 Habtemariam Mulugeta Abate
Habtemariam Mulugeta Abate Prem Kumar2
Prem Kumar2 Mitaw Girma
Mitaw Girma Wondosen Yimam
Wondosen Yimam Birhanu Desu
Birhanu Desu- 1Department of Biomedical Sciences, College of Medicine and Health Sciences, Wollo University, Dessie, Ethiopia
- 2Department of Surgical Nursing, College of Medicine and Health Sciences, Wollo University, Dessie, Ethiopia
- 3Department of Comprehensive Nursing, College of Medicine and Health Sciences, Wollo University, Dessie, Ethiopia
- 4Department of Emergency Medicine and Critical Care Nursing, Wollo University, Dessie, Ethiopia
Background: Despite limited research, health literacy in developing countries like Ethiopia remains low, making it a significant challenge to combat non-communicable diseases.
Objective: To assess the level of health literacy and associated factors among adult type 2 diabetic patients in Woldia Comprehensive Specialized Hospital, North-East Ethiopia, 2022.
Methods and materials: A cross-sectional study was conducted at Woldia Comprehensive Specialized Hospital from April 19 to July 19, 2022, involving 423 participants. Systematic random sampling, face-to-face interviews, and document reviews were used to collect data. The data were coded and entered into Epi-Data version 4.6.0.2, then analyzed using Statistical Package for the Social Sciences (SPSS) version 26. The results were presented in texts, tables, and figures. Bivariable and multivariable logistic regression analyses were performed to identify significant predictors with p-values below 0.05 and to verify the assumptions of binary logistic regression.
Result: General Health Literacy Index was 27.86 (±6.71), and the magnitude of participants with adequate health literacy in the study was 22.2% (95% CI: 18.4–26.3%). Ages (18–35) years [(AOR =14, 95% CI = 3.86–50.77)], ages (36–50) years [(AOR = 15.38, 95% CI = 4.23–55.9)], being male [(AOR = 2.945, 95% CI = 1.570–5.526)], no experiencing depression symptoms [(AOR = 2.673, 95% CI = 1.308–5.463)], not experiencing anxiety [(AOR = 2.001, 95% CI = 1.011–3.960)] and being literate [(AOR = 4.120, 95% CI = 1.397–12.146)] were significantly associated with adequate health Literacy.
Conclusion and recommendations: The magnitude of adequate health literacy was low. Ages (18–35) years, ages (36–50) years, being male, not experiencing depression symptoms, not experiencing anxiety, and being literate were significantly associated with adequate health literacy. Health professionals should regularly implement health education programs for diabetic patients and communities, focusing on females, older adults, the illiterate, and those experiencing depression and anxiety.
Introduction
Metabolic problems are the hallmark of diabetes mellitus, type I diabetes, which is more frequent in young people, and type II diabetes, which is more common in adults, are the two main forms of diabetes (1). Low-to-medium-wage countries have low education levels, exacerbating health literacy (HL) effects. In 2020, the WHO reported that deaths due to diabetes mellitus in Ethiopia numbered ~16,258, accounting for about 2.88% of total deaths. The adjusted death rate was 33.58 per 100,000 people, ranking Ethiopia 80th in the world and 7th in the country among other diseases (2, 3). Currently, diabetic micro- and macro-complications are increasing rapidly in Ethiopia due to poor glycemic control (3).
Health literacy empowers patients to make informed decisions, actively engage with healthcare providers, and understand disease prevention strategies, including lifestyle modifications, medication adherence, and self-monitoring (4). This enhanced understanding ultimately improves self-management and helps control complications associated with diabetes (4). The quality of life for patients with type 2 diabetes can be significantly improved through a combination of reading skills, knowledge, self-care behaviors, decision-making, communication, and access to health information (5, 6). Three studies conducted in Iran strongly support this conclusion by demonstrating the importance of health literacy promotion programs in helping individuals with the disease manage their health more effectively (5–7). However, empowering communities with health literacy remains a significant challenge throughout the world (8–11). Especially Research conducted in Ethiopia on health-related quality of life among diabetic patients has shown the mean scores for the physical health, social health, psychological health, and environmental health domains are all below 50 (12–14). Additionally, the occurrence of complications such as retinopathy, nephropathy, neuropathy, stroke, heart attack, erectile dysfunction, diabetic foot ulcers, diabetic ketoacidosis, hypoglycemia, and other issues is dramatically increasing (15–23). This underscores the need for researchers to prioritize assessing the health literacy status of the community. The probability of dying after being admitted to the hospital for chronic conditions has been associated with lower health literacy (24, 25). The decline in the expansion of health literacy among the general population negatively impacts individuals' psychological, social, and cultural wellbeing. It also leads to increased emergency room visits, which results in higher costs and greater resource use for health institutions, while affecting personal and family life (26–31).
Some studies have indicated that drugstore expenses were higher among respondents with low health literacy compared to those with high health literacy, ranging from $12 to $1,110 (32). Low health literacy skills contribute to an annual increase in healthcare spending of $73 billion, whereas improving health literacy skills could save over $25 billion annually by preventing 1 million hospital visits (26–32). According to research conducted in various countries, the key factors impacting health literacy include age, gender, marital status, educational attainment, ethnicity, and lack of awareness about diabetes (17, 32–37).
According to the Ethiopian National Healthcare Quality Strategy plan Ethiopian government working on the establishment of health education units, peer learning to improve patient care, and the prediction and discussion of patient health needs (38). Despite these efforts, the level of health literacy regarding type 2 diabetes in the community remains a significant challenge.
Currently, the incidence and complications of type 2 diabetes are rapidly increasing worldwide, particularly in Ethiopia. In contrast, various scholars have primarily focused on medical approaches while overlooking the impact of health literacy on diabetic self-care behaviors. Additionally, factors such as membership in diabetic associations, personal glucometer use, distance from health institutions, and khat consumption have not been studied by previous researchers in Ethiopia. This lack of research on health literacy related to type 2 diabetes in Ethiopia is another significant issue. Consequently, ongoing research on health literacy concerning type 2 diabetes is crucial for addressing the incidence, morbidity, mortality, and complications associated with this condition. Therefore, the main goal of this study is to fill the gaps in understanding health literacy among type 2 diabetes patients by introducing important new variables that have not been previously addressed by scholars in Ethiopia. So, this study aimed to assess the magnitude of health literacy and associated factors among adult Type 2 diabetic patients receiving follow-up care at Woldia Comprehensive Specialized Hospital from April 19 to July 19, 2022.
Method and materials
Study setting and period
The study was conducted at Woldia Comprehensive Specialized Hospital, one of the governmental hospitals at the zonal level located in northeastern Ethiopia. The research took place from April 19 to July 19, 2022. This hospital is a vital healthcare institution serving a population of ~1.5 million people. It offers a wide range of medical services, including medical, surgical, obstetric, and orthopedic care. The hospital employs 406 healthcare workers and 240 administrative staff, ensuring comprehensive service delivery. Among its specialized services is a diabetes follow-up program that caters to 1,150 patients with Type 2 diabetes mellitus (T2DM). During the study period, ~1,000 diabetic patients attended follow-up appointments scheduled on various dates.
