
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 28 January 2025
Sec. Infectious Diseases: Epidemiology and Prevention
Volume 13 - 2025 | https://doi.org/10.3389/fpubh.2025.1490809
This article is part of the Research TopicSARS-CoV-2 Vaccines Beyond the Pandemic EraView all 25 articles
 Ana C. Montagud1*
Ana C. Montagud1* Raul Moragues2*
Raul Moragues2* Nancy Vicente-Alcalde3,4
Nancy Vicente-Alcalde3,4 Emilia Montagud5
Emilia Montagud5 José Antonio Hurtado-Sánchez6,7
José Antonio Hurtado-Sánchez6,7 José Tuells2,7
José Tuells2,7Background: Confinement conditions in prison communities are associated with increased susceptibility to infectious outbreaks. The COVID-19 pandemic has been characterized by high transmissibility and clinical severity resulting in a high number of infections and deaths worldwide. Vaccination has been a crucial tool in mitigating its devastating effects. The aim of this study is to asses the prevalence of antibodies against the Spike protein of SARS-CoV-2 in vaccinated prisoners and staff at a specific prison in Alicante.
Methods: A cross-sectional epidemiological study was designed for the population in scope using a rapid lateral flow immunochromatography serological test, conducted on July 27, 2023. Demographic and clinical variables were collected through a questionnaire. Statistical analysis was performed using the SPSS 29.0 software.
Results: A total of 560 people participated in the study; the predominant profile was men (77.3%) with an average age of 45.7 years. 71.4% of subjects were prisoners and 28.6% were prison staff. Regarding the detection of anti-SARS-CoV-2 antibodies obtained through serological test, 60.9% of the sample gave a positive result. 69.1% of participants received the last dose in 2022 or later and 62.2% received booster doses. The vaccines administered in the last dose were Biontech/Pfizer and Moderna in 88.6% of the cases. 59.5% of sample had suffered from COVID-19 and 67.0% did not have any clinical comorbidity. In the regression analysis, it was observed that the variables with a stronger statistical relationship with presence of anti-SARS-CoV-2 antibodies were: the number of years since last vaccine dose was received (aOR: 0.08; 95%CI: 0.05; 0.16) the number of vaccine doses received (aOR: 4.8; 95%CI: 2.9; 8.0) and presenting any comorbidity (aOR: 4.3; 95%CI: 2.4; 8.0). The staff received more booster doses and obtained a better response to seropositivity, with 72.5% of anti-SARS-CoV-2 result positive while prisoners reached 56.3%.
Conclusion: The COVID-19 vaccination status within the prison community following the initiation of primary immunization and subsequent booster doses, shows a low immunization coverage (60.9%), which is below expectations given the immunization strategies implemented since the start of the pandemic. There are notable differences in vaccination rates between prison staff and prisoners. These disparities are concerning, and authorities responsible for prison public health should take a more proactive approach to ensuring vaccination among prisoners.
The conditions of prisoners in penitentiary centers are associated with greater susceptibility to infectious and transmissible diseases. Prison populations are uniquely vulnerable to infectious diseases due to overcrowding, limited healthcare access, and environmental factors (1). Infection caused by the SARS-CoV-2 virus, characterized by high transmissibility and infectivity, has shown a higher risk of infection in prisons than in general population (2, 3) and even up to five times higher in some countries (4, 5). In Spanish prisons, restrictive measures, such as the suspension of visits and inmate confinement, initially succeeded in controlling transmission, yet outbreaks persisted, reflecting the inherent challenges of managing pandemics in prison settings (6). However, despite the effective implementation of preventive measures, penitentiary centers were not exempt from COVID-19 outbreaks. On January 14, 2021, the first confirmed case was recorded at the Alicante II-Villena penitentiary center (CPAII) following a family visit, leading to an outbreak that affected 10% of the prison population before vaccination had begun (7). This underscores the need for specific preventive measures, such as isolating both symptomatic and asymptomatic individuals, contact tracing, and performing PCR tests (7), in addition to achieving high immunization coverage once a vaccine becomes available.
The vaccine shortage required the prioritization of vaccination for the most vulnerable individuals at risk of contracting COVID-19 to minimize its health and economic impacts. The inclusion of prisoners and prison staff as a high-risk group for vaccination was approached heterogeneously worldwide, with significant differences between countries based on their national policies (8, 9). In Spain, the prison population was included in the COVID-19 vaccination recommendations in March 2021 (10), similar to other countries like Poland and Italy, where high vaccination rates with full schedules were achieved (11–13). Specifically, in Spain, 80% of prisoners had received the full vaccination schedule by June 2021 (6).
In general, vaccination coverage in jails and prisons against other communicable and vaccine-preventable diseases, such as HBV, influenza, MMR and pneumococcus, among others, is low (14, 15). Acceptance of vaccines is considered a significant barrier in penitentiary centers, which may contribute to low vaccination coverage (8, 16). This is often due to distrust in potential side effects, skepticism toward the penitentiary administrative system, lack of information, and a lower perception of the risk of contracting COVID-19 (16–21). In this context, the COVID-19 pandemic has marked a significant shift, driving increased vaccination demand within this group, with a greater interest in the COVID-19 vaccine compared to vaccines for other communicable diseases like influenza (22). At our center, a study conducted in mid-2021 to assess the acceptability of the COVID-19 vaccine found high acceptance rates (23).
In the autumn of 2022, early prevention, monitoring and control strategies for COVID-19 in prisons were updated, and the administration of booster doses to the prison population strongly recommended (24, 25). In Spain, the vaccines used for booster doses were the bivalent vaccines BNT162b2 (Comirnaty®-BioNTech-Pfizer) and mRNA-1273 (Spikevax®-Moderna), both designed to target the original strain and the Omicron variant (25). Published results from the American prison population show favorable outcomes, with a reduction in the risk of COVID-19 infection by 22, 23, and 40% for vaccinated individuals, those with previous infection, and vaccinated individuals with prior infection, respectively (26). These findings highlight a favorable immune scenario resulting from the combination of primary immunization, bivalent booster vaccines, and previous infection, leading to 84% immunity against SARS-CoV-2 in the American prison population (27).
