 Desi Debelu
Desi Debelu Sina Temesgen Tolera
Sina Temesgen Tolera Negga Baraki
Negga Baraki Dechasa Adare Mengistu
Dechasa Adare Mengistu- College of Health and Medical Sciences, Haramaya University, Dire Dawa, Ethiopia
Background: Currently, small-scale industries pose significant risks for occupational injuries, particularly in developing countries, including Ethiopia. Despite this problem, there is limited evidence on the prevalence of occupation-related injuries in small-scale industries that can be utilized for proposing interventions. Therefore, this study aims to determine the prevalence of occupational injuries and associated factors among small-scale industry workers in Harar town, Ethiopia.
Methods: A cross-sectional study employing a quantitative analysis was conducted in Harare town, Eastern Ethiopia, from March 12, 2023, to June 1, 2023. The source of population was all small-scale industry workers in Harar town, while the study population was workers working in selected small-scale industries. The sample size was determined based on the previous study finding reported 35.98% prevalence of occupational injuries. A simple random sampling method was employed to select the study participant, resulting in the inclusion of 639 participants in the study. Data were collected using pretested questionnaires and observational checklists, covering sociodemographic, occupational injuries, occupational health and safety practices, work environment, and behavioral related factors. The data were analyzed via SPSS version 22, and a p value of <0.05 was considered the cut-off point for statistical significance in multivariate analysis.
Results: Out of the 639 small-scale industry workers included in the current study, 634 provided a response, resulting in a 99.2% response rate. Among these workers, 417 workers (65.8%) reported exposure to occupational injuries at least once in their careers, of which 223 (35.2%) were exposed to injuries in the last 12 months. The most commonly injured body parts were the hands (34.11%), legs (29.13%), and fingers (26.69%). The study found a significant associations between occupational injuries and type of industry (AOR: 2.41, 95% CI: 1.07, 5.46), educational status (AOR: 2.49, 95% CI: 1.01, 2.83), training (AOR: 1.4, 95% CI: 1.35, 3.22), working space (AOR: 4.6, 95% CI: 2.62, 7.51), and workload (AOR: 2.88, 95% CI: 2.78, 11.64).
Conclusion: More than six out of 10 workers experienced injuries during their careers, with more than one-third being injured in the last 12 months. Workers with lower educational status, have no training, working in poor working conditions, and with higher workloads are at high risk of exposure. This highlights the need for improving occupational health and safety practices, including tailored training and supportive supervision to reduce injury in small-scale industries.
Originality/value: The findings from this study will be important for concerned bodies aiming to improve the occupational health and safety practices in small-scale industries and enhance the safe practices by addressing the safety culture in the working environment and policy making process.
1 Introduction
Rapid industrial, scientific, and social development, coupled with the use of non-renewable natural resources, has significantly increased occupational risks worldwide (1, 2). Small-scale industries (SSIs), including woodworking, metalworking, concrete block, and manufacturing industries, are among the highest-ranked SSIs in terms of risks for occupational injuries (3, 4).
According to global estimates from the International Labor Organization (ILO), poor occupational health and safety contribute to more than 2.3 million deaths annually. Among these deaths, approximately 350,000 result from fatal accidents, whereas approximately 2 million are due to fatal work-related diseases. Additionally, more than 313 million workers experience nonfatal occupational accidents that lead to serious injuries and significant absences from work (5).
In developed countries, occupational health services are available for about 20–50% of the workers, whereas in developing countries, they cover only 5–10% of workers. Despite this disparity, the prevalence of injuries is lower in high-income countries than in middle- and low-income countries (LMICs). For example, fatality and accident rates in Sub-Saharan Africa are significantly higher, accounting for 21 and 16,012 per 100,000 workers, respectively (6, 7).
Furthermore, workdays lost due to occupational injuries represent a significant economic challenge globally. The World Health Organization (WHO) estimates that the economic loss from work-related injuries and diseases accounted for 4% of the global GDP. In 2010 alone, over 313 million workers experienced nonfatal injuries that led to at least 4 days of absence from work (8, 9). Additionally, workers who suffer from occupational injuries may also face social and psychological trauma (10). Therefore, application of a positive psychological measure can significantly improve the implementation of safety measures through incorporating psychological related factors into policy-making or frameworks in the industry (11).
In Ethiopia, occupational injuries are major causes of mortality and morbidity among workers working in small-scale enterprises (12, 13). Many SSIs in Ethiopia lack sufficient safety materials, guidelines, supervision, and policies to prevent workplace injuries and promote worker health. Furthermore, there is a lack of adequate data on the prevalence of work-related injuries due to limited national and local information (14). Some of the studies conducted in Ethiopia were targeted at prevalence of occupational injuries specific to body parts such as ocular injury (15), while the others targeted at workers working in specific industries such as metal manufacturing industry (16), small-scale woodwork industry workers (14, 17), and building construction workers (13). However, this study addresses the prevalence of occupational injuries in different types of small scale industries and body parties, which provide comprehensive evidence that can be utilized by the concerned bodies to take action.
Furthermore, in Harare town, there is no data or evidence on the prevalence of occupational injuries among. Therefore, this study aims to determine the prevalence of occupational injuries and associated factors among small-scale industries workers in the Harare town. The findings from this study are used to understand the extent of the problem and the conditions that lead to injuries, which can help in developing targeted interventions and improving workplace safety for these workers.
2 Literature review (overview)
Currently, the workplace influences the health and safety, as well as the productivity of workers at different levels (18). Industry workers are exposed to huge stressors in their working environment. This exposure is prolonged due to unusual work schedules in many industries (19). Among these industries, small-scale industries, such as construction industries, are facing high safety risks, requiring effective safety leadership to reduce accidents and improve performance (20). According to the ILO report in 2023, more than 2.93 million deaths and 395 million non-fatal work-related injuries and illnesses occurred from occupational accidents and diseases each year around the world. Furthermore, the economic cost of these occupational-related deaths, injuries, and illnesses is estimated at 361 billion dollars each year (21).
Therefore, the hazardous nature of different industries’ activities across the world and higher in the developing countries has led to concerns about the occupational health and safety of the workers. It highlighted the critical need for adopting safe work methods or environments (22, 23). Health and safety is of paramount importance, especially for different organizations and individuals operating in high-risk industrial areas. Therefore, there should be adequate workplace safety management and accident prevention through proper design of working conditions and implementation of basic protection (24, 25).
According to a cross sectional study conducted in Bale Zone, southeast Ethiopia, the prevalence of occupational injury among SSI workers throughout the lifetime, and in the last 1 year was 43.2, and 30%, respectively (26). Another cross sectional study conducted in Ambo town, Ethiopia in 2021, among small scale enterprise workers in 2022 revealed that the prevalence of occupational injuries in the last 1 year was 39.5% (95% CI: 35–44) (27). According to a cross sectional study conducted in Mekele City, Ethiopia in 2013, among SSI workers, the use of personal protective equipment (PPE) [AOR = 3.43, 95%CI: 2.39–4.94] was significantly associated with occupational injury (28). Moreover, a cross sectional study conducted in ambo town in 2021 reported that there was an association between occupational injury among small scale industry workers and not using PPE (AOR = 1.55, 95% CI: 1.03–2.87) (27).
