structural equation modeling, this study employed the maximum likelihood estimation method for model testing. The measurement models of the latent variables SES and physical health demonstrated good reliability and validity (CR for mental health = 0.855 > 0.7, AVE = 0.543 > 0.5, √AVE = 0.736 > 0.05; CR for SES = 0.716 > 0.7, AVE = 0.450, √AVE = 0.670 > 0.153. Although the AVE value for SES was slightly below the ideal threshold of 0.5, previous research had emphasized that all four indicators were crucial for measuring family socioeconomic status. This discrepancy may be attributed to the absence of a key variable for family socioeconomic status in the database. However, the composite reliability (CR) and discriminant validity (√AVE) of SES met the required thresholds. Therefore, despite the slightly lower AVE, we considered the results acceptable.) The fit indices, including RMSEA and CFI, for the baseline model were presented in Table 3. The baseline model analysis indicated that family socioeconomic status significantly affected adolescent health, with unstandardized path coefficients of 0.407 for mental health and 0.274 for physical health, both positive and statistically significant at the p < 0.01 level. These findings confirmed that family socioeconomic status positively influenced adolescent health, with the strongest effect on physical health, supporting Hypothesis 1. Furthermore, within the measurement model of family socioeconomic status, mother’s education level (0.798) exhibited the highest factor loading, followed by father’s education level (0.793). The factor loading for father’s occupation is 0.549, while mother’s occupation had the lowest factor loading (0.479).
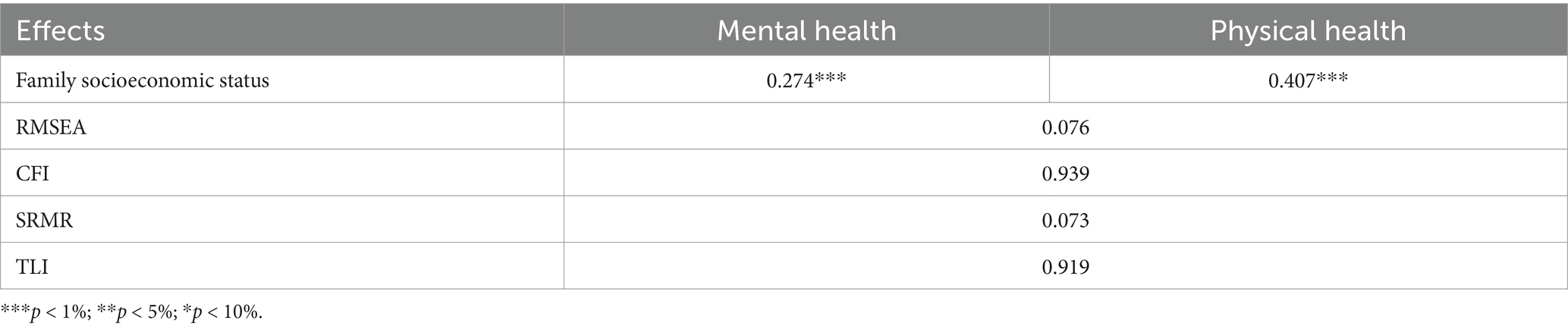
Table 3. The structural equation modeling testing of the relationship between family socioeconomic status and adolescent health.
To explore the mediating effects of parental involvement in youth sports, the mediating variable “parental involvement in youth sports” was added to the baseline model, resulting in the establishment of a mediating model. We again employed the maximum likelihood estimation method for testing, and the analysis results of the mediating model were presented in Table 4. In the mediating model, family socioeconomic status significantly impacted both parental involvement in youth sports and adolescent health and the unstandardized path coefficients for parental involvement in youth sports, mental health and physical health are all positive and significant at the p < 0.01 level. Furthermore, the unstandardized path coefficients for the mediating variable parental involvement in youth sports with mental health and physical health were also positive and significant at the same level. Notably, the unstandardized path coefficient between parental involvement in youth sports and adolescent mental health was higher than that for physical health.
