 Xia Li1,2†
Xia Li1,2† Jiahe Liu3†
Jiahe Liu3† Yanling Hu1,2Xi Huang1,2
Yanling Hu1,2Xi Huang1,2 Yingxin Li1,2
Yingxin Li1,2 Yuan Li1,2
Yuan Li1,2 Zeyao Shi1,2
Zeyao Shi1,2 Ru Yang1,2Hanmei Peng1,2Sisi Ma4
Ru Yang1,2Hanmei Peng1,2Sisi Ma4 Xingli Wan2,5*Wei Peng6,7*
Xingli Wan2,5*Wei Peng6,7*- 1Department of Neonatology Nursing, West China Second University Hospital, Sichuan University, Chengdu, China
- 2Key Laboratory of Birth Defects and Related Diseases of Women and Children, Ministry of Education, Sichuan University, Chengdu, China
- 3School of Mathematics and Statistics, University of Melbourne, Parkville, VIC, Australia
- 4Department of Health Policy and Management, West China School of Public Health and West China Fourth Hospital, Sichuan University, Chengdu, China
- 5Department of Nursing, West China Second University Hospital, Sichuan University, Chengdu, China
- 6Department of Oncology, West China School of Public Health and West China Fourth Hospital, Sichuan University, Chengdu, China
- 7Research Center for Palliative Care, West China-PUMC C.C. Chen Institute of Health, Sichuan University, Chengdu, China
Background: Suicide is a major behavioral issue among children and adolescents, and family functioning potentially influencing its occurrence. Furthermore, positive behavior recognition, as a key component of positive youth development, may act as a mediating factor in the relationship between family functioning and suicide. Non-suicidal self-injury (NSSI) often co-occurs with suicide and may also mediate the impact of family functioning on suicide. Therefore, the aim of this study is to examine the role of family functioning in child and adolescent suicide, with positive behavior recognition and NSSI serving as sequential mediating factors.
Methods: The participants in this study were recruited from the Chengdu Positive Child Development (CPCD) cohort study. The analysis was based on the second round of cross-sectional data from the CPCD cohort. They were required to complete questionnaires that included measures of family functioning, suicide, positive behavior recognition, and NSSI. SPSS 26.0 and Mplus 8.3 were used for descriptive statistical analysis, correlation analysis and mediation effect analysis.
Results: A total of 8,124 participants completed the questionnaires, with an average age of 11.00 ± 2.18 years. The sample comprised 4,195 male and 3,929 female participants. The findings indicate that 17.93% of children and adolescents reported suicide thoughts, 10.06% had formulated suicide plans, and 8.64% had attempted suicide. Poor family functioning shows a significant positive correlation with suicide (r = 0.322, p < 0.01). The multiple mediation effect of positive behavior recognition and NSSI in the association between family functioning and suicide was statistically significant (β = 0.034, 95% CI = 0.027, 0.042).
Conclusion: This study found that poor family functioning is a risk factor for suicide in children and adolescents, with positive behavior recognition and non-suicidal self-injury acting as sequential mediating factors.
1 Introduction
Suicide is a major behavioral concern among children and adolescents. According to data from the World Health Organization (WHO), approximately 703,000 people die by suicide globally each year. In 2019, suicide accounted for 1.3% of all deaths, with a global suicide rate of 9 per 100,000 people. Suicide is the fourth leading cause of death among adolescents aged 15–19. The incidence of suicide attempts among preadolescents under the age of 13 is 2.56%. The lifetime suicide mortality rate in the general population was 7.9 per 100,000 children (1). Currently, mental health is a significant issue for children and adolescents in China. The unique familial and societal pressures faced by Chinese youth, including academic stress and youth unemployment, may contribute to their higher mortality rates compared to those in developed countries (2). In China, the incidence of suicide attempts among children and adolescents under the age of 18 is 3.5%, while the incidence of suicide planning is 6.4% (3).
Family functioning plays a crucial role in the physical and psychological development of children and adolescents. According to family systems theory, individuals with better family functioning tend to have fewer emotional and behavioral issues (4, 5). Prior research has identified family functioning as a potential predictor of suicidal behavior (6–9). Moreover, studies have shown that family functioning influences suicidal behavior both directly and indirectly through mediating factors such as hopelessness, depression, acceptance, and a sense of defeat (7–9).
Positive behavior recognition may have a potential association with family functioning. In recent decades, researchers have gradually shifted their focus in youth development from a “deficit-based” approach to a “positive youth development” approach. The deficit-based approach emphasizes correcting behavioral problems in adolescents, often neglecting their developmental potential, whereas positive youth development focuses on nurturing the assets, abilities, and potential of young people (10, 11). Positive behavior recognition refers to the practice of identifying, acknowledging, and reinforcing desirable behaviors in individuals, and is a key construct in positive youth development (12). Positive behavior recognition seeks to reinforce and sustain desirable behaviors by acknowledging and rewarding them (12, 13). Previous research indicates that rewards are generally perceived as more effective than punishments in fostering positive behavior and enhancing performance among Chinese adolescents (14). Family members play a crucial role in providing positive behavior recognition. Thus, we hypothesize that positive behavior recognition may mediate the relationship between family functioning and suicide.
Self-injurious behaviors are actions that cause deliberate harm to oneself, including non-suicidal self-injury (NSSI), suicidal behavior (15). NSSI is closely related to suicidal behavior. Although suicidal thoughts and behaviors frequently co-occur with self-injury, their underlying causes may differ. Previous studies have established a connection between family functioning and NSSI (16). Therefore, this study hypothesizes that NSSI may also mediate the impact of family functioning on suicide.
Thus, this study will examine the role of family functioning in children and adolescents’ suicide, with positive behavior recognition and NSSI serving as mediating factors (Figure 1). In this study, we aimed to conduct a sequential mediation analysis to examine the interrelationships among family functioning, positive behavior recognition, NSSI, and suicide, with the goal of identifying potential pathways for suicide prevention.
