
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 27 March 2025
Sec. Public Mental Health
Volume 13 - 2025 | https://doi.org/10.3389/fpubh.2025.1502726
This article is part of the Research Topic Youth Mental Health, Particularly in Asian Populations View all 65 articles
 Lei Li1†
Lei Li1† Jia Cai1†
Jia Cai1† Cong Wang1,2Yun-Fei Mu1,2
Cong Wang1,2Yun-Fei Mu1,2 Zhong-Yue Deng1,2Ai-Ping Deng1,3Hong-Jun Song1,3
Zhong-Yue Deng1,2Ai-Ping Deng1,3Hong-Jun Song1,3 Xue-Hua Huang1
Xue-Hua Huang1 Li Yin1
Li Yin1 Yi Huang1,2
Yi Huang1,2 Jin Chen4
Jin Chen4 Jun-Shu Zhao5Bing-Zhi Zhang5Hao Li5
Jun-Shu Zhao5Bing-Zhi Zhang5Hao Li5 Mao-Sheng Ran1,2*
Mao-Sheng Ran1,2*Background: School bullying poses a serious threat to the mental well-being of adolescents. Although previous research has demonstrated a link between school bullying and internet addiction, the psychological mechanism remains poorly understood. This study aimed to explore the mediating roles of depressive and anxiety symptoms, as well as the moderating role of the stigma of mental illness.
Methods: A cross-sectional survey among 82,873 middle and high school, college, and university students in Sichuan Province, China, was conducted for this study. Moderated mediation models were examined using PROCESS macros in SPSS 26.0.
Results: The school bullying was positively correlated with internet addiction, with depression and anxiety symptoms partially mediating internet addiction, respectively. The stigma of mental illness significantly moderated this relationship, revealing a stronger association between school bullying, depression and anxiety symptoms, and internet addiction for adolescents with higher levels of stigma.
Conclusions: These findings emphasize the importance of addressing depressive and anxiety symptoms as well as stigma of mental illness in interventions to prevent school bullying and internet addiction. Programs tailored to these factors are crucial for alleviating the negative impacts of school bullying on the mental health and online behaviors of adolescents.
School bullying is a global phenomenon that threatens the health of adolescent students including the problems of verbal, physical, relational and cyberbullying (1). Extensive research has documented the detrimental effects of school bullying on adolescent development. Evidence from 28 western countries suggests that ~41% of adolescents may be victims of school bullying, which is strongly associated with psychological problem among adolescent students, such as, depression, anxiety, loneliness and sleep disorders (2–5). School bullying can lead to decreased academic performance and increased use of violence and substance abuse by victims and bullies (6–8). Internet addiction has also been considered one of those negative outcomes of school bullying, and the relationship between bullying and Internet addiction is firmly supported (9).
The incidence of Internet addiction is increasing, and there are gender differences (10, 11). Internet addiction can be defined as the uncontrolled internet use despite its negative impact (12, 13). Studies showed that Internet addiction has negative effects on well-being of adolescents, including psychological distress and decreased life satisfaction (14, 15). The self-medication hypothesis posits that individuals who have experienced stressful events tend to rely on substances and drugs to avoid a series of adverse consequences (16). Drawing on this framework, excessive internet use may function as a maladaptive coping strategy analogous to substance abuse, providing temporary relief from bullying-related distress (17). In other words, problematic internet usage may be associated with school bullying. When individuals are bullied by their peers, they may immerse themselves in online activities to avoid being bullied repeatedly and to cope with the negative effects of being bullied (18).
Victims of school bullying may perceive themselves in negative light, triggering not only a sense of sham but also low self-worth and feelings of depression (19–21). Ample evidence strongly supports the relationship between being bullied and adverse mental health outcomes such as depressive and anxiety symptoms (22–24). For example, individuals who have experienced bullying were closely associated with poor psychosocial outcomes, even after adjusting for the impact of initial psychosocial stress (23). A meta-analysis also showed that compared with those who have not experienced school bullying, victims who were bullied at the age of 8 were 1.94 times more likely to exhibit anxiety or depression symptoms at the age of 9 (25). Online social activities are a common coping strategy for individuals with anxiety and depression to relieve negative emotions (26). However, the psychological pathways linking school bullying to internet addiction remain insufficiently explored, particularly regarding potential moderating factors that may exacerbate this relationship. Further studies should be conducted to explore the relationship between school bullying and internet addiction.
Stigma of mental illness may exacerbate the psychological distress of victims of school bullying (27). Childhood abuse and victimization may be key factors influencing the perceived stigma of mental illness in patients (28). Evidence showed that stigma of mental illness among individuals with experiences of school bullying may exacerbate psychological distress (29–32). The stigma of mental illness may reduce self-esteem and is related to depressive and anxiety symptoms as well as deliberate self-harm (33, 34). Studies showed that individuals may use online activities (e.g., internet use) to cope with their psychological distress, such as stigma of mental illness (35, 36). The stigma of mental illness may intensify the relationship between school bullying and internet addiction. However, few studies have been conducted to identify the relationship among stigma of mental illness, school bullying, symptoms of depression and anxiety, and internet addiction.
Thus, this study aimed to explore the underlying mechanisms between school bullying and internet addiction, as well as the relationships among stigma of mental illness, school bullying, depression, anxiety and internet addiction in adolescents. In this study, we hypothesized that: First, school bullying may be positively associated with internet addiction; Second, the depression and anxiety symptoms may play mediating roles the relationship between school bullying and internet addiction, respectively; Third, the stigma of mental illness moderates the relationships among school bullying, depression, anxiety and internet addiction.
We conducted a large-scale online survey among students in Sichuan province, China, from December 14th, 2022 to February 28th, 2023. The multi-stage cluster sampling procedure recruited 90,118 students from 162 educational institutions across Sichuan Province, including junior middle school, senior high school, and universities. Before completing the survey, we acquired all participants to provide online informed consent. Teachers and professors distributed the questionnaires to students via Quick Response (QR) code. This study was approved by the Ethics Committee of West China Hospital, Sichuan University (NO. 2022-1970).
Sociodemographic information, including gender, age, ethnicity, grade, family income, and the only child status was collected. Detailed demographic information and related factors were described in our previous study (37).
