 Hao Li1,2
Hao Li1,2 Weihong Zeng1,2*
Weihong Zeng1,2*- 1Jinhe Center for Economic Research, Xi'an Jiaotong University, Xi'an, Shaanxi, China
- 2Center for Aging and Health Research, Xi'an Jiaotong University, Xi'an, Shaanxi, China
Background: The relationship between leisure sedentary behaviors and mental health remains inconclusive. This study aims to provide evidence on leisure sedentary behaviors on mental health using longitudinal data, along with its moderating and mediating roles.
Methods: We utilized data from four waves (2006–2015) of the China Health and Nutrition Survey (CHNS), focusing on adults who completed their education, with a total sample of 23,693 observations. Leisure sedentary time, the independent variable, was measured based on self-reported data, while mental health issues were the dependent variables based on the Simplified Symptom Self-Rating Scale (SCL) and the Perceived Stress Scale (PSS-14). The primary analysis employed ordinary least squares (OLS) regression. Potential endogeneity was addressed by instrumental variable (IV) method via two-stage least squares (2SLS) regression and a continuous difference-in-differences (DID) design.
Results: Our findings indicate that high levels of sedentary time are associated adversely with mental health issues. Moderating roles show that improving health literacy and reducing sedentary time were effective in alleviating this adverse impact. Among older adults, social engagement and support from female caregivers showed greater potential to reduce the detrimental mental health impact of leisure sedentary time. Furthermore, obesity serve as its mediating role.
Conclusion: This study highlights the potential adverse impact of increased leisure sedentary time on mental health among Chinese population. These results provide a foundation for public health initiatives aimed at addressing the rising prevalence of sedentary behavior and its association with mental health issues.
Introduction
The rapid development of urbanization and technological advancements has led to a significant increase in sedentary behavior. Current estimates suggest that a large proportion of the adult population spends excessive amounts of time being sedentary (1). For example, a European survey reported that over 18% of adults sit for more than 7.5 h per day, with the figure ranging from 9% in Spain to 32% in the Netherlands (2). Similarly, Chinese adults spend an average of 8.5 h per day engaged in sedentary activities (3). As a result, the phrase “sitting is the new smoking” has been popularized in the media to highlight the growing epidemic across many nations (4). The relationship between sedentary behavior and physical health is well-established as the lack of utilization of body systems during sedentary time arguably leads to metabolic, hormonal, and muscular imbalances, which may attenuate the anti-inflammatory effects triggered by human musculature and promote systemic dysfunction (5). However, studies examining the relationship between sedentary behavior and mental health have produced inconsistent findings, despite extensive research on the topic (6, 7).
In addition to the prevalence of sedentary behaviors, there are several reasons to conduct a comprehensive investigation of how sedentary behavior affects mental health. First, inconsistent findings across studies hinder a clear understanding of this relationship. As noted by Higgins et al. (8) research on sedentary behavior is still in its early stages and requires broad inclusion criteria, especially longitudinal study (9). Second, according to the Report on the Development of Chinese National Mental Health (2019–2020), 12–20% of Chinese residents experience poor mental health (10). Unfortunately, a significant proportion of those with mental health issues do not receive the treatment they need (11), especially the impact of lifestyle habits on mental health is becoming increasingly important (12). Third, mental health strongly predicts self-rated health, surpassing physical health in its influence (13). Understanding mental health is, therefore, essential for improving overall wellbeing. Forth, leisure sedentary time is more random than occupational sedentary time, making it easier to detect statistically significant and reliable results.
Previous studies have revealed the relationship between lifestyle habits and mental health. A growing body of research highlights the influence of behaviors such as smoking, and alcohol consumption impact mental health (14). For example, studies point to the fact that smoking is a likely causal risk factor in the development of mental health issues (15). In addition, alcohol consumption is closely associated with the prevalence of depression (16). In particular, long-term heavy drinking can have serious emotional impacts and adverse consequences, including intentional self-harm and even suicide (17). Other factors, such as insufficient sleep, physical activity, and nutrition, also affect mental health (18). Insufficient sleep not only exacerbates mental health issues but may also interact with sedentary behavior, amplifying negative effects on inflammatory markers and psychophysiological health (19, 20). Additionally, research also suggests that physical activity and nutrition have a combined impact on mental health (21).
Regarding sedentary behavior, most studies suggest a correlation between prolonged sedentary time, particularly leisure-time screen use, and poorer mental health outcomes (22). For example, a large-scale study found that sedentary behavior increases the long-term risk of mental health disorders (23). Evidence links higher sedentary time with issues like depression and sadness, particularly when screen use is involved (24). Additionally, two Chinese studies using the CHNS data in 2015 and find increasing the time spent on leisure-time sedentary behavior is linked to lower perceived stress levels (25, 26). However, many of these studies are cross-sectional, limiting causal inferences (9). A longitudinal study following participants for seven years found that increased TV viewing heightened the odds of developing depressive symptoms, particularly among young men (27).
Contrary to this majority, some studies report no association between sedentary behavior and mental health, especially when accelerometer-based measurements are used (28, 29). Additionally, certain studies have found that TV viewing may have a positive role in mental wellbeing by fulfilling social, emotional, and informational needs, particularly during crises such as the COVID-19 pandemic (30). Despite these inconsistencies, the majority of evidence suggests that prolonged sedentary time is associated with an increased risk of mental health issues. Therefore, we propose the following hypothesis:
Hypothesis 1: Prolonged sedentary time is associated with a higher risk of mental health issues.
The relationship between sedentary behavior and mental health may be moderated by health literacy and efforts to reduce sedentary time. Health literacy, defined as the ability to obtain, process, and understand basic health information, significantly influences health outcomes. Higher health literacy can reduce psychological and social dysfunction and promote healthier lifestyles, including less sedentary behavior (31, 32). In addition, reducing or interrupting prolonged sitting is also a practical strategy for mitigating its negative effects. The World Health Organization (WHO) recommends minimizing sedentary time and incorporating regular interruptions (33), such as standing breaks during TV viewing or workplace strategies like walking meetings (34, 35). Based on the previous discussions, we propose the following hypothesis to examine moderating role:
Hypothesis 2a: Health literacy could diminish the negative effect of prolonged leisure sedentary time on mental health.
Hypothesis 2b: Reducing sedentary time could diminish the negative effect of prolonged leisure sedentary time on mental health.
The aging process brings physical and mental changes that profoundly affect quality of life. Older adults, who spend more time sitting and experience higher rates of mental health disorders, are particularly vulnerable (36, 37). In Chinese culture, where family is central (38), family caring and interactions may help mitigate the adverse effects of sedentary behavior on mental health (39). First, caring for elderly family members has been an essential function of families for centuries and is a moral requirement for adult children in some societies where family-oriented norms and values prevail (40). Beyond spouses, children—typically daughters—are the most common informal caregivers (41) as societal expectations and gender norms (42, 43). For instance, Zhao et al. (44) found that families with daughters tend to provide higher-quality informal care than those with sons, particularly for older adults with greater care needs. Second, older adults with stronger social interactions have an increased likelihood of better health and higher increase in mental wellbeing than the socially disengaged (45). Social interactions might encourage people to adopt healthy behaviors, such as various physical activities, that benefit their mental health (46, 47), and social interactions might enhance the diffusion of health-related information by encouraging social interaction among neighbors (46, 48). Based on the previous discussions and analyses, we propose the following hypothesis to examine moderating role:
Hypothesis 3a: Female caregivers are more likely to diminish the negative effect of prolonged leisure sedentary time on mental health.
Hypothesis 3b: Social interaction could diminish the negative effect of prolonged leisure sedentary time on mental health.
After discussing the moderating roles between sedentary time and mental health, we turn our focus on mediating role. Sedentary behavior may indirectly affect mental health through obesity as sedentary activities are low-energy activity (49). Additionally, obesity, biologically, is associated with chronic low-grade inflammation in peripheral tissues (50), thereby leading to depression (51). Based on the previous discussions and analyses, we propose the following hypotheses:
Hypothesis 4: Obesity mediates the relationship between sedentary behavior and mental health.
In summary, this paper examines the relationship between leisure sedentary time and mental health using representative longitudinal data. In addition, to further understand this relationship, we also explore both moderating and mediating effects.
Data and empirical strategy
Data
The China Health and Nutrition Survey (CHNS) is an ongoing large-scale study aimed at determining how China's social and economic development affects the health and nutritional status of the country's population. It is conducted by the Carolina Population Center at the University of North Carolina in Chapel Hill and the National Institute for Nutrition and Health (formerly the National Institute of Nutrition and Food Safety) at the Chinese Center for Disease Control and Prevention. A multistage, random cluster process was used to draw a sample of ~7,200 households comprising more than 30,000 individuals across 15 provinces and municipal cities. The CHNS data-collection rounds were completed in 1989, 1991, 1993, 1997, 2000, 2004, 2006, 2009, 2011, and 2015. Our analysis draws on four waves-2006, 2009, 2011, and 2015—during which data on mental health issues and sedentary behavior were available. We focus on adults who have completed their formal education, resulting in a total of 23,693 observations.
Variables
Mental health issues
The CHNS collected two mental health scales across different years: the Simplified Symptom Self-Rating Scale (SCL) in 2006, 2009, 2011, and 2015 for individuals aged 45 and older, and the Perceived Stress Scale (PSS-14) in 2015 for all adults. To create comprehensive mental health measures, we combined scores from both the SCL and PSS-14 and then standardized them to a mean of zero and a standard deviation of one. Those two metrics were used as dependent variables in our main regressions.
Psychological wellbeing (PWB) is an essential and integral component of health, which is related to cognitive function, social relationships and health status and is a combination of feeling good and effective functioning (52). The PWB was measured by asking participants to answer three questions: “I have as much energy as I had in last year”; “I am as happy now as when I was younger”; “As I get older, things are better than I thought they would be.” Responses were scored on a five-point scale (1–5). To align with the trend of PSS-14, reverse scoring was applied, where higher scores indicate more frequent depressive symptoms and poorer mental health.
Can this newly constructed indicator reflect an individual's mental health relatively accurately? From the content point of view, the first question reflects the individual's health status and is a simplified index of somatization in SCL-90 (mainly reflecting subjective physical discomfort). The second question reflects the individual's psychological state and is a simplified measure of depression, anxiety, hostility, and terror in SCL-90. The third question is the individual's perceptions and attitudes toward the world around them, which is a broader indicator. Therefore, these questions are a great simplification of SCL-90 (53). The SCL has been widely used in previous studies [e.g., (53–55)].
Perceived stress is another important mental health indicator, manifesting as tension and discomfort in response to stressful situations or unfavorable life conditions (56). Prior studies have pointed out that perceived stress is positively associated with depression (57) and anxiety (58). In the 2015 wave, the PSS-14 was incorporated into the project for the first time (26). The PSS-14 is a validated questionnaire developed by Cohen et al. (59), and its Chinese version has been validated (60). It aims to measure the degree to which situations in one's life are appraised as stressful, and the items are designed to measure the extent to which one's life is perceived as unpredictable, uncontrollable, and overloading (59). Responses were scored on a 5-point Likert scale from 1 (“never”) to 5 (“very often”). Scores were calculated by reverse-scoring the positively stated items (4, 5, 6, 7, 9, 10, and 13) and summing the 14 items for a total score. Higher scores indicate greater perceived stress.
