 Nejra Bektas
Nejra Bektas Larisa Besic
Larisa Besic Aida Kulo Cesic
Aida Kulo Cesic Damir Marjanovic
Damir Marjanovic Jasminka Prguda-Mujic4
Jasminka Prguda-Mujic4
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 18 March 2025
Sec. Public Health Education and Promotion
Volume 13 - 2025 | https://doi.org/10.3389/fpubh.2025.1498407
The aim of this pioneering study was to examine the knowledge and attitudes regarding prevention, diagnostic methods, treatment, and recovery aspects related to Helicobacter pylori infection within the general population of Bosnia and Herzegovina (B&H). Study was conducted using the previously designed questionnaire, adapted for the B&H population. The research enrolled 1,031 participants, of whom 58.49% answered predominantly correctly to questions regarding Helicobacter pylori infectivity. Of all participants, 36.18% underwent screening, with 65.95% testing positive, and of those, 93.90% received treatment, mainly antibiotics (92.64%). Of those treated, 74.46% were re-tested and 30.23% of them had relapsed infection. Furthermore, the study identified lower infection rate in younger participants and, contraversaly, in participants with the history of long-term (lasting for more than a year) alcohol consumption, who were also shown to report symptoms' improvement post-treatment. Overall, B&H population demonstrated good knowledge toward Helicobacter pylori infection, with higher levels of knowledge in women, highly educated, or screened for H. pylori. Notably, participants expressed strong support for national Helicobacter pylori screening and thus underscored the importance of planning it in the public health initiatives in B&H. Also, due to the high relapsed infection rate, further effort needs to be directed toward education of risk groups i.e., older age groups, and community on effective measures for Helicobacter pylori prevention and treatment.
The gram-negative bacterium Helicobacter pylori (H. pylori) impacts an estimated 4.4 billion people worldwide, marking it a widespread and significant concern in global health (1, 2), especially after being classified as class I carcinogen associated with the onset of gastric cancer (GC) (3). It can also lead to chronic gastritis, peptic ulcers, and mucosa-associated lymphoid tissue lymphoma (1).
Its prevalence shows variation not only across different countries but also within various regions of the same country (4). The infection tends to be more prevalent among people with lower socioeconomic status and in developing nations (5). Hooi et al. even claimed that H. pylori infection is a global one, and it is not resolving spontaneously (6).
H. pylori is a helix-shaped, microaerophilic, flagellated bacteria that can shape from spiral to coccoid form. These forms seem to help its survival in the host gastric microenvironment, with the spiral form that enables its successful motility, whereas the coccoid form provides its ability to colonize the mucus layer of the gastric epithelium, enhancing its further invasiveness (7). The precise mode of transmission is unclear. However, new infections are thought to occur because of direct human-to-human transmission, via fecal-oral, gastric-oral, oral-oral route. Moreover, in developing countries, H. pylori infection rates increase rapidly within the first 5 years of life and remain consistently high thereafter, suggesting that the bacterium is primarily acquired in early childhood (8–11).
The major challenge in H. pylori eradication is its resistance to antibiotics (12). It is primarily attributed to chromosomal mutations, but additional mechanisms such as efflux pump activity, alterations in membrane permeability, and biofilm formation also contribute to resistance (13–15).
A recent comprehensive review and meta-analysis showed alarming levels of primary and secondary resistance rates to clarithromycin, metronidazole, and levofloxacin, surpassing 15% across all World Health Organization (WHO) regions (16). Moreover, most treatments are administered without prior assessment of antibiotic resistance leading to decreased success of available therapies and increased rate of H. pylori recurrence, a crucial factor impacting its prevalence. The study of the global recurrence rate indicated an escalating annual H. pylori recurrence rate over the decades, rising from 3.9% in the 1990s to 4.8% in the 2010s, potentially contributing to an increase in the number of infected individuals (17). Notably, a study conducted by Zhao et al. showed that European nations exhibited the highest recurrence rates among the regions analyzed (18).
Despite concerted efforts to address H. pylori infection, global public awareness of this issue remains notably low. Moreover, studies conducted among the general population (19) and students (20) have consistently shown insufficient knowledge about H. pylori. Another study showed a lack of knowledge about the established diagnostic and treatment recommendations for H. pylori infection among general practitioners (21). This suggests an urgent need for enhanced education within the realm of continuing medical education, aiming to improve both physicians' and patients' awareness and knowledge concerning H. pylori infection.
The data concerning the incidence of H. pylori infection in Bosnia and Herzegovina (B&H) are lacking, and of GC are old and scarce. Studies reported the GC incidence of 1.26% in 2005 (22) and of 2.21% in 2009 (23). According to the more recent data published by the International Agency of Research on Cancer (IARC) in 2018, the incidence of gastric adenocarcinoma (GAC) in B&H has increased to 10.1%, with the mortality rate of 7.4% (24). Nonetheless, the general understanding of H. pylori prevention and treatment among the population of B&H has never been investigated.
Therefore, the aim of this study was to conduct a comprehensive national survey focusing on the knowledge and attitudes regarding prevention, diagnostic methods, treatment, and recovery aspects related to H. pylori infection in the B&H population.
The study was an online survey-based study, conducted between the 8th June 2024 and 8th September 2024. It engaged citizens of B&H aged 18 and above. The minimum sample size was calculated to be 384, as determined using the formula n = N × Z2 × p × (1 − p) ÷ (N − 1) × d2 + Z2 × p × (1 − p) (25), in which the confidence level (Z) was 95% or 1.96, the maximum variability (p) was 0.5 and margin of error (d) was 5% or 0.05. Prior to participation, participants were asked for verbal consent which was recorded using an audio recorder to confirm informed voluntary participation. An independent community member acted as witness for voluntary informed decision making of participants to take part in the study. The study was approved by the Ethics Committee of the Faculty of Engineering and Natural Sciences, International Burch University.
