 Louise Marron
Louise Marron James Gilroy
James Gilroy Michelle Williams3
Michelle Williams3 Máirín Boland
Máirín Boland- 1Health Service Executive-Health Protection Surveillance Centre, HSE National Health Protection Office, Dublin, Ireland
- 2National Health Security/ Threats Preparedness Programme, HSE National Health Protection Office, Dublin, Ireland
- 3Research & Guideline Development Unit, HSE National Health Protection Office, Dublin, Ireland
- 4UCD School of Public Health, Physiotherapy and Sports Science, University College Dublin, Dublin, Ireland
Introduction: Public health emergency preparedness requires capacities and capabilities to respond to a diverse range of health threats. A key objective of Ireland’s recent Health Protection Strategy is to enable preparedness, prevention, early detection and optimal response to health threats from all-hazards. We aimed to identify priority areas for inclusion in an evidence-based health threats preparedness framework, using lessons from the COVID-19 pandemic, to inform a national health threats strategy and a strengthened emerging health threats function for Ireland.
Methods: We conducted a narrative literature review to inform the health threats preparedness framework development. We carried out literature searches in two phases, from 2017 to 2022, followed by an updated search covering 2022–2024, to ensure all relevant, recent literature was captured. We used a data extraction tool to collate priority areas reported.
Results: Overarching priorities for health threats preparedness are rapid decision-making, an outcomes-based, and ethical approach. Health threats preparedness should include a risk-based, all-hazards, One Health approach, aligned with legislation. Multisectoral partnerships, collaboration and communication nationally and internationally are key, alongside clear governance structures and monitoring and evaluation. Adequate resources are required to operationalize effective and sustainable preparedness. Public health leadership must be to the fore.
Conclusion: An effective health threats preparedness approach is legislatively mandated for European Member States. This evidence review highlights priority areas for a comprehensive health threats preparedness framework. This framework supports the development of a strengthened emerging health threats function in Ireland and may inform other Member States’ preparedness.
Introduction
Arising from the COVID-19 pandemic, a new legislative architecture has strengthened European Union (EU) Member States’ (MS) preparedness and operational readiness for future health crises (1). Public health emergency preparedness (PHEP) is the capability of the public health and healthcare systems, working with others, to prevent, protect against, quickly respond to and recover from health threats and emergencies (2). A public health threat is an event or condition arising from an agent (hazard) with the potential to rapidly harm an exposed population and cause a crisis (3). PHEP is a coordinated and continuous cycle of planning, implementation, measuring performance and taking corrective action, and requires both capacities and capabilities (4).
In Ireland, a new National Health Protection function was established in 2022, as part of a process of public health medicine reform (5). This function takes an all-hazards approach with programmes across surveillance, health security, response and immunization, (6) and it aligns with national health system-wide reform which emphasizes public health and prevention (7). A key objective of Ireland’s recent National Health Protection Strategy (2022–2027) is to enable preparedness, prevention, early detection and optimal response to public health emergencies from all-hazards (5, 8).
A national Public Health Reform Expert Advisory Group reported in September 2023 on Ireland’s public health response to the COVID-19 pandemic (9). An independent expert review commenced in December 2023 to design a national dedicated emerging health threats function and the proposal report was published in October 2024 (10).
We aimed to identify priority areas for inclusion in an evidence-based health threats preparedness framework, informed by learnings from the COVID-19 pandemic; to inform an emerging health threats strategy and function for Ireland; and to contribute to other countries’ work in this area.
Methods
We undertook a narrative literature review to identify the components of an effective health threats preparedness framework. We identified evolving themes and priority areas in health threats preparedness, including those informed by the COVID-19 pandemic, to inform health threat preparedness framework and strategy development.
Information sources and search phases
Search terms were identified by pearl-growing from seminal papers in the field, guided by the consensus of relevant content experts. Using the assistance of an information specialist, we refined our search approach to be specific, capturing literature covering health threats, preparedness/response approach and including a global or cross-border element. The search terms used are included as Box 1. Peer-reviewed and grey literature publications were identified by hand-searching electronic databases, PubMed and Google Scholar, including use of the advanced search feature. A librarian-curated feed (provided by the Health Service Executive (HSE) Library) was also available, which identified relevant papers for inclusion. Additional publications were identified by citation chasing. Targeted hand-searching of the World Health Organization (WHO) and the European Centre for Disease Prevention and Control (ECDC) websites was carried out to identify key strategy and framework documents for inclusion in this review. The initial search covered January 2017 to June 2022 (Phase 1), to develop an initial health threats preparedness framework and was conducted in July 2022, for the launch of Ireland’s first National Health Protection Strategy [5]. The search was updated in February 2024 to cover July 2022 to January 2024 (Phase 2). This was to ensure that relevant and up-to-date literature was captured to inform framework development, including post-pandemic lessons learned.
BOX 1. Search terms
Health threats, health protection threats, communicable disease threats, health threats preparedness, health hazards, public health emergency preparedness and/or planning, response to all hazards, pandemic preparedness, outbreak preparedness and/or response, chemical, biological, radiological and nuclear (CBRN) threats, health security, International Health Regulations (IHR), cross-border health security, port health, international, operational, model, structure, programme.
Eligibility criteria
Publications pertaining to health threats preparedness, particularly those presented through a programmatic or strategic lens, were included in this review. These included peer-reviewed publications and relevant grey literature documents published on organizational websites. Grey literature documents included in this review comprised strategy documents, action plans, frameworks, policy briefs, reports published nationally or internationally, and documents published by international organizations. Documents or publications covering only specific non-communicable health threats were excluded.
Data extraction
Identified full texts underwent single stage screening by one person. Data extraction was undertaken by two researchers in both phases. All outputs were appraised and validated by at least two independent researchers. Findings reported in the included full texts were extracted using a data extraction tool. This tool recorded the author, year of publication, a summary of the key points reported by the authors and the relevant strategic objectives for health threats preparedness that were stated in the document. When extracting data from the full texts included in this review, we employed the steps of two reviewers’ initial familiarization with the full text, thematic categorization, theme review and consensus thematic definition by all authors to achieve a summary of priority key points and relevant strategic objectives for health threats preparedness. Data were collated and compiled under the headings reported in this literature review reflecting those priority areas. A table of included documents is included as Supplementary Table S1.
Results
Study selection
The literature search yielded 116 articles and following removal of duplicates and title, abstract and full text review, 78 articles were included; 27 articles from electronic database searches, and 51 grey literature articles (Figure 1).
