 Xingmin Wei
Xingmin Wei Lu Liu
Lu Liu Kun Liu3
Kun Liu3- 1School of Public Health, Gansu of Chinese Medicine, Lanzhou, China
- 2The Collaborative Innovation Center for Prevention and Control by Chinese Medicine on Disease Related Northwestern Environment and Nutrition, Lanzhou, China
- 3Department of Epidemiology, School of Public Health, Air Force Medical University, Xi’an, China
Objectives: Trichomoniasis one of the most neglected sexually transmitted diseases (STDs), imposes a significant global disease burden. This study aims to assess the burden and trends of trichomoniasis from 1990 to 2021 and to project its incidence from 2022 to 2050.
Methods: This study utilized data from the Global Burden of Disease 2021 study for secondary analysis. We determined the age-standardized incidence rate (ASIR) and disability-adjusted life years (DALYs) of trichomoniasis by sex, age, and socio-demographic index (SDI) level. Changes in burden trends across sex and age were explored from 1990 to 2021, using joinpoint regression. The incidence of trichomoniasis was projected for the period 2022 to 2050, using R software.
Results: From 1990 to 2021, the estimated annual percentage change (EAPC) in the global ASIR of trichomoniasis was 0.09 (95% CI: 0.06 to 0.13). In 2021, the global ASIR of trichomoniasis was 4,133.41 per 100,000 people (95% UI: 3,111.37 to 5,583.56 per 100,000). By population group, the ASIR was higher in men (4,353.43 per 100,000) than in women (3,921.31 per 100,000) in 2021, while the DALY rate was significantly higher in women than in men (6.45 vs. 0.23 per 100,000). When divided by age groups, the trend in ASIR among women aged 30–54 years aligned closely with the overall population incidence trend. In 2021, ASIRs were highest in low SDI regions, and the projected ASIRs by 2050 are 5,680.57 per 100,000 in males and 5,749.47 per 100,000 in females.
Conclusion: Trichomoniasis represents a significant global disease burden, particularly among women in low-income areas and individuals aged 30–54 years. The study highlights the need for targeted strategies to reduce the burden of trichomoniasis-related infections, especially in vulnerable populations.
Introduction
Trichomoniasis is a sexually transmitted disease (STD) caused by Trichomonas vaginalis (1), which spreads primarily through sexual contact, although rare cases involve transmission via contaminated objects (2). Traditionally, a diagnosis is confirmed by detecting Trichomonas in vaginal discharge under a microscope. However, in recent years, it has also been possible to obtain a diagnosis through a single rapid nucleic acid diagnostic test (3). Among symptomatic patients, the most common clinical manifestations are female vaginitis and male urethritis (4), though most men with Trichomonas infection are asymptomatic (5). Additionally, Trichomonas infection increases the risk of human immunodeficiency virus (HIV) transmission, other sexually transmitted infections, pelvic inflammatory disease, and cervical cancer (6, 7). Although trichomoniasis is a relatively common sexually transmitted disease with harmful effects, there is currently no regular screening for any population group except women living with HIV.
According to the latest estimates of the World Health Organization, in 2020, the incidence rate of trichomoniasis among those aged 15–49 was 38.0 per 1,000 in females and 41.0 per 1,000 in males (8). There were 156 million new cases of Trichomonas vaginalis infection (73.7 million in females and 82.6 million in males) (9). A study in Nigeria revealed that the highest prevalence of trichomoniasis (31.9%) was found among individuals aged 38–47 years (39.3%), married adults (76.3%), and those with secondary education (68.9%) (10). A study conducted at a Spanish tertiary care hospital reported a Trichomonas vaginalis prevalence of 0.8%, though fewer than 20% of patients with trichomoniasis were fully screened for other genital pathogens (11). These findings highlight the growing burden of trichomoniasis and underscore the importance of integrating routine vaginal testing for trichomoniasis with gynecological examinations.
Although previous studies have provided valuable insights into the prevalence of trichomoniasis, they have not comprehensively examined long-term trends in its global burden. While the disease is increasingly recognized as a significant yet underemphasized STD, there remains a gap in understanding its temporal dynamics across different regions and populations. Furthermore, while existing data highlight the high burden of trichomoniasis, especially in certain demographic groups, there is limited research on projecting future trends in its incidence.
To address the gaps in understanding the long-term trends and future projections of trichomoniasis, we conducted a comprehensive analysis based on the 2021 Global Burden of Disease (GBD) study.1 We extracted data on trichomoniasis incidence and population from this database for the years 1990–2021, with two primary objectives: first, to explore trends in the global and regional burden of trichomoniasis from 1990 to 2021; and second, to project the burden of trichomoniasis incidence through 2050. By analyzing these trends, we aim to provide valuable insights into how the burden of trichomoniasis may evolve in the coming decades. Our findings will help guide public health efforts, inform policy decisions, and shape targeted interventions necessary to address the rising global burden of trichomoniasis, especially in vulnerable populations.
Methods
Data source
The burden of disease data used in this study were obtained from the Global Burden of Disease (GBD) 2021 study (see text footnote 1). The dataset is initiated and coordinated by the Institute for Health Metrics and Evaluation (IHME). It is a highly open and important resource that can be freely accessed and used by researchers worldwide, strongly promoting international exchanges and development in health research. The dataset has extensive data sources, covering national health statistics, reports from medical institutions, epidemiological surveys, census data, etc. The GBD 2021 has outstanding achievements. It has evaluated 369 diseases and 87 risk factors in 204 countries and 21 regions (12, 13) and these regions are subdivided into 5 SDI segments according to the Socio-Demographic Index (SDI) (14).
This dataset covers the period from 1990 to 2021 and encompasses numerous health indicators such as incidence, prevalence, mortality, disability-adjusted life years, maternal mortality, and exposure situations. It is of great significance in many fields, including public health policy-making, disease prevention and control strategy planning, health economics research, and epidemiological analysis. It builds a unified and standardized platform for researchers from various countries, greatly promotes global health research, facilitates cross-national and cross-regional comparisons and collaborations, and elevates the international exchanges in global health research to a new level.
In this study, the indicators of interest were selected from the GBD database, including data on the number of trichomoniasis cases, incidence rate, Disability-Adjusted Life Years (DALYs), and DALY rates between 1990 and 2021. These data were classified by gender, age, SDI groups, and regions. The age distribution was divided into <20 years old, >85 years old, and every five year intervals between 20 and 85 years old.