Study Design: An institutional-based cross-sectional study design was employed to evaluate the targeted population. The study focused exclusively on adult patients with Type 2 diabetes who were receiving follow-up care at Woldia Comprehensive Specialized Hospital. Participant's eligibility criteria: The study focused on adult patients with Type 2 diabetes who had consistently attended follow-up care at least 6 months prior to the study. However, patients who were unable to communicate due to severe medical conditions during the data collection period were excluded. Participants were systematically selected to ensure a diverse and representative sample of adult patients with Type 2 diabetes.
Study Variables: The dependent variable in this study is adequate health literacy, which reflects an individual's ability to effectively understand and utilize health-related information. Several independent variables influence this outcome, which can be categorized into socio-demographic, behavioral, psychosocial, and clinical factors. Socio-demographic factors include age, average monthly income, occupational status, educational attainment, gender, marital status, and enrollment in community-based health insurance, residency and distance from health institutions collectively influence an individual's access to resources and opportunities for health education. Additionally, Behavioral and psychosocial factors—such as alcohol consumption, khat use, depression, anxiety, and stress—significantly impact health literacy by affecting both the cognitive and emotional capacities to process health information. Additionally, clinical factors such as chronic complications of diabetes mellitus, the number of chronic complications, the duration of diabetes mellitus, treatment regimens, comorbid conditions, self-rated health, membership in a diabetic association, ownership of a personal glucometer, and knowledge of diabetes management play a significant role.
Operational Definitions: Adequate Literacy: if the study participants scored from the General Health Literacy 47-item index questionnaire > 33 points (33, 39–41). Limited Health Literacy: if the study participants scored from the General Health Literacy 47-items index questionnaire ≤ 33 points (33, 39–41). Diabetic Knowledge: study participants with a score greater than or equal to 80% from 14–items in the diabetic knowledge questionnaire had adequate knowledge, while the patients with scores below 80% had inadequate knowledge (29). Self-Care: study participants who scored equal to or greater than the mean score were classified as having good diabetes self-care practice and those who scored below the mean were considered to have poor self-care practice (42).
Self-Rated Health: In this study, it is defined as “good” when the patient reported having excellent, very good, or good health and “poor” when the Participant reported having fair or poor health, according to the Stanford Patient Education Research Center Self-Rated Heath Scale (42). Co-morbidity is an illness or disorder that coexists with diabetes but is mainly unrelated (33). Depression: study participants were scored, Normal: 0–9, Depressed ≥10 (15, 16). Anxiety: study participants were scored, normal: 0–7, Anxious: ≥8 (15). Stress: study participants were scored, normal: 0–14, Stressed: ≥15 (15). Alcohol Drinker: It is defined as the proportion of individuals who have ever used alcoholic drinks such as “tela, tej, katicala/areke, beer, wine, or other drinks that can cause intoxication at least once” in his/her lifetime or respondent who drank alcohol during 1 month preceding the study at least once per month (17, 18). Khat chewing: respondent who chewed the leaves of the khat plant during his lifetime in any amount (17, 18).
Sample size determination and sampling technique
The study sample size was calculated by assuming the prevalence of adequate health literacy at 50% since there was no adequate research done in Ethiopia. The sample size was calculated using the following formula with 95% CI, d = 0.05, Z = 1.96, P = 50%
, after that adding a 10% non-response rate =38.4 + 384 = 422.4 = 423, n = 423.
The response rate was calculated based on the rates reported in previous studies conducted in similar health settings. In earlier research conducted in Ethiopia, the response rate was 90%. For this study, the non-response rate was estimated at 10%. After analyzing our data, the response rate was determined by dividing the total number of participants who provided complete information during data collection by the total sample size, and then multiplying by 100 to express it as a percentage. To contact potential participants, the following steps were followed : First, ethical clearance was obtained from Wollo University's Ethical Review Committee, along with administrative permission from the CEO of Woldia Comprehensive Specialized Hospital. After receiving permission from the CEO, a systematic random sampling method was employed during data collection. The value was calculated as follows: First, the total number of type two diabetic patients who had treatment follow-ups on different appointment dates within the study period was determined by counting the appointment dates listed in the registration book from the previous year. The value was calculated as K = 1,000/423 = 2, where N = 1,000 and n = 423. Subsequently, the first participant was selected using a random lottery method. The next participant was then selected at every two-interval until the required sample size was achieved.
Data collection tools and procedures
Socio-demographic factors: were developed from the literature review and conceptual framework. Health Literacy: The second half of the survey is based on the General Health Literacy Index from the HLS-EU-Q47. This index covers three domains: disease prevention, health promotion, and healthcare. The survey includes 47 direct questions, where participants rate the ease of accessing, interpreting, evaluating, and using health information on a 5-point Likert scale (very easy, easy, difficult, very difficult, and I don't know). The General Health Literacy Index classifies respondents into four categories based on their scores: poor (0–25), problematic (26–33), sufficient (34–42), and outstanding (43–50). In the study, participants scoring 33 or below were categorized as “Inadequate,” while those scoring above 33 were categorized as “Adequate.” The English version of the questionnaire demonstrated internal consistency and reliability, which was assessed by computing Cronbach's alpha, yielding a score of 0.97. Moreover, the tool was previously validated in Debre Tabor, Ethiopia, in a cross-sectional study titled “Information Seeking Behavior About Cancer and Associated Factors Among University Students in Ethiopia” (19). The third section of the questionnaires covers clinical, behavioral, and psychosocial factors, which have been developed, adapted, and refined based on a review of the literature, the conceptual framework, and relevant sources.
Depression, Anxiety, and Stress Scale (DASS-21) was developed by Lovibond and Lovibond's is a validated psychological screening tool designed to assess symptoms of depression, anxiety, and stress. The DASS-21 demonstrates strong reliability, with Cronbach's alpha values of 0.81, 0.89, and 0.78 for its respective subscales. Participants rated their symptoms of depression, anxiety, and stress over the past week using a 7-item scale, with scores ranging from 0 to 3 for each item. These scores were then multiplied by two to obtain the final score. According to the DASS handbook, scores indicating normal levels of depression, anxiety, and stress were categorized as “0” [No], while scores reflecting mild, moderate, severe, or extremely severe levels were categorized as “1” [Yes] (16, 20). Furthermore, the DASS-21 has been utilized multiple times in our country, including in a cross-sectional study conducted in Arsi, Southeast Ethiopia, titled “The Prevalence and Severity of Depression, Anxiety, and Stress among Medical Undergraduate Students of Arsi University and Their Association with Substance Use, Southeast Ethiopia” (21).