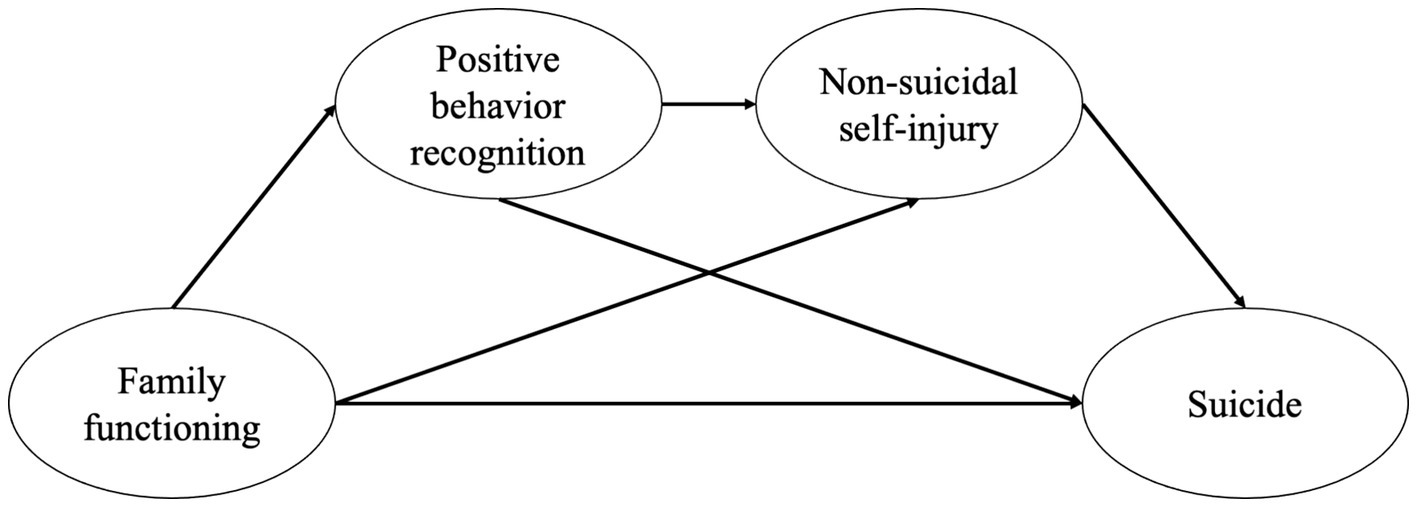
Figure 1. Hypothetical model of the associations among family functioning, suicide, positive behavior recognition, and non-suicidal self-injury.
The hypotheses of this study are as follows:
Hypothesis 1: There is a correlation between family functioning and suicide in children and adolescents.
Hypothesis 2: Family functioning affects suicide in children and adolescents, with positive behavior recognition serving as a mediating factor.
Hypothesis 3: Family functioning affects suicide in children and adolescents, with non-suicidal self-injury serving as a mediating factor.
Hypothesis 4: Family functioning affects suicide in children and adolescents, with positive behavior recognition and non-suicidal self-injury acting as sequential mediators.
2 Materials and methods
2.1 Participants
The participants in this study were recruited from the Chengdu Positive Child Development (CPCD) cohort study, which has been conducted in Chengdu, the capital of Sichuan province, China, since December 2019. The CPCD study, approved by the Medical Ethics Committee of Sichuan University (K2020025), originally aimed to understand the current state of positive development in children and adolescents, as well as psychosocial and behavioral problems, and to evaluate the effects of Positive Child Development program in promoting positive development and addressing psychological and behavioral issues (17). The first round of surveys for the CPCD study was conducted from December 2019 to January 2020, with the second round taking place from June to July 2020. This cohort study utilized cluster sampling to recruit students from Grades 1 through 9 (ages 6–16) across five primary and secondary schools. These schools were distributed as follows: one in downtown Chengdu, two in the southern suburbs, and two in the northern suburbs. Before participation, written informed consent was given by the students’ legal guardians. This included a project overview, survey procedures, potential benefits and risks and confidentiality agreement. All students provided written informed consent before participating. For this mediation analysis, we utilized data from the second round of the survey.
2.2 Data collection
Trained investigators distributed the questionnaires to participants in the classrooms. Before filling out the questionnaires, participants received detailed instructions. They were allowed to ask questions before starting, with investigators providing clarification, but no discussion among participants was permitted during the completion process. The investigators monitored the participants to ensure the questionnaires were completed independently. They also assured participants of the anonymity of the questionnaires to reduce any anxiety or reluctance they may have felt. Participants were allotted 40 to 60 min to complete the questionnaires, and early submission was not allowed to ensure that all responses were fully completed. The questionnaire included several negatively scored items to ensure logical consistency. Any questionnaires with clear logical inconsistencies were excluded from the analysis.
2.3 Measures
2.3.1 Family functioning
Family functioning was assessed using the Chinese Family Assessment Instrument (C-FAI), which has demonstrated strong psychometric properties in previous studies (18, 19). The C-FAI consists of 33 items that evaluate five dimensions of family functioning: “communication” (9 items), “mutuality” (12 items), “parental concern” (3 items), “parental control” (3 items), and “conflict and harmony” (6 items). All items were rated on a 5-point Likert scale, with 1 indicating the highest level of agreement and 5 indicating the highest level of disagreement. A higher total score reflects poorer family functioning.
2.3.2 Suicide
Suicide was assessed using three questions: “Have you ever seriously considered trying to commit suicide?” (suicide thought), “Have you made any specific plan to commit suicide?” (suicide plan), and “How many times have you tried to commit suicide?” (suicide attempt) (17). Participants were asked to report how often they experienced each behavior on a 4-point Likert scale: never, 1 time, 2 times, or 3 or more times.
2.3.3 Positive behaviors recognition
Positive behaviors recognition was assessed using a subscale of the Chinese Positive Youth Development Scale (CPYDS), a comprehensive self-report instrument consisting of 80 items across 15 subscales. These subscales include bonding, resilience, social competence, emotional competence, cognitive competence, behavioral competence, moral competence, self-determination, self-efficacy, clear and positive identity, beliefs in the future, prosocial involvement, prosocial norms, spirituality, and positive behavior recognition. The positive behavior recognition subscale includes four items, each rated on a six-point scale: 1 (strongly disagree), 2 (relatively disagree), 3 (slightly disagree), 4 (slightly agree), 5 (moderately agree), and 6 (strongly agree). Higher scores on this scale reflect a greater recognition of positive behaviors. Previous studies demonstrated that the scale has good validity and reliability (10, 20).
2.3.4 Non-suicidal self-injuries
We used the Chinese version of the Deliberate Self-Harm Inventory (DSHI) to assess non-suicidal self-injury (NSSI) behaviors, which was developed and validated by Gratz (21), and later simplified and shortened by Lundh et al. (22). Nine items related to intentional self-harm behaviors without suicidal intent, such as cutting, burning, scratching, biting, and punching, were measured. Participants were asked to report the frequency of these behaviors using a 4-point Likert scale (Never, 1 time, 2 times, and 3 or more times) for each question. A previous study demonstrated that the scale has good test–retest reliability and validity (21, 23). The Chinese version of the DSHI has also been shown to have good reliability and validity and has been applied to children and adolescents in China (24).