We remain in need of further discussion and application of comprehensive models that integrate the role of cognitive challenges, emotional states, and organization of tasks, work stress, health, and work environmental factors (25). Therefore, timely identification of the gap and solutions for the potential risk factors is critical for the health and safety, as well as for the productivity of the workers. Because improving workers health and safety is paramount for industries, including in reducing the shortage of skilled manpower, strains on supply, and medical costs related to this problem (18).
Therefore, industries need to tailor their workplace safety measures to address the diverse needs of their workforce. In light of this study’s findings, this study aimed to determine the prevalence of occupational injuries and associated factors among small-scale industries workers expected to have a high risk of occupational injuries (11).
2.1 Conceptual framework
A conceptual framework showing the interaction between dependent variables (occupational related injury) and independent variables (Figure 1).
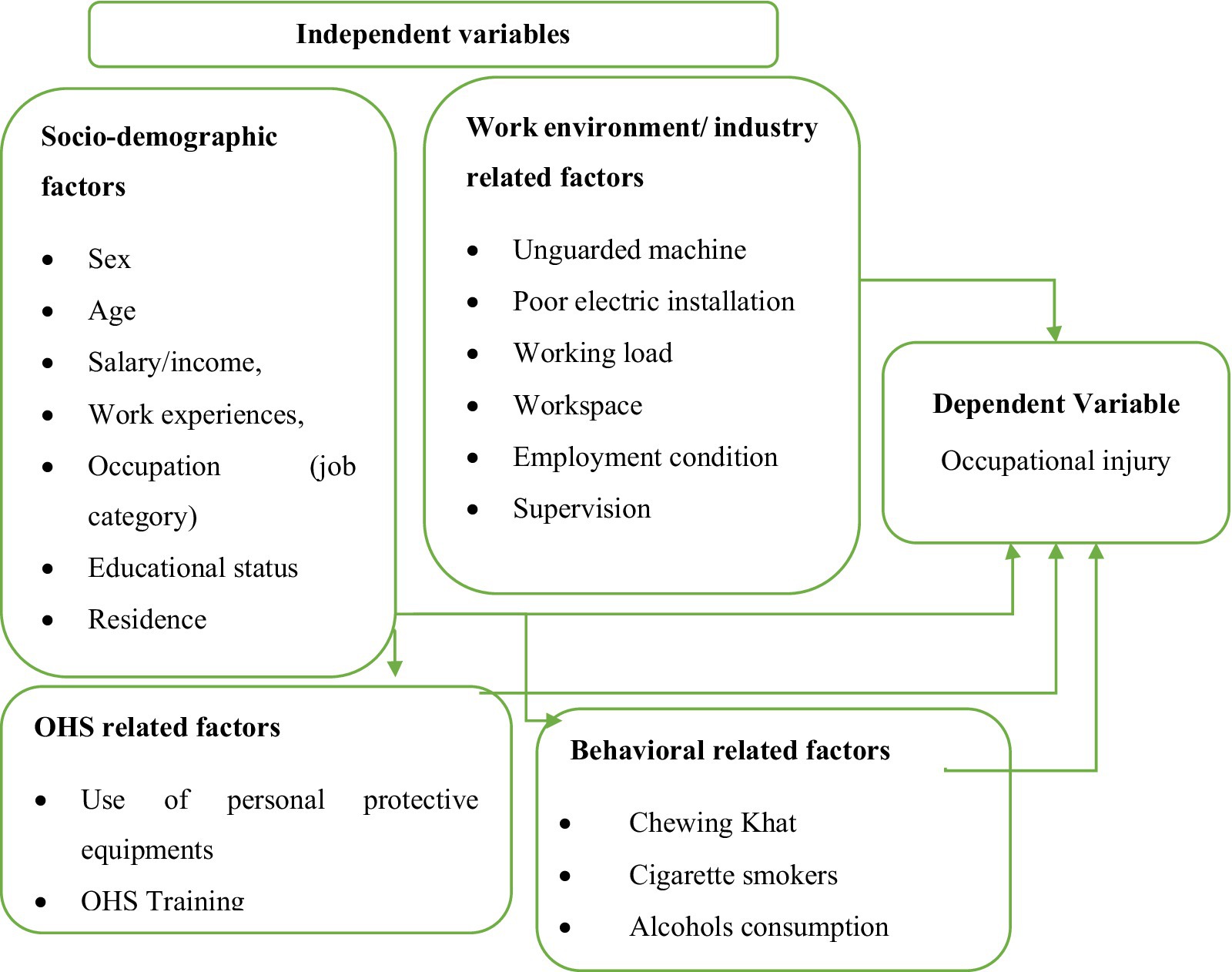
Figure 1. Conceptual framework used to assess factors associated with occupational related injury among small-scale industry workers (Developed by the investigator).
3 Materials and methods
3.1 Study area and period
The study was conducted in Harar town, Eastern Ethiopia, from March 12, 2023 to June 1, 2023. Harar town is located approximately at 520 km from Ethiopia’s capital city, Addis Ababa, and lies at a latitude of 9°19′N and a longitude of 42°7′E. According to the 2015/2016 census, Harari Regional state has a population of 255,690. Harar town has 1,025 SSIs and 3,151 workers in industries such as woodworking, metalworking, construction, and concrete.
3.2 Study design
A cross-sectional study design with quantitative data analysis methods was employed to assess the prevalence of occupational injuries and associated factors among scale industry workers in Harare town.
3.3 Source and study population
All small scale industry workers working in Harare town were a source population, while small scale workers working in the selected industries; woodworking, metalworking, construction, and concrete/stone industries were a study population.
3.4 Inclusion and exclusion criteria
All small-scale industry workers in Harare town who were available during the study period were included in the research. Workers who were on annual leave or who were seriously ill during the data collection period were excluded from the study.
3.5 Sample size determination and sampling techniques
The sample size for the study was calculated using a prevalence rate of 35.98% from a previous study (29), with a 5% margin of error, a 95% confidence interval, and a design effect of 2. Considering a 10% nonresponse rate (58 participants), the total sample size required was 639.
Study participants were selected via a simple random sampling technique after proportional allocation to the required sample size for each SSI category. The SSIs were first stratified on the basis of their type, and then participants were randomly selected from each stratum to ensure representative sampling (Figure 2).