School bullying was assessed by the Chinese version of the Program for International Student Assessment (PISA), a 6-item self-report questionnaire (e.g., “Other students left me out of things on purpose”). Responses were ranked on a 4-point scale (0 = never or almost never; 1 = several times a year; 2 = several times a month; 3 = Once a week or more). Total scores ranged from 0 to18. The PISA has been proven to be reliable and valid (38). In this study, the Cronbach's coefficient for the PISA was 0.918, indicating excellent internal consistency.
Depressive symptoms were evaluated by using the Chinese version of 9-item Patient Health Questionnaire (PHQ-9), which is a self-report questionnaire assessing the severity of depression. Each item was scored on a 4-point Likert scale (range: 0–3). The total scores range from 0 to 27. The PHQ-9 has been proven to be reliable and valid (39, 40). In this study, Cronbach's coefficient for the PHQ-9 was 0.948.
The Chinese version of the Generalized Anxiety Disorder 7-item (GAD-7) scale was used to assess participants' anxiety symptoms. It is a self-report questionnaire for evaluating the severity of anxiety. Each item was scored on a 4-point Likert scale (range: 0–3). The total scores range from 0 to 21. The GDA-7 has been demonstrated to be reliable and valid (41, 42). In this study, Cronbach's coefficient of the GAD-7 was 0.968.
Stigma of mental illness used to assess a adapted version of Link's Perceived Discrimination-Devaluation Scale (LPDDS) (43, 44). The LPDDS is a 13-item self-report questionnaire for assessing the severity of perceived stigma of mental illness. Responses were reported on a 4-point Likert scale, labeled “Strongly Agree” to “Strongly Disagree”. Scores were summed for each item (ranges: LPDDS = 13-52). This scale has good reliability in the general Chinese population (44). In this study, Cronbach's coefficient for the LPDDS was 0.926.
The 20-item Internet Addiction Test (IAT) (45), self-report questionnaire was used to assess Internet addiction. Each item was scored on a 5-point Likert scale (range: 1–5). The total scores ranged from 20 to 100, with a higher score indicating a higher level of internet addiction. The total score ≥40 was defined as internet addiction. The Chinese version of IAT has been proven to be reliable and valid (46). In this study, it had good internal consistency, with a Cronbach's alpha coefficient of 0.956.
Statistical analyses were performed using SPSS 26.0. Descriptive analysis was used to summarize the basic demographic characteristics of the study subjects. For categorical variables, frequencies (n) and percentages (%) were presented, while for continuous variables, mean and standard deviation (SD) were included. The relationships between school bullying, depressive symptoms, anxiety symptoms, Internet addiction, and the stigma of mental illness were initially examined using the Pearson correlation coefficient.
Based on the hypotheses, we conducted mediation and moderated mediation analyses using the SPSS PROCESS v3.5 software developed by Andrew F. Hayes (47). Specifically, PROCESS Model 4 was employed to test the mediation model, with school bullying as independent variable (X), depression and anxiety as mediating variables (M), respectively, and internet addiction as dependent variable (Y).
We utilized PROCESS Model 59 to test the moderated mediation in the conceptual model (Figure 1) where stigma of mental illness served as the moderator variable (W). We defined two values for the stigma of mental illness: a low level (one standard deviation below the mean) and a high level (one standard deviation above the mean), to examine significant moderating effect. Additionally, simple slope computations were carried out for the moderation models to test the significance of the moderation slopes. To simulate the random sampling process and ensure the credibility of the study results, we used repeated sampling statistical method to verify the indirect effect of variable (48). This approach allowed us to estimate the variability of our results and provide a more accurate representation of the relationships among the study variables.
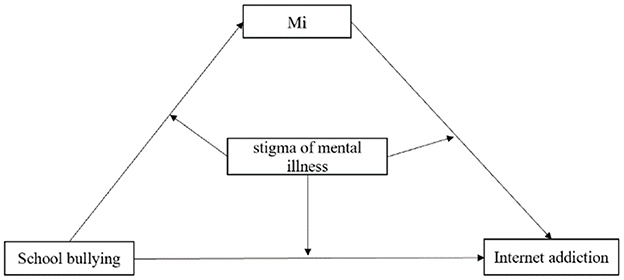
Figure 1. Hypothesized conceptual model of the moderated mediation. Mi represents mediating variables such as depression symptoms and anxiety symptoms.
In total, 82,873 students (92.0 %) provided informed consent and completed the questionnaire survey, while 7245 students (8.0 %) refused to participate. There were 47,487 female students (57.3%), 73,537 Han nationality students (88.7%), and 20,471 only-child students (24.7%). A total of 48,451 students (58.5%) had a monthly family income of less than 4,999 RMB. Table 1 shows the demographic characteristics of the participants in this study.
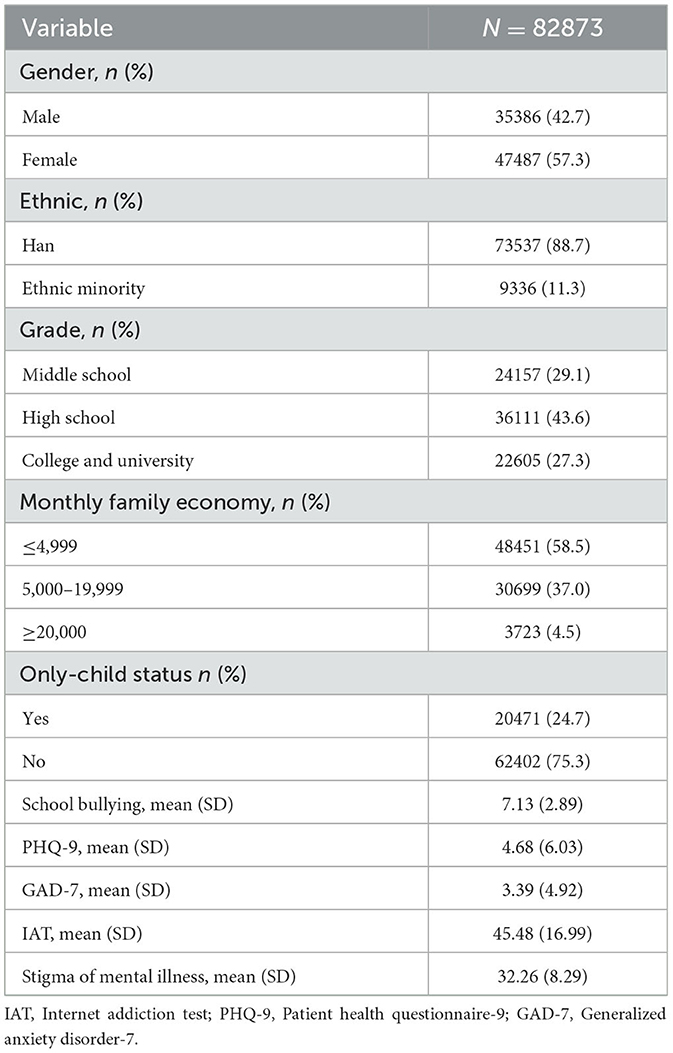
Table 1. Characteristics of the study participants.