Diabetes Knowledge: The Revised Brief Diabetes Knowledge Test (DKT2) was employed to assess diabetes knowledge in adults with type 1 and type 2 diabetes. This test consists of two sections: 14 general knowledge items and nine items related to insulin use. For this study, only the general knowledge items were utilized, with five items excluded due to cultural considerations. Knowledge levels were classified using Bloom's cut-off point, where scores of 80% or higher were deemed indicative of adequate knowledge, while scores below 80% were considered indicative of inadequate knowledge. The internal consistency and reliability were assessed by computing Cronbach's alpha, which resulted in a score of α = 0.843. For this study, only the general knowledge items were utilized, with five items excluded due to cultural considerations, based on previous research conducted in Ethiopia's West Shoa Zone, titled “Factors Associated with Self-Care Practice Among Adult Diabetes Patients in West Shoa Zone, Oromia Regional State, Ethiopia” (20).
Self-Care: The study employed the Revised Summary of Diabetes Self-Care Activities (SDSCA) questionnaire to assess participants' self-care behaviors over the past week. This included adherence to a healthy diet, daily exercise, blood glucose monitoring, foot care, and smoking cessation (21). The study computed mean scores for different domains, including general diet, specific diet, exercise, blood glucose testing, and foot care. Participants were classified based on their overall mean score for diabetic self-care, with those scoring at or above the mean regarded as having good self-care practices, and those scoring below the mean considered to have poor self-care practices. The reliability test evaluated the internal consistency of the tool by calculating Cronbach's alpha, which yielded an overall score of α = 0.680. This method was based on previous studies conducted in Ethiopia, including a study in Gondar titled “Self-Care Practices and Associated Factors Among Patients with Diabetes Mellitus Undergoing Follow-Up at University of Gondar Referral Hospital, Gondar, Northwest Ethiopia” (22).
Self-Rated Health: The study used the Stanford Patient Education Research Center Self-Rated Health Scale to assess participants' self-rated health. The reliability test evaluated the internal consistency of the tool by calculating Cronbach's alpha, which yielded an overall score of α = 0.92 and evaluates health from good to poor (23). Data was collected through face-to-face interviews and document reviews. Two BSc nurses with at least 2 years of clinical experience in the chronic outpatient department were appointed as data collectors, while one nurse was assigned as a supervisor.
Data quality control
The research used standardized tools, translated from Amharic to English, and retranslated for consistency. Face validity was checked, and data collectors and supervisors received training. a pre-test was conducted a week before the main data collection at Dessie Comprehensive Specialized Hospital, involving 10% of the population. During the pre-test, the internal consistency of the tool was assessed using Cronbach's alpha: Healthcare/Access Information = 0.823, Disease Prevention/Apply Information = 0.914, Health Promotion/Access Information = 0.722, Overall health literacy = 0.92. Then modifications were made after the pre-test. The data collection process began, with data collectors managing redundancy by recording participants' medical records.
Data processing and data analysis
EpiData software version 4.6.0.4 and SPSS for Windows version 26 were used in the study to analyze data presented in text, tables, and figures. The binary logistic regression model was applied to identify significant variables. Variables with a p < 0.25 in the bivariable binary logistic regression were included in the multivariable binary logistic regression model. In this model, variables with a p < 0.05 were considered statistically significant. All assumptions for the binary logistic regression model were evaluated and confirmed, Hosmer-Lemeshow test value (0.84). Multicollinearity was assessed using variance inflation factors (VIF) and tolerance, with VIF values below 10 and tolerance values above 0.1 for all predictor variables.
Result
Socio-demographic characteristics of the study participants
Out of a total sample of 423 participants, 419 completed the study, resulting in a response rate of 99%. Among the respondents, 230 (55%) were female. The ages of the participants ranged from 18 to 87 years, with a mean (SD) of 49.65 (±18.239) years. Two hundred fifty-two (60%), lived in urban areas. Regarding marital status, more than half (65%), were married. In terms of educational status, ~112 (27%) were illiterate. More than half (79%), were employed. Concerning income, nearly half, 199 (48%), were classified as Below the Poverty Line. Additionally, 254 (61%) of the respondents were enrolled in community-based health insurance (Table 1).
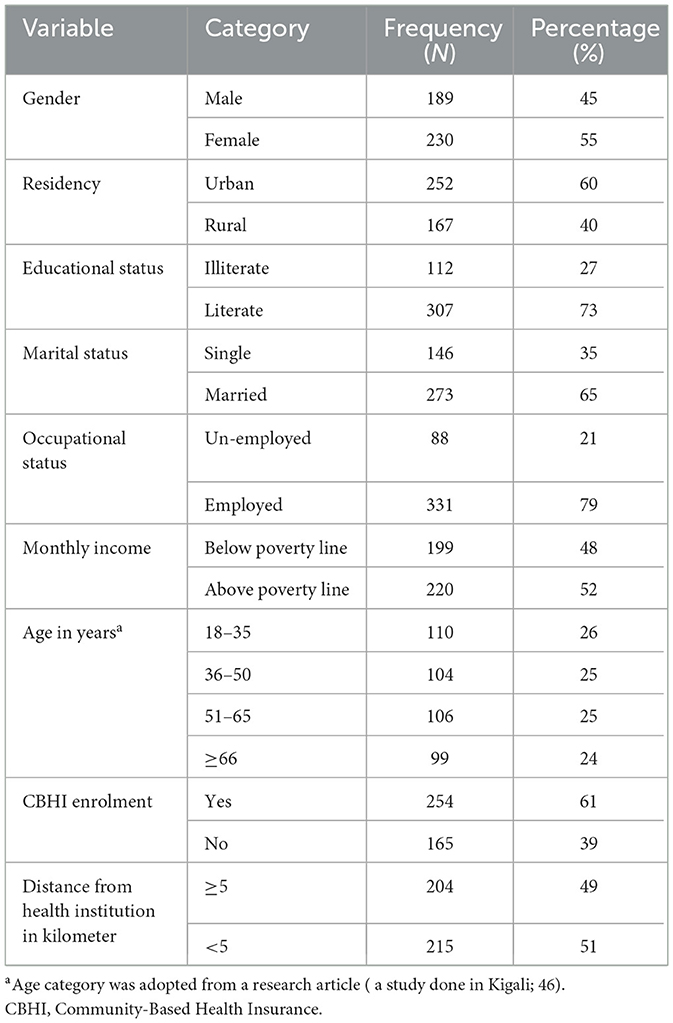
Table 1. Socio-demographic characteristics of type 2 diabetic follow-up participants attending WCSH, Woldia, Northeast Ethiopia from April 19 to July 19, 2022 (n = 419).