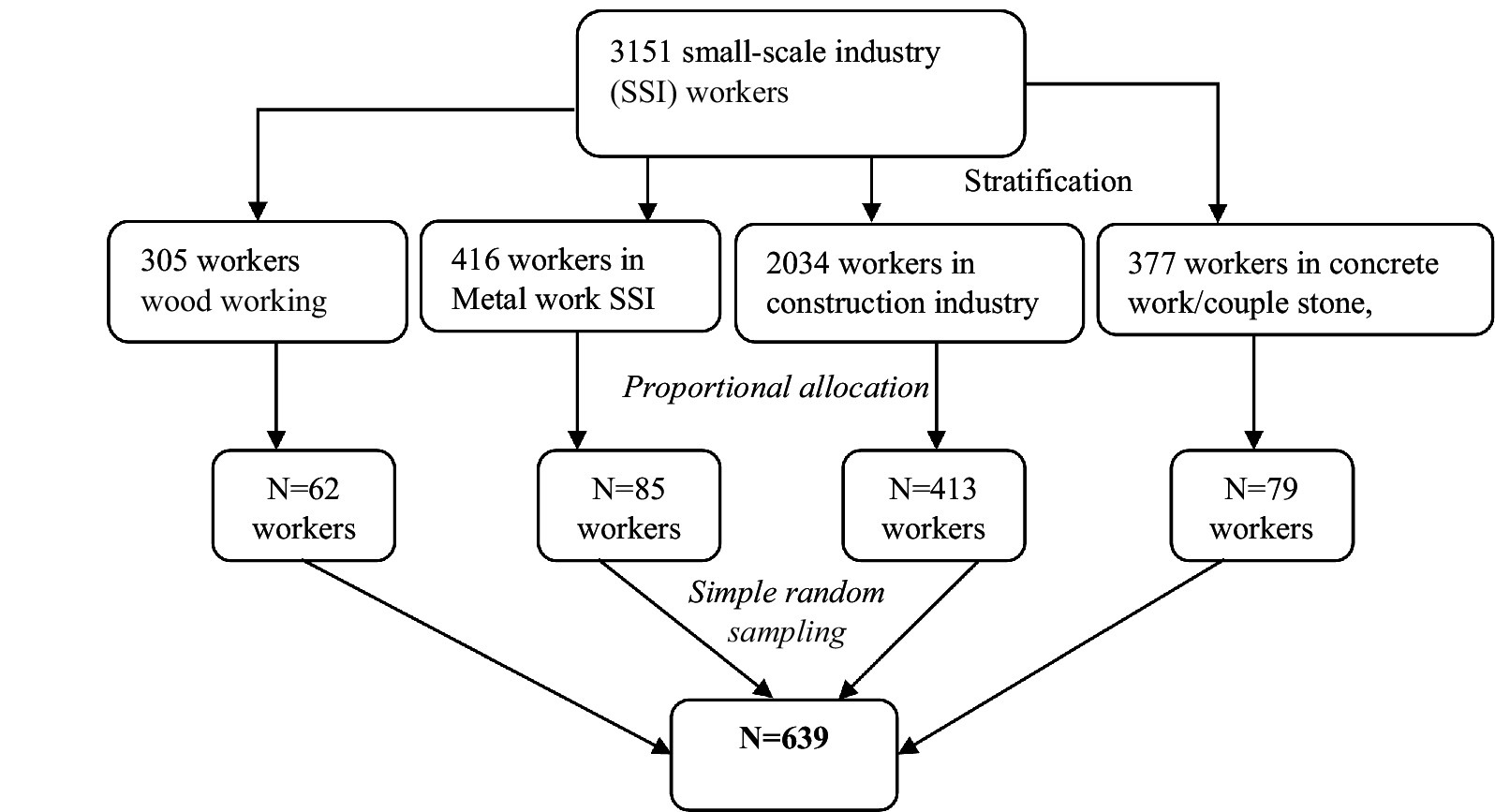
Figure 2. Sampling technique/procedures to be employed in selecting small scale industry workers found in Harare Town, 2023.
3.6 Data collection method
Four BSc holders’ health professionals were involved in data collection to collect all the data required for the study under the guidance of one superior and principal investigator during data collection. A pre-tested structured questionnaire and observational checklist were used to collect data on the following section; sociodemographic characteristics (10 questions), occupational injuries (8 questions), OHS-related factors (10 questions), work environment factors (6 questions), and behavioral-related factors (6 questions). The questionnaire was adapted from the WHO, OSHA, and Ethiopian national guidelines. Moreover, an observational checklist was applied to triangulate the quantitative data. The questionnaire was subsequently translated into the local languages of the study participants, Afan Oromo and Amharic.
3.7 Study variables
Dependent variable: Occupational-related injuries.
Independent variables:
• Sociodemographic aspects (sex, age, income, work experience, occupation, risk perception, educational status, and SSIs ownership)
• OHS-related factors (personal protective equipment, OHS training, and the availability of PPE)
• Work environment conditions (including lighting, workload, workspace, and supervision)
• Behavioral factors (chewing khat, cigarette smoking, and alcohol consumption).
3.8 Data quality control
Before data collection, the questionnaire was pretested in selected SSIs in Haramaya town, Eastern Ethiopia, to assess the clarity, sequence, and relevance of the questions and to estimate the time required for each respondent. Data collectors and supervisors received 1 day of training on the principles, ethics, procedures, and tools used in the study. The principal investigator closely monitored the data collection process, and all completed questionnaires were reviewed daily for consistency and completeness.
3.9 Data processing and analysis
The data were entered, cleaned, and analyzed using SPSS version 22 software. Descriptive statistics, including frequencies and proportions, were used to summarize the data. Bivariate and multivariate logistic regression analyses were employed to assess associations between dependent and independent variables. The crude odds ratio (COR) and adjusted odds ratio (AOR) with 95% confidence intervals were used to describe the relationships between risk factors and occupational injury exposure. Finally, the results are presented in text, tables, and figures. A p value of 0.2 was considered as the cut-off for statistical significance in the bivariate analysis, whereas a p value of 0.05 was used for multivariate analysis.
4 Results
4.1 Sociodemographic characteristics
The survey included 639 small-scale industry workers, of whom 634 provided responses, resulting in a high response rate of 98.6%. Among the respondents, 84.2% were male, and the mean age was 29.04 ± 6.02 years. A significant majority of the workers (93.7%) were temporarily employed and worked more than 8 h each day. Among the study participants, 43.4% had attended elementary school, and 4.6% had no formal education. The income for 76% of the workers ranged from 36.5 to 72.1 USD, with a mean of 50.4 ± 26.6 USD. In terms of the number of years of service in the SSIs, 44.6% had 4–6 years of experience, whereas 38.5% had 3 or fewer years (Table 1).