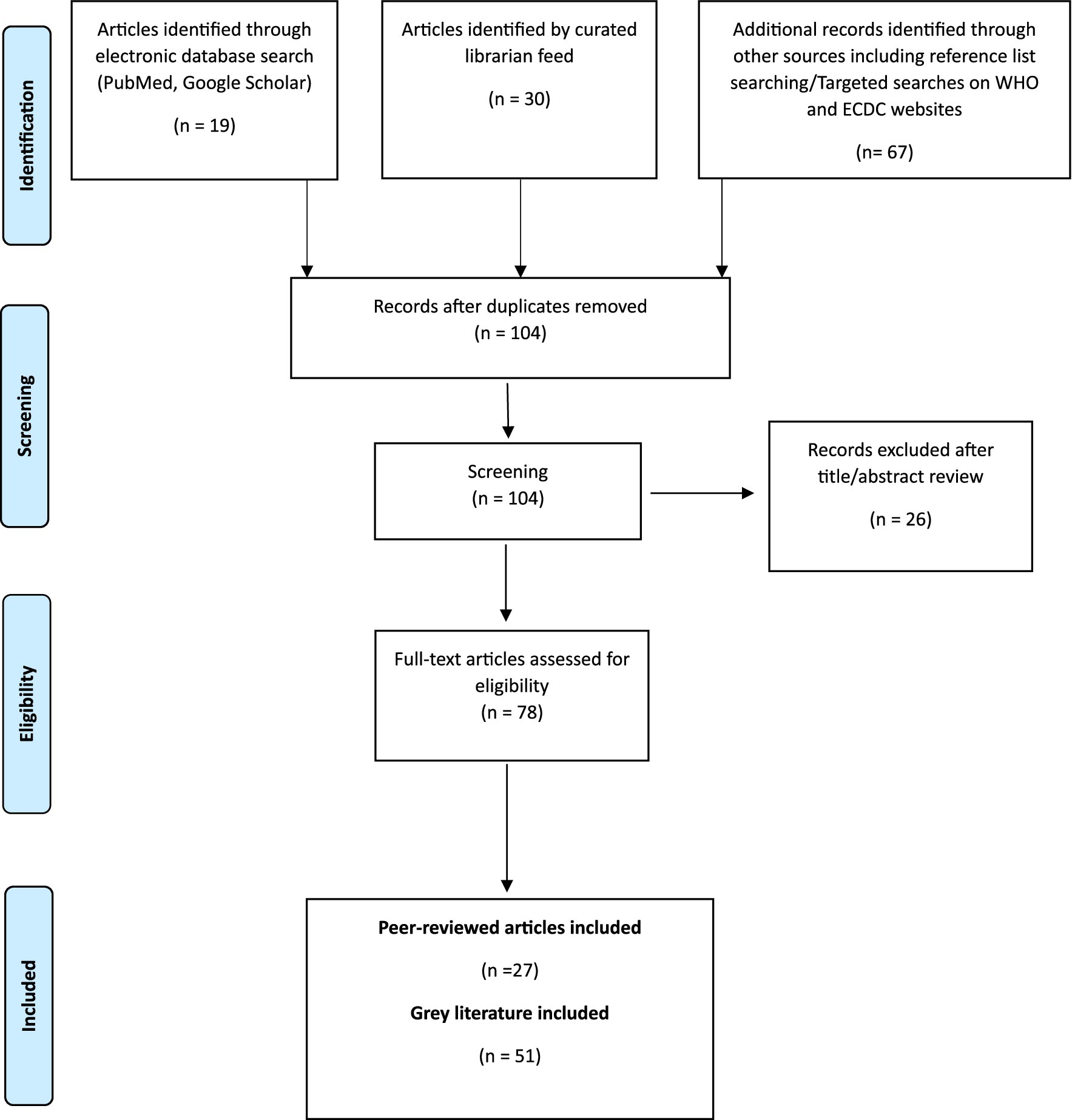
Figure 1. Flow diagram of literature search.
Priority components for a health threats preparedness framework
We report our findings in the context of recent shifts in EU policy and legislation since the onset of the COVID-19 pandemic to strengthen countries’ readiness for serious cross border threats to health. From the literature we propose a health threats preparedness framework with three overarching priorities and 10 key components (Figure 2).

Figure 2. Health threats preparedness framework consisting of three overarching priorities and ten key components.
Overarching priorities
Rapid decision-making
The COVID-19 pandemic highlighted the need for rapid decision-making in response to health threats (11, 12). Public health decision-making at local, national, regional and global levels must be based on real-time, accurate data (13, 14). Rapid decision-making therefore requires prompt identification of threats followed by evidence-based, data-driven, inclusive decision-making to guide timely response (11). Recently strengthened EU legislation is a key enabler, emphasizing the need for early warning systems, partnership with key stakeholders to approach decisions from a One Health approach and joint procurement of medical countermeasures (15). The establishment of the Health Emergency Preparedness and Response Authority (HERA) will enable access to medical countermeasures in a timely manner (16, 17). Shared analysis of threats and jointly agreed priorities for action will strengthen rapid decision-making, with community empowerment key (16, 18).
Outcomes-based
Measuring the components of emergency preparedness is challenging (19). The COVID-19 pandemic identified limitations in how health threats preparedness is measured (11, 20, 21). The pandemic highlighted how markers of preparedness, e.g., measuring capacities, did not correlate with pandemic outcomes (22). Achieving core capacities may not adequately prepare countries for a high-impact health threat (23). An outcomes-based approach has been proposed as an alternative to traditional capacity assessments (21). This approach would evaluate the implementation of interventions and their outcomes and may be more beneficial in identifying preparedness weaknesses (21). Further work is required to develop and validate indicators for relevant outcomes (22). It has been recognized that preparedness assessment should consider contextual factors in which emergencies occur, such as the sociopolitical environment, which may influence outcomes (21).
Ethical approach
Ethical principles and values are central to public health practice (24). Values important to health threats preparedness include equity, trust, public protection, duty of care and solidarity (12, 24–26). These considerations are important in the context of limited resources, challenges with access to medical countermeasures and underlying issues with public trust (24). The COVID-19 pandemic highlighted inequity and the need for an inclusive, equitable approach to preparedness and response (17, 20, 26–28). The pandemic also emphasized the need for information to be communicated accurately, consistently and coherently (11). The operationalization of an ethical approach involves anticipating risks and undertaking preparedness activities specific to relevant, vulnerable populations. These specific activities should inform the development of strategic objectives, priority actions and goals, recognizing vulnerabilities of specific population groups, such as children and those in minority groups (29–32). There is no clear method of monitoring the application of an ethical approach to health threats preparedness reported in the literature.
