
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 18 March 2025
Sec. Public Health Education and Promotion
Volume 13 - 2025 | https://doi.org/10.3389/fpubh.2025.1534731
 Katijah Khoza-Shangase*†
Katijah Khoza-Shangase*† Khothatso Mokhethi†
Khothatso Mokhethi†Background: Recreational noise-induced hearing loss (NIHL) is an increasing public health concern among young adults who frequently use personal listening devices (PLDs) at high volumes for extended periods. Despite this, awareness of NIHL risks remains low, particularly among university students in South Africa.
Objective: This study aimed to assess undergraduate students’ awareness of recreational NIHL, examining their earphone use habits, volume preferences, preventive behaviors, and associations between demographic variables and NIHL awareness.
Methods: A cross-sectional survey was conducted with 154 undergraduate students at a large urban South African university. Quantitative data on listening habits, NIHL awareness, and preventive behaviors were collected and analysed using descriptive including thematic analysis and inferential statistics such as Chi-square tests to examine associations between variables.
Results: Most participants (67.5%) reported daily earphone use, often at moderate (48.1%) or high (33.8%) volumes. Awareness of NIHL was low, with only 9.7% of students feeling very informed. Inferential analysis revealed significant associations between NIHL awareness and age (χ2 = 12.67, p < 0.05), as well as year of study (χ2 = 10.89, p < 0.05), with older students and those in upper academic years (third year or beyond) showing greater awareness. Preventive behaviors were inconsistent; 46.1% of students reported lowering volume, while 13.0% took no preventive measures. Further analysis revealed that students who preferred high volumes were more likely to adopt preventive measures, while those who preferred low volumes often took no action, perceiving their existing habits as safe. Thematic analysis identified concerns about hearing health, barriers to safe listening, influence of social norms, and misconceptions about ear health.
Conclusion: The findings highlight a high prevalence of potentially unsafe listening behaviors and low NIHL awareness among South African university students. Recommendations include university-based hearing health programs, leveraging social media for outreach, integrating education into first-year curricula, and promoting affordable protective options, and social media campaigns targeting safe listening practices. These measures could help foster safer listening habits and reduce NIHL risk within this vulnerable population.
Noise-induced hearing loss (NIHL) has become one of the most common, yet preventable, health concerns worldwide, affecting millions of individuals and contributing to long-term, irreversible hearing impairments (1). Recreational NIHL specifically refers to hearing loss resulting from exposure to high sound levels in leisure settings, including the use of personal listening devices (PLDs) like earphones and headphones (2). As these devices become ubiquitous, especially among young people, the risk of NIHL has increased significantly, with studies indicating that up to 1 billion young individuals worldwide are at risk due to unsafe listening practices with PLDs (3). The WHO reports that globally, these unsafe listening practices are driven largely by prolonged and high-volume use of PLDs (4). With increased urbanization, access to advanced technology, and the normalization of portable audio devices, the potential for recreational NIHL among youth has intensified.
South Africa presents a unique context within this global concern, as it balances rapid technological adoption with persistent socioeconomic and healthcare challenges. The widespread use of smartphones, estimated to be at 26.3 million users, has made PLDs accessible to a broader demographic, including South Africa’s large youth population (5). For many young adults, especially university students, earphones are integrated into daily routines—whether for commuting, studying, exercising, or relaxing. However, research within South Africa has shown that knowledge and awareness of the risks associated with NIHL remain limited among young adults (6, 7). Unlike high-income countries (HICs), where public health interventions and educational programs on NIHL are more established (4, 8), South Africa faces structural challenges in implementing widespread hearing health education (9, 10). Consequently, while South African youth may engage in similar listening behaviors to their global counterparts, they are at heightened risk of unknowingly adopting unsafe listening practices.
Noise-induced hearing loss is a type of sensorineural hearing loss that arises from prolonged exposure to excessive noise, leading to permanent damage to the delicate sensory hair cells within the cochlea of the inner ear (11). This type of hearing impairment is marked by the absence of regenerative capacity in the affected cells, meaning that once hearing is lost, it cannot be restored. NIHL can arise from both occupational and recreational exposure to noise (10). While occupational NIHL, caused by prolonged noise exposure in work environments, has long been recognized and legislatively addressed (12, 13), recreational NIHL is increasingly relevant in the context of PLDs (14–16). High-intensity sound levels—often exceeding the globally recommended limits of 85 dBA—can induce temporary or permanent hearing threshold shifts, leading to issues such as tinnitus and reduced speech intelligibility (17, 18). Studies have shown that prolonged exposure to sound levels above 85 dBA, a commonly used occupational exposure limit globally, can result in permanent hearing damage. This threshold is designed to protect most individuals from significant hearing loss over an 8-h daily exposure period; however, some organizations recommend lower limits, such as 80 dBA or 70 dBA, for enhanced protection. As young people in South Africa and globally increasingly use PLDs at high volumes, the associated risk of NIHL becomes more pronounced.
For undergraduate students, particularly those studying in high-noise urban environments, PLDs often serve as a mechanism to create a personal auditory space (19, 20). This practice has seen consistent growth, yet it is often coupled with potentially unsafe listening behaviors, such as extended listening durations and high-volume settings (19, 21–23). Studies across various countries indicate that young people frequently exceed recommended listening thresholds, such as 85 dBA, and disregard device warnings about high volume exposure (24–26). However, recreational noise exposures, which are often more intense or prolonged, may hinder auditory recovery and contribute to permanent hearing damage even at lower exposure levels The lack of adequate educational programs targeting safe listening practices exacerbates this issue. Studies have shown that a large percentage of students reported no awareness of recreational NIHL risks, with many unsure of the long-term consequences of high-volume listening (7, 23). In South Africa, the scarcity of research on earphone use among university students further limits the potential for targeted interventions that could address these behaviors and improve awareness.
Moreover, South Africa faces unique challenges in addressing this public health concern. While global efforts to prevent NIHL often rely on technological interventions and awareness campaigns, South Africa’s educational and public health sectors may lack the resources to deploy similar strategies comprehensively. South Africa faces structural challenges when compared to HICs, partly due to limited public health funding. For example, South Africa’s public health expenditure accounts for approximately 8.3% of GDP (4), compared to an average of 12% in many developed nations. These funding disparities can hinder the implementation of widespread hearing health education and access to advanced technological interventions. Studies suggest that students’ awareness of safe listening practices is limited, partly due to the absence of consistent messaging within the healthcare and educational frameworks (7, 27, 28). With a youth-dominated population and increasing access to advanced technologies, the risk of recreational NIHL could rise without timely interventions.
Recognizing the importance of context-specific research, this study aims to investigate undergraduate students’ awareness and understanding of recreational NIHL in South Africa, with particular focus on their earphone use habits, volume preferences, preventive behaviors, and associations between demographic variables and NIHL awareness. By exploring students’ awareness of the risks associated with recreational NIHL, this study seeks to inform targeted public health strategies that are not only preventative but also culturally and economically feasible within the South African context. Through such initiatives, the country can take critical steps toward mitigating the risk of NIHL associated with the uncontrolled use of PLDs and fostering healthier listening behaviors among its youth population.
This study employed a cross-sectional, non-experimental, descriptive phenomenological mixed-methods design using a quantitative survey method (29, 30), to examine the awareness, attitudes, and behaviors regarding recreational NIHL among undergraduate students. A cross-sectional design was selected to capture a snapshot of students’ knowledge and behaviors regarding earphone use and NIHL risk, whereas the mixed approach allowed for the identification and quantification of patterns and trends within the sample, while establishing relationships between variables.
The study was conducted among undergraduate students at a large urban university in Johannesburg, South Africa. The institution, located in Gauteng Province, has a significant proportion of South Africa’s youth enrolled, with a current undergraduate population of approximately 20,000, making it an ideal setting to explore recreational NIHL awareness. This population comprises a diverse demographic, including students from various socioeconomic backgrounds, ethnic groups, and fields of study, reflecting the broader diversity of South Africa’s youth. The university is situated in a metropolitan area, attracting students from both urban and rural settings, providing a unique opportunity to explore a wide range of listening behaviors and awareness levels related to recreational noise exposure.
Inclusion criteria were:
• Undergraduate status (enrolled full-time or part-time),
• Age between 18 and 30 years,
• Regular use of earphones or other personal listening devices.
Participants who did not meet these criteria were excluded to ensure a focused sample relevant to recreational NIHL.
A convenience sampling method was employed (31) to recruit participants, targeting undergraduate students across various disciplines. An online survey link was distributed to students via institutional email lists and social media platforms managed by student organizations. Given the anticipated lower response rate often associated with online surveys, all undergraduate students residing in university residences were invited to maximize reach and participation.