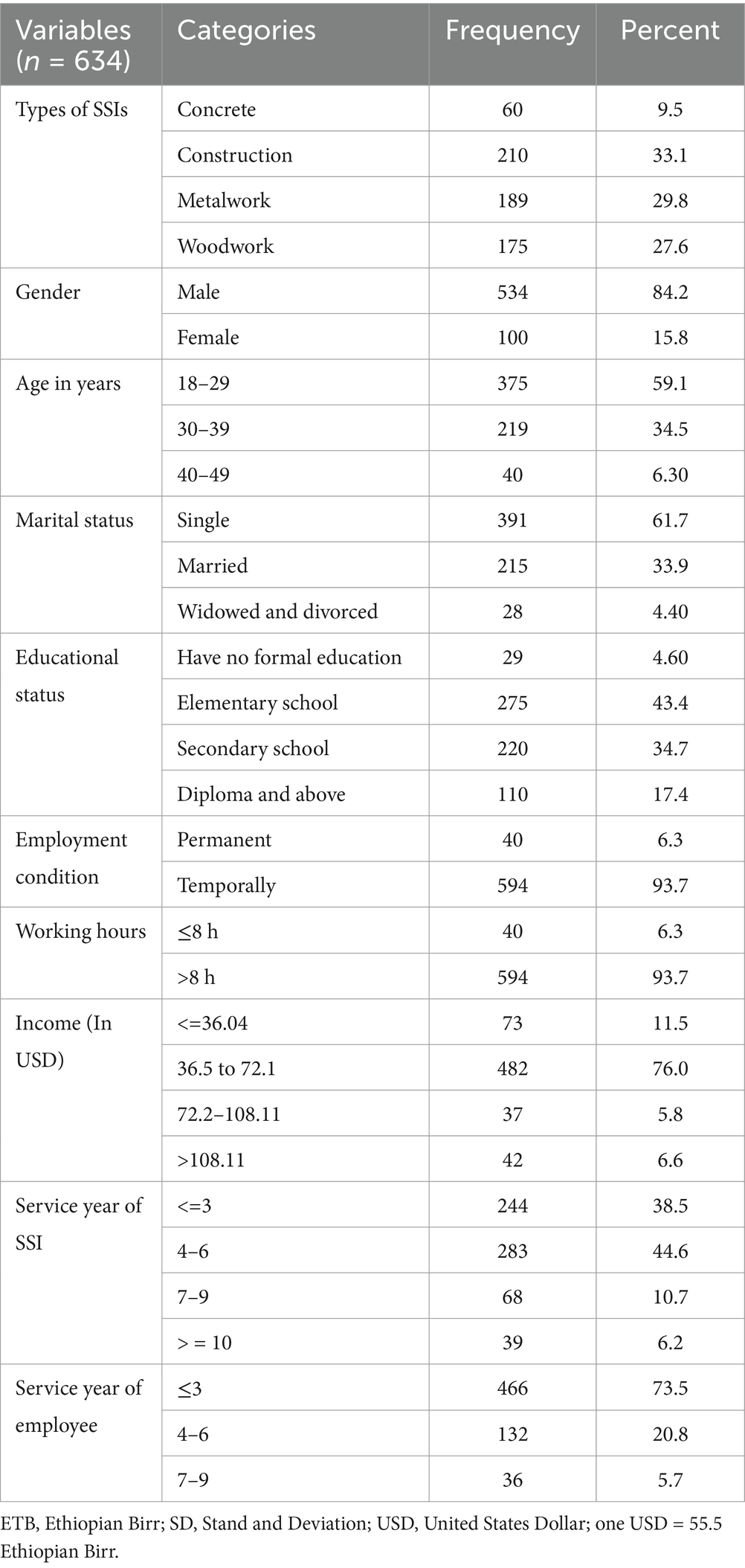
Table 1. Sociodemographic characteristics of small-scale industry workers in Harare town, Ethiopia, 2023.
4.2 Occupational health and safety practice
Among the 634 SSIs workers surveyed, 601 (94.8%) did not have personal protective equipment (PPE), such as gloves, gowns, face shields, or earplugs. Gowns and safety clothing were unavailable for 579 (91.3%) of the SSIs. Only 27 (4.26%) of the workers were reported having adequate PPE. Additionally, 49 (7.7%) of the workers had received training on occupational health and safety. Adequate lighting and workspace were present in 516 (81.4%) and 490 (77.3%) of the SSIs, respectively. Materials were not properly secured in 583 (92.0%) of the SSIs, and only 7 (1.1%) of the SSIs had a first-aid kit (Table 2).
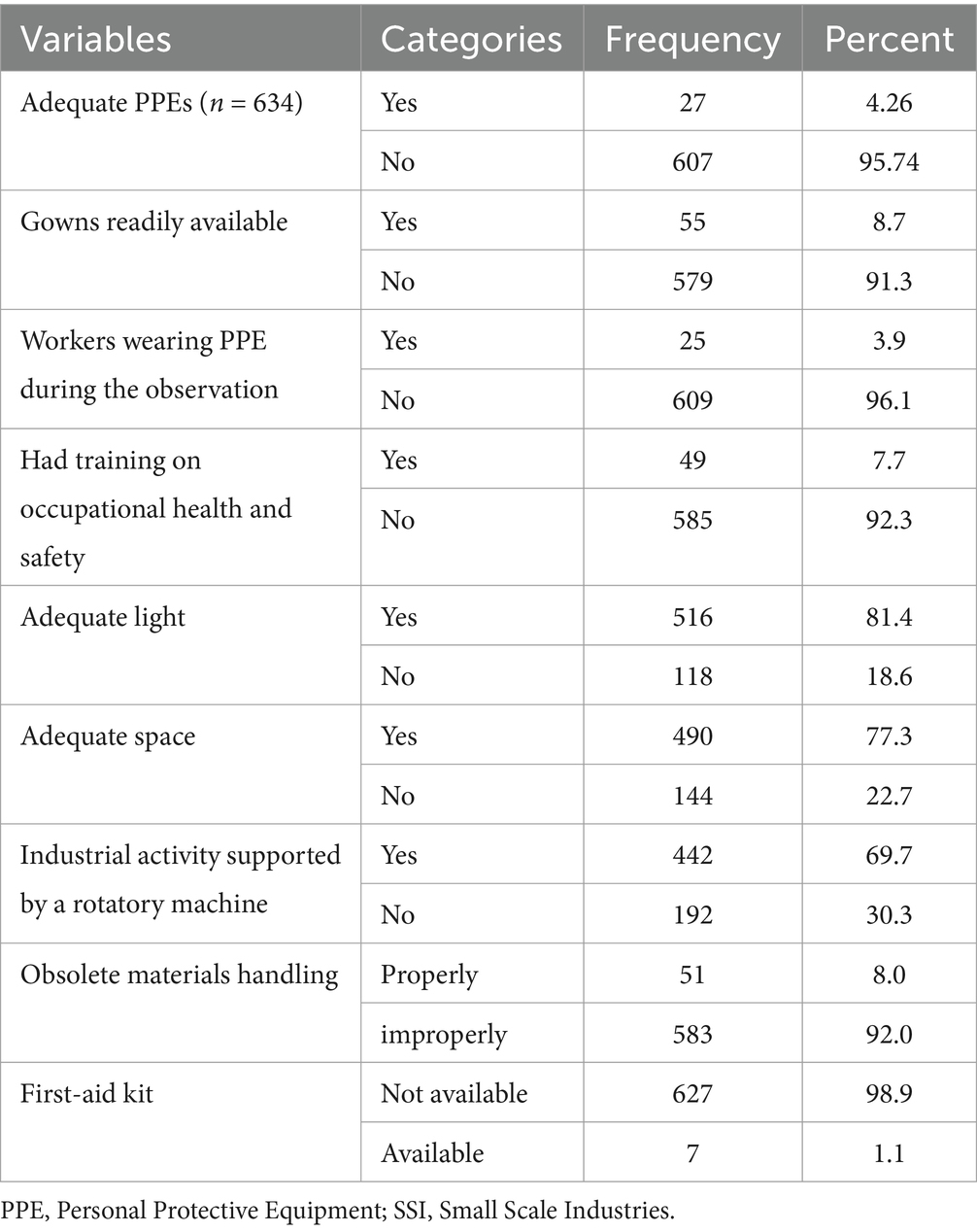
Table 2. Occupational health and safety practices among small-scale industry owners and workers, 2023.