Leisure sedentary time
Sedentary behavior can be measured using subjective or objective methods. In this study, we use self-reported leisure sedentary time as the independent variable due to data constraints. Over recent decades, the ownership of color televisions and access to cable networks among Chinese households have grown significantly (61). During the survey period, more than 90% of Chinese families owned a television (62), making TV-based leisure sedentary time a valid measure.
The CHNS collects data on leisure sedentary time using a single question. Adult participants were asked, “Do you participate in these sedentary activities?” The listed activities included watching TV, watching videos, and playing video games. Participants then provided details on the time spent on these activities, answering two follow-up questions: “How much time do you spend during Monday to Friday?” and “How much time do you spend during Saturday to Sunday?” From these responses, we calculated the total leisure sedentary time. Studies commonly use non-exercise sitting behaviors, especially screen-based activities, to measure sedentary behavior (63). These measures typically show acceptable reliability and validity (64) and have been widely used in previous studies [e.g., (62, 65)].
In our analysis, we computed the independent variable using Equation 1 and applied winsorization at the 1st and 99th percentiles of the sample distributions. The equation is as follows:
Control variables
Referring to prior population-based studies (66, 67), we control for a comprehensive set of individual-, household-, and macro-level characteristics. First, we include individual and household factors such as marital status, sleep duration, physical activity, smoking status, drinking status, body mass index (BMI), self-reported health status, chronic status, and log-transformed annual household income. Additionally, we account for occupational sedentary time, which significantly affects mental health (68). To address multicollinearity issues, we standardize occupational sedentary time to a mean of zero and a standard deviation of one, given its inverse relationship with leisure sedentary time. Dietary factors are also included, as evidence suggests certain dietary patterns positively impact mental health. A balanced diet, rich in vegetables, fruits, whole grains, seafood, nuts, and moderate amounts of low-fat dairy, red meat, and healthy fats, is associated with better mental health outcomes (69). Moreover, dietary quality has been linked to the presence or progression of depressive symptoms (70). To capture dietary influences, we include variables for dietary preferences, a dietary knowledge index, and key nutritional elements. Dietary preferences are measured using four variables: preference for fast food, salty food, vegetables, and sugary foods, each scored from 1 to 5. Higher scores indicate a stronger preference. The dietary knowledge index, constructed from a rich set of dietary knowledge variables, reflects better dietary understanding, with higher scores indicating greater knowledge1. We also control for average daily intake of dietary fat and protein (in grams), where healthier dietary preferences and a higher dietary knowledge index suggest better dietary patterns and quality. Furthermore, to mitigate omitted variable bias related to genetic predisposition, we control for individual disease diagnoses, including mental health and genetic disorders. At the macro level, we include Urbanization, Economic, Health, and Housing Scores, where higher scores represent better development in these domains. Additionally, longitudinal studies are better to disentangle a temporal relationship between sedentary time and mental health issues (71). Thus, we control for year fixed effect. To address the existence of spatial heterogeneity in mental health issues, we also control for fixed effect at individual-level, household-level, and community-level. Age effects are absorbed by these fixed effects.
Table 1 summarizes the descriptive statistics for the sample. The average aggregated mental health score is 22, with a range from 1 to 78. Participants spend an average of 143 min per day in leisure sedentary activities. The average sleep duration is 7.81 h per day, and the mean BMI is 24, ranging from 13 to 32. Additionally, the proportions of individuals who exercise, smoke, drink alcohol, have chronic diseases, or are diagnosed with mental health or genetic disorders are relatively low, averaging 0.12, 0.31, 0.31, 0.30, and 0.01, respectively. Most participants are married, and the average annual household income is 51,660 yuan. Regarding self-reported health status, the average self-reported health score is 2, suggesting that most individuals perceive their health as good. Regarding dietary patterns and quality, most participants report disliking fast food, salty foods, and desserts, while most favor vegetables. The average dietary knowledge index is 22. Average daily intake of dietary fat and protein is 70 g and 64 g, respectively. For macro-level variables, the average Urbanization, Economic, Health, and Housing Scores are 71, 8, 9, and 6, respectively.
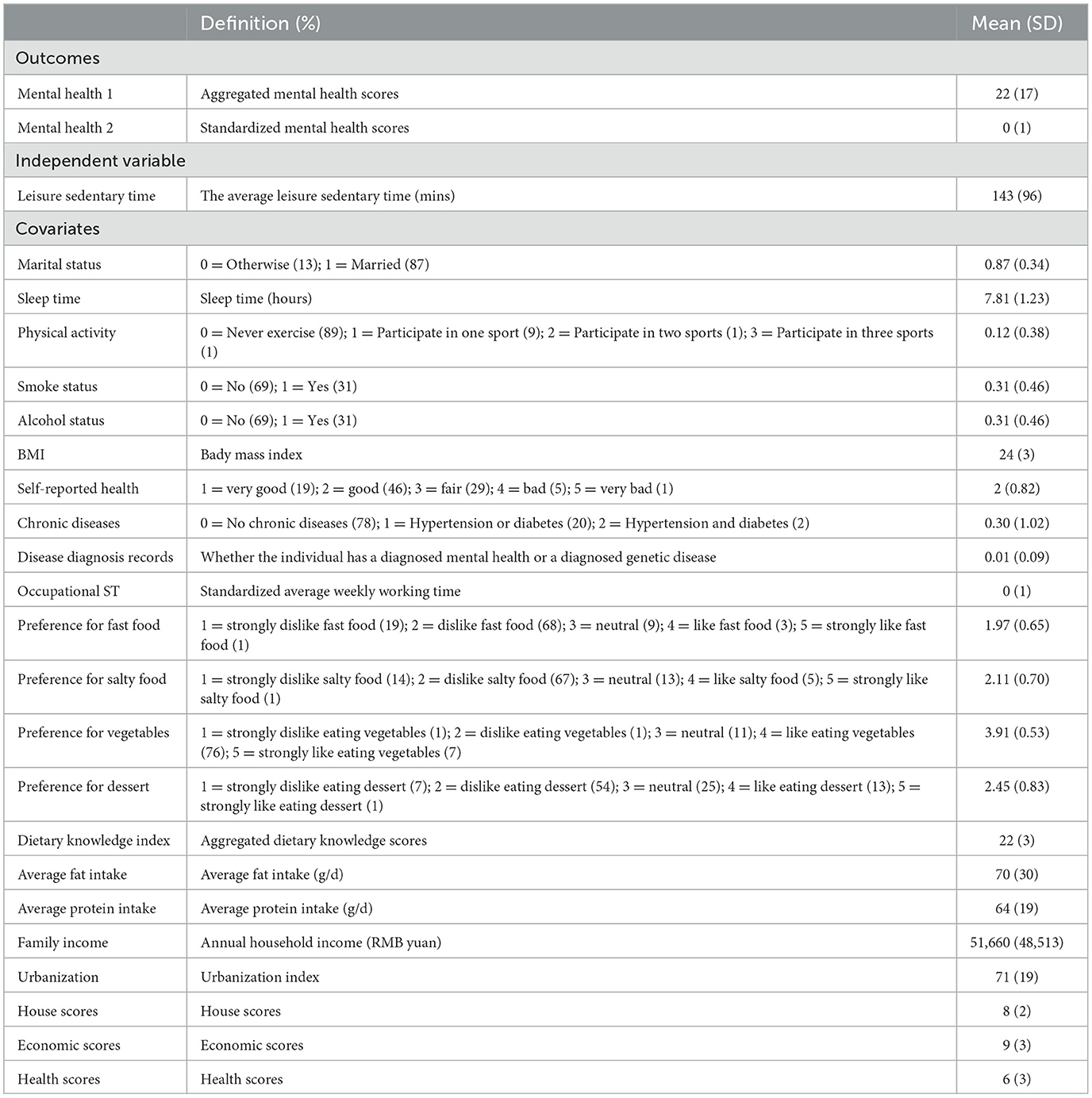
Table 1. Summary statistics of key variables.
Baseline model
We choose the ordinary least squares (OLS) method to test the relationship between leisure sedentary time and mental health issue in Hypothesis 1. The equation for the method is as follows (see Equation 2):
Where Yit is dependent variable for individual i at wave t, and STit represents individual i's leisure sedentary time at wave t. Xit is a set of control variables. δi, δf, and δcommid, represent the fixed effects at individual-level, household-level, and community-level, respectively. τt represents year-fixed effect. β1 is the main coefficient of interest, β1>0 indicates that heightened leisure sedentary time negatively affects mental health issues.
Discussion of endogeneity
Prior studies suggest that inconsistent findings regarding the relationship between sedentary time and mental health may stem from confounding factors, causality issues, and measurement errors (72). This necessitates a comprehensive review of endogeneity concerns.
One potential source of endogeneity, in the context of our study, is omitted variable bias. There are several unobservable factors that are likely to be correlated with both leisure sedentary time and mental health issues and, thus, in a multivariate regression framework, it is difficult to rule out more than one omitted variable, making it impossible to clearly predict the direction of bias. For example, adverse childhood experiences are associated with both higher sedentary behaviors, particularly greater screen time, and worse health conditions (73, 74).
While the fixed effect model is generally known to be effective in addressing omitted variable bias, endogeneity may also emerge from potential measurement error and simultaneity bias. Regarding measurement error bias, previous literature has found that leisure sedentary time was collected through questionnaires, inherently resulting in an underestimation of leisure sedentary time (75). Therefore, will underestimate β1 if β1 is positive. Concurrently, emerging evidence suggests bidirectional associations between sedentary behaviors and mental health issues (76). Individuals with mental health issues are generally less active, and sedentary behavior increases the risk of mental health issues. Thus, simultaneity bias should be considered.
Good instrumental variables must satisfy two assumptions. The first assumption is that they should be strongly correlated with the variable being instrumented. The second assumption is that the instrumental variables are orthogonal to the outcomes. To meet the above assumptions, this paper employs three instrumental variables.
First, building on Munasib and Bhattacharya (77), we adopt Lewbel's higher-moment approach (78). This method, initially designed for measurement error models, is widely applicable in contexts with general correlated-regressor error and multilevel structures (79). It constructs instrument using the third-order centered moment of leisure sedentary time. By design, this variable is strongly correlated with leisure sedentary time but unlikely to be correlated with mental health issues unless a non-linear relationship exists. This approach has been extensively validated in prior studies [e.g., (80, 81)].
Second, Duflo and Saez suggest using the average exogenous characteristics of group-level variables as instruments for endogenous independent variables (82). Therefore, inspired by the peer group effect theory (83), we employ the average leisure sedentary time in the household of individual i as second instrumental variable (group-level IV). The average leisure sedentary time in the household of individual i is strongly influence individual i's leisure sedentary time under the family norms. However, this variable is unlikely to correlate with individual time-varying unobservable characteristics once fixed effects are accounted for (84).
The third instrument is the number of TV channels available to a household. This variable is exogenous, as the availability of television signals in China is determined by national and local broadcasting authorities. At the same time, it is associated with the amount of time spent watching television, making it a valid instrument for leisure sedentary time.
