
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 02 April 2025
Sec. Life-Course Epidemiology and Social Inequalities in Health
Volume 13 - 2025 | https://doi.org/10.3389/fpubh.2025.1488108
 Katie Bates1,2
Katie Bates1,2 Wegene Borena3*
Wegene Borena3* Martin McKee4
Martin McKee4 Lore Hayek5
Lore Hayek5 Paul Bouanchaud6
Paul Bouanchaud6 Zoltán Bánki3Lydia Riepler3
Zoltán Bánki3Lydia Riepler3 Annika Rössler3,7
Annika Rössler3,7 Barbara Falkensammer3Jörg Paetzold8Andreas Walser9Sebastian Schönherr10Lukas Forer10
Barbara Falkensammer3Jörg Paetzold8Andreas Walser9Sebastian Schönherr10Lukas Forer10 Ludwig Knabl3,11
Ludwig Knabl3,11 Janine Kimpel3
Janine Kimpel3 Dorothee von Laer3
Dorothee von Laer3 Hanno Ulmer1*
Hanno Ulmer1*Introduction: In early March 2020, a SARS-CoV-2 outbreak occurred in the ski resort of Ischgl, in Austria. After an initial seroprevalence study in April 2020, a follow-up study in November 2020 showed persistence of high levels of seropositivity. The impacts of SARS-CoV-2 infections and non-pharmaceutical interventions required to reduce transmission were wide-ranging, including worsened mental and physical health and economic damage.
Methods: We analysed data from the Ischgl follow-up study. Of the 1,259 adults that participated in the Ischgl-1 study (Ischgl-1), 801 were followed-up. Seropositivity was defined using presence of binding and neutralizing antibodies at Ischgl-1. At follow-up, 7 months later (Ischgl-2), participants reported changes to self-rated mental and physical health, physical activity, alcohol consumption, smoking and economic status. Changes were compared by serological status, using multivariable logistic and multinomial regression models, where appropriate, and adjusting for factors including age, sex, and morbidity.
Results: 1 in 2 participants reported experiencing a moderate or severe impact of the pandemic. One fifth of participants reported a worsening in their mental health from November 2019 to November 2020; women and participants aged ≥35 to <70 years were disproportionately affected. Seropositivity was associated with a decline in physical health but no decline in mental health or behaviour changes. Very few participants reported any changes in behaviours. The overriding impact the population of Ischgl was economic—50% of participants reported a worsening of their professional and/or financial situation. Declines in self-reported mental health were associated with the overall experience of the pandemic and economic factors.
Conclusion: The population of Ischgl demonstrated a high level of resilience to the pandemic as measured by health. However, certain segments of the population were disproportionately affected, particularly with regard to mental health and economic wellbeing. Future pandemic preparedness must consider how pandemic mitigation strategies can be responsive to context and the wider impacts on mental health and social and economic wellbeing while minimising mortality and safeguarding health systems.
The COVID-19 pandemic had direct and indirect effects on health. Those infected faced increased risk of severe illness (including Long COVID) and death and the resulting pressure on health facilities reduced access for those with other conditions. The non-pharmacological interventions (NPIs) necessary to interrupt transmission of the virus (1), including unprecedented restrictions on daily life, had wider consequences for the health, social and economic situation of individuals and populations (2, 3). These NPIs included travel restrictions, stay-at-home orders, school closures, social distancing, quarantine, and personal protective measures such as face masks and health system strengthening (4).
There are now many studies documenting these direct and indirect health impacts and their uneven distribution within populations. The German National Cohort (NAKO) study measured changes in self-rated health (SRH) among n = 113,928 participants from baseline (between 1 and 5 years prior to 2020) until late April to May 2020, collected in the COVID-NAKO survey. SRH improved for 32% of people but worsened for 12%. Those who were tested for the SARS-CoV-2 virus were more likely to report worsening self-rated health than those who did not, regardless of whether the result was positive or negative, suggesting that the impact of the pandemic on self-rated health may have been indirect (5). In an online survey in Austria, undertaken very early in the pandemic (March to April 2020), 43.3% of respondents rated the psychological impact of the pandemic as moderate or severe (6); women, older adults, and those with poor self-rated health reported higher psychological burdens related to the pandemic.
The term COVID-19 syndemic has been coined to describe the association of direct and indirect health impacts with pre-existing health and socioeconomic inequalities (7). For example, unemployed people in Sweden experienced worse economic (2), while in a multicounty study including the UK, Italy and Slovenia, economic impacts were more pronounced among younger (18–24) and older adults (65+), as well as those with lower levels of education and casual employment status (8). Data from the few countries to measure ethnicity also found marked inequalities (9).
The existing research on mental health impacts of the COVID-19 pandemic are complex and context-dependent, influenced by factors such as levels of support and local incidence rates of SARS-CoV-2. The NAKO Study revealed worse mental health outcomes among those tested for the virus, regardless of test results, with less pronounced effects in low-incidence areas and greater impacts in higher-incidence regions (5). A consistent finding in studies, including the SHARE COVID-19 study, is the presence of increased stress across all age groups, with women experiencing greater mental health declines than men (10). However, anxiety and depression were particularly prevalent among people under 60, especially those aged 20–39, aligning with similar trends observed in the UK and the US (5, 11, 12).
Initially, most studies examining the pandemic’s impact on individuals focussed on direct health effects and relied on data from groups for which there were good data, such as health care workers (13), or patients hospitalised with COVID-19 (14). Later studies, in particular those looking at indirect effects, have used data from app or web-based surveys, all subject to potential bias from participants’ self-selection and/or lacking laboratory confirmation of SARS-CoV-2 infection (15). Some longitudinal household surveys have been exploited to assess the effects of SARS-CoV-2 by adding in serological testing or asking for self-reported SARS-CoV-2 status (16). Whilst useful, more recent studies are limited as participants may have been infected in different waves of the pandemic, with different variants of SARS-CoV-2, in different areas of a country that may have experienced different NPIs, different levels of support, and different epidemiological contexts.
This paper reports findings from the Ischgl study in Austria. Ischgl, a popular area for ski tourism, experienced an outbreak of SARS-CoV-2 in early March 2020. The virus then spread further, mainly to Northern Europe and the US (17–19). An initial population survey, including epidemiological and seroprevalence data, was conducted in April 2020 (Ischgl-1). A follow-up study was conducted in November 2020 (Ischgl-2), following the start of the second wave in Austria in October 2020.
The first signs of the outbreak emerged around 5th March 2020, when the international community pointed to Ischgl as an area of concern. Bars in the area closed on 10th March after cases were linked to an apres-ski bar. On 13th March the Paznaun valley, in which Ischgl is located, was placed into a sudden lockdown by the Federal Chancellor. The lockdown was announced in a press conference at 2 pm and police controls began 2 h later. Residents of Ischgl and foreign guest workers were obliged to stay in the area, but tourists were allowed to leave. This initial lockdown lasted until 23rd April 2020 (20, 21).
After April 2020, Ischgl was subject to the same package of NPIs as the rest of Austria. Between March and November 2020, this included (at differing levels of severity over time) stay-at-home orders, working from home (where possible), school closures, restrictions on gatherings, cancellation of public events, restrictions on internal movement, testing and contract tracing, quarantine and isolation of SARS-CoV-2 cases and suspected cases, international travel restrictions and mask mandates, supported by public information campaigns, income support for people and businesses and health system strengthening (ICU management, purchase of personal protective equipment) (4, 22).
Despite the proliferation of research into the effects of the COVID-19 pandemic on a range of outcomes, the Ischgl follow-up study offers unique insights. The study was undertaken in an immunologically naïve population and provided laboratory-confirmed evidence of infection with follow-up in a population in which over 40% of the adult population was infected. Compared to similar municipalities fewer new infections were reported in Ischgl between the two waves of the survey (23). Capitalising on this unique situation, this study can compare a wide range of outcomes of the COVID-19 pandemic in a broadly static population exposed to the same NPIs in people with and without laboratory-confirmed evidence of infection.
This study aims to assess the impact of the COVID-19 pandemic on self-reported physical and mental health, behaviours, and economic status in Ischgl, Austria. As such, the study aims to contribute to a wider understanding of disparate effects of the pandemic across demographic and socioeconomics groups as well as understanding levels of resilience within a community heavily reliant on tourism. In doing so, the study aims to provides insights that are relevant for developing pandemic preparedness and recovery strategies.
Using single-item measures of self-rated physical health (SRPH) and self-rated mental health (SRMH) widely used in research on inequalities in health in European contexts, this study reports changes in these measures by seropositivity before and after the pandemic (24, 25) The study also assesses self-reported changes in behaviours and economic circumstances before and after the pandemic, by known seropositivity after the SARS-CoV-2 outbreak, and by sociodemographic and socioeconomic factors. In this way, it aimed to assess the association of seropositivity with the outcomes studied and any disparities in the impacts of the pandemic.
After the initial outbreak of SARS-CoV-2, we conducted an initial survey (“Ischgl-1”), with a follow-up study in November 2020 (“Ischgl-2”) (23, 26). Ischgl-1 was a cross-sectional epidemiological survey with measurement of seroprevalence targeted all residents of Ischgl/Tyrol regardless of age or gender. It was conducted between April 21st and 27th, 2020. The study was approved by the ethics committee (EC) of the Medical University of Innsbruck with EC number 1100/2020 (Ischgl-1). 1,259 adults, participated in Ischgl-1, corresponding to around 80% of those living in the town at that time (both permanent residents and seasonal workers). By the end of April 42% of the local population (45% of the adult population) were seropositive, one of the highest seroprevalence levels reported in spring 2020 worldwide (26). The follow-up study, Ischgl-2 (EC Number 1330/2020), was conducted between November 2nd and 8th, 2020.
The current sample comprises the 801 adults aged 18 and over who participated in both Ischgl-1 and Ischgl-2. In Ischgl-1, 1,527 adults were invited to participate, of whom 1,259 (82.4%) agreed (26). 813 (64.6%) of them participated in the follow-up study, Ischgl-2, but 12 were excluded from the analysis due to inconsistent recording of age (n = 9), failure to complete a questionnaire (n = 2) and no blood sample (n = 1). The remaining 801 included slightly more (50.2% vs. 45%) who had been seropositive and more women (54% vs. 51.9%). The age distribution was similar in both studies (23).