4.3 Occupational exposure to injury among SSI workers
Among the 634 SSI workers, 417 (65.8%) experienced injuries at some point in their careers. Of these, 223 (35.2%) had injuries in the past year, and 182 (28.7%) had injuries in the last month. The most common types of injuries were abrasions (189, 45.3%), cuts (155, 37.2%), burns (56, 13.4%), and fractures (17, 4.1%). Only 58 (13.9%) workers reported their injuries to the relevant authorities; of these, no action was taken in 28 cases (48.3%), 14 (24.1%) received treatment, and 16 (27.6%) were given rest for 2 days. The most frequently injured body parts were hands (349, 34.1%), legs (298, 29.1%), and fingers (273, 26.7%; Figure 3).
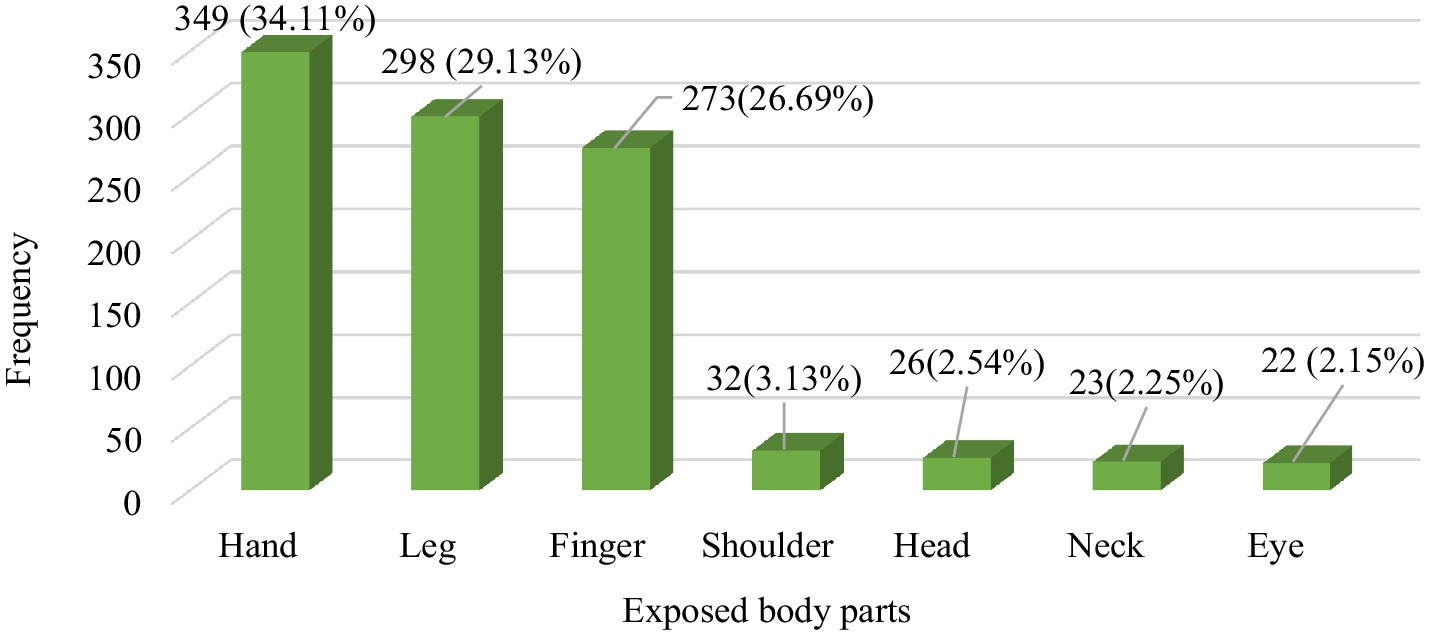
Figure 3. Prevalence (episode) of injuries to exposed body parts, 2023 (n = 1,023).
On the other hand, the current study revealed that the most common causes of injury were machines and hand tools, which accounted for 398 (38.9%) and 258 (25.22%) cases, respectively (Figure 4).
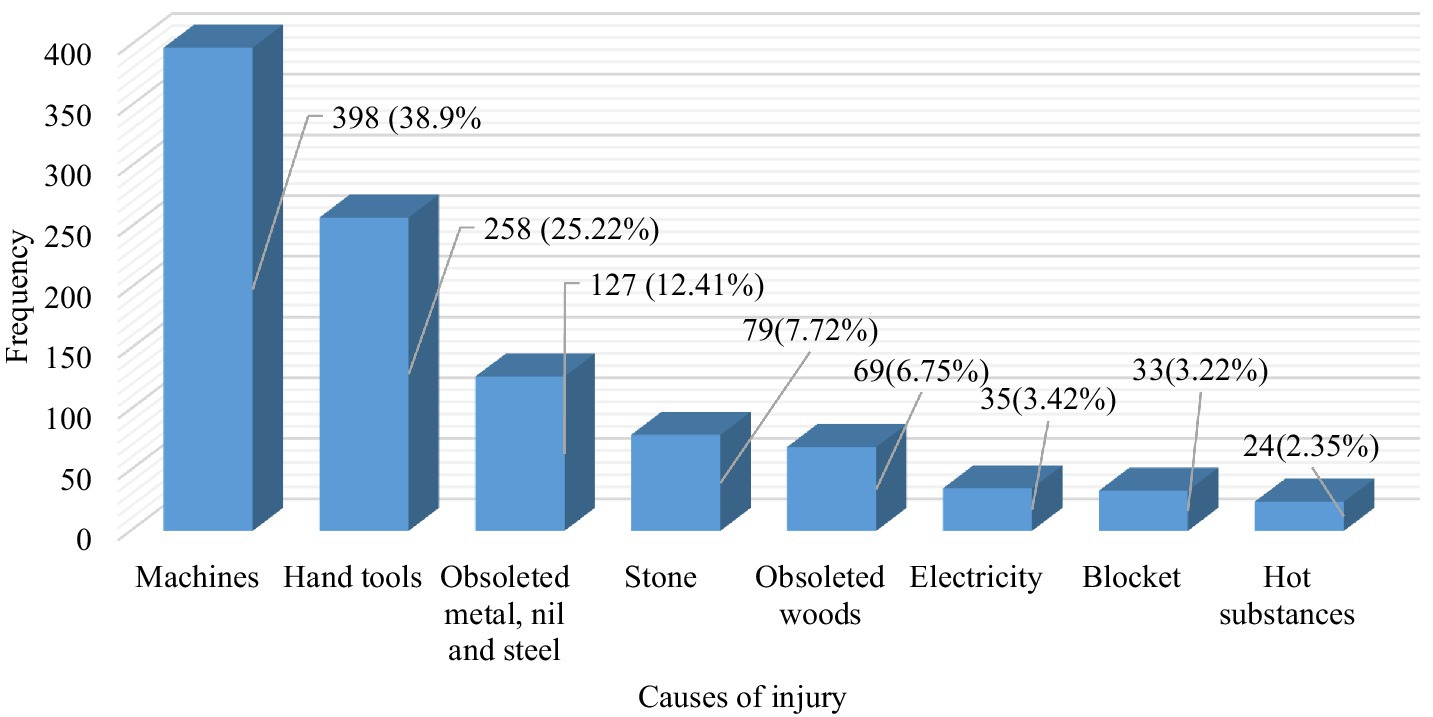
Figure 4. Causes of occupational injury among small-scale industry workers, 2023 (n = 1,023).