Inter-correlations of all variables are presented in Table 2. Generally, school bullying was significantly positively associated with depressive symptoms (r = 0.409, p < 0.01), anxiety symptoms (r = 0.407, p < 0.01), and internet addiction (r = 0.261, p < 0.01). Depressive symptoms (r = 0.445, p < 0.01) and anxiety symptoms (r = 0.413, p < 0.01) were positively associated with internet addiction, respectively. Additionally, the stigma of mental illness was positively related to school bullying (r = 0.070, p < 0.01), depressive symptoms (r = 0.089, p < 0.01), anxiety symptoms (r = 0.089, p < 0.01), and internet addiction (r = 0.014, p < 0.01).
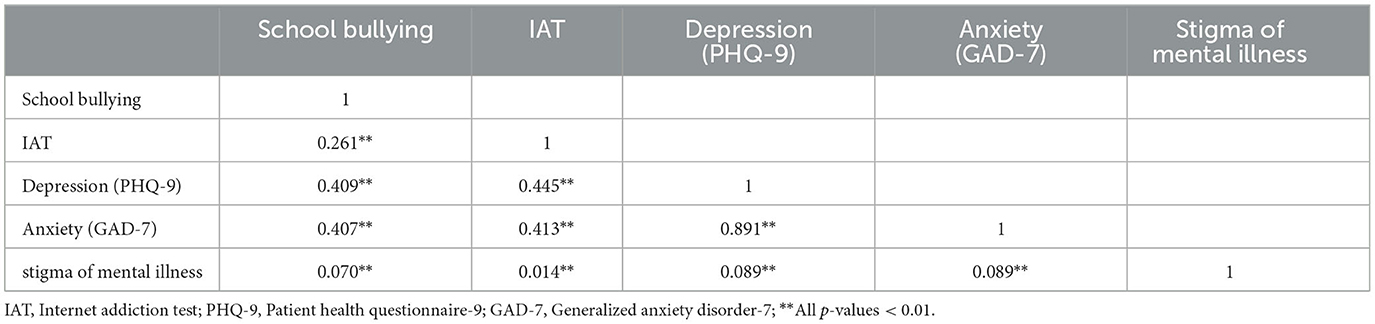
Table 2. Correlations between school bullying, internet addiction, depression and anxiety symptoms, and perceived stigma of mental illness.
Figure 2 showed the results of mediation analyses. As shown in Figure 2a, school bullying was positively associated with depression (β = 0.85, p < 0.0001), which in turn was positively associated with internet addiction (β = 1.14, p < 0.0001). The direct relationship between school bullying and internet addiction was also significant (β = 1.53, p < 0.0001), indicating that depression partially mediated the linking between school bullying and internet addiction (Supplementary Table 1). The indirect effect between school bullying and internet addiction was also significant (indirect effect = 0.97, 95% CI = 0.95–1.00, which accounted for 64.3% of the total effect) (Supplementary Table 2).

Figure 2. Path coefficients for the mediation model. (a) Mediating variable was depression, (b) mediating variable was anxiety. For each connecting line, the standard regression coefficient between those variables was shown. The 5,000-percentile bootstrapped standard error of each regression coefficient was shown in brackets. ***p < 0.0001.
In additional, Figure 2b showed that school bullying was positively associated with anxiety (β = 0.69, p < 0.0001), which in turn was positively associated with internet addiction (β = 1.27, p < 0.0001). The direct relationship between school bullying and internet addiction was also significant (β = 1.53, p < 0.0001), indicating that anxiety partially mediate the linking between school bullying and internet addiction (Supplementary Table 3). The indirect effect between school bullying and internet addiction was significant (indirect effect = 0.88, 95% CI = 0.85-0.90, which accounted for 57.5% of the total effect) (Supplementary Table 4).
Stigma of mental illness can act as an “amplifier” to significantly enhance the negative effects between school bullying, depression, anxiety and internet addiction. As shown in Figure 3, the results of the moderated mediation analyses. In the Figure 3a, firstly, the stigma of mental illness moderated the mediating effect of depression between school bullying and internet addiction, and the interaction effect of school bullying and the stigma of mental illness on internet addiction was significant (β = 0.007, p < 0.0001), which indicates that the stigma of mental illness moderated the direct path between school bullying and Internet addiction. Secondly, the interaction effect of school bullying and the stigma of mental illness on depression was significant (β = 0.008, p < 0.0001), suggesting that the stigma of mental illness moderated the indirect path between school bullying and depression. Thirdly, the interaction effect of depression and the stigma of mental illness on internet addiction was significant (β = 0.008, p < 0.0001), indicating that the indirect path between depression and internet addiction was moderated by the stigma of mental illness (Supplementary Table 5).
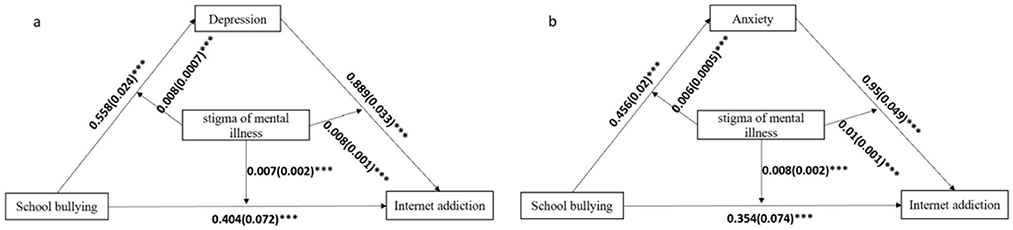
Figure 3. Path coefficients for the moderated mediation model. (a) Mediating variable was depression, (b) mediating variable was anxiety. For each connecting line, the standard regression coefficient between those variables was shown. The 5,000-percentile bootstrapped standard error of each regression coefficient was shown in brackets. ***p < 0.0001.