Ten key components
International enablers
The new European Health Union coordinates EU preparedness activities (33). The 2021 establishment of HERA with its focus on stockpiling, medical countermeasures and data flow, has improved the ability of health systems to respond to health threats in a coordinated manner (16, 18). The EU4Health programme reinforces crisis preparedness, and the strengthened mandate of the ECDC and the Health Security Committee provide critical support for countries in threat preparedness and response (17, 33, 34).
Updated international legislation and regulations emphasize prevention and strengthening of health security (12, 15, 17). The EU Regulation on serious cross border threats to health (2022/2371) covers areas such as cross-EU joint procurement for medical countermeasures, strengthening surveillance activities and establishing EU reference laboratories; key enablers for national threats functions (15). The Regulation aligns with priorities identified in the literature as core components for health threats preparedness, including interoperability, collaboration and an all-hazards approach (17, 22, 24, 35, 36).
Clear governance
Clear governance structures are necessary both at EU member state level and cross-border, alongside public health and political leadership, promoting a culture of preparedness (31, 37). Integration of public health with health and non-health sectors, with explicit leadership and partnership with appropriate accountability, is essential for a coordinated, interoperable, cross-sectoral approach (13, 24, 38). The COVID-19 pandemic highlighted he imperative to improve health governance globally (39, 40).
Understanding and defining where public health sits within governance structures is key; requiring clarity in the identification of principal agencies and authorities, especially in response to non-infectious health threats (13, 24, 41). Establishing roles and responsibilities of stakeholders, with clear governance structures is crucial for preparedness (3, 11, 41, 42).
Active partnerships
A partnership approach to health threats preparedness is emphasized in legislation (12, 15). Preparedness is not an exclusive function of health sectors; it is a shared responsibility requiring a whole-of-government, whole-of-society approach (13, 41, 43–45). Stakeholder mapping and prioritization, strong relationships and partnerships between government sectors, health sectors, commercial sectors, communities and within society can achieve collective preparedness (13, 15, 24, 35, 39, 43–47).
There are increasing risk factors for health emergencies, including climate change and environmental degradation (13, 20, 36, 48–51). Threats to health security can rapidly affect multiple countries highlighting the need for collective preparedness and for more effective international collaboration, active partnerships and common strategic plans (12, 15, 41).
Intersectoral collaboration
Effective intersectoral and multisectoral collaboration in health threats preparedness remains a challenge (31, 41, 52). Health threats preparedness frameworks should include a One Health and all-hazards approach, with support of hazard-specific plans (21, 22).
One health approach
Emerging zoonotic threats and antimicrobial resistance (AMR) threaten both human and animal health, necessitating a One Health approach (35, 45, 52, 53). Responding to the challenges of emerging and re-emerging infections requires strengthening of surveillance, risk assessment and laboratory capacity, and risk communication (35, 47). Information sharing and co-operation between human and animal health services are essential (13, 43). A key lesson from the COVID-19 pandemic is that the concept of One Health should be operationalized at all levels and a One Health approach to disease surveillance should be incorporated into preparedness (11, 21, 28, 39). Countries should invest in One Health preparedness and focus on developing multisectoral and intersectoral collaboration (21, 54).
All-hazards approach, complemented by hazard-specific measures
An all-hazards approach recognizes that risks to human health can emerge from diverse sources, including infections transmitted via goods, food, water or animals as well as chemical, radiation, nuclear and environmental events (30–32, 46, 52). Chemical, biological, radiological and nuclear (CBRN) refers to categories of materials and agents that could harm society due to their accidental or deliberate release, dissemination or impacts (43, 55, 56). CBRN incidents require specific preparedness and response (32, 44, 55, 57, 58). Many elements of preparedness are common to all-hazards (3, 44, 59). Therefore, a common, coordinated intersectoral approach, comprising both all-hazard and hazard-specific measures and capabilities, is required and is mandated by legislation (15, 23, 35, 36, 46, 60).
Threat and risk assessment
All-hazard risk-mapping is required to inform health threat preparedness (31, 52). Identifying and prioritizing threats and the capabilities required to prepare and respond is essential (60, 61). Risk assessments can be undertaken using tools developed by WHO, e.g., the Strategic Toolkit for Assessing Risks (STAR) or the risk communication and community engagement tool (3, 22, 62). WHO benchmarks for strengthening emergency capacities include having established rapid risk assessment processes linked to response plans (63).
While WHO guidance has been designed to be adapted to individual country situations, capacities and requirements (3), there has been a lack of a common methodology used by countries for assessing risk, as well as different perceptions as to what risks are; leading to different policies and different levels of preparedness and response capabilities (55, 56, 61, 64, 65). The need for rationalizing and coordinating risk assessment frameworks incorporating learnings from the COVID-19 pandemic, while allowing countries to identify relevant hazards has been recognized (21, 41).
Surveillance: information for action
Robust and accurate surveillance data are crucial to health threats preparedness, particularly identification of novel pathogens (15, 66, 67). National surveillance systems must be capable of timely detection, assessment and analyses of epidemiological data, including laboratory results, for informed decision-making and reporting of outbreaks and other public health risks (15, 31, 46, 51, 68). Surveillance systems should include indicator and event-based surveillance and should adopt a One Health, all-hazards approach (15, 22, 41, 55, 56, 69, 70). Surveillance must be supported by digital platforms and by integrated, efficient, effective and timely early warning systems, particularly for priority hazards (17, 31, 41, 67, 68). Notification to early warning systems should be supported by having updated contact points and standard operating procedures (4). Data sharing procedures across sectors and regionally and nationally should be strengthened to enable collaborative surveillance (31, 39). Genomic surveillance expanded during the COVID-19 pandemic and is important to strengthen surveillance and increase capacity to detect health threats (71). Genomic data can inform risk assessment, development of medical countermeasures and public health decision-making (72).
Communication including community engagement
Communication is dependent on partnership and collaboration within and outside health sectors (13, 24). Intersectoral risk communication should communicate health threats in a timely, coordinated and transparent manner (3, 31, 55) to enable decision-makers, stakeholders and the public to make informed and appropriate decisions. Risk communication requires adequate resources and multiple communication modalities (4, 35). An all-hazard emergency risk communication function should be integrated into national action plans for emergency preparedness (15, 56). The COVID-19 pandemic highlighted the complexity of communication in a pandemic and the importance of accurate, scientific, expert-led, risk communication during a pandemic (41, 73, 74). It also highlighted communication challenges in the context of scientific uncertainty, an abundance of information, and infodemic management (20, 73, 75).
