
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
POLICY BRIEF article
Front. Public Health, 21 March 2025
Sec. Public Health Education and Promotion
Volume 13 - 2025 | https://doi.org/10.3389/fpubh.2025.1514090
This article is part of the Research TopicEnsuring Public Health: The Active Role of Healthcare ProfessionalsView all 9 articles
 Fazal Jamil1*
Fazal Jamil1* Umaima Mir2
Umaima Mir2 Anum G. Niazi3Shandana Kifayat4Shanlina Kifayat5Sobia Shafiq6Zeeshan Wali7
Anum G. Niazi3Shandana Kifayat4Shanlina Kifayat5Sobia Shafiq6Zeeshan Wali7 Muhammad Ali Jan Khan8Baber Wali9Khadija Tul Kobra10
Muhammad Ali Jan Khan8Baber Wali9Khadija Tul Kobra10 Muhammad Salar Khan11
Muhammad Salar Khan11Pakistan has the third-highest rate of type 2 diabetes globally, following China and India, making this a significant public health crisis. Despite the severity of the issue, efforts from health and policy practitioners to address it remain limited. With millions already diagnosed as pre-diabetic, the rising incidence of diabetes is rapidly becoming a public health emergency that demands immediate attention. This policy brief provides an accessible overview of diabetes, focusing on its types, mechanisms, and preventive measures. It also identifies key contributing factors, such as dietary habits, obesity, physical inactivity, and the influence of modern dietary trends, while proposing strategies for individuals, communities, and policymakers to combat this growing epidemic in Pakistan. The brief emphasizes the need for a multi-level approach that includes public awareness, education, behavioral and dietary changes, and policy interventions to reverse the trend. Strategies discussed include promoting healthy eating, increasing physical activity, managing obesity, and enhancing access to affordable, healthy food. Additionally, the brief highlights the importance of community and government support, such as public health campaigns, infrastructure improvements, and legislative efforts. By adopting this comprehensive approach, Pakistan can take meaningful steps to address the diabetes epidemic and improve public health outcomes.
According to the International Diabetes Federation Diabetes Atlas, Pakistan has the third-highest rate of type 2 diabetes among adults globally, after China and India, making it a growing crisis in the country (1). Furthermore, with an estimated prevalence of 33.6% among individuals aged 20–79, Pakistan now holds the highest global ranking for type 2 diabetes (2). Despite these alarming figures, health and policy practitioners have made limited efforts to address the issue, leaving the country vulnerable to an escalating public health crisis. The situation is even more concerning, with millions already diagnosed as pre-diabetic (3). The rising incidence of diabetes is rapidly becoming a public health emergency that requires immediate attention.
To combat this epidemic, a comprehensive, multi-level approach is necessary, which would cover individual to communal and government level efforts. Our team contends that such an approach would be most effective if it included public awareness, education, outreach, behavioral and dietary changes, along with policy interventions.
This policy brief provides an accessible overview of diabetes, including its types, causes, and preventive measures. It also explores the increasing prevalence of diabetes in Pakistan, identifies contributing factors, and outlines strategies for individuals, communities, and public health authorities to effectively prevent and manage the disease within the country. As this policy brief is aimed at raising public awareness and stimulating policy and community conversations around this critical public health issue in Pakistan, we draw on relevant literature while also relying on our expertise and background to offer suggestions, which aligns with the journal’s scope for this collection.1 To sustain public interest and to convey our message in plain language, we have deliberately minimized the use of dense academic citations and heavy medical jargon.
Diabetes is a chronic medical condition marked by elevated blood sugar levels (hyperglycemia) due to impaired insulin action, insufficient insulin production, or both. Insulin, a hormone produced by the beta cells in the pancreas, facilitates the uptake of glucose from the bloodstream into muscle and other body cells for energy (4).
Among the two primary types of diabetes (type 1 and type 2), type 1 diabetes is an autoimmune disorder in which the body’s immune system destroys insulin-producing beta cells in the pancreas, leading to little or no insulin production (5). In contrast, type 2 diabetes is primarily characterized by insulin resistance and progressive pancreatic beta-cell dysfunction, resulting in relative insulin deficiency and subsequent hyperglycemia (6, 7).2
Hyperglycemia in diabetic patients contributes to cardiovascular complications, kidney dysfunction, and oxidative stress, as well as metabolic dysregulation, which, in turn leads to increased appetite. Several factors contribute to the development of insulin resistance in type 2 diabetes, with obesity, genetics, and environmental and lifestyle factors playing significant roles.