These IVs collectively address the potential endogeneity issues in the relationship between sedentary time and mental health outcomes.
DID method
Despite we employ instrumental variable method to address endogenous concerns, the results are still affected by unobserved factors. Therefore, we draw from National Digital TV Development Plan as an exogenous variation to examine the effect of leisure sedentary time on mental health issues under the continuous difference-in-differences (DID) method. The logic of DID method is that the prevalence of high-definition digital television after policy greatly affects the screen time, thereby affecting mental health.
To meet the demand for high-definition television broadcasts of the 2008 Beijing Olympics, the State Administration of Radio, Film, and Television (SARFT) accelerated the promotion of high-definition digital television. High-definition TV programming and event broadcasts required compatible digital TV and set-top boxes, which significantly boosted demand for set-top boxes. As early as 2003, SARFT released the Digital TV Development Plan and accelerated its implementation in 2008. The plan mandated that by 2010, the digitalization of cable television networks should be largely completed. This target pushed local television stations to speed up the rollout of digital TV. Meanwhile, SARFT reinforced the requirement for the gradual shutdown of analog television signals in 2008, promoting the replacement of analog TV with digital TV. This policy further drove demand for set-top boxes since consumers needed them to receive digital signals. Financially, to accelerate the adoption of digital TV, some local governments introduced subsidy policies for set-top boxes in 2009. Consumers could receive price discounts when purchasing set-top boxes, which further boosted sales. Considering the timing of the plan, we choose 2009 as the cutoff. The regression framework of the continuous DID design is typical written as Equation 3 as follows.
Where the dummy variable Dit is equal to 0 for years from 2009 onwards and 1 otherwise, and other specifications are similar to Equation 2.
Results
Baseline results
To examine the relationship between leisure sedentary time and mental health issues, we estimate Equation 2, with results presented in Table 2. Column (1) uses aggregated mental health scores as the dependent variable, while column (2) uses standardized mental health scores. Both coefficients are positive and statistically significant. Specifically, we find that, on average, one additional minute of leisure sedentary time increases aggregated mental health scores by 0.0010 and standardized mental health scores by 0.0001. A back-of-the-envelope calculation indicates that one day of sedentary behavior increases aggregated mental health scores by 0.1430 and standardized scores by 0.0143. These findings suggest a consistent conclusion: increased leisure sedentary time is associated with mental health issues, supporting Hypothesis 1. However, these results should be interpreted cautiously, as the baseline estimation may be affected by endogeneity issues.
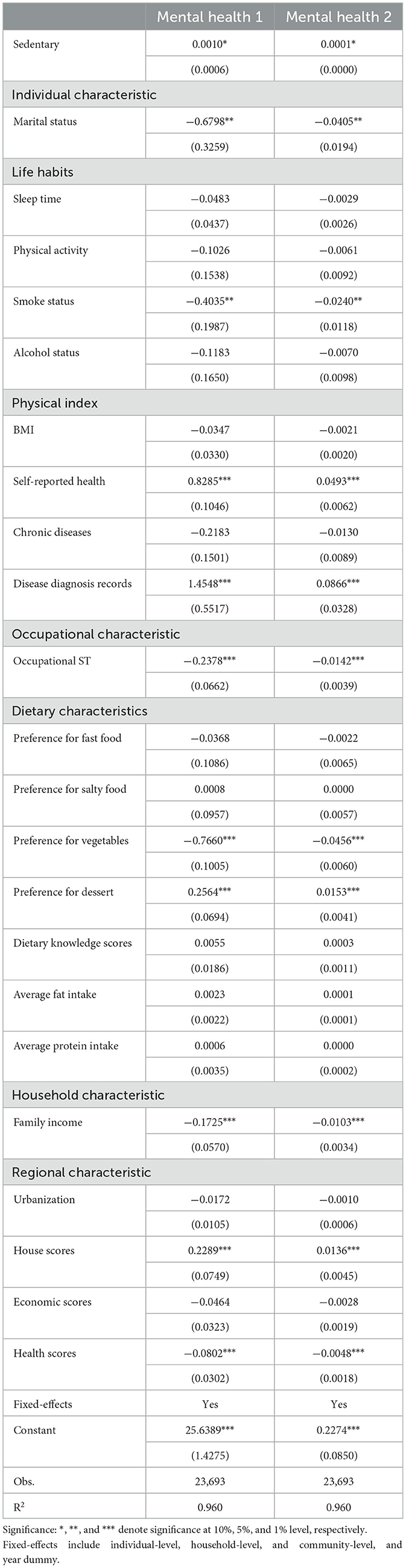
Table 2. Results of baseline regressions about the impact of leisure sedentary time on mental health issues (OLS).
Our analysis also shows that marriage is strongly associated with better mental health. This aligns with existing evidence that marriage improves health through mechanisms such as social support, health behavior regulation, and access to resources that protect health (85). Similarly, physical health, higher family income, and better health scores are positively associated with improved mental health. In contrast, higher housing scores are negatively associated with mental health. One possible explanation is that rapidly rising housing prices in China during the survey period increased stress and mental health risks. Furthermore, individuals diagnosed with mental health issues or genetic disorders tend to report poorer mental health outcomes. Interestingly, we find that smoking is positively associated with mental health. While most studies highlight the adverse impact of smoking on mental health, while some smokers report that smoking helps improve mood, reduce stress, or act as a form of coping (86). We also observe that occupational sedentary time is positively linked to mental health. This may be explained by a shift in sedentary behavior patterns during the survey waves, where leisure sedentary time increased while occupational sedentary time decreased (87). Lastly, dietary characteristics are significantly associated with mental health. For instance, individuals who prefer vegetables tend to have better mental health, while those with a preference for sweets report poorer mental health outcomes.
Instrumental variable results
To alleviate endogenous concerns, Table 3 shows the instrumental variable regression results. Column (3) shows the first-stage IV estimates, indicating a significant positive relationship between the instruments and the endogenous independent variable. The first-stage F-test yields an F-statistic of 1,541, which exceeds the threshold for weak instruments. Additionally, the p-value of the Kleibergen-Paap rk LM statistic is 0.000, indicating that the null hypothesis is rejected, and the instrumental variable passes the unrecognizable test. Concurrently, Sargan test p-values exceed 0.1, confirming the exogeneity of the instrumental variables. Hence, our instrumental variable selection is reasonable. Moving to column (1) and column (2), the result show that the regression coefficients are 0.0017 and 0.0001, respectively, and are significant at the 1% level, which are consistent with the baseline regression. Specially, the coefficients in column (1) and column (2) are larger than those in Table 2, suggesting a potential downward bias in the estimates when endogeneity is not addressed. To examine the valid of Lewbel's IV, Table 4 further reports the results of non-linear relationship between leisure sedentary time and mental health issues. The results show this non-linear relationship is unlikely to be hold, confirming the validity of Lewbel's IV.
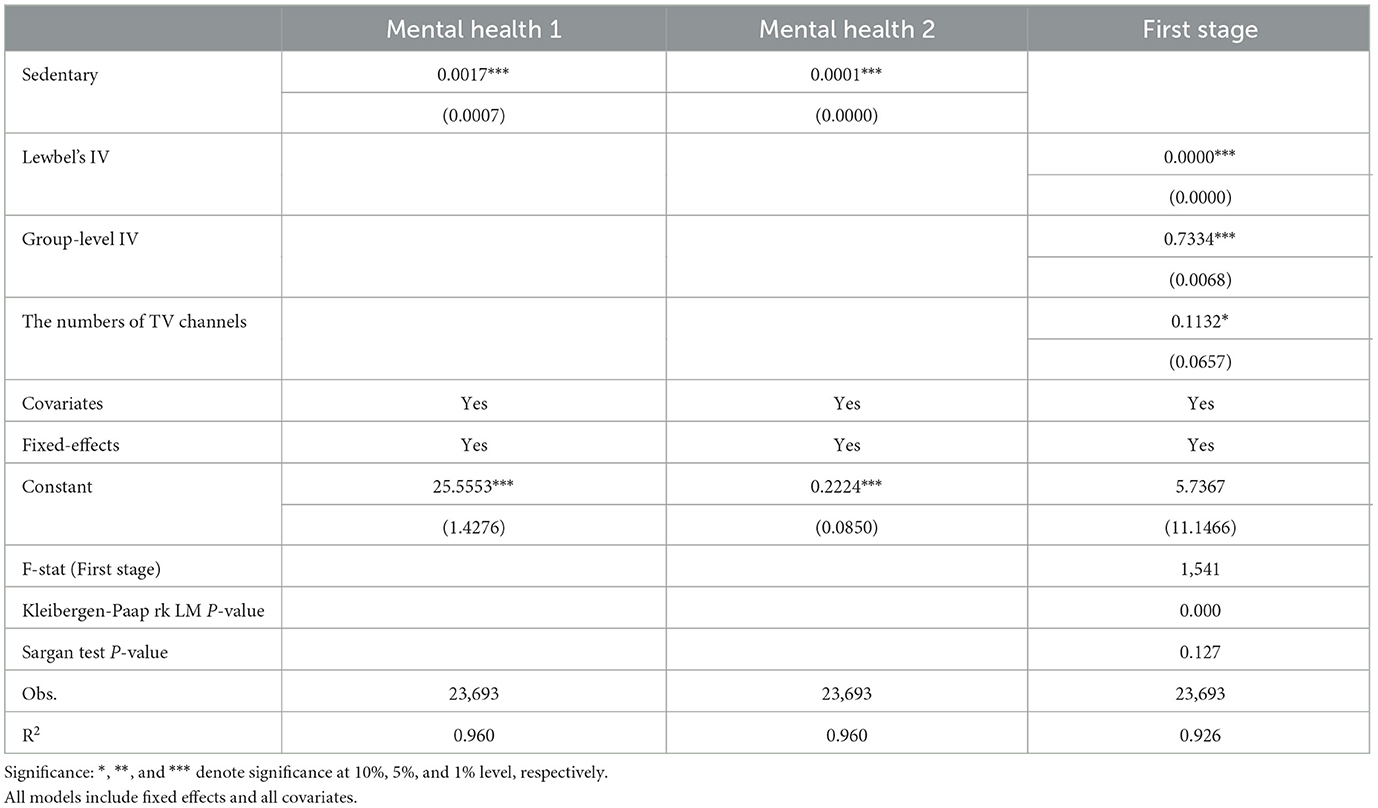
Table 3. Endogenous test of the effect of leisure sedentary time on mental health issues (IV).
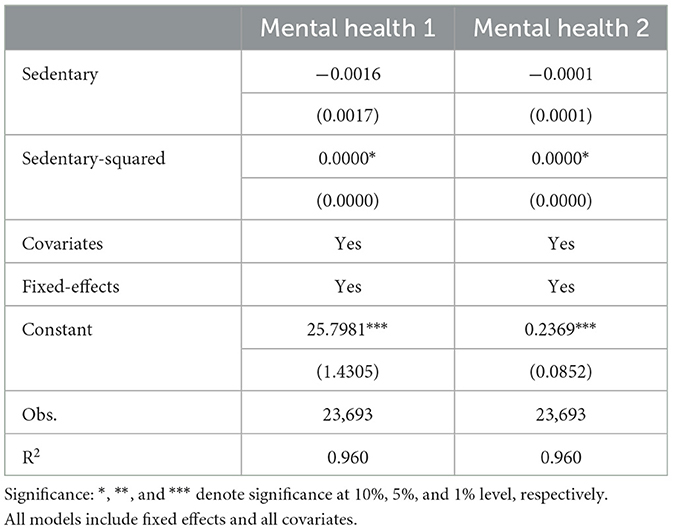
Table 4. The non-linear relationship between leisure sedentary time and mental health issues to examine the validity of Lewbel's IV.