Using a margin of error of ±5% and a confidence level of 95%, a minimum sample size of 30 was calculated as appropriate for the university’s population of undergraduates, however 154 participants volunteered participation. This number was deemed sufficient to achieve statistical validity for generalizing within the target population.
A structured online survey was developed using Google Forms and consisted of four main sections. Each section, except for demographics, included an open-ended question to gather qualitative insights.
1. Demographics: which included age, gender, year of study, and field of study.
2. Earphone use and listening habits: this section assessed the frequency, duration, and volume of earphone use, as well as specific activities during which earphones were commonly used (e.g., studying, exercising, commuting). The exact survey items included:
• “How often do you use earphones or headphones?” (Daily, Several times a week, Occasionally, Rarely)
• “On average, how many hours per day do you use earphones or headphones?” (<1 h, 1–2 h, 3–4 h, 5–6 h, More than 6 h)
• “What volume level do you typically set when using earphones or headphones?” (Low, Moderate, High)
3. Awareness of NIHL: multiple-choice questions assessed participants’ understanding of NIHL, including safe listening practices and the risks associated with prolonged high-volume exposure. Survey items included:
• “Have you ever heard of the term ‘noise-induced hearing loss (NIHL)’?” (Yes/No)
• “Do you know that prolonged exposure to high noise levels can lead to permanent hearing loss?” (Yes/No)
• “How informed do you feel about the risks of noise-induced hearing loss?” (Very informed, Somewhat informed, Slightly informed, Not informed)
Sources of NIHL awareness: participants were asked to identify the sources from which they had learned about NIHL. The survey allowed multiple selections to accommodate the possibility that participants had been exposed to information through various channels, including social media, device warnings, formal education, healthcare consultations, and other (open-ended response).
4. Attitudes and perceptions: this section used a 5-point Likert scale (Strongly Agree, Agree, Neutral, Disagree, Strongly Disagree) to assess participants’ perceptions of earphone use and self-reported behaviors in response to volume warnings. Statements included:
• “Listening to music at high volumes is necessary to enjoy the full experience.”
• “I lower my volume when I receive a warning about high volume exposure.”
• “Using noise-canceling earphones is a good way to reduce the need for high volume.”
• “I am concerned that my earphone use might affect my hearing in the future.”
5. Preferred volume levels and NIHL risk: to approximate noise exposure risk, participants were asked to categorize their typical listening volume into:
• Low volume: comfortable listening level where audio is clearly audible without causing discomfort; approximated at ≤60 dBA.
• Moderate volume: noticeably louder but still comfortable, approximated at 60–80 dBA.
• High volume: loud enough to overpower external noise or potentially cause discomfort, approximated at ≥80 dBA, which is associated with an increased risk of NIHL when sustained over time.
These categories were adapted from existing research on PLD use and NIHL risk.
Preventive measures and volume preferences: participants were asked whether they adopted any hearing protection measures while using PLDs. The question posed was:
• “Do you take any steps to protect your hearing while using earphones or headphones? If yes, what measures do you take?” (Open-ended response)
This question was analysed alongside volume preferences to explore whether a relationship existed between high-volume listening and preventive behaviors, such as lowering volume, limiting listening duration, or using noise-canceling features.
The survey was piloted with 10 undergraduate students who provided feedback on clarity and relevance. Minor revisions were made based on this feedback to enhance the instrument’s comprehensibility and ease of use.
No specific data were collected on the type of personal listening device (e.g., Android, iPhone) or hearing device (e.g., over-the-ear, in-ear, or bone conduction headphones) used by participants. While the survey focused on listening habits, awareness, and preventive behaviors, future research should include these variables to explore potential differences in listening behaviors and preferences based on device type.
Data collection took place over a four-week period. The survey link was distributed twice weekly through institutional channels to encourage participation. Participation was voluntary, and informed consent was obtained digitally before students could access the survey. No personally identifiable information was collected, ensuring full anonymity. Participants were informed that completing the survey implied consent, as approved by the institution’s ethics committee.
This study adhered to stringent ethical guidelines to protect the rights, privacy, and wellbeing of all participants. Ethical approval was obtained from the University’s Human Research Ethics Committee (non-medical) (Protocol number: STA_2024_33) prior to the commencement of the study. Participation was voluntary, and informed consent was obtained digitally before students could access the survey. All survey responses were collected anonymously via a secure online platform to ensure participant confidentiality. Data were stored on a password-protected institutional server, accessible only to the research team. No personally identifiable information was collected, maintaining full anonymity. In compliance with South Africa’s Protection of Personal Information Act (POPIA), the data will be retained securely for 5 years following publication and then permanently deleted (32). Participants were informed about their right to withdraw from the study at any time without consequences.
Through these measures, the study upheld principles of respect, beneficence, and justice, ensuring a rigorous and ethically sound approach to data collection and participant care (33, 34).
Data were cleaned, coded, and analysed using SPSS software (Version 27). The analysis included:
• Descriptive statistics: frequencies, percentages, means, and standard deviations were calculated for demographic variables and survey items, providing an overview of earphone use habits and awareness of NIHL.
• Thematic analysis: the thematic analysis of open-ended survey responses followed Braun and Clarke’s (35) six-step framework to systematically explore students’ awareness, attitudes, and challenges surrounding recreational NIHL. In the first step, familiarization, researchers repeatedly read responses to immerse themselves in the data. The second step, generating initial codes, involved identifying and labeling meaningful segments of text related to NIHL awareness and behaviors. In the third step, searching for themes, similar codes were grouped into preliminary themes. Step four, reviewing themes, refined these themes by ensuring they were coherent, distinct, and accurately represented the data. In the fifth step, defining and naming themes, each theme was clearly defined and contextualized to convey unique aspects of students’ perceptions and experiences. Finally, in step six, producing the report, themes were organized into a narrative that complemented the quantitative findings, providing a richer, more nuanced understanding of the data. This approach provided deeper insights into students’ perceptions and experiences, complementing the quantitative findings and enriching the study’s overall interpretation of NIHL awareness and behaviors.
• Inferential statistics: Chi-square tests were conducted to examine associations between demographic variables (e.g., age, gender, year of study) and awareness of NIHL and listening behaviors. Additionally, one-way ANOVA tests were employed to assess differences in NIHL awareness based on the frequency and duration of earphone use. Moreover, Chi-square was used to test whether there is a significant association between age/year of study and listening duration, determine if volume preferences differ significantly based on demographics, explore whether the primary source of NIHL awareness varies based on academic progression, and to identify whether those who prefer higher volumes are more likely to adopt preventive measures.
To enhance reliability and validity, the survey was piloted with 10 undergraduate students, leading to minor refinements for clarity and ease of use. Content validity was ensured by designing questions based on existing literature on noise-induced hearing loss (NIHL) and personal listening device (PLD) use. For rigor and trustworthiness, the study employed methodological triangulation (30, 36, 37), combining quantitative survey data with thematic analysis of open-ended responses. Researcher triangulation was applied by having multiple investigators review the qualitative findings, minimizing bias. To enhance transferability, detailed descriptions of the study context and participant demographics were provided, allowing for comparisons with similar populations.
A total of 154 undergraduate students completed the survey. Table 1 provides a demographic overview of the 154 undergraduate students who participated in the study. Most participants were between the ages of 18–20 years (46.8%), followed by those aged 21–25 years (39.0%). Female students constituted a larger proportion of the sample (61.7%) compared to male students (38.3%). In terms of academic level, first-year students represented 33.8% of the sample, while the remainder were distributed across the second (26.0%), third (24.0%), and fourth year or above (16.2%). Participants came from diverse fields, with the largest groups being from the Humanities (31.2%) and Health Sciences (24.0%), followed by Engineering and Technology (22.1%), Commerce (13.6%), and other disciplines (9.1%). This demographic distribution highlights the varied academic backgrounds and levels within the sample, providing a broad perspective on students’ awareness and behaviors regarding recreational noise-induced hearing loss.