4.4 Behavioral-related practice
Among the 634 SSI workers, 363 (57.3%) drank alcohol, 283 of whom drank alcohol 1–3 times a week, whereas 80 (22.04%) drank more than three times. Furthermore, 211 (33.3%) of the SSI workers smoked at least one stick of tobacco cigarettes each day, of which 72 (34.12%), 118 (55.92%) and 9.95% of the workers smoked one to three, 4 to 6 and 7–9 sticks of cigarettes, respectively. On the other hand, 610 (96.2%) SSI workers chewed khat, 598 (97.75%) of whom chewed khat more than twice a week, whereas the remaining 12 (2.25%) chewed khat ≤2 times a week.
4.5 Factors associated with occupational related injury among SSI workers
According to the bivariate analysis, SSI workers working in the concrete and metalwork industries were approximately 3.42 times and 1.73 times more likely to be exposed to occupational injury, respectively, than those working in the woodwork industry were. There was a significant association between exposure to injury and the age of the SSI workers, who were in the range of 30–39 years old in comparison to those who were 40–49 years old.
The finding from the multivariate analysis revealed that SSI workers in the concrete industry were approximately 2.41 times more likely (AOR: 2.41, 95% CI: 1.07, 5.46) to be exposed to occupational injuries than those in the woodworking industry were. There was no significant association between occupational injury and age groups; specifically, workers aged 18–29 years (AOR: 1.08, 95% CI: 0.37, 3.18) and 30–39 years (AOR: 1.95, 95% CI: 0.65, 5.82) did not significantly differ from those aged 40–49 years. Workers with no formal education were approximately 2.50 times more likely (AOR: 2.50, 95% CI: 1.01, 2.83) to experience occupational injuries than those with a certificate or higher education. Those who had not received training on occupational health and safety were 1.4 times more likely (AOR: 1.4, 95% CI: 1.35, 3.22) to be injured than those who had received training. Additionally, workers who worked more than 8 h a day were approximately 4.56 times more likely (AOR: 2.88, 95% CI: 2.78, 11.64) to be exposed to occupational injuries than those working 8 h or fewer daily (Table 3).
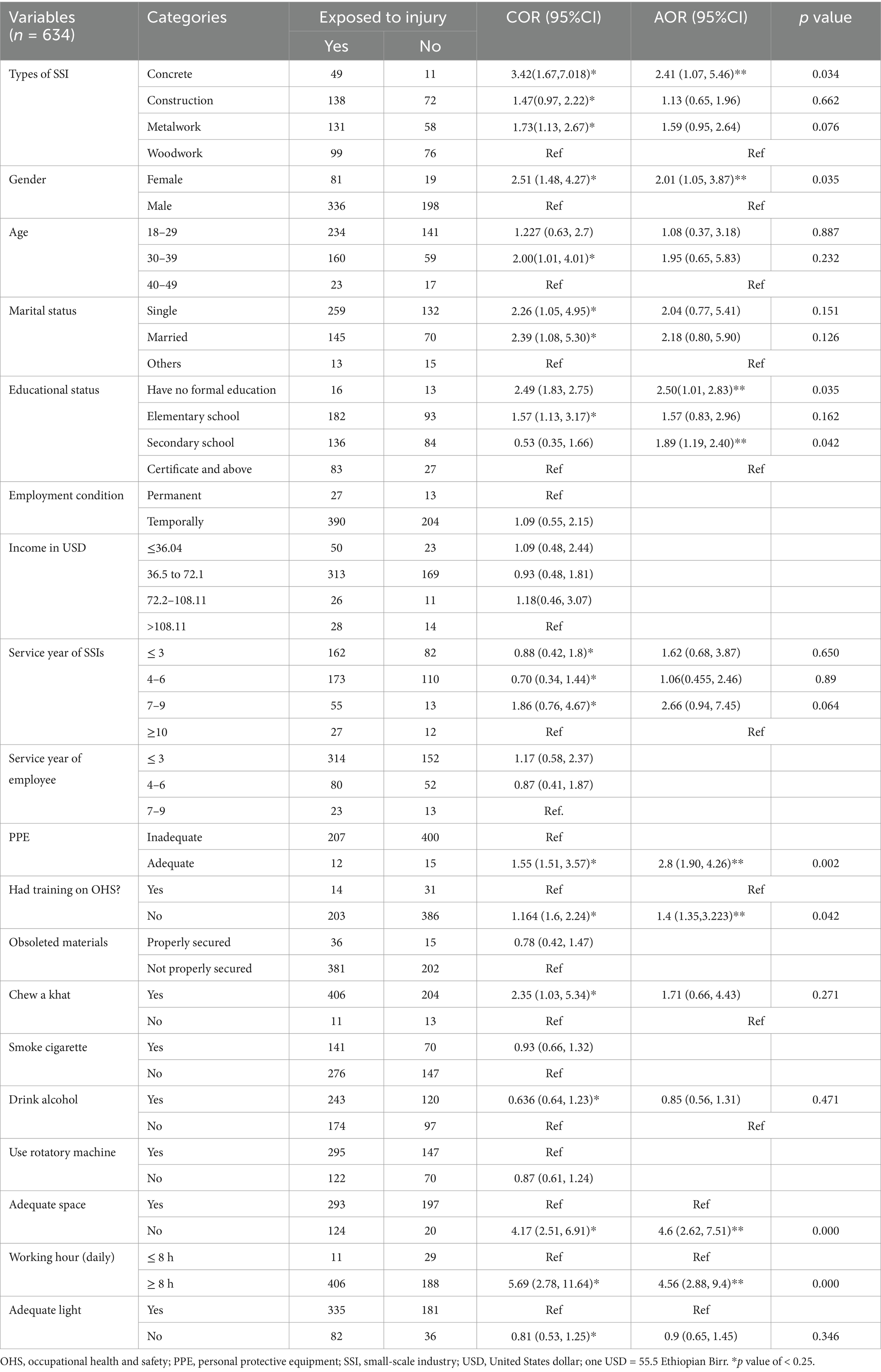
Table 3. Factors associated with occupational exposure to injury among small-scale industry workers working in Harare town, 2023.
5 Discussion
The current study revealed that 65.8% of small scale industry workers were exposed to occupational injuries, which is higher than the other finding reported 43.2% of workers exposed to occupational injuries (26). This discrepancy may be due to differences in the types of industry included in the study, educational levels, and implementation of health and safety practices.