Obesity, particularly visceral fat, is a major contributor to insulin resistance (8). In obese individuals, adipose (fat) tissue releases various biochemical substances (cytokines and hormones) that trigger inflammation and interfere with insulin signaling pathways, leading to insulin resistance. Simply put, excess fat can disrupt normal metabolism by causing inflammation and making it harder for the body to use insulin properly.
Genetics is another determinant for insulin resistance.3 Studies have identified several genetic variants that predispose individuals to impaired insulin signaling, beta-cell dysfunction, and altered glucose metabolism (8). These genetic factors may explain why some individuals develop insulin resistance despite having a normal body weight, while others remain metabolically healthy despite obesity. Inherited predispositions also influence how efficiently the body processes insulin and regulates blood sugar levels, affecting the risk of developing type 2 diabetes.
Beyond genetics and obesity, insulin resistance also develops gradually due to various environmental and lifestyle factors, with dietary habits playing a significant role (9). Overconsumption of refined sugars, processed grains, and high-glycemic carbohydrates results in frequent spikes in blood sugar levels. In response, the body produces excess insulin to manage these sugar spikes. Persistent overproduction of insulin causes the body to become less responsive, or more resistant, to it. Furthermore, this ongoing cycle of elevated blood sugar and excess insulin release leads to dysfunction in insulin-producing cells, ultimately resulting in diabetes. Physical inactivity, poor sleep, and chronic stress further contribute to insulin resistance by altering hormonal balance, inflammatory responses, and glucose metabolism.
Both types of diabetes are important to consider, but in Pakistan, the focus is primarily on type 2 diabetes due to its higher prevalence and preventable nature. According to recent estimates, Pakistan has one of the highest rates of diabetes in the world, with an estimated 33 million adults living with the condition (1).
The rise in diabetes cases in Pakistan can be attributed to three major cultural changes: increased consumption of refined sugars and processed grains, reduced physical activity paired with increased screen time, and more frequent eating and snacking. Western dietary influences have introduced more sugary and processed foods into the Pakistani diet, facilitated by the rapid growth of fast-food restaurants—a trend similar to nutritional shifts seen in other low and middle income countries (LMICs) (10). Moreover, traditional staples such as high-glycemic bread and rice continue to contribute to excessive carbohydrate intake. Decreased physical activity, coupled with more sedentary lifestyles, has further exacerbated the situation by lowering insulin sensitivity and increasing fat storage.
Frequent eating and snacking on unhealthy food may also contribute to the rising incidence of diabetes in Pakistan. While the scientific link between meal frequency and insulin resistance is still being studied, some research suggests that among women who eat breakfast irregularly, meal frequency is associated with a significantly higher risk of developing type 2 diabetes (11). Other studies indicate that frequent meal may contribute to higher BMI (and, by extension, obesity) (12), both of which are major risk factors for insulin resistance.
A critical factor in Pakistan’s diabetes epidemic is central obesity, which is highly prevalent, affecting over 70% of the Pakistani population (13). Excess visceral fat not only contributes to insulin resistance but also promotes chronic inflammation, further accelerating metabolic dysfunction (14). Given this strong link between obesity and diabetes, managing weight effectively is essential to reducing diabetes risk.
Research has consistently shown that weight reduction interventions are among the most effective strategies for preventing type 2 diabetes. The Diabetes Prevention Program (DPP) and similar studies have demonstrated that even modest weight loss (5–10% of body weight) can significantly improve insulin sensitivity and reduce diabetes risk (15). Comprehensive lifestyle interventions, including caloric restriction, increased physical activity, and nutritional counseling, have proven successful in weight management and diabetes prevention efforts (16).
Beyond weight management, insulin resistance itself can be reversed through targeted lifestyle changes. These include reducing the intake of refined sugars and processed grains, focusing on whole foods with low glycemic indices, limiting snacking and incorporating intermittent fasting. While intermittent fasting primarily aids in weight loss, emerging research suggests it may also enhance metabolic flexibility and reduce inflammation (17, 18), both of which play a role in diabetes prevention. Restricting eating to an 8-h window has also been associated with lower insulin levels and improved glucose metabolism (19).
Regular physical activity is equally crucial in this effort. Exercise, particularly after meals, has been shown to improve insulin sensitivity and helps muscles absorb and utilize blood sugar more efficiently (20).