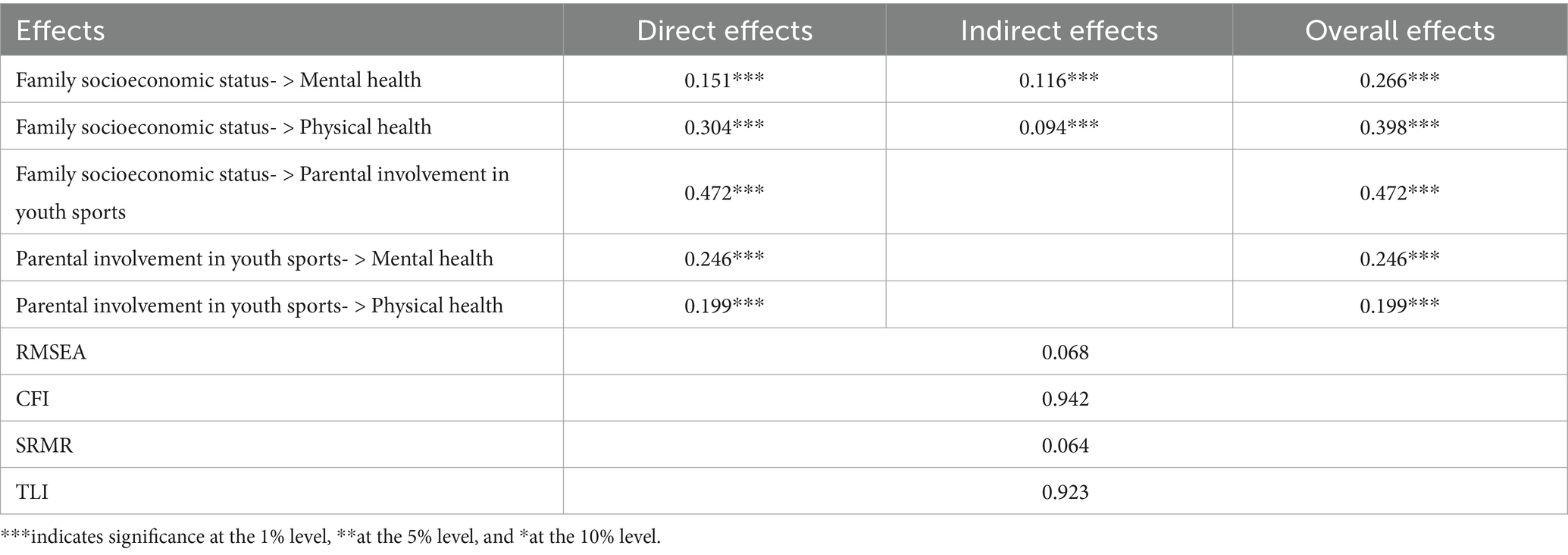
Table 4. The structural equation modeling testing of the mediating role of parental involvement in youth sports.
Thus, the mediating model revealed that parental involvement in youth sports played an important role in the process in which family socioeconomic status affected adolescent health. Family socioeconomic status positively influenced parental involvement in youth sports, which in turn positively impacted adolescent health. Therefore, family socioeconomic status indirectly influenced adolescent health by affecting parental involvement in youth sports, confirming Hypothesis 2.
To better illustrate the impact of the mediating variable, Figures 3, 4 presented the paths of the baseline model and the mediating model, respectively. The examination results indicated that multiple fit indices for both models generally met the standards, achieving acceptable levels of fit.
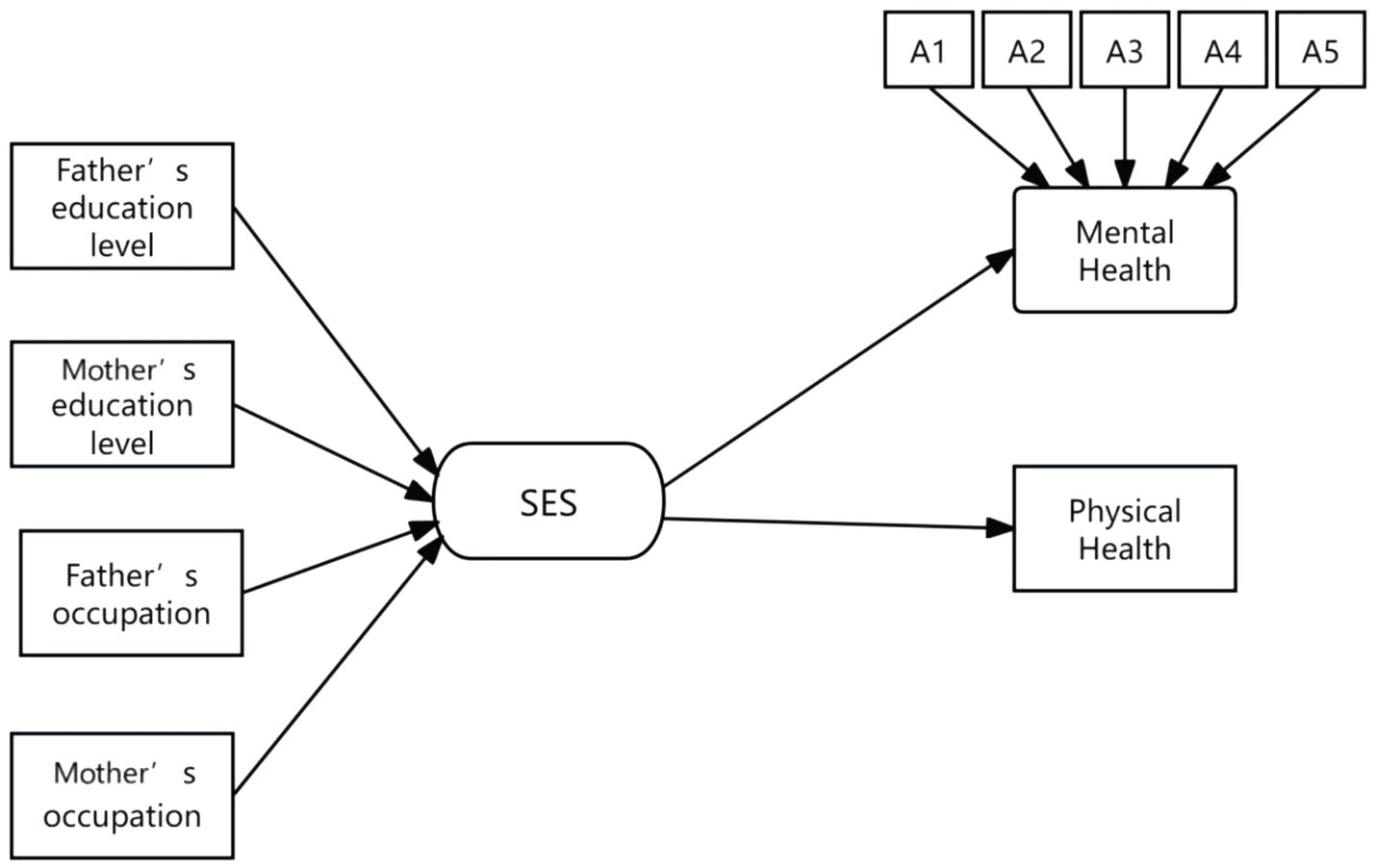
Figure 3. The path of the baseline model. The arrows represent the impact paths; A1 represents: in the past seven days, did you have the following feelings: sadness?; A2: in the past seven days, did you have the following feelings: depression?; A3: in the past seven days, did you have the following feelings: unhappiness?; A4: in the past seven days, did you have the following feelings: a sense of life being meaningless?; A5: in the past seven days, did you have the following feelings: grief?