Evaluation indicators
The age-standardized rate (ASR), is designed to eliminate the influence of different age compositions when comparing incidence rates, DALYs (Disability-Adjusted Life Years), and other data among different populations. Among them, αi and wi, respectively, stand for the age-specific rate and weight of the i-th age group (15).
The Socio-Demographic Index (SDI) provides a comprehensive picture of the development of a country or region. It includes indicators such as the average educational level of women under 25 years old and per capita income.
The Estimated Annual Percentage Change (EAPC) is an indicator used to describe the changes in the ASR between 1990 and 2021. It can demonstrate the long-term trends of the ASR in relation to the disease burden of trichomoniasis. Specifically, the EAPC is obtained by fitting the natural logarithm of the ASR to the calendar years and then applying a regression model. In this formula, β represents the positive or negative trend of the ASR (15). This study used EAPC with 95% confidence intervals (CI) to represent annual changes in ASR from 1990 to 2021 (16).
Statistical analysis
EAPC was used in this study to quantify trends in the burden of trichomoniasis. Changes in the age-standardized incidence rate (ASIR) were used to inform prevention strategies.
Joinpoint regression analyses were performed with Joinpoint 5.0 software from the American National Cancer Institute.2 The software was used to calculate the annual percentage change (APC) to characterize trends in the burden of disease across multiple phases (17).
The Monte Carlo permutation test was applied to evaluate the computational results of the software (18), with the significance level set at α = 0.05. If the p-value is less than 0.05, it indicates that the difference in results is statistically significant at the 5% significance level.
Compared with other methods, APC modeling is more flexible in parameter selection and prior probability distribution, making it more robust and reliable for prediction (19). Therefore, this study used the age-period cohort (APC) model to project the incidence of trichomoniasis by 2050. In the APC model, βi reflects the degree and direction of the impact of certain potential influencing factors in the i-th age group on the studied indicator.
All statistical analyses and data visualizations were performed in R (version 4.3.2), using the BAPC and ggplot2 packages. Map production was done using ArcGIS 10.8 system software. Subgroup analyses were conducted according to gender, age, SDI, and the 21 geographic locations. A p-value of <0.05 was considered statistically significant.
Results
Estimated global burden of trichomoniasis
The incidence of trichomoniasis has been increasing globally from 1990 to 2021, with a notable rise in 2021. In that year, the global ASIR of trichomoniasis infection was 4,133.41 per 100,000 people (95% UI: 3,111.37/100,000 to 5,583.56/100,000) (Table 1). In 2021, the total number of trichomoniasis cases was 3,419.16×105 (95% UI: 2,580.46×105 to 4,642.95×105), compared to 1,978.37×105 cases in 1990, representing a 73% increase from 1990 to 2021. The DALY rates for trichomoniasis showed a stable trend from 1990 to 2021, with a global ASR for DALY of 3.33 per 100,000 (95% UI: 1.37/100,000 to 7.12/100,000) in 2021 (Supplementary Table S1).
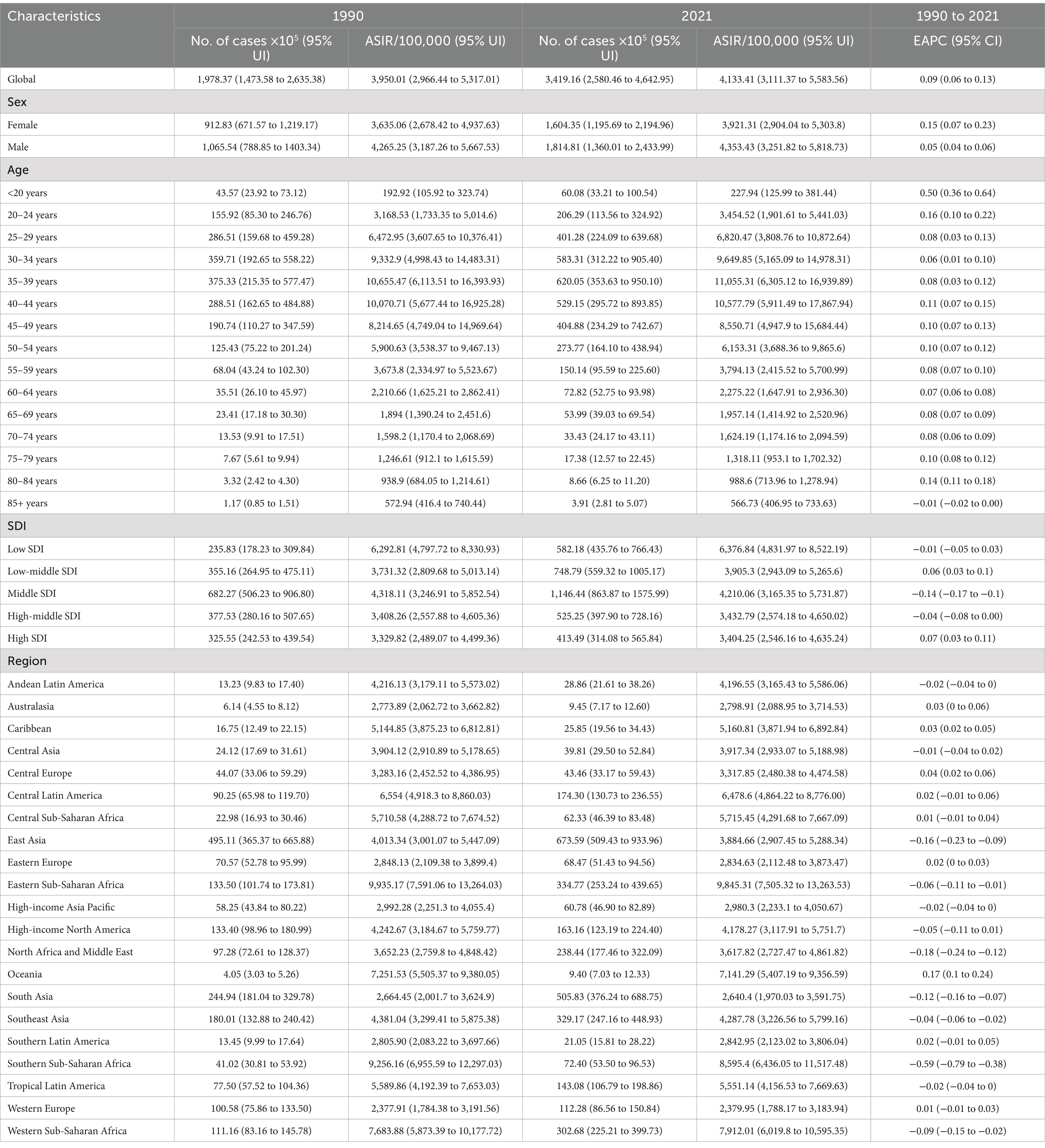
Table 1. Number of trichomoniasis cases, age-standardized incidence rates, and their temporal trends for 1990 and 2021.
