 Sarah M. Bannon
Sarah M. Bannon Andy Rapoport
Andy Rapoport Allison J. Applebaum3
Allison J. Applebaum3
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
POLICY AND PRACTICE REVIEWS article
Front. Public Health, 05 March 2025
Sec. Aging and Public Health
Volume 13 - 2025 | https://doi.org/10.3389/fpubh.2025.1515440
This article is part of the Research TopicReviews and Applications of Implementation Research in Aging and Public HealthView all 13 articles
Single-session interventions (SSIs) are mental health (MH) interventions that intentionally involve a single encounter. In this commentary, we outline issues with existing models of MH care for older adults & their care partners, how SSIs can address barriers, and considerations for research. We encourage the development of SSIs to increase accessibility, scalability, participation, and cost-effectiveness of mental health interventions.
The mental healthcare needs of older adults and their care partners (i.e., family members and other close affiliates providing unpaid care) are rapidly increasing with the aging population. By 2030, one in six people globally will be aged 60 years or older, and by 2050, this demographic will double to 2.1 billion (1). Older adults and their care partners report high rates of clinically elevated emotional distress, significant unmet psychosocial support needs, and dissatisfaction with many aspects of their care.
Addressing the mental health needs of older adults and care partners is infeasible with predominant intervention models. Specifically, standard psychotherapy programs are time-intensive (typically 10–12 sessions), delivered by professionals with advanced training, and available in limited contexts. Mental healthcare remains disorder-driven or focused on single conditions (vs. strengths-driven or accounting for co-occurring conditions). This is a poor fit for older adults and care partners, who frequently navigate comorbid conditions and are interested in strengths-based approaches (2, 3). Recently, evidence-based interventions have been developed for older adults and care partners that are transdiagnostic (i.e., not specific to disease or condition) in nature (4–6). However, most are not feasible to implement at a large-scale due to the time, resources, and trained workforce required.
There is an urgent need for more scalable and sustainable avenues to address the mental healthcare needs of older adults and their care partners. Single-session interventions (SSIs) may represent one possible avenue. SSIs are defined as specific brief and low intensity interventions that intentionally involve a single in-person or online visit or encounter with a program, provider, or service (7). SSIs serve to make treatment more widely available, meeting people where they seek care, and they offer an approach suitable for those who would not otherwise engage in longer-duration interventions. SSIs can be self-guided or facilitated by a professional or lay provider; they can be digital or conducted in-person. By offering support rapidly and in a low-intensity format, SSIs have demonstrated success among high-need populations that may otherwise receive no treatment, such as those on waitlists for mental health clinics (8–11).
Despite their potential benefits, there are few established SSIs specifically designed to address the needs of older adults and their care partners. This commentary highlights the potential of implementing SSIs for older adults and their care partners. Below, we outline (1) unmet needs and issues with existing models of care, (2) potential intervention mechanisms, targets, and benefits of SSIs, and (3) considerations for future research. We aim to encourage the development of SSIs within and outside of healthcare settings to potentially increase accessibility, scalability, participation, and cost-effectiveness of mental health interventions to support older adults and care partners.
Advances in healthcare and improvements in living conditions have successfully prolonged lifespans, but at the same time have led to an increased likelihood for chronic illness exposure and age-related health concerns (12). Older adults experience high rates of co-occurring chronic health conditions (e.g., chronic pain, arthritis, cardiovascular disease, diabetes, depression, and dementia), aging-related impairments of multiple organ system (e.g., frailty, falls, incontinence, delirium), and resultant disability that are “rules rather than exceptions” (1, 13). These issues are emotionally taxing and difficult to navigate for individuals and their care partners who are often described as the “invisible” patients or workforce. Over one-third older adults and their care partners endorse high rates of emotional distress (14, 15). Among older adults—and particularly those with chronic conditions—emotional distress is associated with increased healthcare usage, which places a toll on healthcare systems (16, 17).
Among older adults and care partners, several important structural barriers to mental healthcare exist, including:
Prior generations of adults ages 65 and older were less likely to report concerns to any providers other than primary care physicians, and were less likely to access mental healthcare relative to younger adults (18). However, younger generations including the “baby boomers” that reached >65 in 2020, demonstrate worse mental health than older generations and a greater likelihood to seek mental healthcare services (19). In the decades ahead, there will be a growing demand for mental healthcare. This is an important issue given the lack of appropriately trained professionals (e.g., psychologists, counselors, social workers) to provide services for older adults across cares settings (20). When longer-duration mental health programs are developed, they are often not sustainable to implement in healthcare settings due to the time demands placed on providers (21).
The lack of available workforce is even more of a barrier for care partners, who suffer from significant morbidity themselves and are not considered in routine assessment and mental health support (22). In recent years, U.S. policy changes such as the state-level Care, Advise, Record, Enable (CARE) Act (23) and the 2023 Center for Medicare and Medicaid Innovation (CMMI) Guiding an Improved Dementia Experience (GUIDE) model (24) have encouraged the inclusion of family care partners in comprehensive care packages focused on care transition, coordination, and respite services. While these and other policy initiatives have led to some system-level changes, scheduling difficulties and poor efficiency of care delivery are areas requiring improvement (23, 25).
The demand for mental healthcare dramatically exceeds the number of available providers, leading to long waits being the norm. In the U.S., wait-times for outpatient psychotherapy can last upwards of weeks, even several months (10, 26). Longer wait-times contribute to worsening mental health symptoms (27), even when compared to “no treatment” conditions, in which individuals are not expecting future care (10, 28). Long wait times lead to smaller symptom improvements and increased likelihood of early dropout once mental healthcare has begun (10, 29, 30). Waitlists and delays from referral to visit time in outpatient mental health clinics lead to worse outcomes (e.g., pain, function, physical activity, and mortality), particularly for individuals experiencing frailty, undergoing evaluation for transplants, and following cardiac events (31, 32).
Both older adults and care partners face barriers to engaging in typical duration mental healthcare due to time commitment expectations. Approximately 42% of older adults do not return to mental health interventions after the first session, which increases to 75% after 6 months of treatment (33). Older adults cite a lack of early relief in symptoms as the top reason for dropout (33), suggesting the need for more potent intervention approaches. Older adults often prefer to seek help from their primary care providers for mental health concerns, and providers cite lack of time as an important barrier to intervention (34). Among care partners, dropout from mental health interventions is high (~50%) (35, 36), and many refuse to engage in interventions altogether due to the required time commitments (37).
Many older adults experience changes in memory and cognition, and report anxiety surrounding aging. Performance on cognitive assessment is highly sensitive to individuals’ stress surrounding testing (38). Early mental healthcare is seldom available for older adults experiencing progressive neurocognitive symptoms, leaving many without support during the “window of opportunity” where they can meaningfully participate in interventions (39).
