 Jinsu Yang†
Jinsu Yang† Yuming Shang
Yuming Shang Fengxiao Cao
Fengxiao Cao Huaze Ying
Huaze Ying
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
HYPOTHESIS AND THEORY article
Front. Public Health, 31 March 2025
Sec. Aging and Public Health
Volume 13 - 2025 | https://doi.org/10.3389/fpubh.2025.1478337
This article is part of the Research TopicUrban AgingView all articles
Background: The global ageing population is increasing. As their physical functions deteriorate, older adults face not only physical health challenges but also mental health issues. Enhancing the health status of older adults is imperative to improve their quality of life. However, research on the health status of older adults living in the community is limited, and the association between the built environment and daily activities remains largely unexplored.
Objective: This study aimed to utilize structural equation modeling to (1) explore the interrelationships between the community built environment, daily activities of older adults, and their health, and (2) examine the interrelationships among their correlates.
Methods: For data collection, this study administered structured questionnaires to 494 community-dwelling older adults across ten representative urban communities in Fuzhou, China. The questionnaire comprised four validated sections: demographic characteristics, perceived community built environment features, daily activity and health outcomes. Data analysis employed structural equation modeling (SEM) using AMOS 27.0, with SPSS 27.0 for preliminary analyses, to examine both direct effects of built environment on health outcomes and indirect effects mediated through daily activities.
Results: Structural equation modeling revealed three pathways: Path 1 (community built environment →health of older adults), Path 2 (community built environment → daily exercise for older adults), and Path 3 (daily exercise for older adults →health of older adults). All three pathways were supported, indicating interaction among the factors.
Conclusion: The health status of older adults is influenced by their living environment and daily activities. An improved community built environment can enhance health status among older adults. Furthermore, daily activities serve as partial mediators between community built environments and health outcomes. Our methodology and findings offer valuable insights for optimizing community built environments to promote the health of older adults.
Population aging has emerged as a critical global public health issue and a shared challenge for all countries and regions in the 21st century (1). According to the National Bureau of Statistics of China, the country experienced its first instance of negative population growth in 2022, signifying its official entry into an era of sustained population decline. This demographic shift is accompanied by an increasing degree of aging, exacerbating associated social and public health concerns.
As physiological functions naturally decline with age, health challenges have become a central focus of aging-related issues in China (2, 3). Given that the majority of older adults’ daily activities occur within their residential communities, the built environment of these communities profoundly influences not only their activities but also their overall health status (4). Therefore, investigating the relationship between community built environments and the health of older adults is essential for developing strategies to enhance their well-being.
The World Health Organization (WHO) defines health as a state of complete physical, mental, and social well-being, rather than merely the absence of disease or infirmity (5). Existing research underscores the significant impact of community built environments and daily activities on both the physical and mental health of older residents (6–9). Accordingly, this study conceptualizes health as encompassing both physical and mental health.
Numerous studies have demonstrated that the community built environment significantly affects the health outcomes of older adults (10, 11). First, the high accessibility of community facilities—including recreational spaces (12), sports infrastructures (13), health education resources (14), medical service centers (15), older adult care institutions (16), supermarkets (17)—is crucial for promoting daily activity engagement among older adults. This accessibility effectively encourages older adults to engage in daily activities, thereby improving their overall health. Second, well—connected sidewalks and good crossing facilities facilitate active travel, while a convenient public transportation system augments the propensity of older individuals to engage in outdoor activities, thereby exerting a beneficial influence on their physical and mental health (4, 11, 18). Third, the safety of community spatial is crucial for ensuring the well-being of older adults. Safety of the transportation environment (19), pavement quality (20, 21) and noise management (22) in which older adults live can have an impact on their health. Fourth, the safety of community facilities is one of the core needs of older adults, as it is closely linked to their physical and mental health. Comprehensive security measures, such as barrier-free facilities and surveillance systems, further enhance psychological comfort, encourage outdoor activities, and improve overall physical and mental health (23–25). Fifth, exposure to natural landscapes provides considerable health benefits for older adults. Green spaces with high visibility (26, 27), the usual visual corridors, rich blue-green spaces (28, 29), interactive landscape elements (30), and high tree canopy cover all contribute to stress reduction and better health (31). Finally, the comfort of community site spatial environments influences travel behavior and, consequently, health outcomes. Clean and well-maintained streets with street-side resting places and shelters significantly increase older people’s willingness to walk outdoors, which is essential for physical and mental health (12, 23, 28) (Table 1).