To address the diabetes epidemic in Pakistan, comprehensive public health strategies are vital. Nationwide programs should be implemented to educate the public about healthy eating, weight management, and the risks associated with refined sugars and processed foods. Promoting physical activity through community programs, as well as initiatives in schools and workplaces, is equally important. Enhancing access to affordable, healthy food options—especially in urban areas where sedentary lifestyles and processed foods are more common—can have a significant impact. Additionally, regular screenings for prediabetes and diabetes are crucial for early detection and management.
Addressing the diabetes crisis in Pakistan requires a unified effort at multiple levels, including individuals, communities, and policymakers (see Table 1 for more details). By adopting such a multi-level approach that encourages informed lifestyle changes and the implementation of effective public health strategies, we propose it is possible to reverse the trend and mitigate this growing health crisis.
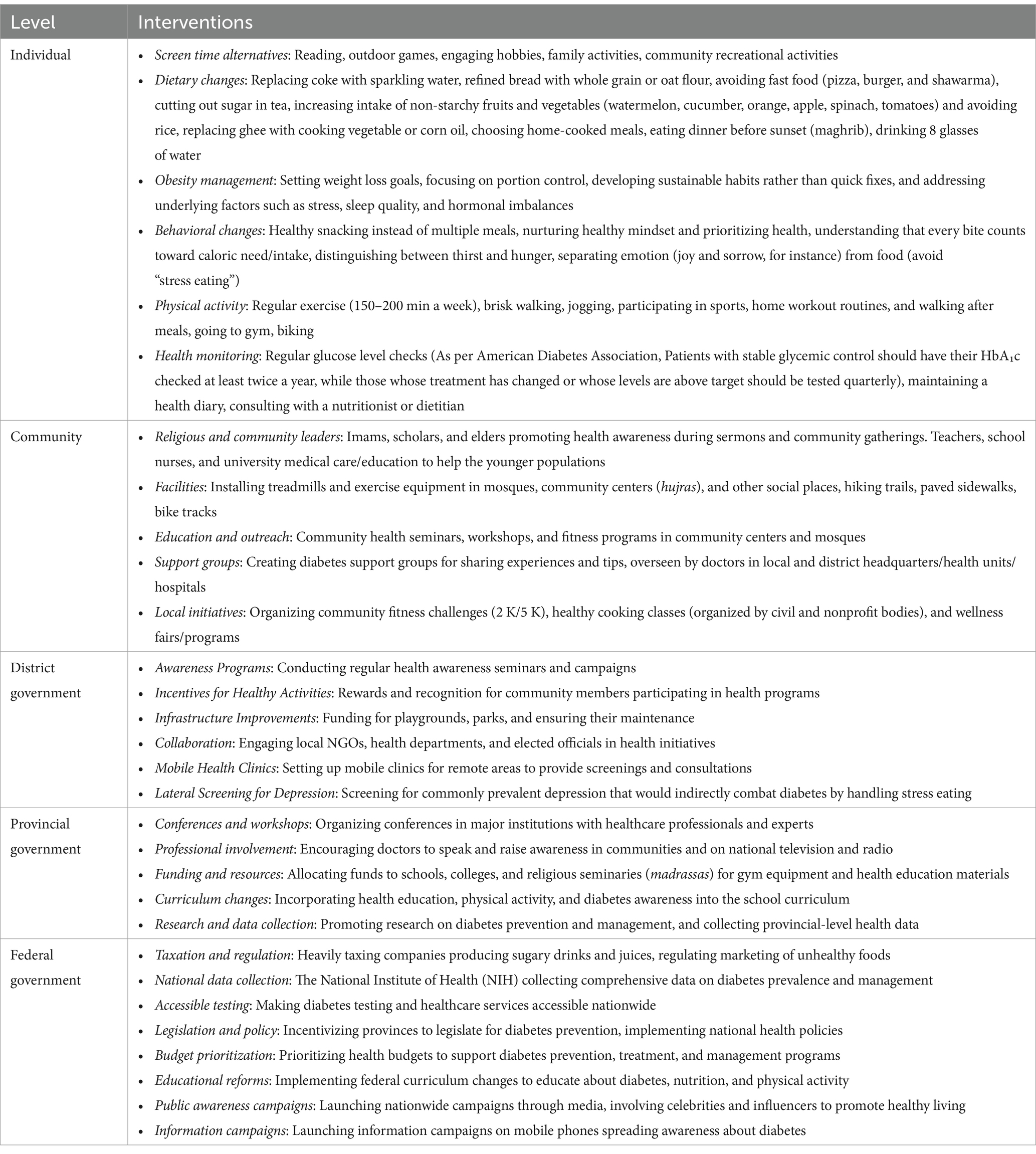
Table 1. A multi-level approach to reduce diabetes in Pakistan.