DID method results
Table 5 further presents the results of DID method. The result of the first two columns show that heightened leisure sedentary time is linked with worse mental health issues. Similarity, the coefficients of the first two columns are larger than those in Table 2, suggesting a potential downward bias in the estimates when endogeneity is not addressed. A back-of-the-envelope calculation suggests that one-day sedentary behavior significantly increases in aggregated mental health scores by 0.315 on average, and standardized mental health scores by 0.0143. A basic premise for using the DID model to evaluate policy effects is that the development trends of the explained variables for the treatment and control groups should be consistent before policy implementation in the pilot. In other words, there should be no statistically significant difference between the treatment and control groups before policy implementation. Therefore, it is necessary to conduct a parallel trend test for the DID model. In this study, we use the period prior to policy implementation, specifically 2009, as the reference group. As shown in Column (3), the coefficients of the parallel trend are insignificant before the policy. In 2011, the first period after policy implementation, the coefficients of the parallel trend are insignificant, which may be attributed to policy lag. However, in the second period after policy implementation, namely in 2015, the coefficients of the parallel trend become statistically significant. It indicates that the DID model in this study passes the parallel trend test, thereby validating the regression results presented in Table 5 to some extent.
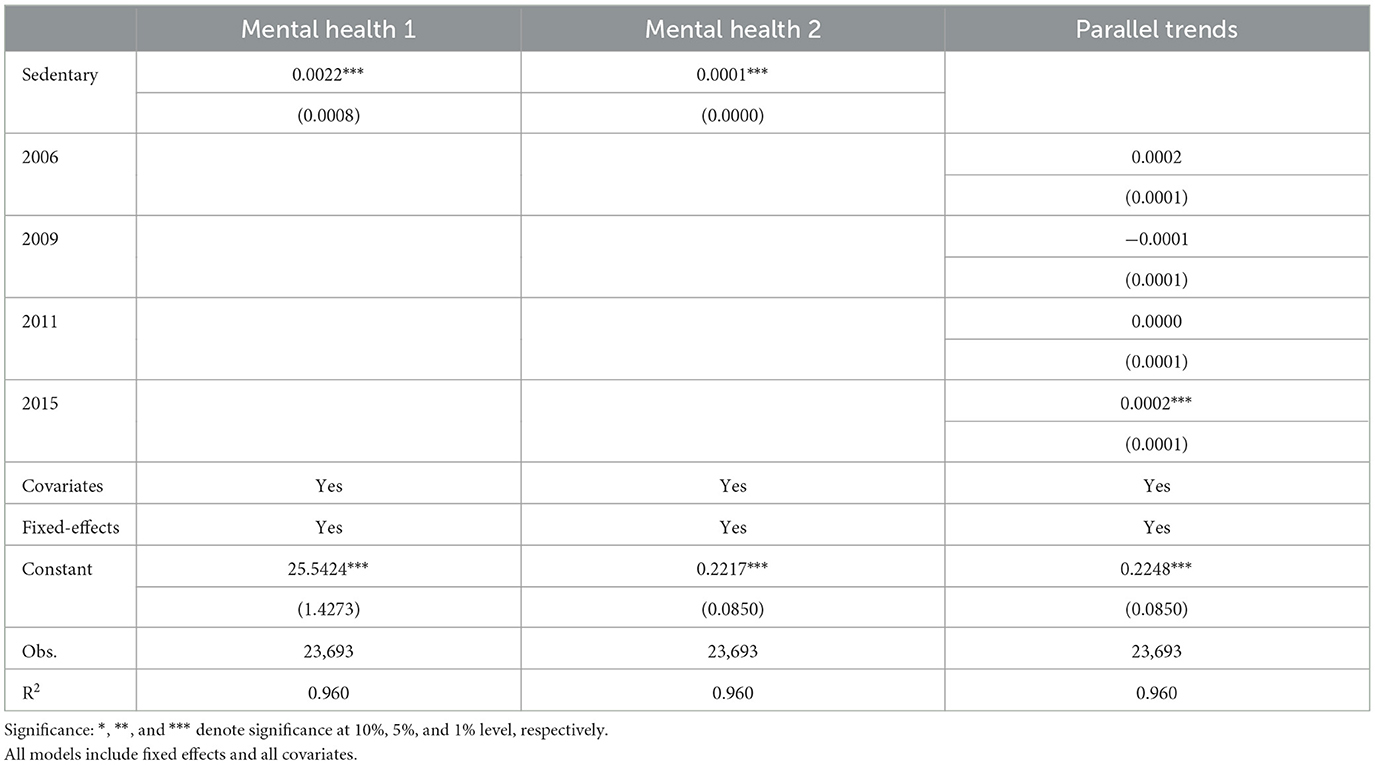
Table 5. Results of DID regressions about the impact of leisure sedentary time on mental health issues.
Moderating effect
The empirical results show that increased leisure sedentary time negatively impacts mental health. Therefore, mitigating this adverse effect is a critical goal for policy interventions and health-promoting behaviors. In this section, we examine moderating factors that may reduce the negative impact of leisure sedentary time on mental health.
First, we examine the moderating role of health literacy. In doing so, we use two measures: whether individuals are familiar with the Chinese Dietary Guidelines (CDG) and whether they have family members who are medical professionals. Familiarity with the CDG reflects a tendency to seek health-related information, while having medical professionals in the family indicates greater health literacy within the household. Based on that, we divide the sample into two groups: those unfamiliar with the CDG vs. those familiar, and households without medical professionals vs. those with medical professionals. Table 6 presents the results. For individuals unfamiliar with the CDG, the coefficient for leisure sedentary time is significantly positive at the 10% level. In contrast, for those familiar with the CDG, the coefficient is positive but not statistically significant at the 10% level. Similarly, households without medical professionals show a significantly positive coefficient at the 5% level, while households with medical professionals exhibit an insignificant coefficient, despite its larger magnitude. These findings indicate that health literacy moderates the relationship between leisure sedentary time and mental health issues, supporting Hypothesis 2a.
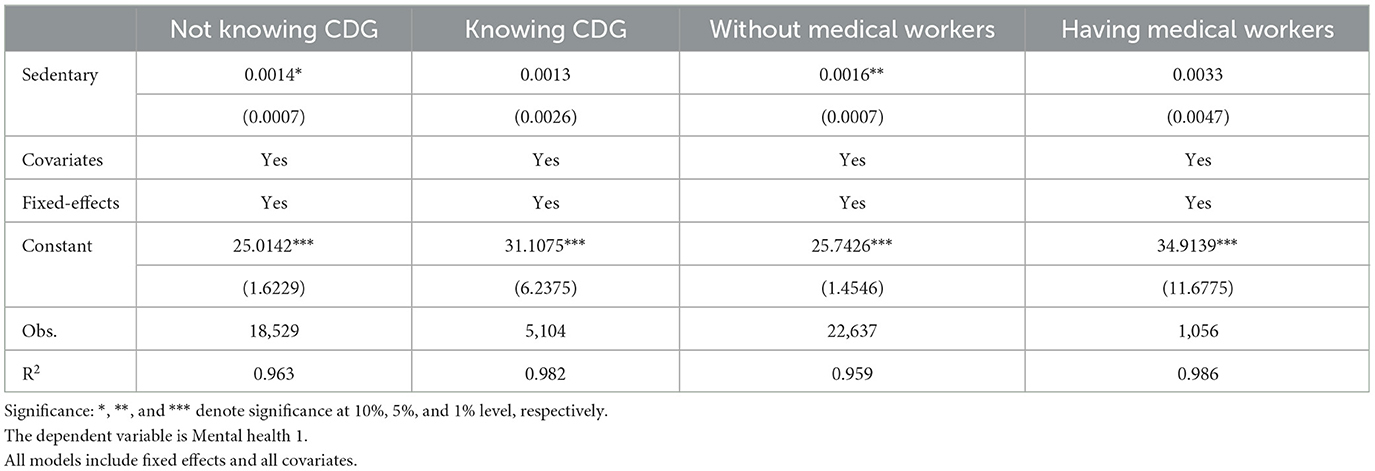
Table 6. Moderating effect—health literacy.
Next, we examine whether reducing prolonged sedentary time improves mental health. We first divide the sample based on the number of accessible TV channels, assuming a correlation between leisure sedentary behavior and television availability. Using the National Digital TV Development Plan as a benchmark, we categorize samples into two groups based on the average number of TV channels before and after 2009 (23 vs. 31 channels). Second, leveraging the longitudinal nature of the CHNS data, we group individuals based on changes in sedentary time over survey years, distinguishing between increased and reduced sedentary time. Table 7 presents the regression results. In the first two columns, households with more TV channels show a stronger negative impact of sedentary time on mental health, reflected by larger coefficients and greater statistical significance. In the last two columns, reduced sedentary time is associated with larger coefficients, though not statistically significant, while increased sedentary time has significant negative effects with a greater magnitude than the baseline regression. These results support Hypothesis 2c.
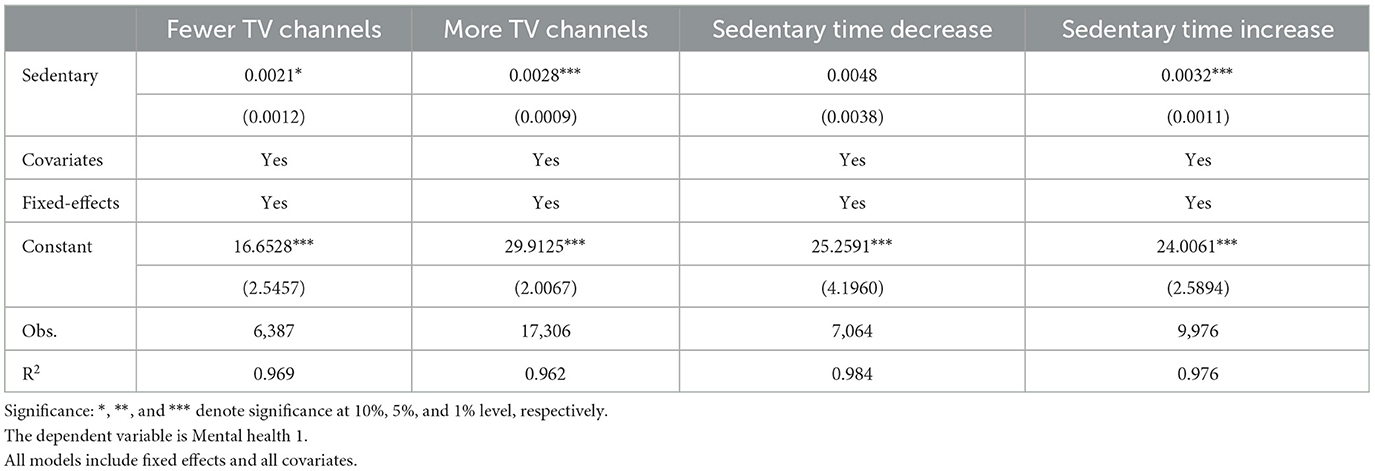
Table 7. Moderating effect—changes in leisure sedentary time.
