
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 16 April 2025
Sec. Life-Course Epidemiology and Social Inequalities in Health
Volume 13 - 2025 | https://doi.org/10.3389/fpubh.2025.1526255
This article is part of the Research TopicAccess and Barriers to Reproductive Health Services among Immigrants and Populations in Conflict ZonesView all 3 articles
 Hermann Badolo1*
Hermann Badolo1* Aristide Romaric Bado2
Aristide Romaric Bado2 Herman Bazié1Yisso Fidèle Bacyé3Romaine Konseiga4
Herman Bazié1Yisso Fidèle Bacyé3Romaine Konseiga4 Hervé Hien1,2
Hervé Hien1,2Introduction: Antenatal care (ANC) is a critical determinant of maternal and infant wellbeing and is a reliable method for reducing maternal and infant mortality. Antenatal care use is considered adequate when the first ANC takes place in the first trimester and the woman completes at least four ANC in accordance with WHO recommendations during her pregnancy. Despite the increasing of the proportion of women having completed at least four ANC in Burkina Faso, the data show that WHO recommendations are far from being respected. This study aimed to determine the evolution of individual, family and community factors associated with the adequate use of ANC in Burkina Faso between 2010 and 2021.
Methods: The data used in this study is procured from the Demographic and Health Surveys carried out in Burkina Faso in 2010 and 2021. Binary logistic regression analysis was used to analyze factors associated with the use of antenatal care. Adjusted odds ratios (AOR) were estimated to assess the strength of associations, and 95% confidence intervals were used for significance testing. A proportion test was used to examine differences in ANC utilization between 2010 and 2021 in Burkina Faso.
Results: In our study sample, 22.92% (95% CI: 22.11–23.74) of the respondents in 2010 had adequate ANC use, compared to 46.34% (95% CI: 45.12–47.58) in 2021. The results demonstrate the influence of the woman’s individual characteristics, the household and the community characteristics on the adequate ANC use in Burkina Faso. Regarding the woman’s individual characteristics, age, educational level, marital status, occupation and modern contraceptive methods use were significantly associated with adequate ANC use in 2010 and 2021. The household wellbeing quintile, the degree of exposure to the media and the region of residence were significantly associated with adequate antenatal care use in 2010 and 2021.
Conclusion: This study notes that Burkina Faso has made enormous progress in improving the coverage of antenatal care between 2010 and 2021, and indicates several factors including individual, family and community factors influencing adequate ANC use. For optimal efficacy, interventions promoting the adoption of antenatal care services must take these outcomes into account.
Maternal health, both globally in general and in developing countries in particular, is at the heart of national and international health sector policies. According to the World Health Organization (WHO), approximately 287,000 women died during or after pregnancy or childbirth in 2020 (1). Nearly 95% of these maternal deaths in 2020, most of which were preventable, occurred in low- and middle-income countries (1). In African countries, maternal mortality is one of the leading causes of death among women and newborns. The main complications and causes of pregnancy-related death are hemorrhage, sepsis, unsafe abortion, hypertension problems and dystocia (2, 3). Most of these deaths and complications could largely be avoided or treated during antenatal care, which aim to prevent, detect early and manage any complications that could affect the health of the mother and the unborn child, as well as support the woman throughout her pregnancy (2, 4). Available data indicate that countries with low ANC coverage tend to have high maternal mortality rates (5, 6). Additionally, it has been demonstrated that early use of antenatal care, starting in the first trimester of pregnancy, plays a critical role in the early detection and treatment of maternal health problems during pregnancy (7). This approach also constitutes a solid basis for adequate care during and after childbirth. Given the importance of ANC, the WHO recommends four antenatal l visits and at least eight contacts for pregnant women. Antenatal care use is considered adequate when the first ANC takes place in the first trimester and the woman completes at least four ANC in accordance with WHO recommendations during her pregnancy (4, 7).
In Burkina Faso, the maternal mortality ratio (MMR) is experiencing a downward trend, going from 341 deaths per 100,000 live births between 2003 and 2010 to 232 deaths per 100,000 live births between 2014 and 2021 (8–10). Despite this progress, difficulties persist regarding certain key indicators of maternal and child health. Indeed, according to reports from demographic and health surveys (DHS), since 2003, the proportion of women having completed at least four antenatal consultations during their pregnancy has increased from 17.6% in 2003 to 33.7% in 2010 and 72.1% in 2021. Furthermore, the proportion of women having undergone their first antenatal consultation during the first trimester of pregnancy also increased from 26.9% in 2003 to 41.2% in 2010 and 47.7% in 2021 (8–10). Despite this progress, these data show that WHO recommendations are far from being respected in Burkina Faso.
Studies conducted in Burkina Faso on antenatal healthcare services have predominantly concentrated on access to and utilization of antenatal care (ANC), investigating the factors that influence these dimensions, including socio-economic, geographical, and cultural determinants (11, 12). Additionally, they analyze the effects of free-of-charge policies on the utilization of maternal health services (13), as well as the repercussions of terrorist attacks and insecurity on access to maternal health services, encompassing ANC visits, assisted deliveries, and cesarean sections (14). Other researchers have assessed the quality and content of care received during ANC visits (15, 16). However, the adequate utilization of antenatal care among women of childbearing age in Burkina Faso has not been explicitly addressed, nor has a comparative analysis been conducted with the data available from the 2010 and 2021 Demographic and Health Surveys (DHS).
With a gross domestic product (GDP) of approximately 768.8 USD per capita in 2020 (17), Burkina Faso is one of the countries with the lowest level of economic development. More than 40% of its population live below the poverty line. The 2021–2022 report of the Human Development Index (HDI) of the United Nations Development Program (UNDP), ranks Burkina Faso 184th out of 191 countries. Burkina Faso’s economy is mainly based on agriculture and mining. Agriculture, which occupies nearly 82% of the active population, is currently hampered by the security context, which limits access to rural areas (17).