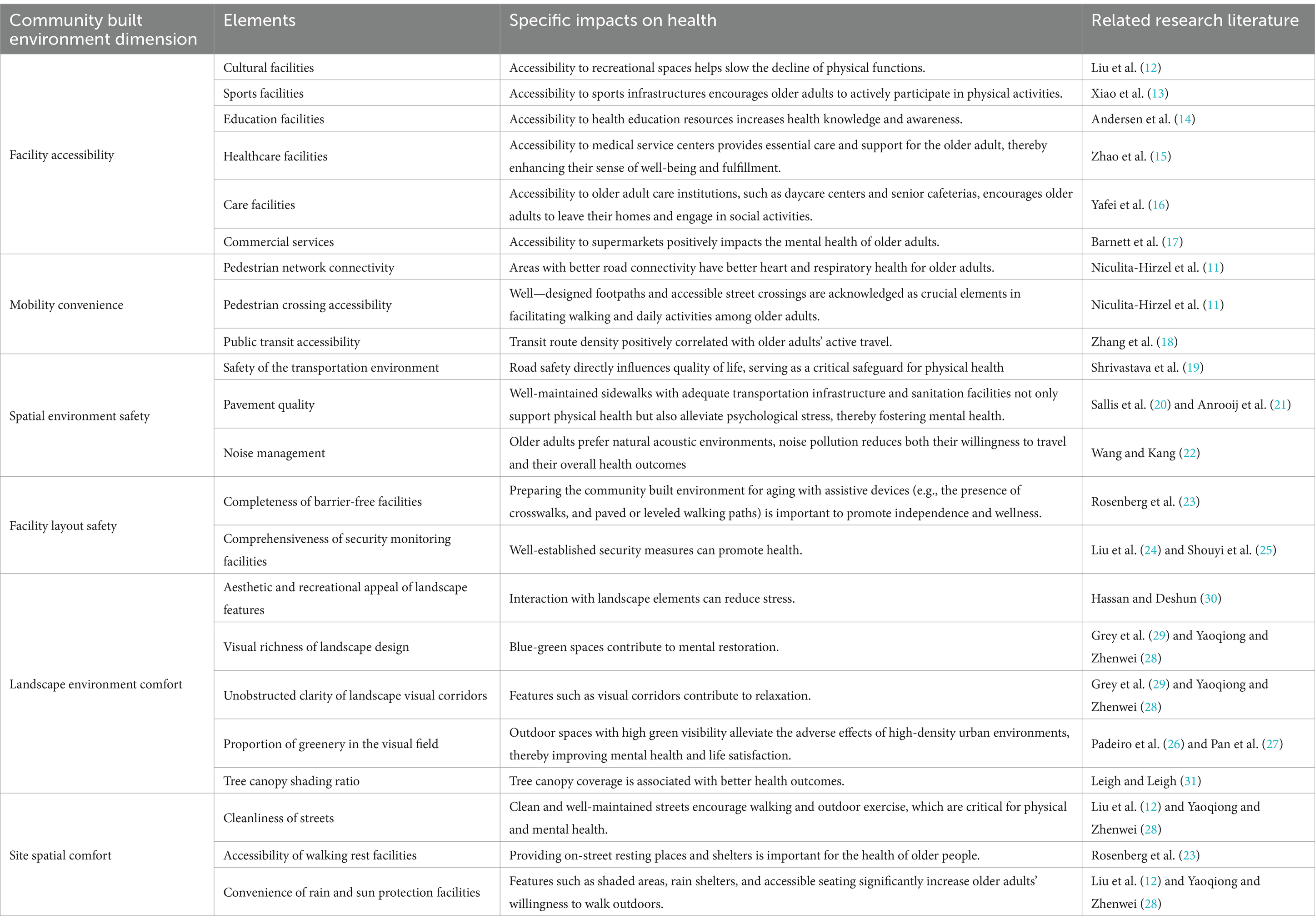
Table 1. Summary of existing research.
Walking and outdoor exercise are two important forms of daily activities for older adults, with profound benefits for their health. Walking, as the most common activity among older adults, offers numerous physical and mental health benefits (32). Regular outdoor activities help prevent functional decline and promote mental health (33–35). Aerobic exercise, in particular, has been shown to mitigate mild cognitive impairment and delay cognitive deterioration (36, 37). The positive relationship between daily activities and health outcomes in older adults is influenced by factors such as activity frequency, duration, and type (38, 39).
In summary, given the significant aging population in China and the high prevalence of health issues among older adults—combined with their substantial reliance on community built environments for daily activities—there is a critical need to address the activity-related needs of older adults to enhance their health and well-being. This enhancement is essential for improving quality of life and life satisfaction among older adults.
Although prior studies have examined the link between community environments and older adults’ health, few have adequately explored the relationship between community built environments, older adults’ daily activities, and health outcomes. Thus, this paper introduces daily activities as a mediating variable and employs a structural equation model to investigate the interrelationships among the community built environment, daily activities, and health in older adults. The goal is to identify pathways and mechanisms within these relationships to inform strategic recommendations for community planning and development. The aim of this study is to propose evidence-based decision-making strategies for community planning updates by analyzing the pathways and mechanisms of interactions between variables, thereby promoting the development of age-friendly health communities.
This cross-sectional study employed structural equation modeling (SEM) to analyze data from community-dwelling older adults in Fuzhou, China. The research methodology employed SEM as the primary analytical framework—a sophisticated multivariate statistical technique that integrates confirmatory factor analysis with path analysis to elucidate relationships between observed indicators and latent constructs.
