
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Public Health, 06 March 2025
Sec. Infectious Diseases: Epidemiology and Prevention
Volume 13 - 2025 | https://doi.org/10.3389/fpubh.2025.1510391
 Oluwafemi Adeagbo1*
Oluwafemi Adeagbo1* Oluwaseun Abdulganiyu Badru2
Oluwaseun Abdulganiyu Badru2 Prince Addo2Amber Hawkins1
Prince Addo2Amber Hawkins1 Monique Janiel Brown2
Monique Janiel Brown2 Xiaoming Li2Rima Afifi1
Xiaoming Li2Rima Afifi1Introduction: Black/African American men who have sex with other men (BMSM) are disproportionately affected by HIV, experience significant disparities in HIV incidence, and face significant barriers to accessing HIV treatment and care services, including pre-exposure prophylaxis (PrEP). Despite evidence of individual and structural barriers to PrEP use in the Midwest, no review has synthesized this finding to have a holistic view of PrEP uptake and barriers. This review examines patterns of, barriers to, and facilitators of PrEP uptake among BMSM in the Midwest, United States (US).
Methods: Five databases (CINAHL Plus, PUBMED, PsycINFO, SCOPUS, and Web of Science) were searched in March 2023. We included studies that focused on BMSM in the Midwestern states; only empirical studies (either quantitative or qualitative or both) were considered. We synthesized the qualitative data and teased out some of the factors inhibiting or facilitating PrEP uptake among BMSM.
Results: We screened 850 articles, and only 22 (quantitative: 12; qualitative: 8; mixed methods: 2) met our set eligibility criteria. Most of the studies were conducted in Chicago. Most BMSM use oral than injectable PrEP. Uptake of PrEP ranged from 3.0 to 62.8%, and the majority reported a prevalence of less than 15%. The barriers include PrEP awareness, PrEP access, PrEP stigma, side effects, PrEP preference, socioeconomic status, medical insurance and support, partner trust, trust in the health system, and precautions with sexual partners. The identified PrEP facilitators include PrEP use until HIV is eradicated, friend influence, experience with dating men living with HIV, safety, phobia for HIV, disdain for condoms, and power to make decisions.
Conclusion: Our review summarized patterns of, barriers to, and facilitators of PrEP uptake among BMSM in the Midwest, United States. The low PrEP uptake of BMSM was primarily attributed to mistrust in the health system and low socioeconomic status. Multimodal and multilevel strategies are needed to improve PrEP uptake among BMSM, including improving the marketing of PrEP to BMSM and removing financial barriers to accessing PrEP service.
Approximately 12% of the United States (US) population were Non-Hispanic Black/African American in 2019 (1), and yet 37.4% of people living with HIV (PLWH) are non-Hispanic Black/African Americans (2). Similarly, Black/African American men who have sex with other men (BMSM) experience significant disparities in HIV incidence, access to HIV care, and prevention across all age groups (3–5). Of the estimated 37,981 new HIV diagnoses in the US in 2022, 70% were among men who have sex with other men (MSM), including BMSM (34%) (6). The Centers for Disease Control and Prevention (CDC) estimated that one in two BMSM will be diagnosed with HIV in their lifetime (7), and BMSM are eight times more likely to be diagnosed with HIV than White MSM in their lifetimes (8).
As of 2022, in the Midwest US, males (79.3%) and Blacks (41.6%) were more likely to be living with HIV, and male-to-male sexual contact (79.2%) was the commonest mode of transmission. Also, eight in ten (81.6%) of new HIV cases were among MSM (9). Furthermore, BMSM are more burdened with HIV than non-Hispanic Whites. For example, Mustanki and colleagues, in their cohort study, found that HIV is more common among BMSM than their Hispanic and non-Hispanic White counterparts (10). Similarly, BMSM are 10 times more likely to be living with HIV than non-Hispanic Whites in Iowa (11). Lack of medical insurance for HIV preventive care, historical discrimination, and structural racism, such as institutional racism and homophobia, are some of the root causes of HIV disparities in the US (12, 13).
Recently, the US government published a plan for “Ending the HIV Epidemic”(EHE) by 2030 (14–16). One of the four strategic goals of the EHE initiative is wider pre-exposure prophylaxis (PrEP) coverage, especially among populations at higher risk of HIV acquisition (14). PrEP is a biomedical medication that, when used consistently by an HIV-negative person, reduces the chances of contracting HIV for all populations, including priority populations such as those who inject drugs and BMSM (12, 17). Effective use of PrEP by BMSM will reduce the HIV burden by halting ongoing HIV transmission and contributing to MSM community-level protection (18). Several studies (including clinical trials) have found PrEP highly effective for HIV prevention, particularly for those at risk, including BMSM (19–21). Despite the documented benefits of PrEP as an effective HIV prevention method, the uptake of this biomedical medication to prevent HIV is very low across the US, including among BMSM (3, 22). According to recent estimates from the CDC, only 30% of the 1.2 million people in the US who might benefit from PrEP were prescribed PrEP in 2021 (23). Common barriers to PrEP uptake included factors such as low socioeconomic status, health insurance, medical mistrust, misinformation about PrEP, as well as racism, discrimination, healthcare providers’ negative attitudes, and PrEP access (12, 22, 24, 25). The COVID-19 pandemic further exacerbated PrEP uptake by intensifying several of these barriers (26, 27).
Several PrEP-related reviews in the US have focused on PrEP uptake, barriers, and facilitators among only MSM or the general population, including MSM and transgender persons (28–30). To our knowledge, no review has synthesized the uptake, barriers, and facilitators of PrEP use among BMSM in the US Midwest states despite increasing rates of new HIV diagnoses cases and rates since 2020 in the Midwest (31), and that 3 of the 7 States with the greatest unmet need for PrEP among Black people were in the Midwest (32). This systematic review aims to investigate patterns of PrEP uptake and identify barriers and facilitators to PrEP uptake among BMSM in the Midwest, US. This would inform the development of interventions to increase PrEP uptake among this priority population and help achieve the goals of the EHE initiative in the US.
This systematic review was conducted in line with the Updated Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) guidelines (33).
Our eligibility criteria followed the population/participants, interventions, comparison, outcome, and study design (PICOS) framework (34). We included empirical studies conducted solely or partly among BMSM in the Midwestern states of the United States. Commentaries, letters to the editor, or expert opinions were not considered. We focused on studies with a primary or secondary focus on PrEP uptake, barriers, or facilitators. We did not limit our search by language or time.