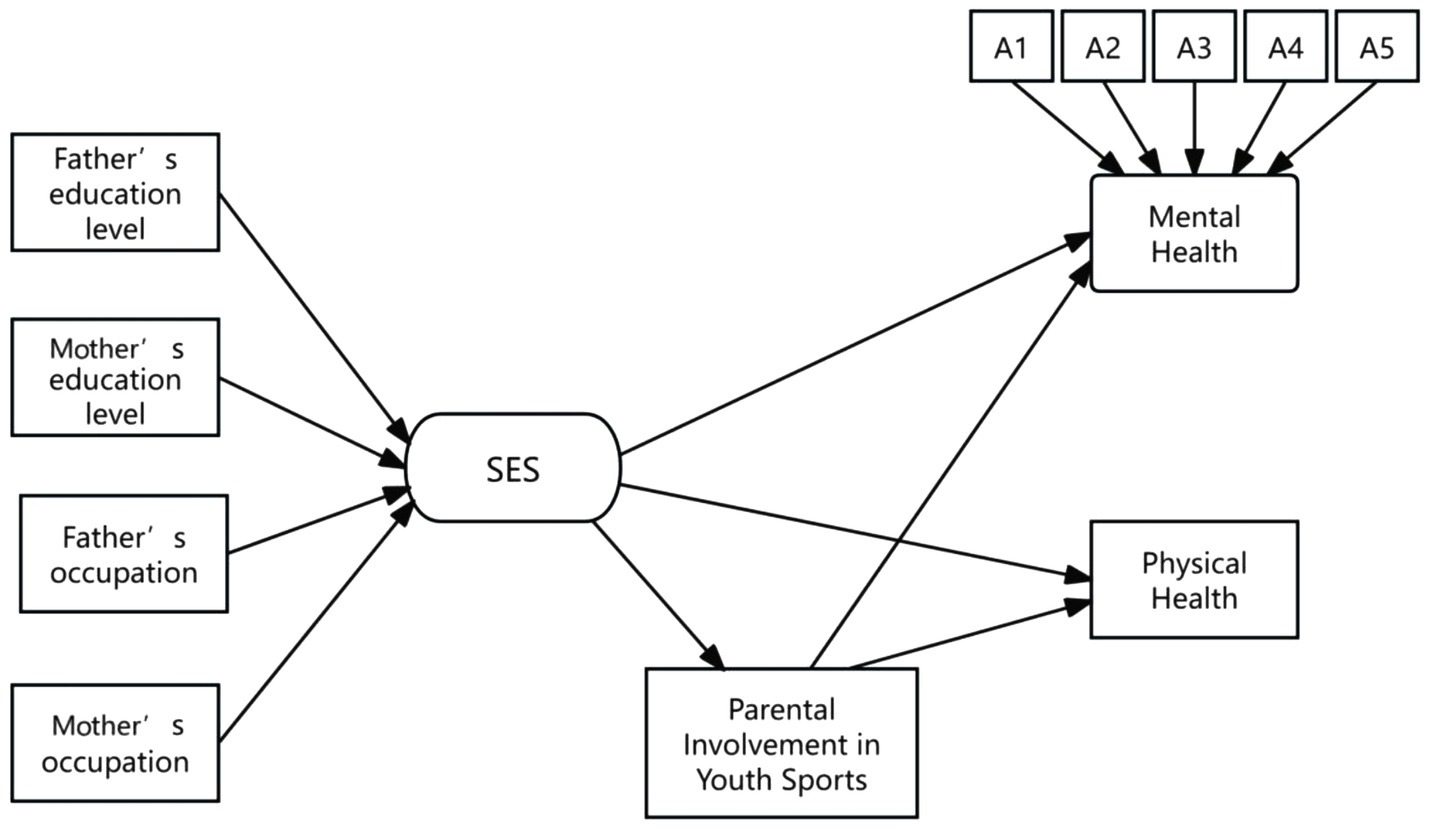
Figure 4. The SEM of the mediating role of parental involvement in youth sports. The arrows represent the impact paths; A1 represents: in the past seven days, did you have the following feelings: sadness?; A2: in the past seven days, did you have the following feelings: depression?; A3: in the past seven days, did you have the following feelings: unhappiness?; A4: in the past seven days, did you have the following feelings: a sense of life being meaningless?; A5: in the past seven days, did you have the following feelings: grief?