The health situation in Burkina Faso, although improving, is characterized by high general and specific mortality rates. Mothers and children constitute the most vulnerable groups. According to various DHSs carried out in Burkina Faso, the infant mortality rate decreased regularly between 1998 and 2021, going from 105 to 30%. Life expectancy at birth continues to increase. Overall, it increased from 42.2 years in 1975 to 61.9 years in 2019, an increase of 19.7 years (8–10, 18, 19).
In addition, in a difficult context marked by COVID-19 and security challenges, there was a general decline in the use of health services in 2020 compared to previous years in Burkina Faso. For example, at the national level, the coverage of the fourth ANC was 38.0% for a target of 60% in 2020. The extreme values were recorded in the Sahel (9.7%) and Cascades (49.3%) regions. None of the regions had reached the target in 2020 (20).
Building on existing research into antenatal care (ANC) utilization in Burkina Faso (11–16, 21–25), this study analyzes factors associated with adequate ANC use in 2010 and 2021 to inform strategies for reducing maternal and neonatal mortality.
The study’ objective is to identify sociocultural and economic determinants—including women’s living environment, reproductive behavior, and individual characteristics—that influence ANC uptake. We hypothesize that enhancing women’s social status (literacy, economic agency, decision-making autonomy), promoting positive reproductive behaviors (family planning, health service engagement), and improving maternal health practices could significantly increase adequate ANC utilization in Burkina Faso. In a country where public health services face a serious lack of equipment, medicines and competent personnel, this study could contribute to providing better guidance, information and awareness-raising activities for women in matters related to the use of antenatal care.
Burkina Faso, a landlocked nation situated in the Sahel region, covers an area of 272,969 km2 and is bordered by Mali to the northwest, Niger to the northeast, Benin to the southeast, and Côte d’Ivoire, Ghana, and Togo to the south. Administratively, the country is divided into 13 regions, 45 provinces, 351 departments, and 8,228 villages. According to the 2019 General Census of Population and Housing (RGPH), Burkina Faso’s population was recorded at 20.5 million, with women constituting 51.7% of this total (10.6 million). Notably, 44% of women (4.66 million) were of reproductive age (15–49 years), highlighting the importance of maternal healthcare services. Furthermore, the 0–4 age group comprised 16.2% of the population (3.3 million), emphasizing the demographic significance of neonatal health outcomes (26).
This study utilizes nationally representative data from the 2010 and 2021 Demographic and Health Surveys (DHS), conducted during periods characterized by ongoing maternal and neonatal health challenges. Burkina Faso’s decentralized administrative structure, along with the socioeconomic disparities across its regions, provides a critical context for analyzing spatial and temporal trends in antenatal care utilization. These data were collected from a representative sample of women of childbearing age (15–49 years), collected during these two household surveys. The DHS reports carried out in 2010 and 2021 provide more details on these surveys (8, 10).
The population studied consists of women of childbearing age, i.e., those aged from 15 to 49 years, who have had at least one live birth during the last 5 years preceding each of these two surveys. If a woman had more than one live birth within the past 5 years, only the utilization of ANC during the most recent birth was taken into account for data analysis in this study. The DHS sample only includes ordinary households, thus excluding populations in collective households such as hospitals, prisons, refugee camps and internally displaced people (Figure 1).
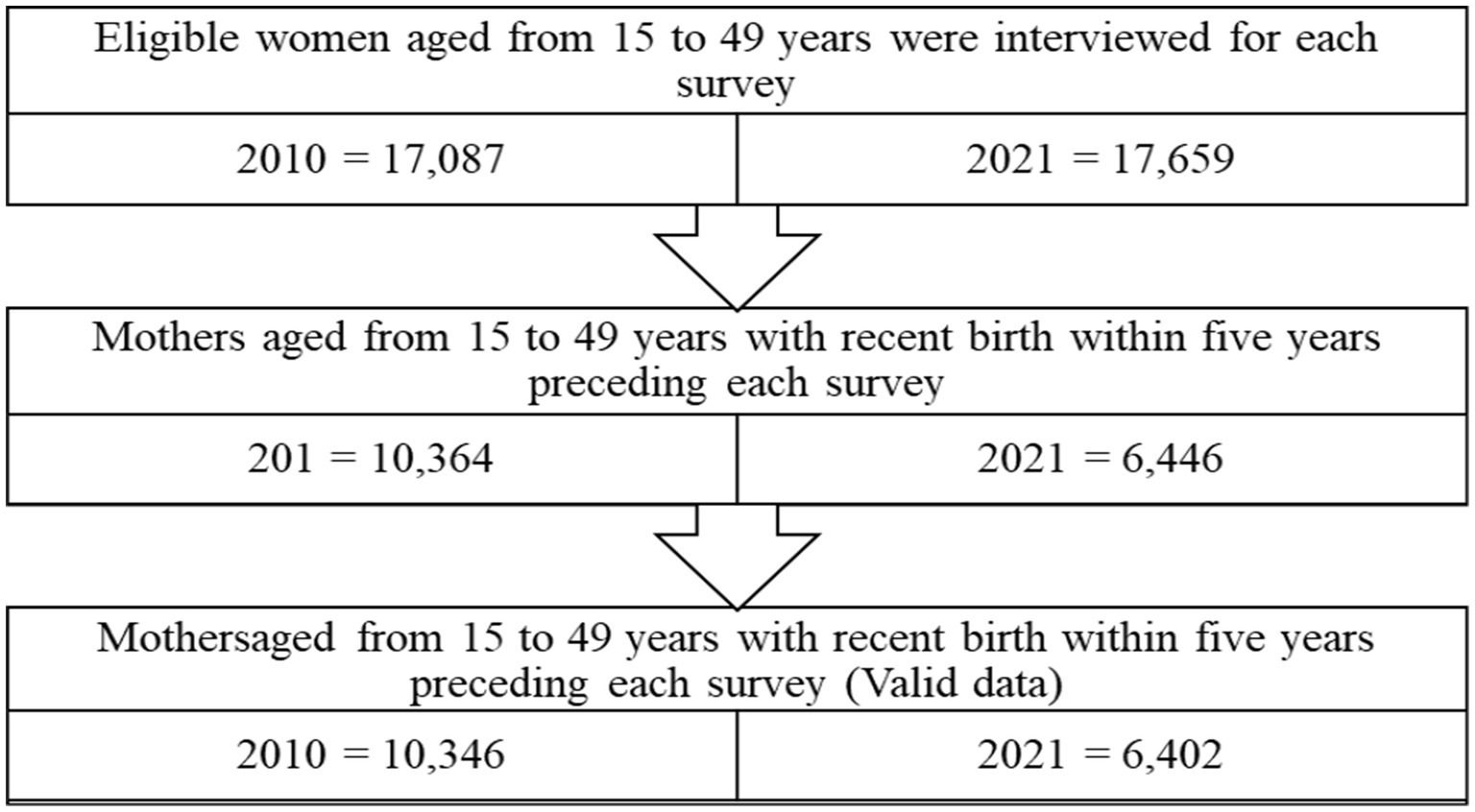
Figure 1. Flowchart showing how the final sample size was obtained.