Older adults and care partners are also increasingly present in emergency and critical care settings, and note a lack of mental health support (40). Older patients experience more frequent care transitions from hospital to home and across facilities relative to younger patients given their increased experience of co-occurring conditions, cognitive impairment, and functional status (41). Care transitions are often challenging times, and rehospitalization is common (41, 42). Specific challenges include: missing information regarding diagnoses and symptoms, a lack of follow up care, new physical health concerns that complicate transition plans, care partner distress, and disagreements on how to navigate care (42). Care transitions will continue to increase as the population ages, leading to a growing interest in “rapid rehabilitation” (43). Acute and transitional care models for discharge that improve the mental health of patients and care partners exist, though most are inaccessible or not feasible to implement in large scale contexts due to time, cost, geographic, and workforce resource constraints (44).
SSIs may be more equipped to address the challenges related to growing demands for mental healthcare support for older adults and care partners in clinic and community settings relative to longer duration interventions (9). SSIs are optimized to achieve meaningful clinical progress within just one session, though visits are sometimes added as needed (i.e., in a “one-at-a-time” manner). This approach may offer specific benefits for participants that are unlikely to attend beyond the first session, which is a substantial portion of older adults and care partners (37). SSIs can meaningfully impact intervention targets through education, skills practice, and support that increases participants’ sense of agency, autonomy, competence, and relatedness (45, 46). A key benefit of SSIs are their flexibility in their format of delivery—they can be delivered as self-guided, digital interventions or implemented by trained professionals or even lay providers within existing systems and settings (e.g., healthcare clinics) (47). Having options for delivery is important given that older adults vary in their technology literacy, and may face time and geographic barriers to engaging in mental health interventions (48).
Systematic and meta reviews of the effectiveness of SSIs have shown evidence of their broad utility in improving outcomes for participants (49). However, at present there is very limited research surrounding the specific applications of SSIs for older adults and care partners. Some SSIs have been developed for adults that successfully improved a range of clinical outcomes for common challenges experienced by older adults and their care partners, including those targeting patient and care partner distress following cancer treatment, pain intensity for individuals with chronic pain, and alcohol consumption for those with frequent overconsumption (50–52).
While there is limited research on SSIs specifically developed for older adults, brief interventions (3–12 sessions) have been developed for older adults to address common challenges that can be adapted to single session formats. For example, behavioral activation is a well-documented approach to reduce depression symptoms, with some interventions demonstrating improvements in 1–2 sessions (53). In addition, compassion-based interventions demonstrate significant effects in reducing emotional distress for both older adults and care partners, though attrition is high (~18%) across studies (2, 54). Such approaches can be used to address the common challenges that older adults face surrounding shame with aging (55), and SSIs may provide an avenue to reduce attrition. Brief interventions have been developed that provide information, practical assistance, and non-judgmental support after sudden loss (56, 57) and to facilitate advanced care planning conversations among families in emergency medicine settings (58). SSIs may be used to reduce the wait times for this form of support and increase its availability. Finally, brief interventions delivered digitally to care partners of adults with chronic health conditions successfully improve care partner psychological health, self-efficacy, caregiving effectiveness, and perceived social support (59). SSIs can further facilitate care partners’ engagement by bypassing time and transportation barriers to reduce burden and improve mental health (60).
For additional SSIs to be successfully adapted, developed, tested, and implemented to address the needs of older adults and their care partners, intervention development and implementation frameworks must be considered. Specifically, the NIH Stage Model for Behavioral Intervention Development can be used to determine whether sufficient information is available on the intervention context, targets, and mechanisms to guide intervention development (NIH Stage Model Stage 0) prior to testing feasibility (61). It is important to conduct preliminary testing to identify and refine any specific modifications or adaptations that must be made to existing SSIs or longer interventions to meet the needs of older adults and care partners, and whether such approaches demonstrate early feasibility (NIH Stage Model Stages 1a-1b). Intervention targets can be selected based on what is known about the unmet needs of older adults, including emotional distress, loneliness, treatment engagement, and illness management. Mechanisms of intervention can include those hypothesized to influence attitude and behavior change in a short time frame, including self-efficacy, hope and optimism, readiness for caregiving, and growth-mindset (45, 46).
Ultimately, we propose that SSIs can provide avenues to increase mental healthcare support: (1) for people who never seek or access specialty services, (2) for treatment settings with provider shortages and long waitlists, and (3) to promote initial and ongoing engagement in care. Figure 1 depicts the ways in which SSIs could be used to enhance the availability of mental healthcare across treatment contexts. Below, we provide several specific examples of ways that SSIs can address gaps and barriers in care. Our goal is to encourage additional research that incorporates older adult and care partner perspectives to develop, adapt, and refine SSIs to address common challenges and increase scalable supports.