Clinical characteristics
The median (IQR) duration of diabetes among participants was 4 years. Regarding chronic diabetic-related complications, less than half, 88 (21%), had developed complications, with 88 (21%) experiencing only one such complication. The most common complication was diabetic-related hypertension, affecting 59 (14%) of participants. Of the total participants, 284 (68%) were using insulin only. Additionally, 98 (23%) had developed co-morbid conditions, with hypertension being the most prevalent, affecting 96 (23%). Among all respondents, 143 (34%) owned a personal glucometer, 17 (4.1%) were members of a diabetic association, and 215 (51%) lived within a 5-kilometer distance from a health institution. More than half, 240 (57%), rated their health as good. Regarding self-care practices, 239 (57%) had poor self-care, and 235 (56%) had inadequate knowledge about diabetes (Table 2).
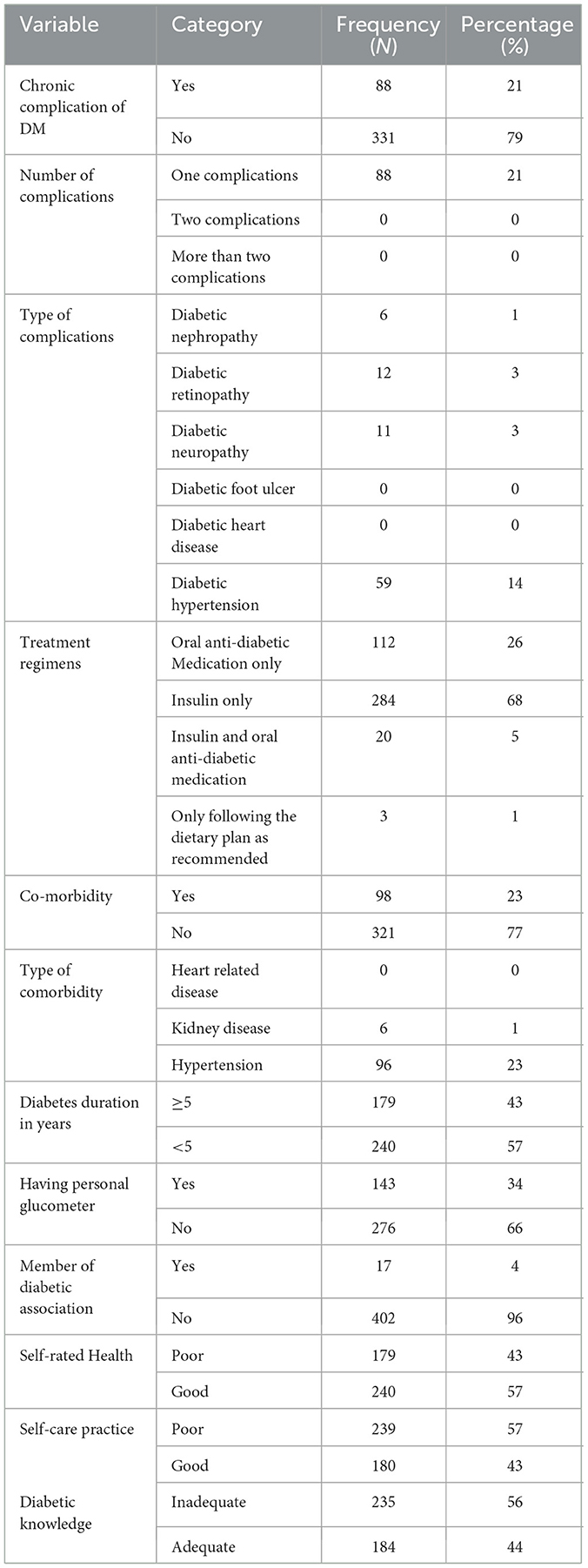
Table 2. Clinical characteristics and diabetic knowledge of type 2 diabetic follow-up participants attending WCSH, Woldia, Northeast Ethiopia from April 19 to July 19, 2022 (n = 419).
Behavioral and psychosocial characteristics
Of the total participants, 173 (41%) reported 148 (35%) experienced depression, more than half of the study participants (54%) experienced anxiety, and 154 (37%) experienced stress. Among the participants, nearly 90 percent of the study participants (377) had never chewed khat, 410 study participants (98%) had never smoked cigarettes, and 289 study participants (69%) had never consumed alcohol (Table 3).
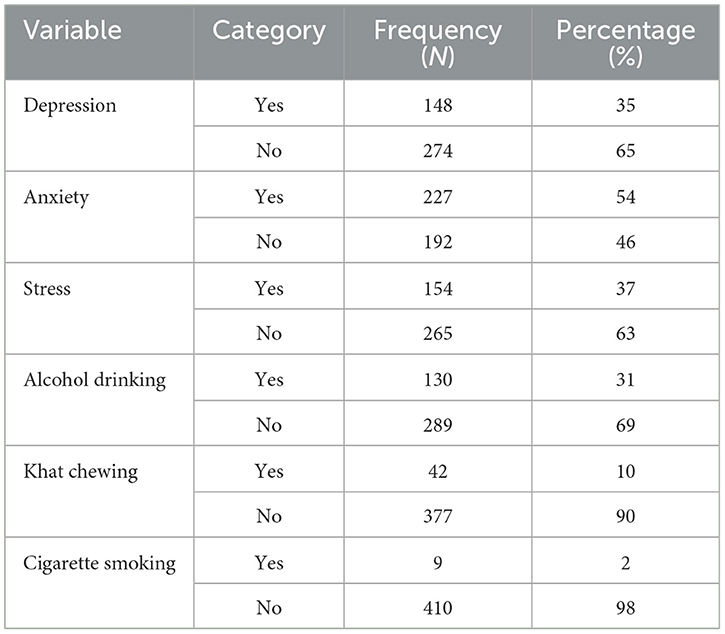
Table 3. Behavioral and psychosocial characteristics of type 2 diabetic follow-up participants attending WCSH, Woldia, Northeast Ethiopia from April 19 to July 19, 2022 (n = 419).
Health literacy level
Study participants, had 34.4% inadequate health literacy, 182 (43.3%), had Problematic health literacy, 18.1% had sufficient health literacy and 4.1% had excellent health literacy (Figure 1).
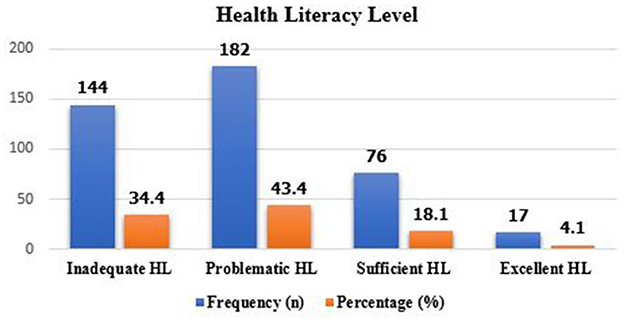
Figure 1. Health literacy level among type 2 diabetic follow-up participants attending WCSH, Woldia, Northeast Ethiopia from april to july 19, 2022 (n = 419).