2.4 Statistical analysis
Statistical analyses were performed using SPSS 26.0 and Mplus 8.3. Missing data were imputed using multiple imputation methods. Descriptive statistics for continuous variables are presented as means and standard deviations (SD), whereas categorical variables are reported as frequencies and proportions. SPSS was used to analyze common method bias and the correlation between variables, while Mplus was utilized for mediation effect analysis. Bootstrapping, a non-parametric resampling procedure, was utilized in this study due to its advantage of not requiring the assumption of normality in the sampling distribution. This method involves repeatedly sampling from the dataset to estimate the effect in each resampled dataset. By performing 5,000 resampling iterations, we generated an empirical approximation of the sampling distribution for the effect of the independent variable on the dependent variable through potential mediators (25, 26). Direct, indirect, and total effects were calculated. Given that the data in this study were self-reported, common method bias may be present. To assess this, Harman’s single-factor test was conducted. A two-sided p-value of <0.05 was considered statistically significant.
3 Results
3.1 Common method bias
Harman’s single-factor test results indicated that 12 factors with eigenvalues greater than 1 were identified, with the first factor accounting for 29.203% of the variance (less than 40%). This suggests that common method bias did not affect the results of this study.
3.2 Characteristics and descriptive results
In the second round of data collection, a total of 8,124 questionnaires were completed. Compared to the first round, 701 participants, mostly Grade 9 students, who were unable to participate due to their high school entrance exam preparations, were lost to follow-up. The response rate was 92.06%. The participants had a mean age of 11.00 ± 2.18 years, consisting of 4,195 males and 3,929 females. The findings indicate that 17.93% of children and adolescents reported suicide thoughts, 10.06% had formulated suicide plans, and 8.64% had attempted suicide. Table 1 presents the characteristics and the descriptive results.
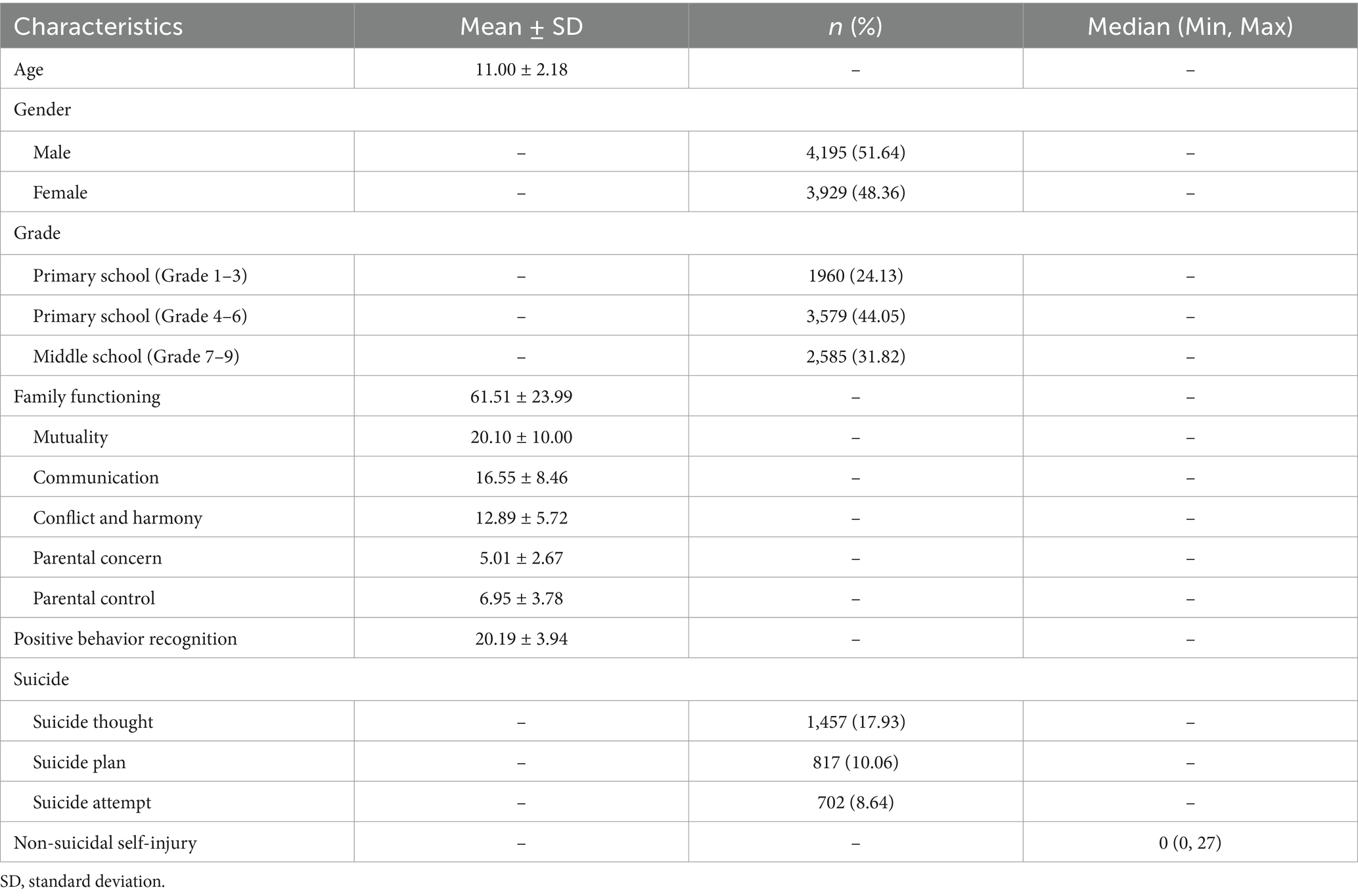
Table 1. The characteristics and descriptive results (n = 8,124).
3.3 Correlation among variables
Table 2 presents the correlations between variables. Gender and age were included in the analysis to account for their potential influence on the measured variables. The results reveal that gender and age are significantly related to positive behavior recognition, NSSI, suicide, and poor family functioning. Poor family functioning shows a significant positive correlation with both suicide and NSSI (r = 0.322, r = 0.331, p < 0.01, respectively), and a significant negative correlation with positive behavior recognition (r = −0.368, p < 0.01). Suicide is significantly positively correlated with NSSI (r = 0.692, p < 0.01) and significantly negatively correlated with positive behavior recognition (r = −0.250, p < 0.01). Moreover, positive behavior recognition is significantly negatively correlated with NSSI (r = −0.250, p < 0.01). The relationships between the scores of the five dimensions (mutuality, communication, conflict and harmony, parental concern, parental control) of family functioning assessed by the C-FAI and positive behavior recognition, suicide, and NSSI mirrored the patterns observed between the C-FAI total score and these variables.