The materials and methods used to test for SARS-CoV-2 antibodies and generate an indicator of previous infection with SARS-CoV-2 have been described elsewhere (23). In brief, blood samples were analysed for SARS-CoV-2-binding antibodies using four immunoassays. Samples were screened for anti-SARS-CoV-2-S1-protein IgA and IgG positivity by a commercially available anti-SARS-CoV-2-IgA and-IgG ELISA (Euroimmun, Lübeck, Germany), respectively, using the fully automated 4-plate benchtop instrument Immunomat™ (Virion/Serion, Würzburg, Germany). For both assays values >1.1 were considered positive. Borderline values (0.8–1.1) in the Euroimmun IgG ELISA were rated positive; for the Euroimmun IgA ELISA borderline values were rated as negative. Samples were additionally immunoassayed for anti-SARS-CoV-2 N-protein IgG (anti-N IgG) antibodies in a fully automated manner on the ARCHITECT i2000SR system (Abbott, Illinois, USA). Samples were considered positive if the detected relative light unit (RLU) was >1.4. Anti-N IgG was also quantified using the ElecsysAnti-SARS-CoV-2 (Roche Diagnostics, Indianapolis, USA) according to manufacturer’s recommendations. A COI of ≥1.0 was considered positive. Titres of SARS-CoV-2 neutralizing antibodies were determined using a replication defective vesicular stomatitis virus (VSV) pseudotyped with SARS-CoV-2 spike protein Titers of ≤1:4 were considered as negative, titres of ≥1:16 as positive.
Plasma samples from Ischgl-1 were analysed. The serostatus of the samples was defined as p, d, a or n depending on the binding antibody assays: p = positive = anti-S IgG+ AND anti-N IgG+ (either Roche or Abbott assay positive); d = discordant = anti-S IgG+ OR anti-N IgG+ (either Roche or Abbott assay); a = only IgA+ = only anti-S IgA+ but anti-S IgG-AND anti-N IgG-; n = negative = anti-S IgG-AND anti-N IgG-AND anti-S IgA-. To calculate the seroprevalence, all individuals with serostatus p were considered as seropositive. Individuals with ‘d’ and ‘a’ samples were considered as seropositive if they had neutralizing antibodies ≥1:16.
Ischgl-2 participants were interviewed to answer a questionnaire which included questions about changes to self-rated physical and mental health between November 2019 and November 2020 (Ischgl-2), pre-existing medical conditions, selected medications and symptoms (from a pre-specified list but with the ability to specify other symptoms) including their duration since April 2020 (Ischgl-1) (Table 1). The questionnaire was designed to generate data comparable with existing surveys, including the Community Response Survey developed by John Hopkins University (JHU CRS) that was specifically developed for assessing the impacts of COVID-19 (27), as well as other research on COVID-19 symptoms known about at the time, modified for the Austrian context and translated into German.
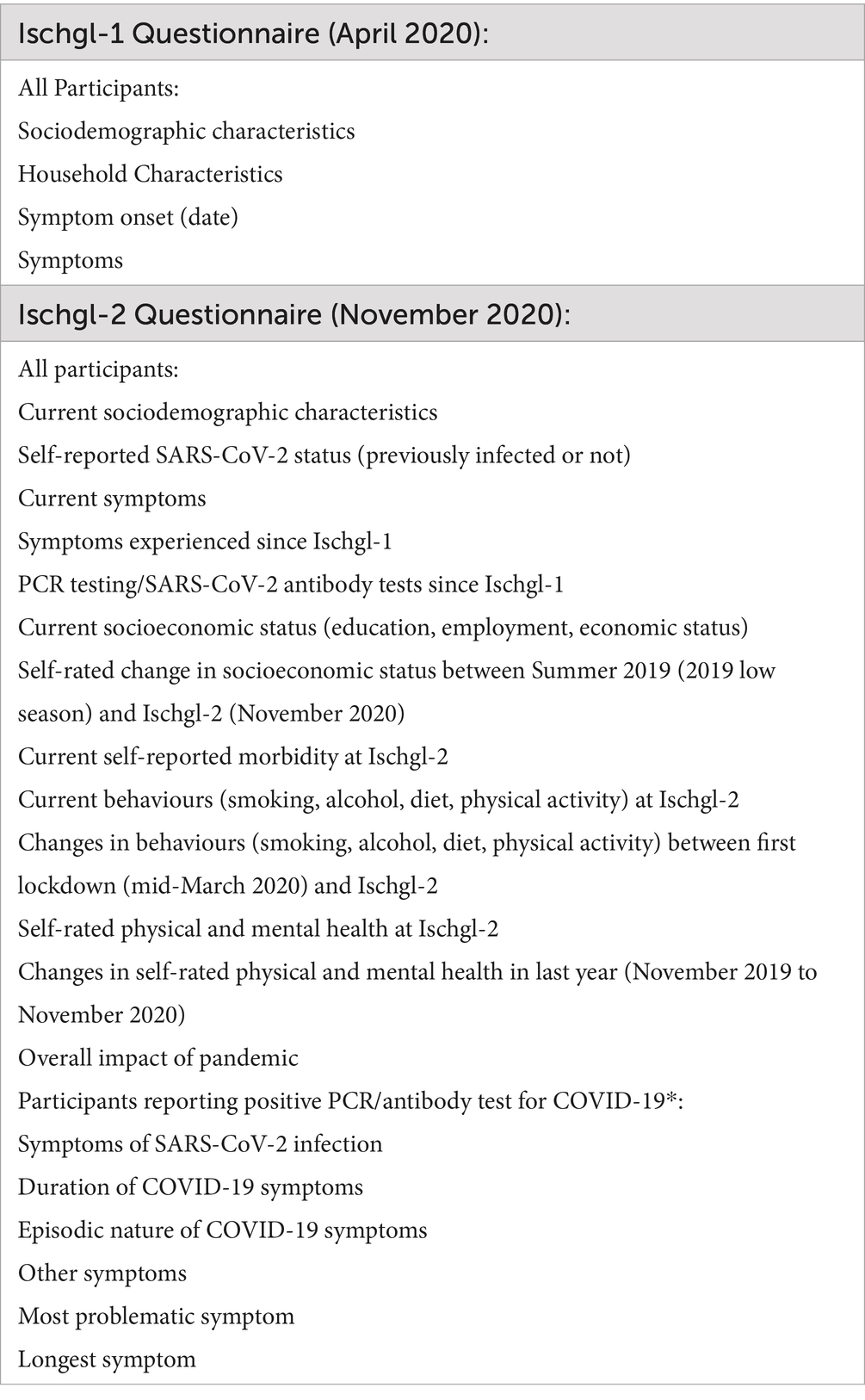
Table 1. Overview of questionnaire Data collected at Ischgl-1 and Ischgl-2.
Data were collected using Askimed, a web-based eCRF system for data collection and management. The system included checks for completeness, internal consistency, and validity. All interviewers attended a pre-fieldwork training session on the questionnaire and the Askimed system [Askimed access date: 20. 07. 2021 (Available online at: https://www.askimed.com/)].
Seropositivity was defined according to status at Ischgl-1 while all outcome measures were defined using data collected at Ischgl-2. These outcome measures were:
At Ischgl-2, all participants were asked to report if their physical or mental health had declined or improved between November 2019 and November 2020 (the last year) on a 5-point scale. The data were dichotomised into declined = 1 (“a lot worse,”” a little worse”) and otherwise = 0 (“no change, “a little better,” “much better”). All participants were also asked to self-report their current physical (SRPH) and mental health (SRMH) at Ischgl-2 by rating them separately on separate single-item 5-point scales (from poor to excellent). For analyses, SRPH and SRMH were dichotomised to poor = 1 (“poor,” “fair”) and good = 0 (“good,” “very good,” “excellent”).
Participants were asked to report if they currently smoke, consume alcohol and exercise and if these behaviours had increased or decreased consumption since the onset of the first lockdown in Ischgl (13th March 2020). For exercise, participants were asked about changes in both frequency and intensity. Categorical variables were constructed for changes in each behaviour (“stayed the same,” “increased,” “decreased”). Additionally, people were asked if their weight had stayed the same, increased or decreased since lockdown. Those who had experienced a change in weight were asked to self-report, in kilograms, their change.
Participants were asked to report any new symptoms they experienced since Ischgl-1 (April 2020), whether these were episodic in nature, their duration (in days) and whether they were still experiencing these symptoms.
Participants rated changes in their individual financial and professional situation since summer 2019 on a 5-point scale; data for both variables were dichotomised to worse = 1 (“significantly worse,” “slightly worse”) and same/improved = 0 (“no change,” “slightly improved,” “much improved”) and the extent to which they agreed that they were concerned about their future financial and professional security agree = 1 (“completely agree,” “agree”) and otherwise = 0 (“neither agree nor disagree,” “disagree,” “strongly disagree”). Summer 2019 was chosen to reflect the natural peaks and troughs in the tourism industry, which is a main source of economic activity in Ischgl.
Participants were asked to rate, on a 4-point scale, the overall impact of the pandemic on their daily lives, a question taken from the JHU CRS (27); data were dichotomised (“moderately/severely affected” = 1 and “a little affected, completely unaffected” = 0).
For the analyses presented here, seropositivity in Ischgl-1 is used to assess the relationship between prior SARS-CoV-2 infection and the outcome measures.
Summary characteristics are presented as means ± standard deviation (SD) or median and Interquartile Range (IQR), where appropriate, for continuous variables and number (n) and percentage (%) for categorical variables.
The relationships between the dependent variables and seropositivity were analysed using multivariate binary and multinomial logistic regression models, where appropriate. Age group (18 to <35 years, ≥35 to <50 years, ≥50 to <70 years, and ≥ 70 years), sex and morbidity (binary variable of self-reported hypertension, diabetes, chronic kidney disease (CKD), cancer, cardiovascular disease (CVD), neurological diseases and other lung diseases = 1, or none) were controlled for in all models. Other covariates included body mass index [“normal or underweight” (<25 kg/m2), “overweight” (≥25 to <30 kg/m2) or obese (≥30 kg/m2)], education (Compulsory/High School/University/Other) and working in the tourism sector (yes/no) as well as the outcome measures outlined above used as covariates in models, where appropriate.