Magnitude of limited health literacy
The Mean (SD) General Health Literacy Index score was 27.8602 (±6.71287). The overall magnitude of adequate health literacy was 22.2 (95% CI 18.4–26.3) whereas, limited health literacy was 77.8% (95% CI 73.8–81.9; Figure 2).
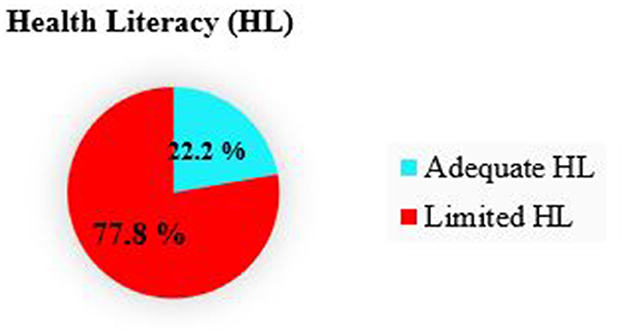
Figure 2. Magnitude of adequate health literacy among type 2 disbetic follow-up participants attending WCHS, Woldia, Northeast Ethiopia from april to july 19, 2022 (n = 419).
Factors associated with limited health literacy
The variables included in the bivariable binary logistic regression analysis and subsequently entered into the multivariable binary logistic regression analysis with a p < 0.25 were age, gender, residency, educational status, income, depression, and anxiety. The multivariable binary logistic regression analysis, conducted using the backward selection method, identified age (18–35) years, age (36–50) years, gender, educational status, depression, and anxiety were significantly associated with adequate health literacy (LHL).
Respondents aged (18–35) years were 14 times more likely to have adequate health literacy as compared to those aged (>=66) years [(AOR =14, 95% CI = 3.86–50.77)].
Respondents aged (36–50) years are 15.38 times more likely to have adequate health literacy as compared with those aged (>=66) years [(AOR = 15.38, 95% CI = 4.23–55.9)].
Being male was 2.945 times more likely to have adequate health literacy as compared to female respondents [(AOR = 2.945, 95% CI = 1.570–5.526)].
Respondents who have not experienced depression symptoms were 2.673 times more likely to have adequate health literacy as compared to respondents who have experienced depression symptoms [(AOR = 2.673, 95% CI = 1.308–5.463)].
Respondents who have not experienced anxiety symptoms were 2 times more likely to have adequate health literacy as compared to respondents who have experienced anxiety symptoms [(AOR = 2.001, 95% CI = 1.011–3.960)].
Being literate was 4.120 times more likely to have adequate health literacy as compared to being illiterate [(AOR = 4.120, 95% CI = 1.397–12.146; Table 4)].
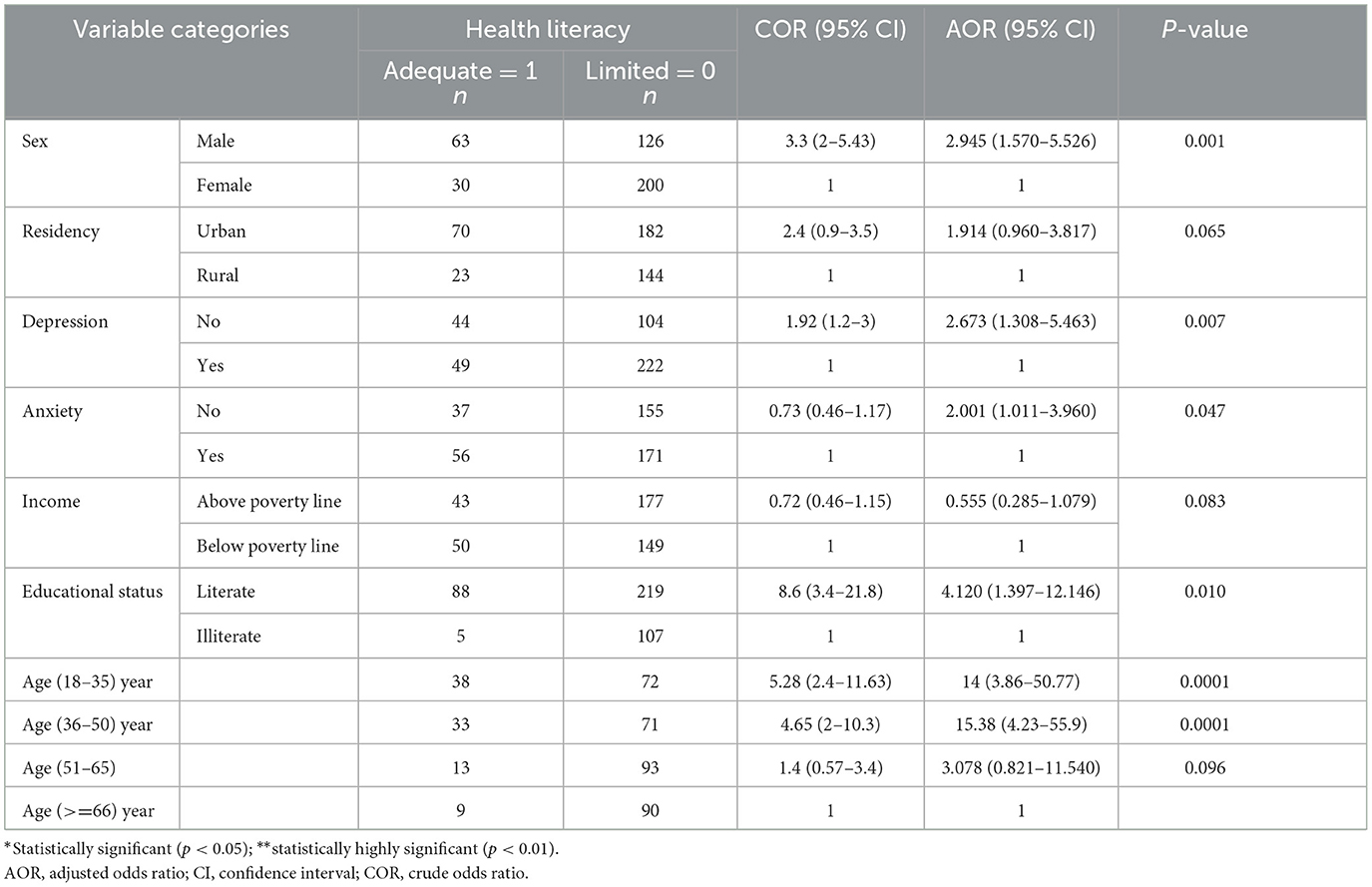
Table 4. Multivariable binary logistic regression on factors associated with adequate health literacy among type 2 diabetic follow-up participants attending WCSH, Woldia, Northeast Ethiopia from April 19 to July 19, 2022 (n = 419).