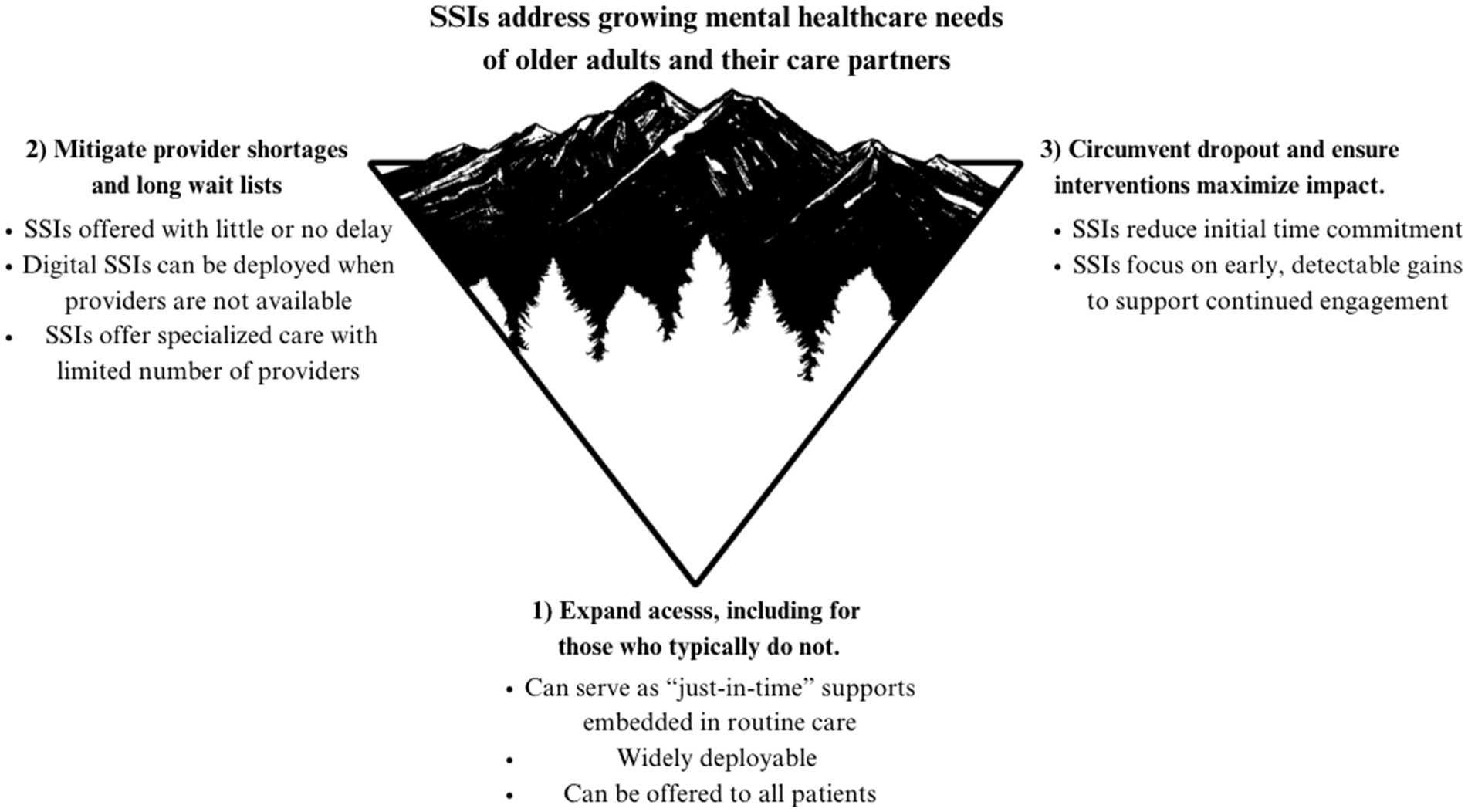
Figure 1. The potential of SSIs to address current gaps in care.
SSIs can serve as embedded, “just-in-time supports” when mental health needs arise in the context of routine healthcare settings and non-specialty clinics (e.g., with respect to emergent medical needs, cognitive decline, acute carer distress). Large scale randomized controlled trials highlight the benefits of systemwide programs for reducing depression symptoms among older adults (62). SSIs can assist in this effort, and reviews demonstrate that most users of scheduled or walk-in SSIs for common challenges in community settings (e.g., depression, anxiety, confidence) found them sufficient and helpful (63). SSIs can also be used to enhance the resiliency of communities of older adults, regardless of whether they are currently experiencing mental or physical illness (64). SSIs can be used to promote the health of entire family units and integrated into primary care clinics and community settings (e.g., public libraries, transportation, religious communities) (65). Given that older adults and care partners experience distress at high rates (66, 67), SSIs can be developed that provide coping skills for participants to effectively prevent chronic distress. While beneficial as standalone care, SSIs can also be a first intervention in a stepped care model (68), as they can be used to supplement and enhance routine assessment, bridge gaps in condition management, and delivered in either an “opt-out” or “opt-in” manner.
SSIs can help mitigate the problems of provider shortages and long waitlists by (1) offering people help immediately when then first reach out for care as a stop-gap, (2) offering brief, evidence-based, digital support even when human-delivered care is not available, and (3) creating opportunities for non-professionals to deliver evidence-based SSIs, again circumventing the issue of limited numbers of licensed professionals.
SSIs can provide waitlisted patients with an interim, low-intensity support that can help mitigate adverse effects of awaiting more sustained care (10, 11). Specifically, single session consultations delivered by clinicians or lay providers have significantly decreased hopelessness, anxiety, and distress and to improve agency among patients a mental healthcare waitlist. Single session consultations have been delivered with fidelity by both trained professionals and lay providers (10, 11).
Therefore, we propose testing SSIs for waitlisted older adults patients and their care partners, focused on managing emotional distress and promoting self-efficacy. Digital SSIs can be leveraged by healthcare systems to streamline the widespread availability of support and information. For example, SSIs can be offered to all patients and care partners in an opt-in model via links sent when appointments are made to provide education and assessment of ongoing challenges. In addition, healthcare systems can also offer a provider-delivered single session consultations to waitlisted patients and care partners to begin to connect them to supports and develop coping plans. Together, these approaches can widely expand the available support and offer a flexible array of programs to participate in based on comfort with technology and preferences for in-person visits.
SSIs can be used to help people feel more comfortable and willing to engage in testing by providing information surrounding common worries and ways of coping. For example, diagnostic disclosure visits for neurodegenerative diseases like Alzheimer’s dementia are often a stressful event for both individuals and care partners, and disclosures are linked to increased emotional distress and changes in social engagement (69). SSIs can target common challenges early after diagnosis (e.g., stigma, overwhelming emotions, reduced self-efficacy), and can offered at the time of a disclosure visit. SSIs could also be used to supplement referrals to additional supports and serve as a rapidly available intervention after screening or testing positive for a condition.
Clinics providing feedback for neuropsychological, genetic, or other clinical biomarker assessments can consider offering a digital or in-person SSI focused on coping with emotional reactions to test results and offering education on adaptive coping behaviors to adjust to changes in dependency. SSIs can also be used to link patients and care partners to additional longer-duration supports and mental health resources. Specifically, dementia care consultation models have successfully linked family caregivers to community supports after diagnosis in primary care settings (70). Such approaches could be expanded to other conditions and/or delivered at specific disclosure visits in a diagnostic process.
SSIs have demonstrated benefits for reducing depression and anxiety symptoms in older adults and care partners navigating a number of common chronic or progressive conditions (e.g., chronic obstructive pulmonary disease; dementia; mood symptoms; cognitive decline) (71, 72). Specifically, one 2 h group interventions providing cognitive behavioral therapy significantly reduced emotional distress for COPD patients relative to education only (71). Among youth patients, SSIs have demonstrated large effects on mood and behavioral concerns (73). Following acute medical events (e.g., stroke, cardiac events, falls), older adults and care partners experience myriad stressors surrounding recovery, long-term care, and end of life considerations (3). Brief individual and dyadic interventions have been developed that address emotional distress early after acute and progressive medical events (4, 74, 75), and can be adapted to focus on the most potent intervention components for digital or person-led SSIs, which can then be carefully tested and deployed in this newer population.
SSIs could be delivered during periods after acute medical events or early after diagnosis of mental or physical health conditions to reduce emotional distress, prevent risk of complications or adverse events, and to promote resiliency. SSIs exist for stroke education and slip training following falls that have improved care partner preparedness, reduce risk, and prevent and subsequent injuries (76, 77).