Community engagement is essential for effective risk communication and preparedness (4, 35, 41, 43, 68, 74). Active, two-way engagement is key to understanding risk perception and identifying and addressing myths and disinformation (53). Communication campaigns for health emergencies should be grounded in behavioral science, and should consider cultural contexts and inclusive language for all populations (20, 53). Investment is key before, during and after health emergencies to enable individuals, families and communities to engage in preparedness (20, 28, 76).
Operational readiness (incorporating health systems)
Achieving operational readiness involves establishing, strengthening and maintaining a multisectoral response infrastructure which focuses on the highest priority all-hazard risks (13, 38, 62). This requires political commitment, coordination, risk assessment, infrastructure, preparedness plans, resources, training, and expert knowledge (13). Health emergencies weaken health systems and weak health systems worsen health emergencies (30, 31). Preparedness is part of health system resilience (77). However, building resilience in health systems is challenging (78). Robust, sustainable and accessible health systems are essential for health threats preparedness (3, 4, 12). There is a need to strengthen health systems to support preparedness (12, 37). Health system response requires rapid risk assessment, testing, diagnostics, contact tracing, clinical evaluation and care, surge workforce and rapidly scalable interventions such as timely procurement and capacity and capability to distribute medical countermeasures (13, 36, 37, 41, 47, 52, 79).
The COVID-19 pandemic exposed vulnerabilities of national health systems and identified the need for targeted preparedness planning and long-term investment in strengthening health systems, including workforce (11, 41). Essential procurement should be informed by national risk profiles, and supply chain management systems should be strengthened to ensure operational readiness (4, 13, 31). A pre-negotiated platform for medical countermeasures would ensure rapid and equitable delivery globally (11, 20, 41, 80).
Resourcing
The COVID-19 pandemic highlighted the need for further financial investment to reduce threats, provide early warning systems and improve capacity to respond to crises (11, 40, 41, 47). Additionally, investing in the highly skilled workforce required for preparedness is essential (28, 31, 41, 70). Investment in preparedness for population health and health security must be sustainable and maintained during the period between emergencies (13). WHO recommend that resources should be integrated into national budgets and planning cycles (35, 52). Adequate resourcing includes investment in facilities, including health facilities, and other infrastructure such as laboratory testing capacities, healthcare surge capacity and management of medical countermeasures (2, 11, 19, 81). Necessary infrastructure and capacity for mobilizing resources and activating preparedness plans should be resourced, and priorities should be established for allocation of limited resources (24).
Dedicated resources should be made available to support an active research and evidence synthesis function. This should include research development and evaluations to inform and accelerate evidence-informed emergency preparedness at all levels (15, 41).
Monitoring and evaluation
Health threats preparedness plans should be updated, reviewed and tested to ensure that adequate capacity for effective preparedness and response is developed, maintained and strengthened (28). Ongoing monitoring and evaluation facilitate continuous learning for quality improvement, through reviewing experiences and incorporating lessons learned (28, 35). Examples of assessments include external evaluations, self-assessment tools, simulation exercises and after-action reviews detailed in the IHR monitoring and evaluation framework (IHRMEF) and the periodic assessments described in Article 8 of the European Regulations (15, 30, 31, 65, 82–85). The need for enhanced preparedness monitoring was a key learning from the COVID-19 pandemic (41, 49). The pandemic highlighted the need to shift focus to an outcomes-based approach for measuring preparedness (21). Ongoing work is required to determine how to effectively monitor preparedness (17).
Summary of findings
This literature review has identified key components for inclusion in a health threats framework. Our proposed framework suggests a model that can be used and adapted to inform health threats preparedness programmes. A summary of the guiding principles to aid development of a health threats framework is in Supplementary Table S2.
Discussion
The literature describes the strong international enablers for health threats preparedness which have been established since COVID-19, both legislative and structural (15). The European Health Union including HERA (16), a stronger European Medicines Agency and a more influential ECDC with increased remit of the Health Security Committee provides a strong basis to support MS threats strategy development. Commentators have discussed the interplay between European stakeholders and MS and the challenge to further clarify roles and responsibilities to avoid ambiguity, overlaps and gaps (16). Member States’ (MS) national threats functions require clear lines of governance within and external to EU health security structures, including in the areas of horizon scanning, threat assessment, procurement and stockpiling, with clarity on joined-up operational implications for MS.
National legislation on emergency response will need to be consistent with updated international legislation. This should encompass legal, administrative and other governmental instruments required to implement the legislation (47, 52) following IHR revision (12), and pandemic treaty negotiations (86). Policy development, adaptation and implementation are core capacities and capabilities to allow national focal points to perform their functions under IHR (2, 12).
Strong public health leadership and governance are described in the literature as critical to ensure resilience, sustainability and accountability to respond immediately to health threats. In Ireland, a Public Health intra-action review of the COVID-19 response found governance to be a leading challenge (87). As with many MS, reform is underway in Ireland; alongside Public Health reform (9) and health service overarching reform (7), it is critical to maintain and further develop our health protection capacities and capabilities to lead on interoperable preparedness and response (5). In Ireland, the strengthening of a health threats function is underway to ensure that the health system is equipped to identify and respond to future crises arising from all hazards. Ongoing reform within our health service and within public health is an opportunity to identify gaps including the need to enhance all hazards surveillance, and strengthen a One Health approach (10).
Active partnerships and intersectoral collaboration are central to any health threats strategy. In addition to much grey literature recently in this area, with a focus on One health and all-hazards, authors discuss the imperative for partnerships in preparedness to enable interoperable response (11, 13, 15, 21, 28, 46). The implication for national frameworks/strategies is to establish partnerships in all key areas, to leverage and build on existing networks, to avoid overlap and bring cohesion, and to plan and exercise scenarios together ahead of any event. A whole-of-government and whole-of-society, national and international approach is critical (13, 41, 43–45). In Ireland, we must continue to identify and focus on vulnerable groups and underserved populations to ensure an equitable and ethical approach to health threats preparedness. This will require collaboration with social and behavioral scientists to tailor consistent and transparent communication before, during and after emergencies.
From the literature other key areas include threat and hazard assessment, informed by surveillance across all-hazards; it will be a new challenge for countries to move beyond the traditional infectious disease focus. Community engagement is critical, particularly for public health social measures (88). Nationally, the health protection function works with key stakeholders including advocacy groups, the HSE national social inclusion office and community representatives. Establishing these collaborative relationships in advance of the next health emergency is crucial and involves co-developing interventions and communications, identifying key influencers and building trust to deliver public health messages.
Literature from mid-2022 onwards critiques the narrow focus pre-COVID within the health system on capacities: the need to build and maintain wider capabilities has been described (60) with proposed frameworks to support ‘health capabilities-based planning’ (examples include capability to provide personal protective equipment (PPE) for staff, capability to undertake waste sterilization) for multiple and diverse threats (60).