Discussion
The magnitude of adequate health literacy among type 2 diabetic follow-up patients in this study was 22.2% (95% CI: 18.4–26.3). According to the findings of this study, type 2 diabetic patients did not receive sufficient health information from healthcare providers. This highlights significant obstacles to diabetic self-care across various health domains, including environmental, social, psychological, physical, and spiritual aspects. One study carried out in Iran indicated that the best way to improve the health and quality of life of people with type 2 diabetes is to create a health literacy promotion program that aims to improve self-care practices (5). Another study condcucted in Southern California on Resident Physician Empathy and Health Literacy Communications associated with diabetic control approved that Patients' understanding of the self-management required for effective diabetes control may be improved through compassionate communication from resident physicians that aligns with their health literacy levels (24).
This study's findings were lower compared to studies conducted at Jimma Comprehensive Specialized Hospital of Ethiopia (53%; 10) and the University Of Gondar Comprehensive Specialized Hospital Of Ethiopia (56.5%; 31). The differences may be due to the findings of this study used 47-items health literacy tool, participants with diabetes for <5 years, a more representative sample size, and the majority experiencing anxiety. Similarly, the findings of this study was lower than Switzerland, Rwanda, Malaysia, “Atlanta and Chicago”, Brazil, Georgina, Iran, Kuwait, and Zabol with magnitudes of adequate health literacy were (33%), (44.7%), (34.7%), (86%), (73.3%), (67%), (36.3%), (35.5%), and (28.7%) (26), (27), (40), (28), (29), (30), (31), (32), and (34) respectively.
The differences observed in the findings of this study can be attributed to several factors. About 40% of participants lived in rural areas, which limited their access to information from media sources like television and radio. Additionally, around 27% of participants were illiterate, and ~48% had incomes below the poverty line. Furthermore, about 66% did not have a glucometer to monitor their blood glucose at home, and 56% lacked adequate knowledge about type 2 diabetes mellitus. As a result, many participants developed chronic complications, such as diabetic retinopathy, diabetic neuropathy, and hypertension. Additionally, around 54% experienced anxiety and about 31% were addicted to alcohol, highlighting significant health challenges compared to other studies. The assessment and decision-making components of health literacy were shown to be responsible for about 25% of the self-care practices in a similar study that was carried out in Tehran on the prediction of self-care behaviors among patients with type 2 diabetes (7).
Being male was significantly associated with adequate health literacy compared to being female. This study's findings align with similar studies conducted in Iran and Saudi Arabia (31, 35). Gender disparities in health literacy related to non-communicable diseases may arise from historically greater educational access for men, more proactive health information-seeking behaviors, and better access to health services. Consequently, men tend to engage more in preventive health behaviors.
Study participants who have not experienced depression symptoms and anxiety showed a positive relationship with adequate health literacy compared to those who have experienced depression symptoms and anxiety. This study finding was consistent with studies conducted in Switzerland and Saudi Arabia (26, 35, 36).
The relationship may be influenced by several factors. Participants without depression or anxiety tend to have better attention, memory, and engagement in health management, enabling them to seek and understand health information effectively. In contrast, those with depression may struggle, resulting in inadequate health literacy about type 2 diabetes. This highlights the need for targeted interventions to improve health literacy for individuals with depression and anxiety.
Literate study participants are strongly associated with adequate health literacy as compared to illiterate ones. This study was concurrent with studies conducted in Turkey, Rio de Janeiro, Brazil, India, Iran, Norway, Jimma Comprehensive Specialized Hospital of Ethiopia, Kuwait, Malaysia, and Saudi Arabia (15, 36, 41, 43, 44, 46, 47, 51) (43–45). Literate individuals have better access to health information, make informed decisions, and enhance critical thinking, which helps them interpret health materials and communicate effectively with providers. This promotes awareness of health issues and preventive measures. Therefore, healthcare providers and organizations should prioritize community engagement in health education to prevent type 2 diabetes and its complications during clinical follow-ups and early screenings.
Study participants whose ages are (18–35) and (36–50) years were strongly associated with adequate health literacy as compared with those whose ages >=66 years. This study aligned with studies conducted in Brazil, Iran, Kuwait, Rio de Janeiro, and Saudi Arabia (29, 31, 32, 35). Young and middle-aged adults are generally more proficient with digital tools for accessing health information, have better cognitive function, and are more familiar with current health guidelines than older adults. Therefore, healthcare providers should prioritize older adults with type 2 diabetes during clinical follow-ups, as their health significantly impacts overall outcomes.
Limitations of the study
The study's limitations include methodological weaknesses, such as cross-sectional nature, potential social desirability bias and recall bias, which may limit its generalizability to the general population and may lead to biased results.
Conclusion
The overall magnitude of adequate health literacy results was lower as comparable to other studies. Being male, ages (18–35), (36–50) years, not experiencing depression symptoms, not experiencing anxiety, and being literate were significantly associated with adequate health literacy.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Wollo University's Ethical review committee. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants' legal guardians/next of kin because verbal consent can be better than written consent in certain contexts, such as in diabetic follow-ups, because it allows for more personal interaction, helping to build rapport. It can also simplify the process, making it easier for patients who may have difficulty with literacy or who feel overwhelmed by paperwork. Additionally, it allows for immediate clarification of any questions, enhancing understanding and comfort during data collection.
Author contributions
HMA: Writing – review & editing, Writing – original draft, Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Software, Resources, Supervision, Validation, Visualization. PK: Writing – review & editing. SA: Writing – review & editing. MG: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Software, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. WY: Writing – review & editing. BD: Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
First, I would like to thank the Department of Adult Health Nursing and the College of Medicine and Health Sciences for allowing me to prepare this thesis. Second, I want to thank my advisors, Samuel Anteneah and Birhanu Desu, for their consistent advice, and also, I am inclined to forward my deepest gratitude to Mitaw Girma and Wondosen Yimam for their constructive comments and advice. Third, I would like to thank Woldia Comprehensive Specialized Hospital staff and managers for their cooperation. Finally, I like to acknowledge the data collectors, supervisors, and participants of the study for their cooperation.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
AOR, Adjusted Odds Ratio; CBHI, Community-Based Health Insurance; COR, Crude Odds Ratio; RDKT, Revised Brief Diabetes Knowledge Test; DM, Diabetes Mellitus; HL, Health Literacy; HLS- EU- Q47, Health Literacy Survey European Questionnaire 47; HRQL, Health related quality of life; IDF, International Diabetes Federation; NCDs, Non-Communicable Diseases; PRIME-MD, Primary Care Evaluation of Mental Disorders; SD, Standard Deviation; SPSS, Statistical Product and Service Solutions; T2DM, Type Two Diabetes Mellitus; TOFHLA, Test of Functional Health Literacy in Adults; WCSH, Woldia Comprehensive Specialized Hospital; WHO, World, Health Organization.