Rapid serological tests based on lateral flow immunochromatography (LFIC) are highly useful tools due to their accessibility, simplicity and cost-effectiveness. They have been employed in numerous epidemiological seroprevalence studies aimed at detecting antibodies against SARS-CoV-2 to assess immune status post-vaccination/infection (28–32).
Given the observed high vaccination acceptance in prison populations and subsequent administration of bivalent booster doses, this study aims to evaluate the humoral immunity resulting from the vaccination using LFIC-based serological tests (32), offering insights into the immune status of this vulnerable population after the implementation of booster doses.
A retrospective cross-sectional epidemiological study was carried out based on the prevalence of antibodies against the “S” protein (Spike) of SARS-CoV-2 in prisoners and staff vaccinated against COVID-19 through a rapid serological test during the month of July 2023 due to availability of resources and the timeline of the vaccination programs. The tests were performed and analyzed by the prison healthcare staff.
The study population consisted of prisoners and prison staff from the CPAII. The inclusion criteria were being an inmate or staff at the Alicante II-Villena prison, over 18 years old, and having been vaccinated with at least one dose of the following vaccines: Comirnaty® (Biontech/Pfizer), Spikevax® (Moderna), Vaxzevria® (AstraZeneca) and Jcovden® (Janssen). All participants were informed about the purpose and implication of the study and voluntarily agreed to participate by signing the informed consent form.
Due to a rapidly changing context, we took as baseline the most adverse situation where 50% of the prison population declared having suffered a previous symptomatic COVID-19 infection. Based on this assumption, we designed the study with the goal of estimating the proportion of people with antibodies with 95% confidence and a margin of error of 6%. We assumed a potential type I error rate of 0.05 and of 0.2 for type II error rate. With this configuration, a sample size of 543 was determined.
“OJABIO® SARS-CoV-2 Neutralizing Antibody Detection Kit (Colloidal Gold Method) from Wenzhou OJA Biotechnology Co., Ltd” was used to detect antibodies against the Spike-protein of SARS-CoV-2. This analytical assay, based on lateral flow immunochromatography was validated using the “surrogate Viral Neutralizing Test” (sVNT) based on “enzyme-linked immunofluorescence assay” (sVNT-ELISA) in healthcare population, which also considered a high-risk group at the time of the study (32). In this test, antibodies against the Spike protein of SARS-CoV-2 present in the sample bind to the SARS-CoV-2 Spike protein conjugated to colloidal gold. The resulting conjugated complex then migrates through the reaction matrix via laminar flow. Once in the reaction matrix, it is captured by anti-Immunoglobulin antibodies (IgG or IgM) fixed to the nitrocellulose membrane. The binding of the antigen–antibody complex is indicated by the formation of a test line (T), signifying the presence of neutralizing antibodies against SARS-CoV-2. An adjacent control line (C) indicates proper technical performance of the test. The presence of both lines is interpreted as a valid positive result. The test readings were performed by two expert researchers following the manufacturer’s instructions.
The following demographic variables were collected: age, sex, and occupation (prisoner or prison staff). Likewise, epidemiological and clinical variables gathered were: previous infection by SARS-CoV-2, presence of chronic diseases (Chronic Obstructive Pulmonary Disease [COPD], autoimmune diseases, diabetes, high blood pressure), number of doses and type of vaccine received, as well as the year when the person was last vaccinated. For the statistical analysis, the information about chronic diseases was recodified as a binary variable: presence or absence of comorbidity.
The data was described using the mean and standard deviation for the continuous variables such as age, vaccine doses received, and years since the last dose. Categorical variables were described using the frequency and proportion of the sample. For both types of variables, 95% Confidence Intervals (CI) were calculated. Furthermore, these were calculated according to the result of the test. Details are broken down for both prison staff and prisoners.
The statistical analysis was performed by calculating Odds Ratios (OR). The OR were calculated by direct calculation for the categorical variables, whereas for the continuous variables logistic regression was used. Furthermore, adjusted Odd Ratios (aOR) were calculated for a specific model including every variable using logistic regression. This model was trained using a stepwise model using Wald’s criterion with a 0.05 significance of entry and 0.10 significance of exit. The data was analyzed using SPSS version 29.0. Results were considered significant when p < 0.05.
The study was carried out following the bases of the Declaration of Helsinki, and approved by two independent Ethics Committees: the Ethics Committee of the University of Alicante (Spain) (File UA-2021-05-07_5, dated 05/24/2021), and the Ethics Committee of the Health Department of the Dr. Balmis Hospital in Alicante (File PI2021-094, Ref: 2021-0214, dated 06/30/2021). The study was approved by the General Secretariat of Penitentiary Institutions, General Subdirectorate of Institutional Relations and Territorial Coordination (exp. number 74258). The participants were informed about the confidentiality measures and their right to withdraw from the study. The information was treated confidentially, and in accordance with Spanish Organic Law 3/2018, of December 5, on the Protection of Personal Data.
At the time that the study, the penitentiary center had a total of 896 prisoners and 178 staff members who had received at least one dose of a SARS-CoV-2 vaccine. The entire eligible population was offered the opportunity to participate, voluntarily and anonymously. A total of 560 individuals agreed to participate (400 prisoners and 160 prison staff) resulting in a 52% response rate (560/1,074 total prison population). Among prisoners, the response rate was of 44.6%, while among prison staff, it was 89.9%.
Descriptive statistics of the sample are shown in Table 1. The majority of participants in the study were prisoners (N = 400; 71.4%), with the remaining participants being prison staff. Notably, over three-quarters of the participants were male (77.3%). Among prisoners, 89.0% were male whereas in the prison staff, males represented about half of the group. Participants ranged in age from 21 to 65 years old, with an average age of 45.7 years. Both prisoners and prison staff had a similar age distribution, except that there were no prison staff over 60 years of age.