Based on the path models in Figures 3, 4, two main findings can be summarized. First, the data analysis confirmed the significant role of socioeconomic status (SES) in adolescent physical and mental health. Specifically, as family SES increases, adolescents tended to exhibit better psychological and physical health. Second, the study provided empirical evidence for the mediating role of parental involvement in youth sports. More specifically, parental involvement in youth sports served as a crucial mediating variable between family SES and adolescent physical and mental health, indicating that SES influences adolescent health partly through the frequency of parental involvement in youth sports. The data further showed that higher SES families tended to have more frequent parental involvement in youth sports, and compared to adolescents who lack such companionship, those whose parents accompanied them in sports activities at least once a week experienced significant improvements in both physical and mental health. It plays a particularly important role in adolescent mental health.
Through the exploration of family socioeconomic status, adolescent health, and parental involvement in youth sports, we found that family socioeconomic status could positively predict the health levels of adolescents and adolescents from families with high socioeconomic status showed significantly better health compared to those from low socioeconomic status families. This finding aligned with numerous existing studies that there is a critical role of family socioeconomic status during adolescence (4, 6, 60). Research has shown that the family sports environment is a key determinant of adolescents’ regular participation in sports (39, 61). Adolescents are less likely to engage in physical activities if their parents are inactive (12, 62). Further research indicated that parents from high-SES families typically had a stronger awareness of health (63) and greater flexibility in both time and finances (64), making them more likely to engage in physical activities with their children.
The findings highlighted the crucial mediating role of parental involvement in youth sports between socioeconomic status and adolescent health. Adolescents in China rarely engaged in sports activities with their parents, particularly those from low socioeconomic backgrounds, where parental participation was notably low. Our study introduced the hypothesis that parental involvement in youth sports acted as a mediating variable and empirically tested this hypothesis. This aligned with prior literature and filled a gap, particularly regarding the role of parental involvement in youth sports in mitigating health disparities among adolescents from low-SES backgrounds. Heradstveit (65) suggested that several indicators of parental socioeconomic status, including family economic welfare and parental education levels, were related to a lack of physical activity among adolescents. Previous research has primarily focused on the role of economic resources (10, 37), whereas this study revealed the mediating role of the sociocultural attributes of parental involvement in youth sports. Therefore, encouraging a supportive family sports environment is essential, especially for parents from low socioeconomic backgrounds, to enhance adolescent health.
The influence of SES on adolescent sports participation shows consistency across countries and cultures. In developed countries such as the United States, Norway, and Northern Europe, adolescents from high-SES families are more inclined to engage in organized sports (66, 67). For example, a research from Germany indicated that Children and adolescents with a high SES spent much more time on PA in organized sports (155 min) than children with a low SES (99 min) and low parental SES correlates with more access for children and adolescents to participation in unorganized sports (37). Generally, participation in organized sports is associated with positive developmental outcomes (67–69). Parents are significant others influencing adolescents’ participation in sports. A Danish longitudinal study demonstrated that parental involvement in children’s sport increased the likelihood that the child participated in organized sports, categorizing parents into four types: unengaged, servicing, self-realization, and super parents (70). However, the study also found that involvement from disadvantaged parents boosted children’s participation in organized sports, whereas involvement from advantaged parents had the opposite effect (70). Research from Hungary indicated that there was a positive interrelation between parental involvement in youth sports and sports performance of their children (71). The findings of this study are not only applicable to China but may also be relevant to other developed countries and middle-income countries.
Additionally, economic development is often associated with higher incomes, better education, and improved healthcare, allowing high-SES families to offer their children superior resources in areas such as nutrition, medical care, sports, and education. However, substantial socioeconomic disparities persist across urban and rural areas, regions, and different income groups, leading to significant heterogeneity in the impact of SES on health (72, 73). Parental involvement in youth sports not only directly benefits adolescent health but also helps reduce health disparities caused by SES, providing valuable insights for policies aimed at improving adolescent health.
Despite the findings indicating the mediating role of parental involvement in youth sports, the study did not delve deeper into the differences among various social groups, such as urban versus rural populations, regional variations, and gender differences, due to space limitations. These issues could constitute a relatively independent study requiring detailed theoretical exploration and data analysis. Furthermore, parental involvement in youth sports is an important yet under-researched concept that merits further investigation by scholars. Given the diverse ways of engaging in sports, parental involvement is not limited to traditional activities. With the rapid development of the global economy, sports are increasingly capturing market share and attracting more people to join in sports consumption and physical activities. Younger generations master more kinds of sports than their parents, raising questions about how these new parents will accompany their children in sports activities, which forms of parental sports involvement will be more appealing to children, and how effective these forms will be for health promotion, and parents from different countries and regions are inclined to which forms of parental sports involvement. Future research could analyze parental involvement in youth sports by using samples from various countries, further enriching the theoretical understanding of this topic.
Addressing the developmental disparities of children from low socioeconomic status families is crucial for promoting health equity and educational balance in China. Policymakers should recognize the underlying mechanisms through which family socioeconomic status influences children’s academic outcomes and consider compensatory policies for children from low socioeconomic backgrounds. Providing educational resources to children from low socioeconomic families can help mitigate the effects of class stratification. Existing research indicated that compared to parents from high socioeconomic backgrounds, parents with low socioeconomic status demonstrated higher effectiveness in involving in their children’s school education (74). In addition to ensuring fairness in traditional educational systems, current inequalities in family education also need attention. The important role of parental involvement in youth sports highlights potential health risk factors for adolescents.