CINAHL Plus, PUBMED, PsycINFO, SCOPUS, and Web of Science were searched in March 2023 using relevant keywords (such as PrEP, barriers, and specific Midwest states), Medical Subject Headings (MeSH) terms, and Boolean operators. For example, we search PubMed with the following terms: (((Barrier* OR problem* OR reluctan* OR concern* OR stigma OR perception OR belief OR attitude OR enabler* OR Motivator* OR facilitator* OR encouragement OR predictor* OR determinant* OR engagement OR uptake OR initiation OR Use OR Utilization OR Utilization OR Compliance OR Adherence) AND (“Pre-Exposure Prophylaxis”[Mesh] OR “pre-exposure prophylaxis” OR PrEP OR Truvada OR Descovy)) AND (“men who have sex with men” OR MSM OR Gay* OR “male couple*” OR homosexual* OR “transgender wom*” OR “trans wom*” OR “bisexual men”)) AND (Iowa OR “Midwest region” OR “Midwestern region” OR “Midwest state*” OR Illinois OR Indiana OR Kansas OR Michigan OR Minnesota OR Missouri OR Nebraska OR “North Dakota” OR Ohio OR “South Dakota” OR Wisconsin). We did not limit our search by date or language. The comprehensive search strategy for other databases is in the Supplementary material. Rayyan, an online article manager (35), was used for the article screening process. Two reviewers (OAB and PA) met to finalize the study eligibility criteria before screening. One reviewer (OAB) removed duplicate articles; two reviewers (OAB and PA) independently performed title and abstract screening. Both reviewers resolved all disagreements through discussions. References of all articles that met our eligibility criteria were manually searched for additional relevant articles.
We extracted the following details from each article that met the set eligibility criteria: author and year of publication, Midwest state, study design, sample size and technique, type of PrEP (pills or injectables), analysis type, BMSM sociodemographic information (i.e., race and age), PrEP uptake, barriers to and facilitators of PrEP use. One reviewer (OAB) extracted all the details, while another reviewer (OAA) checked for accuracy.
All the articles that met the eligibility criteria were subject to methodological rigor assessment using the appropriate Joanna Briggs Institute tools (depending on the study design); one reviewer (OAB) performed this process, which was verified by another reviewer (OAA).
The quantitative findings were summarized descriptively. We synthesized the qualitative data and identified the common factors inhibiting or facilitating PrEP uptake among Black MSM.
The systematic search across five databases produced 850 articles. The duplicates were 437, leaving 413 articles for title and abstract screening. Of these, 270 were excluded as they did not meet our eligibility criteria; the remaining 143 articles were subject to full-text screening. A further 121 articles were excluded for lack of relevant information and having no distinct information for BMSM. Therefore, only 22 articles that met the eligibility criteria were included in this review (Figure 1). All the studies were judged to have high methodological rigor (Table 1).
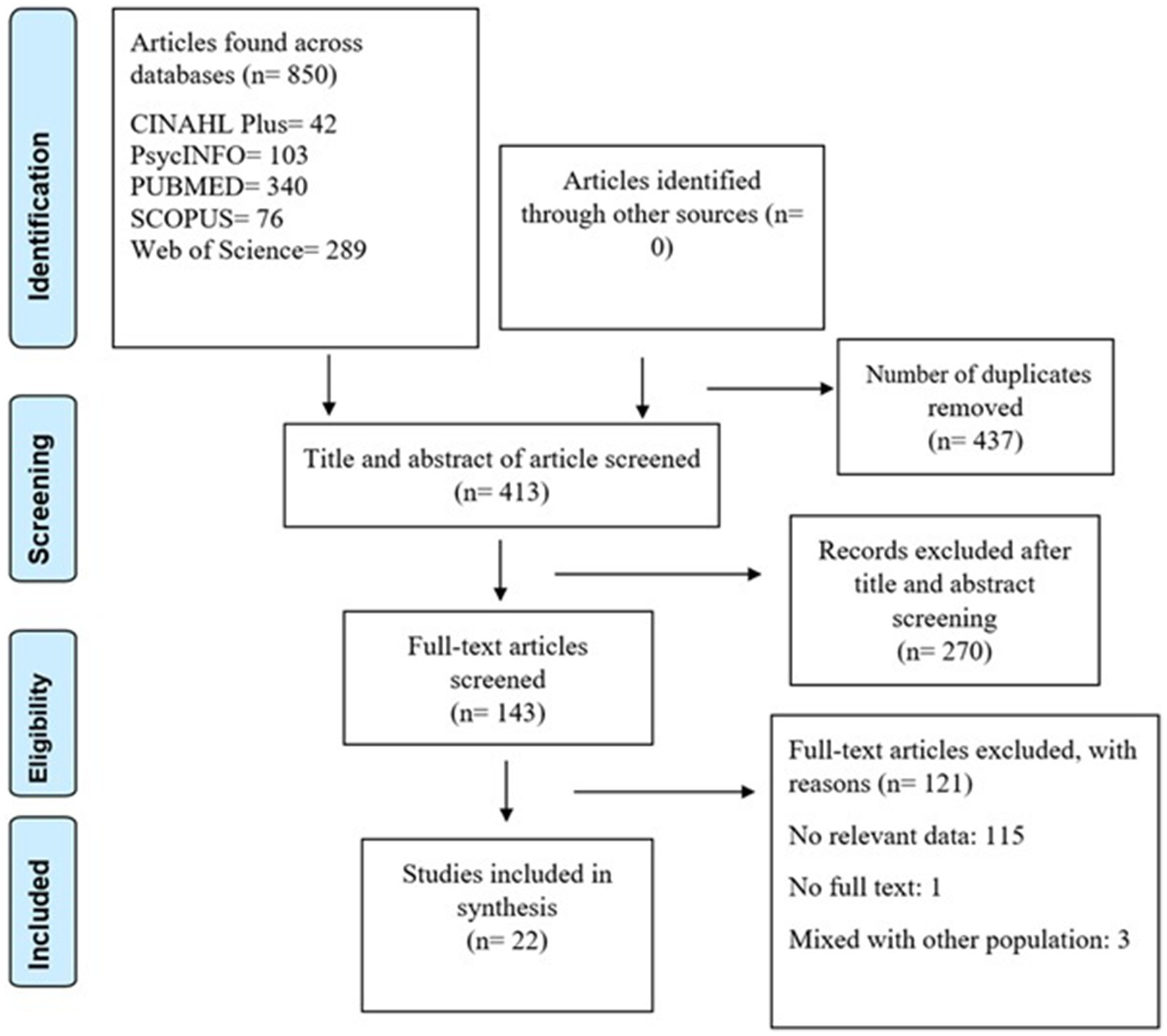
Figure 1. Search strategy flowchart.