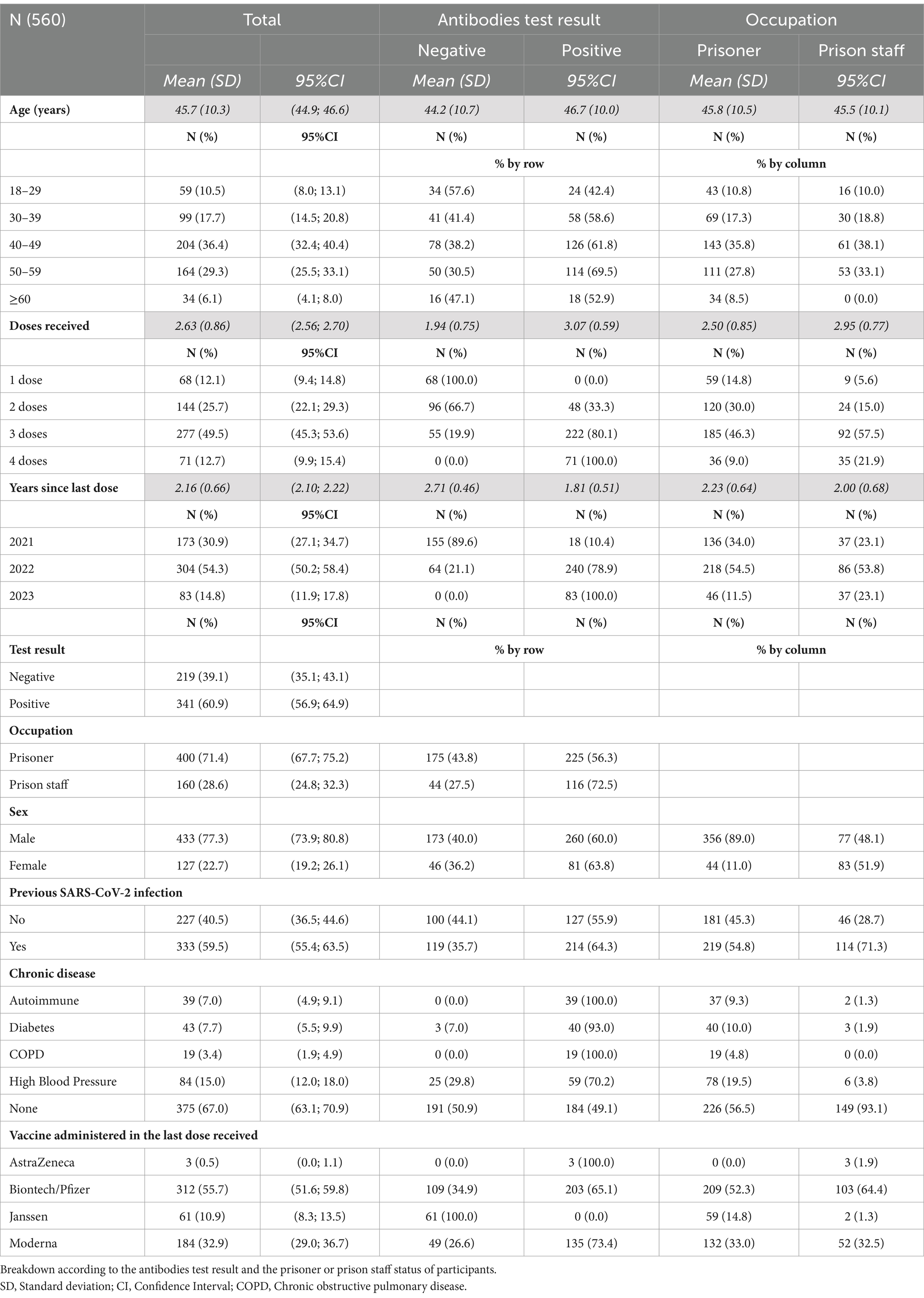
Table 1. Description of demographic, clinical and vaccination variables of the study participants (N = 560).
Out of the 560 tests performed, 341 (60.9%) yielded a positive result, showing the presence of antibodies against the Spike-protein of SARS-CoV-2. The positivity was higher among prison staff (72.5%) than among prisoners (56.3%). There were no significant differences in positivity anti-SARS-CoV-2 antibodies according to gender, with 60.0% positivity in men and 63.8% in women (p = 0.448). The average age of those who tested positive was slightly higher than among those who tested negative (2.5 years older, p = 0.004).
Every participant in the study was vaccinated with at least one vaccine dose. Approximately one half of the subjects declared having received 3 vaccine doses, while a quarter of the sample had received 2 doses, and the remaining subjects were split similarly between 1 and 4 vaccine doses. Those who tested positive had received more vaccine doses, with 3.07 ± 0.59 vaccine doses on average, than those who obtained a negative test result, who had received 1.94 ± 0.75 doses. Prison staff had received more vaccine doses (2.95 ± 0.77) than prisoners, who had received 2.50 ± 0.85 doses.
While 173 (30.9%) participants had not been vaccinated since 2021, slightly over half participants were vaccinated for the last time in 2022, and the remaining 15% had been vaccinated in 2023. The time elapsed since the last vaccination dose was higher among those who tested negative (2.71 ± 0.46 years) than those with a positive antibody test result (1.81 ± 0.51 years), and higher among prisoners (2.23 ± 0.64 years) than within prison staff (2.00 ± 0.68 years).
Six out of 10 participants declared having suffered a previous SARS-CoV-2 infection. Those who had suffered a previous infection showed a significantly higher positivity (64.3%) than those who had not (55.9%) with a p-value for the chi-squared test with 1 degree of freedom of p = 0.048 which indicates that this difference can be considered as statistically significant at a significance level of α = 0.05. Additionally, the incidence of SARS-CoV-2 infection was higher among prison staff (71.3%) than prisoners (54.8%). Around two thirds of the subjects who had suffered a prior infection had antibodies. This was similar in prisoners (63.5%) and prison staff (65.8%), but the positivity was different among those who had not had a previous infection. While 89.1% of the prison staff without a previous infection presented a positive test result, slightly below half of the prisoners who had not suffered a previous SARS-CoV-2 infection showed presence of antibodies (47.5%).