Resourcing is often siloed by sector (21), and the imperative for joined-up interoperable preparedness is key, including resourcing of cross-sectoral research activities to guide evidence-based preparedness. In Ireland, the importance of funding and adequate resources for public health, including all aspects of health threats preparedness, has been acknowledged (10). Maintaining focus on the resources required health threats preparedness outside of crisis situations is essential but remains challenging (10).
Post COVID-19, monitoring of preparedness may need to further develop beyond those currently in use such as WHO SPAR (89) and EU Article 8 (15). Some suggest that intercountry comparison is unhelpful (52). The use of matrix models has been suggested, to monitor and assess achievement of outcomes (21). Individual countries should plan, test and exercise in challenging scenarios testing multisectoral interoperability, communications and connectedness, establishing a baseline within a national context and building on this (21).
Extrapolating from this literature review, we propose that a transformation initiative is needed to support the three overarching themes of rapid shared decision-making, outcomes-based approach, using an ethical lens, and to operationalize the 10 key components.
There has been a call for change from other commentators to ‘facilitate the development of thinking towards systems-based, all-hazards frameworks that acknowledge the wider complexities within which public health operates’ with the socio-political context being key (21). ‘Cross disciplinary thinking’ is described in one paper in developing preparedness tools including addressing inequities. Our threats strategy must incorporate preparedness for special population subgroups with different characteristics both in preparedness planning and response scenarios (32), taking account of issues such as vulnerability, shared governance, access, language and cultural norms (20).
Successful transformation requires that external factors must be taken into account: using for example a PESTLE analysis to monitor the macro environment, including megatrends (90). Scenario planning is being used at EU level to test readiness (91, 92). Preparedness plans of all MS will be assessed under EU legislation over the next 3 years (15); sharing of approaches across countries will support European MS to transform towards best practice, with cross-border interoperability.
A national approach to emerging health threats, in both preparedness and response phases, is a reflection of the national environment at both a political and operational health response level. The application of the 10 key components identified across the three overarching priority areas in any given MS would need to be cognizant of the political environment in which a system is operating, and we present here a brief reflection on this interplay in Ireland, to assist readers in applying the findings in their own political context.
Pre-pandemic, Ireland was facing the unique political challenge of Brexit, requiring additional focus on cross border coordination in health threat preparedness and management (93). Post-pandemic, in October 2024 Ireland’s Expert Group on Emerging Health Threats reported with recommendations to strengthen national emerging threat preparedness, building on innovations that occurred during the pandemic (10). Their report reflects the key components of a threat preparedness framework that we found in this literature review, including shared cross-border surveillance, community engagement and active partnership across the two jurisdictions on the island of Ireland (10).
We consider our experience in Ireland regarding the three overarching priorities identified in this literature review: rapid decision-making, outcomes-based approach and ethical approach. Regarding decision-making, one strength in Ireland’s COVID-19 response was a collaborative approach between political leadership, the Department of Health and the Health Service Executive in Ireland, with response centrally coordinated at the highest political level in the country. However, the challenge of governance/accountability and communication across the health system at the onset of this pandemic has been noted; a detailed review of measures for Nursing Home covering the period to end 2021 recommended linked cross-sectoral teams across the community, with rapid communication channels (94).
For the priority area of outcomes, in Ireland excess mortality was comparatively low and vaccination rates were among the highest in Europe (9). Evidence is now accumulating on unintended consequences of COVID-19 response across Ireland and Europe (95–97), which must be considered as we prepare for any future event.
An ethical and values driven approach is more difficult to measure. Ireland’s National Public Health Emergency Team were advised by a Pandemic Ethics Advisory Group (98) but clearly there are numerous aspects of the response to be considered under an ethical spotlight. In Ireland, a review of the COVID-19 response has recently commenced (October 2024) (99), to provide recommendations to strengthen decision-making, to assist in assessing and balancing the complexity of potential trade-offs for decisions, along with the need for speed and agility, and to provide a framework to ensure democratic processes and civil rights are safeguarded in context of whole of society responses to rapidly moving threats (10, 98).
Limitations
This was a narrative literature review and thus lacks the rigor of a systematic review. Our search was guided by the needs/aims of the review and the subject matter expertise of the team. This approach and the biphasic search strategy may limit the reproducibility of this work. We noted a gap in the literature in relation to country-specific operational structures used in health threats preparedness programmes. Supplementary research, such as qualitative stakeholder consultation, or a targeted scoping review, is required to address this gap. Recent high-level work undertaken, reviewing Public Health systems and structures internationally (100), can inform further development of operational structures focused on all-hazard threats.
Conclusion
As we emerge from the COVID-19 pandemic, we have an opportunity to reflect and consider how best to prepare for such a future eventuality.
This literature review has informed a framework to contribute towards the development of a national evidence-based health threats strategy. A national strategy must be underpinned by multi-level, multisectoral engagement and a whole-of-society, whole-of-government approach that is built on leadership, partnership, collaboration and coordination both nationally and internationally. It must enable rapid decision-making, have a focus on outcomes for our populations, and be ethically sound. Partnership permeates through much of the literature: we must work together across sectors, collaborating with communities, and across boundaries and borders, developing common understandings. Public health leadership, advocacy and collaboration will be essential to the design and implementation of this evidence-informed initiative; working to prevent and protect our populations against diverse health threats.
Our proposed framework for health threats preparedness contains several elements identified in previous frameworks for health threats preparedness, including an emphasis on governance, collaboration and partnership (24). Moreover, our proposed framework also incorporates learnings arising from the COVID-19 pandemic, nationally and internationally (9, 11) and highlights the importance of strengthening systems to enable rapid decision-making and the imperative of participatory community engagement. Additionally, our framework includes more recently proposed approaches such as an outcome-based approach (90), and places all these priorities in the context of relevant legislative and regulatory frameworks (15).
This framework proposes a comprehensive, up to date and evidence-based approach to health threats preparedness which is being used to progress reform and preparedness nationally and may be of interest to other countries who are strengthening health threats preparedness activities. A resourced strategic transformation initiative, based on evidence and context, will enable Ireland to prepare and respond to future threats within the increasingly complex systems in which health emergencies occur.