Parents from different socioeconomic backgrounds should adopt varying strategies for sports companionship. Parents from lower socioeconomic backgrounds should particularly pay more attention to developing skills for parent–child interaction to enhance the quality of their participation in youth sports. The study’s findings reveal ed. that parents from high socioeconomic backgrounds generally have a higher frequency of parental involvement in youth sports than those from low backgrounds. This underscores the need for parents at all socioeconomic levels to prioritize spending time and energy on strengthening communication with their children. Additionally, parents should seek to improve their own sports skills and communication abilities, thereby enhancing the effects of parent–child interactions.
This study, based on CEPS data and employing Stata 16.0 software, used structural equation modeling to examine the intrinsic connections between family socioeconomic status, parental involvement in youth sports, and adolescent health. The results demonstrated that family socioeconomic status had a positive influence on both adolescent physical and mental health, and the frequency of parental involvement in youth sports, it plays a particularly important role in adolescent mental health. Specifically, family socioeconomic status indirectly affected adolescent physical and mental health by influencing the frequency of parental involvement in youth sports, confirming the existence of a mediating effect. Effective parental involvement in youth sports plays a positive role in adolescent physical and mental health. In summary, families with high socioeconomic status were more likely to actively engage in sports activities with their children, leading to improved health outcomes for the children.
Publicly available datasets were analyzed in this study. This data can be found at: http://ceps.ruc.edu.cn/.
Ethical approval was not required for the studies involving humans because the current study is waived from ethical approval. The study is based on the secondary dataset China Education Panel Survey (CEPS). The original data was collected by the National Survey Research Center (NSRC) at Renmin University of China. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements because the consent to participate was obtained by the National Survey Research Center (NSRC) at Renmin University of China.
WY: Writing – original draft, Writing – review & editing. ZX: Funding acquisition, Methodology, Writing – review & editing. HH: Data curation, Formal analysis, Validation, Writing – review & editing. HZ: Software, Visualization, Writing – review & editing. XZ: Visualization, Writing – review & editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This study was supported by the National Social Science Fund in China (grant number 22XTY009).
We express our gratitude to the National Survey Research Center (NSRC) at Renmin University of China for generously sharing their data, as well as the participants who made this study possible.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declare that no Gen AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Braveman, PA, Cubbin, C, Egerter, S, Williams, DR, and Pamuk, E. Socioeconomic disparities in health in the United States: what the patterns tell us. Am J Public Health. (2010) 100:S186–96. doi: 10.2105/AJPH.2009.166082
2. Bradley, RH, and Corwyn, RF. Socioeconomic status and child development. Annu Rev Psychol. (2002) 53:371–99. doi: 10.1146/annurev.psych.53.100901.135233
3. World Health Organization. A conceptual framework for action on the social determinants of health. World Health Organization. (2010).
4. Dennis, E, Manza, P, and Volkow, ND. Socioeconomic status, BMI, and brain development in children. Transl Psychiatry. (2022) 12:33. doi: 10.1038/s41398-022-01779-3
5. Barnett, K, Mercer, SW, Norbury, M, Watt, G, Wyke, S, and Guthrie, B. Epidemiology of multimorbidity and implications for health care, research, and medical education: a cross-sectional study. Lancet. (2012) 380:37–43. doi: 10.1016/S0140-6736(12)60240-2
6. Peverill, M, Dirks, MA, Narvaja, T, Herts, KL, Comer, JS, and McLaughlin, KA. Socioeconomic status and child psychopathology in the United States: a meta-analysis of population-based studies. Clin Psychol Rev. (2021) 83:101933. doi: 10.1016/j.cpr.2020.101933
7. Hoff, E, and Laursen, B. Socioeconomic status and parenting. In Bornstein MH. editor. Handbook of parenting. Routledge. (2019):421–47. doi: 10.4324/9780429401459-13
8. Kennewell, E, Curtis, RG, Maher, C, Luddy, S, and Virgara, R. The relationships between school children's wellbeing, socio-economic disadvantage and after-school activities: a cross-sectional study. BMC Pediatr. (2022) 22:297. doi: 10.1186/s12887-022-03322-1
9. Jury, M, Smeding, A, Stephens, NM, Nelson, JE, Aelenei, C, and Darnon, C. The experience of low-SES students in higher education: psychological barriers to success and interventions to reduce social-class inequality. J Soc Issues. (2017) 73:23–41. doi: 10.1111/josi.12202