Finally, around two out of every three subjects declared having no chronic diseases. Among those who had some comorbidity, 174 were prisoners and 11 were prison staff, indicating a presence of comorbidity in 43.5% of prisoners and only in 6.9% of prison staff. The chronic diseases present were distributed with 15% of subjects reporting high blood pressure, around 7% declaring having an autoimmune disease or diabetes, while the remaining 3.4% suffered from chronic obstructive pulmonary disease. Regarding positivity and comorbidities, prisoners with comorbidity had a positivity of 89.1% compared to prisoners without comorbidities where 31.0% presented antibodies. Furthermore, prisoners with comorbidity have received more vaccine doses (2.99 vs. 2.12 doses); more recently (1.86 years vs. 2.51 years) and are older (49.0 vs. 43.4 years) than prisoners without comorbidities. We would like to highlight how the results obtained for the prison staff differ significantly as we can see next. Those participants without comorbidities obtained a higher positivity (76.5% vs. 18.2%), with no significant differences observed between age or the number of doses received. On the contrary, the variable time since the last dose is influential, since prison staff without comorbidities have received vaccines more recently (1.94 vs. 2.82 years). Regarding the comparison between participants with comorbidities, according to whether they are prisoners or staff, we observe that prisoners with comorbidities have received more vaccine doses (2.99 vs. 2.54 doses), more recently (1.86 vs. 2.82 years ago) and show a higher positivity of 89.1%, which contrasts with the 18.2% among staff with comorbidities. However, there were only 11 members of the prison staff with comorbidities in the sample, which requires non-parametric tests for comparison. The p-values for the Mann–Whitney U test for the quantitative variables and of Fisher’s exact test for positivity were significant in all comparisons indicated (p < 0.001).
Regarding the vaccines administrated in the last administered dose, 88.6% of the subjects received the Biontech/Pfizer and Moderna vaccines. The positivity rate for these subjects was greater than 65%. Those subjects (59 prisoners and 2 prison staff) who received the last dose of the Janssen vaccine in 2021, present a 100% antibody negativity rate. In contrast, 3 out of 3 of the subjects (prison staff) who received the last dose of the AstraZeneca vaccine presented a positive serological result in antibodies although the small sample size of three subjects makes unadvisable drawing strong conclusions.
To assess the statistical significance of these differences in seroprevalence, we calculated the OR for each variable, which can be found in Table 2. When analyzed separately, we observe that all variables considered except for the gender of a participant show significant differences in risk. In particular, the proportion of positive test results was higher in older people, and among those with comorbidities. The positivity was also higher in those who had received more vaccine doses, in those vaccinated more recently, and among those who had previously suffered a SARS-CoV-2 infection.
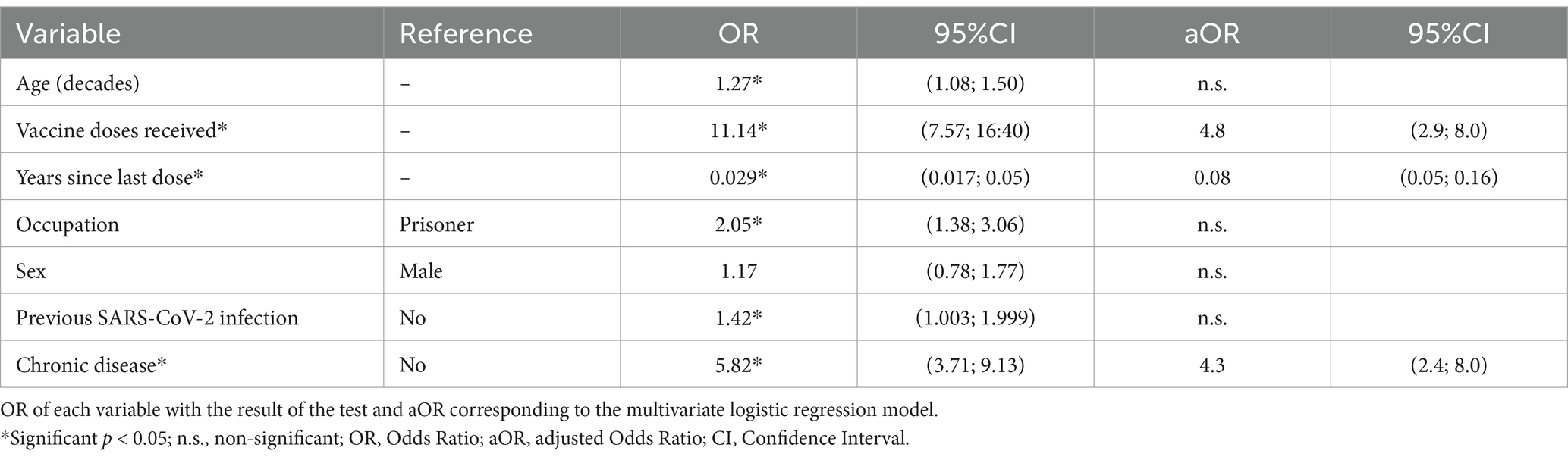
Table 2. Positivity in the antibody test according to demographic, clinical and vaccination variables.
Additionally, a multivariate analysis was performed using logistic regression to adjust for confounding variables. The result of the test was used as target variable and all the remaining variables were used as co-variables, with comorbidity in their binary recodification. The variables age (in decades), vaccine doses received and years since the last dose were included as continuous variables. This model was used to calculate the adjusted aOR. The variables that yielded a significantly higher proportion of positive test results were: having received more doses, i.e., each additional dose increases the odds of a positive test by aOR: 4.8; 95%CI: (2.9; 8.0); lower time since the last vaccine dose, i.e., each year longer since the last vaccination reducing the odds of presenting antibodies by aOR: 0.08; 95%CI: (0.05; 0.16); and suffering a comorbidity (aOR: 4.3; 95%CI: 2.4; 8.0). The remaining variables did not appear as statistically significant in this model.
Regarding potential collinearity between variables, an analysis of the predictive variables yielded variance inflation factors (VIF) with values smaller than 1.6 for all variables except for the number of doses (VIF = 2.86) and the years since the last dose (VIF = 2.57), which are within acceptable levels. Therefore, there is little indication of multicollinearity causing problems in this model.
Available seroepidemiological data on SARS-CoV-2 in prison settings are limited. Reported immunization coverage against SARS-CoV-2 in prisons varies significantly between countries and is influenced by the timing of the pandemic and vaccination policies (33–36). This study is the first seroprevalence study conducted in a penitentiary institution in Spain following the onset of the COVID-19 pandemic and the implementation of booster doses.