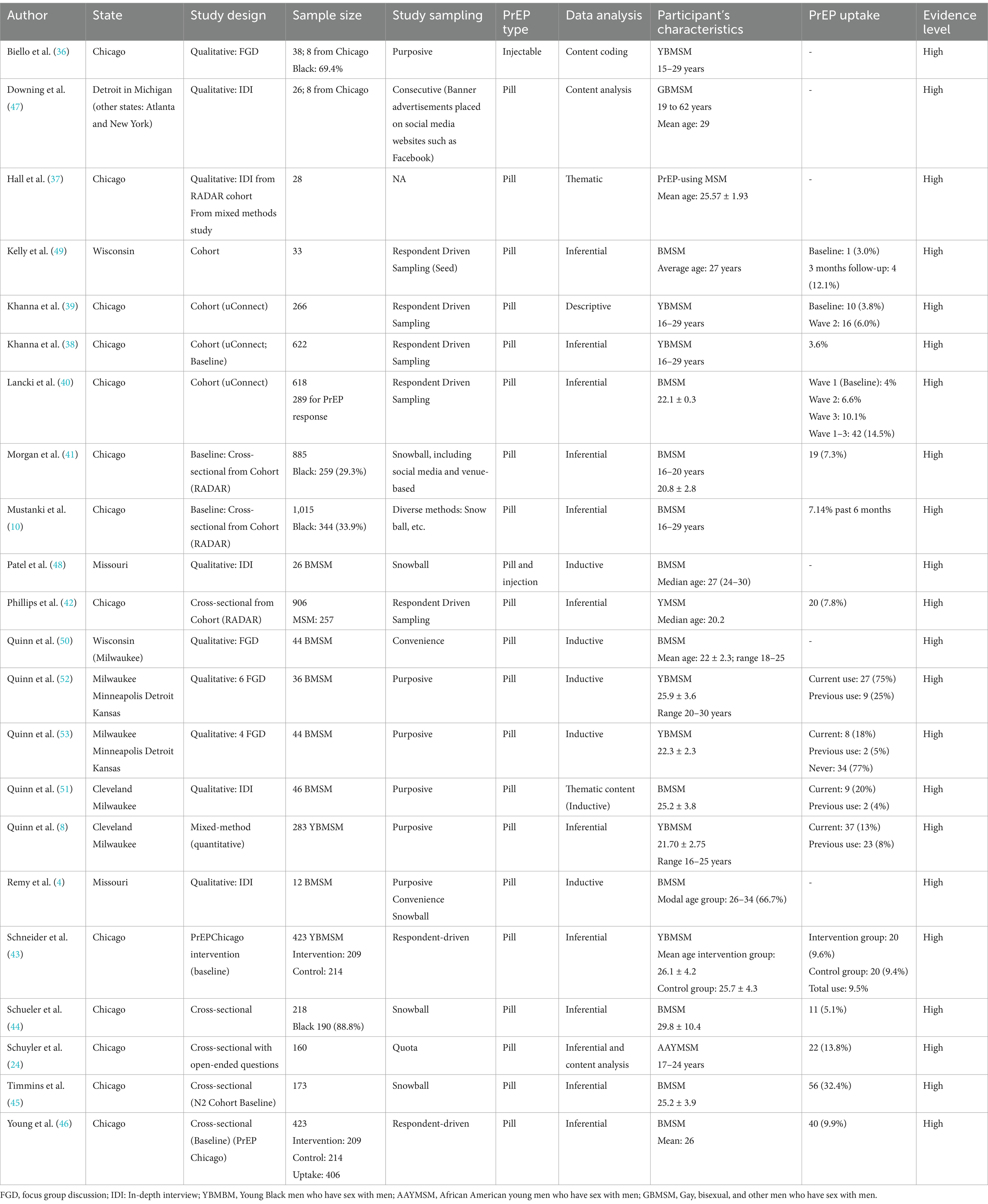
Table 1. Characteristics of the included studies.
Of the 22 studies, 15 (62.5%) were conducted in Chicago (10, 24, 36–46). The remaining studies were conducted in Michigan (47), Missouri (4, 48), and Wisconsin (8, 49–51); two studies focused on four regions: Detroit, Kansas, Milwaukee, and Minneapolis (52, 53).
Twelve (59%) studies were quantitative (10, 24, 38–46, 49), and eight (33%) were strictly qualitative (4, 36, 47, 48, 50–53). Two (8%) studies adopted a mixed methods design (8, 37) but reported either quantitative findings only (8) or qualitative findings only as part of a broader study (37). It is important to stress that seven of the cross-sectional studies analyzed a portion of results from a cohort study (10, 41, 42, 44–46). For studies that conducted qualitative designs, whether qualitative only or from a mixed methods study, five used an in-depth interview approach (4, 37, 47, 48, 51), while four used focus group discussions (36, 50, 52, 53).
Most of the studies (n = 22, 92%) focused only on oral PrEP (i.e., pills), while Biello et al. (36) focused on injectable PrEP and Patel et al. (48) focused on both pills and injectable PrEP. Uptake of PrEP differed across the 12 studies that quantified PrEP uptake, ranging from 3.0 to 32.4% (8, 10, 24, 38, 40–46, 49). However, overall, the findings reveal that most BMSM may not be using PrEP. For instance, 11 studies (79%) reported a PrEP uptake of less than 15% (10, 24, 38–44, 46, 49); and Timmins et al. (45) reported 32.4%. The two studies that reported baseline and follow-up PrEP use recorded little difference between both periods (39, 49).
The barriers to PrEP uptake among BMSM in the Midwest are based on the findings of the included qualitative studies. Several barriers to PrEP uptake emerged, including PrEP unawareness, access, stigma, PrEP side effects, low socioeconomic status, trust in partners, distrust in the health system, and concerns over PrEP adherence (Table 2).