Author contributions
LM: Conceptualization, Formal analysis, Methodology, Writing – original draft, Writing – review & editing. JG: Formal analysis, Methodology, Writing – original draft, Writing – review & editing. MW: Methodology, Writing – original draft, Writing – review & editing. RP: Conceptualization, Methodology, Writing – original draft, Writing – review & editing. MB: Conceptualization, Formal analysis, Methodology, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
We would like to thank Cliodhna O’Mahony from the Health Security Programme for her assistance with the graphics presented in this manuscript. We would also like to thank Gethin White, Health Service Executive Health Library, Dr. Steevens Hospital, Dublin, Ireland, for his assistance with the literature search.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1490850/full#supplementary-material
References
1. McKee, M, and de Ruijter, A. The path to a European health union. The Lancet Regional Health–Europe. (2024) 36:100794. doi: 10.1016/j.lanepe.2023.100794
2. European Centre for Disease Prevention and Control. Public health emergency preparedness – Core competencies for EU member states. Stockholm: ECDC (2017).
3. World Health Organization. WHO guidance on preparing for National Response to health emergencies and disasters. Geneva: WHO (2021).
4. European Centre for Disease Prevention and Control. Health emergency preparedness for imported cases of high-consequence infectious diseases. Stockholm: ECDC (2019).
5. Health Service Executive. Health service executive health protection strategy 2022–2027. Dublin, Ireland: Health Service Executive (2022).
6. Health Service Executive. Health service executive health protection strategy 2022–2027: Year one implementation report. Ireland: Health Service Executive (2023).
7. Committee on The Future of Healthcare. Committee on the future of healthcare-Sláintecare report. Dublin: Houses of the Oireachtas (2017).
8. Kelly C, Gallagher J, Odewumi L, Conway R, Black ME, Concannon K, et al. The approach to developing Ireland’s first national health protection strategy and lessons learnt, December 2021 to October 2022. Eur Secur. (2024) 29:2300326. doi: 10.2807/1560-7917.ES.2024.29.14.2300326
9. Public Health Reform Expert Advisory Group. Report of the public health reform expert advisory group. Ireland: Government of Ireland (2023).
10. Emerging Health Threats Function Expert Steering Group. Report of the emerging health threats function expert steering group. Ireland: Department of Health (2024).
11. European Observatory on Health Systems and Policies. Drawing light from the pandemic: A new strategy for health and sustainable development. Copenhagen: World Health Organization. Regional Office for Europe (2021).
12. World Health Organization. Working group on amendments to the international health regulations (2005). Geneva: WHO (2024).
13. World Health Organization. A strategic framework for emergency preparedness. Geneva: World Health Organization (2017).
14. European Commission. Introducing HERA, the European health emergency preparedness and response authority, the next step towards completing the European health union. Brussels: European Commission (2021).
15. European Parliament and Council of the European Union. Regulation (EU) 2022/2371 of the European Parliament and the council of 23 November 2022 on serious cross-border threats to health and repealing decision no 1081/2013/EU. Luxembourg: Official Journal of the European Union (2022).
16. Wouters, OJ, Forman, R, Anderson, M, Mossialos, E, and McKee, M. The launch of the EU health emergency preparedness and response authority (HERA): improving global pandemic preparedness? Health policy. (2023) 133:104844. doi: 10.1016/j.healthpol.2023.104844
17. Kokki, M, and Ammon, A. Preparing Europe for future health threats and crises - key elements of the European Centre for Disease Prevention and Control's reinforced mandate. Euro surveillance: bulletin Europeen Sur les maladies transmissibles =. Eurp Commun Dis Bull. (2023) 28. doi: 10.2807/1560-7917.ES.2023.28.3.2300033
19. Stoto, MA, Nelson, C, Savoia, E, Ljungqvist, I, and Ciotti, M. A public health preparedness logic model: assessing preparedness for cross-border threats in the European region. Health Secur. (2017) 15:473–82. doi: 10.1089/hs.2016.0126
20. World Health Organization. Strategic preparedness, readiness and response plan to end the global COVID-19 emergency in 2022. Geneva: WHO (2022).
21. Traore, T, Shanks, S, Haider, N, Ahmed, K, Jain, V, Rüegg, SR, et al. How prepared is the world? Identifying weaknesses in existing assessment frameworks for global health security through a one health approach. Lancet. (2023) 401:673–87. doi: 10.1016/S0140-6736(22)01589-6
22. Lee, JM, Jansen, R, Sanderson, KE, Guerra, F, Keller-Olaman, S, Murti, M, et al. Public health emergency preparedness for infectious disease emergencies: a scoping review of recent evidence. BMC Public Health. (2023) 23:420. doi: 10.1186/s12889-023-15313-7
23. Johns Hopkins Center for Health Security. Preparedness for a high-impact respiratory pathogen pandemic. Maryland: Johns Hopkins Center for Health Security (2019).
24. Khan, Y, O’Sullivan, T, Brown, A, Tracey, S, Gibson, J, Généreux, M, et al. Public health emergency preparedness: a framework to promote resilience. BMC Public Health. (2018) 18:1344. doi: 10.1186/s12889-018-6250-7
25. Sharp, A, Jain, V, Alimi, Y, and Bausch, DG. Policy and planning for large epidemics and pandemics – challenges and lessons learned from COVID-19. Curr Opin Infect Dis. (2021) 34:393–400. doi: 10.1097/QCO.0000000000000778
26. McCoy, D, Roberts, S, Daoudi, S, and Kennedy, J. Global health security and the health-security nexus: principles, politics and praxis. BMJ Glob Health. (2023) 8:e013067. doi: 10.1136/bmjgh-2023-013067
27. Alakija, A. Leveraging lessons from the COVID-19 pandemic to strengthen low-income and middle-income country preparedness for future global health threats. Lancet Infect Dis. (2023) 23:e310–7. doi: 10.1016/S1473-3099(23)00279-7
28. World Health Organization. Strengthening pandemic preparedness planning for respiratory pathogens. Geneva: WHO (2022).
30. World Health Organization. NAPHS for All. A 3 step strategic framework for National Action Plan for health security. Geneva: WHO (2018).
31. World Health Organization. NAPHS for all: A country implementation guide for national action plan for health security (NAPHS). Geneva: WHO (2019).
32. Winters, TA, Cassatt, DR, Harrison-Peters, JR, Hollingsworth, BA, Rios, CI, Satyamitra, MM, et al. Considerations of medical preparedness to assess and treat various populations during a radiation public health emergency. Radiat Res. (2023) 199:301–18. doi: 10.1667/RADE-22-00148.1
33. Eerens, D, Hrzic, R, and Clemens, T. The architecture of the European Union’s pandemic preparedness and response policy framework. Eur J Pub Health. (2022) 33:42–8. doi: 10.1093/eurpub/ckac154
34. Parliament, E. Regulation (EU) 2021/22 of the European Parliament and of the council establishing a Programme for the Union's action in the field of health (EU4Health Programme) for the period 2021–2027. Brussels: European Parliament (2021).