The most efficient vaccination strategy reported in prisons against SARS-CoV-2 is the immunization of inmates and staff over 50 years of age, which leads to a significant reduction in COVID-19 incidence by more than 50%, as well as a 41.1% reduction in cases and a 35.9% reduction in deaths (37). In this study, the participants were predominantly young men, with the average age being below 50 years for both prisoners and prison staff. Overall, 60.9% of the participants had antibodies against the Spike protein of SARS-CoV-2, as detected by a rapid serological test, following the implementation of booster doses. There was a trend toward greater positivity with increasing age, regardless of gender.
The presence of anti-SARS-CoV-2 antibodies is influenced by several factors, including previous infection, the time elapsed since the last exposure to the virus (whether through infection or vaccination), and the number of vaccine doses received (28–31, 38). In the sample, the results confirm that having had the disease predisposes individuals to the presence of antibodies, regardless of occupation. Paradoxically, there were significant differences between prisoners and prison staff who had not been infected, with the latter group showing higher positivity for anti-SARS-CoV-2 antibodies. Additionally, the administration of booster doses was associated with much higher positivity for Spike-protein anti-SARS-CoV-2 antibodies. Specifically, it is noteworthy that prison staff received more booster doses and had a better response to seropositivity, with 72.5% positivity compared to 56.3% among prisoners. Given that prison staff received more vaccine doses, this suggests that the presence of antibodies in those who have not been infected with COVID-19 depends on the number of vaccine doses received, indicating that the immunization achieved is a result of the booster vaccination.
Additionally, a significant difference in the presence of antibodies was observed based on the time elapsed since the last dose was administered. The positivity rate for participants vaccinated within the last year (2023) was 100%, in contrast to those vaccinated two or more years ago, who had a lower positivity rate. However, booster doses were first administered in 2022, and the positivity rate for those vaccinated in that year reached almost 80% (Figure 1). This suggests that the immunization coverage achieved after booster doses is maintained even 2 years after the last dose. In other words, the number of years since the last dose may act as a protective factor.
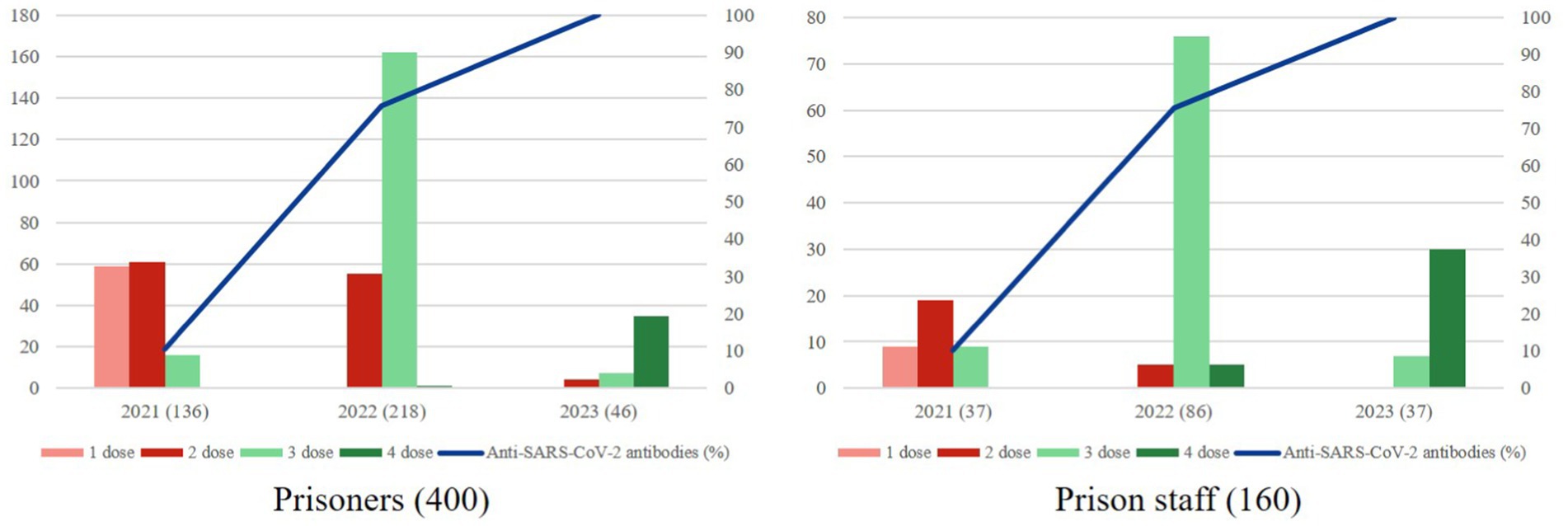
Figure 1. Relation among the distribution of sample according to the year of the last dose vaccine administered and percentage of anti-SARS-CoV-2 antibodies on prisoners and prison staff. Both graphs show each occupational group stratified by the last year in which they were administered a vaccine dose. The left axis shows the number of patients (n) who had received 1, 2, 3, or 4 doses in the last vaccine administration. The right axis shows the percentage of subjects with anti-SARS-CoV-2 antibodies according to the year of the last dose vaccine.
Most participants were vaccinated in 2022, but differences were observed between prisoners and prison staff in the last year, with a lower vaccination rate among the former (Figure 1). According to data published by Vicente-Alcalde et al., vaccine acceptance during the initial immunization period was 90% among prisoners (23), suggesting that a higher vaccination rate could be expected. However, in this study, the response rate among prisoners (44,6%) was low, which could be considered a limitation. Furthermore, the high turnover in this group makes it challenging to monitor vaccination programs, as it is difficult to track vaccinations continuously, ensure that everyone receives the necessary doses, and maintain accurate records, as prisoners and staff enter and leave the system. Likewise, the decrease in the incidence and severity of COVID-19, combined with the voluntary nature of vaccination after primary immunization, may have contributed to a lower perception of risk among prisoners, which is reflected in the lower vaccination rates.
Regarding comorbidities, 94% of the subjects affected by them were prisoners who had received the vaccine, despite their status as a vulnerable group due to social, hygienic, confinement, or institutional health dependency factors. We observed that 86.5% of subjects with comorbidities had received a vaccine dose in 2022 or later, compared to only 60.5% of those without comorbidities. This suggests a high level of awareness and vaccine acceptance among prisoners with chronic diseases, as well as effective management of vaccination programs for prisoners with comorbidities by prison healthcare staff.