The variables under study were taken from the household questionnaire and the individual women’s questionnaire used during these two surveys.
The dependent variable is adequacy of antenatal care use, which is the measure of compliance with prescribed recommendations in terms of timing and frequency of antenatal use. This variable was constructed by combining:
• Timeliness: Timing of the first ANC visit (categorized as “adequate” if initiated in the first trimester);
• Frequency: Total ANC visits (categorized as “adequate” if ≥4 visits);
A dichotomous variable was created (1 = adequate if both criteria were met; 0 = otherwise). This variable was measured dichotomously and coded as 0 for inadequate and 1 for adequate.
The independent variables used in the study were selected based on the results of previous research on the determinants of antenatal care utilization (27–32). At the individual level, this study considered the mothers’ age at the time of delivery, the use of modern contraceptive methods, the mothers’ education level, the mothers’ occupation, the mothers’ marital status, the mothers’ average parity and the interval between pregnancies. At the household level, this study considered the gender of the household head, the household wellbeing quintile, the size of the household and decision-making regarding the woman’s health. At the community level, variables on the degree of exposure to the media, the place of residence and the region of residence were considered.
The data were cleaned, coded and analyzed using Stata version 16.1 software.
Regarding the objectives of this study, the analytical approach includes both a descriptive part and an explanatory part. In the descriptive part, a bivariate analysis made it possible to describe the relationships between the independent variables and the dependent variable. The chi-square (95%) test was used to identify possible statistical links between the dependent variable and the independent variables. The proportion test (95%) was used to examine differences in adequate ANC utilization between 2010 and 2021 in Burkina Faso.
To analyze factors associated with adequate ANC utilization, multivariate binary logistic regression analyses were used. AORs were estimated to assess the strength of associations and, 95% confidence intervals were used for significance testing. All analyses used sampling weights and adjusted for the sampling design (clustering and stratification) to take into account the complex sampling of DHS and to ensure representativeness.
This study included 10,346 women in 2010 and 6,402 women aged 15–49 years who had at least one live birth during the last 5 years preceding these two surveys (Table 1). In 2010, 24.0% (2,481/10,346) resided in urban areas, compared to 29.0% (1,855/6,402) in 2021. Adequate antenatal care (ANC) utilization increased significantly from 22.9% (95% CI: 22.11–23.74) in 2010 to 46.3% (95% CI: 45.12–47.58) in 2021 (p < 0.001).
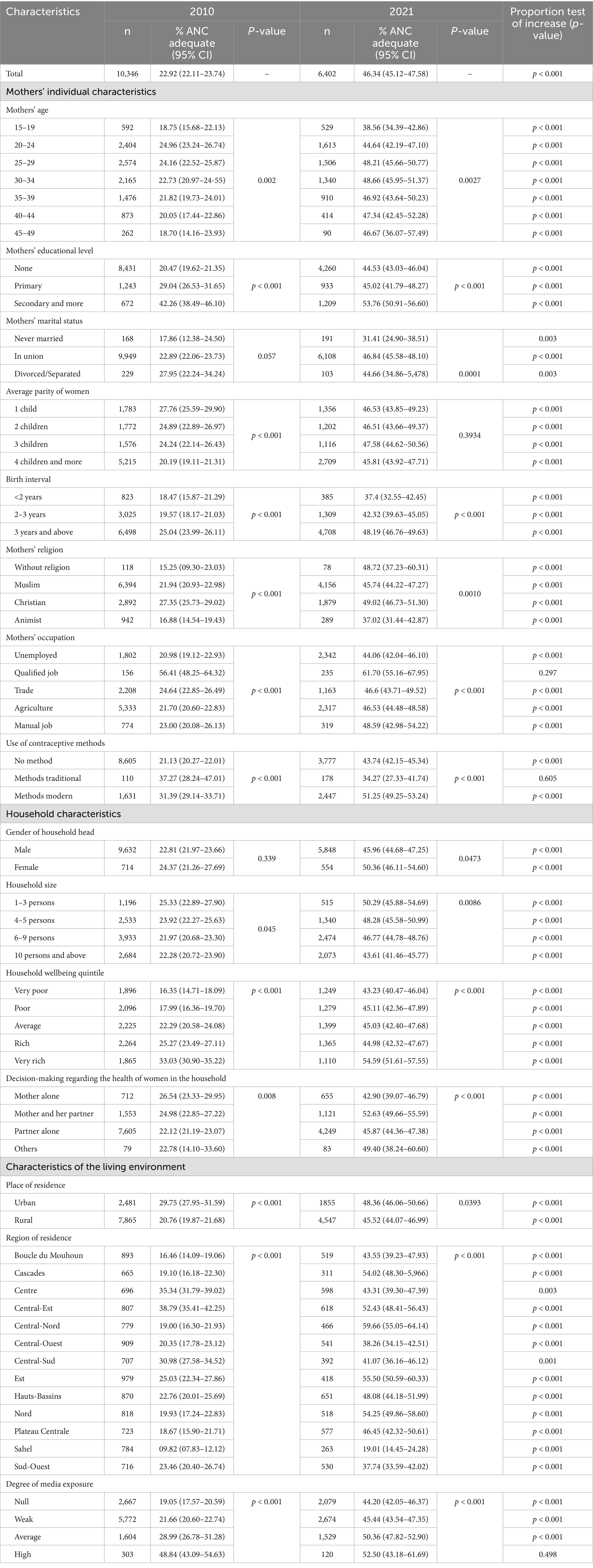
Table 1. Descriptive results of the use of antenatal care among women aged 15–49 based on data from the 2010 and 2021 demographic and health surveys in Burkina Faso.