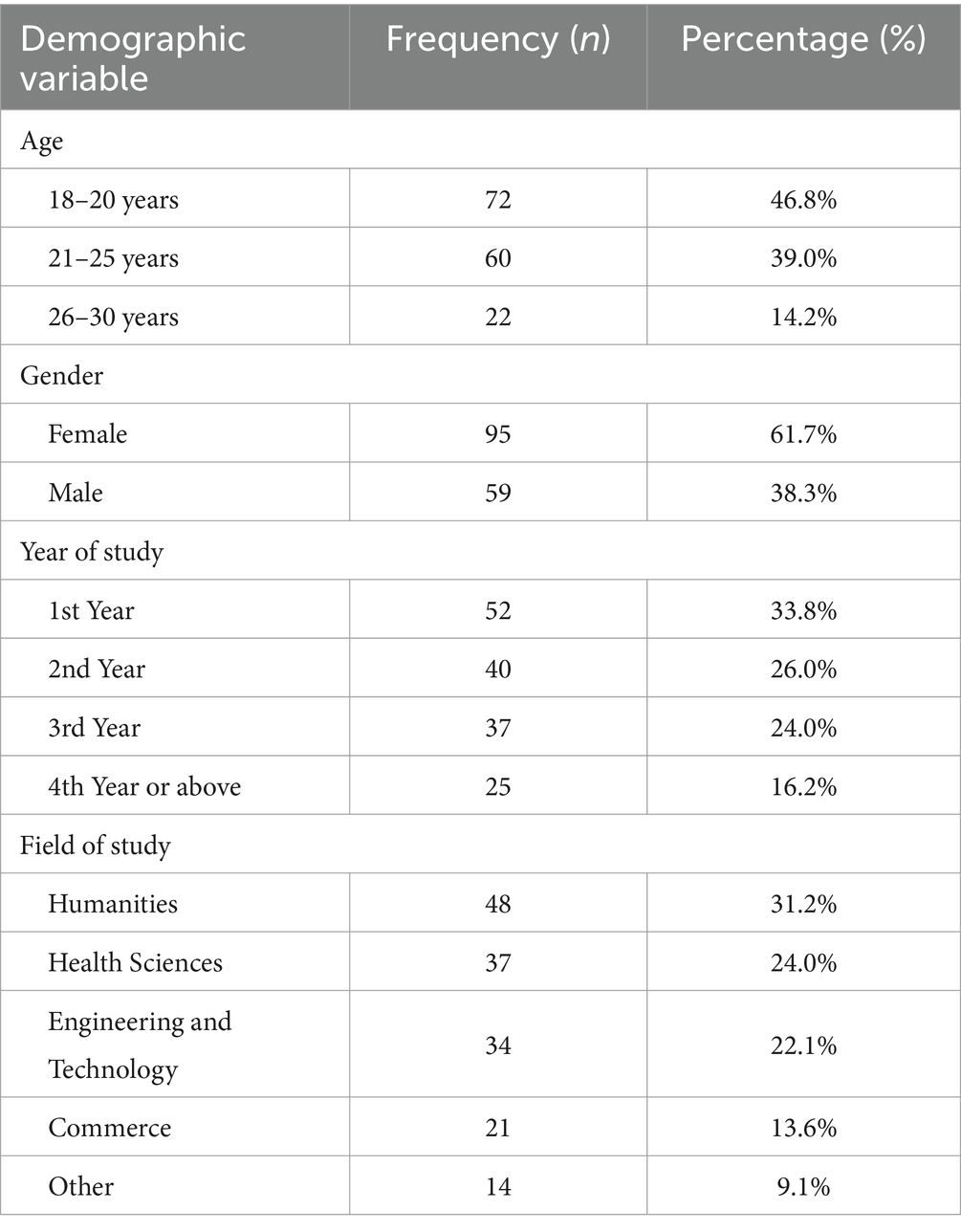
Table 1. Demographic characteristics of respondents (n = 154).
As shown in Table 2, 67.5% of participants reported daily earphone use, while 22.7% used earphones several times a week. Only 5.2% indicated occasional use, and 4.5% reported rare usage.
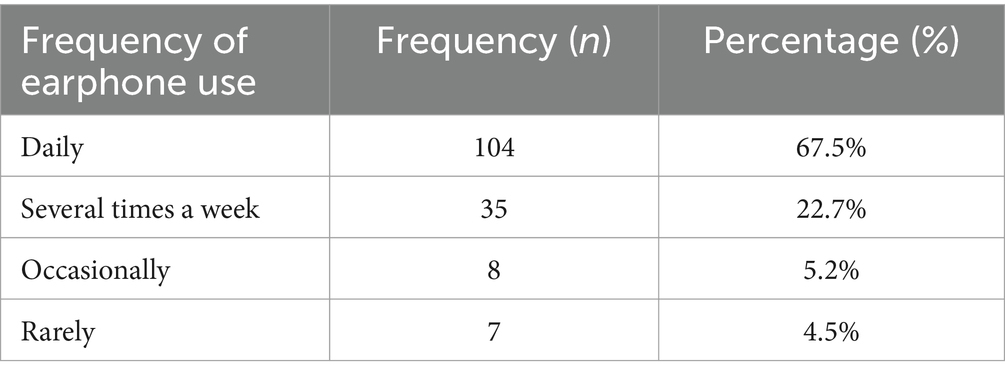
Table 2. Frequency of earphone use among participants (n = 154).
Table 3 illustrates the average duration of daily earphone use among the 154 participants. The largest group (34.4%) reported using earphones for 1–2 h daily, followed closely by those listening for 3–4 h (29.2%). A smaller proportion used earphones for <1 h per day (16.9%), while 13.0% listened for 5–6 h, and 6.5% reported using earphones for more than 6 h daily. These findings indicate that a significant number of students engage in prolonged listening, with potential implications for their risk of noise-induced hearing loss.
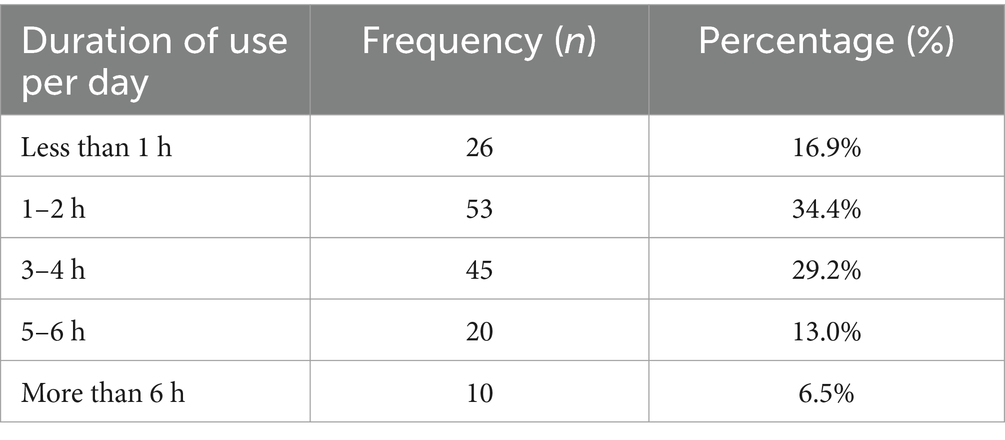
Table 3. Average duration of daily earphone use (n = 154).
Table 4 shows that 48.1% of participants used moderate volume settings, while 33.8% admitted to using high volumes. Alarmingly, 18.4% frequently ignored device warnings about high-volume exposure.
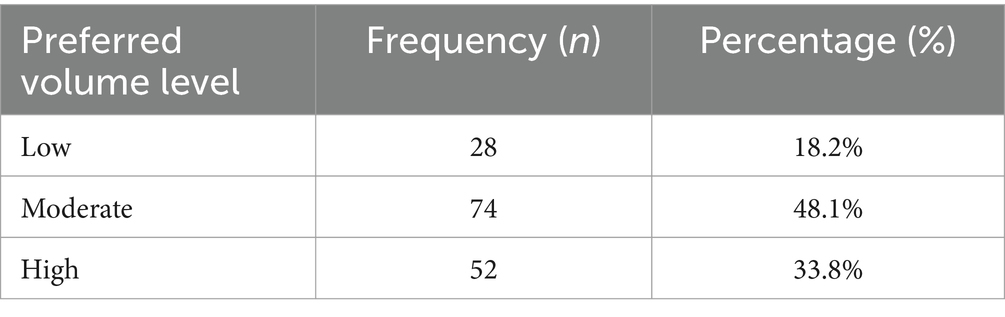
Table 4. Preferred volume levels when using earphones (n = 154).
As indicated in Table 5, 36.4% of participants were not informed about NIHL, and only 9.7% reported being very informed.