Adjusted odds ratios (ORs) from binary logistic regression models are reported and adjusted relative risk ratios (RRs) from multinomial logistic regression models are reported with 95% confidence intervals (95% CI). Statistical tests were two-tailed statistical significance was set at an alpha level of 0.05. All analysis was done using Stata version 17.1 (Stata Corp., College Station, TX, USA).
Table 2 presents the characteristics of participants in the follow-up sample (n = 801). Just over 50% were seropositive in Ischgl-1 (50.3%, n = 403), 54.9% were female (n = 440), median age was 45 years (SD 15.8), one quarter reported at least one specified morbidity (25.7%, n = 205) and over 40% were overweight (BMI ≥ 25 kg/m2, n = 331). There was no significant difference in seropositivity by sex, age, morbidity or BMI in the sample.
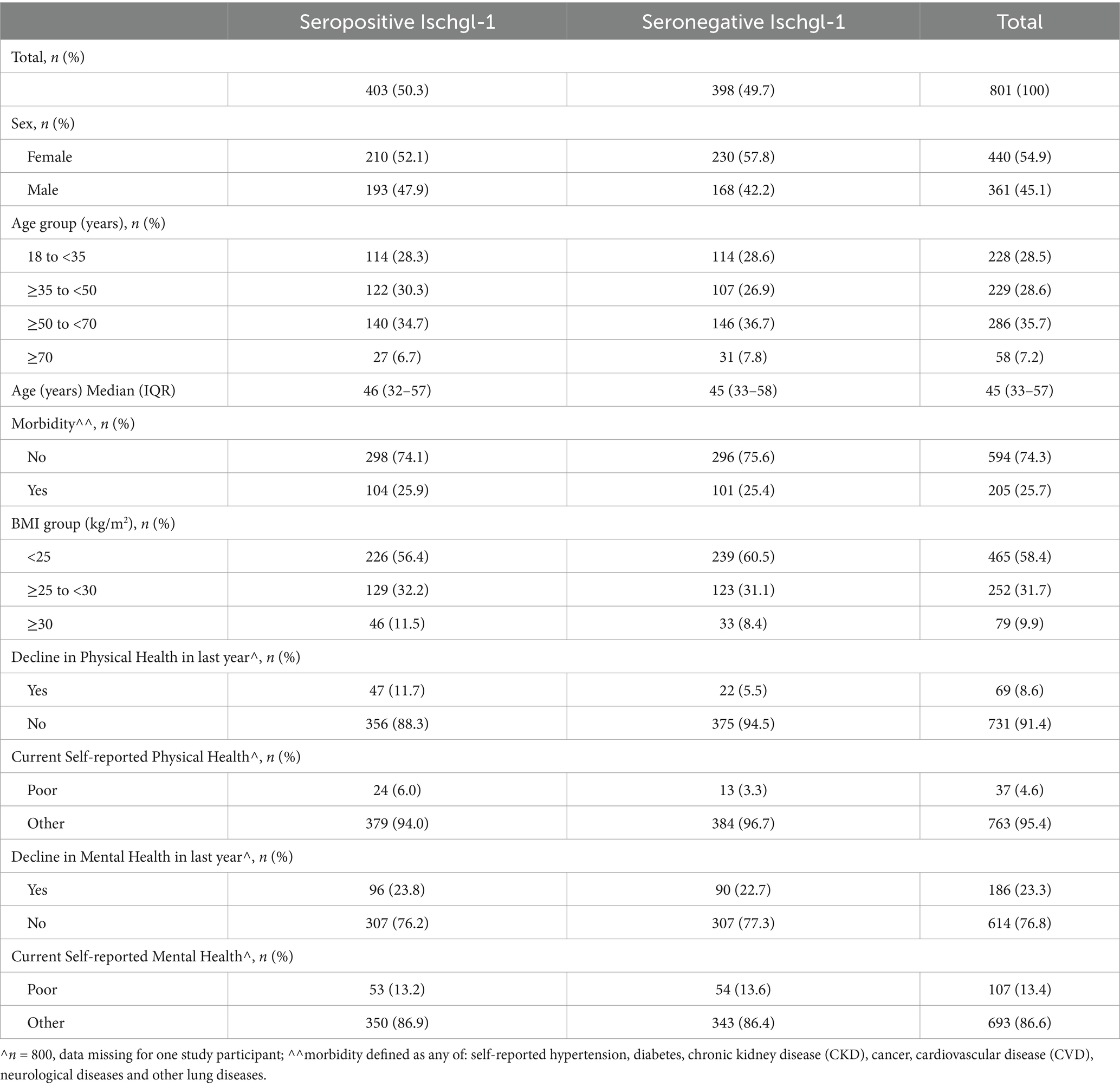
Table 2. Characteristics of follow-up sample (Ischgl-2) by seroprevalence at Ischgl-1.
Figure 1 shows the total percentage of participants reporting negative impacts across all outcome measures in November 2020 by sex, age and seropositivity. Over 55% of participants reported the pandemic had a moderate or severe impact on them. An age gradient was apparent; 63.2% of 18 to <35-year-olds reported a moderate/severe effect of the pandemic compared to 42.9% of adults ≥70 years. A greater proportion of participants reported worse economic outcomes than health outcomes (including negative impacts on behaviours). 8.6% of all participants reported a decline in physical health and nearly a quarter reported a decline in their mental health between November 2019 and November 2020 (the last year). Nearly half of all participants were concerned about their future professional situation (48.4%); the highest proportion of concern was reported among adults aged ≥35 to <50 years (63.9) and the lowest among those aged ≥70 years (5.5%). Similarly, 45.4% of participants were concerned about their future financial situation, with 68.7% of those aged ≥35 to <50 years concerned but only 12.5% of those aged 70 years and over. Only 5.3% of all participants increased alcohol consumption, and only 8.6% of all participants reported a decline in their physical health since the first lockdown implemented in Ischgl in mid-March 2020.
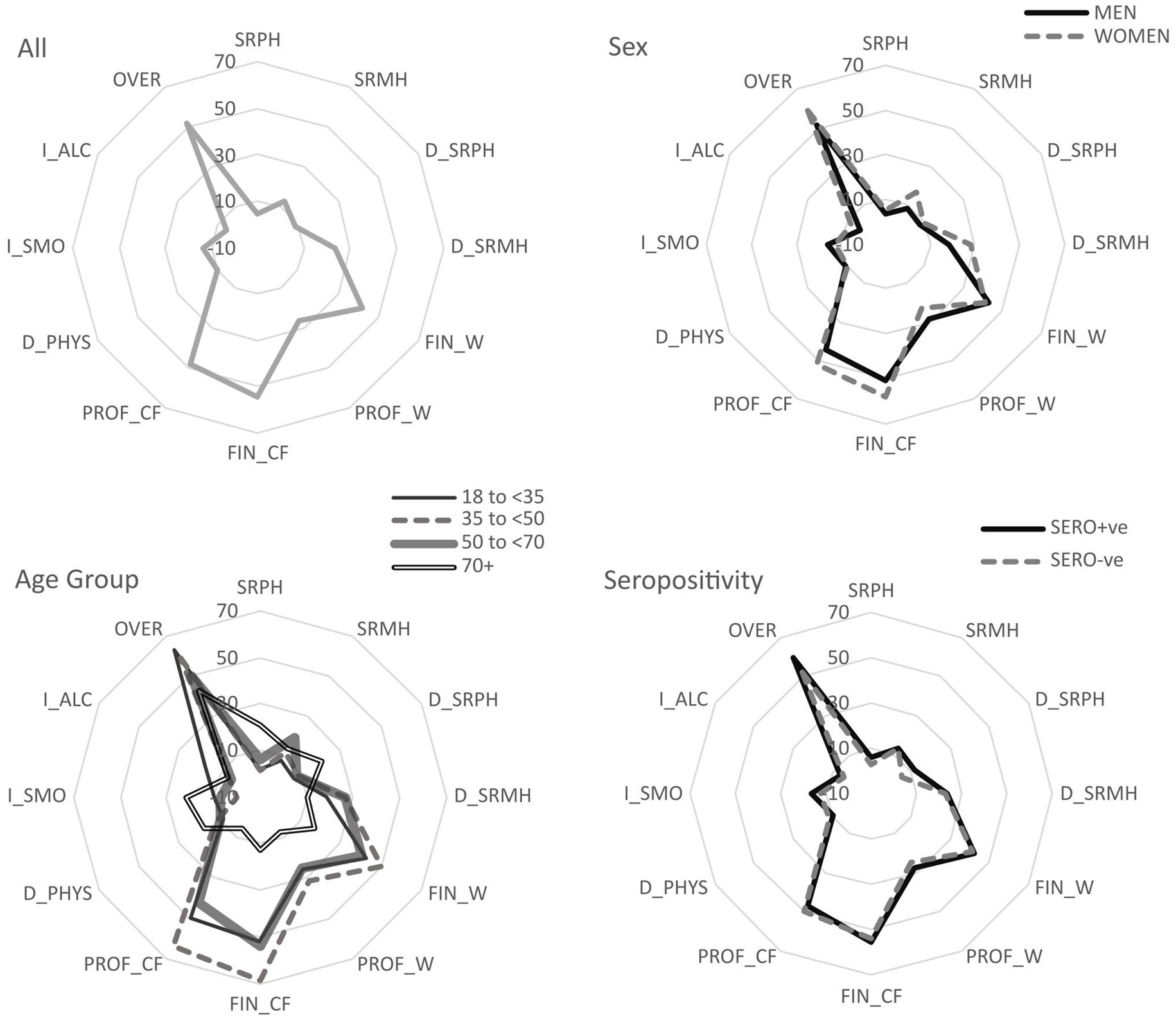
Figure 1. Overview of percentage of participants reporting negative outcomes of the pandemic for each outcome measure, overall and by subgroups. Key: SRPH: self-rated physical health, SRMH: self-rated mental health, D_SRPH: decline in self-rated physical health compared to last year, D_SRMH: decline in self-rated mental health compared to last year, I-ALC: increase in alcohol consumption, I_SMO: increase in smoking, D_PHYS: decline in physical activity, OVER: overall moderate/severe effect of the pandemic, FIN_W: financial situation worse since last summer, PROF_W: professional situation worse since last summer, FIN_CF: completely/strongly agree concerned about future financial situation, PROF_CW: completely/strongly agree concerned about future professional situation. Smoking, Alcohol and Physical Activity % are among people who have ever smoked/consumed alcohol or exercised, not whole sample.