In the Figure 3b, the stigma of mental illness moderated the mediating effect of anxiety between school bullying and internet addiction, and the interaction effect of school bullying and stigma of mental illness on internet addiction was significant (β = 0.008, p < 0.0001). The stigma of mental illness moderated the direct path between school bullying and Internet addiction. Secondly, the interaction effect of school bullying and the stigma of mental illness on anxiety was significant (β = 0.006, p < 0.0001), indicating that the stigma of mental illness might moderate the indirect path between school bullying and anxiety. Thirdly, the interaction effect of anxiety and stigma of mental illness on internet addiction was significant (β = 0.010, p < 0.0001), indicating that the indirect path between anxiety and internet addiction was moderated by the stigma of mental illness (Supplementary Table 6).
The Figure 4 showed that, regardless of whether a simple slope analysis was conducted for the low or high stigma levels of mental illness, school bullying had a significant positive impact on Internet addiction. Under the low stigma level of mental illness, the effect was smaller, indicating that as the stigma of mental illness decreased, the likelihood of Internet addiction when being bullied also decreased (Figures 4a, d). Secondly, at both high and low levels of stigma, the indirect effects of school bullying on Internet addiction through depressive and anxiety symptoms were statistically significant, and the indirect effects gradually decreased as the stigma level decreased. This showed that as the stigma of mental illness decreases, the impact of school bullying on depressive and anxiety symptoms can be effectively alleviated (Figures 4b, e). Finally, depressive symptoms had a significant positive impact on Internet addiction in the high stigma group, and depressive symptoms also had a significant positive impact on Internet addiction in the low stigma group (Figure 4c). Similarly, in the high stigma mental illness group, the impact of anxiety symptoms on Internet addiction was significantly higher than that in the low stigma mental illness group (Figure 4f).
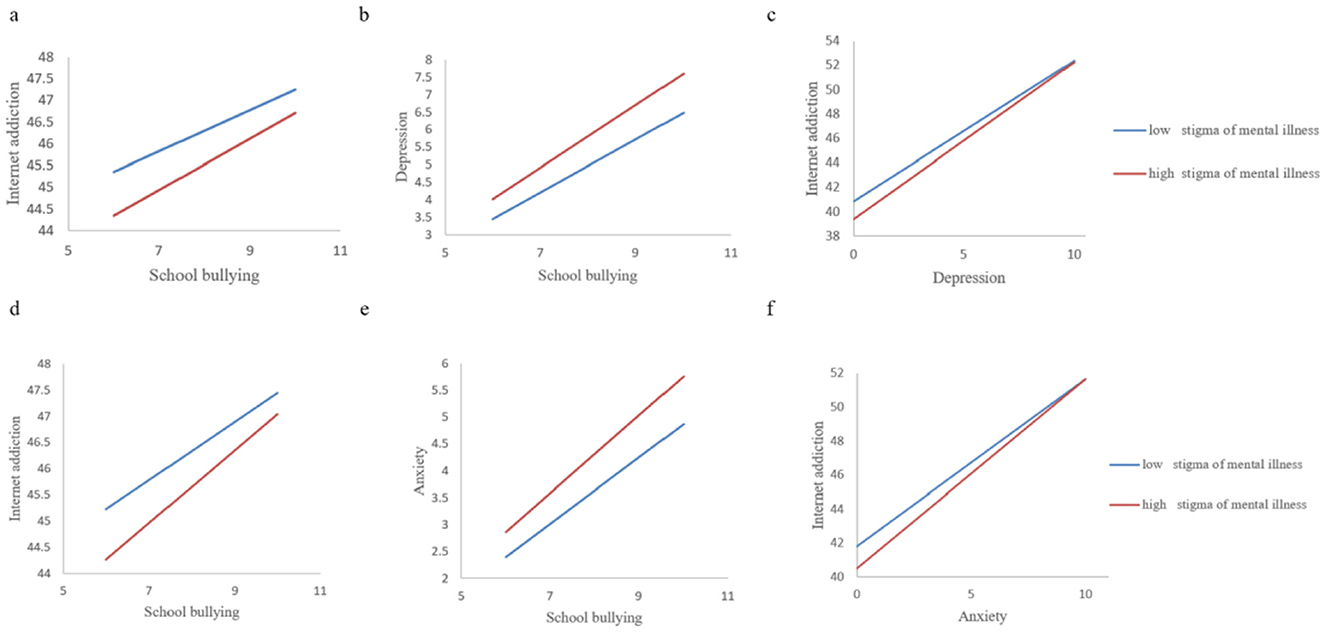
Figure 4. Moderation of the effect of stigma of mental illness between school bullying on internet addiction. (a) Stigma of mental illness moderated the relationship between school bullying and internet addiction. (b) Stigma of mental illness moderated the relationship between school bullying and depression. (c) Stigma of mental illness moderated the relationship between depression and internet addiction. (d) Stigma of mental illness moderated the relationship between school bullying and internet addiction. (e) Stigma of mental illness moderated the relationship between school bullying and anxiety. (f) Stigma of mental illness moderated the relationship between anxiety and internet addiction.
This study extends prior research by systematically examining how stigma of mental illness moderates the mediated pathways linking school bullying to internet addiction through depression and anxiety—a novel contribution to the literature. Our results fully confirmed the first and second hypotheses, demonstrating that school bullying is linked to internet addiction, and that symptoms of depression and anxiety mediate this association. Furthermore, we found that the stigma of mental illness moderates the association among school bullying, depression and anxiety symptoms, and internet addiction, which fully supports the third hypothesis. Specifically, although there is a strong relationship among school bullying, depression and anxiety symptoms as well as internet addiction, the linkage between those variables were stronger when the level of stigma of mental illness was high.
The results of this study demonstrate the link between school bullying and internet addiction, consistent with previous studies (49). Adolescents who experiencing bullying may be more likely to develop internet addiction as a coping mechanism, using online using online platforms to manage negative emotions, establish virtual relationships, and compensate for a lack of social connections in the real world. These behaviors may provide a sense of belonging and escape from the distress caused by bullying (50). Bullying has become one of the causes for the increase in psychological and medical problems. The necessity to prevent bullying incidents from recurring and to stop bullies from further harassing the victims has grown (51). These findings underscore the importance of developing psychosocial services and interventions to reduce school bullying and prevent internet addiction among adolescents.