The survey investigating awareness and attitudes toward H. pylori infection in physicians and the public population developed by Wu et al. was adapted to local characteristics of the general population in B&H (26). Initially, the survey underwent translation into Bosnian language and subsequent translation back into English. Before distributing the survey to the public, a pilot study was conducted among 20 non-health professionals, employees at the International Burch University, to ensure the clarity of the survey and its suitability for the general population. After the survey validation, it was published as a Google Form document, and widely distributed via the Internet (through social networks such as Facebook and Instagram, as well as calling and messaging applications such as Viber, WhatsApp, Messenger) across the entirety of B&H. It was open for 90 days and took ~15 min to complete it.
The questionnaire encompassed questions about knowledge and attitudes toward H. pylori infection. All participants were asked about their demographics, lifestyle habits associated with H. pylori infection, overall knowledge, and attitudes related to H. pylori testing. Categorization of the occupations was done according to the standard classification of occupations of the government of the Federation of B&H (27). Those who hadn't undergone H. pylori screening/testing were presented with questions about their reasons for not being tested and their willingness to undergo testing. For those expressing willingness, subsequent questions focused on their attitudes toward testing of their family members.
On the other hand, participants who had undergone H. pylori screening/testing were asked about their attitudes toward testing of their family members, test results, and treatment regimen. Participants who were infected but did not receive treatment were questioned about their reasons for abstaining from treatment. For patients who were infected and had received treatment, the survey investigated the experienced symptoms, treatment regimen employed, treatment duration, adverse drug reactions, follow-up attendance, symptoms' improvement post-treatment, and relapsed infection rate. The complete survey text can be made available upon request from the corresponding author.
Data analysis was performed using MS Excel and R Statistical Software (v4.2.3; R Core Team 2021) (28). Participants fell into three knowledge groups: low (answering incorrectly or with “don't know”), moderate (1–3 correct answers), and high (4–5 correct answers) based on Wu et al.'s approach (26). The study linked H. pylori infection to participant demographics, habits associated with H. pylori infection, knowledge on H. pylori, screening status and status of H. pylori infection. It also explored symptoms' improvement post-treatment alongside adverse drug reactions and follow-up attendance. Using Fisher's exact test and Cramer's V measurement, associations were gauged as weak (<0.1), moderate (0.11–0.31), or strong (>0.31). Data were presented as numbers/percentages or median/IQR. In all statistical tests p < 0.05 was considered statistically significant.
Comprehensive demographic characteristics, lifestyle habits associated with H. pylori infection, knowledge on H. pylori, screening status and status of H. pylori infection of participants are presented in Table 1. A total of 1,031 people participated in the survey. Estimated participation rate was ~0.036%. Most of the included participants were in the youngest age group (18–29 years) (44.03%) while other age groups (30–39; 40–49; 50 and above) showed approximately similar percentage of includeness (18.62%, 16.88%, 20.47%, respectively). Most participants were women (73.04%), living in urban areas (65.37%), and highly educated (faculty 64.69%, secondary school 33.56%, elementary school 1.75%). Most participants in the survey were experts, scientists, technicians and other professional occupations (35.11%) as well as students (27.16%).

Table 1. Demographic characteristics, lifestyle habits associated with H. pylori infection, knowledge on H. pylori, screening status and status of H. pylori infection of participants (N = 1,031).
Regarding personal habits associated with H. pylori infection, the largest number of participants, 83.41%, indicated at least one listed habit. In addition, most participants reported long-term (lasting for more than a year) consumption of carbohydrates (58.20%), sweets (48.50%) and coffee (47.72%).
Of all, 818 participants (79.34%) were familiar with H. pylori bacteria. Among the 373 (36.18%) participants that were screened/tested for H. pylori infection any time prior to survey, 246 (65.95%) reported their positive status.
Effects of demographic characteristics, lifestyle habits associated with H. pylori infection, screening status and status of H. pylori infection on participants knowledge of H. pylori are presented in Table 2. Sex, educational level, participants' screening for H. pylori status and occupation had significant effect on knowledge of H. pylori. Women compared to men (63.61% vs. 44.60%, p = 0.017), more educated participants compared to the less educated ones (faculty 60.72%, secondary school 55.78%, elementary school 27.78%, p = 0.000), those screened for H. pylori compared to the ones who were not screened (72.39% vs. 50.61%, p = 0.004), and those categorized as officials and members of legislative bodies, officials of state bodies, directors compared to production occupations (66.67% vs. 40.91% p = 0.001) showed significantly higher proportion of high knowledge of H. pylori.

Table 2. Effects of demographic characteristics, lifestyle habits associated with H. pylori infection, screening status and status of H. pylori infection on participants knowledge of H. pylori tested by Fisher's exact test with p < 0.05 considered statistically significant (shown in bold), and 4–6 correct options were referred to “High,” 1–3 correct options were referred to “Moderate,” and incorrect or unclear answers were referred to “Low.”
Military occupations and students had significantly lower frequency of high knowledge of H. pylori compared to other occupations (p = 0.001).
Age and residence had no significant effect on knowledge of H. pylori. Although participants aged 30–39 years and older participants aged 50 and up showed the highest frequency of high awareness regarding H. pylori (65.10%, 62.09%, respectively), compared to middle-aged (40–49 years) and younger adults (18–29 years) (58.05%, 54.19%, respectively) age had no significant effect on knowledge (p = 0.716). Similarly, although urban participants had a higher frequency of high knowledge answers (61.57%) compared to suburban and rural ones (54.29% vs. 50.34% respectively), residence did not significantly affect the knowledge (p = 0.452).