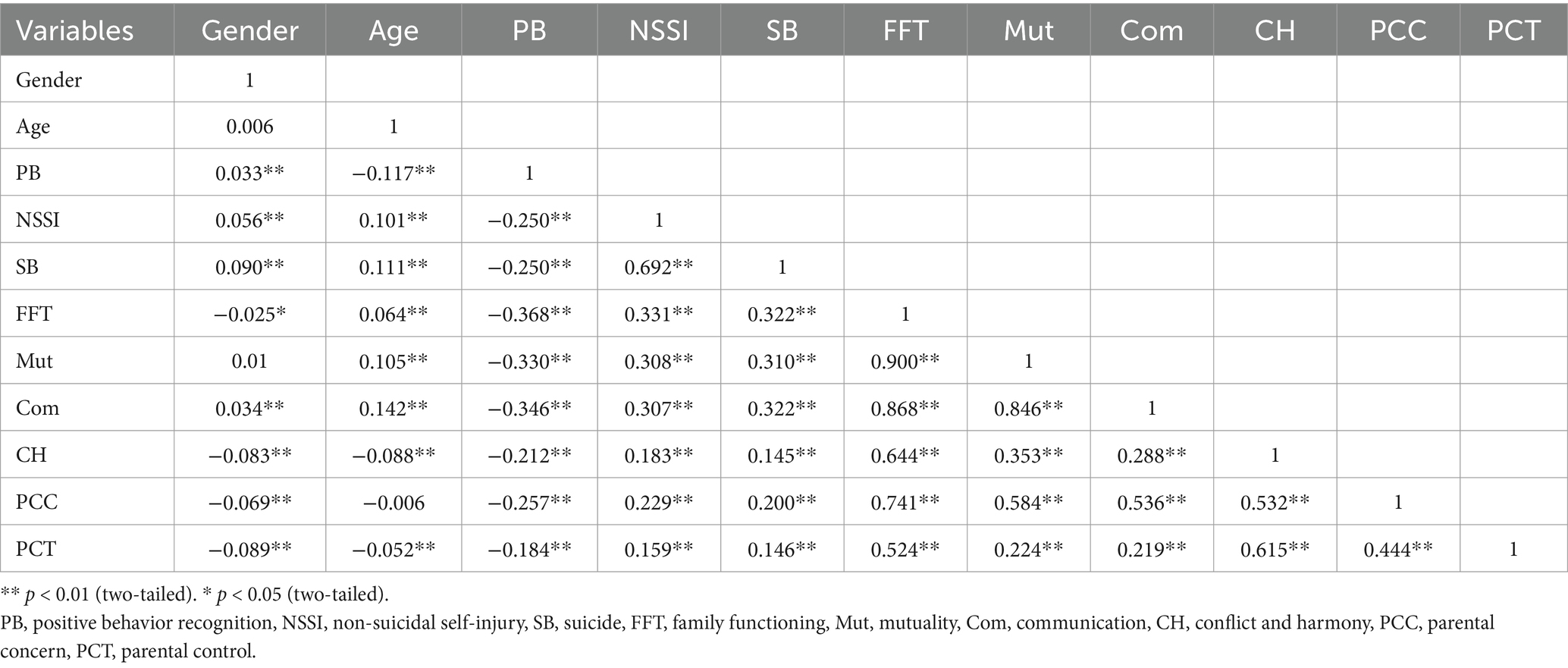
Table 2. The correlation analysis of family functioning, suicide, the positive behavior recognition, and non-suicidal self-injury.
3.4 Testing of mediation effects
Mediation analysis was conducted, with age and gender included as control variables. Family functioning was the independent variable, suicide was the dependent variable, and positive behavior recognition and NSSI acted as mediators. The path coefficient results are presented in Figure 2. The mediation analysis revealed that positive behavior recognition significantly mediated the relationship between family functioning and suicide (β = 0.021, 95% CI = 0.013, 0.028). Similarly, NSSI was found to mediate this relationship (β = 0.166, 95% CI = 0.149, 0.184). Moreover, the multiple mediation effect of positive behavior recognition and NSSI was significant (β = 0.034, 95% CI = 0.027, 0.042). In total, the indirect effects accounted for 75.17% of the total effect (Table 3).
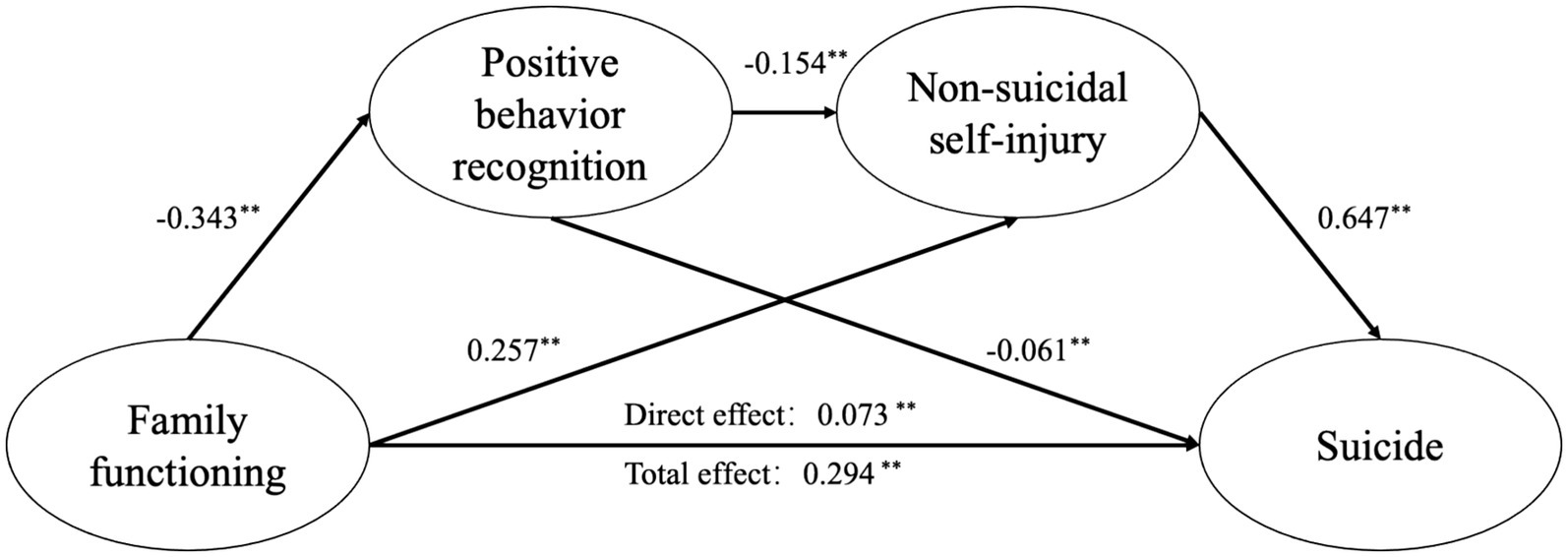
Figure 2. Mediation model of the positive behavior recognition and non-suicidal self-injury on path from family functioning to suicide. ** p < 0.001 (two-tailed), adjusting for age, gender.