Finally, we focus on older adults and examine the moderating roles of caregiver gender and social interaction. To investigate Hypothesis 3b, we use the gender composition of caregivers. Older adults are assumed to interact more with female caregivers when daughters constitute the majority of caregivers, as the CHNS does not explicitly ask about the primary caregiver's gender. We also examine the role of urban parks as facilitators of social interaction. Parks provide spaces for physical activity, relaxation, and community engagement, which enhance mental health and wellbeing (88). While beneficial for all age groups, parks hold particular significance for older adults (89). Using the question “Does your house have a park nearby?”, we classify older adults into two groups: those with nearby parks and those without. We hypothesize that proximity to parks promotes social activities, reduces sedentary time, and improves mental health. Table 8 reports the results. In households with predominantly female caregivers, older adults experience fewer mental health issues, as evidenced by smaller coefficients in the first two columns. Regarding social interaction, older adults living near parks exhibit insignificant coefficients, suggesting that social activities mitigate the adverse mental health effects of sedentary behavior. In contrast, individuals without park access show significant and larger coefficients, indicating that limited social interaction exacerbates mental health problems. In summary, these findings support Hypotheses 3a and 3b.
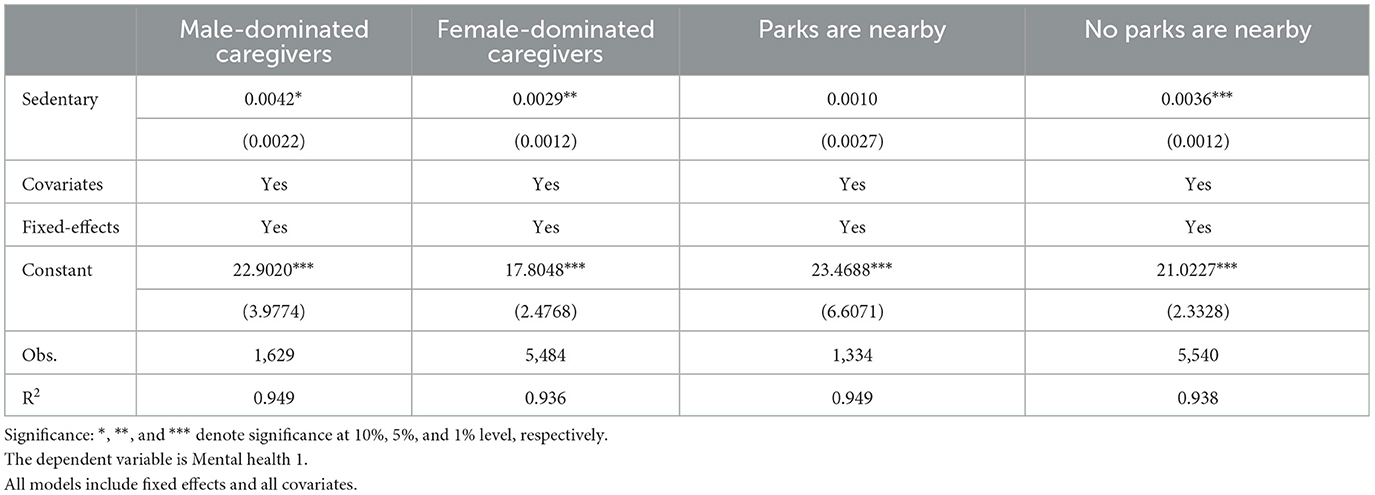
Table 8. Moderating effect—older adults' population.
Mediating effect
The literature suggests that obesity is a potential channel underlying our results. However, it remains necessary to test whether this channel is valid in our context. To address this, we use BMI, overweight status, and waist circumference as mediating factors. In the CHNS, weight is measured to the nearest 0.1 kg using a calibrated beam scale with participants wearing lightweight clothing, while height is measured to the nearest 0.1 cm using a portable stadiometer with participants barefoot (90). BMI (kg/m2) is calculated as a mediating factor, and overweight status is defined as a BMI > 25 based on Chinese criteria (91). Waist circumference is measured at the midpoint between the bottom of the rib cage and the top of the iliac crest at the end of exhalation. Table 9 presents the empirical results. The findings show that increased leisure sedentary time is associated with higher BMI, a greater likelihood of being overweight, and higher waist circumference. These results support Hypothesis 4.
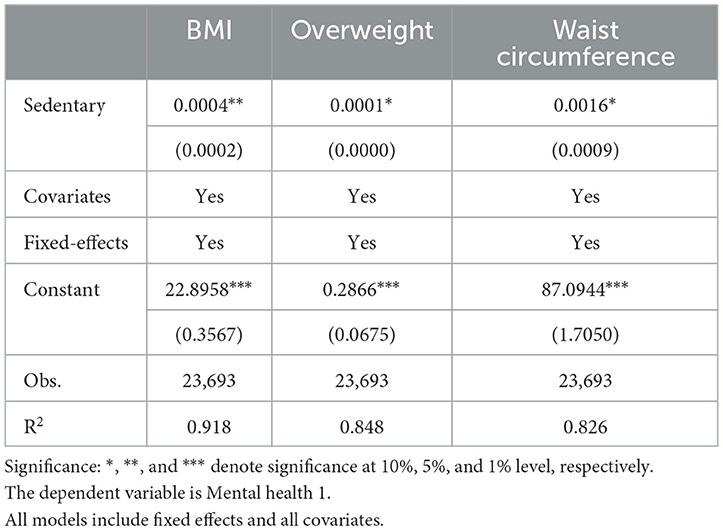
Table 9. Mediating effect—BMI and obesity.
Heterogeneity analyses
In our analysis, we control for occupational sedentary time to address concerns about omitted variable bias in the relationship between occupational sedentary time and mental health. To further examine the role of occupational sedentary time, we conduct a heterogeneous analysis by occupational type. The sample is divided into three categories: light physical work, medium physical work, and heavy physical work. Table 10 presents the results. Individuals engaged in light and medium physical work show a higher risk of mental health issues compared to those in heavy physical work. Moreover, the coefficients in the first two columns are larger than the baseline results, suggesting that individuals with high levels of both leisure and occupational sedentary time face worse mental health outcomes.
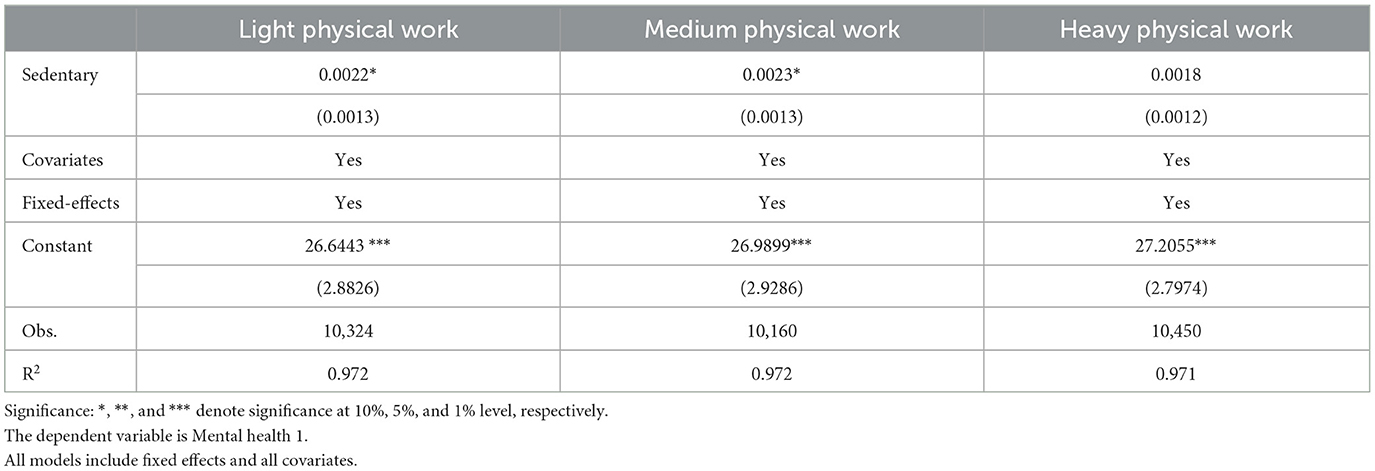
Table 10. Heterogeneity—occupational types.
Robustness analyses
Our analysis focuses on adults who have completed formal education as the main sample. To test whether this sample restriction affects the generalizability of the findings, we perform several subsample analyses to ensure robustness. First, we exclude groups that may bias the results, including the oldest-old population (aged ≥80 years), individuals reporting poor health status, those diagnosed with genetic diseases, recently retired individuals, and individuals diagnosed with muscle diseases. The first three groups are more likely to experience mental health issues, while the last two are more likely to engage in sedentary behavior. Additionally, we randomly select 80% of the sample to further test the model's robustness. Tables 11, 12 present the robustness checks. The results across all subsamples remain consistent with the baseline findings, confirming the reliability of the empirical results.
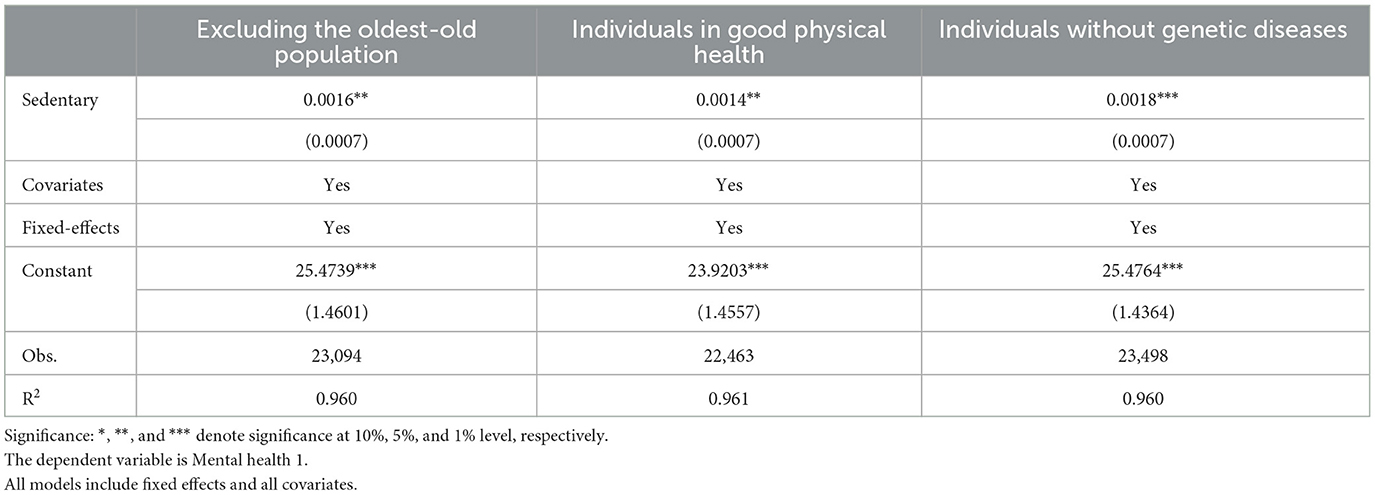
Table 11. Robustness checks 1.