Those in the seropositive group were more than twice as likely to report a decline in physical health than the seronegative (11.7 and 5.5%, respectively, Table 3). After adjusting for age, sex, BMI, education and morbidity, seropositive participants remained more than twice as likely as the seronegative to report a decline in SRPH (OR 2.38 (95% CI: 1.39, 4.09), Table 4). Other associations seen in the bivariate analysis also remained similar after adjustment (Tables 3, 4).
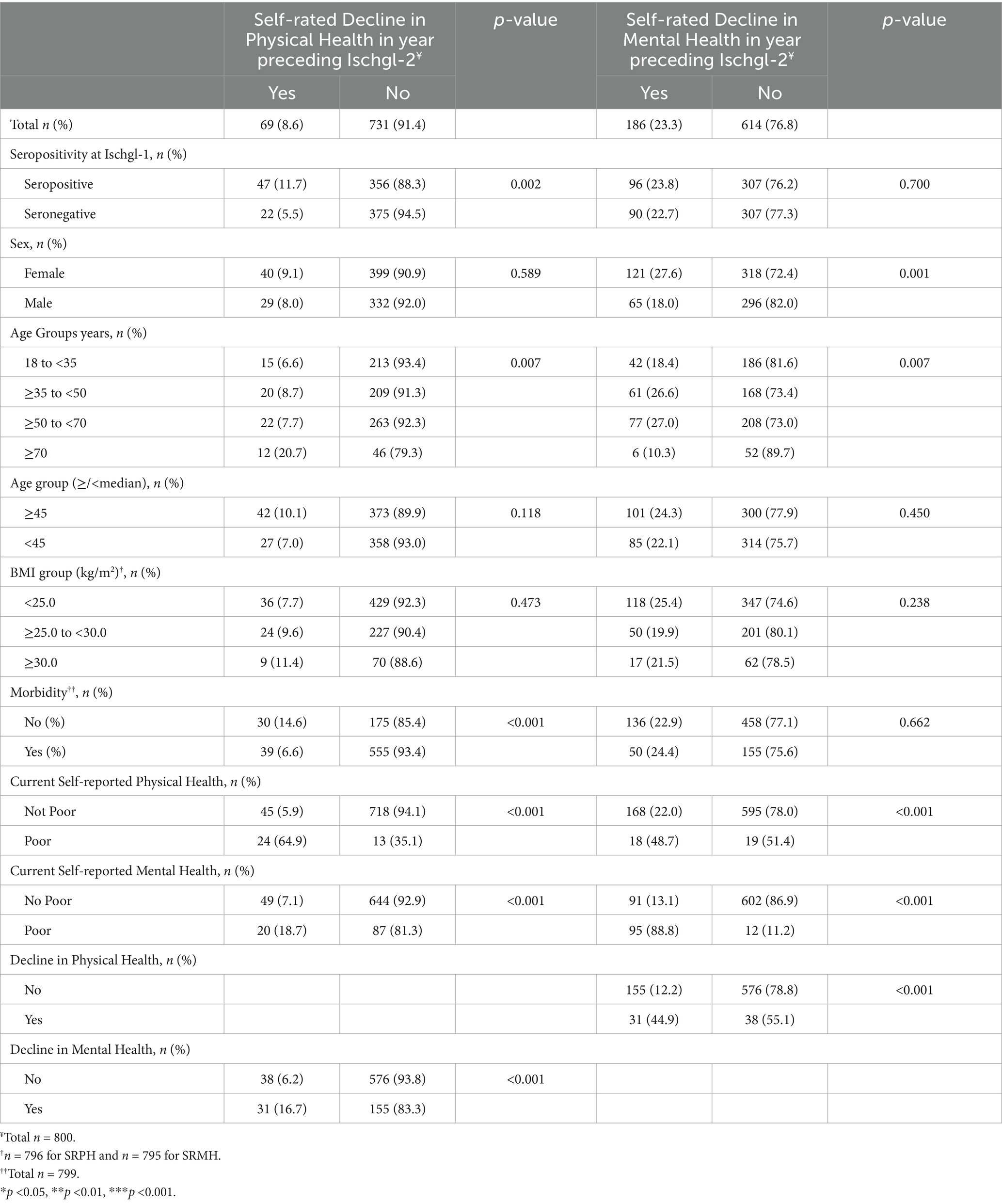
Table 3. Decline in SRPH and decline in SRMH by seropositivity at Ischgl-1.
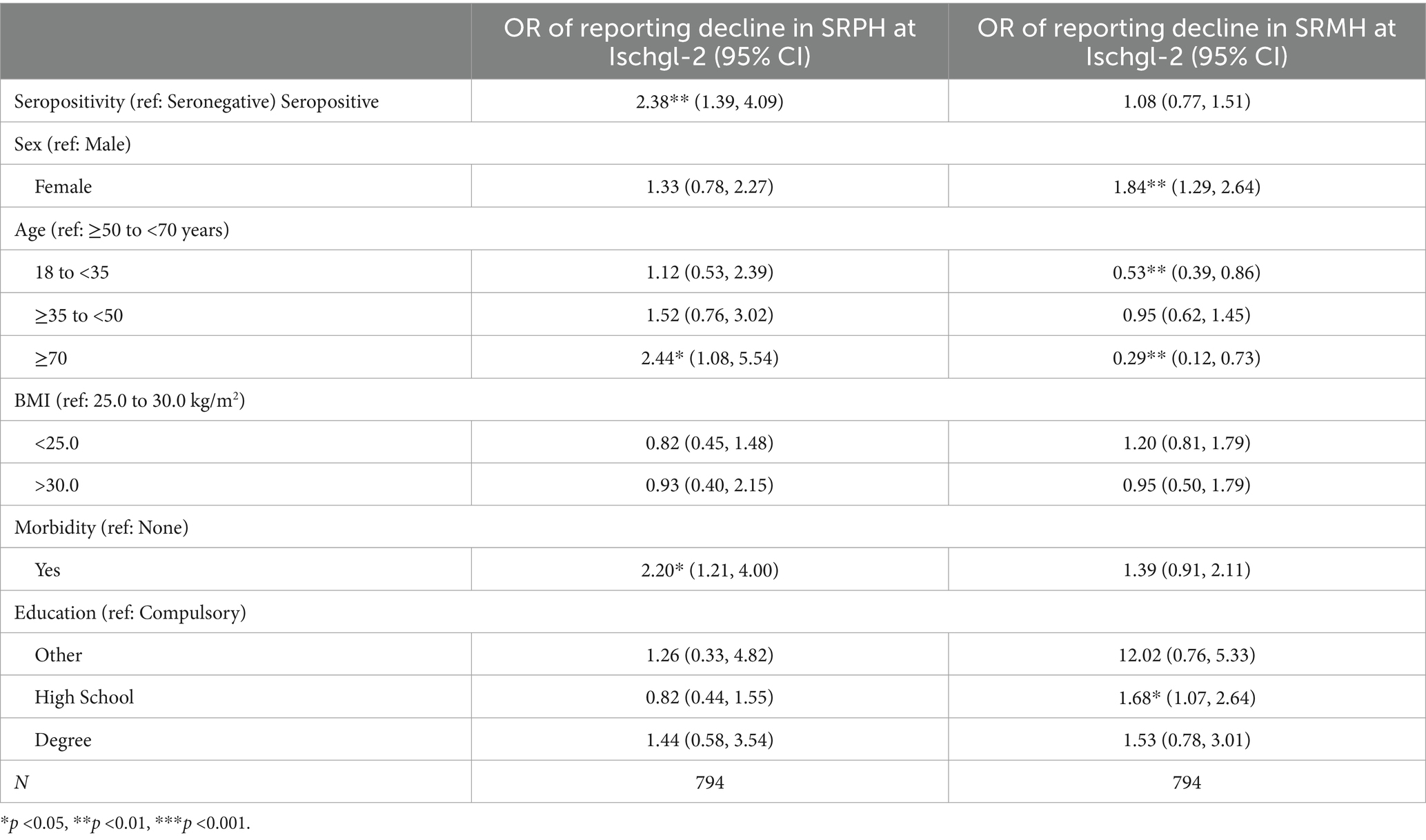
Table 4. Adjusted odds ratios (OR) for reporting decline in SRPH and decline in SRMH at Ischgl-2.
23.3% reported that their mental health had declined in the last year (Table 3; Figure 1); 13.4% of participants rated their current mental health as poor (Table 5). In contrast to the situation with SRPH, there was no significant difference in the proportion reporting a decline in SRMH by seropositivity. This remained non-significant after full adjustment for the same variables as used with SRPH (Tables 3, 4).