Table 1 presents the percentages of women aged 15–49 who carried out adequate ANC use during their last pregnancy in 2010 and 2021. We note that, whatever the year, the individual characteristics of the woman (age, educational level, marital status, occupation, religion, average parity and pregnancy interval), household characteristics (size, Household wellbeing quintile and decision-making regarding the health of the woman) and community characteristics (place of residence, region of residence and degree of exposure to the media) were significantly associated with adequate ANC use. However, gender of household head in 2010 and average parity in 2021 were not significantly associated with adequate ANC use.
Between 2010 and 2021, the utilization of antenatal care (ANC) during pregnancy improved markedly across most demographic groups within the study population, indicating progress in maternal health equity. While women in skilled occupations, traditional contraceptive users, and those with high media exposure exhibited no significant changes, historically marginalized groups experienced notable gains. Among mothers aged 45–49 years, the completion rate of adequate ANC rose from 18.70% (95% CI: 14.16–23.93) to 46.67% (95% CI: 36.07–57.49)—a nearly 2.5-fold increase. Similarly, multiparous women (those with four or more children) witnessed their ANC coverage more than double, increasing from 20.19% (95% CI: 19.11–21.31) to 45.81% (95% CI: 43.92–47.71).
Socioeconomic disparities also narrowed during this period. Mothers engaged in manual labor, for instance, increased their ANC utilization from 23.00% (95% CI: 20.08–26.13) to 48.59% (95% CI: 42.98–54.22), while those in female-headed households progressed from 24.37% (95% CI: 21.26–27.69) to 50.36% (95% CI: 46.11–54.60). Notably, mothers in very poor households—a demographic often disproportionately excluded from healthcare—achieved a rise from 16.35% (95% CI: 14.71–18.09) to 43.23% (95% CI: 40.47–46.04). Even non-religious mothers, a demographic frequently overlooked in health interventions, saw their ANC completion rates surge from 15.25% (95% CI: 9.30–23.03) to 48.72% (95% CI: 37.23–60.31).
Paradoxically, access to media did not uniformly predict improvements: mothers without media exposure still doubled their ANC utilization (19.05% [95% CI: 17.57–20.59] to 44.20% [95% CI: 42.05–46.37]). These trends collectively underscore a shift toward broader accessibility of ANC over the decade. However, persistent gaps among skilled workers, traditional method users, and women exposed to media suggest that systemic barriers—such as workplace constraints, cultural preferences, or fragmented health messaging—may require targeted policy attention.
The results of the multivariate logistic regression are presented in Table 2. Maternal age, education, and contraceptive use were consistently associated with adequate antenatal care (ANC) utilization across both survey years. Women aged 20–44 years exhibited significantly higher odds of adequate ANC use compared to adolescents (15–19 years), with the strongest association in 2021 (AOR = 1.68, 95% CI:1.18–2.40 for ages 40–44). Secondary education or higher increased the likelihood of adequate ANC utilization in both 2010 (AOR = 1.48, 95% CI:1.16–1.88) and 2021 (AOR = 1.38, 95% CI:1.16–1.64). Modern contraceptive use remained a robust predictor (2010: AOR = 1.29, 95% CI:1.13–1.48; 2021: AOR = 1.34, 95% CI:1.20–1.50).