10. Xia, M, Penghui, H, and Zhou, Y. How parental socioeconomic status contribute to children's sports participation in China: a cross-sectional study. J Community Psychol. (2020) 48:2625–43. doi: 10.1002/jcop.22439
11. Li, D, and Guo, X. The effect of the time parents spend with children on children's well-being. Front Psychol. (2023) 14:1096128. doi: 10.3389/fpsyg.2023.1096128
12. Doggui, R, Gallant, F, and Bélanger, M. Parental control and support for physical activity predict adolescents’ moderate to vigorous physical activity over five years. Int J Behav Nutr Phys Act. (2021) 18:1–10. doi: 10.1186/s12966-021-01107-w
13. Lee, E-J, So, W-Y, Youn, H-S, and Kim, J. Effects of school-based physical activity programs on health-related physical fitness of korean adolescents: a preliminary study. Int J Environ Res Public Health. (2021) 18:2976. doi: 10.3390/ijerph18062976
14. Pyper, E, Harrington, D, and Manson, H. The impact of different types of parental support behaviours on child physical activity, healthy eating, and screen time: a cross-sectional study. BMC Public Health. (2016) 16:1–15. doi: 10.1186/s12889-016-3245-0
15. Badura, P, Geckova, AM, Sigmundova, D, van Dijk, JP, and Reijneveld, SA. When children play, they feel better: organized activity participation and health in adolescents. BMC Public Health. (2015) 15:1–8. doi: 10.1186/s12889-015-2427-5
16. Chen, P, Wang, D, Shen, H, Yu, L, Gao, Q, Mao, L, et al. Physical activity and health in Chinese children and adolescents: expert consensus statement (2020). Br J Sports Med. (2020) 54:1321–31. doi: 10.1136/bjsports-2020-102261
17. Kuhn, AW, Grusky, AZ, Cash, CR, Churchwell, AL, and Diamond, AB. Disparities and inequities in youth sports. Curr Sports Med Rep. (2021) 20:494–8. doi: 10.1249/JSR.0000000000000881
18. Mueller, CW, and Parcel, TL. Measures of socioeconomic status: alternatives and recommendations. Child Dev. (1981) 52:13–30. doi: 10.2307/1129211
19. Cockerham, WC. “Health lifestyles: bringing structure back”. In Cockerham WC, editor. The New Blackwell Companion to Medical Sociology. Wiley Blackwell. (2021):150–70. doi: 10.1002/9781119633808.ch8
20. Dahl, E. Social mobility and health: cause or effect? BMJ. (1996) 313:435–6. doi: 10.1136/bmj.313.7055.435
21. Lumme, S, Manderbacka, K, Karvonen, S, and Keskimäki, I. Trends of socioeconomic equality in mortality amenable to healthcare and health policy in 1992–2013 in Finland: a population-based register study. BMJ Open. (2018) 8:e023680. doi: 10.1136/bmjopen-2018-023680
22. Weber, M. Class status and power In: H Gerth and CW Mills, editors. From max Weber: Essays in sociology. New York: Oxford University Press (1946)
23. Verropoulou, G, and Zakynthinou, M. Contrasting concurrent and childhood socioeconomic predictors of self-rated health among older European men and women. J Biosoc Sci. (2017) 49:478–97. doi: 10.1017/S0021932016000250
24. Link, BG, and Phelan, J. Social conditions as fundamental causes of disease. J Health Soc Behav. (1995) 35:80–94. doi: 10.2307/2626958
25. Poulain, T, Vogel, M, and Kiess, W. Review on the role of socioeconomic status in child health and development. Curr Opin Pediatr. (2020) 32:308–14. doi: 10.1097/MOP.0000000000000876
26. Torsheim, T, Nygren, JM, Rasmussen, M, Arnarsson, AM, Bendtsen, P, Schnohr, CW, et al. Social inequalities in self-rated health: a comparative cross-national study among 32,560 Nordic adolescents. Scand J Public Health. (2018) 46:150–6. doi: 10.1177/1403494817734733
27. Yang, D, Hu, S, and Li, M. The influence of family socioeconomic status on adolescents’ mental health in China. Int J Environ Res Public Health. (2022) 19:7824. doi: 10.3390/ijerph19137824
28. Ibrahim, AK, Kelly, SJ, Adams, CE, and Glazebrook, C. A systematic review of studies of depression prevalence in university students. J Psychiatr Res. (2013) 47:391–400. doi: 10.1016/j.jpsychires.2012.11.015
29. Cao, M, Tian, Y, Lian, S, Yang, X, and Zhou, Z. Family socioeconomic status and adolescent depressive symptoms: a moderated mediation model. J Child Fam Stud. (2021) 30:2652–63. doi: 10.1007/s10826-021-02068-1
30. Zou, R, Xu, X, Hong, X, and Yuan, J. Higher socioeconomic status predicts less risk of depression in adolescence: serial mediating roles of social support and optimism. Front Psychol. (2020) 11:1955. doi: 10.3389/fpsyg.2020.01955
31. Jeon, GS, Ha, Y, and Choi, E. Effects of objective and subjective socioeconomic status on self-rated health, depressive symptoms, and suicidal ideation in adolescents. Child Indic Res. (2013) 6:479–92. doi: 10.1007/s12187-013-9180-z
32. Angoorani, P, Mahmoodi, Z, Ejtahed, H-S, Heshmat, R, Motlagh, ME, Qorbani, M, et al. Determinants of life satisfaction and self-rated health in Iranian children and adolescents: a structure equation model. BMC Pediatr. (2022) 22:1–10. doi: 10.1186/s12887-021-03044-w
33. Bronfenbrenner, U. Contexts of child rearing: problems and prospects. Am Psychol. (1979) 34:844–50. doi: 10.1037/0003-066X.34.10.844
34. Coleman, JS. Social capital in the creation of human capital. Am J Sociol. (1988) 94:S95–S120. doi: 10.1086/228943