Table 1 outlines three types of interventions: individual, community, and policymaker interventions. These interventions primarily work synchronously and interdependently. For example, individuals depend on community support, and communities rely on individual participation for the successful implementation of many interventions. Similarly, policymaker support is crucial for both communities and individuals to carry out some of these interventions. This relationship is illustrated in Figure 1.
Figure 1. Multi-level interventions to combat diabetes in Pakistan.
Now let us briefly explain the interventions this multi-level approach may entail at various levels in the following paragraphs.
At the individual level, tackling diabetes begins with lifestyle changes (21) and behavioral adjustments (20), as also supported by studies from the Diabetes Prevention Program (DPP) (Diabetes Prevention Program Group, 2002). Reducing screen time and opting for alternative activities, such as outdoor games or family engagements, can help individuals become more active, thereby reducing the risk of type-2 diabetes (22). Dietary changes are crucial as well (23): swapping sugary drinks for healthier options like sparkling water, avoiding fast foods, and opting for whole grains and non-starchy fruits and vegetables can make a significant difference. Additionally, individuals should aim to reduce their portion sizes, avoid snacking between meals to reduce caloric intake, and eat dinner earlier in the evening, followed by a walk, to help regulate insulin levels.
Effective obesity management, which includes a combination of dietary modifications, portion control, and mindful eating habits, is essential in reducing diabetes risk. Low carbohydrate and Mediterranean diets have also been shown to be effective for weight loss (24).
Physical activity plays a key role in managing insulin sensitivity, as reported in various studies (25–27). Engaging in regular exercise, such as brisk walking or jogging, for 150–200 min a week, as recommended by health guidelines, helps regulate blood sugar and manage obesity effectively (22, 28).
Health monitoring is also necessary. Individuals should regularly check their glucose levels based on risk factors and as advised by medical doctors,4 maintain a health diary, and consult with nutritionists to ensure they stay on track with their health goals.
Communities have the power to support individual efforts through collective health promotion activities (29). In Pakistan, religious and community leaders, such as imams and teachers, can be instrumental in raising awareness about diabetes prevention during sermons and other gatherings. For instance, imams can remind the public during Friday khutba (sermon) of the saying of the Prophet Muhammad (PBUH): “Verily your body has right upon you.”
Worship places such as mosques and churches, community centers and other social spaces (i.e., hujras) can be powerful platforms for implementing programs that promote communal health and provide other social services (30), and even more so in a culturally and religiously vibrant Muslim country like Pakistan (31). These places can be equipped with exercise equipment, such as treadmills, and can host community-driven initiatives like fitness challenges, healthy cooking classes, wellness fairs, and other community activities that encourage people to adopt healthier lifestyles (32).
Education and outreach efforts are also critical at the community level. Workshops and seminars focused on diabetes prevention, particularly in community hubs like mosques and schools, can help disseminate important information, as they have been proven effective in promoting overall wellbeing (31, 33). Additionally, establishing diabetes support groups, overseen by medical professionals, can create a supportive network where individuals share experiences and practical strategies for managing the condition—an approach that has been reported as effective in chronic disease management (34, 35).
Various policy approaches in LMICs have been shown to be effective in disease management and other health-related outcomes (36, 37). Pakistan itself has a track record of successful policy approaches in curtailing COVID-19 and increasing immunization rates (38).
Just as Pakistan treated COVID-19 “an existential threat” and mobilized resources and collaboration, policymakers should take similarly coordinated actions at the district, provincial, and federal levels to effectively manage the diabetes crisis.
At the district level, governments can implement awareness campaigns and offer incentives for community members to participate in health programs. Improving infrastructure by funding playgrounds and parks will encourage physical activity, while mobile health clinics can ensure that remote areas have access to screenings and consultations. It is also important to screen for common mental health conditions like depression, which can contribute to stress eating and exacerbate diabetes.