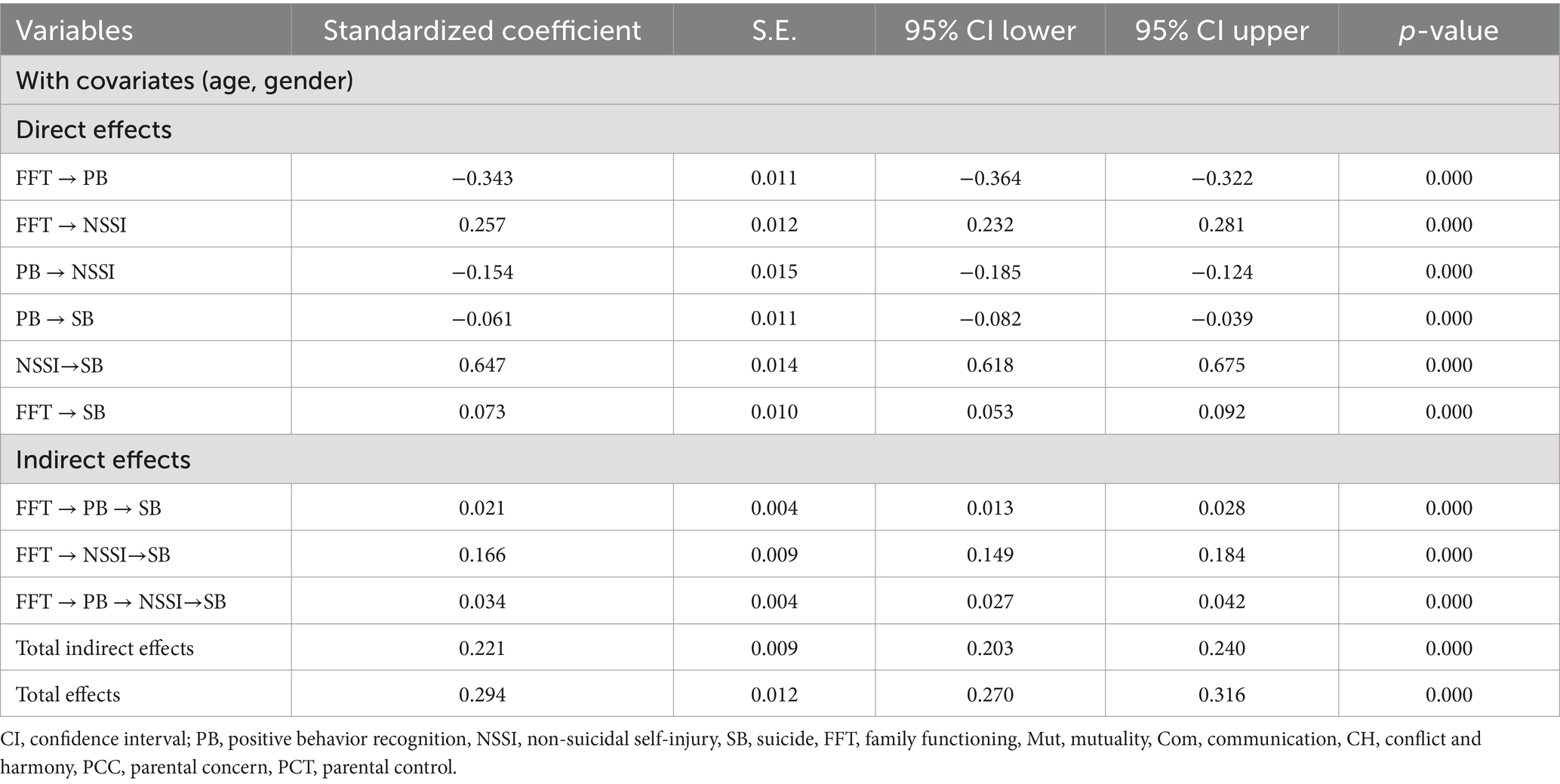
Table 3. Results of mediation analysis with covariates (n = 8,124).
4 Discussion
The findings of this study reveal a positive association between poor family functioning and suicide in children and adolescents. Specifically, a poor family functioning is linked to an increased likelihood of suicide among this population, thereby supporting Hypothesis 1 (H1). These findings are consistent with those of previous studies (4, 7–9, 27). Based on the correlation analysis, the scores for the five dimensions of family functioning (mutuality, communication, conflict and harmony, parental concern) were all significantly positively associated with suicide. Additionally, Alvarez-Subiela et al. identified specific family factors influencing suicide, including negligence, affectionless control, insecure attachment, and stressful life events as risk factors, while parental care and security serve as protective factors for adolescent suicide (6). This indicates that family interventions could serve as potential strategies for suicide prevention. Enhancing family functioning through improved communication and mutual care among family members may help prevent suicide in children and adolescents. It is also noteworthy that discrepancies exist between children’s and adolescents’ self-reports of family functioning and their parents’ reports (28). Children and adolescents generally report poorer family functioning than their parents do (28). In this study, we used data from the children’s self-reports to avoid any potential misestimation of the relationship between family functioning and suicide that might result from using parental reports.