The two main vaccines administered at CPAII are mRNA-based, and both have achieved a positivity rate for anti-SARS-CoV-2 antibodies greater than 65%. These vaccines are designed to induce a specific immune response against the SARS-CoV-2 Spike protein, resulting in the formation of neutralizing antibodies (39). However, not all anti-SARS-CoV-2 Spike antibodies exhibit neutralizing activity, nor do they have the same efficacy against all variants (30–42). Based on published data, it appears that additional vaccine doses enhance neutralization (41). Stufano et al. observed that the neutralizing capacity of antibodies generated after the initial vaccination schedule was limited against the Omicron variant, but this capacity increased when booster doses of the BNT162b2 mRNA vaccine were administered (38). These findings support the need to continue vaccination programs with booster doses of mRNA vaccines in prison settings to ensure maximum protection and safety against potential critical variants of SARS-CoV-2.
Among the limitations of the study, the overall response rate of 52% should be highlighted. However, when considering participation by occupational group, we observed a higher response rate among prison staff (89.9%) compared to prisoners (44.6%). Additionally, while neutralizing antibodies are those that confer immunity, the serological test used in this study does not specifically evaluate the neutralizing capacity of Spike-protein antibodies. Nevertheless, it has been previously validated for detecting neutralizing antibodies against SARS-CoV-2 (32). Moreover, comparative studies between serological techniques and neutralization assays have shown a high correlation in their results (32, 43). These findings support the use of rapid serological tests as a useful tool for assessing the humoral immunity generated against SARS-CoV-2 in high-risk environments, such as the prison population. Additionally, while sex and age were considered as variables, there could be other potential confounders such as socio-demographic differences between prisoners and staff. Other socio-demographic variables, such as the prisoners’ employment prior to incarceration, place of birth, education level, marital status, etc., were not collected and, therefore, were not included in the analysis.
In conclusion, the findings indicate relatively low vaccination coverage against COVID-19 among prisoners compared to prison staff, underscoring the need to continue booster vaccination programs to achieve sustained immunity against SARS-CoV-2, as supported by other studies (38–42). Rapid serological tests can serve as a valuable tool for guiding preventive policies against communicable diseases such as COVID-19 in prison settings.
The raw data supporting the conclusions of this article will be made available by the authors without undue reservation.
The studies involving humans were approved by Ethics Committee of the University of Alicante (Spain) (File UA-2021-05-07_5, dated 05/24/2021), and the Ethics Committee of the Health Department of the Dr. Balmis Hospital in Alicante (File PI2021-094, Ref: 2021-0214, dated 06/30/2021). The study was approved by the General Secretariat of Penitentiary Institutions, General Subdirectorate of Institutional Relations and Territorial Coordination (exp. number 74258). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
ACM: Conceptualization, Formal analysis, Investigation, Writing – original draft, Writing – review & editing. RM: Data curation, Formal analysis, Validation, Writing – original draft, Writing – review & editing. NV-A: Conceptualization, Data curation, Funding acquisition, Resources, Writing – original draft. EM: Investigation, Resources, Writing – original draft. JH-S: Investigation, Resources, Writing – original draft. JT: Conceptualization, Funding acquisition, Supervision, Writing – original draft, Writing – review & editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This work was supported by an advisory contract from the University of Alicante with reference WENZHOU-OJABIO1-21T and no one reports personal fees received from the biotech company.
We want to thank the voluntary participation of both prisoners and prison staff of the Alicante II-Villena penitentiary center (CPAII).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Simpson, PL, Simpson, M, Adily, A, Grant, L, and Butler, T. Prison cell spatial density and infectious and communicable diseases: a systematic review. BMJ Open. (2019) 9:e026806. doi: 10.1136/bmjopen-2018-026806
2. Nowotny, KM, Seide, K, and Brinkley-Rubinstein, L. Risk of COVID-19 infection among prison staff in the United States. BMC Public Health. (2021) 21:1036. doi: 10.1186/s12889-021-11077-0
3. Macmadu, A, and Brinkley-Rubinstein, L. Essential strategies to curb COVID-19 transmission in prisons and jails. Am J Public Health. (2021) 111:776–7. doi: 10.2105/AJPH.2021.306206
4. Saloner, B, Parish, K, Ward, JA, DiLaura, G, and Dolovich, S. COVID-19 cases and deaths in federal and state prisons. JAMA. (2020) 324:602–3. doi: 10.1001/jama.2020.12528
5. Blair, A, Parnia, A, and Siddiqi, A. A time-series analysis of testing and COVID-19 outbreaks in Canadian federal prisons to inform. Can Commun Dis Rep. (2021) 47:66–76. doi: 10.14745/ccdr.v47i01a10
6. Hernando, V, Vázquez, I, Díaz, A, Gómez-Pintado, P, Martínez-Aznar, C, and Acín, E. COVID-19 pandemic in prisons in Spain: characteristics of cases and implemented control measures, March 2020–June 2022. Public Health. (2023) 218:45–52. doi: 10.1016/j.puhe.2023.02.013
7. Vicente-Alcalde, N, Ruescas-Escolano, E, Franco-Paredes, C, and Tuells, J. Control of a COVID-19 outbreak in a Spanish prison: lessons learned in outbreak control. Front Med (Lausanne). (2022) 9:806438. doi: 10.3389/fmed.2022.806438
8. Ismail, N, Tavoschi, L, Moazen, B, Roselló, A, and Plugge, E. COVID-19 vaccine for people who live and work in prisons worldwide: a scoping review. PLoS One. (2022) 17:e0267070. doi: 10.1371/journal.pone.0267070
9. EU Agency for Fundamental Rights. Coronavirus pandemic in the EU–fundamental rights implications: vaccine rollout and equality of access in the EU 2021. (2021). Available at: https://fra.europa.eu/sites/default/files/fra_uploads/fra-2021-coronavirus-pandemic-eu-bulletin-vaccines_en.pdf (Accessed April 22, 2024).