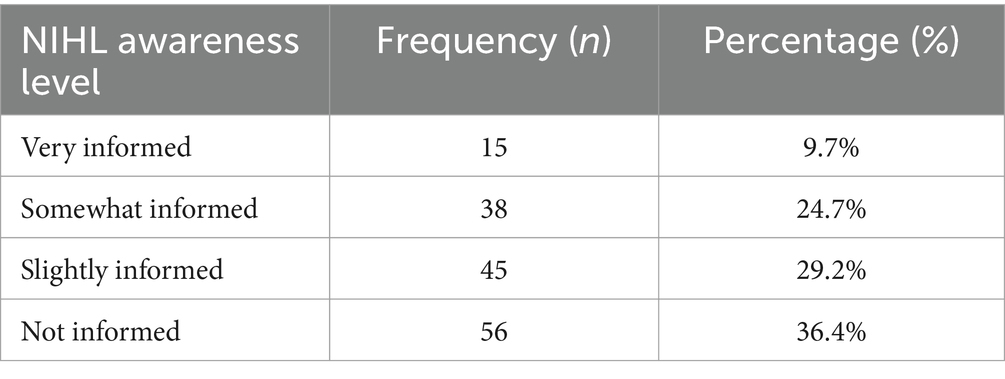
Table 5. Awareness of noise-induced hearing loss (NIHL) among participants (n = 154).
Table 6 presents the sources of information on NIHL awareness among the 154 participants, with social media being the most reported source (44.2%), followed by device warnings (32.5%).
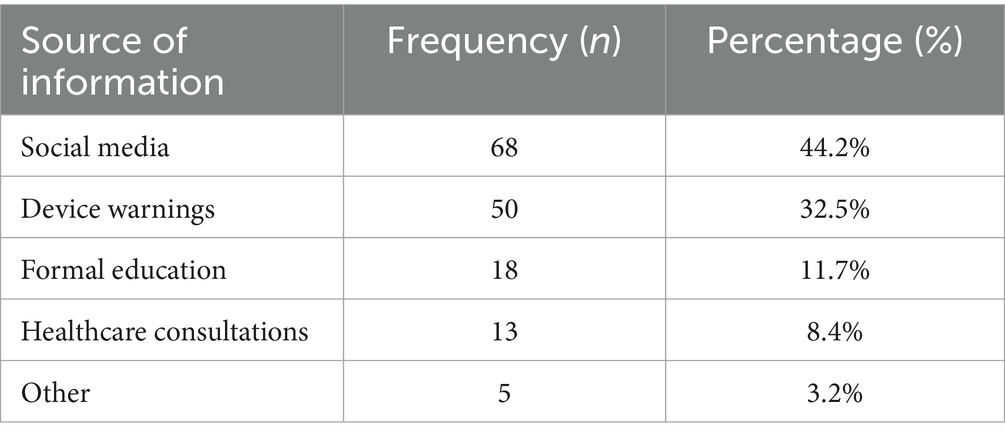
Table 6. Sources of information on NIHL awareness (n = 154).
Table 7 indicates that nearly half of the participants (46.1%) actively reduced their volume levels, while 31.8% limited listening time. A significant 13% took no preventive actions.
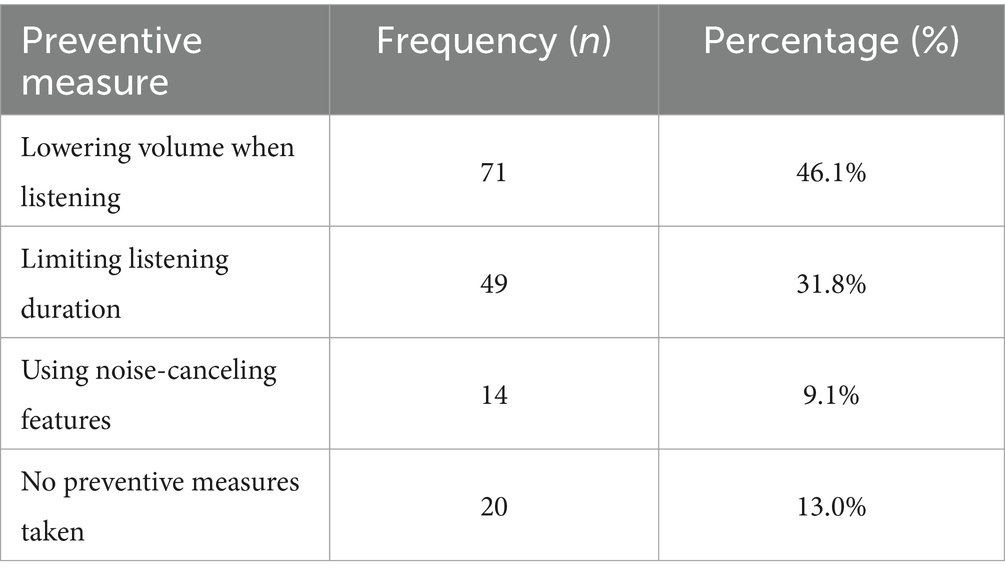
Table 7. Preventive measures taken by participants (n = 154).
Qualitative responses provided insights into students’ awareness, attitudes, and personal experiences with NIHL. Thematic analysis of these responses yielded five key themes:
Many participants expressed growing concerns about the potential long-term impact of earphone use on their hearing. Some reported experiencing symptoms such as tinnitus or occasional hearing discomfort, prompting concerns about possible NIHL.
“Sometimes, after listening for a few hours, my ears feel uncomfortable. I worry this might lead to permanent damage.”—Participant 18
“I’ve noticed a ringing in my ears after long listening sessions, and it scares me that this could become permanent.”—Participant 29
A significant number of participants acknowledged they had little knowledge of NIHL prior to the study. For many, this was the first time they were prompted to consider the potential risks associated with their listening habits. Respondents expressed a desire for more awareness campaigns targeting young adults.
“I never knew about NIHL before this survey. I think universities should talk about this more.”—Participant 67
“I didn’t realize listening at high volumes could actually damage my hearing. More information about this would be really helpful.”—Participant 82
Participants cited practical challenges, such as noise in public spaces and peer pressure, as barriers to lowering earphone volume or reducing listening time. Additionally, some mentioned that noise-canceling features in earphones, though helpful, were not affordable.
“I usually turn up the volume because I’m in noisy areas. I wish there was a way to block out external noise without turning the volume up so high.”—Participant 103
“It’s hard to keep the volume low when I’m in a busy, noisy place. Earphones help me concentrate, but I end up turning the sound way up.”—Participant 56
Social influences and peer norms around high-volume listening were prevalent among respondents. Many shared that friends’ behaviors influenced their own practices, with volume often set to match group listening standards.
“Most of my friends listen at high volumes, so I guess I do the same to not feel left out.”—Participant 141
“Everyone around me uses earphones all the time, so it’s just become normal to listen at high volumes, especially when we’re in groups.”—Participant 94
Some respondents believed that intermittent use of earphones at high volumes would not result in permanent damage. While continuous noise exposure does present a greater risk of NIHL, prolonged intermittent exposure to high-volume audio can still lead to cumulative auditory damage over time, particularly if recovery periods are insufficient (38).
“I thought as long as I don’t listen every day, my ears would be fine. I didn’t know the long-term effects could still happen.”—Participant 188
“I assumed only people who work in loud environments are at risk for hearing loss. I didn’t know that regular earphone use could have an impact too.”—Participant 118
Chi-square tests examined associations between demographic variables (age, gender, and year of study) and NIHL awareness. As far as age and awareness was concerned, a significant association was found between age and NIHL awareness (χ2 = 12.67, p < 0.05), with older students (21–30 years) more likely to be informed than younger students (18–20 years). As far as year of study and awareness was concerned, third-year students and beyond had higher awareness levels compared to first-year students (χ2 = 10.89, p < 0.05), suggesting that awareness may increase as student’s progress academically.
Further inferential analysis on duration of daily earphone use, preferred volume levels, sources of information of NIHL awareness, preventive measures, as well as preventive measures and volume preference relationship
Hypothesis: older students (21–30 years) and those in later years of study (third year or beyond) are more likely to limit their earphone use to shorter durations due to greater awareness of NIHL risks or busier academic schedules (Table 8).
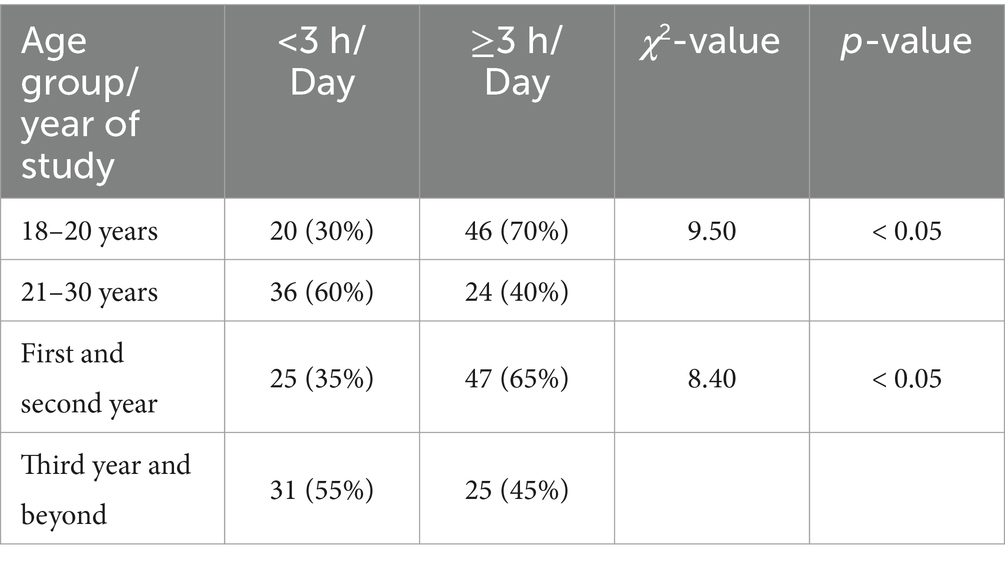
Table 8. Duration of daily earphone use (n = 154).