Family functioning not only directly impacts suicide but also influences it through mediating factors such as hopelessness, depression, acceptance, and so on. This study demonstrates that positive behavior recognition serves as a mediating factor in the relationship between family functioning and suicide, supporting Hypothesis 2 (H2). The goal of recognizing positive behavior is to reward and acknowledge such actions, thereby reinforcing the individual’s positive behaviors (12, 13). There is a negative correlation between poor family functioning and positive behavior recognition. In other words, better family functioning is associated with more effective recognition of positive behaviors. This may be related to the fact that recognition often comes from family members, and families with better functioning are more likely to offer such recognition (12). Additionally, positive behavior recognition has a negative impact on suicide, meaning that it serves as a protective factor against suicide. From a humanistic perspective, positive behavior is indicative of healthy human development. Positive behavior recognition may foster positive youth development by encouraging the maintenance of constructive behaviors, thereby reducing negative behaviors such as suicide and self-injury. The indirect pathway “family functioning → positive behavior recognition → suicide” is established. Specifically, family functioning indirectly affects the risk of suicide through its impact on positive behavior recognition.
This study also confirms that NSSI mediates the relationship between family functioning and suicide, supporting Hypothesis 3 (H3). Previous research has established the influence of family functioning on self-injurious behavior (16, 29–34). Specifically, aspects such as family intimacy and adaptability, the family environment, and family conflict have been found to significantly impact self-injurious behavior (30, 32). The connection between self-injury and suicide is particularly strong. Self-injurious behaviors refer to actions that deliberately inflict harm on oneself (15, 35). NSSI is defined as the intentional destruction or alteration of bodily tissue without suicidal intent, and includes behaviors such as cutting, head banging, burning, hitting oneself, scratching to the point of bleeding, and interfering with wound healing (36, 37). Suicidal behaviors, on the other hand, are self-injurious actions carried out with the intent to end one’s life, such as hanging/strangulation, severe cutting, or jumping from a height (37, 38). Suicidal thoughts refer to the contemplation or planning of actions aimed at ending one’s life (i.e., suicidal ideation or plan) (37). While suicidal behavior and NSSI differ in terms of intent, frequency, and lethality, these behaviors often co-occur (15). Some studies suggest that NSSI or self-harm is a risk factor for suicidal behavior (39–41) and may also serve as a precursor to suicidal behavior (42, 43). The findings of this study confirm that NSSI mediates the pathway between family functioning and suicide, indicating that family functioning indirectly influences suicide through NSSI. Several intervention programs aimed at preventing NSSI have been reported (44–46), suggesting that targeting NSSI prevention may serve as an effective intervention strategy to reduce the risk of suicide.
Research on the link between positive behavior recognition and NSSI is scarce. Nonetheless, the correlation analysis conducted in this study demonstrates a significant negative relationship between positive behavior recognition and NSSI, suggesting that improved positive behavior recognition is associated with a reduced risk of NSSI. Additional analyses using data from this cohort show a significant negative correlation between positive youth development and NSSI, with NSSI potentially serving as a predictor of positive youth development (47). Given that positive behavior recognition is an integral component of positive youth development, the observed correlation between positive behavior recognition and NSSI can be interpreted within this context. Positive behavior recognition and NSSI function as sequential mediators in the pathway from family functioning to suicide. The mediation effect is confirmed, supporting Hypothesis 4 (H4). Theoretically, targeting any point within the mediation pathways could impact suicide outcomes. The demonstration of sequential mediation highlights potential intervention targets for addressing suicide.
The findings of this study highlight the importance of focusing on children and adolescents experiencing poor family functioning, as this group is at a higher risk for suicide. Additionally, suicide prevention efforts should emphasize comprehensive interventions that strengthen family functioning and promote positive behavior recognition. Given China’s family-centered cultural context, family-based interventions should be a core component of suicide prevention efforts, as families play a pivotal protective role in safeguarding the mental health and well-being of children and adolescents. Moreover, the results indicate that the mediating effect of NSSI represents the largest proportion of the total effect, suggesting that NSSI may serve as a key mediator that requires focused attention. Furthermore, this study utilized self-reported data from participants, which may not fully capture or distinguish between NSSI and suicide, given the potential overlap between these behaviors. As a result, there may be an overestimation of the mediating effect of NSSI in the association between family functioning and suicide. Therefore, caution is warranted in the interpretation of these findings.
An additional point to note is that the second round of data used in this study (collected in June–July 2020) coincided with the COVID-19 pandemic. Given the significant stressors related to the pandemic, such as lockdown measures, heightened family stress, and alterations in social interactions, it is likely that family functioning and mental health were affected. Consequently, the study’s findings may differ in non-pandemic situations, suggesting that these results should be interpreted with caution.
5 Limitations
This study utilized data from round 2 of the CPCD cohort study for analysis but did not conduct a longitudinal analysis of the results from rounds 1 and 2. Consequently, no conclusions can be drawn about the longitudinal relationship between family functioning and suicide. The CPCD cohort is still ongoing, and it is anticipated that future longitudinal analyses will offer evidence regarding the relationship between family functioning and suicide. Additionally, when examining the impact of family functioning on suicide, there may be other potential confounding variables (e.g., mental health status, family history of mental disorders) beyond age and gender that could be relevant. This study did not account for these factors, and their influence on the results should be considered.
6 Conclusion
Among children and adolescents, family functioning has a significant impact on suicide, both directly and indirectly. Positive behavior recognition and NSSI serve as mediators, with both individual and sequential mediation effects being confirmed. Considering the substantial influence of family functioning on suicide, we emphasize the importance of family-based interventions in suicide prevention for children and adolescents. The mechanisms underlying the influence of family functioning on suicide are complex, and, in addition to the known mediators, other potential mediators or moderators may exist and require further investigation.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the Medical Ethics Committee of Sichuan University. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
XL: Conceptualization, Data curation, Formal analysis, Writing – original draft. JL: Formal analysis, Writing – original draft. YH: Resources, Writing – review & editing. XH: Writing – review & editing, Investigation. YiL: Investigation, Writing – review & editing. YuL: Investigation, Writing – review & editing. ZS: Investigation, Writing – review & editing. RY: Investigation, Writing – review & editing. HP: Investigation, Writing – review & editing. SM: Investigation, Writing – review & editing. XW: Conceptualization, Resources, Supervision, Writing – review & editing. WP: Resources, Supervision, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This study was funded by the Study of Diet and Nutrition Assessment and Intervention Technology from Active Health and Aging Technologic Solutions Major Project of National Key R&D Program (2020YFC2006300), the International Institute of Spatial Lifecourse Epidemiology (ISLE), and the Hong Kong Polytechnic University (19H0642).
Acknowledgments
We thank all participants for providing their information.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. World Health Organization. Suicide worldwide in 2019: global health estimates. Geneva: World Health Organization. (2021).