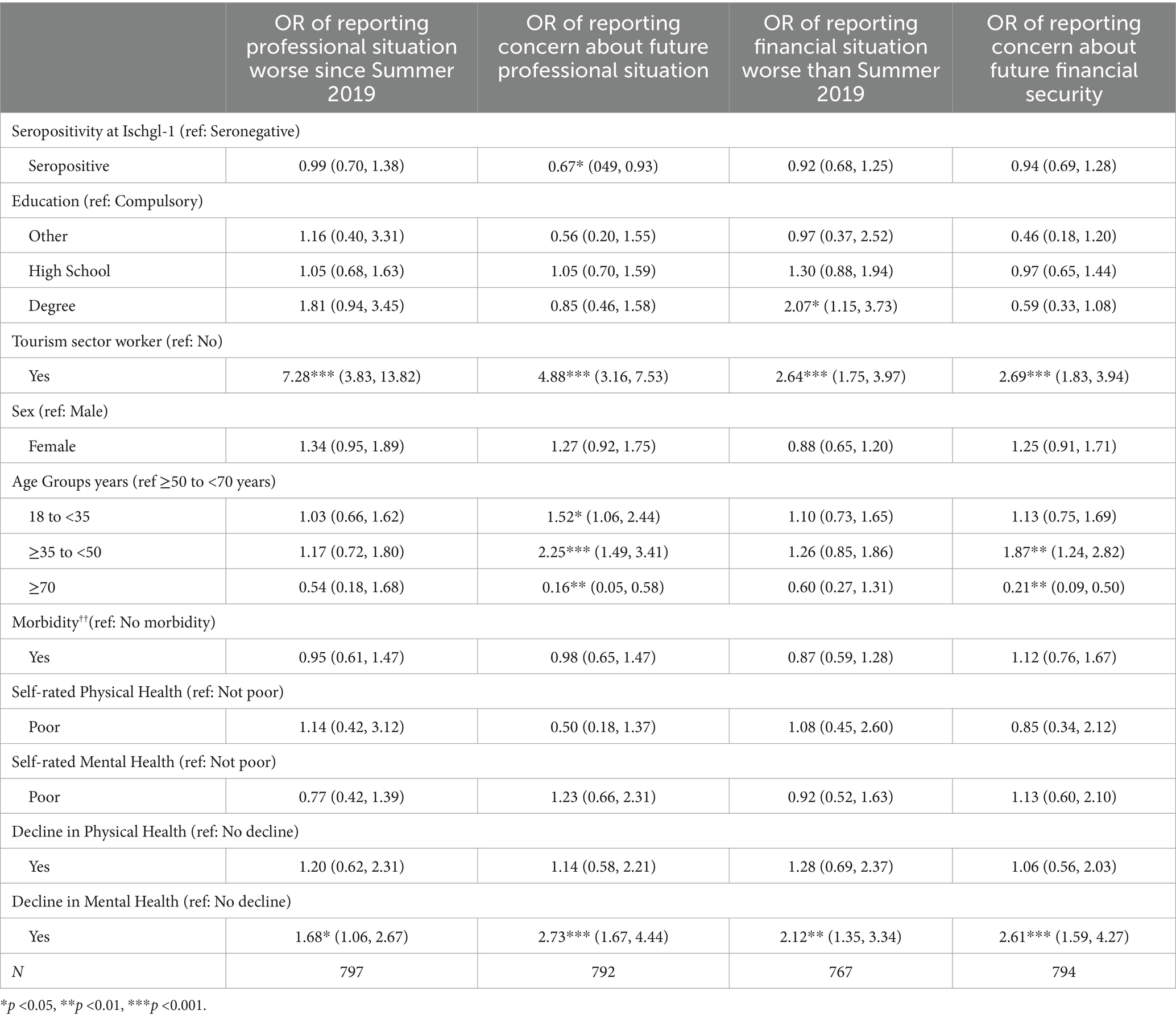
Table 5. Adjusted odds ratios for economic outcome measures.
Data on current smoking, alcohol consumption and exercise are reported in Web Appendix 3. Overall, 32.3% of the participants currently smoke, 83.0% consume alcohol and 13.6% do not exercise. People who were seropositive at Ischgl-1 were less likely to report currently smoking than those who were seronegative [OR 0.62 (95% CI: 0.45, 0.84)]; no relationship between seropositivity and current alcohol consumption or exercise was found (Web Appendix 4). Seropositivity was not associated with changes in smoking, alcohol consumption or exercise patterns since the first lockdown in mid-March 2020.
The majority of participants self-reported no change in weight (75.3%). In adjusted analyses, seropositivity was not associated with the risk of weight gain compared to stable weight but was associated with weight loss [RR 1.99, (95% CI: 1.11, 3.56)].
Participants reported any new episodes of symptoms they experienced since Ischgl-1. For participants who were seropositive, this analysis excludes symptoms that participants attributed to their infection with SARS-CoV-2. Participants reported similar proportions of experiencing new symptoms (seropositive 52.4%, seronegative 51.3%, Figure 2) and similar numbers of different symptoms since Ischgl-1 (mean among seropositive—1.3 different symptoms (95% CI: 1.1, 5.2; mean seronegative 1.4 different symptoms [95% CI: (1.2, 1.5)].
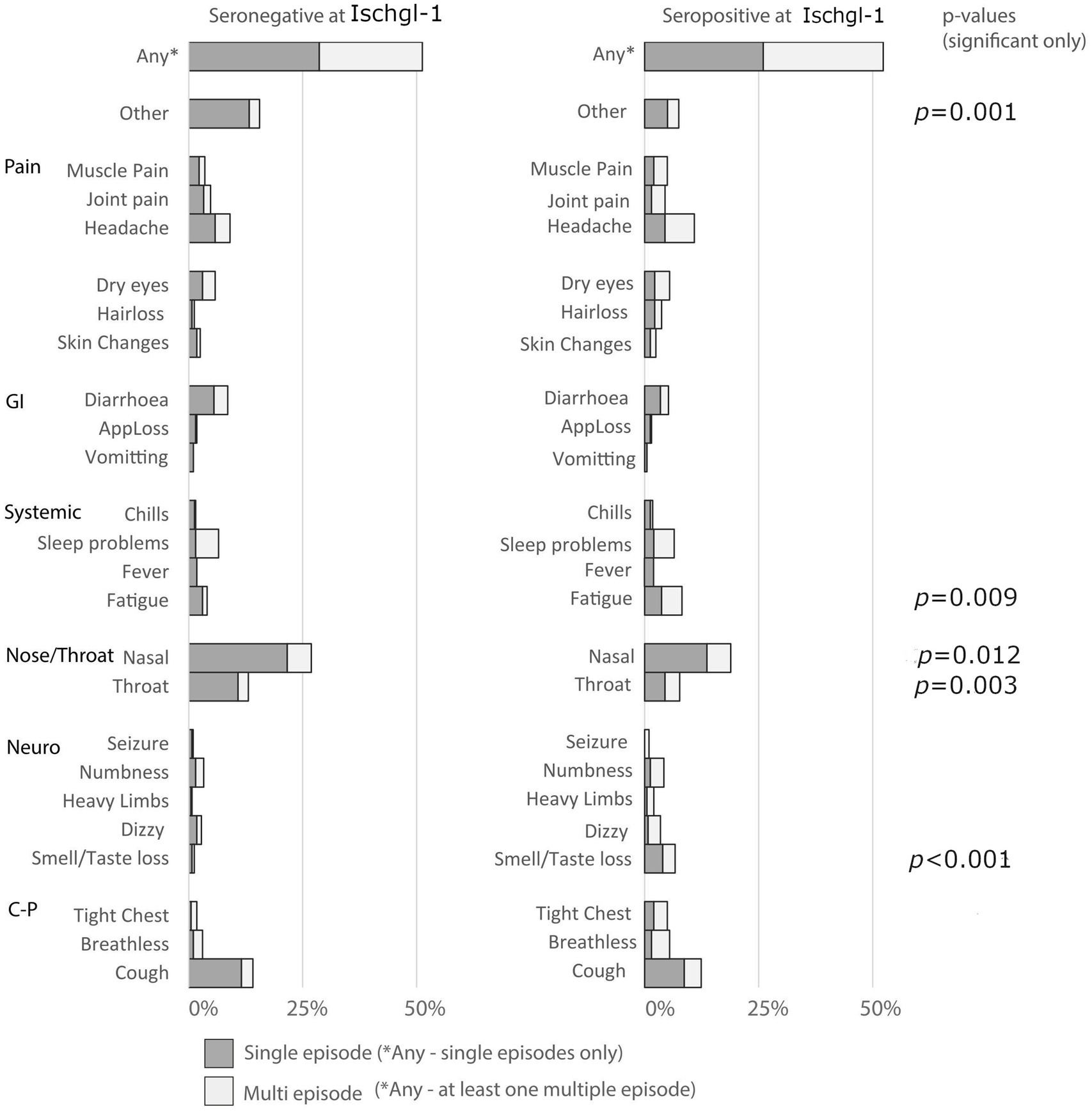
Figure 2. New onset symptoms since Ischgl-1. Key: GI: gastrointestinal, Neuro: Neurological, C-P: Cardiopulmonary.
People who were seropositive at Ischgl-1 were more likely to report new episodes of loss of taste and/or smell [OR 5.73 (95% CI: 2.16, 15.22)], tight chest [OR 2.91 (95% CI: 1.20, 7.06)] and fatigue [OR 2.07 (95% CI: 1.11, 3.86)] than seronegative participants. Seropositive participants reported fewer new episodes of nasal (runny/blocked nose) [OR 0.60 (95% CI: 0.42, 0.84)] and throat symptoms [OR 0.56 (95% CI: 0.35, 0.90)] than seronegative participants (Web Appendix 6). No other significant associations between seropositivity and specific symptoms were found among the sample. Hair loss was only reported among women (n = 20/440); among women being seropositive was associated with an increased odds of hair loss [OR 3.18 (95% CI: 1.12, 8.98)] compared to seronegative women.
In November 2020, over 1 in 4 adults in Ischgl considered their professional situation to be worse than the summer before (summer 2019, the last “normal” low season for tourism since the outbreak) and nearly half of all adults (48.4%) were concerned about their future professional situation. 42.1% of adults reported a worsening of their financial situation and 54.6% were concerned about how it might change in the future. Seropositivity was not significantly associated with changes in professional or financial situation, nor with concern about future finances. Participants seropositive at Ischgl-1 were a third less likely to be concerned about their professional future than seronegative participants (OR 0.67 (95% CI: 0.49, 0.93) Table 5).
Overall, just over half of all participants reported that the COVID-19 pandemic had influenced their lives moderately or severely (55.6%, Web Appendix 8). In all models, being younger, experiencing a decline in mental health and worsened professional and financial situation were associated with reporting a moderate/severe impact of the pandemic overall (Models 1–4, Table 6). Seropositivity was only found to be significantly associated with the overall effect of the pandemic in multivariate analyses once controlling for concern for future professional and financial situation (Model 4, Table 6).