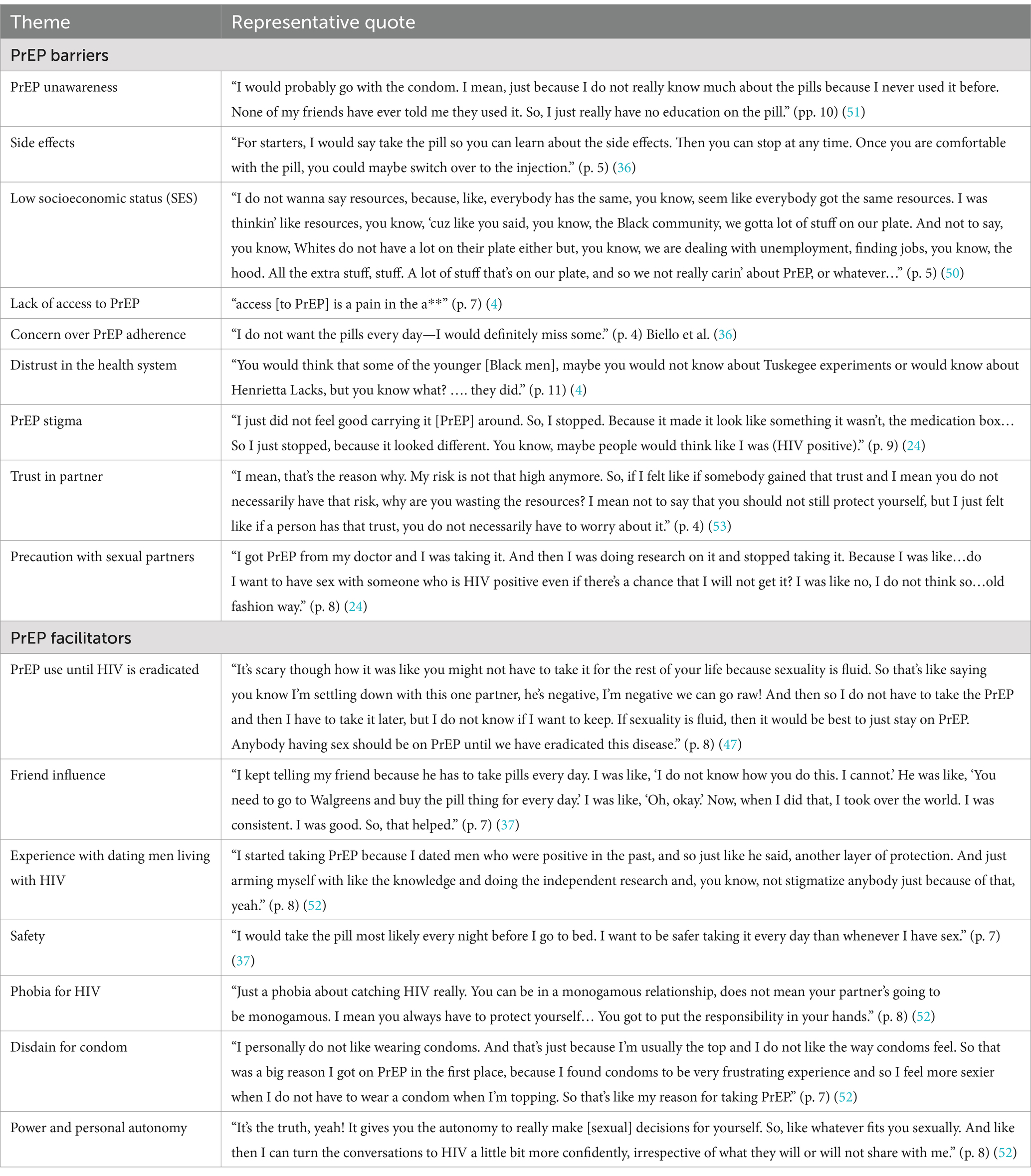
Table 2. Barriers and facilitators to PrEP uptake.
Regarding the PrEP barriers, being unaware of PrEP was common among BMSM in the Midwest. Some BMSM reported that they had never heard of PrEP (51). PrEP side effects were inhibiting factors for those who were aware of PrEP (36). Additionally, we found that low socioeconomic status often prevents access to PrEP. Specifically, some BMSM were uninsured compared to their White counterparts and, as a consequence, do not have money to pay for PrEP-related care when needed, exacerbated by the difficulty in securing jobs (50).
Furthermore, BMSM reported structural-related issues in accessing PrEP. For example, many BMSM reported they could not access PrEP in health facilities for reasons such as health workers not being aware of it or refusing to make it available to them, and even when available, the wait time can be very long (4). Another barrier is distrust of the health system. BMSM continues to refer to historical unethical practices experienced by the Black community, such as the Henrietta Lacks and the Tuskegee experiments, as a reason for not using PrEP (4).
BMSM reported that the fear of others knowing that they are using PrEP is a primary reason they are not interested in PrEP uptake (24, 36). According to some of them, they risk being seen with PrEP if they opt to take it and fear that people will assume they are living with HIV (24, 36). There is evidence that the concern of being labeled “HIV positive” led to the discontinuation of PrEP among some BMSM (24). Interestingly, some BMSM in monogamous relationships trust their partner, and they seem not to be interested in PrEP because they perceive their HIV risk to be low, and they do not want to lose their partner’s trust (24, 53). Moreover, some BMSM did not see a need to be on PrEP because they do not intend to have sexual intercourse with an infected person (24).
We found several factors that made BMSM utilize PrEP, including the safety it provides, having friends who use PrEP, fear of HIV, dislike for condoms, and experience dating men living with HIV. Specifically, some BMSM reported that they adhered to PrEP because they had friends who were on PrEP (37). Furthermore, BMSM were more likely to use PrEP if they had had an experience dating men living with HIV (52), mainly because it protects or provides safety against HIV infection (37, 53).
Another interesting reason for PrEP uptake was the sexual autonomy and power it provides because BMSM on PrEP have more flexibility in sexual decision-making (52). Moreover, they felt that it was better to be on PrEP than use condoms, which they perceived to be “frustrating” and less enjoyable (52). BMSM also alluded that they choose to use PrEP because of fear of contracting HIV (52), and many chose to remain on PrEP until HIV is “eradicated” (47).
This systematic review assessed barriers and facilitators to PrEP use among BMSM in the Midwestern states. The uptake of PrEP appears low among BMSM in the Midwest. Most of the studies that quantified PrEP uptake reported a prevalence of less than 15%, and we found several barriers that could influence the lack of PrEP use among BMSM from qualitative studies only. This leaves a gap that needs to be filled by researchers interested in PrEP-related research.
One major barrier to PrEP uptake was the lack of PrEP awareness and knowledge among BMSM. Coukan et al. (54) found a similar issue in their review of barriers to PrEP among underserved populations and MSM in the United Kingdom (UK). Knowledge and awareness of PrEP should precede its access and uptake. This calls for more sensitization of PrEP not just for BMSM in the Midwest but also for all key or priority populations globally. Lack of awareness was not limited to BMSM alone; we also found evidence of a lack of knowledge and awareness of PrEP among healthcare providers. Previous US reviews have also reported a similar finding from a pool of studies across several states (30, 55). Lancki et al. (40) reported that the extent to which healthcare providers influence low PrEP awareness and uptake among those who need it might be uncertain, but it is worrisome as it directly impacts counseling and PrEP prescription for BMSM in the US, and could have a negative effect on interventions (30, 56).