35. Welk, GJ, Wood, K, and Morss, G. Parental influences on physical activity in children: an exploration of potential mechanisms. Pediatr Exerc Sci. (2003) 15:19–33. doi: 10.1123/pes.15.1.19
36. De León Marcos, Á, Rivera Navarro, J, Cereijo Tejedor, L, and Tejero, MF. Physical activity inequalities in adolescents from areas of different socioeconomic status. J Phys Act Health. (2024) 1:1–8. doi: 10.1123/jpah.2024-0521
37. Rittsteiger, L, Hinz, T, Oriwol, D, Wäsche, H, Santos-Hövener, C, and Woll, A. Sports participation of children and adolescents in Germany: disentangling the influence of parental socioeconomic status. BMC Public Health. (2021) 21:1–17. doi: 10.1186/s12889-021-11284-9
38. McNeal, RB Jr. Parental involvement as social capital: differential effectiveness on science achievement, truancy, and dropping out. Soc Forces. (1999) 78:117–44. doi: 10.1093/sf/78.1.117
39. Kovács, K, and Pusztai, G. An empirical study of Bourdieu’s theory on capital and habitus in the sporting habits of higher education students learning in central and Eastern Europe. Sport Educ Soc. (2023) 29:496–510. doi: 10.1080/13573322.2022.2164266
40. Mollborn, S, Rigles, B, and Pace, JA. Healthier than just healthy”: families transmitting health as cultural capital. Soc Probl. (2021) 68:574–90. doi: 10.1093/socpro/spaa015
41. Tan, M, Cai, L, and Bodovski, K. An active investment in cultural capital: structured extracurricular activities and educational success in China. J Youth Stud. (2022) 25:1072–87. doi: 10.1080/13676261.2021.1939284
42. Stalsberg, R, and Pedersen, AV. Effects of socioeconomic status on the physical activity in adolescents: a systematic review of the evidence. Scand J Med Sci Sports. (2010) 20:368–83. doi: 10.1111/j.1600-0838.2009.01047.x
43. Conger, RD, Conger, KJ, Elder, GH Jr, Lorenz, FO, Simons, RL, and Whitbeck, LB. A family process model of economic hardship and adjustment of early adolescent boys. Child Dev. (1992) 63:526–41. doi: 10.2307/1131344
44. Conger, RD, Conger, KJ, and Martin, MJ. Socioeconomic status, family processes, and individual development. J Marriage Fam. (2010) 72:685–704. doi: 10.1111/j.1741-3737.2010.00725.x
45. Liu, G, Zhao, Z, Li, B, Pan, Y, and Cheng, G. Parental psychological well-being and parental emotional warmth as mediators of the relationship between family socioeconomic status and children’s life satisfaction. Curr Psychol. (2023) 42:23958–65. doi: 10.1007/s12144-022-03568-z
46. Niemeier, BS, Hektner, JM, and Enger, KB. Parent participation in weight-related health interventions for children and adolescents: a systematic review and meta-analysis. Prev Med. (2012) 55:3–13. doi: 10.1016/j.ypmed.2012.04.021
47. Babkes, ML, and Weiss, MR. Parental influence on children’s cognitive and affective responses to competitive soccer participation. Pediatr Exerc Sci. (1999) 11:44–62. doi: 10.1123/pes.11.1.44
48. Eriksen, IM, and Stefansen, K. What are youth sports for? Youth sports parenting in working-class communities. Sport Educ Soc. (2022) 27:592–603. doi: 10.1080/13573322.2021.1894114
49. Verloigne, M, Van Lippevelde, W, Maes, L, Brug, J, and De Bourdeaudhuij, I. Family-and school-based correlates of energy balance-related behaviours in 10–12-year-old children: a systematic review within the ENERGY (EuropeaN Energy balance research to prevent excessive weight gain among youth) project. Public Health Nutr. (2021) 15:1380–95. doi: 10.1017/S1368980011003168
50. Vasconcellos, F, Seabra, A, Katzmarzyk, PT, Kraemer-Aguiar, LG, Bouskela, E, and Farinatti, P. Physical activity in overweight and obese adolescents: systematic review of the effects on physical fitness components and cardiovascular risk factors. Sports Med. (2014) 44:1139–52. doi: 10.1007/s40279-014-0193-7
51. Ghekiere, A, Carver, A, Veitch, J, Salmon, J, Deforche, B, and Timperio, A. Does parental accompaniment when walking or cycling moderate the association between physical neighbourhood environment and active transport among 10–12 year olds? J Sci Med Sport. (2016) 19:149–53. doi: 10.1016/j.jsams.2015.01.003
52. Furusa, MG, Knight, CJ, and Hill, DM. Parental involvement and children’s enjoyment in sport. Qual Res Sport, Exerc Health. (2021) 13:936–54. doi: 10.1080/2159676X.2020.1803393
53. Lundberg, O, and Manderbacka, K. Assessing reliability of a measure of self-rated health. Scand J Soc Med. (1996) 24:218–24. doi: 10.1177/140349489602400314
54. Mossey, JM, and Shapiro, E. Self-rated health: a predictor of mortality among the elderly. Am J Public Health. (1982) 72:800–8. doi: 10.2105/AJPH.72.8.800
55. Idler, EL, and Benyamini, Y. Self-rated health and mortality: a review of twenty-seven community studies. J Health Soc Behav. (1997) 38:21–37. doi: 10.2307/2955359
56. Yang, L, and Dai, Y-S. Will family social capital and school environment affect adolescent mental health? Empirical analysis based on CEPS data. China Youth Study. (2019) 1:47–56. doi: 10.19633/j.cnki.11-2579/d.2019.0007
57. Winkleby, MA, Jatulis, DE, Frank, E, and Fortmann, SP. Socioeconomic status and health: how education, income, and occupation contribute to risk factors for cardiovascular disease. Am J Public Health. (1992) 82:816–20. doi: 10.2105/AJPH.82.6.816