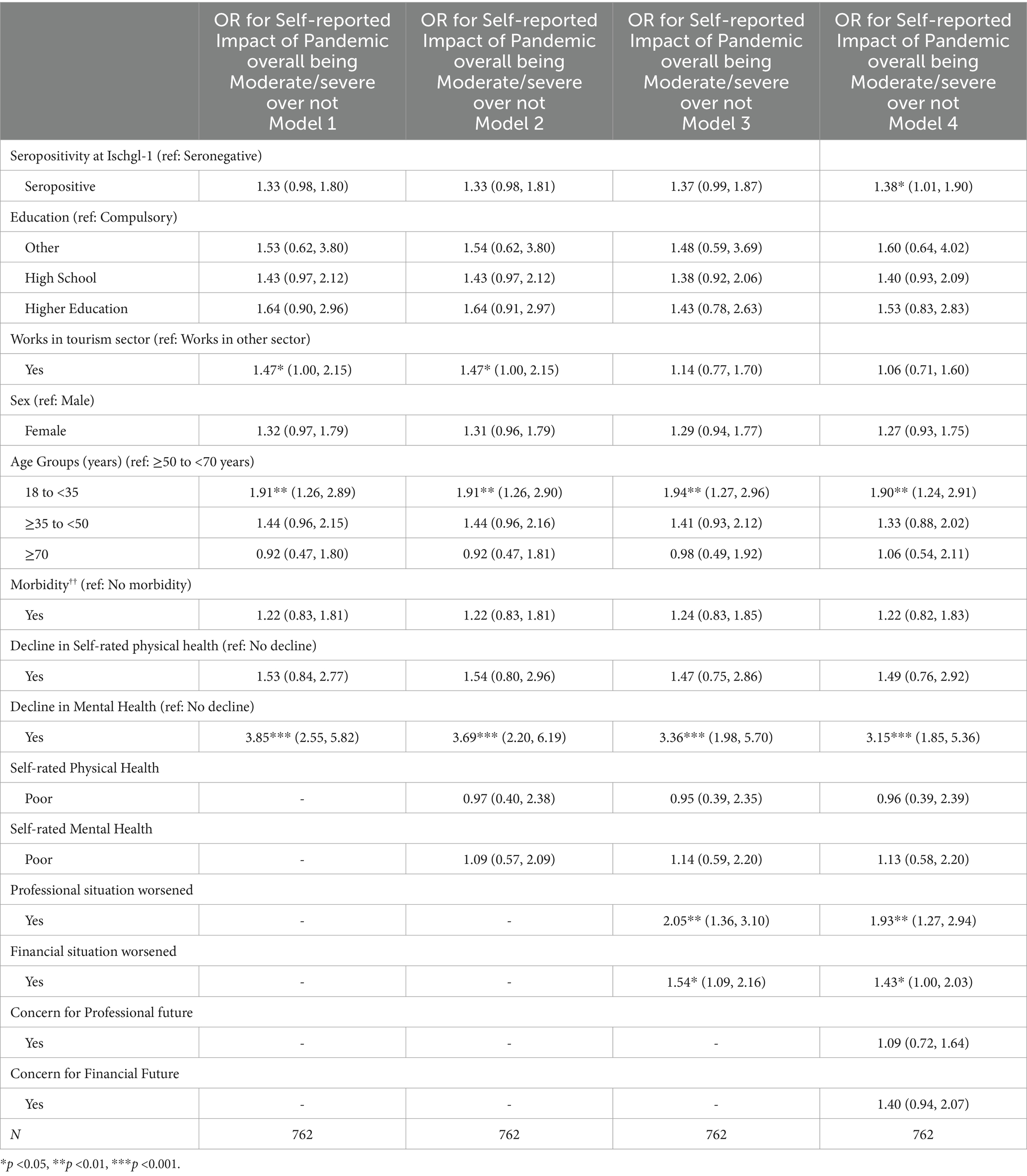
Table 6. Adjusted odds ratios for overall impact of pandemic vs. otherwise.
All results reported are from adjusted analyses and control for seropositivity.
Those aged 18 to <35 years were significantly more likely to report a moderate or severe effect of the pandemic than those aged ≥50 to <70 years (OR 1.90 (1.24, 2.91) Model 4, Table 6). Whilst people 18 to <35 years had the lowest levels of current poor SRMH at Ischgl-2 (Web Appendix 1) nearly 1 in 4 reported a decline in MH since November 2019 (in the last year) (Table 3). This age group was 1.5 times as likely to be concerned for their future professional and economic circumstances than those aged ≥50 to <70 years (Table 5); the magnitude of the difference was even greater when the comparison was with those aged 70 years and above. Alcohol consumption since Ischgl-1 reduced in this age group compared to the others (Web Appendix 5). Those aged 18 to <35 years old were more likely to report nasal symptoms, throat symptoms and fatigue since Ischgl-1 than those aged ≥50 to <70 years (Web Appendix 6).
People aged ≥35 to <50 years were not more likely to report a moderate or severe impact of the pandemic than those aged ≥50 to <70 years (Table 6). Additionally, those in this age group were not more likely to report their economic situation had worsened since summer 2019 than those aged ≥50 to <70 years. However, they were more likely to be concerned about their future economic circumstances than those aged ≥50 to <70 years (Table 5). In this age group, 26.6% reported a decline in mental health in the last year, compared to just over 1 in 10 among those aged ≥70 (Table 3).
Whilst people aged ≥50 to <70 years were not significantly more likely to report a moderate or severe impact of the pandemic compared to those aged 70 years and over (Table 6), they were more likely to be concerned about their about both their future professional and economic circumstances than adults those aged ≥70 years (Table 5). In this age group, the greatest proportion (27.0%) reported a decline in mental health, similar to those aged ≥35 to <50 years (Table 3). They were 1.85 times as likely to report a decline in mental health compared to the youngest age group (18 to <35, 95% CI: 1.16, 2.96) and 3.41 times as likely to report a decline compared to those aged ≥70 (95% CI: 1.37, 8.51).
People aged 70 and older were least likely to be concerned about their future economic circumstances, and least likely to report a decline in mental health. As expected, the oldest age group (≥70 years) were significantly more likely to report a decline in physical health (OR 2.44 (95% CI: 1.08, 5.54) Table 4).
Age group was not associated with changes in smoking and physical activity.
Women were nearly 40% more likely to report a moderate or severe overall effect of the pandemic than men (Table 6). Whilst no differences were found in a decline in SRPH by sex, women were more likely to report a decline in mental health (OR 1.84 (95% CI: 1.29, 2.64), Table 4).
Sex was not significantly associated with any changes in smoking, alcohol consumption or physical activity in the last year (Web Appendix 5). There were no significant associations between sex and changes in professional or economic circumstances, nor in concern for these in the future.
People working in the tourism sector were nearly 50% more likely to report a moderate or severe impact of the pandemic than others (OR 1.47 (95% CI: 1.00, 2.15) Model 2, Table 6). This effect was no longer significant when controlling for changes and concern for economic circumstances (Model 3 and 4, Table 6). A person working in tourism was seven times more likely to report worsening in their professional situation and nearly three times as likely to report worsening in their financial situation than people working in other sectors (Table 5). Tourism workers were more likely be concerned for both their future professional activity and finances—even when controlling for any decline in economic circumstances since summer 2019 (Web Appendix 7).
People working in tourism were twice as likely to report a decline in SRMH [OR 2.03 (95% CI: 1.26, 3.27)] although the effect was attenuated when controlling for worsening financial and professional status [OR 1.68 (95% CI: 1.01, 2.79)] and became non-significant when additionally controlling for professional and financial concerns [OR 1.26 (95% CI: 0.74, 2.14)], indicating a clear nexus between mental health and economic effects.
No differences were found between those working in tourism and others in changes in SRPH, smoking, alcohol consumption or physical activity.
The present study examines the association between prior infection with SARS-CoV-2 and wide-ranging impacts of the COVID-19 pandemic, including changes in self-rated physical and mental health, behaviours and economic status. It also analysed disparities in outcomes by sociodemographic characteristics.
We found that seropositivity was associated with indicators of worsened physical health (although absolute levels were low) and certain symptoms in the subsequent months, but not changes in behaviours.
Combining the ≥50 to <70 and ≥70 age groups, 11.0% reported worsened SRPH, similar to the Austrian SHARE study (10.9% of those over 50), which compared pre-SARS-CoV-2 data to June 2020. Though using a different time frame and a three-point response scale (28), both studies align. Despite the low absolute prevalence of poor physical health in our study, it was linked to seropositivity, suggesting a limited but lasting impact of SARS-CoV-2 on self-reported health.
Behavioural changes were even more limited than those in self-reported physical health and were unrelated to seropositivity. Few changes were noted; smoking increased more than it decreased, while alcohol consumption declined and physical activity rose. The drop in alcohol use aligns with NPI-related bar closures, but increased physical activity contrasts with most studies showing declines (29). his may reflect altered work patterns and unique access to the Alps in Ischgl, allowing for socially distanced exercise. Differences in pre-pandemic activity norms, like Iceland’s reliance on team sports, and study design variations may also explain these trends (30).
Despite stable behaviours and modest health declines, 1 in 2 participants reported a moderate or severe pandemic impact, mainly on mental health and finances—both unrelated to seropositivity. This underscores the strong, lasting indirect effects of the pandemic.
By November 2020, 8 months into the pandemic, 15.7% of participants reported poor physical or mental health. Over 20% saw a mental health decline since November 2019, with few improving, while 10% reported worse physical health. In August 2019, the OECD found 7.8% of Austrians aged 15+ had poor SRH. Though that study did not separate physical and mental health, our findings suggest mental health decline was a major pandemic impact (31).
A March–April 2020 study in Austria found 43% of those over 16 reported moderate or severe psychological impact, with higher rates in women (6). Our study, conducted in November 2020, found lower rates of poor SRMH (13.4%) and SRMH decline (23.3%). Differences may stem from study design, bias, and timing. Early 2020 saw strict NPIs, while by November, the population had adapted, possibly easing mental health effects despite Ischgl’s second wave. The NAKO study linked lower psychological distress to lower incidence rates, and Ischgl’s relatively few new infections may have mitigated mental health declines (23).