Interventions to improve PrEP awareness should be bidirectional, focusing on BMSM (and other priority populations) and healthcare providers; the latter may be more important than the former. An earlier systematic review of healthcare providers’ barriers to PrEP in the US found no intervention tailored toward the improvement of healthcare providers’ knowledge (55); Pleuhs and colleagues also reported the willingness of healthcare providers to prescribe PrEP after an educational intervention; this gap needs urgent attention (55).
Another barrier that impedes on BMSM’s PrEP uptake was low SES. We found that BMSM with low SES were less likely to initiate PrEP and other health services. This perhaps led to complete neglect of the healthcare system and interest in PrEP. Some BMSM prioritized earning a living in the face of unemployment, which is perceived to be more prevalent among Black/African American populations (57).
Furthermore, lack of access to PrEP was a major a barrier. BMSM appeared to have issues accessing health facilities to obtain PrEP, similar to the findings of earlier reviews (30, 54). The lack of access to PrEP may be due to financial difficulties, lack of medical insurance, and limited deliveries of PrEP to Black communities (30). Also, despite the implementation of TelePrEP in Iowa to address access and other barriers, only a few African Americans (17/167) initiated PrEP (58). Innovative strategies are required to overcome PrEP access, especially for BMSM and other priority populations (59).
HIV-related stigma was another barrier identified in this review. HIV-related stigma may have a negative effect on PrEP uptake because there are concerns that being on PrEP may attracts social stigma, particularly enacted stigma, and some BMSM were worried about being perceived to be sexually deviant or promiscuous. Other reviews focused on MSM and transgender persons in the US and UK have established a similar observation (28, 30, 54, 55). Public health experts in the HIV space need to sensitize the larger community about PrEP benefits to reduce the PrEP-related stigma.
Moreover, another important barrier to PrEP uptake among BMSM was their knowledge of previous unethical experiments like the Tuskegee experiment with the Black or African American community Throughout history, the health system has not earned the trust of the Black community following previous unethical experiments (e.g., the Tuskegee experiment), and HIV treatment is a famous example, which unfortunately seems to be playing out with PrEP. Lack of trust in the health system was reported by several PrEP-related reviews (28, 30, 54, 55).
Regarding PrEP facilitators, this review found that BMSM were not interested in using PrEP if they trusted that their partners were faithful to them and if they were in a monogamous relationship. We did not find an earlier review with a similar observation among BMSM. Naturally, trust strengthens the bond between couples. Some may argue that having trust in a partner may not be a barrier to PrEP use as there may not be a need to be on PrEP if there are no risks. Interestingly, we also found that trust did not matter to some BMSM as they were on PrEP to limit their risk of contracting HIV. Also, being in a monogamous relationship does not necessarily mean that one’s partner may not have other sexual partners, which led to regular PrEP use by some BMSM. This result corroborates other primary studies conducted in the US and Vietnam (60, 61).
The present review provides some insights into factors that influence PrEP use among BMSM. BMSM were more likely to use PrEP if they had friends living with HIV, perhaps due to perceived susceptibility to HIV. Not surprisingly, those who have previously dated men living with HIV were motivated to be on PrEP to reduce their chances of contracting HIV (62).
This review found that some BMSM prefer condomless sexual intercourse, claiming that condoms reduce pleasure, and choose to reduce HIV risk by being on PrEP. The debate on the sensitivity of condoms has been long discussed. However, it may be acceptable to choose from the range of HIV preventive strategies available since all the preventive strategies have a similar objective – preventing HIV. Also, some BMSM chose to be on PrEP to minimize HIV risk, irrespective of the level of trust for their partners (63).
This review is not without limitations. This is the first review to report about BMSM in the US Midwest. However, the findings may not generalize to other BMSM outside the Midwest or the US because the context may differ. Our coding of the themes may not have captured the true picture of what individual studies intended, as we cannot access the full transcripts and interview guides. Also, a few studies had a small number of non-BMSM participants in their sample, which may have impacted our findings. Moreover, some studies were conducted by the same authors who may have published these studies using the same data and population, which may influence our conclusions. Additionally, many of the previous reviews that we compare our results to focus mostly on urban areas. Therefore, we are not able to differentiate between urban and rural communities in our paper. Also, we could not perform a meta-analysis for quantitative data due to the heterogeneity of the data obtained from the included studies. For instance, some studies had a few participants who were bisexual (men who have sex with men and women, and others had transgender women who have sex with men). A pooled estimate of the uptakes may be possible with a sub-group meta-analysis; however, because of the variation in population and study designs, we may be committing type 2 error due to fewer studies in each subgroup analysis. It was not advisable to pool estimates with traces of heterogeneity and bias (64).