Among the small scale industry workers exposed to occupational injuries, 35.2% had sustained injuries in the past year. This prevalence is higher than other findings reported in previous studies conducted in Bale, Ethiopia (26), Addis Ababa, Ethiopia (17), and Kampala, Uganda (30), which reported 30, 14.7, and 32.4% prevalence of occupational injuries, respectively. The variation in prevalence of occupational injury may be attributed to differences in occupational health and safety practices, access to or utilization of personal protective equipment, the types of small scale industries, and the characteristics of the study populations.
Furthermore, current study revealed that the most common body parts exposed to occupational injury were the hands, legs, and fingers, which accounted for 349 (34.11%), 298 (29.13%), and 273 (26.69%) exposure episodes, respectively. However, another study conducted in Addis Ababa, Ethiopia, reported that the prevalence of leg and finger/hand injuries among construction workers was 46.6 and 43.5%, respectively (31). The variation in the prevalence of occupational injuries among different body parts may be attributed to the workload, behavior-related factors, supportive supervision, or types of material or devices employed to implement the activities.
Furthermore, the current study revealed that 601 (94.8%) SSI workers did not use personal protective equipment, which was higher than the findings reported by a study conducted in Hawassa town, Ethiopia, which reported 57.4% of the workers did not access or lack PPE during their work (14). The difference in the utilization of personal protective equipment may be due to the variation in working environment-related factors, inadequate awareness, and lack of supervision on occupational health and safety The current study revealed that 594 (93.7%) small scale industry workers worked more than 8 h daily, which was significantly greater than the findings of another study conducted in Addis Ababa, Ethiopia, which reported that 8.1% of the employees had working less than 8 h per day (31). Furthermore, the current study revealed that only 49 (7.7%) SSI workers had training on occupational health and safety, which was lower than the findings reported from Addis Ababa City in 2015, which report 16.0% of employees had received workplace safety training (31). These differences may be due to variations in the implementation of occupational health and safety (OHS) practices and the availability of supportive supervision from both governmental and nongovernmental organizations.
The findings from multivariate analysis revealed that small scale industry workers working in the concrete industry were approximately 2.41 times (AOR: 2.41, 95% CI: 1.07, 5.46) more likely to be exposed to occupational injury, whereas those working in the metal industry were 1.59 times (AOR: 1.59, 95% CI: 1.02, 2.64) more likely to be exposed to injury than woodwork industry workers. The findings of the present study were in line with those of another study conducted in Mekele City, Ethiopia, in 2013, which reported that being a metal worker [AOR: 3.17, 95% CI: 2.07–4.85] or a woodworker [AOR: 2.34, 95% CI: 1.39–3.92] was associated with high prevalence of occupational injury. Furthermore, the findings of the current study are supported by another study conducted in Addis Ababa, Ethiopia, that reported an association between occupational injury and job categories (AOR: 3.52, 95% CI: 1.08, 11.41) (17). In general these findings highlight that the concrete and metal industries have greater risks of occupational injuries than the other industries. The increased risk may be due to different factors such as the nature of the work, implementation of occupational health and safety measures, and the overall working environment.
In addition, this study revealed that small scale industry workers working in industries with inadequate space are approximately 4.6 times (AOR: 4.6, 95% CI: 2.62, 7.51) more likely to be exposed to occupational injury than those working in industries with adequate space. This finding was in line with the finding from another study conducted in Addis Ababa, Ethiopia, which reported a significant association (AOR: 3.85; 1.14, 13.04) between inadequate work space and occupational injury among SSI workers (17).
According to the current study, small scale industry workers who had training or orientation toward occupational health and safety were 1.4 (AOR: 1.4, 95% CI: 1.35, 3.22) times more likely to be exposed to injury than those who had no training. This finding was supported by the findings reported by another study conducted in Ambo town, Ethiopia, which reported a significant association between occupational injury and training occupational health and safety (AOR: 2.05, 95% CI: 1.26–4.37) (27).
Small scale industry workers working more than 8 h daily are 4.56 times (AOR: 4.56, 95% CI: 2.88, 9.4) more likely to be exposed to occupational injury than those working less than 8 h daily. The finding of this study is in line with another finding reported by a study conducted in Mekele City, Ethiopia, which reported an association between occupational injury among small scale industry workers and workload [AOR = 2.73, 95% CI: 1.92–3.87].
In general, this study revealed that a significant proportion of small scale industry workers in Harare town experienced occupational injuries, with a notably high prevalence of injury. The findings highlight critical gaps in occupational health and safety practices, including the need for improved PPE utilization, enhanced safety training, and better workspace conditions. Addressing these issues could significantly reduce the risk of occupational injuries among SSI workers.
5.1 Limitation of the study
The current study mainly focused on the survey results aimed at determining the prevalence of occupational injuries among small-scale industry workers, and not addressed laboratory analysis. Therefore, the authors of this work recommend further studies that incorporate the laboratory analysis or experimental studies, particularly to determine the level of exposure for different hazards and assess the health risk. The future researcher should also consider how the cognitive challenges, emotional states, and work stress influence occupational health and safety practice as well as occupational injuries.
6 Conclusion
The current study revealed that more than 6 out of 10 small-scale industry workers were exposed to injuries during their career time, of which more than one-third of small-scale industry workers were exposed to occupational injuries in the last year. Furthermore, this study found a statistically significant association between occupational injuries and lower educational status, having no training, poor working conditions, and higher workloads. Therefore, the study highlights the need to implement occupational health and safety practices, including targeted training for small scale industry workers and supportive supervision, to reduce the risk of occupational injuries.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Haramaya University College of Health and Medical Science Institutional Health Research Ethics Review Committee (IHRERC). Ethical approval number: Ref. No. IHRERC/025/2021. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
DD: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Resources, Software, Validation, Visualization, Writing – original draft, Writing – review & editing. ST: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. NB: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. DM: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Supervision, Validation, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
AOR, adjusted odds ratio; COR, crude odds ratio; GDP, gross domestic product; ILO, International Labor Organization; LMICs, low- and middle-income countries; SSIs, small-scale Industries; WHO, World Health Organization.
References
1. Jerie, S . Occupational health and safety problems among workers in the wood processing industries in Mutare, Zimbabwe. J Emerg Trends Econ Manag Sci. (2012) 3:278–85.
2. El-Aziz, A, Ashraf, D, Gamal, D, and Emam, MH. The golden ratio in classical orders and interior design application mechanism. Int Design J. (2019) 9:119–29. doi: 10.21608/idj.2019.83430
3. Okun, A, Lentz, TJ, Schulte, P, and Stayner, L. Identifying high-risk small business industries for occupational safety and health interventions. Am J Ind Med. (2001) 39:301–11. doi: 10.1002/1097-0274(200103)39:3<301::AID-AJIM1018>3.0.CO;2-L
4. Nakata, A, Ikeda, T, Takahashi, M, Haratani, T, Hojou, M, Swanson, NG, et al. The prevalence and correlates of occupational injuries in small-scale manufacturing enterprises. J Occup Health. (2006) 48:366–76. doi: 10.1539/joh.48.366
5. Organization IL . Global trends on occupational accidents and diseases. World Day Saf Health Work. (2015) 1:1–7.
6. Khanzode, VV, Maiti, J, and Ray, PK. Occupational injury and accident research: a comprehensive review. Saf Sci. (2012) 50:1355–67. doi: 10.1016/j.ssci.2011.12.015
7. Hämäläinen, P, Takala, J, and Saarela, KL. Global estimates of occupational accidents. Saf Sci. (2006) 44:137–56. doi: 10.1016/j.ssci.2005.08.017
8. WHO . Occupational health program of WHO headquarters, Geneva, Switzerland. Global Occupational Health Network. (2003) 14:803–24.