The most prevalent impact of the pandemic in our study population was economic; 50% of people reported a worsening of their professional and/or financial situation. This did not differ by seropositivity. However, certain segments of the population were disproportionately affected by particular impacts of the pandemic.
Tourism workers faced the greatest professional and financial impact due to NPIs, reflecting the sector’s local importance. Early in the pandemic, the economic effects of NPIs were unclear. By October 2020, a Tyrolean government report estimated the early ski season closure cut Ischgl’s seasonal revenue by 20–30% (17), despite mitigation efforts. Our study supports the well-known link between economic strain and mental health. Tourism workers had higher SRMH decline rates from November 2019–2020, explained by financial and job pressures. Similar findings were reported in Germany’s NAKO study (32).
Other population groups were also disproportionately affected by the pandemic—with differential effects by age and sex, in line with other studies in other European populations, and in Austria (6, 33). Overall, those aged 18 to <35 years who were most likely to report a moderate or severe overall impact effect of the pandemic, despite older age groups being at greatest risk for serious illness and mortality caused by COVID-19. For example, at Ischgl-1, only 2% of all participants found to be seropositive had been hospitalised because of COVID-19, yet 14.8% of seropositive participants aged over 70 were hospitalised. In November 2020, the oldest age group was more likely to report declines in SRPH since November 2019 than other age groups, but these declines did not appear to be directly exacerbated by SARS-CoV-2 infection. In a stratified analysis, no relationship was found between seropositivity and a decline in SRPH among this age group. However, those over 70 years of age were far less likely to be concerned about their economic future than the other age groups, and less likely to report any declines in mental health. Declines in mental health and current poor MH were most acute in the middle age groups (≥35 to <50 and ≥ to <70 years) which is in line with the SHARE study when comparing to older age groups (34).
Women were more likely to report a moderate or severe effect of the pandemic than men. In line with the Traunmüller study in Austria, we also found women reported more worsening of their mental health (6). Of the 13% of participants reporting poor SRMH, the majority were women, in line with pre-pandemic studies which have consistently shown women tend to report higher rates of psychological distress than men, reasons for which remain unclear conclusive but have been linked to differences in exposure to risks for developing, vulnerabilities to, experiences of, and responses to mental health between genders (6, 35). Women in our study were also more likely to report declines in their mental health than men. Other studies have linked the disproportionate effect of the pandemic on women’s mental health to be associated with changes in social networks, social activities and contact and social isolation, alongside changes in care-giving responsibilities including a greater responsibility for homeschooling during lockdowns, despite potential other benefits from working from home (10, 36). Further research would be needed to understand these factors in the Austrian context, and it is important to highlight our study lacks data on wider social networks that are clearly integral to both the wider impacts of NPIs and understanding how NPIs impact people. Indeed, the fact that our study population experienced the same NPIs and there were no gender differences in laboratory-confirmed seropositivity suggests it is not NPIs or SARS-CoV-2 infection, per se, that has led to this disparity.
The strength of this study is that it is based on a population with laboratory-confirmed SARS-CoV-2 status, all infected in the same outbreak and experiencing the same waves of the pandemic and NPIs. Nonetheless, it has some limitations. It relies on self-reported data, which introduces the possibility of recall bias concerning their health, behaviours, or economic status. Also, while the situation in Ischgl provides an unusual opportunity to undertake such a study, as a community heavily reliant on tourism the generalisability of the findings is limited. Another limitation stems from the timing of data collection. The follow-up survey occurred in November 2020, during the second wave of the COVID-19 pandemic, and will not capture the long-term effects of the virus or the non-pharmaceutical interventions used to control its spread. Also, while we examined some behaviours directly related to health, there may be others, such as gambling, that could have been impacted by the pandemic. Our health assessments relied on single-item measures for physical and mental health, which, while widely used, may not fully capture the complexity of health changes experienced by participants. Additionally, variations in the intensity and timing of infection waves and NPIs within Austria could introduce variability not fully addressed in the analysis. Finally, we lacked data on social networks, which may be relevant given the impact of social connectivity on mental health during periods of restrictive measures.
This study reinforces recommendations that have been made by others in the light of experience during the pandemic. Mental health emerged as a critical concern, particularly for women and middle-aged adults, many of whom reported declines in well-being. Pandemic preparedness should include the ability to scale up online counselling and other forms of remote support, some of which could be delivered by volunteers with basic training and appropriate safeguards. Economic strain, especially for workers in tourism-reliant regions like Ischgl, highlights the need for financial aid and job retraining programmes that can be deployed during and after a pandemic. Looking ahead, especially in the light of climate change and its impact on snow cover, diversifying local economies in ski resorts will offer longer-term stability. For younger adults who expressed concerns about job security, initiatives like internships, apprenticeships, and guaranteed job opportunities can help stabilise their professional trajectories. There is a clear need to monitor individuals with persistent physical symptoms.
Preparedness for future pandemics must include tailoring non-pharmaceutical interventions to specific community contexts, aiming to minimise mental health and economic impacts. Collecting appropriate data on social, psychological, and economic outcomes during health crises is vital for holistic response plans. Gender-sensitive policies should also be prioritized to address the disproportionate burdens on women, such as expanded childcare support, flexible work arrangements, and mental health initiatives tailored to their needs.
Whilst the effects of the pandemic reported by participants in Ischgl were wide-ranging, the population of Ischgl was relatively resilient to the impact of the pandemic in terms of physical health and behaviours. However, half of the population considered the overall effect of the pandemic to be moderate or severe by November 2020. Considerable strain was apparent among the economically active population. Women and middle-aged participants were disproportionality affected in terms of their mental health. Furthermore, a clear nexus exists between economic pressures and declines in mental health, as reflected in the concerns of those working in the tourism sector, which dominates the economy of Ischgl. In future pandemics particular attention should be given to communities built on tourism, but the experience of Ischgl highlights that such populations, supported by appropriate government policies, can be resilient and recover well.
There are idiosyncrasies in the experience of Ischgl during the COVID-19 pandemic—which highlight the importance of context in pandemic preparedness. Equally, many impacts in Ischgl were seen in other European studies. Whilst many countries worldwide were able to use modelling to inform measures to prevent deaths during the pandemic, it is widely accepted that, in most countries, evidence on the social and economic impacts of mitigation policies were less reliable and available (37). The provision of timely and robust data detailing the wider aspects of the impact during these crucial phases, particularly social and economic aspects, should be a priority in future pandemic preparedness, aiming to reduce the length and depth of the indirect effects of a pandemic.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Medical University Innsbruck Ethics Committee. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
KB: Conceptualization, Data curation, Formal analysis, Funding acquisition, Methodology, Project administration, Writing – original draft, Writing – review & editing. WB: Investigation, Project administration, Writing – original draft, Writing – review & editing, Conceptualization, Formal analysis. MM: Conceptualization, Investigation, Writing – original draft, Writing – review & editing. LH: Writing – original draft, Writing – review & editing. PB: Writing – original draft, Writing – review & editing. ZB: Formal analysis, Writing – original draft, Writing – review & editing. LR: Writing – original draft, Writing – review & editing. AR: Writing – original draft, Writing – review & editing. BF: Writing – original draft, Writing – review & editing. JP: Writing – original draft, Writing – review & editing. AW: Writing – original draft, Writing – review & editing. SS: Data curation, Software, Writing – original draft, Writing – review & editing. LF: Data curation, Software, Writing – original draft, Writing – review & editing. LK: Writing – original draft, Writing – review & editing. JK: Formal analysis, Writing – original draft, Writing – review & editing. DV: Conceptualization, Funding acquisition, Investigation, Supervision, Writing – original draft, Writing – review & editing. HU: Conceptualization, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing.
The author(s) declare that financial support was received for the research and/or publication of this article. This research was funded in whole or in part by the Austrian Science Fund (FWF) [Grant-DOI 10.55776/M3069].
We thank Bianca Neurauter for excellent assistance when organizing the study. We thank Brigitte Müllauer, Lisa-Maria Raschbichler, Albert Falch, Maria Huber, Teresa Harthaller, and Eva Hochmuth for excellent technical support. We would like to thank the volunteers who helped with blood collection etc. at the study site (Agnes Scharrer, Leonie Mauser, Albert Falch, Liesa-Marie Schreiber, Alina Mracsna, Lisa-Maria Raschbichler, Anastasia von Canal, Magdalena Fruhwirth, Anna Haslwanter, Maria Holzknecht, Benedikt Leonhard, Maria Huber, Bianca Neurauter, Martin Anegg, Brigitte Müllauer, Martin Klieber, Carina Praxmarer, Michael Unterhofer, David Bante, Nina Fernbach, Eva Hochmuth, Rosmarie Gstraunthaler, Fatima Aslam, Sophia Schmidt, Frederik Radvan, Teresa Harthaller, Hanna Salvotti, Theodora Todorovic, Jonas Huber, Theresa Genser, Katharina Wagner, Valentin Schiessendoppler, Lena Hinterstoisser, Verena Söll).