SSIs could assist with this growing challenge by providing a context to assess and identify support needs and promote treatment engagement for all partners in care. SSIs can be developed to prioritize specific points of care transitions (e.g., prior to returning home from hospitalization; following a transition to a skilled nursing facility), to offer a context for assessing and supporting patient and care partners’ needs. Such approaches could include a digital SSI for care partners featuring education on common challenges in care transitions, and training in coping skills to manage distress and promote positive adjustment. Following a transition, SSIs could be offered to assess any issues arising during the care transition and to support coordinated care across care teams.
SSIs reduce the time and effort to engage in care and could lower rates of dropout by increasing odds of early, detectable treatment gains. SSIs may expand the reach of mental health interventions to those who decline to participate in interventions. By focusing on the most potent content and skills, SSIs may also be able to enhance engagement in care for longer-duration interventions and management of physical conditions. SSIs could also be used to rapidly engage individuals in mental health care in community settings. Given that many older adults do not seek mental health support or are primarily interested in support from primary care providers (34), digital or hybrid SSIs could be developed for older adults and care partners that target common challenges with less of a commitment requirement than traditional interventions. For example, SSIs have been developed emphasizing ongoing screening and motivational enhancement that successfully reduce substance use among community dwelling older adults and individuals in primary care settings (52, 78, 79).
When designing new services, important questions surrounding implementation must be thoroughly considered. Implementation science frameworks such as the Consolidated Framework for Implementation Research (CFIR) (80) and the Reach Effectiveness, Adoption, Implementation, Maintenance (RE-AIM) model (81) can be consulted throughout the intervention development process to identify and evaluate factors that influence the successful implementation of interventions (82). Both the CFIR and RE-AIM frameworks consider the broader context of delivery of SSIs, and can be used to understand to best develop an intervention that fits the intended environment and target population (e.g., acute or emergency care, outpatient therapy clinics, community settings). Another key tool is the health equity implementation framework (83). This framework is designed to promote implementation equitably amongst minoritized populations. The health equity approach can be used to develop SSIs that are specifically designed to meet the needs of individuals that most consistently experience barriers in access to care, and to account for differences in needs across intended users. The goal of each of these frameworks is to better understand how factors such as intervention setting, personnel, culture, and operation might serve as barriers and facilitators to successful implementation. Figure 2 provides a description of key questions drawn from the NIH Stage Model, CFIR, and RE-AIM model that are important to consider in developing SSIs for older adults.
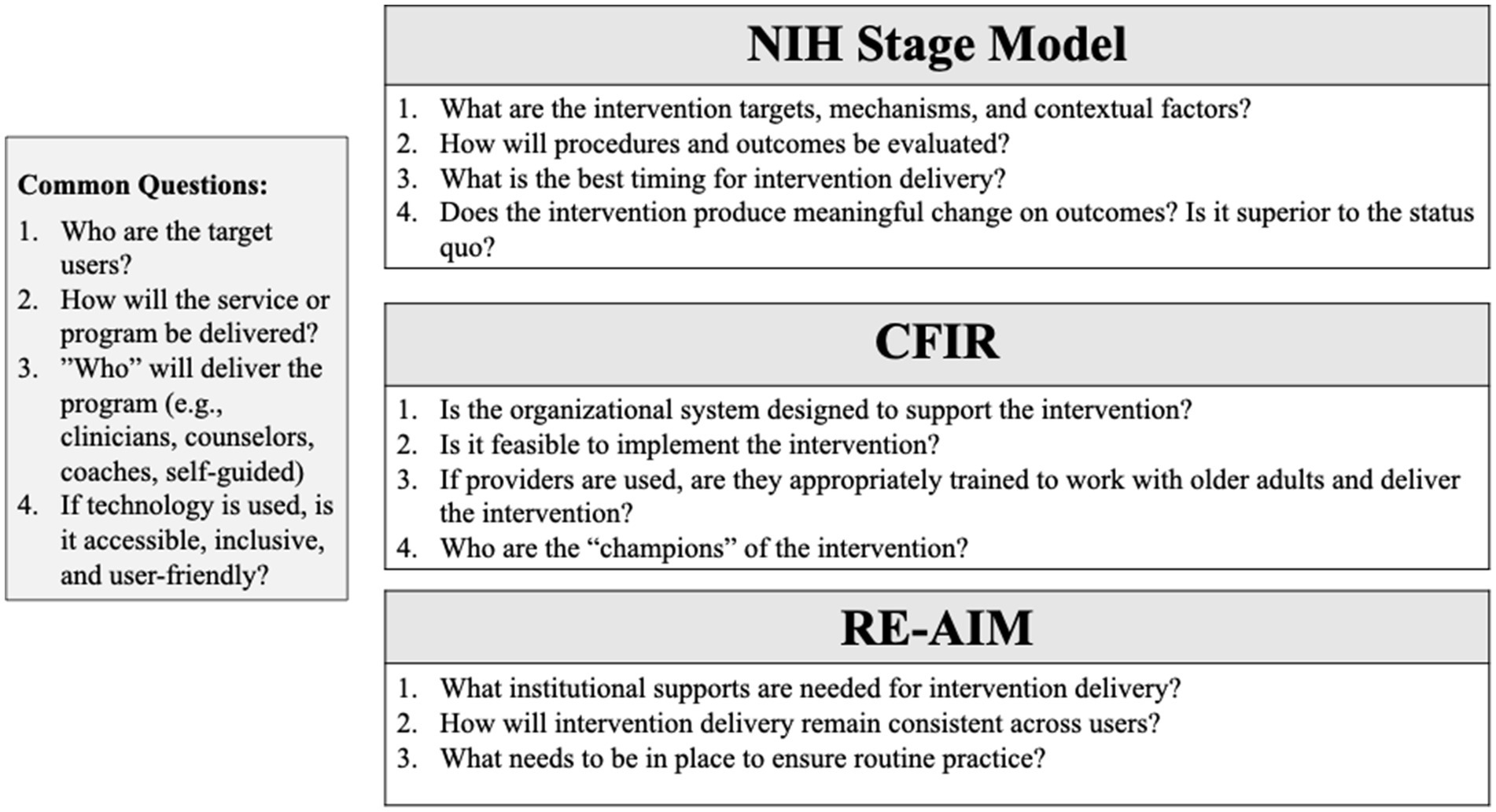
Figure 2. Key questions to inform the design of SSIs for older adults and care partners.