Hypothesis: younger students (18–20 years) and those in earlier years of study are more likely to prefer high volume levels compared to older students and those in upper academic years, due to lower awareness of NIHL risks (Table 9).
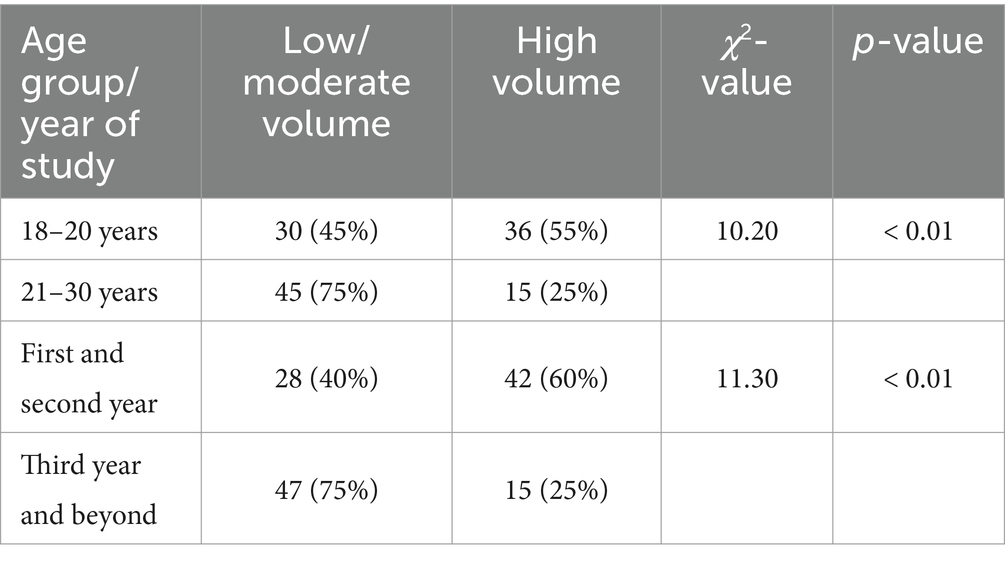
Table 9. Preferred volume levels (n = 154).
Hypothesis: students in upper academic years are more likely to cite healthcare consultations and formal education as their sources of awareness, while younger students are more reliant on social media and device warnings (Table 10).
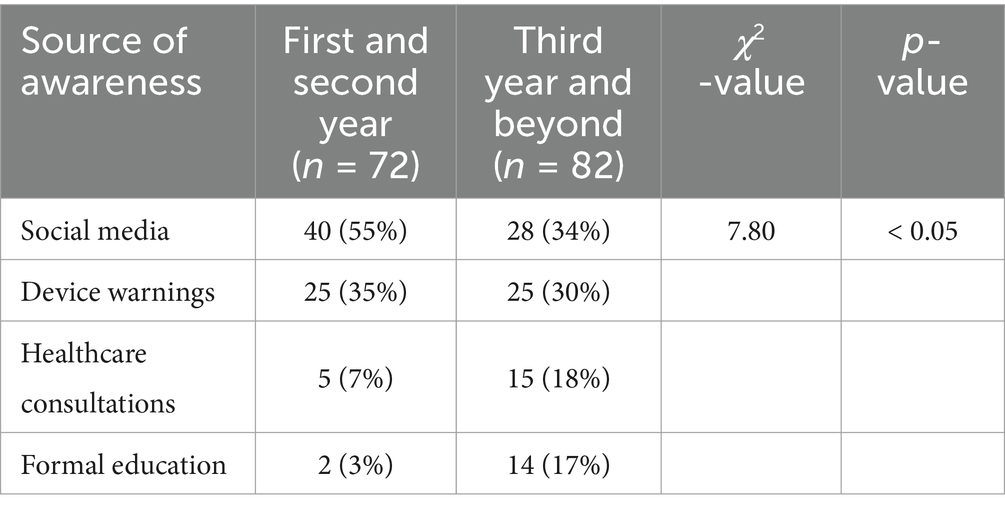
Table 10. Sources of NIHL awareness (n = 154).
Hypothesis: students who prefer high volumes are more likely to adopt preventive measures like noise-canceling features and limiting duration, as they may be aware of the risks associated with their listening habits (Table 11).
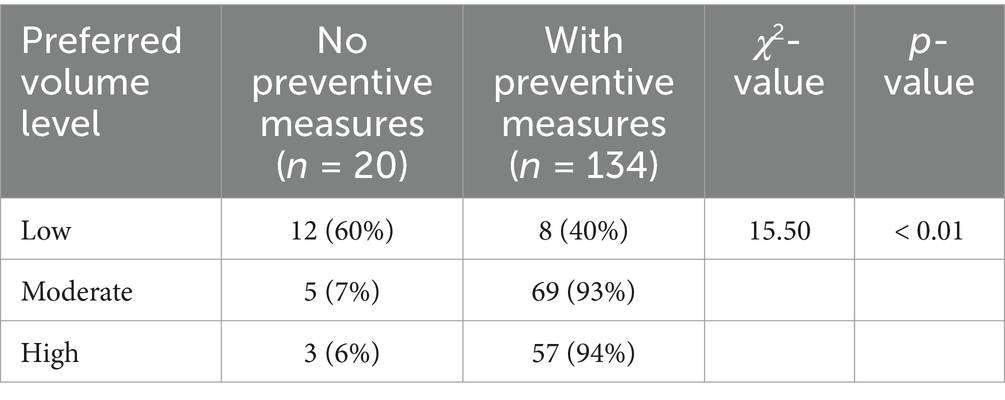
Table 11. Preventive measures (n = 154).
Further analysis revealed a significant relationship between preferred volume levels and the likelihood of adopting preventive measures (χ2 = 15.42, p < 0.01). Among respondents who reported taking no preventive action (n = 20), 60% preferred “low” volume levels, while 35% preferred “moderate” and 5% preferred “high” volumes. Conversely, those who reported adopting preventive measures (n = 134) were distributed across volume preferences as follows: 6% (low), 51% (moderate), and 43% (high). These findings suggest that respondents who prefer “low” volumes may perceive their existing behavior as inherently safe, reducing the perceived need for additional preventive measures.
The demographic profile of the sample, which consisted largely of young adults aged 18–25, is reflective of the typical university undergraduate population in South Africa (39). The WHO identified young adults, such as this group, as susceptible to recreational NIHL, as they represent a demographic that frequently engages in high-volume, prolonged listening on personal devices, putting them at increased risk of hearing damage (4). Additionally, findings from AlQahtani et al. (40) and Mahomed and Panday (7) found similarly low levels of NIHL awareness among young adults internationally and in South Africa. This lack of awareness, particularly among younger students and first-year participants, may suggest limited exposure to hearing health education and preventive campaigns, which have historically focused more on occupational NIHL than on recreational sources.
A striking 67.5% of participants reported using earphones daily, with a notable proportion listening at moderate to high volume levels. This regular use is in line with findings from previous research, such as Srihari et al. (23), which noted that nearly 90% of students reported listening to audio at volume levels above 60%, often exceeding safe listening thresholds. High daily usage was further supported by self-reported durations, with over 63.4% of participants listening for more than an hour per day and a significant portion listening for 3–4 h daily. These findings are particularly relevant within the South African context, where urban noise pollution is common (41), and earphones may serve as a means of creating a personal auditory space. However, in HICs, noise-canceling headphones are generally more accessible due to higher market penetration, but their high cost may still limit widespread use. Similarly, in South Africa, cost constraints and limited awareness of noise-canceling technology as a preventive option may lead students to rely on increasing volume to block out background noise, potentially increasing the risk of NIHL. Thus, the high levels of earphone use combined with moderate to high volumes highlight a key risk factor for NIHL among South African youth, raising the need for accessible alternatives and affordable protective options.