10. Ministerio de Sanidad, Consumo y Bienestar Social (España). Comisión de Salud Pública tras revisión y propuesta realizada por la Ponencia de Programa y Registro de Vacunaciones junto con el Grupo de Trabajo Técnico de Vacunación COVID-19 y el Grupo de Trabajo de Vacunación COVID-19 en la Población Infantil. Actualización 5 - Estrategia de vacunación frente a COVID-19 en España 2021. (2021). Available at: https://www.sanidad.gob.es/areas/promocionPrevencion/vacunaciones/covid19/Actualizaciones_Estrategia_Vacunacion/docs/COVID-19_Actualizacion5_EstrategiaVacunacion.pdf (Accessed May 15, 2024).
11. Augustynowicz, A, Bachurska, B, Wójcik, M, Borowska, M, Czerw, A, Opolski, J, et al. COVID-19-infections and immunization of inmates in penitentiary institutions in Poland in 2021. Int J Environ Res Public Health. (2022) 19:13725. doi: 10.3390/ijerph192113725
12. World Health Organization. WHO/Europe shows high rates of COVID-19 vaccination in prisons. (2021). Available at: https://www.who.int/europe/news/item/15-07-2021-who-europe-shows-high-rates-of-covid-19-vaccination-in-prisons (Accessed May 15, 2024).
13. Vella, R, Giuga, G, Piizzi, G, Alunni Fegatelli, D, Petroni, G, Tavone, AM, et al. Health Management in Italian Prisons during COVID-19 outbreak: a focus on the second and third wave. Healthcare (Basel). (2022) 10:282. doi: 10.3390/healthcare10020282
14. Vicente-Alcalde, N, Ruescas-Escolano, E, Harboe, ZB, and Tuells, J. Vaccination coverage among prisoners: a systematic review. Int J Environ Res Public Health. (2020) 17:7589. doi: 10.3390/ijerph17207589
15. Vicente-Alcalde, N, Tuells, J, Egoavil, CM, Ruescas-Escolano, E, Altavilla, C, and Caballero, P. Immunization coverage of inmates in Spanish prisons. Int J Environ Res Public Health. (2020) 17:8045. doi: 10.3390/ijerph17218045
16. Kerrison, EMT, and Hyatt, JM. COVID-19 vaccine refusal and medical distrust held by correctional officers. Vaccines (Basel). (2023) 11:1237. doi: 10.3390/vaccines11071237
17. Lessard, D, Ortiz-Paredes, D, Park, H, Varsaneux, O, Worthington, J, Basta, NE, et al. Barriers and facilitators to COVID-19 vaccine acceptability among people incarcerated in Canadian federal prisons: a qualitative study. Vaccine X. (2022) 10:100150. doi: 10.1016/j.jvacx.2022.100150
18. Ortiz-Paredes, D, Varsaneux, O, Worthington, J, Park, H, MacDonald, SE, Basta, NE, et al. Reasons for COVID-19 vaccine refusal among people incarcerated in Canadian federal prisons. PLoS One. (2022) 17:e0264145. doi: 10.1371/journal.pone.0264145
19. Chin, ET, Leidner, D, Ryckman, T, Liu, YE, Prince, L, Alarid-Escudero, F, et al. COVID-19 vaccine acceptance in California state prisons. N Engl J Med. (2021) 385:374–6. doi: 10.1056/NEJMc2105282
20. Shabir, A, Alkubaisi, NA, Shafiq, A, Salman, M, Baraka, MA, Mustafa, ZU, et al. COVID-19 vaccination status as well as factors associated with COVID-19 vaccine acceptance and hesitancy among prisoners and the implications. Vaccines (Basel). (2023) 11:1081. doi: 10.3390/vaccines11061081
21. Osman, I, Williams, A, Pierson, K, Ryu, E, and Shlafer, RJ. Facilitators and barriers to COVID-19 vaccination among incarcerated people and staff in three large, state prisons: a cross-sectional study. Health Justice. (2023) 11:38. doi: 10.1186/s40352-023-00240-x
22. Cassarino, N, Ahnger-Pier, KK, and Wurcel, A. Trends in COVID-19 and influenza vaccine ordering and distribution in Massachusetts jails. Vaccine. (2023) 41:6607–11. doi: 10.1016/j.vaccine.2023.09.045
23. Vicente-Alcalde, N, Sferle, SM, Franco-Paredes, C, and Tuells, J. Acceptance of the COVID-19 vaccine by prisoners and staff in Spanish prisons. Vaccines (Basel). (2023) 11:1547. doi: 10.3390/vaccines11101547
24. Ministerio del Interior Secretaría de Instituciones Penitenciarias. Adecuación de las Medidas de la Estrategia de Detección Temprana, Vigilancia y Control del COVID-19 tras la Fase Aguda de la Pandemia para los Centros Penitenciarios Dependientes de la Secretaría General de Instituciones Penitenciarias. (2021). Available at: https://www.sanidad.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov/documentos/COVID-19_Adaptacion_Estrategia_Vigilancia_Centros_Penitenciarios.pdf (Accessed June 7, 2024).
25. Ministerio de Sanidad (España). Consejo Interterritorial Sistema Nacional de Salud. Recomendaciones de vacunación frente a COVID-19 para el otoño en España. (2021). Available at: https://www.sanidad.gob.es/areas/promocionPrevencion/vacunaciones/covid19/Historico_COVID-19/docs/Recomendaciones_vacunacion_Otono_Covid_VF.pdf (Accessed June 7, 2024).