Overall, participants had a good knowledge of H. pylori, with more than a half (58.49%) answering four to six out of six questions correctly.
Attitudes toward H. pylori screening/testing and treatment are presented in Table 3. Most of the participants (63.82%) were not screened for the H. pylori infection. The most common reason for not participating in screening was no obvious symptoms and not willing to check themselves (41.64%) and the test not being included in regular health examination (25.53%). Even though, not screened participants showed high frequency of support for screening (72.04%) while 25.23% were neutral and only 2.74% were against the screening.
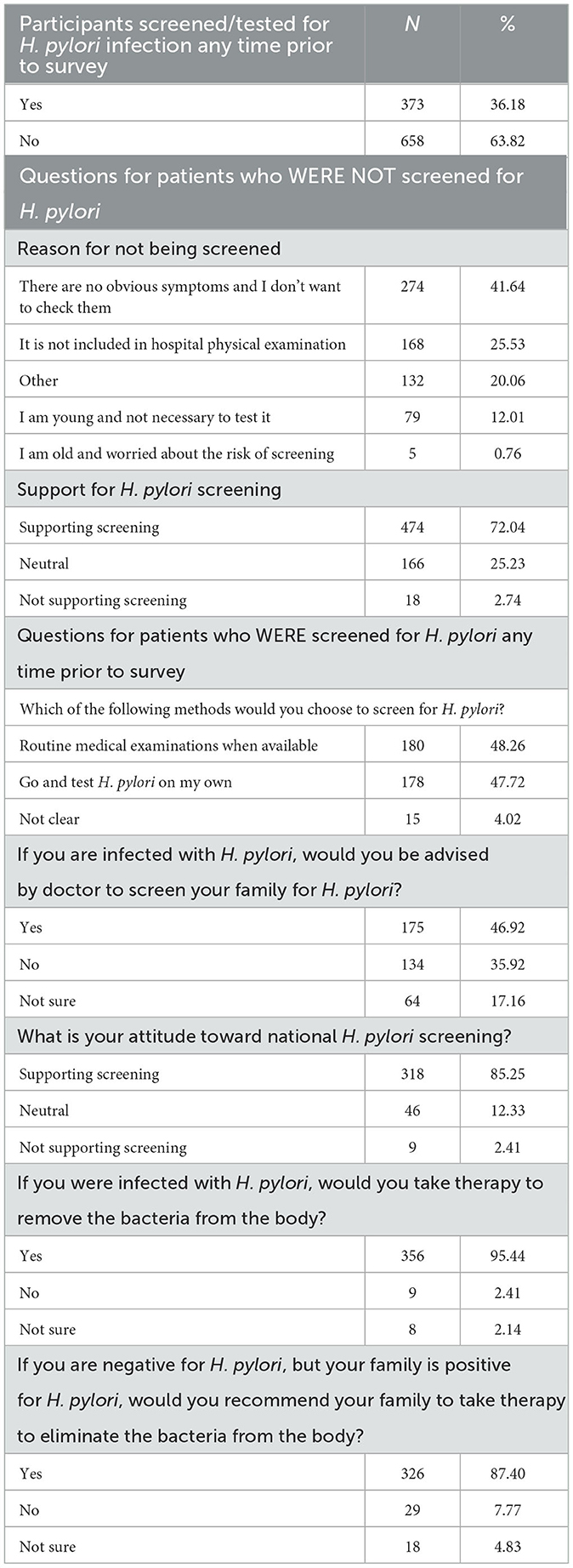
Table 3. Attitudes toward H. pylori screening/testing and treatment.
The screened participants showed a higher level of support for screening programs, with 85.25% in favor. Among screened participants, 46.92% would recommend testing for other members of their family, whilst 35.92% would not. The majority would take the therapy to remove the bacteria (95.44%) and would recommend it to their family members who had tested positive (87.40%).
H. pylori infection treatment regimen, adverse drug reactions and treatment effectivness in participants who were tested positive at H. pylori screening/testing are presented in Table 4. Of 373 screened participans, 246 (65.95%) had confirmed H. pylori infection. Most of them, 231 (93.90%), received the treatment. While only minority of participants (15.38%) stated fear of relapse after infection and that the presence of H. pylori infection has no impact on health and life (30.77%) as specific reason for not receiving treatment, most participants stated no specific reasons for not receiving treatment (69.23%).

Table 4. H. pylori infection treatment regimen, adverse drug reactions and treatment effectivness in participants who were tested positive at H. pylori screening/testing.
Most of the treated participants were given antibiotics (92.64%) in a standard combination triple or quadruple therapy (92.21%), and the duration of the treatment in most participants lasted more than 14 days (30.30%). Of 231 treated participants, 58.01% experienced adverse drug reaction, mainly abdominal pain (36.36%) and diarrhea (18.18%). Also, 28.57% of participants experienced some level of worry caused by the treatment.
Most of the treated participants (85.72%) reported symptoms' improvement after therapy, with 28.57% reporting “slight improvement.” Eight participants (3.46%) said that the treatment worsened their symptoms. Some of the treated participants also continued to experience additional difficulties post-treatment, with 54 participants (23.38%) complained about having to give up some of their favorite foods due to illness, and 35 participants (15.15%) complained that illness had forced them to follow a diff8erent diet. The participants also reported issues such as belching or flatulence, stomach (upper belly) fullness, heartburn, and feeling nervous or afraid because of their condition. Other symptoms and difficulties experienced post treatment are shown in Table 5.