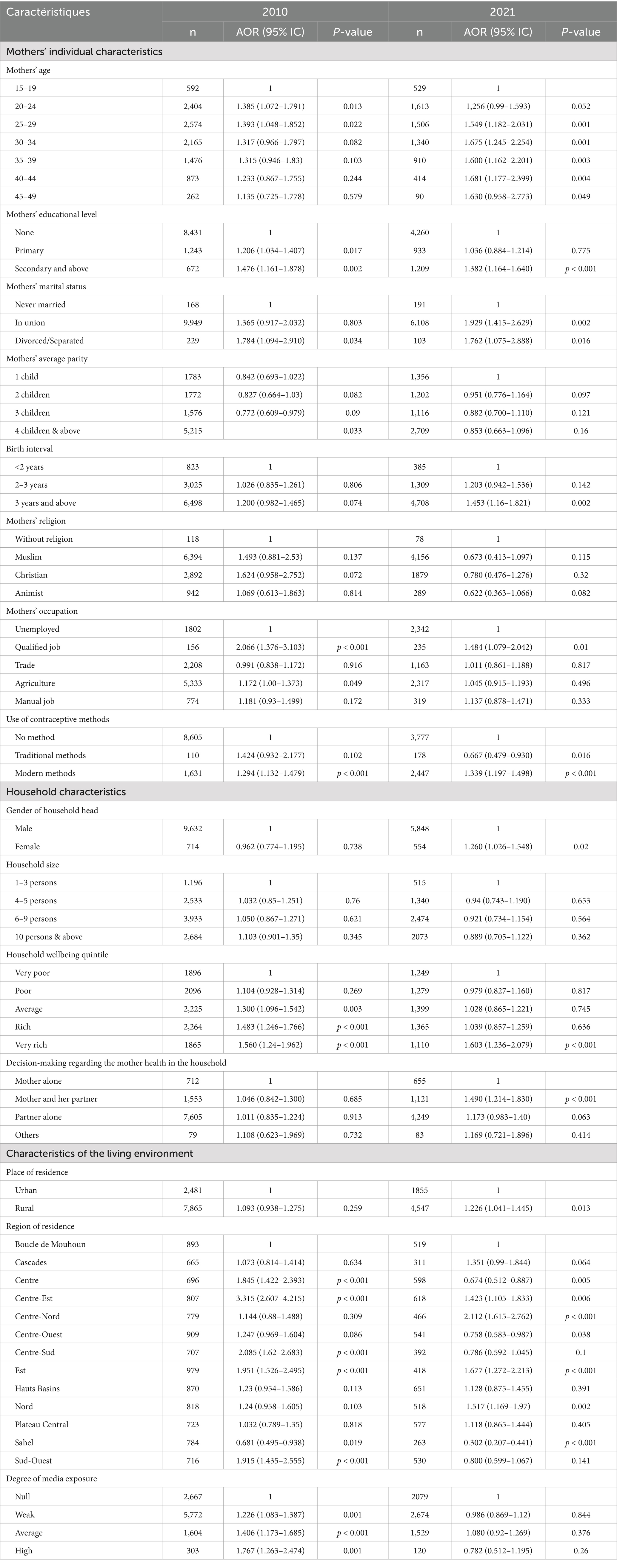
Table 2. Factors associated with the use of antenatal care among women aged 15–49 based on data from the 2010 and 2021 demographic and health surveys in Burkina Faso.
Household wealth quintile significantly influenced ANC utilization, though its impact narrowed by 2021. In 2010, even average wealth (AOR = 1.30, 95% CI:1.10–1.54) increased ANC use, but by 2021, only the very rich quintile showed a strong association (AOR = 1.60, 95% CI:1.24–2.08). Female-headed households in 2021 had higher ANC utilization (AOR = 1.26, 95% CI:1.03–1.55). In 2010, individual autonomy played a central role in ANC utilization. However, by 2021, shared decision-making between partners became a more significant predictor (AOR = 1.49, 95% CI: 1.21–1.83). Geographic inequities persisted, with women in the Sahel region facing significantly lower odds of adequate ANC utilization in both 2010 (AOR = 0.68, 95% CI:0.50–0.94) and 2021 (AOR = 0.30, 95% CI:0.21–0.44) compared to Boucle du Mouhoun. Conversely, the Centre-Est region showed consistently higher utilization (2010: AOR = 3.32, 95% CI:2.61–4.22; 2021: AOR = 1.42, 95% CI:1.11–1.83), likely due to concentrated health infrastructure. Rural residence became a positive predictor in 2021 (AOR = 1.23, 95% CI:1.04–1.45), suggesting potential improvements in rural healthcare access.
Meanwhile, the role of media exposure as a driver of ANC utilization diminished. In 2010, women with high media exposure were significantly more inclined to seek ANC services (AOR = 1.77, 95% CI: 1.26–2.47). By 2021, however, this association had dissipated.
The results indicate a significant improvement in access to adequate ANC consultations for pregnant women in Burkina Faso between 2010 and 2021. The results demonstrate the influence of mothers’ individual characteristics, household and community characteristics on the adequate ANC use in Burkina Faso. Concerning the mothers’ individual characteristics, her age, educational level, marital status, occupation and use of modern contraceptive methods were significantly associated with adequate ANC use in 2010 and 2021. The results of this study show a significant association between household characteristics (household wellbeing quintile, degree of media exposure and region of residence) and adequate ANC utilization in 2010 and 2021. The gender of the household head, decision-making regarding the mother’s health and the place of residence were significantly associated with adequate ANC use in 2021 only.
It is well recognized that women’s age plays an important role in the utilization of maternal health services (33, 34). In this study, middle-aged mothers were more likely to have adequate ANC use visits than younger and older mothers.
It appears in this study and in others (27, 32, 34–38) that women who have a low education level, encounter more difficulties in ensuring adequate use of antenatal care. This can be explained by the fact that less educated women often encounter significant challenges in acquiring knowledge about their health, comprehending the medical system, and understanding the mechanisms of antenatal care. This lack of awareness constitutes a critical factor contributing to delays in accessing the first antenatal care appointment, as many of these women remain uninformed regarding the appropriate timing and objectives of antenatal care (39).
Mothers’ occupation appears to have a very strong influence on their use of ANC services. The results of this study showed that working mothers were more likely to make multiple antenatal visits than unemployed mothers. This conclusion is consistent with that of Assefa and Tadesse (40), Tawiah (41), Sharma et al. (42), as well as Badolo (22). These results could be explained by the fact that working pregnant women have a larger social network which could allow them to access more information relating to pregnancy, including antenatal care. The information provided by their coworkers and that obtained in their workplace increased their knowledge about pregnancy, which ultimately enabled them to perform antenatal visits as recommended (43).
Household wellbeing quintile was strongly and positively associated with the use of ANC services. The findings indicated that women living in impoverished households were less likely to engage in adequate ANC utilization compared to their counterparts in rich households. Similar results were reported in previous studies conducted in Uganda (44), Ethiopia (27), and Nepal (33). These studies indicated that women living in very poor or poor households sought ANC services less frequently than those living in wealthier households.