35. World Health Organization. Asia Pacific strategy for emerging diseases and public health emergencies (APSED III): advancing implementation of the international health regulations (2005): Working together towards health security. Manila: WHO Regional Office for the Western Pacific (2017).
37. Lal, A, Abdalla, SM, Chattu, VK, Erondu, NA, Lee, T-L, Singh, S, et al. Pandemic preparedness and response: exploring the role of universal health coverage within the global health security architecture. Lancet Glob Health. (2022) 10:e1675–83. doi: 10.1016/S2214-109X(22)00341-2
38. Naughton, P, Kelly, C, White, P, Kennedy, E, Healy, A, Collins, A, et al. Lessons from inter-disciplinary collaboration to mitigate SARS-CoV-2 transmission in schools, Ireland, 2020/2021, to inform health systems and multisectoral recovery. Front Public Health. (2022) 10:1072566. doi: 10.3389/fpubh.2022.1072566
39. World Health Organization. Strengthening WHO preparedness for and response to health emergencies. Geneva: WHO (2023).
40. Deloitte Centre for Health Solutions. Bridging the gap: Protecting the nation from public health threats. London: Deloitte Centre for Health Solutions (2021).
41. World Health Organization. Preparedness and resilience for emerging threats module 1: Planning for respiratory pathogen pandemics. Geneva: WHO (2023).
42. The Lancet Global Health. The future of the international health regulations. Lancet Glob Health. (2022) 10:e927. doi: 10.1016/S2214-109X(22)00254-6
43. Department of Health and Human Services. National Health Security Strategy 2019–2022. USA: Department of Health and Human Services (2019).
44. European Commission. Action plan to enhance preparedness against chemical, biological, radiological and nuclear security risks. Brussels: European Commission (2017).
45. The Australian Government Department of Health. Australia's National Action Plan for health security 2019–2023. Australia: The Australian Government Department of Health (2018).
46. World Health Organization. International health regulations (2005) -3rd edition. Geneva: WHO (2016).
47. World Health Organization. Report of the review committee in the functioning of the international health regulations (2005) during the COVID-19 response. Geneva: WHO (2021).
48. Phuong, J, Riches, NO, Calzoni, L, Datta, G, Duran, D, Lin, AY, et al. Toward informatics-enabled preparedness for natural hazards to minimize health impacts of climate change. J Am Med Inform Assoc. (2022) 29:2161–7. doi: 10.1093/jamia/ocac162
49. Gontariuk, M, Krafft, T, Rehbock, C, Townend, D, Van der Auwermeulen, L, and Pilot, E. The European Union and public health emergencies: expert opinions on the Management of the First Wave of the COVID-19 pandemic and suggestions for future emergencies. Front Public Health. (2021) 9:9. doi: 10.3389/fpubh.2021.698995
50. Public Health England. PHE infectious diseases strategy 2020–2025. England: Public Health England (2019).
52. World Health Organization. Action plan to improve public health preparedness and response in the WHO European region 2018–2023. Denmark: WHO (2019).
53. European Centre for Disease Prevention and Control. A literature review on community and institutional emergency preparedness synergies. Stockholm: ECDC (2017).
54. Elnaiem, A, Mohamed-Ahmed, O, Zumla, A, Mecaskey, J, Charron, N, Abakar, MF, et al. Global and regional governance of one health and implications for global health security. Lancet. (2023) 401:688–704. doi: 10.1016/S0140-6736(22)01597-5
55. Parliament, E. Member States' preparedness for CBRN threats. Brussels: European Parliament (2018).
56. Parliament, E. EU preparedness and responses to chemical, biological, radiological and nuclear (CBRN) threats. Brussels: European Parliament (2021).
57. Gromek, P, and Szklarski, Ł. Modern technologies in enhancing situational awareness and preparedness for CBRN events in urban areas. Perspective of European Commission call in 2022. Journal of modern. Science. (2023) 53:362–90. doi: 10.13166/jms/176678
58. Nazari, S, Sharififar, S, Ahmadi Marzaleh, M, Zargar, S, Azarmi, S, and Akbari, SY. Structural elements and requirements in forming prehospital health response teams in response to chemical, biological, radiation, and nuclear incidents (CBRN), a comparative review study. Disaster Med Public Health Prep. (2023) 17:e300. doi: 10.1017/dmp.2022.259
59. Centers for Disease Control and Prevention. CDC Global Health strategy 2019–2021. USA: CDC (2019).
60. Zawadzki, M, and Montibeller, G. A framework for supporting health capability-based planning: identifying and structuring health capabilities. Risk Anal. (2023) 43:78–96. doi: 10.1111/risa.14014
61. European Centre for Disease Prevention and Control. ECDC tool for the prioritisation of infectious disease threats – Handbook and manual. Stockholm: ECDC (2017).
62. Ario, AR, Makumbi, I, Bulage, L, Kyazze, S, Kayiwa, J, Wetaka, MM, et al. The logic model for Uganda's health sector preparedness for public health threats and emergencies. Glob Health Action. (2019) 12:1664103. doi: 10.1080/16549716.2019.1664103
63. World Health Organization. WHO benchmarks for strengthening health emergency capacities. Geneva: WHO (2023).
64. Wijesinghe, PR, Ofrin, RH, Bhola, AK, Inbanathan, FY, and Bezbaruah, S. Pandemic influenza preparedness in the WHO South-East Asia region: a model for planning regional preparedness for other priority high-threat pathogens. WHO South-East Asia journal of public health. (2020) 9:43–9. doi: 10.4103/2224-3151.282995
65. European Centre for Disease Prevention and Control. HEPSA – Health emergency preparedness self-assessment tool. Stockholm: ECDC (2018).
66. European Centre for Disease Prevention and Control. ECDC Strategy 2021–2027. Stockholm: ECDC (2021).
67. European Centre for Disease Prevention and Control. Long-term qualitative scenarios and considerations of their implications for preparedness and response to the COVID-19 pandemic in the EU/EEA. Stockholm: ECDC (2022).
68. Department of Health and Social Care. Transforming rhe public health system: Reforming the public health system for the challenge of our times. United Kingdom: Department of Health and Social Care (2022).
69. Welsh Government. The communicable disease outbreak plan for Wales. Wales: Government of Wales (2020).
70. Department of Health and Human Services. Strategic plan for 2020–2023. USA: Department of Health and Human Services (2020).
71. World Health Organization. Update to requirements for reporting COVID-19 surveillance data under the international health regulations (IHR 2005). Geneva: WHO (2023).
72. World Health Organization. Global genomic surveillance strategy for pathogens with pandemic and epidemic potential, 2022–2032. Geneva: WHO (2022).