From 1990 to 2021, men always had more cases of trichomoniasis infections than women did (Figure 1A), and the number of cases of trichomoniasis infections in men peaked at 1,814.81×105 (95% UI: 1,360.01×105 to 2,433.99×105) in 2021. Meanwhile a similarly higher ASIR in men compared to women, ASIR for men tops out at 4,353.43/100,000 (95% UI: 3,251.82/100,000 to 5,818.73/100,000) in 2021. However, the DALY and ASR for DALY are much higher for females than for males (Figure 1B), and the ASR of DALY for women was highest in 2021 at 6.45/100,000 (95% UI: 2.65/100,000 to 13.87/100,000).
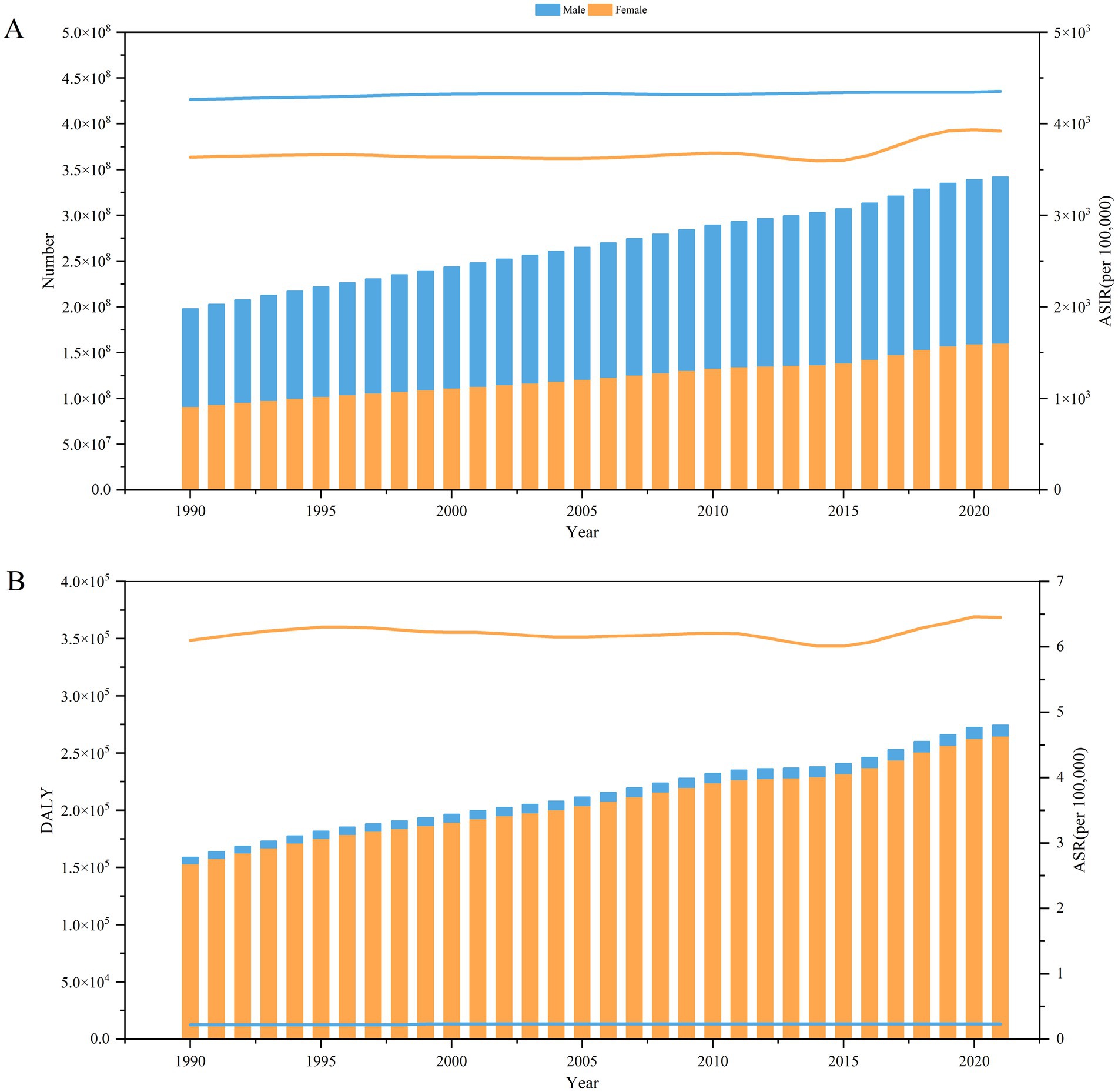
Figure 1. Burden of trichomoniasis by sex, 1990–2021. (A) Number of trichomoniasis cases (left) and ASIRs (right) by sex. (B) Trichomoniasis DALY (left) and ASR for DALY (right) by sex. ASIR, age-standardized incidence rate; DALY, disability-adjusted life year; ASR, age-standardized rate; SDI, Socio-demographic Index.
The number of cases of trichomoniasis infections from 1990 to 2021 increased in all age groups, while the EAPC was −0.01 (95% CI: −0.02 to 0.00) in the 85+ age group and positive in the rest of the age groups (Table 1). Indicates that except for the 85+ age group, ASIR for the rest of the population showed an overall increasing trend over the 30 years, with the fastest increase occurring in the <20 years age group. The three highest ASIRs for trichomonas infections in 2021 were 35 to 39 years (11,055.31/100,000), 40–44 years (10,577.79/100,000) and 30–34 years (9,649.85/100,000). DALY for trichomonas infection increased in all age groups from 1990 to 2021 (Supplementary Table S1).
The incidence of cases increased in all SDI regions over 32 years (Figure 2A). The highest increase in cases was in the low SDI region (147%), and the lowest in the high SDI region (27%). EAPC were positive in low-middle SDI and high SDI trichomoniasis ASIRs, and negative in the remaining SDI regions (Table 1). DALY for trichomoniasis infections from 1990 to 2021 increased in all five SDI regions, but the EAPC was negative in all SDI areas (Supplementary Table S1). This indicates a downward trend in ASR for DALY in all SDI regions over the last 32 years (Figure 2B).