2. Chen, TJ, Dong, B, Dong, Y, Li, J, Ma, Y, Liu, D, et al. Matching actions to needs: shifting policy responses to the changing health needs of Chinese children and adolescents. Lancet. (2024) 403:1808–20. doi: 10.1016/S0140-6736(23)02894-5
3. Chang, Q, Shi, Y, Yao, S, Ban, X, and Cai, Z. Prevalence of suicidal ideation, suicide plans, and suicide attempts among children and adolescents under 18 years of age in mainland China: a systematic review and Meta-analysis. Trauma Violence Abuse. (2024) 25:2090–102. doi: 10.1177/15248380231205828
4. Adams, DM, Overholser, JC, and Lehnert, KL. Perceived family functioning and adolescent suicidal behavior. J Am Acad Child Adolesc Psychiatry. (1994) 33:498–507. doi: 10.1097/00004583-199405000-00008
5. Beavers, R, and Hampson, RB. The Beavers systems model of family functioning. J Fam Ther. (2000) 22:128–43. doi: 10.1111/1467-6427.00143
6. Alvarez-Subiela, X, Castellano-Tejedor, C, Villar-Cabeza, F, Vila-Grifoll, M, and Palao-Vidal, D. Family factors related to suicidal behavior in adolescents. Int J Environ Res Public Health. (2022) 19:9892. doi: 10.3390/ijerph19169892
7. Kwok, SY. Perceived family functioning and suicidal ideation: hopelessness as mediator or moderator. Nurs Res. (2011) 60:422–9. doi: 10.1097/NNR.0b013e31823585d6
8. Peng, B, Hu, N, Guan, L, Chen, C, Chen, Z, and Yu, H. Family functioning and suicidal ideation in college students: a moderated mediation model of depression and acceptance. Front Public Health. (2023) 11:1137921. doi: 10.3389/fpubh.2023.1137921
9. Yang, Q, Hu, YQ, Zeng, ZH, Liu, SJ, Wu, T, and Zhang, GH. The relationship of family functioning and suicidal ideation among adolescents: the mediating role of defeat and the moderating role of meaning in life. Int J Environ Res Public Health. (2022) 19:15895. doi: 10.3390/ijerph192315895
10. Shek, DTL, Sin, AMH, and Lee, TY. The Chinese positive youth development scale: a validation study. Res Soc Work Pract. (2007) 17:380–91. doi: 10.1177/1049731506296196
11. Shek, DTL, Sun, RCF, and Merrick, J. Positive youth development constructs: conceptual review and application. ScientificWorldJournal. (2012) 2012:1–3. doi: 10.1100/2012/152923
12. Law, BM, Siu, AM, and Shek, DT. Recognition for positive behavior as a critical youth development construct: conceptual bases and implications on youth service development. Sci World J. (2012) 2012:809578:1–7. doi: 10.1100/2012/809578
13. Cheng, HC, Siu, AM, and Leung, MC. Recognition for positive behavior as a positive youth development construct: conceptual bases and implications for curriculum development. Int J Adolesc Med Health. (2006) 18:467–73. doi: 10.1515/IJAMH.2006.18.3.467
14. Wan, F, and Salili, F. Perceived effectiveness of reward and punishment strategies by Hong Kong secondary school students. Psychologia. (1996) 39:261–75.
15. Hamza, CA, Stewart, SL, and Willoughby, T. Examining the link between nonsuicidal self-injury and suicidal behavior: a review of the literature and an integrated model. Clin Psychol Rev. (2012) 32:482–95. doi: 10.1016/j.cpr.2012.05.003
16. Wang, Y, Luo, B, Hong, B, Yang, M, Zhao, L, and Jia, P. The relationship between family functioning and non-suicidal self-injury in adolescents: a structural equation modeling analysis. J Affect Disord. (2022) 309:193–200. doi: 10.1016/j.jad.2022.04.124
17. Zhao, L, Shek, DTL, Zou, K, Lei, Y, and Jia, P. Cohort profile: Chengdu positive child development (CPCD) survey. Int J Epidemiol. (2022) 51:e95–e107. doi: 10.1093/ije/dyab237
18. Shek, DTL, Leung, KH, Li, X, and Dou, D. Psychometric properties of the Chinese family assessment instrument: evidence from mainland China. Front Psychol. (2023) 14:1290224. doi: 10.3389/fpsyg.2023.1290224
19. Shek, DTL, and Ma, CMS. The Chinese family assessment instrument (C-FAI) hierarchical confirmatory factor analyses and factorial invariance. Res Soc Work Pract. (2010) 20:112–23. doi: 10.1177/1049731509355145
20. Zhu, X, Chu, CKM, Wu, X, and Shek, DTL. Validation of a Chinese positive youth development scale: dimensionality and factorial invariance. PLoS One. (2024) 19:e0303531. doi: 10.1371/journal.pone.0303531
21. Gratz, KL. Measurement of deliberate self-harm: preliminary data on the deliberate self-harm inventory. J Psychopathol Behav Assess. (2001) 23:253–63. doi: 10.1023/A:1012779403943
22. Lundh, LG, Karim, J, and Quilisch, E. Deliberate self-harm in 15-year-old adolescents: a pilot study with a modified version of the deliberate self-harm inventory. Scand J Psychol. (2007) 48:33–41. doi: 10.1111/j.1467-9450.2007.00567.x
23. Bjärehed, J, and Lundh, LG. Deliberate self-harm in 14-year-old adolescents: how frequent is it, and how is it associated with psychopathology, relationship variables, and styles of emotional regulation? Cogn Behav Ther. (2008) 37:26–37. doi: 10.1080/16506070701778951
24. Lan, T, Jia, X, Lin, D, and Liu, X. Stressful life events, depression, and non-suicidal self-injury among Chinese left-behind children: moderating effects of self-esteem. Front Psych. (2019) 10:244. doi: 10.3389/fpsyt.2019.00244
25. Ko, J, Sequeira, IR, Skudder-Hill, L, Cho, J, Poppitt, SD, and Petrov, MS. Metabolic traits affecting the relationship between liver fat and intrapancreatic fat: a mediation analysis. Diabetologia. (2023) 66:190–200. doi: 10.1007/s00125-022-05793-4
26. Preacher, KJ, and Hayes, AF. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav Res Methods. (2008) 40:879–91. doi: 10.3758/BRM.40.3.879
27. Wong, SMY, Ip, CH, Hui, CLM, Suen, YN, Wong, CSM, Chang, WC, et al. Prevalence and correlates of suicidal behaviours in a representative epidemiological youth sample in Hong Kong: the significance of suicide-related rumination, family functioning, and ongoing population-level stressors. Psychol Med. (2023) 53:4603–13. doi: 10.1017/S0033291722001519