If SSIs incorporate mobile technology through smart devices, websites, and/or mobile applications, they should be developed with attention to the specific barriers and facilitators of technology use for older adults identified in the literature (84, 85). Mobile health interventions have demonstrated benefits on mental and physical health outcomes for older adults with chronic illnesses, though frustration with technology remain barriers to the uptake and efficacy of existing interventions (86, 87). Digital SSIs have been integrated into emails for all patients, with significant effects on aspects of resiliency such as empowerment (88). With both technology-based and in-person SSIs, interventions should be developed by meaningfully including the perspectives of the intended users.
Given the rapidly increasing aging population that is likely to require additional supports in the coming years, healthcare systems can begin by prioritizing the implementation of SSIs in high-need contexts (e.g., care settings with waiting lists). SSIs offer transdiagnostic solutions to support the resilience of older adults and their care partners given their brief, targeted nature and potential to yield significant benefits in less time. These approaches have the potential to disseminate new approaches to care delivery, re-allocate resources, promote patient-centered care, and support positive outcomes (89). SSIs can be implemented as stand-alone services or as adjunctive care to improve treatment engagement and can be tailored to multiple points in care journeys. SSIs can also be used to facilitate adjustment to care transitions. For healthcare systems and communities, intervention development and implementation frameworks should be consulted to evaluate what structure and supports are needed to encourage the development of SSIs in high-need settings, with specific attention to the considerations of older adults (89).
SB: Conceptualization, Investigation, Resources, Supervision, Writing – original draft, Writing – review & editing. AR: Methodology, Writing – original draft, Writing – review & editing. AA: Conceptualization, Supervision, Writing – review & editing. JS: Supervision, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was supported by a grant from the National Institute on Aging (1K23AG075188-03) to Sarah M. Bannon.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Gen AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. World Health Organization. World report on ageing and health. Winston-Salem, North Carolina, United States: World Health Organization (2015).
2. Murfield, J, Moyle, W, and O’Donovan, A. Mindfulness- and compassion-based interventions for family carers of older adults: a scoping review. Int J Nurs Stud. (2021) 116:103495. doi: 10.1016/j.ijnurstu.2019.103495
3. Plys, E, Bannon, S, Keeney, T, and Vranceanu, A-M. Spilling over at the boiling point: a commentary on the need for dyadic approaches to psychosocial care with older adults and their care-partners in postacute rehabilitation. Rehabil Psychol. (2023) 68:271–80. doi: 10.1037/rep0000504
4. Bannon, SM, Grunberg, VA, Manglani, HR, Lester, EG, Ritchie, C, and Vranceanu, A-M. Together from the start: a transdiagnostic framework for early dyadic interventions for neurodegenerative diseases. J Am Geriatr Soc. (2022) 70:1850–62. doi: 10.1111/jgs.17801
5. Crowe, M, Jordan, J, Burrell, B, Jones, V, Gillon, D, Harris, S, et al. Clinical effectiveness of transdiagnostic health management interventions for older people with multimorbidity: a quantitative systematic review. J Adv Nurs. (2016) 72:2315–29. doi: 10.1111/jan.13011
6. Schaeuffele, C, Schulz, A, Knaevelsrud, C, Renneberg, B, and Boettcher, J. CBT at the crossroads: the rise of Transdiagnostic treatments. Int J Cogn Ther. (2021) 14:86–113. doi: 10.1007/s41811-020-00095-2
7. Schleider, JL, Dobias, M, Sung, J, Mumper, E, and Mullarkey, MC. Acceptability and utility of an open-access, online single-session intervention platform for adolescent mental health. JMIR Mental Health. (2020) 7:e20513. doi: 10.2196/20513
8. Ching, BC, Bennett, SD, Morant, N, Heyman, I, Schleider, JL, Fifield, K, et al. Growth mindset in young people awaiting treatment in a paediatric mental health service: a mixed methods pilot of a digital single-session intervention. Clin Child Psychol Psychiatry. (2023) 28:637–53. doi: 10.1177/13591045221105193
9. Cohen, K, Dobias, M, Morris, R, and Schleider, J. Improving uptake of mental health crisis resources: randomized test of a single-session intervention embedded in social media. J Behav Cogn Ther. (2023) 33:24–34. doi: 10.1016/j.jbct.2022.12.001
10. Schleider, JL, Sung, J, Bianco, A, Gonzalez, A, Vivian, D, and Mullarkey, MC. Open pilot trial of a single-session consultation service for clients on psychotherapy wait-lists. Behav Ther. (2021) 44:8–15.
11. Sung, JY, Bugatti, M, Vivian, D, and Schleider, JL. Evaluating a telehealth single-session consultation service for clients on psychotherapy wait-lists. Pract Innov. (2023) 8:141–61. doi: 10.1037/pri0000207
12. Bergman, H, Karunananthan, S, Robledo, LM, Brodsky, J, Chan, P, Cheung, M, et al. Understanding and meeting the needs of the older population: a global challenge. Canadian Geriatr J. (2013) 16:61–5. doi: 10.5770/cgj.16.60
13. Weidman, AJ. Establishing a sustainable healthcare delivery workforce in the wake of COVID-19. J Healthc Manag. (2022) 67:234–43. doi: 10.1097/JHM-D-22-00100
14. Curran, E, Rosato, M, Ferry, F, and Leavey, G. Prevalence and factors associated with anxiety and depression in older adults: gender differences in psychosocial indicators. J Affect Disord. (2020) 267:114–22. doi: 10.1016/j.jad.2020.02.018
15. Moitra, M, Owens, S, Hailemariam, M, Wilson, KS, Mensa-Kwao, A, Gonese, G, et al. Global mental health: where we are and where we are going. Curr Psychiatry Rep. (2023) 25:301–11. doi: 10.1007/s11920-023-01426-8