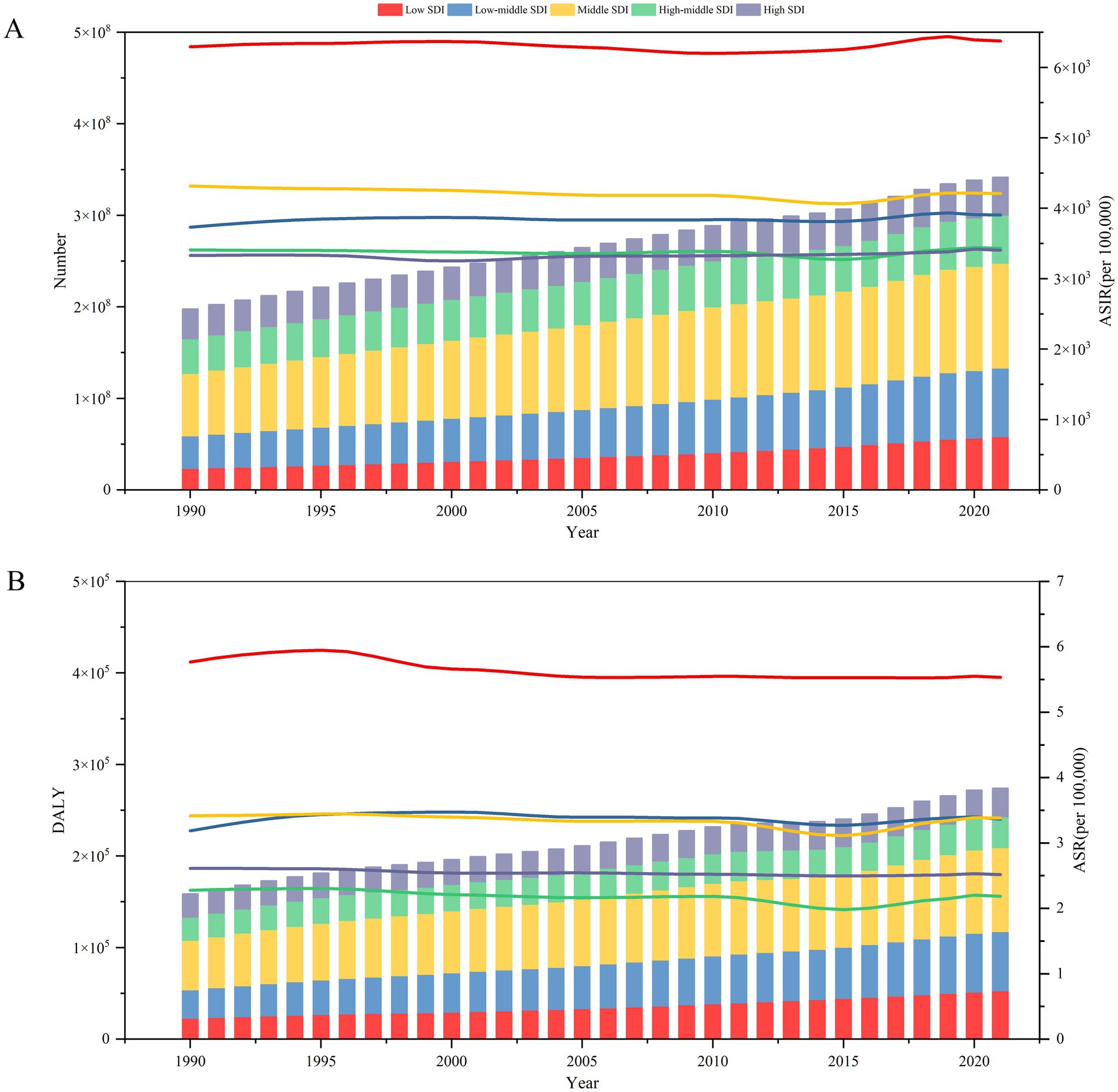
Figure 2. Burden of trichomoniasis by SDI, 1990–2021. (A) Number of trichomoniasis cases (left) and ASIRs (right) by SDI subgroup. (B) Trichomoniasis DALY (left) and ASR for DALY (right) by SDI subgroup. ASIR, age-standardized incidence rate; DALY, disability-adjusted life year; ASR, age-standardized rate; SDI, Socio-demographic Index.
The burden of trichomoniasis infection varies significantly between countries. The three countries with the highest ASIRs in 2021 are the United Republic of Tanzania, Zambia and Mozambique (Table 1 and Figure 3). China had the highest number of infections in 2021 (65,088,138) and the lowest was Tokelau (91). The highest ASIR is found in Eastern Sub-Saharan Africa, with the lowest being found in Western Europe (Table 1 and Figure 3). The ASIR by an average of 0.09 (95% CI: 0.06 to 0.13) per annum over the same period (from 3,950.01/100,000 in 1990 to 4,133.41/100,000 in 2021). The largest increase in ASIR was in Benin (EAPC = 0.27; 95% CI: 0.09 to 0.46), next is Morocco, and largest ASIR reduction was in South Africa (EAPC = −0.68). The highest ASIR and ASR for DALY 2021 are in Sub-Saharan Africa. The lowest ASIR and ASR for DALY in 2021 were in Western Europe.