References
1. Hinkle JL, Cheever KH. Medical-Surgical Nursing. 14th ed. In: Squazzo K, Stegman JK, Gray L, editors. Philadelphia, PA: Wolters Kluwer (2018). p. 3843–61.
2. Zeru MA, Tesfa E, Mitiku AA, Seyoum A, Bokoro TA. Prevalence and risk factors of type-2 diabetes mellitus in Ethiopia: systematic review and meta-analysis. Sci Rep. (2021) 11:21733. doi: 10.1038/s41598-021-01256-9
3. Abebe N, Addise D, Kebede T. Diabetes in Ethiopia 2000–2016 prevalence and related acute and chronic complications. Reaserch gate. (2015) 2:31–6.
4. American Association of Diabetes Educators. Cultural and health literacy considerations with diabetes. Diabetes educator. (2019).
5. Ahmadzadeh H, Heizomi H, Nadrian H, Shirzadi S, Pirehbabi K, Fathi B, et al. Development of a health literacy promotion program (HeLPP) to promote self-care behaviors and quality of life among rural patients with type 2 diabetes: preliminary results. J Heal Lit. (2024) 9:40–54. doi: 10.22038/jhl.2024.76462.1505
6. Jafari A, Zadehahmad Z, Armanmehr V, Talebi M, Tehrani H. The evaluation of the role of diabetes health literacy and health locus of control on quality of life among type 2 diabetes using the path analysis. Sci Rep. (2023) 13:1–11. doi: 10.1038/s41598-023-32348-3
7. Jahangirimehr A, Azizpour M, Kalanfarmanfarma K, Yarmohammadi S. Prediction of self-care behaviors among type 2 diabetes patients in Tehran based on health literacy in 2020 : a cross-sectional study. J Heal Lit. (2024) 10:22–32. doi: 10.22038/jhl.2024.78030.1625
8. Dunn P, Margaritis V, Anderson CL. Understanding health literacy skills in patients with cardiovascular disease and diabetes. Qual Rep. (2017) 22:33–46. doi: 10.46743/2160-3715/2017.2548
9. Rüegg R, Abel T. Challenging the association between health literacy and health: the role of conversion factors. Health Promot Int. (2022) 37: daab054. doi: 10.1093/heapro/daab054
10. Tilahun D, Abera A, Nemera G. Communicative health literacy in patients with non-communicable diseases in Ethiopia: a cross-sectional study. Trop Med Health. (2021) 49:57. doi: 10.1186/s41182-021-00345-9
11. Christova MHA, CG. Health Literacy in Physiotherapy Education. Helpe. (2012). Available at: https://helpe.eu.com/intellectual-outputs/
12. Shimels T, Kassu RA, Bogale G, Muleta MB, Akalu GT, Getachew A, et al. Health-related quality of life of patients with type 2 diabetes mellitus and hypertension in Addis Ababa, Ethiopia. Ethiop J Health Sci. (2022) 32:381–92. doi: 10.4314/ejhs.v32i2.19
13. Feyisa BR, Yilma MT, Tolessa BE. Predictors of health-related quality of life among patients with diabetes on follow-up at nekemte specialised Hospital, Western Ethiopia: a cross-sectional study. BMJ Open. (2020) 10:1–8. doi: 10.1136/bmjopen-2019-036106
14. Reba K, Argaw Z, Walle B, Gutema H. Health-related quality of life of patients with diagnosed type 2 diabetes in Felege Hiwot referral hospital, North West Ethiopia: a cross-sectional study. BMC Res Notes. (2018) 11:4–9. doi: 10.1186/s13104-018-3625-x
15. Yeshaw Y, Mossie A. Depression, anxiety, stress, and their associated factors among Jimma university staff, Jimma, southwest Ethiopia, 2016: a cross-sectional study. Neuropsychiatr Dis Treat. (2017) 13:2803–12. doi: 10.2147/NDT.S150444
16. Nakie G, Segon T, Melkam M, Desalegn GT, Zeleke TA. Prevalence and associated factors of depression, anxiety, and stress among high school students in, Northwest Ethiopia, 2021. BMC Psychiatry. (2022) 22:1–12. doi: 10.1186/s12888-022-04393-1
17. Tessema ZT, Zeleke TA. Spatial distribution and factors associated with khat chewing among adult males 15-59 years in Ethiopia using a secondary analysis of ethiopian demographic and health survey 2016: spatial and multilevel analysis. Psychiatry J. (2020) 2020:1–12. doi: 10.1155/2020/8369693
18. Tavakoly Sany SB, Esmaeily A, Lael-Monfared E, Tehrani H, Ferns G, Jafari A. Organizing framework to investigate associations between diabetes knowledge, health literacy, and self-care behaviors in patients with type 2 diabetes based on the extended parallel process model. J Diabetes Metab Disord. (2020) 19:1283–92. doi: 10.1007/s40200-020-00642-w
19. Gedefaw A, Yilma TM, Endehabtu BF. Information seeking behavior about cancer and associated factors among university students, Ethiopia: a cross-sectional study. Cancer Manag Res. (2020) 12:4829–39. doi: 10.2147/CMAR.S259849
20. Gurmu Y, Gela D, Aga F. Factors associated with self-care practice among adult diabetes patients in west shoa zone, oromia regional state, Ethiopia. BMC Health Serv Res. (2018) 18:4–11. doi: 10.1186/s12913-018-3448-4
21. Schmitt A, Gahr A, Hermanns N, Kulzer B, Huber J, Hakk T. The diabetes self-management questionnaire (DSMQ). J Heal Qual Life Outcomes. (2013) 11:1. doi: 10.1186/1477-7525-11-138
22. Aschalew AY, Yitayal M, Minyihun A, Bisetegn TA. Self-care practice and associated factors among patients with diabetes mellitus on follow up at University of Gondar Referral Hospital, Gondar, Northwest Ethiopia. BMC Res Notes. (2019) 12:1–6. doi: 10.1186/s13104-019-4630-4
23. Hosseini RS, Momtaz YA, Mohammadi-Shahboulaghi F, Sahaf R, Soroush MR. Validity and reliability of self rated health (SRH) measure among Iranian community-dwelling older adults. J Gerontol Geriatr. (2019) 2019:103–8.