16. Himelhoch, S, Weller, WE, Wu, AW, Anderson, GF, and Cooper, LA. Chronic medical illness, depression, and use of acute medical services among Medicare beneficiaries. Med Care. (2004) 42:512–21. doi: 10.1097/01.mlr.0000127998.89246.ef
17. Sporinova, B, Manns, B, Tonelli, M, Hemmelgarn, B, MacMaster, F, Mitchell, N, et al. Association of Mental Health Disorders with Health Care Utilization and Costs among Adults with Chronic Disease. JAMA Netw Open. (2019) 2:e199910. doi: 10.1001/jamanetworkopen.2019.9910
18. Crabb, R, and Hunsley, J. Utilization of mental health care services among older adults with depression. J Clin Psychol. (2006) 62:299–312. doi: 10.1002/jclp.20231
19. Zheng, H, and Echave, P. Are recent cohorts getting worse? Trends in US adult physiological status, mental health, and health behaviors across a century of birth cohorts. Am J Epidemiol. (2021) 190:2242–55. doi: 10.1093/aje/kwab076
20. Carpenter, BD, Gatz, M, and Smyer, MA. Mental health and aging in the 2020s. Am Psychol. (2022) 77:538–50. doi: 10.1037/amp0000873
21. Cremers, G, Taylor, E, Hodge, L, and Quigley, A. Effectiveness and acceptability of low-intensity psychological interventions on the well-being of older adults: a systematic review. Clin Gerontol. (2022) 45:214–34. doi: 10.1080/07317115.2019.1662867
22. Reynolds, CF III, Jeste, DV, Sachdev, PS, and Blazer, DG. Mental health care for older adults: recent advances and new directions in clinical practice and research. World Psychiatry. (2022) 21:336–63. doi: 10.1002/wps.20996
23. Rodakowski, J, Leighton, C, Martsolf, GR, and James, AE. Caring for family caregivers: perceptions of CARE act compliance and implementation. Qual Manag Healthc. (2021) 30:1–5. doi: 10.1097/QMH.0000000000000278
24. Ramesh, T, Kadakia, K, and Moura, L. Transforming value-based dementia care—implications for the GUIDE model. JAMA Intern Med. (2024) 184:237–9. doi: 10.1001/jamainternmed.2023.7669
25. Leighton, C, Fields, B, Rodakowski, JL, Feiler, C, Hawk, M, Bellon, JE, et al. A multisite case study of caregiver advise, record, enable act implementation. The Gerontologist. (2020) 60:776–86. doi: 10.1093/geront/gnz011
26. Peipert, A, Krendl, AC, and Lorenzo-Luaces, L. Waiting lists for psychotherapy and provider attitudes toward low-intensity treatments as potential interventions: survey study. JMIR Format Res. (2022) 6:e39787. doi: 10.2196/39787
27. Steinert, C, Stadter, K, Stark, R, and Leichsenring, F. The effects of waiting for treatment: a meta-analysis of waitlist control groups in randomized controlled trials for social anxiety disorder. Clin Psychol Psychother. (2017) 24:649–60. doi: 10.1002/cpp.2032
28. Furukawa, TA, Noma, H, Caldwell, DM, Honyashiki, M, Shinohara, K, Imai, H, et al. Waiting list may be a nocebo condition in psychotherapy trials: a contribution from network meta-analysis. Acta Psychiatr Scand. (2014) 130:181–92. doi: 10.1111/acps.12275
29. Reitzel, LR, Stellrecht, NE, Gordon, KH, Lima, EN, Wingate, LR, Brown, JS, et al. Does time between application and case assignment predict therapy attendance or premature termination in outpatients? Psychol Serv. (2006) 3:51–60. doi: 10.1037/1541-1559.3.1.51
30. Swift, JK, and Greenberg, RP. Premature discontinuation in adult psychotherapy: a meta-analysis. J Consult Clin Psychol. (2012) 80:547–59. doi: 10.1037/a0028226
31. Lai, JC, Dodge, JL, Kappus, MR, Dunn, MA, Volk, ML, Duarte-Rojo, A, et al. Changes in frailty are associated with waitlist mortality in patients with cirrhosis. J Hepatol. (2020) 73:575–81. doi: 10.1016/j.jhep.2020.03.029
32. Lewis, AK, Harding, KE, Snowdon, DA, and Taylor, NF. Reducing wait time from referral to first visit for community outpatient services may contribute to better health outcomes: a systematic review. BMC Health Serv Res. (2018) 18:869. doi: 10.1186/s12913-018-3669-6
33. Grover, S, Mehra, A, Chakrabarti, S, and Avasthi, A. Dropout rates and reasons for dropout from treatment among elderly patients with depression. J Geriatr Mental Health. (2018) 5:121. doi: 10.4103/jgmh.jgmh_29_17
34. Lavingia, R, Jones, K, and Asghar-Ali, AA. A systematic review of barriers faced by older adults in seeking and accessing mental health care. J Psychiatr Pract. (2020) 26:367–82. doi: 10.1097/PRA.0000000000000491
35. Gitlin, LN, Jutkowitz, E, and Gaugler, JE. Dementia caregiver intervention research now and into the future: Review and recommendations. Washington, DC: Commissioned Paper for the National Academies of Science, Engineering and Medicine NIA Decadal Study (2020).
36. Parker, M, Barlow, S, Hoe, J, and Aitken, L. Persistent barriers and facilitators to seeking help for a dementia diagnosis: a systematic review of 30 years of the perspectives of carers and people with dementia. Int Psychogeriatr. (2020) 32:611–34. doi: 10.1017/S1041610219002229
37. Qiu, D, Hu, M, Yu, Y, Tang, B, and Xiao, S. Acceptability of psychosocial interventions for dementia caregivers: a systematic review. BMC Psychiatry. (2019) 19:23. doi: 10.1186/s12888-018-1976-4
38. Sindi, S, Fiocco, AJ, Juster, R-P, Pruessner, J, and Lupien, SJ. When we test, do we stress? Impact of the testing environment on cortisol secretion and memory performance in older adults. Psychoneuroendocrinology. (2013) 38:1388–96. doi: 10.1016/j.psyneuen.2012.12.004
39. Isaacson, RS, and Saif, N. A missed opportunity for dementia prevention? Current challenges for early detection and modern-day solutions. J Prev Alzheimers Dis. (2020) 7:291–3. doi: 10.14283/jpad.2020.23
40. Akinosoglou, K, Schinas, G, Almyroudi, MP, Gogos, C, and Dimopoulos, G. The impact of age on intensive care. Ageing Res Rev. (2023) 84:101832. doi: 10.1016/j.arr.2022.101832
41. Vognar, L, and Mujahid, N. Healthcare transitions of older adults: an overview for the general practitioner. R I Med J. (2015) 98:15.