9. Safety, I . Health at work: A vision for sustainable prevention: XX world congress on Safety and health at work 2014: Global forum for prevention, 24–27 august 2014, Frankfurt. Geneva: Germany/International Labour Office, ILO (2014).
10. International Labour Organization . Geneva: International Labour Office. 1–82. Available at: https://www.ilo.org/sites/default/files/wcmsp5/groups/public/@dgreports/@dcomm/documents/publication/wcms_686645.pdf (Accessed March 12, 2024).
11. MG SP, KSA, Rajendran, S, and Sen, KN. The role of psychological contract in enhancing safety climate and safety behavior in the construction industry. J Eng Design Technol. (2024) doi: 10.1108/JEDT-07-2023-0315
12. Gebremeskel, TG, and Yimer, T. Prevalence of occupational injury and associated factors among building construction workers in Dessie town, Northeast Ethiopia; 2018. BMC Res Notes. (2019) 12:1–6. doi: 10.1186/s13104-019-4436-4
13. Mersha, H, Mereta, ST, and Dube, L. Prevalence of occupational injuries and associated factors among construction workers in Addis Ababa, Ethiopia. J public health epidemiol. (2017) 9:1–8. doi: 10.5897/JPHE2016.0883
14. Girma, B, Ejeso, A, Ashuro, Z, and Birhanie, AM. Occupational injuries and associated factors among small-scale woodwork industry workers in Hawassa, southern Ethiopia: a cross-sectional study. Environmental health insights. (2022) 16:11786302221080829. doi: 10.1177/11786302221080829
15. Mengistu, HG, Alemu, DS, Alimaw, YA, and Yibekal, BT. Prevalence of occupational ocular injury and associated factors among small-scale industry workers in Gondar town, Northwest Ethiopia. Clin Optom. (2019) 13:167–74. doi: 10.2147/OPTO.S290257
16. Benti, A, Kumie, A, and Wakuma, S. Prevalence of occupational injury and associated factors among workers in large-scale metal manufacturing factories in Addis Ababa, Ethiopia. Ethiop J Health Dev. (2019) 33:94–101.
17. Mulugeta, H, Tefera, Y, and Gezu, M. Nonfatal occupational injuries among workers in microscale and small-scale woodworking enterprise in Addis Ababa, Ethiopia. J Environ Public Health. (2020) 2020:1–8. doi: 10.1155/2020/6407236
18. Patel, V, Chesmore, A, Legner, CM, and Pandey, S. Trends in workplace wearable technologies and connected-worker solutions for next-generation occupational safety, health, and productivity. Adv Intell Syst. (2022) 4:2100099. doi: 10.1002/aisy.202100099
19. Engelbrecht, I, Horn, S, Badenhorst, CJ, and du Plessis, JL. Beyond the clock: revisiting occupational exposure limits (OELs) for unusual work schedules in the south African mining industry. Saf Sci. (2024) 176:106542. doi: 10.1016/j.ssci.2024.106542
20. Sankar, SS, and Anandh, K. Navigating leadership styles through qualitative exploration for enhanced safety in the construction sector. Saf Sci. (2024) 175:106495. doi: 10.1016/j.ssci.2024.106495
21. ILO . International Labour Organization. Safety and health at work. (2023). Available at: https://www.ilo.org/global/topics/safety-and-health-at-work/lang--en/index.htm. (December 21, 2024).
22. Rajendran, S . Enhancing construction worker safety performance using leading indicators. Pract Period Struct Des Constr. (2013) 18:45–51. doi: 10.1061/(ASCE)SC.1943-5576.0000137
23. Wanberg, J, Harper, C, Hallowell, MR, and Rajendran, S. Relationship between construction safety and quality performance. J Constr Eng Manag. (2013) 139:04013003. doi: 10.1061/(ASCE)CO.1943-7862.0000732
24. Derdowski, LA, and Mathisen, GE. Psychosocial factors and safety in high-risk industries: a systematic literature review. Saf Sci. (2023) 157:105948. doi: 10.1016/j.ssci.2022.105948
25. Hofmann, DA, Burke, MJ, and Zohar, D. 100 years of occupational safety research: from basic protections and work analysis to a multilevel view of workplace safety and risk. J Appl Psychol. (2017) 102:375–88. doi: 10.1037/apl0000114
26. Dida, N, Darega, J, Lemesa, F, Kassim, J, and Woldemichael, B. Occupational injury and its correlated factors among small-scale industry workers in towns of bale zone, Southeast Ethiopia. J Environ Public Health. (2019) 2019:1–8. doi: 10.1155/2019/4987974
27. Daba, C, Atamo, A, and Gebrehiwot, M. Small scale enterprise workers require attention: what predicts the level of occupational injuries? Environmental health insights. (2022) 16:11786302221104949. doi: 10.1177/11786302221104949
28. Berhe, A, Yemane, D, Gebresilassie, A, Terefe, W, and Ingale, L. Magnitude of occupational injuries and associated factors among small-scale industry workers in mekelle city, northern Ethiopia. Occupational Med Health Affairs. (2015) 3, 1–6. doi: 10.4172/2329-6879.1000197
29. Molla, GA, Salgedo, WB, and Lemu, YK. Prevalence and determinants of work related injuries among small and medium scale industry workers in Bahir Dar town, north West Ethiopia. Annals of occup environ med. (2015) 27:1–6. doi: 10.1186/s40557-015-0062-3
30. Kiconco, A, Ruhinda, N, Halage, AA, Watya, S, Bazeyo, W, Ssempebwa, JC, et al. Determinants of occupational injuries among building construction workers in Kampala City. Uganda BMC Public Health. (2019) 19:1–11. doi: 10.1186/s12889-019-7799-5
Keywords: injury, occupational injury, small-scale industry, Harar town, work place, Ethiopia
Citation: Debelu D, Tolera ST, Baraki N and Mengistu DA (2025) Prevalence of occupational injuries and associated factors among small scale industry Workers in Harar Town, eastern Ethiopia. Front. Public Health. 13:1532799. doi: 10.3389/fpubh.2025.1532799
Edited by:
Paulo Santos, University of Coimbra, PortugalReviewed by:
K. S. Anandh, Faculty of Engineering and Technology, IndiaKamal Selvaraj, Annamalai University, India
Copyright © 2025 Debelu, Tolera, Baraki and Mengistu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Desi Debelu, ZGVzaWRlYmVsdUBnbWFpbC5jb20=