The survey revealed that 36.4% of respondents were not informed about NIHL, and only a small fraction (9.7%) were very informed. This limited awareness is a critical finding, as NIHL knowledge directly influences safe listening behaviors. Internationally, research by Fasanya and Strong (38) and Ansari et al. (21) found similar deficits in NIHL awareness, with Fasanya and Strong noting that only 14% of their sample were well-informed about the risks associated with high-volume listening. These studies emphasize the need for proactive education initiatives targeting young adults. In South Africa, this gap in awareness can be contextualized within the limited presence of public health campaigns focused on recreational NIHL. The current study’s findings align with Mahomed and Panday’s (7) results from a South African university sample, where many students were unaware of NIHL and often dismissed warnings about volume limits on devices. The reliance on social media (44.2%) and device warnings (32.5%) as the primary sources of NIHL-related information further indicates a missed opportunity for structured educational outreach. These informal sources may lack comprehensive and accurate information on NIHL, suggesting that targeted public health interventions, potentially integrated within university programs, are crucial for raising awareness and encouraging preventive practices. Furthermore, social representation theory provides a valuable framework for understanding how young adults perceive music and loudness. Manchaiah et al. (42) found that music holds social and emotional significance, with loudness often associated with enjoyment, escapism, and peer acceptance. Similarly, the cross-cultural study on social representation of “loud music” (43) showed that young people tend to understand loud music as an embodiment of freedom and expression, which can lead to a disregard for hearing health risks. These psychosocial factors may partially explain why university students in this study rely on high volume listening despite limited awareness of NIHL. Public health interventions should consider these perceptions, framing safe listening habits as compatible with enjoyment rather than a restriction. These public health interventions could be conducted by Audiology, Environmental Health, and/or Occupational Health and Safety students as part of their supervised practical training.
In terms of preventive behaviors, almost half of the participants (46.1%) reported lowering their listening volume, and 31.8% limited listening duration as a form of self-protection. However, 13% admitted to taking no preventive measures at all. These findings mirror those from Mutawakkil et al. (44) and Dehnert et al. (45), who found that young adults rarely take active steps to protect their hearing unless they have prior knowledge of NIHL or experience hearing discomfort. Within the South African context, barriers to preventive behaviors may include lack of information, social norms that encourage high-volume listening, and practical limitations such as cost-effective noise-canceling options. The relationship between volume preferences and preventive measures was examined. Among respondents who preferred high volume (n = 52), 40.4% reported lowering their volume as a preventive measure, while 19.2% used noise-canceling features to avoid increasing volume in noisy environments. Conversely, among those who preferred low volume (n = 28), 64.3% indicated they did not feel the need for additional preventive measures, as their listening habits were already cautious. This further supports the need for interventions that recognize music-related behaviors as culturally embedded, rather than purely individual choices. As previously identified by Manchaiah et al. (42, 43), addressing social representations of music and loudness may help in designing more effective strategies that balance hearing health with youth music culture. These findings suggest that participants with higher volume preferences may take more deliberate actions to mitigate the risks of noise-induced hearing loss (NIHL) compared The thematic analysis revealed that students often turned up the volume to counter external noise or to match social settings, which aligns with reports from Dehnert et al. (45) that young adults often listen to music at unsafe levels in social contexts. This social influence, evident in responses such as “Most of my friends listen at high volumes, so I do the same,” highlights a need for interventions that not only provide information on NIHL but also address social norms around listening habits to those who prefer lower volume levels.
The thematic analysis findings revealed further insights into students’ perceptions and experiences, highlighting five key themes: (1) concerns about hearing health, (2) limited awareness, (3) barriers to safe listening, (4) peer influence, and (5) misconceptions about ear health. Firstly, as far as concerns about hearing health were concerned, several participants expressed worry about the potential for hearing loss, with some noting physical discomfort after prolonged listening sessions. This aligns with Fasanya and Strong (38), who also found that prolonged earphone use led to self-reported symptoms of auditory discomfort. These concerns, however, were often reactive rather than preventive, suggesting a lack of proactive awareness on how to prevent hearing damage before symptoms arise.
As far as limited awareness and desire for information was concerned, participants’ calls for more information on NIHL highlight a crucial gap in health education. Responses like “I never knew about NIHL before this survey” illustrate the need for targeted NIHL education within South African universities. Ansari et al. (21) and Mutawakkil et al. (44) have both emphasized that young adults’ awareness of safe listening practices is low, which correlates with the lack of formal hearing health education observed in South Africa. As far as barriers to safe listening practice were concerned, practical challenges, such as external noise in public spaces, were frequently mentioned. This issue, particularly relevant in urban South African settings, often leads students to raise earphone volume. Compared to students in HICs with greater access to affordable noise-canceling options, South African students may find it harder to adopt safe listening practices, thus increasing their risk for NIHL. The influence of peer norms on listening habits theme showed that social influences were evident, with participants admitting that peer behaviors shaped their listening habits. This finding aligns with international literature indicating that social norms significantly affect young adults’ listening volumes (46, 47). In South Africa, where social gatherings and recreational music consumption are culturally significant, addressing peer influence could play a central role in changing listening behaviors. Lastly, as far as misconceptions about ear health, some participants believed that intermittent use of earphones at high volumes would not result in permanent damage, a misconception noted by other studies (38). This gap in knowledge may partly explain why many students engage in potentially unsafe listening behaviors despite acknowledging potential discomfort. This finding highlights the importance of dispelling misconceptions and educating students on the cumulative impact of sound exposure on hearing health.
The inferential analysis revealed significant associations between demographic factors—specifically age and year of study—and students’ awareness of NIHL. Older students (aged 21–30) and those in upper academic years (3rd year or beyond) demonstrated higher levels of awareness compared to younger and first-year students. These findings suggest that exposure to university education over time may positively impact awareness, potentially through increased access to health information or experiences that raise awareness of personal health risks. This trend aligns with evidence that show a correlation between educational progression and health awareness, indicating that NIHL prevention efforts might be particularly impactful if introduced early in students’ academic journeys. Targeted NIHL awareness programs during orientation or in first-year courses could help bridge this awareness gap, equipping students with the knowledge to adopt safer listening behaviors sooner.
The additional inferential analysis provided insights into how demographics such as age and year of study influence listening behaviors, awareness, and preventive measures among undergraduate students. These findings not only underscore patterns of potentially unsafe listening habits but also highlight specific groups that would benefit from targeted interventions. Firstly, when it comes to duration of daily earphone use, the analysis revealed that younger students (18–20 years) and those in earlier academic years were more likely to report prolonged earphone use (≥3\geq 3 ≥ 3 h/day) compared to older students and those in upper academic years. This is consistent with previous studies suggesting that younger individuals may prioritize recreational activities like music listening, often overlooking the potential risks of prolonged noise exposure. Older students and those further along in their studies may have greater academic demands or awareness of health risks, which could explain their shorter listening durations. These findings suggest the need for early education campaigns targeting first-year students, emphasizing safe listening practices to mitigate long-term risks of NIHL. Secondly, as far as preferred volume levels were concerned, younger students and those in earlier academic years were significantly more likely to prefer high volume levels compared to their older peers. This aligns with research indicating that younger individuals often prioritize auditory immersion, especially in noisy environments, without fully understanding the risks of high-volume listening. Interestingly, students in their third year or beyond were more likely to prefer low or moderate volumes, potentially reflecting greater awareness of NIHL risks or experience with auditory discomfort. This highlights the importance of addressing high-volume listening behaviors early in academic programs, perhaps through orientation workshops or peer-led initiatives focused on hearing health. Thirdly, when it comes to sources of NIHL awareness, the sources of NIHL awareness differed significantly by academic year. Students in earlier years relied heavily on informal sources such as social media (55%) and device warnings (35%), whereas those in upper academic years were more likely to cite formal education (17%) and healthcare consultations (18%) as their primary sources. This suggests that exposure to structured educational content increases with academic progression, reinforcing the value of integrating hearing health education into first- and second-year curricula. Leveraging trusted channels like social media and device interfaces could also be a practical strategy for reaching younger students, given their reliance on these platforms for information. Lastly, as far as preventive measures go, a significant association was found between preferred volume levels and the adoption of preventive measures. Interestingly, students who preferred high volumes were more likely to adopt measures such as using noise-canceling features or limiting listening duration. This finding may reflect a recognition among these individuals of the risks associated with their listening habits, prompting compensatory actions to protect their hearing. Conversely, those who preferred low volumes were less likely to adopt preventive measures, suggesting that these individuals may perceive their low-volume listening behavior as sufficient to protect their hearing, aligning with prior research indicating that perceived risk influences preventive behaviors. However, it is important to note that even low-volume listening can contribute to cumulative auditory damage if paired with prolonged listening durations. Therefore, public health campaigns could capitalize on these findings by emphasizing the importance of adopting comprehensive preventive measures, regardless of perceived safety, to mitigate the long-term risks of NIHL, encouraging broader adoption of preventive behaviors.