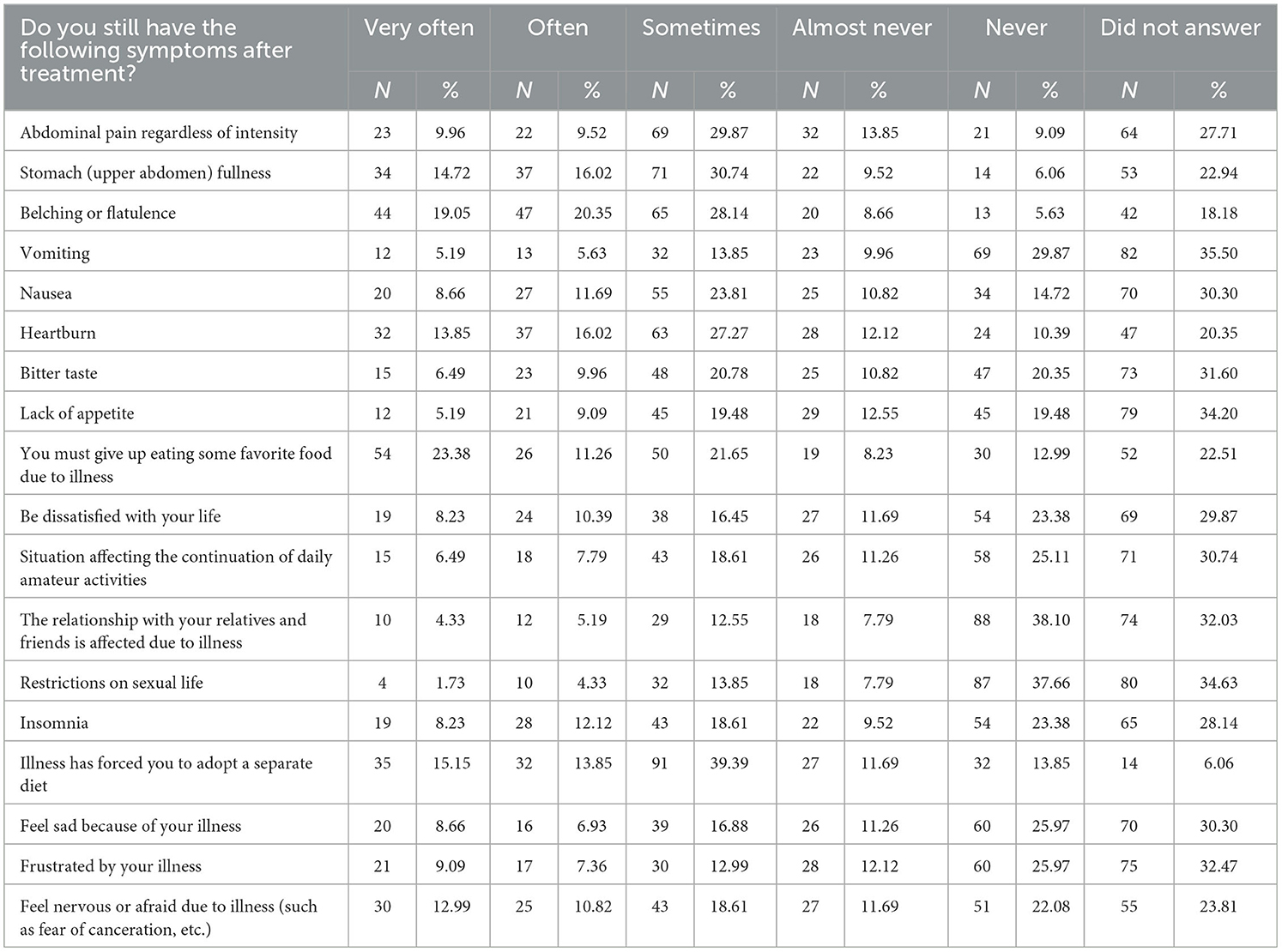
Table 5. Symptoms and difficulties experienced post-treatment.
Most of the treated participants (74.46%) went to a re-testing after the treatment, with 30.23% of them who had relapsed infection after treatment.
The impact of demographic characteristics and lifestyle habits associated with H. pylori infection on the incidence of H. pylori infection is shown in Table 6. H. pylori infection was moderately associated with participants' age and occupation, whereas exhibited a strong association with lifestyle habits associated with H. pylori infection.

Table 6. The impact of demographic characteristics and lifestyle habits associated with H. pylori infection on the incidence of H. pylori infection.
The H. pylori infection rate was age-dependent with the oldest age group (50 and up) being the most (76.34%, p = 0.003), and the youngest age group being least likely to have been infected (46.73%). Agricultural, hunting and breeding, forest and fishing workers (80%) were most likely to have been infected, followed by officials and members of legislative bodies, officials of state bodies, directors (78.57%), as well as production workers (77.78%) and simple occupations (elementary school education) (76.60%) (p = 0.000). The highest proportions of non-infected participans were among military occupations (50.50%), students (37.21%) and participans with the secondary level of education i.e., service and commercial (37.04%) and office and counter workers (36.96%).
Among the lifestyle habits associated with infection, participants who reported long-term alcohol consumption were least likely to have been infected (4%, p < 0.001).
The sex and place of residence showed no impact on H. pylori infection rates.