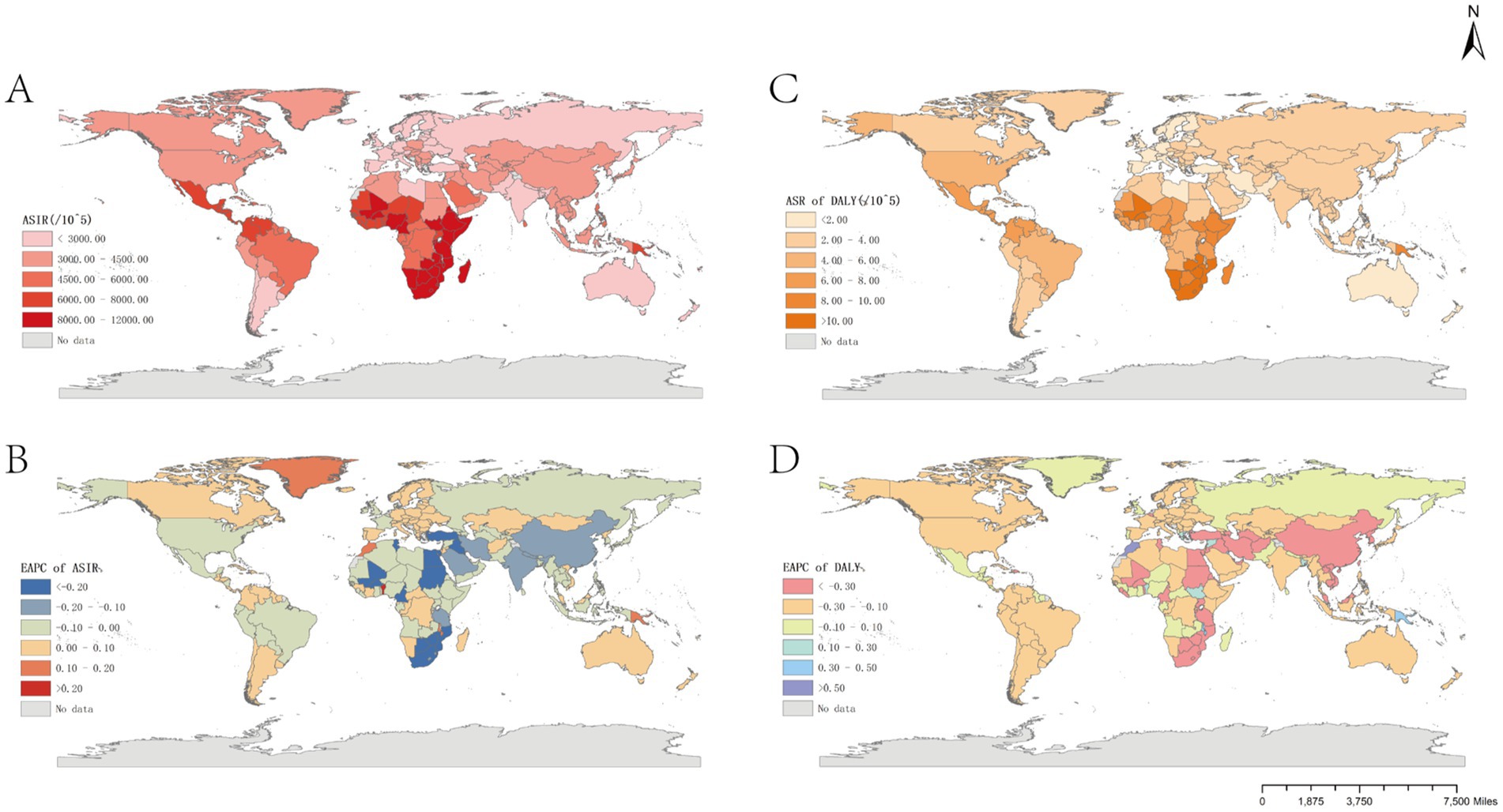
Figure 3. Global burden of trichomoniasis in 204 countries and territories. (A) ASIR in 2021. (B) EAPC for ASIR, 1990–2021. (C) ASR for DALY in 2021. (D) EAPC for ASR of trichomoniasis DALY, 1990–2021. ASIR, age-standardized incidence rate; EAPC, estimated annual percentage change.
Joinpoint analysis results
As shown in Supplementary Figure S1, joinpoint regression analysis identified the age-specific trends in the burden of trichomoniasis in men from 1990 to 2021. The ASIR for overall trichomoniasis in men showed a fluctuating increase up to age 69, followed by a fluctuating decrease after wards. Similarly, as shown in Supplementary Figure S2, joinpoint regression analysis revealed that from 1990 to 2021, the ASIR for age-specific trichomoniasis in women increased with some volatility up to age 84, but declined precipitously after age 85. The fastest-growing ASIR occurred in the 25–29 age group from 2015 to 2019 (APC = 3.37).
ASIR trends in the 30–54 year-old female population align with the overall population’s ASIR trends.
Incidence projections
The projected incidence of trichomoniasis from 2022 to 2050 was calculated based on trichomoniasis burden data from 1990 to 2021. The incidence for 2022 to 2050 was projected by sex using Bayesian age-period-cohort analysis. The findings show that overall, overall, the incidence of trichomoniasis is expected to increase significantly in the future, with a notable gender difference (Figure 4). The projected number of cases by 2050 is 4,873.70×105, with an ASIR projected to be 5,832.60 per 100,000 people.
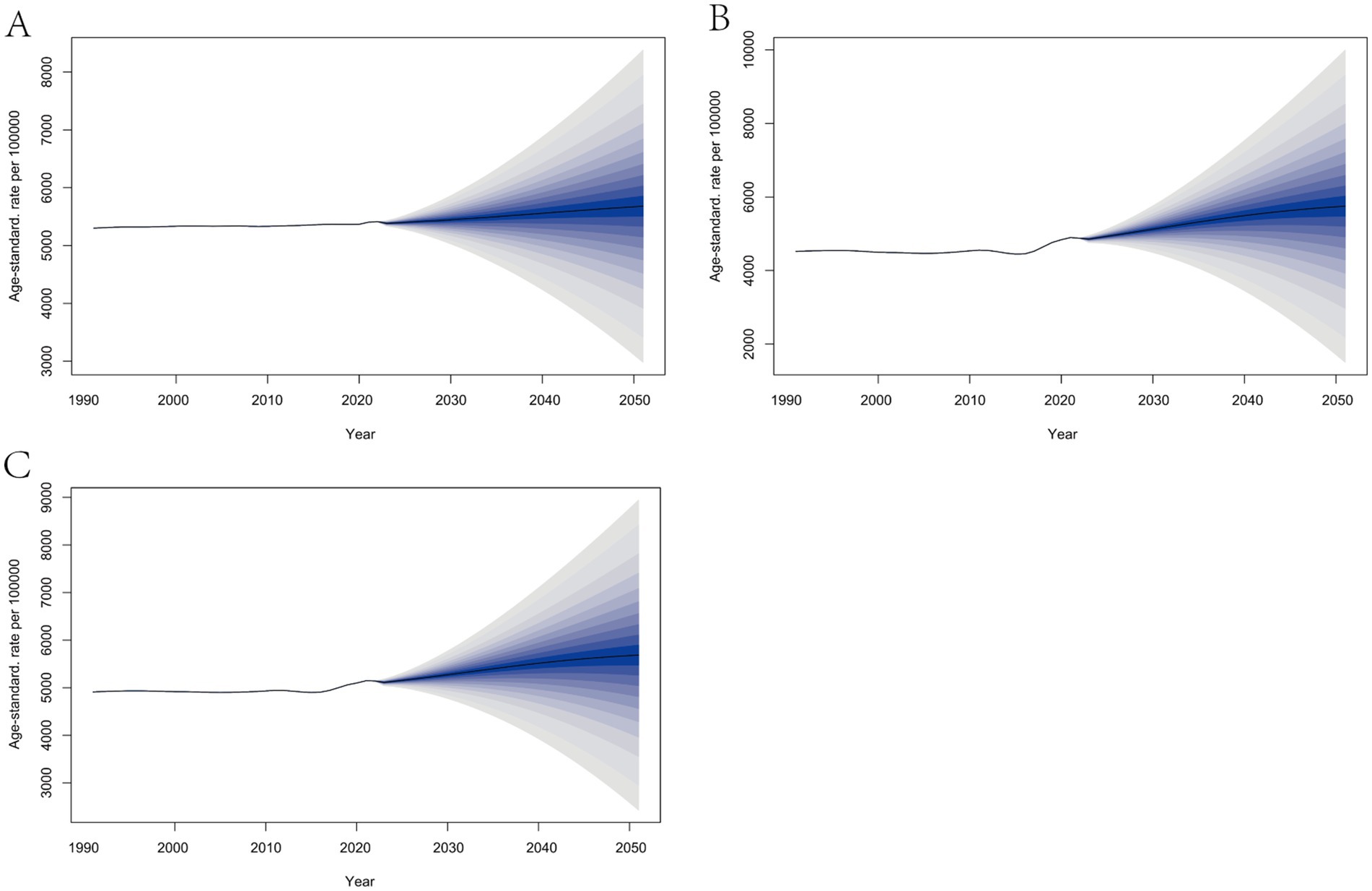
Figure 4. Projected incidence of trichomoniasis, 2022–2050. (A) Incidence in males. (B) Incidence in females. (C) Total incidence.