At the provincial level, governments should focus on organizing conferences and workshops with healthcare professionals to raise awareness about diabetes prevention. Allocating funds for gym equipment and health education materials in schools and religious seminaries will further encourage healthy lifestyles. Incorporating diabetes prevention into the school curriculum and promoting research on diabetes management are additional strategies to address this growing crisis.
Finally, at the federal level, broad policy changes are necessary. Islamabad can introduce taxes on sugary drinks and regulate the marketing of unhealthy foods. Nationwide diabetes testing should be made accessible, and comprehensive data collection by the National Institute of Health (NIH) will enable informed decision-making. Public awareness campaigns featuring celebrities and influencers may also help promote healthy living, while educational reforms that include lessons on nutrition and physical activity will equip future generations with the knowledge they need to prevent diabetes. Legislation that prioritizes health budgets and supports diabetes prevention programs is also essential.
Addressing Pakistan’s diabetes epidemic requires a coordinated, multi-level approach that engages individuals, communities, and policymakers. Through lifestyle changes including obesity management, community support, and strategic policy interventions, Pakistan can combat the rising prevalence of diabetes and work to reverse the trend. These efforts must be widespread and collaborative, ensuring that every level of society contributes to this urgent public health mission. We acknowledge that this approach is just one of many possibilities, and the policy recommendations we propose are suggestions that, if implemented, can help mitigate the diabetes crisis and improve public health outcomes.
FJ: Writing – original draft. UM: Writing – original draft. AN: Writing – review & editing. ShandK: Writing – review & editing. ShanlK: Writing – review & editing. SS: Writing – review & editing. ZW: Writing – review & editing. MAJK: Writing – review & editing. BW: Writing – review & editing. KK: Writing – review & editing. MSK: Writing – review & editing, Writing – original draft.
The author(s) declare that no financial support was received for the research and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declare that no Gen AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. ^https://www.frontiersin.org/research-topics/64734/ensuring-public-health-the-active-role-of-healthcare-professionals/overview
2. ^Insulin resistance refers to a condition where the body’s cells do not respond to insulin effectively (6). Insulin sensitivity, on the other hand, refers to the normal metabolic state where the body efficiently utilizes insulin (39).
3. ^Genetics is also in fact a crucial factor for insulin deficiency in type 1 diabetes.
4. ^According to American Diabetic Association latest guidelines (40), patients with stable glycemic control should have their HbA₁c (Hemoglobin A1c) checked at least twice a year, whereas those whose treatment has changed or whose levels are above target should be tested quarterly.
1. Magliano, D, and Boyko, EJ. IDF diabetes atlas. with International Diabetes Federation, editor. 10th ed (2021) International Diabetes Federation.
2. Saher, T, Al-Worafi, YM, Iqbal, MN, Wahid, A, Iqbal, Q, Khan, A, et al. Doctors’ adherence to guidelines recommendations and glycaemic control in diabetic patients in Quetta, Pakistan: findings from an observational study. Front Med. (2022) 9:978345. doi: 10.3389/fmed.2022.978345
3. Umar Hasan, S, and Rehman Siddiqui, MA. Nationwide prevalence of type 2 diabetes mellitus and pre-diabetes in Pakistan: a systematic review and meta-analysis. Diabetes Res Clin Pract. (2024) 216:111815. doi: 10.1016/j.diabres.2024.111815
4. Laville, M, and Nazare, J-A. Diabetes, insulin resistance and sugars. Obes Rev. (2009) 10:24–33. doi: 10.1111/j.1467-789X.2008.00562.x
5. D’Addio, F, Ben Nasr, M, Lunati, ME, and Fiorina, P. Chapter 31—autoimmune (type 1) diabetes In: ME Gershwin, GC Tsokos, and B Diamond, editors. The rose and Mackay textbook of autoimmune diseases. 7th ed. Cambridge, MA, USA: Academic Press (2024). 585–601.