The impact of demographic characteristics, lifestyle habits associated with H. pylori infection, adverse drug reactions during treatment and re-testing after treatment on the estimated symptoms' improvement post-treatment is shown in Table 7. Estimated symptoms' improvement after the treatment was moderately associated with age, occupation, lifestyle habits associated with H. pylori infection and adverse drug reactions.

Table 7. The effect of demographic characteristics, lifestyle habits associated with H. pylori infection, adverse drug reactions during treatment and re-testing after treatment on the estimated symptoms' improvement post-treatment.
Youngest participants were least likely to report symptoms' improvement (25%, p = 2.00E-07) and most likely to report worsening of symptoms post-treatment (5.36%). Office and counter employees followed by military occupations were most likely to report improvement (52% and 50%, respectively), while agricultural, hunting and breeding, forest and fishing workers and retirees were most likely to report complete improvement (50% and 30.77%, respectively, p = 1.00E-07). Retirees (older than 65 years of age) and military occupations were least likely to report no change or worsening. The association was defined as moderate. Another moderate association was observed between consuming none of the listed habits associated with H. pylori infection and symptoms' improvement, i.e., participants who consumed none of the habits associated with H. pylori infection or reported long-term alcohol consumption were most likely to have reported symptoms' improvement (53.57%, 50.50%, p = 1.00E-07). Participants who reported long-term seafood consumption were most likely to report worsening (12.50%). Complete improvement and improvement were more likely for those with long-term alcohol consumption or no adverse drug reactions during treatment (p = 0.023).
No significant association was found between estimated symptoms' improvement after the treatment and sex, place of residence or re-testing after the treatment.
This was the first national survey on the knowledge and attitudes regarding diagnostics, treatment and recovery aspects related to H. pylori infection in the B&H population. The findings indicated that the general population had a good knowledge about H. pylori infection with more than half of the participants (58.49%) correctly answering nearly all questions. Of all participants, 36.18% underwent screening for H. pylori, with 65.95% testing positive, and of those, 93.90% received treatment, mainly antibiotics (92.64%) in a standard combination triple or quadruple therapy (92.21%) longer than 14 days (30.30%). Of all treated participants, 58.01% experienced adverse drug reaction, mainly abdominal pain (36.36%) and diarrhea (18.18%). Most of the treated participants, 85.72%, reported symptoms' improvement after therapy, but also went to a re-testing after the treatment (74.46%), with 30.23% of them who had relapsed infection. Being woman, highly educated, or already screened for H. pylori status was associated with higher knowledge of H. pylori, while being younger, student/with secondary level of education or with the history of long-term alcohol consumption was associated with lower rate of H. pylori infection. In addition, being older, with no history of consuming habits associated with H. pylori infection or with the history of long-term alcohol consumption was associated with symptoms improvement. Although most participants (63.82%) were not screened for the H. pylori infection, most of them (72.04%) as well as of those screened (85.25%) expressed support for a national H. pylori screening plan.
The relationships between higher educational levels and a lower prevalence of specific diseases demonstrate why knowledge is such an important aspect in both physical and psychological health. Notably, people with elementary school education or less had a disease prevalence rate 1.64 times greater than people with college degree or more (29). In this sense, our study yielded similar results, with more educated participants demonstrating greater knowledge than less educated persons. Furthermore, this study highlighted a potential link between knowledge levels and participants' inclination to participate in screening. Those who underwent screening for H. pylori infection demonstrated higher knowledge compared to those who did not undergo screening. This underscores the importance of educational programs for the general population, contributing to increased participation in screenings and disease awareness. The association with education is evident in professions such as officials and members of legislative bodies, state officials, directors, experts, scientists, technicians, and other professional occupations that require higher education. These occupations demonstrated higher knowledge levels. On the other hand, production workers, including machine operators, vehicle operators, and assemblers, as well as occupations that don't require higher education, exhibited lower knowledge levels.
Notably, the screening rate of 36.18% in our study surpasses the screening rate of 27.9% reported in a neighboring country Croatia (30). The predominant rationale behind the non-testing was the absence of symptoms. This poses a potential challenge, given that the infection typically manifests asymptomatically. Additionally, participants highlighted the omission of testing in routine hospital physical examinations. Conversely, those who underwent testing identified routine medical examinations, when accessible, as the optimal testing approach. Subsequently, it may be crucial to consider integrating H. pylori testing into the standard medical examinations within the healthcare system of B&H. This is also in line with strong support for national H. pylori screening shown in this study.
Study participants demonstrated strong endorsement for therapy, not only for themselves but also for their family members in the event of infection. This support is underscored by the noteworthy statistic that 93.90% of participants who tested positive for H. pylori underwent treatment. However, high resistance rates to clarithromycin (28.26%), quinolones (36.96%), and to both antibiotics (8.69%) were detected recently in the tested biopsies taken from the patients with dyspepsia in B&H (31). The reported clarithromycin resistance rate in B&H is slightly higher than in neighboring countries Serbia (24%) (32) and Croatia (21.2%) (33). This resistance could potentially limit the efficacy of the treatment, highlighting a potential rationale for considering its extension. This consideration is especially pertinent given the high relapsed infection rate among treated participants (30.23%).
Emphasizing the key role of extending treatment duration to increase eradication rates, a survey of the European H. pylori Care Registry found that physicians in the South-East region predominantly prescribed 7-day treatment regimens (34), as well as the triple treatment. Despite this, our results show that most treated participants were on treatment for longer than 14 days.