The incidence rate for males levels off, while the incidence rate for females increases significantly. Although the ASIR for males remains much higher than for females, it is expected that the ASIR for females will catch up with that of males by 2043. The ASIR for males is projected to be 5,680.57 per 100,000, and for females, 5,749.47 per 100,000 in 2050.
Discussion
This study provides a synthesis of global trichomoniasis burden estimates over the past 32 years. Between 1990 and 2021, both the incidence of trichomoniasis and its DALYs (Disability-Adjusted Life Years) increased. The primary factor contributing to this trend is likely the rapid growth of the world population, which has led to a larger population base. Trichomoniasis also exhibited elevated age-standardized incidence rates (ASIR) and age-standardized rates for DALY (ASR) over this period. A key reason for the increasing burden may be that most trichomoniasis cases are asymptomatic (20). Consequently, many individuals do not seek diagnosis or treatment, which facilitates the disease’s spread among sexual partners (21).
The transmission and prevalence of trichomoniasis exhibit significant differences between males and females. The ASIR indicates that it is higher in males than in females, while the ASR of DALY shows that it is higher in females than in males. This conclusion is consistent with the research findings of Leiwen Fu (15) and those of Poole et al. (22).
The differences in infection rates may be due to both behavioral and physiological factors. Men tend to change partners more frequently and have earlier sexual initiation compared to women (23). However, women are more severely affected by trichomoniasis because of their unique pathophysiology, which increases their risk of infertility, cervicitis, and cervical cancer following infection (4, 6, 7). Although men are often asymptomatic, their ability to unknowingly transmit the infection highlights the need for more accessible and responsive testing for men (24).
The burden of trichomoniasis also varies by age group. We observed the most significant change in ASIR among the <20 age group, likely due to the initially low ASIR in this group, making any increase more noticeable. A negative Estimated Annual Percentage Change (EAPC) and an increasing number of cases in the 85+ age group suggest a rise in the aging population. Furthermore, the negative EAPC and increasing cases in this age group suggest that the incidence of trichomoniasis is not under control, but rather that the ASIR is declining due to the growing proportion of older adult individuals in the global population (25). These trends imply that as the global population continues to grow, trichomoniasis infections will likely rise, underscoring the need for enhanced preventive and control strategies. In 2021, the 30–44 age group exhibited significantly higher ASRs for both incidence and DALY compared to other age groups. This may be due to an increase in sexual partners and unsafe sexual practices, which is consistent with findings from a British study that identified age as an independent risk factor for Trichomonas vaginalis infection (26).
Another major finding from the current study is that the ASIR and ASR for DALY associated with trichomoniasis decreased with higher levels of the Socio-Demographic Index (SDI). This supports the work of Zheng et al. (27). SDI is a reflection of a nation’s or region’s economic development, and the results suggest that trichomoniasis remains a persistent issue in low-income areas. Developing countries, particularly in sub-Saharan Africa, have higher DALY rates, indicating they bear the heaviest burden of trichomoniasis. Possible contributing factors include better early diagnosis and treatment in developed countries, and a lack of awareness and active treatment in developing regions (28). However, it is worth noting that EAPC for ASIRs is negative in low-SDI areas, while EAPC for ASIRs is positive in high-SDI areas. In economically disadvantaged regions, asymptomatic or mildly symptomatic infections may be underreported as resources are directed toward more urgent health concerns. In contrast, higher-income areas may experience better disease control measures, leading to lower case numbers, but resulting in a higher EAPC when ASIRs increase.
Regional differences in the ASIRs of trichomoniasis are also quite remarkable. The incidence rate is relatively high in African countries, followed by that in Oceania and Latin America. Cultural beliefs and lifestyle factors may contribute to these disparities (29). It has been demonstrated that condom use, as a reliable method of preventing STIs, significantly reduces the rates of trichomoniasis transmission (30). However, in regions with limited sexual health education, lower condom usage results in higher ASIRs. For instance, despite efforts to improve healthcare, Benin still experiences one of the highest EAPCs, likely due to inadequate public health infrastructure (31).
Joinpoint analysis revealed differences in trends across age groups and between sexes. In men, the highest ASIR occurred in the 35–39 age group in 2003, while women reached their peak ASIR in the same age group in 2019. This suggests that the 35–39 age group represents the highest risk for developing trichomoniasis. Since women aged 30–54 accounted for 79.96% of the total incidence, and the burden of trichomoniasis in this group closely mirrors the overall population trend, this age group plays a significant role in determining the total burden of disease. These findings align with the study by Asmah et al. (32), which found a stronger correlation between trichomoniasis and age in women compared to men, with the older adult being less affected.