We synthesized common and ubiquitous barriers to PrEP uptake among BMSM in the Midwestern states of the US, including lack of PrEP awareness by BMSM and healthcare providers, PrEP access, PrEP stigma, and distrust in the health system. For BMSM using PrEP, friends influences, experiences dating other men living with HIV, displeasure from condoms, and fear of HIV were some of the reasons they opted for PrEP. Although these barriers and facilitators are not unique to the Midwest, they are important to consider in developing HIV prevention interventions in the region. Fundamental issues must be addressed to flatten the HIV curve for BMSM and other sexual minority populations. Multimodal and multilevel strategies are needed to improve PrEP uptake among BMSM. Poor knowledge or lack of PrEP awareness is arguably the major barrier to PrEP uptake because intention to act (use PrEP) may be influenced by knowledge of PrEP. Although knowledge of PrEP does not necessarily increase PrEP use (as the history of institutional and structural racism may impede PrEP uptake), PrEP awareness can serve as the entry point to its use. Therefore, the increase in PrEP awareness and knowledge is important. Furthermore, the initiative and funds directed toward HIV treatment can be replicated in HIV prevention, particularly the availability and accessibility of low-cost or free PrEP for users. Moreover, perhaps due to previous unethical experiments and individual experience engaging with HIV care, there is a need to build the trust of those with default mistrust for biomedical innovations through genuine information about PrEP (including its potential side-effects) and community engagements, with an emphasis on Black communities. Biomedical and HIV researchers must show transparency in trials and clinical research to boost the confidence of the target population, such as MSM and other priority populations. Finally, more advocacy on the importance of PrEP and the need to support persons interested in PrEP is needed while discouraging PrEP-related stigma. Innovations like long-lasting PrEP, such as injectable PrEP, and portraying PrEP as a medication for all rather than a specific population with a risk for HIV may help improve the visibility and acceptance of PrEP.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
OA: Conceptualization, Project administration, Supervision, Validation, Writing – original draft, Writing – review & editing. OB: Data curation, Formal analysis, Investigation, Methodology, Project administration, Visualization, Writing – original draft, Writing – review & editing. PA: Investigation, Methodology, Writing – original draft, Writing – review & editing. AH: Writing – original draft, Writing – review & editing. MB: Supervision, Writing – original draft, Writing – review & editing. XL: Supervision, Writing – original draft, Writing – review & editing. RA: Supervision, Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Gen AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1510391/full#supplementary-material
1. OMH. (2023) Black/African American - the Office of Minority Health. Available online at: https://minorityhealth.hhs.gov/omh/browse.aspx?lvl=3&lvlid=61
2. CDC. (2024) Fast facts: HIV in the US by race and ethnicity. Available online at: https://www.cdc.gov/hiv/data-research/facts-stats/race-ethnicity.html
3. Mouhanna, F, Castel, AD, Sullivan, PS, Kuo, I, Hoffman, HJ, Siegler, AJ, et al. Small-area spatial-temporal changes in pre-exposure prophylaxis (PrEP) use in the general population and among men who have sex with men in the United States between 2012 and 2018. Ann Epidemiol. (2020) 49:1–7. doi: 10.1016/j.annepidem.2020.07.001
4. Remy, LM, Majee, W, Teti, M, and Enriquez, M. Perceptions of black men who have sex with men about accessing and taking PrEP: a qualitative study. J HIV AIDS Soc Serv. (2020) 19:263–82. doi: 10.1080/15381501.2020.1824843
5. Rouffiac, A-E, Whiteley, L, Brown, L, Mena, L, Craker, L, Healy, M, et al. A Mobile intervention to improve uptake of pre-exposure prophylaxis for southern black men who have sex with men: protocol for intervention development and pilot randomized controlled trial. JMIR Res Protoc. (2020) 9:e15781. doi: 10.2196/15781
6. CDC. (2024). Fast facts: HIV in the United States. Available online at: https://www.cdc.gov/hiv/data-research/facts-stats/index.html
7. CDC. (2021). Pre-exposure prophylaxis for the prevention of HIV infection in the United States – 2021 update: a clinical practice guideline. Available online at: https://stacks.cdc.gov/view/cdc/112360 (Accessed September 01, 2024).
8. Quinn, KG, Dickson-Gomez, J, Craig, A, John, SA, and Walsh, JL. Intersectional discrimination and PrEP use among Young black sexual minority individuals: the importance of black LGBTQ communities and social support. AIDS Behav. (2023) 27:290–302. doi: 10.1007/s10461-022-03763-w
9. AIDSVu. (2022) AIDSVu: location profile for the HIV epidemic in the Midwest. Location profile – AIDSVu. Available online at: https://map.aidsvu.org/profiles/region/midwest/overview
10. Mustanski, B, Morgan, E, D’Aquila, R, Birkett, M, Janulis, P, and Newcomb, ME. Individual and network factors associated with racial disparities in HIV among Young men who have sex with men: results from the RADAR cohort study. J Acquir Immune Defic Syndr. (2019) 80:24–30. doi: 10.1097/QAI.0000000000001886
11. State of Iowa Department of Health and Human Services. (2023). State of Iowa HIV disease end-of-year 2022 surveillance report. Available online at: https://publications.iowa.gov/id/eprint/47082 (Accessed September 13, 2024).
12. Badru, OA, and Adeagbo, OA. The perception of HIV self-testing and willingness to use mHealth for HIV prevention among black men who have sex with men in Iowa, United States: a qualitative study. Digit Health. (2024) 10:20552076241302250. doi: 10.1177/20552076241302250
13. Bowleg, L, Malekzadeh, AN, Mbaba, M, and Boone, CA. Ending the HIV epidemic for all, not just some: structural racism as a fundamental but overlooked social-structural determinant of the US HIV epidemic. Curr Opin HIV AIDS. (2022) 17:40–5. doi: 10.1097/COH.0000000000000724
14. Fauci, AS, Redfield, RR, Sigounas, G, Weahkee, MD, and Giroir, BP. Ending the HIV epidemic: a plan for the United States. JAMA. (2019) 321:844–5. doi: 10.1001/jama.2019.1343
15. Kim, JYH, Barth, SK, Monroe, AK, Ahsan, S, Kovacic, J, Senn, S, et al. The impact of COVID-19 on the HIV continuum of care: challenges, innovations, and opportunities. Expert Rev Anti-Infect Ther. (2023) 21:831–46. doi: 10.1080/14787210.2023.2239503
16. Nosyk, B, Fojo, AT, Kasaie, P, Enns, B, Trigg, L, Piske, M, et al. The testing imperative: why the US ending the human immunodeficiency virus (HIV) epidemic program needs to renew efforts to expand HIV testing in clinical and community-based settings. Clin Infect Dis. (2023) 76:2206–8. doi: 10.1093/cid/ciad103