To consistently achieve eradication rates of 90% and mitigate the need for retreatment and patient dropout, physicians should be encouraged to employ quadruple therapies, as these regimens consistently yield eradication rates of ≥90% (34). This is in line with our results with nearly all participants reported receiving triple/quadruple treatment, and majority of them reported improvement after the treatment. Also, the authors of mentioned recent study on antibiotic resistance in B&H recommended the use of bismuth quadruple or non-bismuth concomitant quadruple therapy due to the high resistance rates to clarithromycin and quinolones (31). Accordingly, in the future it may be imperative to examine the effect of prolonged treatment as well as the effectiveness of the prescribed triple/quadruple treatment, especially in light of high rate of antibiotic resistance in B&H (31).
Assessing the association between demographic characteristics and lifestyle habits with H. pylori infectivity, numerous studies have identified poor hygienic conditions during the childhood, such as inadequate hand hygiene and insufficient access to clean water for washing, as well known risk factors associated with H. pylori infection (8–11, 35, 36), while some studies found no association (37, 38).
To date, no study on hygiene in B&H, nor on the association between hygiene and the prevalence of H. pylori was conducted.
In our study, we found that besides the youngest age group being least likely to have been infected (46.73%), participants who reported long-term alcohol consumption were, unexpectedly, also least likely to be infected (4%, p < 0.001). This is consistent with the results of a dose-response meta-analysis of observational studies that suggested moderate alcohol intake to be associated with a 22% reduction in H. pylori infection and its elimination (39). Additionally, a previous study by Kuepper-Nybelen et al. indicated an inverse relationship between alcohol consumption and H. pylori infection, suggesting that alcohol intake may contribute to the elimination of H. pylori infection among adults (40). This could serve as a foundation for further larger scale investigation to elucidate this association.
In addition, next to participants who consumed none of the habits associated with H. pylori infection, those who reported long-term alcohol consumption were also most likely to have reported symptoms improvement post-treatment (53.57%, 50.50%, p = 1.00E-07). Furthermore, symptoms improvement or complete resolution of symptoms were more likely for those with long-term alcohol consumption (50.00%, p = 1.00E-07). Our finding on potentially protective effect of long-term alcohol consumption is indeed intriguing and controversial. However, given the strong link between alcohol consumption and GC, the results of our study should only be used to further highlight the complexity of H. pylori infection and to suggest that more controlled studies are needed to determine whether alcohol consumption truly influences H. pylori prevalence or may facilitate symptoms' improvement post-treatment, and if so, through which mechanisms.
On the contrary, participants who reported long-term seafood consumption were not likely to have H. pylori infection, which is consistent with an earlier study demonstrated that a high intake of seafood was associated with a lower prevalence of H. pylori infection (41). However, participants who reported long-term seafood consumption were more likely to report worsening of symptoms (12.50%). It is surprising that factors such as seafood consumption, alongside with long-term conserved food intake, and those categorized as “other” demonstrated a negative impact on post-treatment recovery.
Notably, among the participants in this study, the younger ones were less likely to report improvement and more likely to report worsening. A plausible explanation for this pattern could be that younger people are less prone to experiencing dyspepsia or peptic ulcers, consequently reducing the likelihood of benefits in symptoms reduction from clearing the infection. This trend is consistent with the anticipated outcomes of screening and treatment in older participants (42).
Although our results provide background for more targeted studies, the study had several limitations. Firstly, the study included small convenience sample of participants and only those with sufficient digital literacy and Internet access which limits the generalizability of the findings. Secondly, the unequal sample of men and women as well the different age groups of participants could introduce bias. Also, the largest number of participants were highly educated which potentially might have caused the bias toward the higher knowledge score and more favorable attitudes toward screening and other healthcare interventions, which also limits the generalizability of the findings. Finally, no clear definitions for the time for reporting the screening/testing, treatment, re-testing for relapsed infection, and reporting the symptoms after the received treatment were given.
In perspective, it is crucial to assess the duration and the effectiveness of treatment for patients with H. pylori infection in B&H. It can partly be assessed by investigating physicians' awareness, knowledge and practices concerning H. pylori infection and its treatment. Also, considering the widespread population support for national H. pylori testing, the implementation of a national education campaign could prove beneficial, especially considering its absence thus far.
This pioneering study offers a first comprehensive overview of knowledge, attitudes, diagnostics, treatment and recovery aspects toward H. pylori infection within the general population of B&H. Overall, B&H population demonstrated good knowledge toward H. pylori infection and expressed strong support for national H. pylori screening underscoring the importance of planning it in the public health initiatives in B&H. Also, due to the reported high relapsed infection rate, further effort needs to be directed toward community education, with a focus on the risk groups, i.e., older age groups, on effective measures for H. pylori prevention, early detection and treatment. Moreover, to gain a more comprehensive understanding of the H. pylori landscape in the B&H further research is needed to assess the duration and the effectiveness of treatment for patients with H. pylori infection.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethical review and approval was granted by the Ethics Committee of the Faculty of Engineering and Natural Sciences, International Burch University. Participants were asked for verbal consent which was recorded using an audio recorder to confirm informed voluntary participation. An independent community member acted as witness for voluntary informed decision making of participants to take part in the study. The social media data was accessed and analyzed in accordance with the platform's terms of use and all relevant institutional/national regulations.