Our predictions for the future show a steady trend in ASIR for men, but a sharp increase in ASIR for women. This may reflect greater vulnerability in women, compounded by lower education levels and poorer financial status.
Based on the Global Burden of Disease (GBD) 2021 study, this research outlines the ongoing global burden of trichomoniasis and provides projections through 2050. However, this study has limitations. The GBD database is heavily concentrated in economically developed countries, and some poorer or developing regions may lack sufficient health data. Furthermore, because trichomoniasis is not a notifiable disease and many cases are asymptomatic, its true prevalence may be underreported. This study highlights the increasing burden of trichomoniasis over the past 32 years and projects its continued rise through 2050, offering valuable insights to help authorities in different countries and regions develop effective prevention and control strategies.
Conclusion
The global burden of trichomoniasis is rising. While men have higher ASIRs, women bear a greater DALY burden, highlighting the need for expanded testing options for men and more effective treatments for women, particularly those aged 30–54. The study revealed an inverse correlation between ASIR and SDI, indicating that trichomoniasis remains prevalent in low-income areas. Projections suggest a continued increase in global ASIR by 2050, especially among women. To mitigate this burden, strengthening sexual health education and STI surveillance in high-risk populations and regions is essential.
Data availability statement
Publicly available datasets were analyzed in this study. This data can be found here: https://ghdx.healthdata.org/gbd-2021.
Ethics statement
Ethical approval was not required for the study involving humans in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and the institutional requirements.
Author contributions
XW: Data curation, Formal analysis, Methodology, Writing – original draft, Writing – review & editing, Project administration. LL: Data curation, Formal analysis, Methodology, Writing – original draft, Writing – review & editing, Visualization. KL: Data curation, Formal analysis, Methodology, Writing – review & editing. XQ: Data curation, Formal analysis, Methodology, Writing – review & editing. JW: Supervision, Writing – review & editing. LJ: Supervision, Writing – review & editing. LS: Supervision, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research was supported by the National Natural Science Foundation of China (82273689; 82160900) and the Joint Scientific Research Foundation of Gansu Province (24JRRA876). The National Natural Science Foundation of China (82273689), project director is KL. The National Natural Science Foundation of China (82160900), project director is JW. The Joint Scientific Research Foundation of Gansu Province (24JRRA876), project director is JW.
Acknowledgments
We appreciate the constructive comments made by our colleagues on this manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1530227/full#supplementary-material
SUPPLEMENTARY FIGURE S1 | Joinpoint regression analyses for different male age subgroups. (A) <20 years; (B) 20–24 years; (C) 25–29 years; (D) 30–34 years; (E) 35–39 years; (F) 40–44 years; (G) 45–49 years; (H) 50–54 years; (I) 55–59 years; (J) 60–64 years; (K) 65–69 years; (L) 70–74 years; (M) 75–79 years; (N) 80–84 years; (O) 85+ years. APC, Annual Percent Change.
SUPPLEMENTARY FIGURE S2 | Joinpoint regression analyses for different female age subgroups. (A) <20 years; (B) 20–24 years; (C) 25–29 years; (D) 30–34 years; (E) 35–39 years; (F) 40–44 years; (G) 45–49 years; (H) 50–54 years; (I) 55–59 years; (J) 60–64 years; (K) 65–69 years; (L) 70–74 years; (M) 75–79 years; (N) 80–84 years; (O) 85+ years. APC, Annual Percent Change.
Footnotes
1. ^https://ghdx.healthdata.org/gbd-2021
2. ^https://surveillance.cancer.gov/help/joinpoint/tech-help/citation
References
1. Schwebke, JR, and Burgess, D. Trichomoniasis. Clin Microbiol Rev. (2004) 17:794–803. doi: 10.1128/cmr.17.4.794-803.2004
2. Kellock, D, and O'Mahony, CP. Sexually acquired metronidazole-resistant Trichomoniasis in a lesbian couple. Genitourin Med. (1996) 72:60–1. doi: 10.1136/sti.72.1.60
3. Morris, SR, Bristow, CC, Wierzbicki, MR, Sarno, M, Asbel, L, French, A, et al. Performance of a single-use, rapid, point-of-care Pcr device for the detection of Neisseria Gonorrhoeae, chlamydia trachomatis, and trichomonas Vaginalis: a cross-sectional study. Lancet Infect Dis. (2021) 21:668–76. doi: 10.1016/s1473-3099(20)30734-9
4. Van Gerwen, OT, Opsteen, SA, Graves, KJ, and Muzny, CA. Trichomoniasis. Infect Dis Clin N Am. (2023) 37:245–65. doi: 10.1016/j.idc.2023.02.001
5. Muzny, CA. Why does trichomonas Vaginalis continue to be a "neglected" sexually transmitted infection? Clin Infect Dis. (2018) 67:218–20. doi: 10.1093/cid/ciy085
6. Van Gerwen, OT, Craig-Kuhn, MC, Jones, AT, Schroeder, JA, Deaver, J, Buekens, P, et al. Trichomoniasis and adverse birth outcomes: a systematic review and Meta-analysis. BJOG. (2021) 128:1907–15. doi: 10.1111/1471-0528.16774
7. Lindrose, AR, Htet, KZ, O'Connell, S, Marsh, J, and Kissinger, PJ. Burden of Trichomoniasis among older adults in the United States: a systematic review. Sex Health. (2022) 19:151–6. doi: 10.1071/sh22009
8. WHO. Sti: incident cases of trichomoniasis in 15- 49 year olds (per 1000). (2025). Available at: https://www.who.int/data/gho/data/indicators/indicator-details/GHO/incident-cases-of-trichomoniasis-in-individuals-(per-1000)
9. WHO. Sti: incident cases of trichomoniasis in 15- 49 year olds (per 1000). (2025). Available at: https://www.who.int/data/gho/data/indicators/indicator-details/GHO/incident-cases-of-trichomoniasis-in-individuals-(in-millions)