Our findings indicate a significant positive association between media exposure and the utilization of antenatal care (ANC) in 2010; however, this association was no longer significant by 2021. This change may be attributed to improvements in access to health services in Burkina Faso between 2010 and 2021, which likely reduced reliance on media to raise awareness among women regarding pregnancy monitoring. Notably, since 2016, the government has undertaken a substantial recruitment initiative for trained community-based health workers with a commendable level of education, aimed at ensuring that populations have access to quality health services (45). These community-based health workers are now equipped to treat common childhood illnesses, provide family planning advice, and assist pregnant women in accessing appropriate healthcare. By 2024, the coverage of administrative villages by pairs of community-based health workers reached 93.08%. This community-based initiative has undoubtedly contributed to enhancing awareness of health issues among both urban and rural populations, as well as to an increased utilization of maternal health care services.
While our analysis highlights mothers’ individual factors, household and community factors associated with adequate ANC, implementation of the policy of free care for mothers and children such as the Gratuité programme (46) and other health financing reforms (e.g., performance-based financing) may have contributed to observed trends. These substantials health policy marked a pivotal moment in maternal health by eliminating financial barriers that previously hindered access to care. These policies of providing free healthcare may contribute significantly to the attainment of the Sustainable Development Goals (SDGs) concerning maternal and child health. Since its introduction, data reveal a notable transformation. Women, who were formerly constrained by financial considerations or geographical distance, are now seeking healthcare services earlier and more frequently. In their study, Offosse et al. demonstrated that 72% of women now attend at least four antenatal check-ups, facilitated by the provision of free healthcare, while 53% initiate these check-ups as early as the first trimester of pregnancy, representing a remarkable increase compared to previous years (13). However, these policies were not directly measured in our models. Future studies should incorporate these policies implementation data to disentangle their effects.
This study has some limitations. The data used is procured from the DHS, which use a robust multistage probability sampling methodology to select clusters and households. The first limitation lies in the cross-sectional nature of the data collected, which means that the dependent and explanatory variables were measured simultaneously and therefore cannot guarantee any causality of the associations. Additionally, the 5-year recall period may seem long and could question the validity of the responses but limiting it to the most recent births would reduce this risk. However, in African contexts, some births occur before the age of 15 years. The operational definition of reproductive age limited by default to the interval of 15 to 49 years, limits the actual population subject to maternity events. Some cultural variables, potentially relevant to explaining the adequacy of antenatal care, were not considered in this study because they were missing from the database. Also, the smaller subgroups (e.g., mothers aged 45–49, women with secondary education) may have reduced statistical power and the findings for these groups should be interpreted with caution.
In sum, we note that Burkina Faso has made enormous progress in improving the coverage of antenatal care between 2010 and 2021. This has highlighted factors that influence the adequate ANC use, both at the individual, household and community level. At the individual level, age, occupation, education level and use of modern contraceptive methods were factors significantly associated with adequate ANC use. At the household and community level, living in a female-headed household, living in a wealthy household, living in a rural area, decision-making in the household in relation to the mother’s health and region of residence, were significantly associated with adequate ANC monitoring. To achieve optimal efficacy, interventions aimed at promoting the adequate ANC use must take these finding into account.
The findings of this study have important implications for the design of health policy regarding maternal health in Burkina Faso. Policies that encourage women’s use of modern contraceptive methods and promote women’s participation in the labor market could likely help increase attendance at antenatal care services. Therefore, government policies should target uneducated, unemployed and economically disadvantaged women to increase the rate of adequate ANC use.
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/supplementary material.
The studies involving humans were approved by Le comité d’éthique pour la recherche en santé, Burkina Faso. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
HBad: Conceptualization, Data curation, Formal analysis, Methodology, Software, Visualization, Writing – original draft, Writing – review & editing. AB: Writing – review & editing. HBaz: Writing – review & editing. YB: Writing – review & editing. RK: Writing – review & editing. HH: Writing – review & editing.
The author(s) declare that financial support was received for the research and/or publication of this article. But the two DHS data collection were supported by the Government of Burkina Faso, the United States Agency for International Development (USAID), the United States Presidential Malaria Initiative (PMI), the Bank World, the Global Fund through PADS, UNICEF and UNFPA.
We would like to express our gratitude to the Government of Burkina Faso, the United States Agency for International Development (USAID), the United States Presidential Malaria Initiative (PMI), the Bank World, the Global Fund through PADS, UNICEF and UNFPA for funding these two DHS data collections. We sincerely thank the ICF for permission to use the Demographic and Health Survey data of Burkina Faso. We gratefully acknowledge all the fieldworkers, supervisors, and data managers for their work in the field. Finally, we thank the study population.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Gen AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
ANC, Antenatal care; AOR, Adjusted odds ratios; CI, Confidence intervals; DHS, Demographic and health surveys; HDI, Human Development Index; INSD, National Institute of Statistics and Demography; OR, Odds ratios; WHO, World Health Organization.
1. OMS, UNICEF, UNFPA. Tendances de la mortalité maternelle de 2000 à 2020: estimations de l’OMS, de l’UNICEF, du FNUAP, du Groupe de la Banque mondiale et de la Division de la population des Nations Unies: résumé d’orientation. Available online at: https://iris.who.int/handle/10665/372258 (Accessed May 31, 2024).