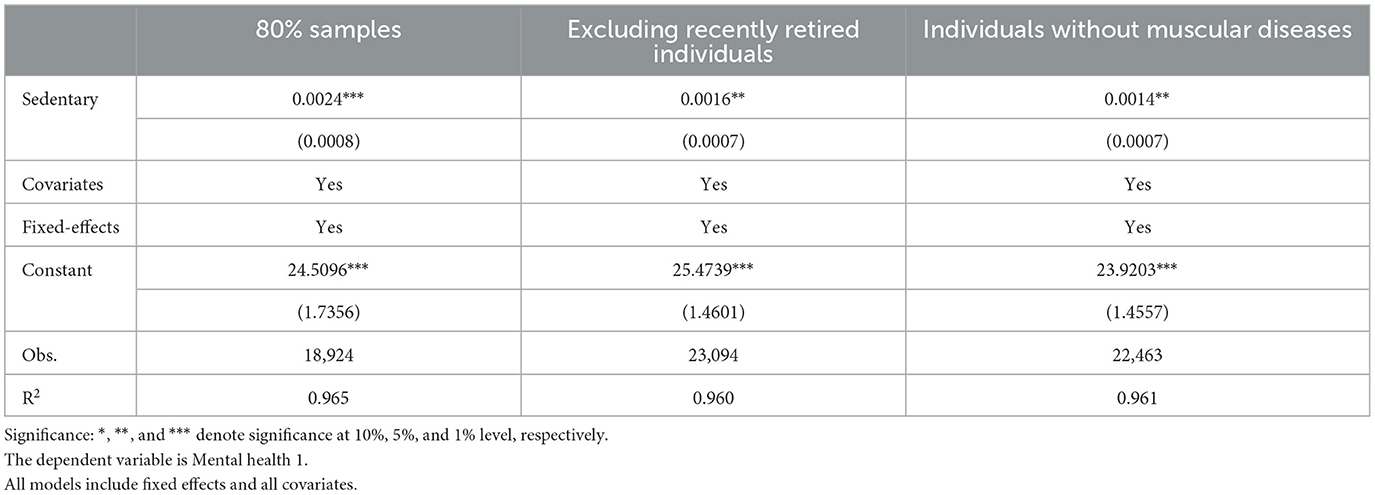
Table 12. Robustness checks 2.
Discussion
In recent decades, technological advancements have transformed daily life, offering convenience and comfort while increasing sedentary time. Prolonged sedentary time has become a defining feature of modern life and a pressing public health concern. Simultaneously, the fast-paced nature of contemporary life has heightened stress levels from work and personal responsibilities, leading many individuals to experience psychological sub-health (92). Thus, understanding the relationship between sedentary time and mental health is therefore crucial.
This article investigates the relationship between leisure sedentary time and mental health issues using a representative longitudinal sample of the Chinese population. By employing Ordinary Least Squares (OLS) regression, instrumental variable methods, and the Difference-in-Differences framework, we find that prolonged leisure sedentary time negatively affects mental health, primarily through its impact on obesity. Our findings align with existing literature on the adverse effects of sedentary behavior on mental health, which has primarily relied on cross-sectional data.
We also identify several moderating factors unique to the Chinese context that may mitigate the negative effects of sedentary time. These include promoting health literacy and reducing sedentary time across the population, as well as fostering caregiving by women and enhancing social interactions for older adults. First, in January 2008, the Chinese Ministry of Health issued the “Chinese Resident Health Literacy—Basic Knowledge and Skills (Trial),” the first government document defining health literacy. This initiative marked a critical step in promoting health education in China. However, subsequent surveys revealed that health literacy rates were only 8.8% in 2012 and 11.58% in 2016 (93, 94). By 2023, the rate had improved to 29.7% (95), but it remains low compared to other countries. Improving health literacy is therefore essential to preventing health issues and promoting wellbeing. Second, the eldercare system in China predominantly follows the “9073” structure: 90% of older adults are cared for by family members, 7% by community services, and 3% in nursing homes. Filial piety, a cultural virtue emphasizing respect and care for one's parents, underpins this model. Traditionally, sons bore the primary responsibility for eldercare. However, with the One-Child Policy and rising female workforce participation, daughters now provide both practical and emotional support (96). Intergenerational support, particularly emotional support, has been shown to reduce the stress of aging and positively influence health outcomes. Third, social interactions, which include personal and environmental interactions, are vital for mental health and psychological wellbeing. Older adults who actively engage in social activities report lower levels of loneliness (97). Accessible destinations such as parks, squares, and cultural facilities foster social connections. Parks, in particular, have been shown to encourage physical activity and social ties, contributing to better mental health and reduced sedentary behaviors (98, 99).
Regarding mechanisms, we identify obesity as a primary mediating factor. Additionally, prior research suggests other pathways: screen-based activities may overstimulate the central nervous system, increasing anxiety (100), while disrupted sleep patterns linked to screen use can exacerbate anxiety (101). Prolonged sedentary behavior is also associated with increased inflammatory markers, which may impact mental health (102).
Our findings yield three policy implications. First, prolonged sedentary time worsens mental health, underscoring the need for government campaigns to raise awareness about its risks. Efforts should focus on improving health literacy, as health literacy interventions have been shown to foster behavior change (103). For example, the Healthy China 2030 Plan identifies health literacy as a key strategy for improving public health. Additionally, local governments should also provide accessible fitness equipment and promote physical activity through initiatives like urban greenways, which have been shown to reduce sedentary behavior (104). Second, governments should support female caregivers, especially daughters, who play a crucial role in eldercare. Policies could include financial incentives or tax benefits for caregiving daughters and encourage employers to offer flexible work arrangements for women engaged in eldercare, such as remote work or part-time schedules. Third, creating accessible and engaging spaces for older adults can reduce sedentary behavior. Governments could subsidize social activities, such as senior tour groups, while communities could promote participation in local events to foster social interaction.
This study also has limitations. First, the findings are rooted in China's cultural and institutional context. Factors such as Confucian traditions and the health system shape health behaviors and outcomes, so caution is needed when generalizing these results to other countries. Replication studies in diverse settings could enhance external validity. Second, sedentary time was self-reported, which may lead to underestimation. Combining self-reports with accelerometer data in future research could improve accuracy. Third, while the fixed-effects method, IV method and DID method mitigate endogeneity, residual bias or confounding variables may persist. Experimental designs could further validate these findings. Finally, data limitations prevented an in-depth exploration of biological pathways, which future studies could address.
Conclusion
In conclusion, our research finds that prolonged leisure sedentary time negatively affects mental health. Additionally, our study reveals moderating roles of promoting health literacy and reducing sedentary time across the population, as well as fostering caregiving by women and enhancing social interactions for older adults. Finally, we identify obesity as a primary mediating factor. The above findings are significant given the global rise in both sedentary behaviors and mental health challenges.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
CHNS was approved by the Institutional Review Board at the University of North Carolina at Chapel Hill and local IRB (Institutional Review Board or Ethics Committee). The patients/participants provided their written informed consent to participate in this study.
Author contributions
HL: Conceptualization, Formal analysis, Writing – original draft. WZ: Supervision, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was supported by the Social Sciences Funds of Shannxi Province in China under Grant numbers 2020D004.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
1. ^The dietary knowledge index includes 1) Eating vegetables and fruits is beneficial to health; 2) Eating less sugar is beneficial to health; 3) Eating a variety of foods is beneficial to health; 4) Eating less high-fat food is beneficial to health; 5) Eating dairy products is beneficial to health; 6) Eating soy products is beneficial to health.
References
1. Bauman A, Ainsworth BE, Sallis JF, Hagstromer M, Craig CL, Bull FC, et al. The descriptive epidemiology of sitting. A 20-country comparison using the international physical activity questionnaire (IPAQ). Am J Prev Med. (2011) 41:228–35. doi: 10.1016/j.amepre.2011.05.003
2. Loyen A, van der Ploeg HP, Bauman A, Brug J, Lakerveld J. European sitting championship: prevalence and correlates of self-reported sitting time in the 28 European Union member states. PLoS ONE. (2016) 11:e0149320. doi: 10.1371/journal.pone.0149320
3. Peters TM, Moore SC, Xiang YB, Yang G, Shu XO, Ekelund U, et al. Accelerometer-measured physical activity in Chinese adults. Am J Prev Med. (2010) 38:583–91. doi: 10.1016/j.amepre.2010.02.012
4. Diaz KM, Howard VJ, Hutto B, Colabianchi N, Vena JE, Safford MM, et al. Patterns of sedentary behavior and mortality in us middle-aged and older adults: a national cohort study. Ann Intern Med. (2017) 167:465–75. doi: 10.7326/M17-0212
5. Pedersen BK. IL-6 signalling in exercise and disease. Biochem Soc Trans. (2007) 35:1295–7. doi: 10.1042/BST0351295
6. Teychenne M, Ball K, Salmon J. Sedentary behavior and depression among adults: a review. Int J Behav Med. (2010) 17:246–54. doi: 10.1007/s12529-010-9075-z
7. Huang Y, Li L, Gan Y, Wang C, Jiang H, Cao S, et al. Sedentary behaviors and risk of depression: a meta-analysis of prospective studies. Transl Psychiatry. (2020) 10:26. doi: 10.1038/s41398-020-0715-z
8. Higgins S, Pomeroy A, Bates LC, Paterson C, Barone Gibbs B, Pontzer H, et al. Sedentary behavior and cardiovascular disease risk: An evolutionary perspective. Front Physiol. (2022) 13:962791. doi: 10.3389/fphys.2022.962791
9. Hoare E, Milton K, Foster C, Allender S. The associations between sedentary behaviour and mental health among adolescents: a systematic review. Int J Behav Nutr Phys Act. (2016) 13:108. doi: 10.1186/s12966-016-0432-4
10. Fu X, Zhang K, Chen X. The Report on the Development of China's National Mental Health (2019-2020). Beijing: Social Sciences Academic Press.