The mediating effect analysis revealed that symptoms of depressive and anxiety play pivotal roles in the relationship between school bullying and internet addiction. Specifically, school bullying increases the risk of depression and anxiety symptoms, and these symptoms, in turn, increase the risk of Internet addiction. This finding is consistent with previous research, which indicates a strong association between school bullying and mental health problems (2, 52, 53).
Adolescents experiencing bullying in the early school years reported negative emotions, such as depression or anxiety. They are often associated with the bullying incidents (54). Several mechanisms may underline the relationships between school bullying and mental health problems. Firstly, being bullied disrupts emotional regulation, leading to an increase in negative emotions and impaired emotion management, thus contributing to the occurrence of internalized anxiety and depression problems (55). Secondly, being bullying fosters rumination. Through continuous negative thoughts and fears about the bullying experience, rumination can lead to an increase in depressive and anxiety symptoms (56). Thirdly, bulling can affect adulthood through a stress process model. The traumatic stress caused by bullying can alter stress responses, leading to a long-term increase in inflammatory processes, overwhelming the psychological and biological stress processes of the victims (57).
Depressive and anxiety symptoms can have numerous negative consequences, including sleep disturbance, and internet addiction (58, 59). Students who have experienced school bullying may prefer to communicate with others through social media platforms, sharing their bullying experiences and seeking comfort, rather than interacting with familiar individuals in the real world, particularly when they feel an increased sense of loneliness (60). These findings emphasize the need for psychosocial interventions to reduce internet addiction, depression and anxiety symptoms, and improve the mental health outcomes among students who have experienced school bullying. By addressing the underlying mechanisms and consequences of school bullying, interventions can be tailored to meet the specific needs of this vulnerable population.
A key finding of this study was that the stigma of mental illness plays a moderating role in the relationship between school bullying, depression and anxiety symptoms, and internet addiction among adolescent students. It is noteworthy that both high and low levels of stigma of mental illness were positively correlated with anxiety, depression and Internet addiction. However, the positive association with mental illness was stronger at the high level of stigma, suggesting that a high level of stigma may exacerbate the relationships between school bullying, mental health problems, and internet addiction. This finding is consistent with existing research which demonstrates a link between the stigma of mental illness and various forms of psychological distress (30, 31). An intensified stigma associated with mental illness may lead to increased vulnerability to negative psychological outcomes, such as depression and anxiety, among these who have experienced school bullying. In addition, a high level of stigma may also contribute to increased online activities and decreased help-seeking behaviors, including reluctance to receive psychological or pharmacological treatment (61).
The results of this study underscore the critical role of stigma of mental illness in the complex relationships among school bullying, depression and anxiety, and internet addiction. The differential moderating effects of stigma suggest that interventions should adopt a tiered approach: universal anti-bullying programs for all students, combined with targeted stigma-reduction strategies for high-risk subgroups exhibiting elevated psychological distress (62). By addressing the moderating effect of stigma, interventions can be designed to more effectively mitigate the negative consequences of school bullying and promote mental health and well-being among students (63).
In this study, we utilized the LPDDS to assess stigma of mental illness, which specifically measures perceived stigma rather than internal stigma. It is noteworthy that victims of bullying often experience severe emotional distress due to psychological and physical violence, as well as social marginalization among their peers (64). This can lead to the development of a negative self-concept, decreased self-esteem, and perceived weakness (65). Research showed that individuals who perceive a higher degree of stigma are more likely to internalize and self-stigmatize (66). Both perceived and self-stigma can have deleterious effects on students' psychological well-being, treatment-seeking behaviors, and academic performance (67).
This study has significant implications for clinical practice. Firstly, it highlights the importance of considering experiences of school bullying as well as depression and anxiety symptoms when addressing students' internet addiction. The implementation of anti-bullying programs and intervention techniques has been shown to be effective in reducing bullying and victimization (68, 69). Given the crucial role that depressive and anxiety symptoms play in linking school bullying to internet addiction, it is essential to take actions to help students manage these symptoms and enhance treatment outcomes.
This study has several limitations that should be acknowledged. As a cross-sectional study, we are unable to determine the causal relationships among variables. Future research could adopt a longitudinal design or an experimental design to further validate these relationships. While the large sample size enhances statistical power, the regional focus on Sichuan Province—an area with specific socioeconomic and educational characteristics—may limit the generalizability of findings to other cultural contexts. Future studies could be conducted in other regions or countries to verify whether our findings are widely applicable. Although we employed validated scales to minimize measurement error, the cross-sectional design precludes causal inferences, and self-reports may be influenced by recall bias or underreporting of stigmatized experiences. We believe that the large sample size, the validated scales, and the innovative introduction of 'stigma of mental illness' as a moderating variable have provided a solid theoretical foundation and empirical support for our research. We look forward to future research that further explores these complex relationships and employs multiple data collection methods to enhance the reliability of the research results.
This study contributes to understanding the associative mechanisms between school bullying and internet addiction. It explores the mediating roles of depressive and anxiety symptoms, as well as the moderating role of the stigma of mental illness. Depressive symptoms and anxiety symptoms play mediating roles between school bullying and internet addiction, respectively. Notably, the mediating effects of both depressive and anxiety symptoms were stronger for among students who report a higher level of stigma related to mental illness. These results point out that when formulating and implementing effective interventions for students who have suffered from school bullying, there is an urgent need to address depressive and anxiety symptoms and reduce the stigmatization of mental health.
The data analyzed in this study is subject to the following licenses/restrictions: The de-identified data are available on reasonable request to the corresponding author. Requests to access these datasets should be directed to bXNyYW5jZEBvdXRsb29rLmNvbQ==.
The studies involving humans were approved by the West China Hospital, Sichuan University has an Ethics Committee and provided ethical approval for this study (NO. 2022-1970). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants' legal guardians/next of kin.
LL: Formal analysis, Investigation, Methodology, Software, Writing – original draft. JCa: Data curation, Investigation, Project administration, Writing – review & editing. CW: Investigation, Supervision, Writing – review & editing. Y-FM: Conceptualization, Data curation, Writing – review & editing. Z-YD: Investigation, Project administration, Writing – review & editing. A-PD: Investigation, Supervision, Writing – review & editing. H-JS: Investigation, Supervision, Writing – review & editing. X-HH: Visualization, Writing – review & editing. LY: Validation, Writing – review & editing. YH: Data curation, Writing – review & editing. JCh: Investigation, Supervision, Validation, Writing – review & editing. J-SZ: Investigation, Project administration, Writing – review & editing. B-ZZ: Investigation, Resources, Writing – review & editing. HL: Methodology, Resources, Writing – review & editing. M-SR: Conceptualization, Funding acquisition, Methodology, Project administration, Resources, Writing – review & editing.