42. Gettel, CJ, Serina, PT, Uzamere, I, Hernandez-Bigos, K, Venkatesh, AK, Rising, KL, et al. Emergency department-to-community care transition barriers: a qualitative study of older adults. J Am Geriatr Soc. (2022) 70:3152–62. doi: 10.1111/jgs.17950
43. Ross, DM, Ramirez, B, Rotarius, T, and Liberman, A. Health care transitions and the aging population: a framework for measuring the value of rapid rehabilitation. Health Care Manag. (2011) 30:96–117. doi: 10.1097/HCM.0b013e318216ed89
44. McNabney, MK, Green, AR, Burke, M, Le, ST, Butler, D, Chun, AK, et al. Complexities of care: common components of models of care in geriatrics. J Am Geriatr Soc. (2022) 70:1960–72. doi: 10.1111/jgs.17811
45. Deci, EL, and Ryan, RM. Self-determination theory. Handb. Theor Soc Psychol. (2012) 1:416–36. doi: 10.4135/9781446249215.n21
46. Ghaderi, A, and Welch, E. A broad range: from simple and brief to intensive single-session interventions: commentary on Schleider et al. (2023). Int J Eat Disord. (2023) 56:875–7. doi: 10.1002/eat.23949
47. Schleider, JL, and Beidas, RS. Harnessing the single-session intervention approach to promote scalable implementation of evidence-based practices in healthcare. Front Health Serv. (2022) 2:997406. doi: 10.3389/frhs.2022.997406
48. Leung, DKY, Wong, NHL, Yau, JHY, Wong, FHC, Liu, T, Kwok, W, et al. Hybrid-delivered community psychoeducation for people aged 50 and older: a mixed-method evaluation and lesson learned. Internet Interv. (2024) 35:100699. doi: 10.1016/j.invent.2023.100699
49. Schleider, JL, Zapata, JP, Rapoport, A, Wescott, A, Ghosh, A, Kaveladze, B, et al. Single-session interventions for mental health problems and service engagement: umbrella review of systematic reviews and meta-analyses. Ann Rev Clin Psychol. (2025) 21. doi: 10.1146/annurev-clinpsy-081423-025033
50. Chambers, SK, Girgis, A, Occhipinti, S, Hutchison, S, Turner, J, McDowell, M, et al. A randomized trial comparing two low-intensity psychological interventions for distressed patients with cancer and their caregivers. Oncol Nurs Forum. (2014) 41:E256–66. doi: 10.1188/14.ONF.E256-E266
51. Dubé, M-O, Dillon, S, Gallagher, K, Ryan, J, and McCreesh, K. One and done? The effectiveness of a single session of physiotherapy compared to multiple sessions to reduce pain and improve function and quality of life in patients with a musculoskeletal disorder: a systematic review with meta-analyses. Arch Phys Med Rehabil. (2023) 105:1171–80. doi: 10.1016/j.apmr.2023.09.017
52. Kaner, EF, Dickinson, HO, Beyer, F, Pienaar, E, Schlesinger, C, Campbell, F, et al. The effectiveness of brief alcohol interventions in primary care settings: a systematic review. Drug Alcohol Rev. (2009) 28:301–23. doi: 10.1111/j.1465-3362.2009.00071.x
53. Cole, MG. Brief interventions to prevent depression in older subjects: a systematic review of feasibility and effectiveness. Am J Geriatr Psychiatry. (2008) 16:435–43. doi: 10.1097/JGP.0b013e318162f174
54. Russell, BS, Lincoln, CR, and Starkweather, AR. Distress tolerance intervention for improving self-management of chronic conditions: a systematic review. J Holist Nurs. (2019) 37:74–86. doi: 10.1177/0898010118777327
55. Rush, KL, Watts, WE, and Stanbury, J. Older adults’ perceptions of weakness and ageing. Int J Older People Nursing. (2013) 8:1–9. doi: 10.1111/j.1748-3743.2011.00280.x
56. McGill, K, Bhullar, N, Batterham, PJ, Carrandi, A, Wayland, S, and Maple, M. Key issues, challenges, and preferred supports for those bereaved by suicide: insights from postvention experts. Death Stud. (2023) 47:624–9. doi: 10.1080/07481187.2022.2112318
57. Nam, I. Effect of a brief family-based treatment on complicated grief in bereaved older adults. Ann Geriatr Med Res. (2018) 22:94–7. doi: 10.4235/agmr.2018.22.2.94
58. Pajka, SE, Hasdianda, MA, George, N, Sudore, R, Schonberg, MA, Bernstein, E, et al. Feasibility of a brief intervention to facilitate advance care planning conversations for patients with life-limiting illness in the emergency department. J Palliat Med. (2021) 24:31–9. doi: 10.1089/jpm.2020.0067
59. Zhai, S, Chu, F, Tan, M, Chi, N-C, Ward, T, and Yuwen, W. Digital health interventions to support family caregivers: an updated systematic review. Digit Health. (2023) 9:20552076231171967. doi: 10.1177/20552076231171967
60. Guay, C, Auger, C, Demers, L, Mortenson, WB, Miller, WC, Gélinas-Bronsard, D, et al. Components and outcomes of internet-based interventions for caregivers of older adults: systematic review. J Med Internet Res. (2017) 19:e313. doi: 10.2196/jmir.7896
61. Onken, L. Implementation science at the National Institute on Aging: the principles of it. Public Policy Aging Rep. (2022) 32:39–41. doi: 10.1093/ppar/prab034
62. Reynolds, CF, Cuijpers, P, Patel, V, Cohen, A, Dias, A, Chowdhary, N, et al. Early intervention to reduce the global health and economic burden of major depression in older adults. Annu Rev Public Health. (2012) 33:123–35. doi: 10.1146/annurev-publhealth-031811-124544
63. Hymmen, P, Stalker, CA, and Cait, C-A. The case for single-session therapy: does the empirical evidence support the increased prevalence of this service delivery model? J Ment Health. (2013) 22:60–71. doi: 10.3109/09638237.2012.670880
64. Panagou, C, and MacBeth, A. Deconstructing pathways to resilience: a systematic review of associations between psychosocial mechanisms and transdiagnostic adult mental health outcomes in the context of adverse childhood experiences. Clin Psychol Psychother. (2022) 29:1626–54. doi: 10.1002/cpp.2732
65. Buysse, DJ, Germain, A, Moul, DE, Franzen, PL, Brar, LK, Fletcher, ME, et al. Efficacy of brief behavioral treatment for chronic insomnia in older adults. Arch Intern Med. (2011) 171:887–95. doi: 10.1001/archinternmed.2010.535
66. Roth, DL, Perkins, M, Wadley, VG, Temple, EM, and Haley, WE. Family caregiving and emotional strain: associations with quality of life in a large national sample of middle-aged and older adults. Qual Life Res. (2009) 18:679–88. doi: 10.1007/s11136-009-9482-2
67. Taylor, HO, Taylor, RJ, Nguyen, AW, and Chatters, L. Social isolation, depression, and psychological distress among older adults. J Aging Health. (2018) 30:229–46. doi: 10.1177/0898264316673511