73. Berg, SH, Shortt, MT, Røislien, J, Lungu, DA, Thune, H, and Wiig, S. Key topics in pandemic health risk communication: a qualitative study of expert opinions and knowledge. PLoS One. (2022) 17:e0275316. doi: 10.1371/journal.pone.0275316
74. European Centre for Disease Prevention and Control. The Swedish advice-making process for distance learning in schools, November 2020–April 2021. An after-action review. Stockholm: ECDC (2023).
75. European Centre for Disease Prevention and Control. The EU experience in the first phase of COVID-19: Implications for measuring preparedness. Stockholm: ECDC (2022).
76. European Centre for Disease Prevention and Control. Community engagement for public health events caused by communicable disease threats in the EU/EEA. Stockholm: ECDC (2020).
77. Copeland, S, Hinrichs-Krapels, S, Fecondo, F, Santizo, ER, Bal, R, and Comes, T. A resilience view on health system resilience: a scoping review of empirical studies and reviews. BMC Health Serv Res. (2023) 23:1297. doi: 10.1186/s12913-023-10022-8
78. Ewert, B, Wallenburg, I, Winblad, U, and Bal, R. Any lessons to learn? Pathways and impasses towards health system resilience in post-pandemic times. Health Econ Policy Law. (2022) 18:66–81. doi: 10.1017/S1744133122000238
79. Li, MK, Sodhi, MS, Tang, CS, and Yu, JJ. Preparedness with a system integrating inventory, capacity, and capability for future pandemics and other disasters. Prod Oper Manag. (2023) 32:564–83. doi: 10.1111/poms.13887
80. The independent panel for pandemic preparedness and response. COVID-19: make it the last pandemic (2021).
81. Rose, DA, Murthy, S, Brooks, J, and Bryant, J. The evolution of public health emergency management as a field of practice. Am J Public Health. (2017) 107:S126–33. doi: 10.2105/AJPH.2017.303947
82. Naik, R, Maxwell, N, Jones, T, and Dopson, SA. Public health emergency preparedness: qualitative analysis of after-action reports. Disaster Med Public Health Prep. (2023) 17:e523. doi: 10.1017/dmp.2023.201
83. European Centre for Disease Prevention and Control. Conducting in-action and after-action reviews of the public health response to COVID-19: Update. Stockholm: ECDC (2023).
84. European Union Strengthened international health regulations & preparedness in the EU. Monitoring and evaluation of IHR (2005) core capacities and implementation of decision 1082/2013/EU at the European level. The European Commission (2023).
85. World Health Organization. International health regulations monitoring and evaluation framework. Geneva: WHO (2018).
86. Taylor, L. World leaders commit to greater collaboration over future pandemics. BMJ. (2023) 382:2195. doi: 10.1136/bmj.p2195
87. O’Connor, E, O’Riordan, M, Morrissey, MC, Dever, N, O’Mahony, C, Romanowski, S, et al. A methodological approach to intra-action reviews - application and adaptation of existing global guidance during the COVID-19 pandemic response in Ireland, 2021. Euro Surveill. (2023) 28:2200475. doi: 10.2807/1560-7917.ES.2023.28.13.2200475
88. European Centre for Disease Prevention and Control. Public health and social measures for health emergencies and pandemics in the EU/EEA: Recommendations for strengthening preparedness planning. Stockholm: ECDC (2024).
89. World Health Organization. IHR states parties self-assessment annual report (SPAR) (2024) Available at: https://www.who.int/emergencies/operations/international-health-regulations-monitoring-evaluation-framework/states-parties-self-assessment-annual-reporting
90. Dente, MG, Riccardo, F, Declich, S, Milano, A, Robbiati, C, Agrimi, U, et al. Strengthening preparedness against global health threats: a paradigm shift based on one health approaches. One Health. (2022) 14:100396. doi: 10.1016/j.onehlt.2022.100396
91. Orellana García, LP, Kaur, K, Brand, H, and Schröder-Bäck, P. Scenario planning: an alternative approach to European Commission for combating antimicrobial resistance by 2050. South Eastern Eur J Public Health. (2021) 16. doi: 10.56801/seejph.vi.186
92. Nabbe, M, and Brand, H. The European health union: European Union’s concern about health for all. Concepts, definition, and scenarios. Healthcare. (2021) 9. doi: 10.3390/healthcare9121741
93. Boland, M, and O'Riordan, M. Preparedness and management of global public health threats at points of entry in Ireland and the EU in the context of a potential Brexit. Glob Health. (2019) 15:53. doi: 10.1186/s12992-019-0496-4
94. Frazer K, Mitchell L, Stokes D, Crowley E, Kelleher C. COVID-19 nursing homes expert panel examination of measures to 2021: report to the minister for health. Dublin: Department of Health (2021).
95. Janssen, C, Kover, I, Kyratsis, Y, Kop, M, Boland, M, Boersma, FK, et al. The corona pandemic and participatory governance: responding to the vulnerabilities of secondary school students in Europe. IJDRR. (2023) 88:103608. doi: 10.1016/j.ijdrr.2023.103608
96. O'Reilly, S, Kathryn Carroll, H, Murray, D, Burke, L, McCarthy, T, O'Connor, R, et al. Impact of the COVID-19 pandemic on cancer care in Ireland-perspectives from a COVID-19 and Cancer working group. J Cancer Policy. (2023) 36:100414. doi: 10.1016/j.jcpo.2023.100414
97. Guzman, V, Doyle, F, Foley, R, Craven, P, Crowe, N, Wilson, P, et al. Socio-ecological determinants of older people’s mental health and well-being during COVID-19: a qualitative analysis within the Irish context. Front Public Health. (2023) 11:11. doi: 10.3389/fpubh.2023.1148758
98. Department of Health. Ethical framework for decision making in a pandemic. Ireland: Department of Health (2020).
99. Government of Ireland. Evaluation of the response to the COVID-19 pandemic - independent pandemic evaluation panel terms of reference. Ireland: Government of Ireland (2024).
Keywords: preparedness, health threats, all-hazards, pandemic planning, emergency planning, one health, health security
Citation: Marron L, Gilroy J, Williams M, Parlour R and Boland M (2025) A narrative literature review to inform the development of a health threats preparedness framework in Ireland. Front. Public Health. 13:1490850. doi: 10.3389/fpubh.2025.1490850
Edited by:
Christine Bevc, RTI International, United StatesReviewed by:
Arnold Bosman, Transmissible Public Health Support, NetherlandsAmber Mehmood, University of South Florida, United States
Copyright © 2025 Marron, Gilroy, Williams, Parlour and Boland. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Louise Marron, bWFycm9ubEB0Y2QuaWU=