The author(s) declare that financial support was received for the research and/or publication of this article. This study was supported by the Initial Research Fund, West China Hospital (WCH, No: 136220012, PI: M-SR).
The authors would like to acknowledge the support of the all schools where this research was conducted.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Gen AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1502726/full#supplementary-material
1. Olweus D. School bullying: development and some important challenges. Annu Rev Clin Psychol. (2013) 9:751–80. doi: 10.1146/annurev-clinpsy-050212-185516
2. Klomek AB, Kleinman M, Altschuler E, Marrocco F, Amakawa L, Gould MS. High school bullying as a risk for later depression and suicidality. Suicide Life Threat Behav. (2011) 41:501–16. doi: 10.1111/j.1943-278X.2011.00046.x
3. Gong Z, Reinhardt JD, Han Z, Ba Z, Lei S. Associations between school bullying and anxiety in children and adolescents from an ethnic autonomous county in China. Psychiatry Res. (2022) 314:114649. doi: 10.1016/j.psychres.2022.114649
4. Liang Y, Wang Q, Chen J, Zhang Y, Li S, Xiong M, et al. profiles and transitions of loneliness and depressive symptoms among migrant children: predictive role of bullying victimization. J Youth Adolesc. (2023) 52:2606–19. doi: 10.1007/s10964-023-01847-x
5. Ding H, Cao L, Xu B, Li Y, Xie J, Wang J, et al. Involvement in bullying and sleep disorders in Chinese early adolescents. Front Psychiatry. (2023) 14:1115561. doi: 10.3389/fpsyt.2023.1115561
6. Ringdal R, Espnes GA, Eilertsen MEB, BjØrnsen HN, Moksnes UK. Social support, bullying, school-related stress and mental health in adolescence. Nordic Psychol. (2020) 72:1–18. doi: 10.1080/19012276.2019.1710240
7. Zhang XiaoYan ZX, Ra ChaeLin Ra C, Zhang DongLan ZD, Zhang YunTing ZY, MacLeod KE. The impact of school social support and bullying victimization on psychological distress among California adolescents. Calif J Health Promot. (2016) 14:56–67. doi: 10.32398/cjhp.v14i2.1875
8. Bowes L, Joinson C, Wolke D, Lewis G. Peer victimisation during adolescence and its impact on depression in early adulthood: prospective cohort study in the United Kingdom. BMJ. (2015) 350:h2469. doi: 10.1136/bmj.h2469
9. Vessey JA, Difazio RL, Neil LK, Dorste A. Is there a relationship between youth bullying and internet addiction? An integrative review. Int J Ment Health Addict. (2022) 2022:1–25. doi: 10.1007/s11469-021-00731-8
10. Lozano-Blasco R, Robres AQ, Sánchez AS. Internet addiction in young adults: A meta-analysis and systematic review. Comput Human Behav. (2022) 130:107201. doi: 10.1016/j.chb.2022.107201
11. Mari E, Biondi S, Varchetta M, Cricenti C, Fraschetti A, Pizzo A, et al. Gender differences in internet addiction: a study on variables related to its possible development. (2023) 9:100247. doi: 10.1016/j.chbr.2022.100247
12. Tang D, Wei F, Qin B, Liu T, Zhou M. coooolll: a deep learning system for twitter sentiment classification*. In: Proceedings of the 8th international workshop on semantic evaluation (SemEval 2014) (2017), 208–12.
13. Deng AP, Wang C, Cai J, Deng ZY, Mu YF, Song HJ, et al. Effects of internet addiction and academic satisfaction on mental health among college students after the lifting of COVID-19 restrictions in China. Front Psychiatry. (2023) 14:1243619. doi: 10.3389/fpsyt.2023.1243619
14. Giumetti GW, Kowalski RM. Cyberbullying via social media and well-being. Curr Opin Psychol. (2022) 45:101314. doi: 10.1016/j.copsyc.2022.101314
15. Bansal S, Garg N, Singh J, Van Der Walt F. Cyberbullying and mental health: past, present and future. Front Psychol. (2023) 14:1279234. doi: 10.3389/fpsyg.2023.1279234
16. Cappell H. Alcohol and Tension Reduction: An Update on Research and Theory (1987). New York City: Guilford Press.
17. Hsieh YP, Shen ACT, Wei HS, Feng JY, Huang SCY, Hwa HL. Associations between child maltreatment, PTSD, and internet addiction among Taiwanese students. Comput. Human Behav. (2016) 56:209–14. doi: 10.1016/j.chb.2015.11.048
18. Zhai B, Li D, Jia J, Liu Y, Sun W, Wang Y. Peer victimization and problematic internet use in adolescents: The mediating role of deviant peer affiliation and the moderating role of family functioning. Addict Behav. (2019) 96:43–9. doi: 10.1016/j.addbeh.2019.04.016
19. Modin B, Låftman SB, Östberg V. Bullying in context: an analysis of psychosomatic complaints among adolescents in Stockholm. J School Violence. (2014) 14:382–404. doi: 10.1080/15388220.2014.928640
20. Östberg V, Modin B, Låftman SB. Exposure to school bullying and psychological health in young adulthood: a prospective 10-year follow-up study. J School Violence. (2018) 17:194–209. doi: 10.1080/15388220.2017.1296770
21. Lai S, Li J, Shen C, Zhang S, Yang Y, Zhang X, et al. School bullying victimization and depression symptoms in adolescents: the mediating role of internet addiction and moderating role of living areas. Psychiatr Q. (2024) 95:481–96. doi: 10.1007/s11126-024-10083-w
22. Boyes ME, Bowes L, Cluver LD, Ward CL, Badcock NA. Bullying victimisation, internalising symptoms, and conduct problems in South African children and adolescents: a longitudinal investigation. J Abnorm Child Psychol. (2014) 42:1313–24. doi: 10.1007/s10802-014-9888-3
23. Arseneault L, Bowes L, Shakoor S. Bullying victimization in youths and mental health problems: 'much ado about nothing'? Psychol Med. (2010) 40:717–29. doi: 10.1017/S0033291709991383