As far as implications for public health are concerned, these findings emphasize the need for tailored public health strategies to address potentially unsafe listening behaviors in specific demographic groups. Younger students and those in earlier academic years represent a particularly vulnerable group due to their preference for prolonged listening durations and high volumes. Public health campaigns could focus on this group by: (1) integrating hearing health education into early university curricula, as several studies have emphasized the importance of embedding hearing conservation education in formal academic programs to promote long-term behavior change (48); (2) collaborating with social media platforms to disseminate information about NIHL since research has shown that young adults frequently obtain health-related information through social media, making it a valuable tool for raising awareness and promoting safe listening habits (49); (3) encouraging the use of noise-canceling devices to reduce the need for high volumes - while noise-canceling technology can help lower listening volumes, accessibility and affordability remain concerns, particularly in low- and middle-income countries (50); thus subsidies or student discounts could increase adoption; and (4) expanding NIHL education to high school students, given that many individuals develop listening habits in adolescence, early intervention at the high school level could be more effective in preventing NIHL; and prior research suggests that school-based hearing conservation programs can significantly improve awareness and modify risky listening behaviors before university (51). These strategies, supported by literature, emphasize the need for earlier interventions beyond university settings. We recommend that policymakers explore school-based initiatives that introduce hearing health education in secondary education curricula, ensuring that safe listening behaviors are established before student’s transition to university life.
Conversely, students in upper academic years may benefit from advanced educational content that reinforces safe listening habits and provides resources for managing auditory health. Efforts to engage this group should also involve promoting formal healthcare consultations for hearing assessments.
As valuable as current findings are, they should be interpreted with the identified limitations in mind. This study has several limitations that may affect the generalizability and depth of the findings. Firstly, the sample size of 154 students, though sufficient for initial insights, may limit the ability to generalize findings to the broader population of South African university students. Secondly, the use of convenience sampling could introduce selection bias, as participants who voluntarily completed the survey may have different levels of interest or awareness about NIHL compared to the general student body. Additionally, data were collected through self-reported responses, which can be influenced by social desirability bias, potentially leading students to overestimate their preventive behaviors or awareness levels. The cross-sectional nature of the study also limits the ability to assess causality, meaning we cannot determine if awareness levels directly impact listening behaviors over time. Furthermore, this study was conducted at a single urban university, and findings may differ in rural settings or among students from various socioeconomic backgrounds, suggesting the need for further research across diverse academic institutions and demographic groups in South Africa. Finally, this study did not collect data on the specific types of personal listening devices (e.g., Android, iPhone) or hearing devices (e.g., over-the-ear, in-ear, or bone conduction headphones) used by participants. These factors could influence listening behaviors, device preferences, and associated risks of noise-induced hearing loss, representing a valuable area for future research. Moreover, the absence of direct decibel measurements, limits the ability to quantify noise exposure risks. Future research should address these gaps by exploring the influence of device types and linking listening behaviors to measurable sound levels.
This study highlights the prevalence of potentially unsafe listening behaviors and low NIHL awareness among South African undergraduate students. Younger students and those in earlier academic years were more likely to engage in prolonged listening and high-volume use, emphasizing the need for early intervention. Findings suggest that targeted public health initiatives are essential. Recommendations include integrating hearing health education into early university curricula and high school programs, leveraging social media for awareness campaigns, and promoting affordable noise-canceling options to reduce high-volume exposure. However, public health interventions must also consider the social and cultural representations of music and loudness, as these factors influence how young adults perceive safe listening behaviors. As identified in cross-cultural studies, loud music is often associated with freedom, social connection, and personal expression. Therefore, effective strategies should frame safe listening as enhancing, rather than restricting, the music experience. While this study provides valuable insights, limitations include the lack of objective decibel measurements and data on specific device types. Future research should address these gaps to refine prevention strategies. By implementing evidence-based interventions, policymakers and educators can help establish safer listening habits and reduce the long-term risk of NIHL among young adults.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by the University of the Witwatersrand’s Human Research Ethics Committee (non-medical) (protocol number: STA_2024_33). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
KK-S: Conceptualization, Formal analysis, Methodology, Resources, Software, Supervision, Validation, Writing – original draft, Writing – review & editing. KM: Conceptualization, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Gen AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Salari, N, Hosseinian-Far, A, Zarei, H, Rasoulpoor, S, Ghasemi, H, Elyasi, H, et al. The global prevalence of noise induced hearing impairment among industrial workers: a systematic review and Meta-analysis. Indian J Otolaryngol Head Neck Surg. (2024) 76:5035–49. doi: 10.1007/s12070-024-05032-9
2. Feder, K, Marro, L, McNamee, J, and Michaud, D. Prevalence of loud leisure noise activities among a representative sample of Canadians aged 6–79 years. JASA. (2019) 146:3934–46. doi: 10.1121/1.5132949
4. World Bank Group. Current health expenditure (% of GDP). Washington, DC: World Bank Group (2024).
5. Taylor, J. (2023). Smartphone users in South Africa 2014-2023. Statista. Available online at: https://www.statista.com/statistics/488376/forecast-of-smartphone-users-in-south-africa/ (Accessed December 7, 2021).
6. Knoetze, M, Mahomed-Asmail, F, Manchaiah, V, and Swanepoel, DW. Sound-level monitoring earphones with smartphone feedback as an intervention to promote healthy listening behaviors in young adults. Ear Hear. (2021) 42:1173–82. doi: 10.1097/AUD.0000000000001029
7. Mahomed, H, and Panday, S. Awareness, attitudes and perceptions of students towards leisure noise in Durban, South Africa. SAJCD. (2024) 71:a1040. doi: 10.4102/sajcd.v71i1.1040.e1.e10
8. Waterworth, CJ, Marella, M, O’Donovan, J, Bright, T, Dowell, R, and Bhutta, MF. Barriers to access to ear and hearing care services in low-and middle-income countries: a scoping review. Glob Public Health. (2022) 17:3869–93. doi: 10.1080/17441692.2022.2053734
9. Khoza-Shangase, K. Preventive audiology: ramping up efforts towards an ear and hearing healthy nation In: K Khoza-Shangase, editor. Preventive audiology: An African perspective. Cape Town: AOSIS Books (2022a). 1–20.
10. Moroe, NF. Early detection and management of occupational and environmental noise In: K Khoza-Shangase, editor. Preventive audiology: An African perspective. Cape Town: AOSIS (2022)
11. Natarajan, N, Batts, S, and Stankovic, KM. Noise-induced hearing loss. J. Clin Med. (2023) 12:2347. doi: 10.3390/jcm12062347
12. Moroe, N, Khoza-Shangase, K, Kanji, A, and Ntlhakana, L. The management of occupational noise–induced hearing loss in the mining sector in Africa: a systematic review–1994 to 2016. Noise Vibr Worldwide. (2018) 49:181–90. doi: 10.1177/0957456518781860
13. Moroe, N, and Khoza-Shangase, K. Management of occupational noise induced hearing loss in the mining sector in South Africa: where are the audiologists? J Occup Health. (2018) 60:376–82. doi: 10.1539/joh.2018-0020-OA
14. Ehlert, K. Perceptions of public primary school teachers regarding noise-induced hearing loss in South Africa. SAJCD. (2017) 64:1–12. doi: 10.4102/sajcd.v64i1.185
15. Elmazoska, I, Mäki-Torkko, E, Granberg, S, and Widén, S. Associations between recreational noise exposure and hearing function in adolescents and young adults: a systematic review. JSLHR. (2024) 67:688–710. doi: 10.1044/2023_JSLHR-23-00397
16. Roberts, B, and Neitzel, RL. Noise exposure limit for children in recreational settings: review of available evidence. J Acoust Soc Am. (2019) 146:3922–33. doi: 10.1121/1.5132540
17. Dehankar, SS, and Gaurkar, S. Impact on hearing due to prolonged use of audio devices: a literature review. Cureus. (2022) 14:11. doi: 10.7759/cureus.31425.14.e31425
18. Khoza-Shangase, K. Risk factors for occupational noise-induced hearing loss in African mines: arguing for contextualisation In: K Khoza-Shangase and NF Moroe, editors. Occupational noise induced hearing loss: An African perspective. Cape Town: AOSIS Books (2022b). 39–57.