28. Lipschitz, JM, Yen, S, Weinstock, LM, and Spirito, A. Adolescent and caregiver perception of family functioning: relation to suicide ideation and attempts. Psychiatry Res. (2012) 200:400–3. doi: 10.1016/j.psychres.2012.07.051
29. Cassels, M, van Harmelen, AL, Neufeld, S, Goodyer, I, Jones, PB, and Wilkinson, P. Poor family functioning mediates the link between childhood adversity and adolescent nonsuicidal self-injury. J Child Psychol Psychiatry. (2018) 59:881–7. doi: 10.1111/jcpp.12866
30. Gao, Y, Wang, Y, Wang, Z, Ma, M, Li, H, Wang, J, et al. Family intimacy and adaptability and non-suicidal self-injury: a mediation analysis. BMC Psychiatry. (2024) 24:210. doi: 10.1186/s12888-024-05642-1
31. Kelada, L, Hasking, P, and Melvin, G. The relationship between nonsuicidal self-injury and family functioning: adolescent and parent perspectives. J Marital Fam Ther. (2016) 42:536–49. doi: 10.1111/jmft.12150
32. Liang, K, Zhao, L, Lei, Y, Zou, K, Ji, S, Wang, R, et al. Nonsuicidal self-injury behaviour in a city of China and its association with family environment, media use and psychopathology. Compr Psychiatry. (2022) 115:152311. doi: 10.1016/j.comppsych.2022.152311
33. Ren, Y, Lin, MP, Liu, YH, Zhang, X, Wu, JY, Hu, WH, et al. The mediating role of coping strategy in the association between family functioning and nonsuicidal self-injury among Taiwanese adolescents. J Clin Psychol. (2018) 74:1246–57. doi: 10.1002/jclp.22587
34. Zhou, SC, Zhou, Z, Tang, Q, Yu, P, Zou, H, Liu, Q, et al. Prediction of non-suicidal self-injury in adolescents at the family level using regression methods and machine learning. J Affect Disord. (2024) 352:67–75. doi: 10.1016/j.jad.2024.02.039
35. Glenn, CR, Lanzillo, EC, Esposito, EC, Santee, AC, Nock, MK, and Auerbach, RP. Examining the course of suicidal and nonsuicidal self-injurious thoughts and behaviors in outpatient and inpatient adolescents. J Abnorm Child Psychol. (2017) 45:971–83. doi: 10.1007/s10802-016-0214-0
36. Heath, NL, Toste, JR, Nedecheva, T, and Charlebois, A. An examination of nonsuicidal self-injury among college students. J Ment Health Couns. (2008) 30:137–56. doi: 10.17744/mehc.30.2.8p879p3443514678
37. Nock, MK, and Favazza, AR. Nonsuicidal self-injury: definition and classification. Understanding nonsuicidal self-injury: origins, assessment, and treatment. Washington, DC, US: American Psychological Association; (2009). p. 9–18.
38. Andover, MS, and Gibb, BE. Non-suicidal self-injury, attempted suicide, and suicidal intent among psychiatric inpatients. Psychiatry Res. (2010) 178:101–5. doi: 10.1016/j.psychres.2010.03.019
39. Boxer, P. Variations in risk and treatment factors among adolescents engaging in different types of deliberate self-harm in an inpatient sample. J Clin Child Adolesc Psychol. (2010) 39:470–80. doi: 10.1080/15374416.2010.486302
40. Chartrand, H, Sareen, J, Toews, M, and Bolton, JM. Suicide attempts versus nonsuicidal self-injury among individuals with anxiety disorders in a nationally representative sample. Depress Anxiety. (2012) 29:172–9. doi: 10.1002/da.20882
41. Corcoran, P, Reulbach, U, Perry, IJ, and Arensman, E. Suicide and deliberate self harm in older Irish adults. Int Psychogeriatr. (2010) 22:1327–36. doi: 10.1017/S1041610210001377
42. Castellví, P, Lucas-Romero, E, Miranda-Mendizábal, A, Parés-Badell, O, Almenara, J, Alonso, I, et al. Longitudinal association between self-injurious thoughts and behaviors and suicidal behavior in adolescents and young adults: a systematic review with meta-analysis. J Affect Disord. (2017) 215:37–48. doi: 10.1016/j.jad.2017.03.035
43. Asarnow, JR, Porta, G, Spirito, A, Emslie, G, Clarke, G, Wagner, KD, et al. Suicide attempts and nonsuicidal self-injury in the treatment of resistant depression in adolescents: findings from the TORDIA study. J Am Acad Child Adolesc Psychiatry. (2011) 50:772–81. doi: 10.1016/j.jaac.2011.04.003
44. Muehlenkamp, JJ, Walsh, BW, and McDade, M. Preventing non-suicidal self-injury in adolescents: the signs of self-injury program. J Youth Adolesc. (2010) 39:306–14. doi: 10.1007/s10964-009-9450-8
45. McCauley, E, Berk, MS, Asarnow, JR, Adrian, M, Cohen, J, Korslund, K, et al. Efficacy of dialectical behavior therapy for adolescents at high risk for suicide: a randomized clinical trial. JAMA Psychiatry. (2018) 75:777–85. doi: 10.1001/jamapsychiatry.2018.1109
46. Rockstroh, F, Edinger, A, Josi, J, Fischer-Waldschmidt, G, Brunner, R, Resch, F, et al. Brief psychotherapeutic intervention compared with treatment as usual for adolescents with nonsuicidal self-injury: outcomes over a 2-4-year follow-up. Psychother Psychosom. (2023) 92:243–54. doi: 10.1159/000531092
Keywords: adolescent, child, self-injurious behavior, family functioning, suicide
Citation: Li X, Liu J, Hu Y, Huang X, Li Y, Li Y, Shi Z, Yang R, Peng H, Ma S, Wan X and Peng W (2025) The association of family functioning and suicide in children and adolescents: positive behavior recognition and non-suicidal self-injury as sequential mediators. Front. Public Health. 13:1505960. doi: 10.3389/fpubh.2025.1505960
Edited by:
Yibo Wu, Peking University, ChinaReviewed by:
Jader Piccin, Federal University of Rio Grande do Sul, BrazilSiti Hafizah Zulkiply, Institute for Public Health, Malaysia
Copyright © 2025 Li, Liu, Hu, Huang, Li, Li, Shi, Yang, Peng, Ma, Wan and Peng. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xingli Wan, eGluZ2xpd2FuQDEyNi5jb20=; Wei Peng, cGVuZ3dlaUBzY3UuZWR1LmNu
†These authors have contributed equally to this work