26. Tan, ST, Kwan, AT, Rodríguez-Barraquer, I, Singer, BJ, Park, HJ, Lewnard, JA, et al. Infectiousness of SARS-CoV-2 breakthrough infections and reinfections during the omicron wave. Nat Med. (2023) 29:358–65. doi: 10.1038/s41591-022-02138-x
27. Ko, L, Malet, G, Chang, LL, Nguyen, H, and Mayes, R. COVID-19 infection rates in vaccinated and unvaccinated inmates: a retrospective cohort study. Cureus. (2023) 15:e44684. doi: 10.7759/cureus.44684
28. Montagud, AC, Vicente-Alcalde, N, Gabaldón-Bravo, EM, Hurtado-Sánchez, JA, Montagud, E, Egoavil, CM, et al. Vacunación contra la COVID-19 en la Universidad de Alicante (España): detección de anticuerpos neutralizantes frente al sars-CoV-2 mediante test serológico rápido, un estudio transversal [COVID-19 vaccination at the University of Alicante (Spain): detection of neutralizing antibodies against SARS-CoV-2 by rapid serological test, a cross-sectional study]. Rev Esp Salud Publica. (2023) 97:e202312111
29. Montagud, AC, Llenas-García, J, Moragues, R, Perez-Bernabeu, A, Alcocer-Pertegaz, MJ, García-Gómez, FJ, et al. Prevalencia de anticuerpos neutralizantes frente al SARS-CoV-2 inducidos tras 2 dosis de vacuna BNT162b2 (Pfizer–BioNTech) en trabajadores sanitarios [Prevalence of generated neutralizing antibodies against SARS-CoV-2 after two doses of BNT162b2 (Pfizer–BioNTech) vaccine in health staffs]. Rev Clin Esp. (2024) 224:197–203. doi: 10.1016/j.rce.2024.01.009
30. Tapari, A, Braliou, GG, Papaefthimiou, M, Mavriki, H, Kontou, PI, Nikolopoulos, GK, et al. Performance of antigen detection tests for SARS-CoV-2: a systematic review and Meta-analysis. Diagnostics (Basel). (2022) 12:1388. doi: 10.3390/diagnostics12061388
31. Tuells, J, Egoavil, CM, Pena Pardo, MA, Montagud, AC, Montagud, E, Caballero, P, et al. Seroprevalence study and cross-sectional survey on COVID-19 for a plan to reopen the University of Alicante (Spain). Int J Environ Res Public Health. (2021) 18:1908. doi: 10.3390/ijerph18041908
32. Tuells, J, Parra-Grande, M, Santos-Calle, FJ, Montagud, AC, Egoavil, CM, García-Rivera, C, et al. Detection of neutralizing antibodies against SARS-CoV-2 post-vaccination in health care staffs of a large tertiary hospital in Spain by using a rapid test LFIC and sVNT-ELISA. Vaccines (Basel). (2022) 10:510. doi: 10.3390/vaccines10040510
33. Andrade, SGA, Andrade, FM, Silva, AD, Cardoso, MRA, Ferraz, GR, Barros, ENC, et al. Overview of SARS-COV-2 infection at the Butantan penitentiary progression center. Rev Saude Publica. (2023) 57:10s. doi: 10.11606/s1518-8787.2023057004717
34. Gétaz, L, Wolff, H, Gonçalves, L, Togni, G, Stringhini, S, Chacowry Pala, K, et al. SARS-CoV-2 seroprevalence study after the first wave among persons living and working in an overcrowded Swiss prison. Int J Prison Health. (2022) 19:392–9. doi: 10.1108/IJPH-01-2022-0002
35. Kronfli, N, Dussault, C, Maheu-Giroux, M, Halavrezos, A, Chalifoux, S, Sherman, J, et al. Seroprevalence and risk factors for severe acute respiratory syndrome coronavirus 2 among incarcerated adult men in Quebec, Canada, 2021. Clin Infect Dis. (2022) 75:e165–73. doi: 10.1093/cid/ciac031
36. Moazen, B, Ismail, N, Agbaria, N, Mazzilli, S, Petri, D, Amaya, A, et al. Vaccination against emerging and reemerging infectious diseases in places of detention: a global multistage scoping review. Front Public Health. (2024) 12:1323195. doi: 10.3389/fpubh.2024.1323195
37. CV, MC, O'Mara, O, van Leeuwen, E, CMMID COVID-19 Working GroupJit, M, and Sandmann, F. The impact of COVID-19 vaccination in prisons in England and Wales: a metapopulation model. BMC Public Health. (2022) 22:1003. doi: 10.1186/s12889-022-13219-4
38. Stufano, A, Buonvino, N, Trombetta, CM, Pontrelli, D, Marchi, S, Lobefaro, G, et al. COVID-19 outbreak and BNT162b2 mRNA vaccination coverage in a correctional facility during circulation of the SARS-CoV-2 omicron BA1 variant in Italy. Vaccines (Basel). (2022) 10:1137. doi: 10.3390/vaccines10071137
39. Golob, JL, Lugogo, N, Lauring, AS, and Lok, AS. SARS-CoV-2 vaccines: a triumph of science and collaboration. JCI Insight. (2021) 6:e149187. doi: 10.1172/jci.insight.149187
40. Sharun, K, Tiwari, R, Dhama, K, Emran, TB, Rabaan, AA, and Al Mutair, A. Emerging SARS-CoV-2 variants: impact on vaccine efficacy and neutralizing antibodies. Hum Vaccin Immunother. (2021) 17:3491–4. doi: 10.1080/21645515.2021.1923350
41. Rescigno, M, Agrati, C, Salvarani, C, Giannarelli, D, Costantini, M, Mantovani, A, et al. Neutralizing antibodies to omicron after the fourth SARS-CoV-2 mRNA vaccine dose in immunocompromised patients highlight the need of additional boosters. Front Immunol. (2023) 14:1104124. doi: 10.3389/fimmu.2023.1104124
42. Trombetta, CM, Marchi, S, Leonardi, M, Stufano, A, Lorusso, E, Montomoli, E, et al. Evaluation of antibody response to SARS-CoV-2 variants after 2 doses of mRNA COVID-19 vaccine in a correctional facility. Hum Vaccin Immunother. (2022) 18:2153537. doi: 10.1080/21645515.2022.2153537
Keywords: anti-SARS-CoV-2 antibodies, COVID-19, SARS-CoV-2, rapid serological test, lateral flow immunochromatography, prisons
Citation: Montagud AC, Moragues R, Vicente-Alcalde N, Montagud E, Hurtado-Sánchez JA and Tuells J (2025) Seroprevalence against SARS-CoV-2 after booster vaccination in a prison in Alicante (Spain). Front. Public Health. 13:1490809. doi: 10.3389/fpubh.2025.1490809
Edited by:
Farid Rahimi, Australian National University, AustraliaReviewed by:
Salvatore Zaffina, Bambino Gesù Children’s Hospital (IRCCS), ItalyCopyright © 2025 Montagud, Moragues, Vicente-Alcalde, Montagud, Hurtado-Sánchez and Tuells. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ana C. Montagud, YW5hLmNlcmRhQHF1aXJvbnNhbHVkLmVz; Raul Moragues, cmF1bC5tb3JhZ3Vlc0B1YS5lcw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.