24. Morton KR, Flynn PM, Cho J, Chukwueke I. Resident physician empathy and health literacy communications associated with diabetes control. J Heal Lit. (2024) 8:104–15. doi: 10.22038/jhl.2023.73703.1455
25. Tefera YG, Gebresillassie BM, Emiru YK, Yilma R, Hafiz F, Akalu H, et al. Diabetic health literacy and its association with glycemic control among adult patients with type 2 diabetes mellitus attending the outpatient clinic of a university hospital in Ethiopia. PLoS ONE. (2020) 15:1–15. doi: 10.1371/journal.pone.0231291
26. Huang YM, Shiyanbola OO, Chan HY, Smith PD. Patient factors associated with diabetes medication adherence at different health literacy levels: a cross-sectional study at a family medicine clinic. Postgrad Med. (2020) 132:328–36. doi: 10.1080/00325481.2020.1749499
27. Mukanoheli V, Uwamahoro MC, Mbarushimana V, Meharry P. Functional health literacy and self-care behaviors among type 2 diabetic patients at a university teaching hospital in Kigali. Rwanda J Med Heal Sci. (2020) 3:49–59. doi: 10.4314/rjmhs.v3i1.7
28. Jacobson KL, Faughnan J, Myers L, Dubost A, Courtade L, von Lutcken S, et al. An innovative health literacy approach designed to improve patient understanding of medication labeling. Ther Innov Regul Sci. (2021) 55:1180–92. doi: 10.1007/s43441-021-00325-5
29. de Castro SH, Brito GN, Gomes MB. Health literacy skills in type 2 diabetes mellitus outpatients from an university-affiliated hospital in Rio de Janeiro, Brazil. Diabetol Metab Syndr. (2014) 6:1–5. doi: 10.1186/1758-5996-6-126
30. Thurston MM, Bourg CA, Phillips BB, Huston SA. Impact of health literacy level on aspects of medication nonadherence reported by underserved patients with type 2 diabetes. Diabetes Technol Ther. (2015) 17:187–93. doi: 10.1089/dia.2014.0220
31. Haghdoost AA, Karamouzian M, Jamshidi E, Sharifi H, Rakhshani F, Mashayekhi N, et al. Health literacy among Iranian adults: findings from a nationwide population-based survey in 2015. East Mediterr Heal J. (2019) 25:828–36. doi: 10.26719/emhj.19.017
32. Hussein SH, Almajran A, Albatineh AN. Prevalence of health literacy and its correlates among patients with type II diabetes in Kuwait: a population based study. Diabetes Res Clin Pract. (2018) 141:118–25. doi: 10.1016/j.diabres.2018.04.033
33. Koster ES, Philbert D, Dijk L, Van Rademakers J, Smet PAGM De, Bouvy ML, et al. Research in social and administrative pharmacy recognizing pharmaceutical illiteracy in community pharmacy : agreement between a practice-based interview guide and questionnaire based assessment. Res Soc Adm Pharm. (2018) 14:812–6. doi: 10.1016/j.sapharm.2018.01.009
34. Mohammad AB, Mehdi K. Relationship between health literacy and self-care behaviors in diabetic patients type II referred to the center of diabetes control and prevention in zabol. J Heal Lit. (2018) 3:10–9. doi: 10.22038/jhl.2018.10927
35. Almigbal TH, Almutairi KM, Vinluan JM, Batais MA, Alodhayani A, Alonazi WB, et al. Association of health literacy and self-management practices and psychological factor among patients with type 2 diabetes mellitus in Saudi Arabia. Saudi Med J. (2019) 40:1158–66. doi: 10.15537/smj.2019.11.24585
36. Franzen J, Mantwill S, Rapold R, Schulz PJ. The relationship between functional health literacy and the use of the health system by diabetics in Switzerland. Eur J Public Health. (2013) 24:997–1003. doi: 10.1093/eurpub/ckt202
37. Sangkawichai P, Kamchang P, Paisawaeng K, Wongpimkham P, Saita S, Vittaporn S, et al. Factors associated with health literacy and self-care behaviors among patients with type 2 diabetes: a mixed method study in Ko Kha District, Lampang Province, Northern Thailand. J Heal Res. (2024) 38:301–10. doi: 10.56808/2586-940X.1086
38. Gündogdu S, Kilavuz A. Factors Associated with health literacy and diabetes burden, and the relationship between health literacy and diabetes burden in elderly individuals with type 2 diabetes mellitus. Geriatr Bilim Derg. (2023) 6:20–31. doi: 10.47141/geriatrik.1250884
40. Abdullah A, Ng CJ, Liew SM, Ambigapathy S, V P, Chinna K. Prevalence of limited health literacy and its associated factors in patients with type 2 diabetes mellitus in Perak, Malaysia: a cross-sectional study. BMJ Open. (2020) 10:e039864. doi: 10.1136/bmjopen-2020-039864
41. Charoghchian Khorasani E, Tavakoly Sany SB, Orooji A, Ferns G, Peyman N. Health literacy in Iranian women: a systematic review and meta-analysis. Iran J Public Health. (2020) 49:860–74. doi: 10.18502/ijph.v49i5.3203
42. Yilmazel G, Cici R. Limited health literacy is associated with poorer clinical outcomes in elderly with type 2 diabetes mellitus. Universa Med. (2019) 38:179. doi: 10.18051/UnivMed.2019.v38.179-185
43. Debnath P, Natasha K, Ali L, Bhaduri T, Roy TK, Bera S, et al. Ayurpharmacoepidemiology perspective: health literacy (knowledge and practice) among older diabetes patients visiting ayurveda teaching hospitals in India. J Evidence-Based Complement Altern Med. (2017) 22:242–50. doi: 10.1177/2156587216643641
44. Finbråten HS, Guttersrud Ø, Nordström G, Pettersen KS, Trollvik A, Wilde-Larsson B. Explaining variance in health literacy among people with type 2 diabetes: the association between health literacy and health behaviour and empowerment. BMC Public Health. (2020) 20:1–12. doi: 10.1186/s12889-020-8274-z
45. World Bank. Poverty & Equity Brief: Africa Eastern & Southern Ethiopia [Internet]. (2021). Available at: http://databank.worldbank.org/data/download/poverty/987B9C90-CB9F-4D93-AE8C-750588BF00QA/AM2020/Global_POVEQ_ETH.pdf
Keywords: diabetes, Ethiopia, health literacy, magnitude, Woldia
Citation: Mulugeta Abate H, Kumar P, Anteneah S, Girma M, Yimam W and Desu B (2025) Health literacy and associated factors among adult type 2 diabetic patients in Woldia Comprehensive Specialized Hospital, North-East Ethiopia, 2022. Front. Public Health 13:1502852. doi: 10.3389/fpubh.2025.1502852
Received: 03 December 2024; Accepted: 27 January 2025;
Published: 18 February 2025.
Edited by:
Edson da Silva, Universidade Federal dos Vales do Jequitinhonha e Mucuri, BrazilReviewed by:
Hadi Tehrani, Mashhad University of Medical Sciences, IranSrivani Gowru, University of Cincinnati, United States
Copyright © 2025 Mulugeta Abate, Kumar, Anteneah, Girma, Yimam and Desu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mitaw Girma, Z2lybWFtaXRhdzU1QGdtYWlsLmNvbQ==