11. Phillips MR, Zhang J, Shi Q, Song Z, Ding Z, Pang S, et al. Prevalence, treatment, and associated disability of mental disorders in four provinces in China during 2001–05: an epidemiological survey. Lancet. (2009) 373:2041–53. doi: 10.1016/S0140-6736(09)60660-7
12. Tsai AC, Chi SH, Wang JY. Cross-sectional and longitudinal associations of lifestyle factors with depressive symptoms in >/= 53-year old Taiwanese—results of an 8-year cohort study. Prev Med. (2013) 57:92–7. doi: 10.1016/j.ypmed.2013.04.021
13. Levinson D, Kaplan G. What does self rated mental health represent. J Public Health Res. (2014) 3:287. doi: 10.4081/jphr.2014.287
14. Nagasu M, Kogi K, Yamamoto I. Association of socioeconomic and lifestyle-related risk factors with mental health conditions: a cross-sectional study. BMC Public Health. (2019) 19:1759. doi: 10.1186/s12889-019-8022-4
15. Taylor GMJ, Itani T, Thomas KH, Rai D, Jones T, Windmeijer F, et al. Prescribing prevalence, effectiveness, and mental health safety of smoking cessation medicines in patients with mental disorders. Nicotine Tob Res. (2020) 22:48–57. doi: 10.1093/ntr/ntz072
16. Awaworyi Churchill S, Farrell L. Alcohol and depression: evidence from the 2014 health survey for England. Drug Alcohol Depend. (2017) 180:86–92. doi: 10.1016/j.drugalcdep.2017.08.006
17. Haw C, Hawton K, Casey D, Bale E, Shepherd A. Alcohol dependence, excessive drinking and deliberate self-harm. Soc Psychiat Epidemiol. (2005) 40:964–71. doi: 10.1007/s00127-005-0981-3
18. You Y, Chen Y, Wei M, Tang M, Lu Y, Zhang Q, et al. Mediation role of recreational physical activity in the relationship between the dietary intake of live microbes and the systemic immune-inflammation index: a real-world cross-sectional study. Nutrients. (2024) 16:777. doi: 10.3390/nu16060777
19. You Y. Accelerometer-measured physical activity and sedentary behaviour are associated with C-reactive protein in US adults who get insufficient sleep: A threshold and isotemporal substitution effect analysis. J Sports Sci. (2024) 42:527–36. doi: 10.1080/02640414.2024.2348906
20. You Y, Chen Y, Zhang Y, Zhang Q, Yu Y, Cao Q. Mitigation role of physical exercise participation in the relationship between blood cadmium and sleep disturbance: a cross-sectional study. BMC Public Health. (2023) 23:1465. doi: 10.1186/s12889-023-16358-4
21. You Y, Wang R, Li J, Cao F, Zhang Y, Ma X. The role of dietary intake of live microbes in the association between leisure-time physical activity and depressive symptoms: a population-based study. Appl Physiol Nutr Metab. (2024) 49:1014–24. doi: 10.1139/apnm-2023-0550
22. Zhai I, Zhang Y, Zhang D. Sedentary behaviour and the risk of depression. A meta-analysis Br J Sports Med. (2015) 49:705–9. doi: 10.1136/bjsports-2014-093613
23. Vancampfort D, Stubbs B, Mugisha J, Firth J, Schuch FB, Koyanagi A. Correlates of sedentary behavior in 2,375 people with depression from 6 low- and middle-income countries. J Affect Disord. (2018) 234:97–104. doi: 10.1016/j.jad.2018.02.088
24. Hamer M, Stamatakis E, Mishra GD. Television- and screen-based activity and mental well-being in adults. Am J Prev Med. (2010) 38:375–80. doi: 10.1016/j.amepre.2009.12.030
25. Peng J, Ren H. The association of physical activity and leisure-time sedentary behavior with perceived stress among Chinese adults: a cross-sectional study based on the Chinese health and nutrition survey data. Prev Med Rep. (2024) 45:102829. doi: 10.1016/j.pmedr.2024.102829
26. Cao B, Zhao Y, Ren Z, McIntyre RS, Teopiz KM, Gao X, et al. Are physical activities associated with perceived stress? the evidence from the China health and nutrition survey, Front Public Health. (2021) 9:697484. doi: 10.3389/fpubh.2021.697484
27. Primack BA, Swanier B, Georgiopoulos AM, Land SR, Fine MJ. Association between media use in adolescence and depression in young adulthood: a longitudinal study. Arch Gen Psychiatry. (2009) 66:181–8. doi: 10.1001/archgenpsychiatry.2008.532
28. Konopka M, Köhler S, Stehouwer C, Schaper N, Henry R, Van der Kallem C, et al. Accelerometer-derived sedentary time and physical activity and the incidence of depressive symptoms – the Maastricht study. Psychol Med. (2020) 52:1–8. doi: 10.1017/S0033291720004924
29. Appelqvist-Schmidlechner K, Raitanen J, Vasankari T, Kyröläinen H, Häkkinen A, Honkanen T, et al. Relationship between accelerometer-based physical activity, sedentary behavior, and mental health in young finnish men. Front Public Health. (2022) 10:820852. doi: 10.3389/fpubh.2022.820852
30. Yu H, Alizadeh F. Ameliorative effects of television watching behavior and motivation on the fear of COVID-19 in Older Chinese adults during the pandemic. Psychol Res Behav Manag. (2024) 17:2631–40. doi: 10.2147/PRBM.S462085
31. Haeri-Mehrizi A, Mohammadi S, Rafifar S, Sadighi J, Kermani RM, Rostami R, et al. Health literacy and mental health: a national cross-sectional inquiry. Sci Rep. (2024) 14:13639. doi: 10.1038/s41598-024-64656-7
32. Saunders TJ, MacDonald DJ, Copeland JL, Longmuir PE, Barnes JD, Belanger K, et al. The relationship between sedentary behaviour and physical literacy in Canadian children: a cross-sectional analysis from the RBC-CAPL Learn to Play study. BMC Public Health. (2018) 18:1037. doi: 10.1186/s12889-018-5892-9
33. Bull FC, al-Ansari SS, Biddle S, Borodulin K, Buman MP, Cardon G, et al. World Health Organization 2020 guidelines on physical activity and sedentary behavior. Br J Sports Med. (2020) 54:1451–62. doi: 10.1136/bjsports-2020-102955
34. Greenwood-Hickman MA, Renz A, Rosenberg DE. Motivators and barriers to reducing sedentary behavior among overweight and obese older adults. Gerontologist. (2016) 56:660–8. doi: 10.1093/geront/gnu163
35. Parry S, Straker L, Gilson ND, Smith AJ. Participatory workplace interventions can reduce sedentary time for office workers–a randomised controlled trial. PLoS ONE. (2013) 8:e78957. doi: 10.1371/journal.pone.0078957
36. De Mendonça Lima CA, Ivbijaro G. Mental health and wellbeing of older people: opportunities and challenges. Ment Health Fam Med. (2013) 10:125.
37. Leask CF, Harvey JA, Skelton DA. Exploring the context of sedentary behaviour in older adults (what, where, why, when and with whom). Eur Rev Aging Phys Activity. (2015) 12:1–8. doi: 10.1186/s11556-015-0146-7
38. Zhou LY. Theory of confucian culture of the negative effects on the development of China's commercial law. J Law Soc. (2014) 10:3–4. doi: 10.19387/j.carolcarrollnki
39. Shi Z. Does the number of children matter to the happiness of their parents? J Chin Sociol. (2016) 3:1–24. doi: 10.1186/s40711-016-0031-4
40. Ng HY, Griva K, Lim HA, Tan JY. The burden of filial piety: A qualitative study on caregiving motivations amongst family caregivers of patients with cancer in Singapore. Psychol Health. (2016) 31:1293–310. doi: 10.1080/08870446.2016.1204450
41. Norton E. Chapter 17 long-term care. Handb Health Econ. (2000) 1:955–94. doi: 10.1016/S1574-0064(00)80030-X
42. Aronson, J. Women's sense of responsibility for the care of old people: “But who else is going to do it?”. Gender Soc. (1992) 6: 8–29. doi: 10.1177/089124392006001002
43. Fleming PJ. Current trends in the study of gender norms and health behaviors. Curr Opini Psychol. (2015) 5:72–7. doi: 10.1016/j.copsyc.2015.05.001
44. Zhao P, Zhang Y, Harper S, Zeng W, Li S. Functional transitions among older adults in rural China: examining the differential roles of care from daughters' and sons' families. J Gerontol: Series B. (2024) 79:gbae133. doi: 10.1093/geronb/gbae133
45. Park S, Smith J, Dunkle RE. Social network types and well-being among South Korean older adults. Aging Men Health. (2014) 18:72–80. doi: 10.1080/13607863.2013.801064
46. Kawachi I, Kennedy BP, Glass R. Social capital and self-rated health: a contextual analysis. Am J Public Health. (1999) 89:1187–93. doi: 10.2105/AJPH.89.8.1187
47. McNeill LH, Kreuter MW, Subramanian S. Social environment and physical activity: a review of concepts and evidence. Soc Sci Med. (2006) 63:1011–22. doi: 10.1016/j.socscimed.2006.03.012
48. Forrest R, Kearns A. Social cohesion, social capital and the neighbourhood. Urban Stud. (2001) 38:2125–43. doi: 10.1080/00420980120087081
49. Bullock VE, Griffiths P, Sherar LB, Clemes SA. Sitting time and obesity in a sample of adults from Europe and the USA. Ann Hum Biol. (2017) 44:230–6. doi: 10.1080/03014460.2016.1232749
50. Gregor MF, Hotamisligil GS. Inflammatory mechanisms in obesity. Annu Rev Immunol. (2011) 29:415–45 doi: 10.1146/annurev-immunol-031210-101322
51. Miller AH, Raison CL. The role of inflammation in depression: from evolutionary imperative to modern treatment target. Nat Rev Immunol. (2016) 16:22–34. doi: 10.1038/nri.2015.5
52. Huppert FA. Psychological well-being: evidence regarding its causes and consequences. Appl Psychol. (2009) 1:137–64. doi: 10.1111/j.1758-0854.2009.01008.x
53. Chen F, Zhang X, Chen Z. Air pollution and mental health: evidence from China Health and Nutrition Survey. J Asian Econ. (2023) 86:101611. doi: 10.1016/j.asieco.2023.101611
54. Lee Y-H, Shelley M, Liu C-T, Chang Y-C. Assessing the association of food preferences and self-reported psychological well-being among middle-aged and older adults in contemporary China-results from the China Health and Nutrition Survey. Int J Environ Res Public Health. (2018) 15:463. doi: 10.3390/ijerph15030463
55. Wu T, Hou X, Zhang F, Sharma M, Zhao Y, Shi Z. Association between self-reported food preferences and psychological well-being during perimenopausal period among chinese women. Front Psychol. (2020) 11:1196. doi: 10.3389/fpsyg.2020.01196
56. Yang TZ, Huang HT. An epidemiological study on stress among urban residents in social transition period. Chin J Epidemiol. (2003) 9:11–5. doi: 10.3760/j.issn:0254-6450.2003.09.004
57. Cristóbal-Narváez P, Haro JM. Perceived stress and depression in 45 low- and middle-income countries. J Affect Disord. (2020) 274:799–805. doi: 10.1016/j.jad.2020.04.020
58. Mundy EA, Weber M, Rauch SL, Killgore WDS, Simon NM, Pollack MH, et al. Adult anxiety disorders in relation to trait anxiety and perceived stress in childhood. Psychol Rep. (2015) 117:473–89. doi: 10.2466/02.10.PR0.117c17z6
59. Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. (1983) 24:385–96. doi: 10.2307/2136404