6. Goldstein, BJ. Insulin resistance as the core defect in type 2 diabetes mellitus. Am J Cardiol. (2002) 90:3–10. doi: 10.1016/S0002-9149(02)02553-5
7. Wysham, C, and Shubrook, J. Beta-cell failure in type 2 diabetes: mechanisms, markers, and clinical implications. Postgrad Med. (2020) 132:676–86. doi: 10.1080/00325481.2020.1771047
8. James, DE, Stöckli, J, and Birnbaum, MJ. The aetiology and molecular landscape of insulin resistance. Nat Rev Mol Cell Biol. (2021) 22:751–71. doi: 10.1038/s41580-021-00390-6
9. Musso, G, Gambino, R, De Michieli, F, Cassader, M, Rizzetto, M, Durazzo, M, et al. Dietary habits and their relations to insulin resistance and postprandial lipemia in nonalcoholic steatohepatitis. Hepatology. (2003) 37:909–16. doi: 10.1053/jhep.2003.50132
10. Malik, VS, Willett, WC, and Hu, FB. Global obesity: trends, risk factors and policy implications. Nat Rev Endocrinol. (2013) 9:13–27. doi: 10.1038/nrendo.2012.199
11. Mekary, RA, Giovannucci, E, Cahill, L, Willett, WC, van Dam, RM, and Hu, FB. Eating patterns and type 2 diabetes risk in older women: breakfast consumption and eating frequency123. Am J Clin Nutr. (2013) 98:436–43. doi: 10.3945/ajcn.112.057521
12. Kahleova, H, Lloren, JI, Mashchak, A, Hill, M, and Fraser, GE. Meal frequency and timing are associated with changes in body mass index in Adventist health study 2. J Nutr. (2017) 147:1722–8. doi: 10.3945/jn.116.244749
13. Basit, A, Askari, S, Zafar, J, Riaz, M, Fawwad, A, and Members, NDSP. NDSP 06: prevalence and risk factors for obesity in urban and rural areas of Pakistan: a study from second National Diabetes Survey of Pakistan (NDSP), 2016-2017. Obes Res Clin Pract. (2021) 15:19–25. doi: 10.1016/j.orcp.2020.11.007
14. Kahn, SE. The relative contributions of insulin resistance and beta-cell dysfunction to the pathophysiology of type 2 diabetes. Diabetologia. (2003) 46:3–19. doi: 10.1007/s00125-002-1009-0
15. Diabetes Prevention Program Group. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med. (2002) 346:393–403. doi: 10.1056/NEJMoa012512
16. Tuomilehto, J, Lindström, J, Eriksson, JG, Valle, TT, Hämäläinen, H, Ilanne-Parikka, P, et al. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N Engl J Med. (2001) 344:1343–50. doi: 10.1056/NEJM200105033441801
17. Cabo, R.De, and Mattson, M. P. (2019). Effects of intermittent fasting on health, aging, and disease. N Engl J Med, 381, 2541–2551. doi: 10.1056/NEJMra1905136
18. Patterson, RE, and Sears, DD. Metabolic effects of intermittent fasting. Annu Rev Nutr. (2017) 37:371–93. doi: 10.1146/annurev-nutr-071816-064634
19. Sutton, EF, Beyl, R, Early, KS, Cefalu, WT, Ravussin, E, and Peterson, CM. Early time-restricted feeding improves insulin sensitivity, blood pressure, and oxidative stress even without weight loss in men with prediabetes. Cell Metab. (2018) 27:1212–1221.e3. doi: 10.1016/j.cmet.2018.04.010
20. American Diabetes Association. Physical activity/exercise and diabetes: a position statement of the American Diabetes Association. Diabetes Care. (2025) 39:2065–79. doi: 10.2337/dc16-1728
21. Lambrinou, E, Hansen, TB, and Beulens, JW. Lifestyle factors, self-management and patient empowerment in diabetes care. Eur J Prev Cardiol. (2019) 26:55–63. doi: 10.1177/2047487319885455
22. Hamasaki, H. Daily physical activity and type 2 diabetes: a review. World J Diabetes. (2016) 7:243–51. doi: 10.4239/wjd.v7.i12.243
23. Khazrai, YM, Defeudis, G, and Pozzilli, P. Effect of diet on type 2 diabetes mellitus: a review. Diabetes Metab Res Rev. (2014) 30:24–33. doi: 10.1002/dmrr.2515
24. Ajala, O, English, P, and Pinkney, J. Systematic review and meta-analysis of different dietary approaches to the management of type 2 diabetes123. Am J Clin Nutr. (2013) 97:505–16. doi: 10.3945/ajcn.112.042457
25. Admiraal, WM, van Valkengoed, IGM, De Munter, JS, Stronks, K, Hoekstra, JBL, and Holleman, F. The association of physical inactivity with type 2 diabetes among different ethnic groups. Diabet Med. (2011) 28:668–72. doi: 10.1111/j.1464-5491.2011.03248.x