17. Badru, O, Hlongwa, M, and Adeagbo, OA. Knowledge and awareness of pre-exposure prophylaxis among men in sub-Saharan Africa: a scoping review protocol. Health Sci Rep. (2025) 8:e70377. doi: 10.1002/hsr2.70377
18. Raymond, HF, Snowden, JM, Guigayoma, J, McFarland, W, and Chen, Y-H. Community levels of PrEP use among men who have sex with men by race/ethnicity, San Francisco, 2017. AIDS Behav. (2019) 23:2687–93. doi: 10.1007/s10461-019-02428-5
19. Dunville, R, Harper, C, Johns, MM, Heim Viox, M, Avripas, S, Fordyce, E, et al. Awareness and willingness to use biomedical prevention strategies for HIV among sexual and gender minority youth: results from a national survey. J Adolesc Health. (2021) 68:199–206. doi: 10.1016/j.jadohealth.2020.05.032
20. Harawa, NT, Schrode, KM, McWells, C, Weiss, RE, Hilliard, CL, and Bluthenthal, RN. Small randomized controlled trial of the new passport to wellness HIV prevention intervention for black men who have sex with men (BMSM). AIDS Educ Prev. (2020) 32:311–24. doi: 10.1521/aeap.2020.32.4.311
21. Jourdain, H, de Gage, SB, Desplas, D, and Dray-Spira, R. Real-world effectiveness of pre-exposure prophylaxis in men at high risk of HIV infection in France: a nested case-control study. Lancet Public Health. (2022) 7:e529–36. doi: 10.1016/S2468-2667(22)00106-2
22. Adeagbo, O, Harrison, S, Qiao, S, and Li, X. Pre-exposure prophylaxis (PrEP) uptake among black men who have sex with men (BMSM) in the southern U.S. Int J Environ Res Public Health. (2021) 18:9715. doi: 10.3390/ijerph18189715
23. CDC. (2023) Monitoring selected national HIV prevention and care objectives by using HIV surveillance data United States and 6 dependent areas, 2021. Available online at: https://www.cdc.gov/hiv/library/reports/hiv-surveillance/vol-28-no-4/index.html
24. Schuyler, A, Alidina, Z, Dolcini, MM, Harper, G, Fortenberry, JD, Singh, R, et al. Pre-exposure prophylaxis (PrEP) dissemination: adapting diffusion theory to examine PrEP adoption. AIDS Behav. (2021) 25:3145–58. doi: 10.1007/s10461-021-03345-2
25. Seyedroudbari, S, Ghadimi, F, Grady, G, Uzosike, O, Nkwihoreze, H, Jemmott, JB, et al. Assessing structural racism and discrimination along the pre-exposure prophylaxis continuum: a systematic review. AIDS Behav. (2024) 28:3001–37. doi: 10.1007/s10461-024-04387-y
26. Kerzner, M, De, AK, Yee, R, Keating, R, Djomand, G, Stash, S, et al. Pre-exposure prophylaxis (PrEP) uptake and service delivery adaptations during the first wave of the COVID-19 pandemic in 21 PEPFAR-funded countries. PLoS One. (2022) 17:e0266280. doi: 10.1371/journal.pone.0266280
27. Koppe, U, Marcus, U, Albrecht, S, Jansen, K, Jessen, H, Gunsenheimer-Bartmeyer, B, et al. Barriers to using HIV pre-exposure prophylaxis (PrEP) and sexual behaviour after stopping PrEP: a cross-sectional study in Germany. BMC Public Health. (2021) 21:159. doi: 10.1186/s12889-021-10174-4
28. Dang, M, Scheim, AI, Teti, M, Quinn, KG, Zarwell, M, Petroll, AE, et al. Barriers and facilitators to HIV pre-exposure prophylaxis uptake, adherence, and persistence among transgender populations in the United States: a systematic review. AIDS Patient Care STDs. (2022) 36:236–48. doi: 10.1089/apc.2021.0236
29. Garrison, LE, and Haberer, JE. Pre-exposure prophylaxis uptake, adherence, and persistence: a narrative review of interventions in the U.S. Am J Prev Med. (2021) 61:S73–86. doi: 10.1016/j.amepre.2021.04.036
30. Mayer, KH, Agwu, A, and Malebranche, D. Barriers to the wider use of pre-exposure prophylaxis in the United States: a narrative review. Adv Ther. (2020) 37:1778–811. doi: 10.1007/s12325-020-01295-0
31. AIDSVu. (2022) Understanding the current HIV epidemic in the Midwest. Location profile – AIDSVu. Available online at: https://map.aidsvu.org/profiles/region/midwest/overview
32. AIDSVu. (2022). AIDSVu releases new data showing significant inequities in PrEP use among black and Hispanic Americans. Available online at: https://aidsvu.org/prep-use-race-ethnicity-launch-22/
33. Moher, D, Shamseer, L, Clarke, M, Ghersi, D, Liberati, A, Petticrew, M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. (2015) 4:148–60. doi: 10.1186/2046-4053-4-1
34. Eldawlatly, A, Alshehri, H, Alqahtani, A, Ahmad, A, Al-Dammas, F, and Marzouk, A. Appearance of population, intervention, comparison, and outcome as research question in the title of articles of three different anesthesia journals: a pilot study. Saudi J Anaesth. (2018) 12:283. doi: 10.4103/SJA.SJA_767_17
35. Ouzzani, M, Hammady, H, Fedorowicz, Z, and Elmagarmid, A. Rayyan—a web and mobile app for systematic reviews. Syst Rev. (2016) 5:1–10. doi: 10.1186/S13643-016-0384-4
36. Biello, KB, Hosek, S, Drucker, MT, Belzer, M, Mimiaga, MJ, Marrow, E, et al. Preferences for injectable PrEP among Young U.S. cisgender men and transgender women and men who have sex with men. Arch Sex Behav. (2018) 47:2101–7. doi: 10.1007/s10508-017-1049-7
37. Hall, C, Bundy, C, Foran, J, Newcomb, M, Carrillo, H, Watkins-Hayes, C, et al. Identifying strategies for improving pre-exposure prophylaxis adherence: perspectives from a sample of highly adherent Young men who have sex with men. AIDS Behav. (2023) 27:506–17. doi: 10.1007/s10461-022-03785-4
38. Khanna, AS, Michaels, S, Skaathun, B, Morgan, E, Green, K, Young, L, et al. Preexposure prophylaxis awareness and use in a population-based sample of young black men who have sex with men. JAMA Intern Med. (2016) 176:136–8. doi: 10.1001/jamainternmed.2015.6536
39. Khanna, AS, Schumm, P, and Schneider, JA. A comparison of temporal Facebook networks of young men who have sex with men (MSM), differentiated by awareness and use of preexposure prophylaxis (PrEP). Ann Epidemiol. (2017) 27:176–80. doi: 10.1016/j.annepidem.2016.11.006
40. Lancki, N, Almirol, E, Alon, L, McNulty, M, and Schneider, JA. Preexposure prophylaxis guidelines have low sensitivity for identifying seroconverters in a sample of young black MSM in Chicago. AIDS. (2018) 32:383–92. doi: 10.1097/QAD.0000000000001710
41. Morgan, E, Moran, K, Ryan, DT, Mustanski, B, and Newcomb, ME. Threefold increase in PrEP uptake over time with high adherence among Young men who have sex with men in Chicago. AIDS Behav. (2018) 22:3637–44. doi: 10.1007/s10461-018-2122-5
42. Phillips, G II, Neray, B, Birkett, M, Felt, D, Janulis, P, and Mustanski, B. Role of social and sexual network factors in PrEP utilization among YMSM and transgender women in Chicago. Prev Sci. (2019) 20:1089–97. doi: 10.1007/s11121-019-00995-6