19. Marron, KH, Marchiondo, KT, Stephenson, S, Wagner, S, Cramer, IM, Wharton, T, et al. College students’ personal listening device usage and knowledge. Int J Audiol. (2014) 54:384–90. doi: 10.3109/14992027.2014.986691
20. You, S, Kwak, C, and Han, W. Use of personal listening devices and knowledge/attitude for greater hearing conservation in college students: data analysis and regression model based on 1009 respondents. Int J Environ Res Public Health. (2020) 17:2934. doi: 10.3390/ijerph17082934
21. Ansari, H, Mohammadpoorasl, A, Rostami, F, and Naieni, KH. Pattern of use of earphone and music player devices among Iranian adolescents. Int J Prev Med. (2014) 5:776–81.
22. Mohammadpoorasl, A, Hajizadeh, M, Marin, S, Heydari, P, and Ghalenoei, M. Prevalence and pattern of using headphones and its relationship with hearing loss among students. Health Scope. (2018) 7:65901. doi: 10.5812/jhealthscope.65901
23. Srihari, APS, and Kumar, L. Analysis of potential risk of hearing loss among students using personal audio devices. NJPPP. (2021) 11:462–5. doi: 10.5455/njppp.2021.11.11301202027122020
24. Alzhrani, F, Al-Saleh, S, Asrar, S, Al-Dhafeeri, A, Al-Baqami, B, Al-Harbi, M, et al. Community awareness of noise-induced hearing loss from portable listening devices and possible preventive measures. J Nat Sci Med. (2020) 11:1–114. doi: 10.4103/JNSM.JNSM_29_19
25. Bakshi, SS, Kalidoss, VK, Ramesh, S, and Shankar, MK. How harmful is your personal listening device: a knowledge and attitude survey among college-going students of India. Saudi J Otorhinolaryngol Head Neck Surg. (2021) 23:41–6. doi: 10.4103/sjoh.sjoh_55_20
26. Vogel, I, Brug, J, Van der Ploeg, CP, and Raat, H. Adolescents risky MP3-player listening and its psychosocial correlates. Health Educ Res. (2011) 26:254–64. doi: 10.1093/her/cyq091
27. Booi, M. Unsafe listening habits–managing noise exposure beyond the workplace. Occup Health South Afr. (2019) 25:103–5. Available at: https://hdl.handle.net/10520/EJC-16227e4e5e
28. Seedat, RY, Ehlers, R, Lee, Y, Mung’omba, C, Plaatjies, K, Prins, M, et al. Knowledge of the audiological effects, symptoms and practices related to personal listening devices of health sciences students at a south African university. JLO. (2020) 134:20–3. doi: 10.1017/S0022215120000092
29. McKim, CA. The value of mixed methods research: a mixed methods study. J Mix Methods Res. (2017) 11:202–22. doi: 10.1177/1558689815607096
30. Zohrabi, M. Mixed method research: instruments, validity, reliability and reporting findings. TPLS. (2013) 3:262. doi: 10.4304/tpls.3.2.254-262
31. Etikan, İ, Musa, SA, and Alkassim, RS. Comparison of convenience sampling and purposive sampling. AJTAS. (2016) 5:11. doi: 10.11648/j.ajtas.20160501.11
32. Pina, E, Ramos, J, Jorge, H, Váz, P, Silva, J, Wanzeller, C, et al. Data privacy and ethical considerations in database management. J Cybersecur Priv. (2024) 4:494–517. doi: 10.3390/jcp4030024
33. Shapiro, H. Ethical considerations in research on human subjects. The sixth annual Raymond Waggoner lecture. Ann Arbor, MI: University of Michigan (2001).
34. Varkey, B. Principles of clinical ethics and their application to practice. Med Princ Pract. (2020) 30:17–28. doi: 10.1159/000509119
35. Braun, V, and Clarke, V. Using thematic analysis in psychology. Qual Res Psychol. (2006) 3:77–101. doi: 10.1191/1478088706qp063oa
36. Johnson, JL, Adkins, D, and Chauvin, SW. A review of the quality indicators of rigor in qualitative research. Am J Pharm Educ. (2020) 84:7120. doi: 10.5688/ajpe7120
37. Morse, JM, Barrett, M, Mayan, M, Olson, K, and Spiers, J. Verification strategies for establishing reliability and validity in qualitative research. Sage J. (2002) 1:13–22. doi: 10.1177/160940690200100202
38. Fasanya, BK, and Strong, JD. Younger generation safety: hearing loss and academic performance degradation among college student headphone users. Adv Intel Syst Comput. (2019) 9:522–31. doi: 10.1007/978-3-319-94589-7_51
39. Khoza-Shangase, K, and Kalenga, M. English additional language undergraduate students’ engagement with the academic content in their curriculum in a south African speech-language and hearing training program. Front Educ. (2024) 9:1258358. doi: 10.3389/feduc.2024.1258358
40. AlQahtani, AS, Alshammari, AN, Khalifah, EM, Alnabri, AA, Aldarwish, HA, Alshammari, KF, et al. Awareness about the relation of noise induced hearing loss and use of headphones at hail region. Ann Med Surg. (2022) 73:103113. doi: 10.1016/j.amsu.2021.103113
41. Moroe, N, and Mabaso, P. Quantifying traffic noise pollution levels: a cross-sectional survey in South Africa. Sci Rep. (2022) 12:3454. doi: 10.1038/s41598-022-07145-z
42. Manchaiah, V, Zhao, F, Widén, S, Auzenne, J, Beukes, EW, Ahmadi, T, et al. Social representation of “music” in young adults: a cross-cultural study. Int J Audiol. (2017) 56:24–32. doi: 10.1080/14992027.2016.1227481
43. Manchaiah, V, Zhao, F, Widen, S, Auzenne, J, Beukes, EW, Ahmadi, T, et al. Social representation of “loud music” in young adults: a cross-cultural study. JAAA. (2017) 28:522–33. doi: 10.3766/jaaa.16046
44. Mutawakkil, AFM, Ridwan, AR, and Taufik, NHT. He effects of earphone use on the incidence of noise-induced hearing loss: an empirical study of senior high school students in Banda a. IJISRT. (2021) 6:885–92. Available at: https://ijisrt.com/assets/upload/files/IJISRT21DEC417.pdf
45. Dehnert, K, Raab, U, Pérez-Àlvarez, C, Steffens, T, Bolte, G, Fromme, H, et al. Total leisure noise exposure and its association with hearing loss among adolescents. Int J Audiol. (2015) 54:665–73. doi: 10.3109/14992027.2015.1030510
46. Diviani, N, Zanini, C, Amann, J, Chadha, S, Cieza, A, and Rubinelli, S. Awareness, attitudes, and beliefs about music-induced hearing loss: towards the development of a health communication strategy to promote safe listening. Patient Educ Couns. (2019) 102:1506–12. doi: 10.1016/j.pec.2019.03.013
47. Meinke, DK, and Martin, WH. Development of health Communications for Promotion of Safe Listening: A review. Make Listening Safe. Geneva: World Health Organization (2017).
48. Evans, A, Rennie-Salonen, B, Wijsman, S, and Ackermann, B. A scoping review of occupational health education programs for music students and teachers. RSME. (2024) 46:493–515. doi: 10.1177/1321103X241235794
49. McKinley, C, Luo, Y, and Brennan, J. Linking health consciousness and social media information seeking to college students COVID-19 prevention behavior: examining a modified IMBP model. West J Commun. (2023) 24:1–24. doi: 10.1080/10570314.2023.2294711
50. Hutson, P, and Hutson, J. Expanding sensory kit utilization across age and contexts: bridging gaps for inclusive accessibility. J Ment Health. (2024) 1:699. Available at: https://digitalcommons.lindenwood.edu/cgi/viewcontent.cgi?article=1705&context=faculty-research-papers
Keywords: recreational noise-induced hearing loss, earphones, undergraduate students, South Africa, hearing health awareness, personal listening devices
Citation: Khoza-Shangase K and Mokhethi K (2025) Recreational noise induced hearing loss: South African undergraduate students’ perspectives. Front. Public Health. 13:1534731. doi: 10.3389/fpubh.2025.1534731
Edited by:
Syed Arslan Haider, Capital University of Science and Technology, PakistanReviewed by:
David Tomé, Polytechnic of Porto, PortugalCopyright © 2025 Khoza-Shangase and Mokhethi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Katijah Khoza-Shangase, S2F0aWphaC5LaG96YS1TaGFuZ2FzZUB3aXRzLmFjLnph
†ORCID: Katijah Khoza-Shangase, https://orcid.org/0000-0002-6220-9606
Khothatso Mokhethi, https://orcid.org/0009-0008-1091-1867
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.