26. Bird, SR, and Hawley, JA. Update on the effects of physical activity on insulin sensitivity in humans. BMJ Open Sport Exerc Med. (2017) 2:e000143. doi: 10.1136/bmjsem-2016-000143
27. Mann, S, Beedie, C, Balducci, S, Zanuso, S, Allgrove, J, Bertiato, F, et al. Changes in insulin sensitivity in response to different modalities of exercise: a review of the evidence. Diabetes Metab Res Rev. (2014) 30:257–68. doi: 10.1002/dmrr.2488
28. Fogelholm, M. Walking for the management of obesity. Dis Manag Health Out. (2005) 13:9–18. doi: 10.2165/00115677-200513010-00002
29. Brown, ER. Community action for health promotion: a strategy to empower individuals and communities. Int J Health Serv. (1991) 21:441–56. doi: 10.2190/AKCP-L5A4-MXXQ-DW9K
30. Niazi, AG, Ahmed, N, Kifayat, S, Kifayat, S, Niazi, MA, and Khan, MS. Urban churches show an increase in attendance, donations, and finances during the COVID-19 pandemic in the USA: evidence from the united Methodist church. J Relig Health. (2024) 63:3206–32. doi: 10.1007/s10943-024-02046-z
31. Abu-Ras, W, Aboul-Enein, BH, Almoayad, F, Benajiba, N, and Dodge, E. Mosques and public health promotion: a scoping review of faith-driven health interventions. Health Educ Behav. (2024) 51:677–90. doi: 10.1177/10901981241252800
32. Woolf, SH, Dekker, MM, Byrne, FR, and Miller, WD. Citizen-centered health promotion: building collaborations to facilitate healthy living. Am J Prev Med. (2011) 40:S38–47. doi: 10.1016/j.amepre.2010.09.025
33. Alaca, B. (2022). The role of mosques in promoting well-being in Muslim communities. Available at: http://hdl.handle.net/1807/125438 (Accessed February 10, 2025).
34. Bernhard, G, Ose, D, Baudendistel, I, Seidling, HM, Stützle, M, Szecsenyi, J, et al. Understanding challenges, strategies, and the role of support networks in medication self-management among patients with type 2 diabetes: a qualitative study. Diabetes Educ. (2017) 43:190–205. doi: 10.1177/0145721717697243
35. Huh, J., and Ackerman, M. S. (2012). Collaborative help in chronic disease management: supporting individualized problems. Proceedings of the ACM 2012 Conference on Computer Supported Cooperative Work, 853–862. doi: 10.1145/2145204.2145331
36. Banerjee, AV, Duflo, E, Glennerster, R, and Kothari, D. Improving immunisation coverage in rural India: clustered randomised controlled evaluation of immunisation campaigns with and without incentives. BMJ. (2010) 340:c2220. doi: 10.1136/bmj.c2220
37. Khan, MS. Improving the Covid-19 vaccination rate in Pakistan—a multipronged policy approach. Front Public Health. (2021) 9:729102. doi: 10.3389/fpubh.2021.729102
38. Khan, AA, Abdullah, M, Khan, R, Kazmi, T, Sultan, F, Aamir, S, et al. Pakistan’s national COVID-19 response: lessons from an emergent response to the pandemic. Front Public Health. (2024) 12:1379867. doi: 10.3389/fpubh.2024.1379867
39. Borai, A, Livingstone, C, and Ferns, GAA. The biochemical assessment of insulin resistance. Ann Clin Biochem. (2007) 44:324–42. doi: 10.1258/000456307780945778
Keywords: type 2 diabetes, prevention measures (PM), policy interventions, Pakistan, obesity, public awareness, dietary changes, risk factors
Citation: Jamil F, Mir U, Niazi AG, Kifayat S, Kifayat S, Shafiq S, Wali Z, Khan MAJ, Wali B, Kobra KT and Khan MS (2025) A multi-level approach to reduce exploding type 2 diabetes in Pakistan. Front. Public Health. 13:1514090. doi: 10.3389/fpubh.2025.1514090
Edited by:
Niccolo Persiani, University of Florence, ItalyReviewed by:
Gregory Westcott, Beth Israel Deaconess Medical Center and Harvard Medical School, United StatesCopyright © 2025 Jamil, Mir, Niazi, Kifayat, Kifayat, Shafiq, Wali, Khan, Wali, Kobra and Khan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fazal Jamil, ZmphbWlsQG1lcmN5LmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.