10. Obetta, KC, Ogbonna, IO, Oyigbo, DN, Ugwu, OO, Ugwu, KO, Onah, BN, et al. Prevalence of Trichomoniasis infection among adults in Nigerian community settings. Medicine. (2023) 102:e34585. doi: 10.1097/md.0000000000034585
11. Bolumburu, C, Zamora, V, Muñoz-Algarra, M, Portero-Azorín, F, Escario, JA, and Ibáñez-Escribano, A. Trichomoniasis in a tertiary Hospital of Madrid, Spain (2013-2017): prevalence and pregnancy rate, coinfections, metronidazole resistance, and endosymbiosis. Parasitol Res. (2020) 119:1915–23. doi: 10.1007/s00436-020-06688-2
12. GBD 2017 Risk Factor Collaborators. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990-2017: a systematic analysis for the global burden of disease study 2017. Lancet. (2018) 392:1923–94. doi: 10.1016/s0140-6736(18)32225-6
13. GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the global burden of disease study 2019. Lancet. (2020) 396:1204–22. doi: 10.1016/s0140-6736(20)30925-9
14. Ammar, A, Trabelsi, K, Hermassi, S, Kolahi, AA, Mansournia, MA, Jahrami, H, et al. Global disease burden attributed to low physical activity in 204 countries and territories from 1990 to 2019: insights from the global burden of disease 2019 study. Biol Sport. (2023) 40:835–55. doi: 10.5114/biolsport.2023.121322
15. Fu, L, Sun, Y, Han, M, Wang, B, Xiao, F, Zhou, Y, et al. Incidence trends of five common sexually transmitted infections excluding Hiv from 1990 to 2019 at the global, regional, and National Levels: results from the global burden of disease study 2019. Front Med. (2022) 9:851635. doi: 10.3389/fmed.2022.851635
16. Fan, J, Li, X, Yu, X, Liu, Z, Jiang, Y, Fang, Y, et al. Global burden, risk factor analysis, and prediction study of ischemic stroke, 1990–2030. Neurology. (2023) 101:e137–50. doi: 10.1212/WNL.0000000000207387
17. Chen, HS, Zeichner, S, Anderson, RN, Espey, DK, Kim, HJ, and Feuer, EJ. The Joinpoint-jump and Joinpoint-comparability ratio model for trend analysis with applications to coding changes in health statistics. J Off Stat. (2020) 36:49–62. doi: 10.2478/jos-2020-0003
18. Li, HZ, and Du, LB. Application of Joinpoint regression model in Cancer epidemiological time trend analysis. Zhonghua Yu Fang Yi Xue Za Zhi. (2020) 54:908–12. doi: 10.3760/cma.j.cn112150-20200616-00889
19. Riebler, A, and Held, L. Projecting the future burden of Cancer: Bayesian age-period-cohort analysis with integrated nested Laplace approximations. Biom J. (2017) 59:531–49. doi: 10.1002/bimj.201500263
20. CDC. CDC’S Sexually Transmitted Infections Treatment Guidelines, 2021. (2021). Available online at: https://www.cdc.gov/std/treatment-guidelines/default.htm.
21. Donders, GGG, Ruban, K, Depuydt, C, Bellen, G, Vanden Broeck, D, Jonckheere, J, et al. Treatment attitudes for Belgian women with persistent trichomonas vaginalis infection in the vlarest study. Clin Infect Dis. (2019) 68:1575–80. doi: 10.1093/cid/ciy736
22. Poole, DN, and McClelland, RS. Global epidemiology of trichomonas vaginalis. Sex Transm Infect. (2013) 89:418–22. doi: 10.1136/sextrans-2013-051075
23. Wong, T, Singh, A, Mann, J, Hansen, L, and McMahon, S. Gender differences in bacterial Stis in Canada. BMC Womens Health. (2004) 4:S26. doi: 10.1186/1472-6874-4-S1-S26
24. Daugherty, M, Glynn, K, and Byler, T. Prevalence of trichomonas Vaginalis infection among us males, 2013-2016. Clin Infect Dis. (2019) 68:460–5. doi: 10.1093/cid/ciy499
25. Sadigov, R. Rapid growth of the world population and its socioeconomic results. ScientificWorldJournal. (2022) 2022:8110229. doi: 10.1155/2022/8110229
26. Nicholls, JE, Turner, KME, North, P, Ferguson, R, May, MT, Gough, K, et al. Cross-sectional study to evaluate trichomonas Vaginalis positivity in women tested for Neisseria Gonorrhoeae and Chlamydia trachomatis, attending genitourinary medicine and primary care clinics in Bristol. South West England Sex Transm Infect. (2018) 94:93–9. doi: 10.1136/sextrans-2016-052942
27. Zheng, Y, Yu, Q, Lin, Y, Zhou, Y, Lan, L, Yang, S, et al. Global burden and trends of sexually transmitted infections from 1990 to 2019: an observational trend study. Lancet Infect Dis. (2022) 22:541–51. doi: 10.1016/S1473-3099(21)00448-5
28. Fernando, SD, Herath, S, Rodrigo, C, and Rajapakse, L. Clinical features and sociodemographic factors affecting trichomonas Vaginalis infection in women attending a central sexually transmitted diseases Clinic in Sri Lanka. Indian J Sex Transm Dis AIDS. (2012) 33:25–31. doi: 10.4103/0253-7184.93813
29. Haffejee, F, and Maksudi, K. Understanding the risk factors for Hiv acquisition among refugee women in South Africa. AIDS Care. (2020) 32:37–42. doi: 10.1080/09540121.2019.1687833
30. Mabaso, N, and Abbai, NS. A review on trichomonas Vaginalis infections in women from Africa. S Afr J Infect Dis. (2021) 36:254. doi: 10.4102/sajid.v36i1.254
31. Houngbo, PT, De Cock, BT, Bunders, J, Coleman, HLS, Medenou, D, Dakpanon, L, et al. Ineffective healthcare Technology Management in Benin's public health sector: the perceptions of key actors and their ability to address the Main problems. Int J Health Policy Manag. (2017) 6:587–600. doi: 10.15171/ijhpm.2017.17
Keywords: trichomoniasis, global burden, trend analysis, sexually transmitted disease, annual percentage change
Citation: Wei X, Liu L, Liu K, Qin X, Wu J, Jiang L and Shang L (2025) Global burden of trichomoniasis: current status, trends, and projections (1990–2021). Front. Public Health. 13:1530227. doi: 10.3389/fpubh.2025.1530227
Edited by:
Nigel Yarlett, Pace University, United StatesReviewed by:
Yunus Emre Beyhan, Yuzuncu Yil University, TürkiyeHarry P. De Koning, University of Glasgow, United Kingdom
Thomas Agyarko-Poku, Kwame Nkrumah University of Science and Technology, Ghana
Copyright © 2025 Wei, Liu, Liu, Qin, Wu, Jiang and Shang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xingmin Wei, d2VpeG0yMDA0QDEyNi5jb20=; Lu Liu, MjE0MzUxNDYzM0BxcS5jb20=
†These authors have contributed equally to this work