NB: Conceptualization, Formal analysis, Investigation, Visualization, Methodology, Project administration, Writing – original draft, Writing – review & editing. LB: Data curation, Software, Supervision, Writing – original draft, Writing – review & editing. AK: Conceptualization, Supervision, Methodology, Validation, Visualization, Writing – original draft, Writing – review & editing. DM: Conceptualization, Investigation, Supervision, Validation, Writing – original draft, Writing – review & editing. JP-M: Conceptualization, Formal analysis, Investigation, Methodology, Supervision, Visualization, Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Chey WD, Leontiadis GI, Howden CW, Moss SF. ACG clinical guideline: treatment of Helicobacter pylori infection. Am J Gastroenterol. (2017) 112:212–39. doi: 10.1038/ajg.2016.563
2. McNicholl AG, Oroli GI, Howden CW, Moss SF. ACG clinical guideline: treatmeregistry on the management of Helicobacter pylori infection (Hpylori GI,Helicobacter. (2019) 24:5. doi: 10.1111/hel.12630
3. International Agency for Research on Cancer. Schistosomes, liver flukes and Helicobacter pylori. IARC Monogr Eval Carcinog Risks Hum. (1994) 61:1–241.
4. Vilaichone R. Extremely high prevalence of Helicobacter pylori infection in Bhutan. World J Gastroenterol. (2013) 19:2806. doi: 10.3748/wjg.v19.i18.2806
5. Lehours P. Actual diagnosis of Helicobacter pylori infection. Minerva Gastroenterol Dietol. (2018) 64:267–79. doi: 10.23736/S1121-421X.18.02494-7
6. Hooi JKY, Lai WY, Ng WK, Suen MMY, Underwood FE, Tanyingoh D, et al. Global prevalence of Helicobacter pylori infection: systematic review and meta-analysis. Gastroenterology. (2017) 153:420–9. doi: 10.1053/j.gastro.2017.04.022
7. Baj J, Forma A, Sitarz M, Portincasa P, Garruti G, Krasowska D, et al. Helicobacter pylori virulence factors—mechanisms of bacterial pathogenicity in the gastric microenvironment. Cells. (2020) 10:27. doi: 10.3390/cells10010027
8. Kusters JG, van Vliet AHM, Kuipers EJ. Pathogenesis of Helicobacter pylori infection. Clin Microbiol Rev. (2006) 19:449–90.
9. Weyermann M, Rothenbacher D, Brenner H. Acquisition of Helicobacter pylori infection in early childhood: independent contributions of infected mothers, fathers and siblings. Am J Gastroenterol. (2008) 104:182–9.
10. Hunt RH, Xiao SD, Megraud F, Leon-Barua R, Bazzoli F, van der Merwe S, et al. Helicobacter pylori in developing countries. World gastroenterology organisation global guideline. J Gastrointestin Liver Dis. (2011) 20:299–304. doi: 10.1097/MCG.0b013e31820fb8f6
11. Dattoli VCC, Veiga RV, Da Cunha SS. Pontes-de-Carvalho LC, Barreto ML, Alcrs, fathers and sSeroprevalence and potential risk factors for Helicobacter pylori infection in Brazilian children. Helicobacter. (2010) 15:273–8.
12. Yonezawa H, Osaki T, Kamiya S. Biofilm formation by Helicobacter pyloriand its involvement for antibiotic resistance. Biomed Res Int. (2015) 2015:1–9.
13. Zanotti G, Cendron L. Structural aspects of Helicobacter pylori antibiotic resistance. Adv Exp Med Biol. (2019) 1149:227–41.
14. Fauzia KA, Miftahussurur M, Syam AF, Waskito LA, Doohan D, Rezkitha YAA, et al. Biofilm formation and antibiotic resistance phenotype of Helicobacter pylori clinical isolates. Toxins. (2020) 12:473. doi: 10.3390/toxins12080473
15. Tshibangu-Kabamba E, Yamaoka Y. Helicobacter pylori infection and antibiotic resistance- from biology to clinical implications. Nat Rev Gastroenterol Hepatol. (2021) 18:613Gastroenterol1038/s41575-021-00449-x
16. Savoldi A, Carrara E, Graham DY, Conti M, Tacconelli E. Prevalence of antibiotic resistance in Helicobacter pylori: a systematic review and meta-analysis in world health organization regions. Gastroenterology. (2018) 155:1372–82. doi: 10.1053/j.gastro.2018.07.007
17. Hu Y, Wan JH, Li XY, Zhu Y, Graham DY, Lu NH. Systematic review with metaons. ic resistance in ngs. t of ucated peHelicobacter pylori. Aliment Pharmacol Ther. (2017) 46:773–9. doi: 10.1111/apt.14319
18. Zhao H, Yan P, Zhang N, Feng L, Chu X, Cui G, et al. The recurrence rate of Helicobacter pylori in recent 10 years: a systematic review and meta-analysis. Helicobacter. (2021) 26:e12852. doi: 10.1111/hel.12852
19. Teng TZJ, Sudharsan M, Yau JWK, Tan W, Shelat VG. Helicobacter pylori knowledge and perception among multi-ethnic Asians. Helicobacter. (2021) 26:e12794. doi: 10.1111/hel.12794
20. Hafiz TA, D10. perception among multi-ethnic Asians. tic review witHelicobacter pylori infection: comparison of knowledge between health science and non-health science university students. Int J Environ Res Public Health. (2021) 18:8173. doi: 10.3390/ijerph18158173
21. Cano-Contreras AD, Rascc Healthents. etween h, Ríos-Gálvez S, Maza YJ, Meixueiro-Daza A, et al. Approach, attitudes, and knowledge of general practitioners in relation to Helicobacter pylori is inadequate. There is much room for improvement! Rev Gastroenterol México. (2018) 83:16–24. doi: 10.1016/j.rgmxen.2017.08.005
22. Mimica M. Choice of age cut-off for endoscopy in dyspepsia in developing countries according to incidence of gastric cancer. Coll Antropol. (2005) 29:599ropol. Available online at: https://hrcak.srce.hr/5277 (accessed February 16, 2025).