68. Bower, P, and Gilbody, S. Stepped care in psychological therapies: access, effectiveness and efficiency: narrative literature review. Br J Psychiatry. (2005) 186:11–7. doi: 10.1192/bjp.186.1.11
69. Amano, T, Reynolds, A, Scher, C, and Jia, Y. The effect of receiving a diagnosis of Alzheimer’s disease and related dementias on social relationships of older adults. Dement Geriatr Cogn Disord. (2021) 50:401–6. doi: 10.1159/000519581
70. Fortinsky, RH, Kulldorff, M, Kleppinger, A, and Kenyon-Pesce, L. Dementia care consultation for family caregivers: collaborative model linking an Alzheimer’s association chapter with primary care physicians. Aging Ment Health. (2009) 13:162–70. doi: 10.1080/13607860902746160
71. Kunik, ME, Braun, U, Stanley, MA, Wristers, K, Molinari, V, Stoebner, D, et al. One session cognitive behavioural therapy for elderly patients with chronic obstructive pulmonary disease. Psychol Med. (2001) 31:717–23. doi: 10.1017/S0033291701003890
72. Manalai, G, Manalai, P, Dutta, R, Fegan, G, and Scrofani, P. Rapid improvement of depressive symptoms and cognition in an elderly patient with a single session of piano playing: a clinical treatment report. Aging Clin Exp Res. (2012) 24:278–80. doi: 10.1007/BF03325258
73. Schleider, JL, and Weisz, JR. Little treatments, promising effects? Meta-analysis of single-session interventions for youth psychiatric problems. J Am Acad Child Adolesc Psychiatry. (2017) 56:107–15. doi: 10.1016/j.jaac.2016.11.007
74. Hoffmann, T, Ownsworth, T, Eames, S, and Shum, D. Evaluation of brief interventions for managing depression and anxiety symptoms during early discharge period after stroke: a pilot randomized controlled trial. Top Stroke Rehabil. (2015) 22:116–26. doi: 10.1179/1074935714Z.0000000030
75. Vranceanu, A-M, Bannon, S, Mace, R, Lester, E, Meyers, E, Gates, M, et al. Feasibility and efficacy of a resiliency intervention for the prevention of chronic emotional distress among survivor-caregiver dyads admitted to the neuroscience intensive care unit: a randomized clinical trial. JAMA Netw Open. (2020) 3:e2020807. doi: 10.1001/jamanetworkopen.2020.20807
76. Robles, MC, Springer, MV, Corches, CL, Burke, JF, Lin, CC, Oliver, A, et al. Stroke ready very brief intervention improves immediate postintervention stroke preparedness. Circ Cardiovasc Qual Outcomes. (2020) 13:e006643. doi: 10.1161/CIRCOUTCOMES.120.006643
77. Wang, Y, Wang, S, Liu, X, Lee, A, Pai, Y-C, and Bhatt, T. Can a single session of treadmill-based slip training reduce daily life falls in community-dwelling older adults? A randomized controlled trial. Aging Clin Exp Res. (2022) 34:1593–602. doi: 10.1007/s40520-022-02090-3
78. Han, BH, Masukawa, K, Rosenbloom, D, Kuerbis, A, Helmuth, E, Liao, DH, et al. Use of web-based screening and brief intervention for unhealthy alcohol use by older adults. J Subst Abus Treat. (2018) 86:70–7. doi: 10.1016/j.jsat.2018.01.002
79. Scott, DM, Petras, H, Kalu, N, Cain, GE, Johnson, DB, Sloboda, Z, et al. Implementation of screening, brief intervention, and referral for treatment in the aging network of care to prevent alcohol, recreational drug, and prescription medication misuse. Prev Sci. (2020) 21:972–8. doi: 10.1007/s11121-020-01154-y
80. Damschroder, LJ, Reardon, CM, and Lowery, JC. The consolidated framework for implementation research (CFIR) In: Handbook on implementation science. Winston-Salem, North Carolina, United States: Edward Elgar Publishing (2020). 88–113.
81. Glasgow, RE, Vogt, TM, and Boles, SM. Evaluating the public health impact of health promotion interventions: the RE-AIM framework. Am J Public Health. (1999) 89:1322–7. doi: 10.2105/AJPH.89.9.1322
82. Birken, SA, Powell, BJ, Presseau, J, Kirk, MA, Lorencatto, F, Gould, NJ, et al. Combined use of the consolidated framework for implementation research (CFIR) and the theoretical domains framework (TDF): a systematic review. Implement Sci. (2017) 12:2. doi: 10.1186/s13012-016-0534-z
83. Woodward, EN, Matthieu, MM, Uchendu, US, Rogal, S, and Kirchner, JE. The health equity implementation framework: proposal and preliminary study of hepatitis C virus treatment. Implement Sci. (2019) 14:26. doi: 10.1186/s13012-019-0861-y
84. Nimmanterdwong, Z, Boonviriya, S, and Tangkijvanich, P. Human-centered Design of Mobile Health Apps for older adults: systematic review and narrative synthesis. JMIR Mhealth Uhealth. (2022) 10:e29512. doi: 10.2196/29512
85. Wilson, J, Heinsch, M, Betts, D, Booth, D, and Kay-Lambkin, F. Barriers and facilitators to the use of e-health by older adults: a scoping review. BMC Public Health. (2021) 21:1–12. doi: 10.1186/s12889-021-11623-w
86. Lee, JJN, Abdul Aziz, A, Chan, S-T, Raja Abdul Sahrizan, RSF, Teh, Y-T, Iqbal, U, et al. Effects of mobile health interventions on health-related outcomes in older adults with type 2 diabetes: a systematic review and meta-analysis. J Diabetes. (2023) 15:47–57. doi: 10.1111/1753-0407.13346
87. Rostam Niakan Kalhori, S, Rahmani Katigari, M, Talebi Azadboni, T, Pahlevanynejad, S, and Hosseini Eshpala, R. The effect of m-health applications on self-care improvement in older adults: a systematic review. Inform Health Soc Care. (2023) 48:292–331. doi: 10.1080/17538157.2023.2171878
88. Nieuwboer, CC, Fukkink, RG, and Hermanns, JM. Single session email consultation for parents: an evaluation of its effect on empowerment. British J Guid Counsell. (2015) 43:131–43. doi: 10.1080/03069885.2014.929636
Keywords: single session, brief intervention, older adults, care partners, caregivers, mental health
Citation: Bannon SM, Rapoport A, Applebaum AJ and Schleider JL (2025) The potential of single session intervention approaches to enhance the mental health and resilience of older adults, care partners, and healthcare systems. Front. Public Health. 13:1515440. doi: 10.3389/fpubh.2025.1515440
Edited by:
Marcia G. Ory, Texas A&M University, United StatesReviewed by:
Tetiana Nickelsen, Texas A and M University, United StatesCopyright © 2025 Bannon, Rapoport, Applebaum and Schleider. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sarah M. Bannon, c2FyYWguYmFubm9uQG1vdW50c2luYWkub3Jn
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.