24. Fekkes M, Pijpers FI, Fredriks AM, Vogels T, Verloove-Vanhorick SP. Do bullied children get ill, or do ill children get bullied? A prospective cohort study on the relationship between bullying and health-related symptoms. Pediatrics. (2006) 117:1568–74. doi: 10.1542/peds.2005-0187
25. Reijntjes A, Kamphuis JH, Prinzie P, Telch MJ. Peer victimization and internalizing problems in children: a meta-analysis of longitudinal studies. Child Abuse Negl. (2010) 34:244–52. doi: 10.1016/j.chiabu.2009.07.009
26. Firth J, Torous J, Nicholas J, Carney R, Rosenbaum S, Sarris J. Can smartphone mental health interventions reduce symptoms of anxiety? A meta-analysis of randomized controlled trials. J Affect Disord. (2017) 218:15–22. doi: 10.1016/j.jad.2017.04.046
27. Boyes ME, Pantelic M, Casale M, Toska E, Newnham E, Cluver LD. Prospective associations between bullying victimisation, internalised stigma, and mental health in South African adolescents living with HIV. J Affect Disord. (2020) 276:418–23. doi: 10.1016/j.jad.2020.07.101
28. Corrigan PW, Rao D. On the self-stigma of mental illness: stages, disclosure, and strategies for change. Can J Psychiatry. (2012) 57:464–9. doi: 10.1177/070674371205700804
29. Cheng CM, Chang CC, Wang JD, Chang KC, Ting SY, Lin CY. Negative impacts of self-stigma on the quality of life of patients in methadone maintenance treatment: the mediated roles of psychological distress and social functioning. Int J Environ Res Public Health. (2019) 16:1299. doi: 10.3390/ijerph16071299
30. Chan KL, Lee CS, Cheng CM, Hui LY, So WT, Yu TS, et al. Investigating the relationship between weight-related self-stigma and mental health for overweight/obese children in Hong Kong. J Nerv Ment Dis. (2019) 207:637–41. doi: 10.1097/NMD.0000000000001021
31. Ahorsu DK, Lin CY, Imani V, Griffiths MD, Su JA, Latner JD, et al. A prospective study on the link between weight-related self-stigma and binge eating: Role of food addiction and psychological distress. Int J Eat Disord. (2020) 53:442–50. doi: 10.1002/eat.23219
32. McKeague L, Hennessy E, O'Driscoll C, Heary C. Retrospective accounts of self-stigma experienced by young people with attention-deficit/hyperactivity disorder (ADHD) or depression. Psychiatr Rehabil J. (2015) 38:158–63. doi: 10.1037/prj0000121
33. McMahon EM, Reulbach U, Corcoran P, Keeley HS, Perry IJ, Arensman E. Factors associated with deliberate self-harm among Irish adolescents. Psychol Med. (2010) 40:1811–9. doi: 10.1017/S0033291709992145
34. Dolezal L. Shame anxiety, stigma and clinical encounters. J Eval Clin Pract. (2022) 28:854–60. doi: 10.1111/jep.13744
35. Brand M, Young KS, Laier C, Wölfling K, Potenza MN. Integrating psychological and neurobiological considerations regarding the development and maintenance of specific Internet-use disorders: an Interaction of Person-Affect-Cognition-Execution (I-PACE) model. Neurosci Biobehav Rev. (2016) 71:252–66. doi: 10.1016/j.neubiorev.2016.08.033
36. Brand M, Wegmann E, Stark R, Müller A, Wölfling K, Robbins TW, et al. The Interaction of Person-Affect-Cognition-Execution (I-PACE) model for addictive behaviors: update, generalization to addictive behaviors beyond internet-use disorders, and specification of the process character of addictive behaviors. Neurosci Biobehav Rev. (2019) 104:1–10. doi: 10.1016/j.neubiorev.2019.06.032
37. Ran MS, Wang C, Cai J, Deng ZY, Mu YF, Huang Y, et al. The mutual overlapping impact of stress and infection on mental health problems in adolescents and youths during and after COVID-19 pandemic in China. J Affect Disord. (2024) 347:500–8. doi: 10.1016/j.jad.2023.12.009
38. OECD. PISA 2012 Results: Ready to Learn. Students' Engagement, Drive and Self-Beliefs (Volume III). Paris: OECD Publishing (2012).
39. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. (2001) 16:606–13. doi: 10.1046/j.1525-1497.2001.016009606.x
40. Sun XY, Li YX, Yu CQ, Li LM. [Reliability and validity of depression scales of Chinese version: a systematic review]. Zhonghua Liu Xing Bing Xue Za Zhi. (2017) 38:110–6. doi: 10.3760/cma.j.issn.0254-6450.2017.01.021
41. Shih YC, Chou CC, Lu YJ, Yu HY. Reliability and validity of the traditional Chinese version of the GAD-7 in Taiwanese patients with epilepsy. J Formos Med Assoc. (2022) 121:2324–30. doi: 10.1016/j.jfma.2022.04.018
42. Zhang C, Wang T, Zeng P, Zhao M, Zhang G, Zhai S, et al. Reliability, validity, and measurement invariance of the general anxiety disorder scale among chinese medical university students. Front Psychiatry. (2021) 12:648755. doi: 10.3389/fpsyt.2021.648755
43. Link BG, Struening EL, Neese-Todd S, Asmussen S, Phelan JC. On Describing and Seeking to Change the Experience of Stigma. J Psychiatr Rehabil Skills. (2002) 6:201–31. doi: 10.1080/10973430208408433
44. Chan SKW, Tam WWY, Lee KW, Hui CLM, Chang WC, Lee EHM, et al. A population study of public stigma about psychosis and its contributing factors among Chinese population in Hong Kong. Int J Soc Psychiatry. (2016) 62:205–13. doi: 10.1177/0020764015621941
45. Young KS. Internet Addiction: The emergence of a new clinical disorder. Cyberpsychol Behav. (2009) 1:237–44. doi: 10.1089/cpb.1998.1.237
46. Lai CM, Mak KK, Watanabe H, Ang RP, Pang JS, Ho RC. Psychometric properties of the internet addiction test in Chinese adolescents. J Pediatr Psychol. (2013) 38:794–807. doi: 10.1093/jpepsy/jst022
47. Hayes AF. An index and test of linear moderated mediation. Multivariate Behav Res. (2015) 50:1–22. doi: 10.1080/00273171.2014.962683