2. Maleya, A, Kakudji, YK, Mwazaz, RM, Nsambi, JB, Ngwej, HI, Mukuku, O, et al. Issues materno-fœtales des grossesses non suivies à Lubumbashi, République Démocratique du Congo. Pan Afr Med J. (2019) 33:66. doi: 10.11604/pamj.2019.33.66.18528
3. Kayentao, AKB, Coulibaly, O, Dembele, M, Guindo, M, Teguete, I, Diawara, SI, et al. Factors associated with antenatal care’s challenges in Kita and san health districts (Mali). Health Sci Dis. (2022) 23:73–8. doi: 10.5281/hsd.v23i11.4006
4. OMS. Recommandations de l’OMS concernant les soins prénatals pour que la grossesse soit une expérience positive. (2017). Available online at: https://apps.who.int/iris/bitstream/handle/10665/259584/9789242549911-fre.pdf (Accessed May 31, 2024).
5. Afaya, A, Azongo, TB, Dzomeku, VM, Afaya, RA, Salia, SM, Adatara, P, et al. Women’s knowledge and its associated factors regarding optimum utilisation of antenatal care in rural Ghana: a cross-sectional study. PLoS One. (2020) 15:e0234575. doi: 10.1371/journal.pone.0234575
6. WHO. WHO recommendations on antenatal care for a positive pregnancy experience: summary: highlights and key messages from the World Health Organization’s 2016 global recommendations for routine antenatal care. World Health Organization (2018). Available online at: https://apps.who.int/iris/bitstream/handle/10665/259947/WHO-RHR-18.02-eng.pdf (Accessed June 25, 2024).
7. Manyeh, AK, Amu, A, Williams, J, and Gyapong, M. Factors associated with the timing of antenatal clinic attendance among first-time mothers in rural southern Ghana. BMC Pregnancy Childbirth. (2020) 20:47. doi: 10.1186/s12884-020-2738-0
8. INSD, ICF International. Enquête Démographique et de Santé et à Indicateurs Multiples du Burkina Faso 2010. INSD et ICF International (2012). Available online at: https://www.dhsprogram.com/pubs/pdf/FR256/FR256.pdf (Accessed May 31, 2024).
9. INSD, ICF International. Enquête démographique et santé 2003. (2004). Available online at: https://dhsprogram.com/pubs/pdf/FR154/FR154.pdf (Accessed May 31, 2024).
10. INSD, ICF International. Enquête Démographique et de Santé du Burkina Faso 2021 INSD and ICF International. (2023). Available online at: https://dhsprogram.com/pubs/pdf/FR378/FR378.pdf
11. Coulibaly-Kone, AS, Kourouma, KR, Mla, Y, Millogo, T, Akoua, TK, Doukoure, D, et al. Predictors of the numbers of antenatal visits in Burkina Faso and cote d’ivoire: a cross sectional study. Rev Afr Méd Santé Publ. (2024) 7:327–50.
12. Samadoulougou, S, Sawadogo, KC, and Robert, A. Regional disparities of late entry to antenatal care and associated sociodemographic barriers in Burkina Faso. Rev Epidemiol Sante Publique. (2018) 66:S435. doi: 10.1016/j.respe.2018.05.546
13. Offosse, MJ, Yameogo, P, Ouedraogo, AL, Traoré, Z, and Banke-Thomas, A. Has the Gratuité policy reduced inequities in geographic access to antenatal care in Burkina Faso? Evidence from facility-based data from 2014 to 2022. Front Glob Women Health. (2024) 5:1345438. doi: 10.3389/fgwh.2024.1345438
14. Druetz, T, Browne, L, Bicaba, F, Mitchell, MI, and Bicaba, A. Effects of terrorist attacks on access to maternal healthcare services: a national longitudinal study in Burkina Faso. BMJ Glob Health. (2020) 5:e002879. doi: 10.1136/bmjgh-2020-002879
15. Conrad, P, Schmid, G, Tientrebeogo, J, Moses, A, Kirenga, S, Neuhann, F, et al. Compliance with focused antenatal care services: do health workers in rural Burkina Faso, Uganda and Tanzania perform all ANC procedures? Trop Med Int Health. (2012) 17:300–7. doi: 10.1111/j.1365-3156.2011.02923.x
16. Sheffel, A, Tampe, T, Katwan, E, and Moran, AC. Development of indicators for integrated antenatal care service provision: a feasibility study in Burkina Faso, Kenya, Malawi, Senegal and Sierra Leone. BMJ Open. (2023) 13:e065358. doi: 10.1136/bmjopen-2022-065358
17. Ministère de la santé. Plan national de développement sanitaire 2011–2020. Ministère de la santé, Burkina Faso. (2011).
18. INSD. Enquête par grappe et à indicateurs multiples de 2006 (MICS). INSD and ICF International. (2008).
20. ONSP. Rapport 2020 sur l’état de santé de la population du Burkina Faso. (2021). Available online at: https://onsp.minsante.bf/publicationsingle?publication=20 (Accessed June 3, 2024).
21. Niang, M, Dupéré, S, and Bédard, E. Le non-recours aux soins prénatals au Burkina Faso. Sante Publique. (2015) 27:405–14.
22. Badolo, H. Determinants of health care use and mothers’ preventative and curative health care practices in Burkina Faso. (2022). Available online at: https://etd.uwc.ac.za/handle/11394/9321 (Accessed August 19, 2024).
23. De Allegri, M, Ridde, V, Louis, VR, Sarker, M, Tiendrebéogo, J, Yé, M, et al. Determinants of utilisation of maternal care services after the reduction of user fees: a case study from rural Burkina Faso. Health Policy. (2011) 99:210–8. doi: 10.1016/j.healthpol.2010.10.010
24. Belaid, L. Facteurs contextuels dans l’évaluation d’une politique de santé maternelle au Burkina Faso. (2015). Available online at: https://papyrus.bib.umontreal.ca/xmlui/handle/1866/11812 (Accessed May 31, 2024).