23. Salkic NN, Zildzic M, Zerem E, Smajic M, Gegic A, Alibegovic E, et al. Simple uninvestigated dyspepsia: age threshold for early endoscopy in Bosnia and Herzegovina. Eur J Gastroenterol Hepatol. (2009) 21:39–44.
24. Cancer Today. Global Cancer Observatory: Cancer Today. Lyon: International Agency for Research on Cancer. (2024). Available online at: https://gco.iarc.who.int/today (accessed 16 February 2025).
25. Arya R, Antonisamy B, Kumar S. Sample size estimation in prevalence studies. Ind J Pediat. (2012) 79:1482–8. doi: 10.1007/s12098-012-0763-3
26. Wu Y, Su T, Zhou X, Lu N, Li Z, Du Y. Awareness and attitudes regarding Helicobacter pylori infection in Chinese physicians and public population: A national crosshsectional survey. Helicobacter. (2020) 25:4. doi: 10.1111/hel.12705
27. Standardna Klasifikacija Zanimanja. Available online at: http://www.fbihvlada.gov.ba/bosanski/zakoni/2004/odluke/176.htm (accessed 24 March 2024).
28. Team RDC. R: A Language and Environment for Statistical Computing. Vienna: R Foundation for Statistical Computing. (2010).
29. Dai X, Li W. Impact of education, medical services, and living conditions on health: evidence from China health and nutrition survey. Healthcare. (2021) 9:1122. doi: 10.3390/healthcare9091122
30. Cindro PV Bukipact Bukipact of education medical services and living co. Helicobacter pylori infection in croatian population: knowledge, attitudes and factors influencing incidence and recovery. Healthcare. (2022) 10:833. doi: 10.3390/healthcare10050833
31. Hasukić I, Salkić N, Tihić N, Alibegović E, Hasukić Š, Jahić A. Helicobacter pylori resistance to clarithromycin and quinolones in patients with dyspepsia in Tuzla Canton, Bosnia and Herzegovina. Med Glas (Zenica). (2023) 20:163–8. doi: 10.17392/1609-23
32. Milivojevic V, Babic I, Kekic D, Rankovic I, Sagdati S, Panic N, et al. Current trends in the management of Helicobacter pylori infection in Serbia: preliminary results from the European Registry on H. pylori. Manage Digest Dis. (2022) 41:377–86. doi: 10.1159/000528389
33. Tonkic A, Tonkic M, Brnic D, Novak A, Puljiz Z, Simunic M. Time trends of primary antibiotic resistance of Helicobacter pylori isolates in southern Croatia. J Chemother. (2012) 24:182–4. doi: 10.1179/1973947812y.0000000001
34. Nyssen OP Bordin D Tepes B Ptrends Ptrends of primary antibiotic r. European registry on Helicobacter pylori management (HP-EuReg): Patterns and trends in first-line empirical eradication prescription and outcomes of 5 years and 21533 patients. Gut. (2020) 70:40–54. doi: 10.1136/gutjnl-2020-321372
35. Schwarz S, Morelli G, Kusecek B, Manica A, Balloux F, Owen RJ, et al. Horizontal vs. familial transmission of Helicobacter pylori. PLoS Pathog. (2008) 4:1000180. doi: 10.1371/journal.ppat.1000180
36. Brown LM. Helicobacter pylori: epidemiology and routes of transmission. Epidemiol Rev. (2000) 22:283l Re doi: 10.1093/oxfordjournals.epirev.a018040
37. Lynn TV, Bruce MG, Landen M, Beller M, Bulkow L, Gold B, et al. Helicobacter pylori infection among non-Native educators in Alaska. Int J Circumpolar Health. (2007) 66:135–43.
38. Lin DB, Lin JB, Chen CY, Chen SC, Chen WK. Seroprevalence of Helicobacter pylori infection among schoolchildren and teachers in Taiwan. Helicobacter. (2007) 12:258–64.
39. Liu SY, Han XC, Sun J, Chen GX, Zhou XY, Zhang GX. Alcohol intake and Helicobacter pylori infection: a dose–response meta-analysis of observational studies. Infect Dis. (2015) 48:303–9. doi: 10.3109/23744235.2015.1113556
40. Kuepper-Nybelen J, Rothenbacher D, Brenner H. Relationship between lifetime alcohol consumption and Helicobacter pylori infection. Ann Epidemiol. (2005) 15:607–13. doi: 10.1016/j.annepidem.2004.11.001
41. Xia Y, Meng G, Zhang Q, Liu L, Wu H, Shi H, et al. Dietary patterns are associated with Helicobacter pylori infection in Chinese adults: a cross-sectional study. Sci Rep. (2016) 6:1. doi: 10.1038/srep32334
Keywords: Helicobacter pylori, knowledge, population, infection, survey
Citation: Bektas N, Besic L, Kulo Cesic A, Marjanovic D and Prguda-Mujic J (2025) The first study on population knowledge and attitudes regarding prevention, diagnostic methods, treatment, and recovery aspects related to Helicobacter pylori infection in Bosnia and Herzegovina. Front. Public Health 13:1498407. doi: 10.3389/fpubh.2025.1498407
Received: 18 September 2024; Accepted: 03 March 2025;
Published: 18 March 2025.
Edited by:
Raffaele Pellegrino, University of Campania Luigi Vanvitelli, ItalyReviewed by:
Marja-Liisa Hänninen, University of Helsinki, FinlandCopyright © 2025 Bektas, Besic, Kulo Cesic, Marjanovic and Prguda-Mujic. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nejra Bektas, bmVqcmEuYmVrdGFzQHN0dS5pYnUuZWR1LmJh
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.