48. Hayes AF, Preacher KJ. Quantifying and testing indirect effects in simple mediation models when the constituent paths are nonlinear. Multivariate Behav Res. (2010) 45:627–60. doi: 10.1080/00273171.2010.498290
49. Lo CK, Ho FK, Emery C, Chan KL, Wong RS, Tung KT, Ip P. Association of harsh parenting and maltreatment with internet addiction, and the mediating role of bullying and social support. Child Abuse Negl. (2021) 113:104928. doi: 10.1016/j.chiabu.2021.104928
50. Chen J, Xiong Y, Wang Q, Xu X, Qin X, Ren P. Peer victimization and Internet addiction among adolescents: the role of anger rumination and social dominance orientation. J Adolesc. (2023) 95:1578–89. doi: 10.1002/jad.12227
51. Bansal S, Garg N, Singh J. Perpetrators' perspective on cyberbullying: a qualitative systematic review with bibliometric analysis. Library Hi Tech. (2023) 43:423–55. doi: 10.1108/lht-06-2023-0265
52. Klomek AB, Sourander A, Kumpulainen K, Piha J, Tamminen T, Moilanen I, et al. Childhood bullying as a risk for later depression and suicidal ideation among Finnish males. J Affect Disord. (2008) 109:47–55. doi: 10.1016/j.jad.2007.12.226
53. Chen HWB, Gardner ES, Clarkson T, Eaton NR, Wiggins JL, Leibenluft E, et al. Bullying perpetration and victimization in youth: associations with irritability and anxiety. Child Psychiatry Hum Dev. (2022) 53:1075–82. doi: 10.1007/s10578-021-01192-9
54. Evangelio C, Rodríguez-González P, Fernández-Río J, Gonzalez-Villora S. Cyberbullying in elementary and middle school students: a systematic review. (2022) 176:104356. doi: 10.1016/j.compedu.2021.104356
55. Adrian M, Jenness JL, Kuehn KS, Smith MR, McLaughlin KA. Emotion regulation processes linking peer victimization to anxiety and depression symptoms in adolescence. Dev Psychopathol. (2019) 31:999–1009. doi: 10.1017/S0954579419000543
56. McLaughlin KA, Nolen-Hoeksema S. Rumination as a transdiagnostic factor in depression and anxiety. Behav Res Ther. (2011) 49:186–93. doi: 10.1016/j.brat.2010.12.006
57. Lereya ST, Copeland WE, Costello EJ, Wolke D. Adult mental health consequences of peer bullying and maltreatment in childhood: two cohorts in two countries. Lancet Psychiatry. (2015) 2:524–31. doi: 10.1016/S2215-0366(15)00165-0
58. Li Y, Li G, Liu L, Wu H. Correlations between mobile phone addiction and anxiety, depression, impulsivity, and poor sleep quality among college students: a systematic review and meta-analysis. J Behav Addict. (2020) 9:551–71. doi: 10.1556/2006.2020.00057
59. Palesh OG, Collie K, Batiuchok D, Tilston J, Koopman C, Perlis ML, et al. A longitudinal study of depression, pain, and stress as predictors of sleep disturbance among women with metastatic breast cancer. Biol Psychol. (2007) 75:37–44. doi: 10.1016/j.biopsycho.2006.11.002
60. Van Rooij AJ, Kuss DJ, Griffiths MD, Shorter GW. The (co-)occurrence of problematic video gaming, substance use, and psychosocial problems in adolescents. J Behav Addict. (2014) 3:157–65. doi: 10.1556/JBA.3.2014.013
61. Healy KL, Thomas HJ, Sanders MR, Scott JG. Empirical and theoretical foundations of family interventions to reduce the incidence and mental health impacts of school bullying victimization. Int Rev Psychiatry. (2022) 34:140–53. doi: 10.1080/09540261.2022.2045260
62. Ran MS, Rohlof H, Li J, Persaud A, Zhang TM, Lewis-Fernández R. Global call to reduce the stigma of mental illness and COVID-19 Worldwide. Psychiatry. (2023) 86:87–90. doi: 10.1080/00332747.2022.2113317
63. Zhang TM, Zhang XF, Meng XD, Huang Y, Zhang W, Gong HH, et al. Comparison of stigmatizing views towards COVID-19 and mental disorders among adolescent and young adult students in China. Front Psychiatry. (2023) 14:1170540. doi: 10.3389/fpsyt.2023.1170540
64. Knack JM, Jensen-Campbell LA, Baum A. Worse than sticks and stones? Bullying is associated with altered HPA axis functioning and poorer health. Brain Cogn. (2011) 77:183–90. doi: 10.1016/j.bandc.2011.06.011
65. Evans R, Hurrell C. (2016). The role of schools in children and young people's self-harm and suicide: systematic review and meta-ethnography of qualitative research. BMC Public Health. 16:401. doi: 10.1186/s12889-016-3065-2
66. Corrigan PW, Watson AC. Understanding the impact of stigma on people with mental illness. (2002) 1:16.
67. Guarneri JA, Oberleitner DE, Connolly S. Perceived stigma and self-stigma in college students: a literature review and implications for practice and research. Basic Appl Soc Psychol. (2019) 41:48–62. doi: 10.1080/01973533.2018.1550723
68. Gaffney H, Ttofi MM, Farrington DP. What works in anti-bullying programs? Analysis of effective intervention components. J Sch Psychol. (2021) 85:37–56. doi: 10.1016/j.jsp.2020.12.002
Keywords: school bullying, internet addiction, stigma of mental illness, depression, anxiety
Citation: Li L, Cai J, Wang C, Mu Y-F, Deng Z-Y, Deng A-P, Song H-J, Huang X-H, Yin L, Huang Y, Chen J, Zhao J-S, Zhang B-Z, Li H and Ran M-S (2025) The association between school bullying and internet addiction among adolescents: a moderated mediation model. Front. Public Health 13:1502726. doi: 10.3389/fpubh.2025.1502726
Received: 27 September 2024; Accepted: 14 March 2025;
Published: 27 March 2025.
Edited by:
Wulf Rössler, Charité University Medicine Berlin, GermanyReviewed by:
Suhans Bansal, University of Petroleum and Energy Studies, IndiaCopyright © 2025 Li, Cai, Wang, Mu, Deng, Deng, Song, Huang, Yin, Huang, Chen, Zhao, Zhang, Li and Ran. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mao-Sheng Ran, bXNyYW5jZEBvdXRsb29rLmNvbQ==
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.