43. Schneider, JA, Young, L, Ramachandran, A, Michaels, S, Cohen, H, Robinson, I, et al. A pragmatic randomized controlled trial to increase PrEP uptake for HIV prevention: 55-week results from PrEPChicago. J Acquir Immune Defic Syndr. (2021) 86:31–7. doi: 10.1097/QAI.0000000000002518
44. Schueler, K, Ferreira, M, Nikolopoulos, G, Skaathun, B, Paraskevis, D, Hatzakis, A, et al. Pre-exposure prophylaxis (PrEP) awareness and use within high HIV transmission networks. AIDS Behav. (2019) 23:1893–903. doi: 10.1007/s10461-019-02411-0
45. Timmins, L, Schneider, JA, Chen, Y-T, Goedel, WC, Brewer, R, Callander, D, et al. Sexual identity, sexual behavior and pre-exposure prophylaxis in black cisgender sexual minority men: the N2 cohort study in Chicago. AIDS Behav. (2021) 25:3327–36. doi: 10.1007/s10461-021-03246-4
46. Young, LE, Schumm, P, Alon, L, Bouris, A, Ferreira, M, Hill, B, et al. PrEP Chicago: a randomized controlled peer change agent intervention to promote the adoption of pre-exposure prophylaxis for HIV prevention among young black men who have sex with men. Clin Trials. (2018) 15:44–52. doi: 10.1177/1740774517730012
47. Downing, MJ, Wiatrek, SE, Zahn, RJ, Mansergh, G, Olansky, E, Gelaude, D, et al. Video selection and assessment for an app-based HIV prevention messaging intervention: formative research. mHealth. (2023) 9:53. doi: 10.21037/mhealth-21-53
48. Patel, RR, Crane, JS, López, J, Chan, PA, Liu, AY, Tooba, R, et al. Pre-exposure prophylaxis for HIV prevention preferences among young adult African American men who have sex with men. PLoS One. (2018) 13:9484. doi: 10.1371/journal.pone.0209484
49. Kelly, JA, Amirkhanian, YA, Walsh, JL, Brown, KD, Quinn, KG, Petroll, AE, et al. Social network intervention to increase pre-exposure prophylaxis (PrEP) awareness, interest, and use among African American men who have sex with men. AIDS Care. (2020) 32:40–6. doi: 10.1080/09540121.2020.1739207
50. Quinn, K, Bowleg, L, and Dickson-Gomez, J. “The fear of being black plus the fear of being gay”: the effects of intersectional stigma on PrEP use among young black gay, bisexual, and other men who have sex with men. Soc Sci Med. (2019) 232:86–93. doi: 10.1016/j.socscimed.2019.04.042
51. Quinn, KG, Christenson, E, Spector, A, Amirkhanian, Y, and Kelly, JA. The influence of peers on PrEP perceptions and use among young black gay, bisexual, and other men who have sex with men: a qualitative examination. Arch Sex Behav. (2020) 49:2129–43. doi: 10.1007/s10508-019-01593-x
52. Quinn, KG, Christenson, E, Sawkin, MT, Hacker, E, and Walsh, JL. The unanticipated benefits of PrEP for young black gay, bisexual, and other men who have sex with men. AIDS Behav. (2020) 24:1376–88. doi: 10.1007/s10461-019-02747-7
53. Quinn, KG, Zarwell, M, John, SA, Christenson, E, and Walsh, JL. Perceptions of PrEP use within primary relationships among young black gay, bisexual, and other men who have sex with men. Arch Sex Behav. (2020) 49:2117–28. doi: 10.1007/s10508-020-01683-1
54. Coukan, F, Murray, K-K, Papageorgiou, V, Lound, A, Saunders, J, Atchison, C, et al. Barriers and facilitators to HIV pre-exposure prophylaxis (PrEP) in specialist sexual health Services in the United Kingdom: a systematic review using the PrEP care continuum. HIV Med. (2023) 24:893–913. doi: 10.1111/hiv.13492
55. Pleuhs, B, Quinn, KG, Walsh, JL, Petroll, AE, and John, SA. Health care provider barriers to HIV pre-exposure prophylaxis in the United States: a systematic review. AIDS Patient Care STDs. (2020) 34:111–23. doi: 10.1089/apc.2019.0189
56. Zhang, HL, Rhea, SK, Hurt, CB, Mobley, VL, Swygard, H, Seña, AC, et al. HIV Preexposure prophylaxis implementation at local health departments: a statewide assessment of activities and barriers. J Acquir Immune Defic Syndr. (2018) 77:72–7. doi: 10.1097/QAI.0000000000001546
57. Adeagbo, O. Barriers and facilitators to pre-exposure prophylaxis uptake among Black/African American men who have sex with other men in Iowa: COM-B model analysis. Ther Adv Infect Dis. (2024) 11:20499361241267151. doi: 10.1177/20499361241267151
58. Chasco, EE, Shafer, C, Dillon, DMB, Owens, S, Ohl, ME, and Hoth, AB. Bringing Iowa TelePrEP to scale: a qualitative evaluation. Am J Prev Med. (2021) 61:S108–17. doi: 10.1016/j.amepre.2021.05.040
59. Bonacci, RA, Smith, DK, and Ojikutu, BO. Toward greater pre-exposure prophylaxis equity: increasing provision and uptake for Black and Hispanic/Latino individuals in the U.S. Am J Prev Med. (2021) 61:S60–72. doi: 10.1016/j.amepre.2021.05.027
60. García, MC, Duong, QL, Meyer, SB, and Ward, PR. Multiple and concurrent sexual partnerships among men who have sex with men in Viet Nam: results from a National Internet-based Cross-sectional Survey. Health Promot Int. (2016) 31:dau097–143. doi: 10.1093/heapro/dau097
61. Pines, HA, Karris, MY, and Little, SJ. Sexual partner concurrency among partners reported by MSM with recent HIV infection. AIDS Behav. (2017) 21:3026–34. doi: 10.1007/s10461-017-1855-x
62. Ware, NC, Wyatt, MA, Haberer, JE, Baeten, JM, Kintu, A, Psaros, C, et al. What’s love got to do with it? Explaining adherence to Oral antiretroviral pre-exposure prophylaxis for HIV-Serodiscordant couples. J Acquir Immune Defic Syndr. (2012) 59:463–8. doi: 10.1097/QAI.0b013e31824a060b
63. Kahle, EM, Sharma, A, Sullivan, S, and Stephenson, R. The influence of relationship dynamics and sexual agreements on perceived partner support and benefit of PrEP use among same-sex male couples in the U.S. AIDS Behav. (2020) 24:2169–77. doi: 10.1007/s10461-020-02782-9
Keywords: PrEP, barriers, facilitators, African American, Black, MSM, Midwest, United States
Citation: Adeagbo O, Badru OA, Addo P, Hawkins A, Brown MJ, Li X and Afifi R (2025) Pre-exposure prophylaxis uptake among Black/African American men who have sex with other men in Midwestern, United States: a systematic review. Front. Public Health. 13:1510391. doi: 10.3389/fpubh.2025.1510391
Edited by:
Kimberly A. Koester, University of California, San Francisco, United StatesReviewed by:
Ryan Whitacre, Public Health Institute, United StatesCopyright © 2025 Adeagbo, Badru, Addo, Hawkins, Brown, Li and Afifi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Oluwafemi Adeagbo, b2x1d2FmZW1pLWFkZWFnYm9AdWlvd2EuZWR1
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.