25. Dabiré, E. Déterminants de l’utilisation des services prénatals dans les pays en développement: cas du Burkina Faso. (2002). Available online at: https://papyrus.bib.umontreal.ca/xmlui/bitstream/handle/1866/29059/Dabire_Ernest_2001_memoire.pdf?sequence=1 (Accessed May 31, 2024).
26. INSD. Recensement général de la population et de l’habitation de 2029 (RGPH-2019). Volume I: Evaluation de la qualité des données, Etat, structure et dynamique de la population. (2022). Available online at: https://www.insd.bf/fr/resultats (Accessed August 23, 2024).
27. Tiruaynet, K, and Muchie, KF. Determinants of utilization of antenatal care services in Benishangul Gumuz region, Western Ethiopia: a study based on demographic and health survey. BMC Pregnancy Childbirth. (2019) 19:115. doi: 10.1186/s12884-019-2259-x
28. Sahito, A, and Fatmi, Z. Inequities in antenatal care, and individual and environmental determinants of utilization at national and sub-national level in Pakistan: a multilevel analysis. Int J Health Policy Manag. (2018) 7:699–710. doi: 10.15171/ijhpm.2017.148
29. Chama-Chiliba, CM, and Koch, SF. Utilization of focused antenatal care in Zambia: examining individual- and community-level factors using a multilevel analysis. Health Policy Plan. (2015) 30:78–87. doi: 10.1093/heapol/czt099
30. Acharya, P, Kismul, H, Mapatano, MA, and Hatløy, A. Individual- and community-level determinants of child immunization in the Democratic Republic of Congo: a multilevel analysis. PLoS One. (2018) 13:e0202742. doi: 10.1371/journal.pone.0202742
31. Nketiah-Amponsah, E, Senadza, B, and Arthur, E. Determinants of utilization of antenatal care services in developing countries: recent evidence from Ghana. Afr J Econ Manag Stud. (2013) 4:58–73. doi: 10.1108/20400701311303159
32. Ricketts, TC, and Goldsmith, LJ. Access in health services research: the battle of the frameworks. Nurs Outlook. (2005) 53:274–80. doi: 10.1016/j.outlook.2005.06.007
33. Shrestha, G. Factors related to utilization of antenatal care in Nepal: a generalized linear approach. J Kathmandu Med Coll. (2013) 2:69–74. doi: 10.3126/jkmc.v2i2.10629
34. Fosu, GB. Childhood morbidity and health services utilization: cross-national comparisons of user-related factors from DHS data. Soc Sci Med. (1994) 38:1209–20. doi: 10.1016/0277-9536(94)90186-4
35. Simkhada, B, Van, TER, Porter, M, and Simkhada, P. Factors affecting the utilization of antenatal care in developing countries: systematic review of the literature. J Adv Nurs. (2008) 61:244–60. doi: 10.1111/j.1365-2648.2007.04532.x
36. Zerai, A, and Tsui, AO. The relationship between prenatal care and subsequent modern contraceptive use in Bolivia, Egypt and Thailand. Afr J Reprod Health. (2001) 5:68–82. doi: 10.2307/3583432
37. Barasa, KS, Wanjoya, AK, and Waititu, AG. Analysis of determinants of antenatal care services utilization in Nairobi County using logistic regression model. Am J Theor Appl Stat. (2015) 4:322–8. doi: 10.11648/j.ajtas.20150405.12
38. Nebeb, GT, Salgedo, W, and Alemayehu, Y. Antenatal care utilization in Debre Tabor, north West Ethiopia. Gynecol Obstet. (2015) 5:2161–0932. doi: 10.4172/2161-0932.1000339
39. Rode, A. Le" non-recours" aux soins des populations précaires. Constructions et réceptions des normes. [PhD Thesis] Université Pierre Mendès-France-Grenoble II (2010) Available online at: https://theses.hal.science/tel-00488403/ (Accessed June 21, 2024).
40. Enyew Assefa, EA, and Mekonnen Tadesse, MT. Factors related to the use of antenatal care services in Ethiopia: application of the zero-inflated negative binomial model. (2017). Available online at: https://www.cabidigitallibrary.org/doi/full/10.5555/20173320272 (Accessed June 20, 2024).
41. Tawiah, EO. Maternal health care in five sub-Saharan African countries. Afr Popul Stud. (2011) 25. doi: 10.11564/25-1-264
42. Sharma, SK, Sawangdee, Y, and Sirirassamee, B. Access to health: women’s status and utilization of maternal health services in Nepal. J Biosoc Sci. (2007) 39:671–92. doi: 10.1017/S0021932007001952
44. Kalule-Sabiti, I, Amoateng, AY, and Ngake, M. The effect of socio-demographic factors on the utilization of maternal health Care Services in Uganda. Afr Popul Stud. (2014) 28:515–25. doi: 10.11564/28-1-504
45. Ministère de la Santé. Stratégie nationale de santé communautaire 2024–2028. (2024). Available online at: https://www.sante.gov.bf/fileadmin/bfa_strategie_nationale_de_sante_communautaire_2024-2028.pdf (Accessed August 23, 2024).
Keywords: antenatal care, health service use, associated factors, women of childbearing age, Burkina Faso
Citation: Badolo H, Bado AR, Bazié H, Bacyé YF, Konseiga R and Hien H (2025) Factors associated with adequate antenatal care use among women of childbearing age in Burkina Faso: finding from the 2010 and 2021 demographic and health surveys. Front. Public Health. 13:1526255. doi: 10.3389/fpubh.2025.1526255
Edited by:
Comfort Z. Olorunsaiye, Arcadia University, United StatesReviewed by:
Bang Nguyen Pham, Papua New Guinea Institute of Medical Research, Papua New GuineaCopyright © 2025 Badolo, Bado, Bazié, Bacyé, Konseiga and Hien. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hermann Badolo, YmFkaG9sb2JpQGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.