LK was employed by company Tyrolpath Obrist Brunhuber GmbH.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1488108/full#supplementary-material
1. Nader, IW, Zeilinger, EL, Jomar, D, and Zauchner, C. Onset of effects of non-pharmaceutical interventions on COVID-19 infection rates in 176 countries. BMC Public Health. (2021) 21:1472. doi: 10.1186/s12889-021-11530-0
2. Gröndal, M, Ask, K, Luke, TJ, and Winblad, S. Self-reported impact of the COVID-19 pandemic, affective responding, and subjective well-being: a Swedish survey. PLoS One. (2021) 16:e0258778. doi: 10.1371/journal.pone.0258778
3. Douglas, M, Katikireddi, SV, Taulbut, M, McKee, M, and McCartney, G. Mitigating the wider health effects of covid-19 pandemic response. BMJ. (2020) 369:m1557. doi: 10.1136/bmj.m1557
4. Bates, K, and Hayek, L. Austria: a ski resort as the virus slingshot of Europe In: D Lilleker, M Grfegor, and E Novelli, editors. Political communication and COVID-19: Governance and rhetoric in times of crisis, C.I. London: Routledge (2021)
5. Peters, A, Rospleszcz, S, Greiser, KH, Dallavalle, M, and Berger, KComplete list of authors available under: Collaborators. The impact of the COVID-19 pandemic on self-reported health. Dtsch Arztebl Int. (2020) 117:861–7. doi: 10.3238/arztebl.2020.0861
6. Traunmüller, C, Stefitz, R, Gaisbachgrabner, K, and Schwerdtfeger, A. Psychological correlates of COVID-19 pandemic in the Austrian population. BMC Public Health. (2020) 20:1395. doi: 10.1186/s12889-020-09489-5
7. Fronteira, I, Sidat, M, Magalhães, JP, de Barros, FPC, Delgado, AP, Correia, T, et al. The SARS-CoV-2 pandemic: a syndemic perspective. One Health. (2021) 12:100228. doi: 10.1016/j.onehlt.2021.100228
8. Osterrieder, A, Cuman, G, Pan-Ngum, W, Cheah, PK, Cheah, PK, Peerawaranun, P, et al. Economic and social impacts of COVID-19 and public health measures: results from an anonymous online survey in Thailand, Malaysia, the UK, Italy and Slovenia. BMJ Open. (2021) 11:e046863. doi: 10.1136/bmjopen-2020-046863
9. Zaccardi, F, Tan, PS, Shah, BR, Everett, K, Clift, AK, Patone, M, et al. Ethnic disparities in COVID-19 outcomes: a multinational cohort study of 20 million individuals from England and Canada. BMC Public Health. (2023) 23:399. doi: 10.1186/s12889-023-15223-8
10. Scheel-Hincke, LL, Ahrenfeldt, LJ, and Andersen-Ranberg, K. Sex differences in activity and health changes following COVID-19 in Europe—results from the SHARE COVID-19 survey. Eur J Pub Health. (2021) 31:1281–4. doi: 10.1093/eurpub/ckab096
11. Pierce, M, Hope, H, Ford, T, Hatch, S, Hotopf, M, John, A, et al. Mental health before and during the COVID-19 pandemic: a longitudinal probability sample survey of the UK population. Lancet Psychiatry. (2020) 7:883–92. doi: 10.1016/S2215-0366(20)30308-4
12. McGinty, EE, Presskreischer, R, Han, H, and Barry, CL. Psychological distress and loneliness reported by US adults in 2018 and April 2020. JAMA. (2020) 324:93–4. doi: 10.1001/jama.2020.9740
13. Ortoleva Bucher, C, Delmas, P, Oulevey Bachmann, A, and Gilles, I. Stressors, self-reported overall health, potential protective factors and the workplace well-being of nurses during the COVID-19 pandemic in Switzerland: a longitudinal mixed-methods study protocol. BMJ Open. (2021) 11:e057021. doi: 10.1136/bmjopen-2021-057021
14. Potere, N, Valeriani, E, Candeloro, M, Tana, M, Porreca, E, Abbate, A, et al. Acute complications and mortality in hospitalized patients with coronavirus disease 2019: a systematic review and meta-analysis. Crit Care. (2020) 24:389. doi: 10.1186/s13054-020-03022-1
15. Menni, C, Valdes, AM, Freidin, MB, Sudre, CH, Nguyen, LH, Drew, DA, et al. Real-time tracking of self-reported symptoms to predict potential COVID-19. Nat Med. (2020) 26:1037–40. doi: 10.1038/s41591-020-0916-2
16. University of Essex, Institute for Social and Economic Research. Understanding society: COVID-19 study, 2020–2021. [data collection]. UK Data Service (2021) doi: 10.5255/UKDA-SN-8644-11
17. Gudbjartsson, DF, Helgason, A, Jonsson, H, Magnusson, OT, Melsted, P, Norddahl, GL, et al. Spread of SARS-CoV-2 in the Icelandic population. N Engl J Med. (2020) 382:2302–15. doi: 10.1056/NEJMoa2006100
18. Popa, A, Genger, JW, Nicholson, MD, Penz, T, Schmid, D, Aberle, SW, et al. Genomic epidemiology of superspreading events in Austria reveals mutational dynamics and transmission properties of SARS-CoV-2. Sci Transl Med. (2020) 12:2555. doi: 10.1126/scitranslmed.abe2555
19. Bluhm, A, Christandl, M, Gesmundo, F, Ravn Klausen, F, Mančinska, L, Steffan, V, et al. SARS-CoV-2 transmission routes from genetic data: a Danish case study. PLoS One. (2020) 15:e0241405. doi: 10.1371/journal.pone.0241405
20. Hersche, B, Kern, B, Stuber-Berries, N, Rohrer, R, Trkola, A, and Weber, K Management COVID-19-Pandemiie Tirol (Bericht der unabhängigen expertekommission) Land Tirol (2020)
21. Pollak, M., Kowarz, N., and Partheymüller, J., (2020). Chronology of the Corona crisis in Austria - part 2: From the first easing of measures towards restoring normality, U.o.V. Austrian Corona Panel Project, Editor.
22. Hale, T, Angrist, N, Goldszmidt, R, Kira, B, Petherick, A, Phillips, T, et al. A global panel database of pandemic policies (Oxford COVID-19 government response tracker). Nat Hum Behav. (2021) 5:529–38. doi: 10.1038/s41562-021-01079-8
23. Borena, W, Bánki, W, Bates, K, Winner, H, Riepler, L, Rössler, A, et al. “Persistence of immunity to SARS-CoV-2 over time in the ski resort Ischgl.” eBioMedicine. (2021) 70. doi: 10.1016/j.ebiom.2021.103534
24. Ahmad, F, Jhajj, AK, Stewart, DE, Burghardt, M, and Bierman, AS. Single item measures of self-rated mental health: a scoping review. BMC Health Serv Res. (2014) 14:398. doi: 10.1186/1472-6963-14-398
25. Baćak, V, and Ólafsdóttir, S. Gender and validity of self-rated health in nineteen European countries. Scand J Public Health. (2017) 45:647–53. doi: 10.1177/1403494817717405
26. Knabl, L, Mitra, T, Kimpel, J, Rössler, A, Volland, A, Walser, A, et al. “High SARS-CoV-2 Seroprevalence in children and adults in the Austrian ski resort Ischgl.” Commun. Med.. (2021) 1:4. doi: 10.1038/s43856-021-00007-1
28. Lüdecke, D, and von dem Knesebeck, O. Worsened self-rated health in the course of the COVID-19 pandemic among older adults in Europe. Eur J Pub Health. (2023) 33:1148–54. doi: 10.1093/eurpub/ckad143
29. Stephanie, S, Trott, M, Tully, M, Shin, J, Barnett, Y, Butler, L, et al. Changes in physical activity and sedentary behaviours from before to during the COVID-19 pandemic lockdown: a systematic review. BMJ Open Sport Exerc Med. (2021) 7:e000960. doi: 10.1136/bmjsem-2020-000960
30. Gestsdottir, S, Gisladottir, T, Stefansdottir, R, Johannsson, E, Jakobsdottir, G, and Rognvaldsdottir, V. Health and well-being of university students before and during COVID-19 pandemic: a gender comparison. PLoS One. (2021) 16:e0261346. doi: 10.1371/journal.pone.0261346
32. Dragano, N, Reuter, M, Peters, A, Engels, M, Schmidt, B, Greiser, KH, et al. “Zunahme psychischer Störungen während der COVID-19-Pandemie – die Rolle beruflicher und finanzieller Belastungen”. Dtsch Arztebl Int. (2022) 119:179–87. doi: 10.3238/arztebl.m2022.0133
33. Dale, R, Budimir, S, Probst, T, Humer, E, and Pieh, C. Quality of life during the COVID-19 pandemic in Austria. Front Psychol. (2022) 13:934253. doi: 10.3389/fpsyg.2022.934253
34. Mendez-Lopez, A, Stuckler, D, McKee, M, Semenza, JC, and Lazarus, JV. The mental health crisis during the COVID-19 pandemic in older adults and the role of physical distancing interventions and social protection measures in 26 European countries. SSM - Popul Health. (2022) 17:101017. doi: 10.1016/j.ssmph.2021.101017
35. Viertiö, S, Kiviruusu, O, Piirtola, M, Kaprio, J, Korhonen, T, Marttunen, M, et al. Factors contributing to psychological distress in the working population, with a special reference to gender difference. BMC Public Health. (2021) 21:611. doi: 10.1186/s12889-021-10560-y
36. Wels, J, and Hamarat, N. A shift in women’s health? Older workers’ self-reported health and employment settings during the COVID-19 pandemic. Eur J Pub Health. (2022) 32:80–6. doi: 10.1093/eurpub/ckab204
Keywords: self-reported health, SARS-CoV-2 infection, pandemic (COVID-19), mental health, physical health, economic impacts, behaviour
Citation: Bates K, Borena W, McKee M, Hayek L, Bouanchaud P, Bánki Z, Riepler L, Rössler A, Falkensammer B, Paetzold J, Walser A, Schönherr S, Forer L, Knabl L, Kimpel J, von Laer D and Ulmer H (2025) Changes in self-reported physical and mental health, behaviour and economic status among adults by known seropositivity and sociodemographic factors before and after the COVID-19 pandemic outbreak in Ischgl, Austria. Front. Public Health. 13:1488108. doi: 10.3389/fpubh.2025.1488108
Edited by:
Cyrille Delpierre, INSERM Public Health, FranceReviewed by:
Birute Strukcinskiene, Klaipėda University, LithuaniaCopyright © 2025 Bates, Borena, McKee, Hayek, Bouanchaud, Bánki, Riepler, Rössler, Falkensammer, Paetzold, Walser, Schönherr, Forer, Knabl, Kimpel, von Laer and Ulmer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hanno Ulmer, aGFubm8udWxtZXJAaS1tZWQuYWMuYXQ=; Wegene Borena, d2VnZW5lLmJvcmVuYUBpLW1lZC5hYy5hdA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.