60. Huang F, Wang H, Wang Z, Zhang J, Du W, Su C, et al. Psychometric properties of the perceived stress scale in a community sample of Chinese. BMC Psychiatry. (2020) 20:130. doi: 10.1186/s12888-020-02520-4
61. Du SF, Wang HJ, Zhang B, Zhai FY, Popkin BM. China in the period of transition from scarcity and extensive undernutrition to emerging nutrition-related non-communicable diseases, 1949-1992. Obes Rev. (2014) 1:8–15. doi: 10.1111/obr.12122
62. Wei X, Zang Y, Jia X, He X, Zou S, Wang H, et al. Age, period and cohort effects and the predictors of physical activity and sedentary behaviour among Chinese children, from 2004 to 2011. BMC Public Health. (2017) 17:353. doi: 10.1186/s12889-017-4215-x
63. Sedentary Behaviour Research Network. Letter to the editor: standardized use of the terms “sedentary” and “sedentary behaviours”. Appl Physiol Nutr Metab. (2012) 37:540–2. doi: 10.1139/h2012-024
64. Lubans DR, Hesketh K, Cliff DP, Barnett LM, Salmon J, Dollman J, et al. A systematic review of the validity and reliability of sedentary behaviour measures used with children and adolescents. Obes Rev. (2011) 12:781–99. doi: 10.1111/j.1467-789X.2011.00896.x
65. Yan Z, Xiang N, Meng J, Liang H, Yue Z. Understanding the effect of retirement on health behaviors in China: Causality, heterogeneity and time-varying effect. Front Public Health. (2022) 10:952072. doi: 10.3389/fpubh.2022.952072
66. You Y, Chen Y, Liu R, Zhang Y, Wang M, Yang Z, et al. Inverted U-shaped relationship between sleep duration and phenotypic age in US adults: a population-based study. Sci Rep. (2024) 14:6247. doi: 10.1038/s41598-024-56316-7
67. Li H, Zeng W. Leisure sedentary time and elevated blood pressure: evidence from the statutory retirement policy. Front Public Health. (2024) 12:1468221. doi: 10.3389/fpubh.2024.1468221
68. Sakakibara K, Miyanaka D, Tokita M, Kawada M, Mori N, Hamsyah F, et al. Association of work-related sedentary behavior with mental health and work engagement among Japanese White- and Blue-Collar workers. J Occup Environ Med. (2023) 65:e695–702. doi: 10.1097/JOM.0000000000002952
69. Hosker DK, Elkins RM, Potter MP. Promoting mental health and wellness in youth through physical activity, nutrition, andsleep. Child Adolesc Psychiatr Clin N Am. (2019) 28:171–93. doi: 10.1016/j.chc.2018.11.010
70. Ramin S, Mysz MA, Meyer K, Capistrant B, Lazovich D, Prizment A. A prospective analysis of dietary fiber intake and mental health quality of life in the Iowa Women's Health Study. Maturitas. (2020) 131:1–7. doi: 10.1016/j.maturitas.2019.10.007
71. Zhang J, Yang SX, Wang L, Han LH, Wu XY. The influence of sedentary behaviour on mental health among children and adolescents: a systematic review and meta-analysis of longitudinal studies. J Affect Disord. (2022) 306:90–114. doi: 10.1016/j.jad.2022.03.018
72. van der Ploeg HP, Hillsdon M. Is sedentary behaviour just physical inactivity by another name? Int J Behav Nutr Phys Act. (2017) 14:142. doi: 10.1186/s12966-017-0601-0
73. Raney JH, Testa A, Jackson DB, Ganson KT, Nagata JM. Associations between adverse childhood experiences, adolescent screen time and physical activity during the COVID-19 pandemic. Acad Pediatr. (2022) 22:1294–9. doi: 10.1016/j.acap.2022.07.007
74. Swedo EA, D'Angelo DV, Fasula AM, Clayton HB, Ports KA. Associations of adverse childhood experiences with pregnancy and infant health. Am J Prev Med. (2023) 64:512–24. doi: 10.1016/j.amepre.2022.10.017
75. Copeland JL, Ashe MC, Biddle SJH, Brown WJ, Buman MP, Chastin S, et al. Sedentary time in older adults: a critical review of measurement, associations with health, and interventions. Br J Sports Med. (2017) 51:1539. doi: 10.1136/bjsports-2016-097210
76. Clayborne ZM, Colman I. Associations between depression and health behaviour change: findings from 8 cycles of the Canadian Community Health Survey. Can J Psychiatry. (2019) 64:30–8. doi: 10.1177/0706743718772523
77. Munasib A, Bhattacharya S. Is the ‘Idiot's Box' raising idiocy? Early and middle childhood television watching and child cognitive outcome. Econ Educ Rev. (2010) 29:873–83. doi: 10.1016/j.econedurev.2010.03.005
78. Lewbel A. Constructing instruments for regressions with measurement error when no additional data are available, with an application to patents and R&D. Econometrica. (1997) 65:1201–13. doi: 10.2307/2171884
79. Ebbes P, Bockenholt U, Wedel, M. Regressor and random-effects dependencies in multilevel models. Statistica Neerlandica. (2004) 58:161–78. doi: 10.1046/j.0039-0402.2003.00254.x
80. Mingyi W, Zhongyi Z, Xiaoyu L, Siwei X. Labor price distortion and export product markups: Evidence from China labor market. China Econ Rev. (2023) 77:101901. doi: 10.1016/j.chieco.2022.101901
81. Calcagnini G, Farabullini F. The impact of guarantees on bank loan interest rates. Appl Financ Econ. (2014) 24:397–412. doi: 10.1080/09603107.2014.881967
82. Duflo E, Saez E. Participation and investment decisions in a retirement plan: the influence of colleagues' choices. J Public Econ. (2000) 85:121–48. doi: 10.1016/S0047-2727(01)00098-6
83. Evans WN, Oates W, Schwab RM. Measuring peer group effects: a study of teenage behavior. J Polit Econ. (1992) 100:966–91. doi: 10.1086/261848
84. Krueger AA. Estimates of the economic return to schooling from a new sample of twins. Am Econ Rev. (1994) 84:5. Available at: https://www.jstor.org/stable/2117766
85. Williams K. Marital status, marital transitions, and health: a gendered life course perspective. J Health Soc Behav. (2004) 45:81–98. doi: 10.1177/002214650404500106
86. Taylor GMJ, Sawyer K, Kessler D, Munafò MR, Aveyard P, Shaw A. Views about integrating smoking cessation treatment within psychological services for patients with common mental illness: a multi-perspective qualitative study. Health Expect. (2021) 24:411–20. doi: 10.1111/hex.13182
87. Ding C, Feng G, Yuan F, Gong W, Yao Y, Ma Y, et al. Temporal trends and recent correlates in sedentary behaviors among Chinese adults from 2002 to 2010–2012. Int J Environ Res Public Health. (2020) 17:158. doi: 10.3390/ijerph17010158
88. Tinsley HEA, Tinsley DJ, Croskeys CE. Park usage, social milieu, and psychosocial benefits of park use reported by older urban park users from four ethnic groups. Leis Sci. (2002) 24:199–218. doi: 10.1080/01490400252900158
89. Clarke P, Nieuwenhuijsen ER. Environments for healthy ageing: a critical review. Maturitas. (2009) 64:14–9. doi: 10.1016/j.maturitas.2009.07.011
90. Xi B, Liang Y, He T, Reilly KH, Hu Y, Wang Q, et al. Secular trends in the prevalence of general and abdominal obesity among Chinese adults, 1993-2009. Obes Rev. (2012) 13:287–96. doi: 10.1111/j.1467-789X.2011.00944.x
91. Luo H, Li J, Zhang Q, Cao P, Ren X, Fang A, et al. Obesity and the onset of depressive symptoms among middle-aged and older adults in China: evidence from the CHARLS. BMC Public Health. (2018) 18:909. doi: 10.1186/s12889-018-5834-6
92. Galderisi S, Heinz A, Kastrup M, Beezhold J, Sartorius N. Toward a new definition of mental health. World Psychiatry. (2015) 14:231–3. doi: 10.1002/wps.20231
93. Li L, Li YH, Nie XQ, Huang XG, Shi MF, et al. Influence factors of health literacy monitoring of Chinese residents on 2012. Chinese J Health Educ. (2015) 2:104–7. doi: 10.16168/j.cnki.issn.1002-9982.2015.02.002
94. National Health and Family Planning Commission. Results of Chinese Residents Health Literacy in 2016 was Released. (2017). Available at: http://www.gov.cn/xinwen/2017-11/22/content_5241572.htm (accessed November 22, 2017).
95. Health Literacy Level of Chinese. Residents to Increase to 29.70 Per cent by 2023. (2023). Available at: http://www.nhc.gov.cn/xcs/s3582/202404/287e15ca9fd148b5ab9debce59f58c6d.shtml (accessed April 24, 2024).
96. Zhang Y, Harper S. Son or daughter care in relation to self-reported health outcomes for older adults in China. Front Public Health. (2022) 9:793873. doi: 10.3389/fpubh.2021.793873
97. Wang J, Zhou Y, Zhang Q, Li J, Zhai D, Li J, et al. Loneliness among older Chinese individuals: the status quo and relationships with activity-related factors. BMC Geriatr. (2024) 24:42. doi: 10.1186/s12877-023-04611-9
98. Twohig-Bennett C, Jones A. The health benefits of the great outdoors: a systematic review and meta-analysis of greenspace exposure and health outcomes. Environ Res. (2018) 166:628–37. doi: 10.1016/j.envres.2018.06.030
99. Edwards N, Hooper P. The park physical activity questionnaire (Park-PAQ): a reliable measurement tool for park-based and total physical activity. Health Place. (2023) 83:103085. doi: 10.1016/j.healthplace.2023.103085
100. Wang X, Perry AC. Metabolic and physiologic responses to video game play in 7- to 10-year-old boys. Arch Pediatr Adolesc Med. (2006) 160:411–5. doi: 10.1001/archpedi.160.4.411
101. Dworak M, Schierl T, Bruns T, Struder HK. Impact of singular excessive computer game and television exposure on sleep patterns and memory performance of school-aged children. Pediatrics. (2007) 120:978–85. doi: 10.1542/peds.2007-0476
102. McMahon EM, Corcoran P, O'Regan G, Keeley H, Cannon M, Carli V, et al. Physical activity in European adolescents and associations with anxiety, depression and well-being. Eur Child Adolesc Psychiatry. (2017) 26:111–22. doi: 10.1007/s00787-016-0875-9
103. Walters R, Leslie SJ, Polson R, Cusack T, Gorely T, et al. Establishing the efficacy of interventions to improve health literacy and health behaviours: a systematic review. BMC Public Health. (2020) 20:1040. doi: 10.1186/s12889-020-08991-0
Keywords: risky health behavior, leisure sedentary time, mental health, health-promoting behavior, China
Citation: Li H and Zeng W (2025) Is leisure sedentary time associated with mental health issues? Evidence from China Health and Nutrition Survey. Front. Public Health 13:1517830. doi: 10.3389/fpubh.2025.1517830
Received: 27 October 2024; Accepted: 17 January 2025;
Published: 06 February 2025.
Edited by:
Huixuan Zhou, Beijing Sport University, ChinaReviewed by:
Yanwei You, Tsinghua University, ChinaYuquan Chen, Monash University, Australia
Sungjin Park, Yonsei University, Republic of Korea
Copyright © 2025 Li and Zeng. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Weihong Zeng, emVuZ3doQG1haWwueGp0dS5lZHUuY24=