58. Z-X, SUN. The study on family socioeconomic status of academic failure. Tsinghua J Educ. (1999) 1:50–4.
59. Brown, TA. Confirmatory factor analysis for applied research. 2nd ed. New York, NY: The Guilford Press (2015).
60. Gallego, A, Olivares-Arancibia, J, Yáñez-Sepúlveda, R, Gutiérrez-Espinoza, H, and López-Gil, JF. Socioeconomic status and rate of poverty in overweight and obesity among Spanish children and adolescents. Children. (2024) 11:1020. doi: 10.3390/children11081020
61. Quarmby, T, and Dagkas, S. Children's engagement in leisure time physical activity: exploring family structure as a determinant. Leis Stud. (2010) 29:53–66. doi: 10.1080/02614360903242560
62. Sanz-Arazuri, E, Ponce-de-León-Elizondo, A, and Valdemoros-San-Emeterio, MÁ. Parental predictors of physical inactivity in Spanish adolescents. J Sports Sci Med. (2012) 11:95–101.
63. Bánfai-Csonka, H, Bánfai, B., Jeges, S., Gyebnár, B., and Betlehem, J.. Health literacy among participants from neighbourhoods with different socio-economic statuses in the southern region of Hungary: a pilot study. BMC Public Health. (2020) 20:1060. doi: 10.1186/s12889-020-08959-0
64. Andersen, PL, and Bakken, A. Social class differences in youths’ participation in organized sports: what are the mechanisms? Int Rev Sociol Sport. (2019) 54:921–37. doi: 10.1177/1012690218764626
65. Heradstveit, O, Haugland, S, Hysing, M, Stormark, KM, Sivertsen, B, and Bøe, T. Physical inactivity, non-participation in sports and socioeconomic status: a large population-based study among Norwegian adolescents. BMC Public Health. (2020) 20:1–9. doi: 10.1186/s12889-020-09141-2
66. Tandon, PS, Kroshus, E, Olsen, K, Garrett, K, Qu, P, and McCleery, J. Socioeconomic inequities in youth participation in physical activity and sports. Int J Environ Res Public Health. (2021) 18:6946. doi: 10.3390/ijerph18136946
67. Lagestad, P, Mikalsen, H, Ingulfsvann, LS, Lyngstad, I, and Sandvik, C. Associations of participation in organized sport and self-organized physical activity in relation to physical activity level among adolescents. Front Public Health. (2019) 7:129. doi: 10.3389/fpubh.2019.00129
68. Mooses, K, and Kull, M. The participation in organised sport doubles the odds of meeting physical activity recommendations in 7–12-year-old children. Eur J Sport Sci. (2020) 20:563–9. doi: 10.1080/17461391.2019.1645887
69. Panza, MJ, Graupensperger, S, Agans, JP, Doré, I, Vella, SA, and Evans, MB. Adolescent sport participation and symptoms of anxiety and depression: a systematic review and meta-analysis. J Sport Exerc Psychol. (2020) 42:201–18. doi: 10.1123/jsep.2019-0235
70. Qunito Romani, A. Parental behaviour and children’s sports participation: evidence from a Danish longitudinal school study. Sport Educ Soc. (2020) 25:332–47. doi: 10.1080/13573322.2019.1577235
71. Kovács, K, Oláh, ÁJ, and Pusztai, G. The role of parental involvement in academic and sports achievement. Heliyon. (2024) 10:e24290. doi: 10.1016/j.heliyon.2024.e24290
72. Buoncristiano, M, Williams, J, Simmonds, P, Nurk, E, Ahrens, W, Nardone, P, et al. Socioeconomic inequalities in overweight and obesity among 6-to 9-year-old children in 24 countries from the World Health Organization European region. Obes Rev. (2021) 22:e13213. doi: 10.1111/obr.13213
73. Ekholuenetale, M, Tudeme, G, Onikan, A, and Ekholuenetale, CE. Socioeconomic inequalities in hidden hunger, undernutrition, and overweight among under-five children in 35 sub-Saharan Africa countries. J Egypt Public Health Assoc. (2020) 95:1–15. doi: 10.1186/s42506-019-0034-5
Keywords: family socioeconomic status, adolescents’ physical health, adolescents’ mental health, parental involvement in youth sports, the mediating role
Citation: Yang W, Xiang Z, Hu H, Zheng H and Zhao X (2025) The impact of family socioeconomic status on adolescent mental and physical health: the mediating role of parental involvement in youth sports. Front. Public Health. 13:1540968. doi: 10.3389/fpubh.2025.1540968
Edited by:
Daniel Robert Neuspiel, Atrium Healthcare, United StatesReviewed by:
Jingyi Tan, Lundquist Institute for Biomedical Innovation, United StatesCopyright © 2025 Yang, Xiang, Hu, Zheng and Zhao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zubing Xiang, eHpiQGNxdS5lZHUuY24=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.