The analytical protocol proceeded through sequential phases of theoretical model construction, systematic data collection, and statistical model fitting. SEM facilitated the simultaneous examination of direct pathways (community built environment → health outcomes) and indirect pathways mediated through daily activities, while accounting for measurement error inherent in psychosocial constructs. This methodological approach enabled precise quantification of parameter estimates for each hypothesized relationship, thereby illuminating the relative magnitude of environmental factors influencing older adults’ health outcomes and the mediating mechanisms through which these effects manifest.
This study provides a thorough review and synthesis of existing literature, organizing the community built environment into six key dimensions: facility accessibility, mobility convenience, spatial environment safety, facility layout safety, landscape environment comfort, and site spatial comfort. Additionally, the daily activities of older adult participants are classified into two primary types: walking and outdoor exercise. Following the ten health standards established by the World Health Organization, older adult health is divided into two categories: physical and mental health. Prior research indicates that the community built environment significantly impacts both the daily activities and overall health of older adults. Furthermore, these daily activities exhibit reciprocal effects on health outcomes. Based on these insights, three hypotheses (H1, H2, and H3) are proposed (Figure 1).
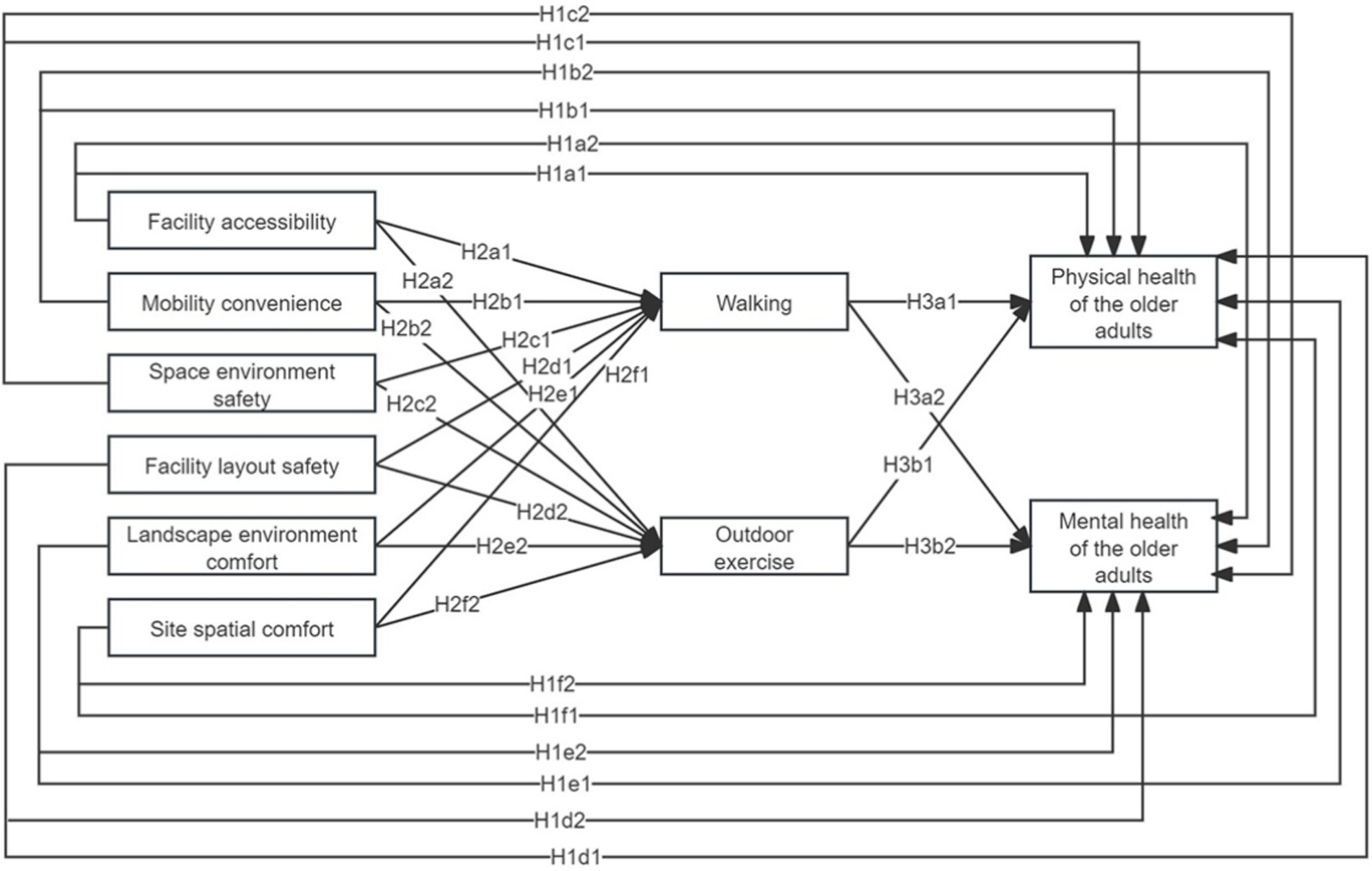
Figure 1. Diagram of the hypothetical model.
H1: The community built environment has a significant direct positive impact on the health of older adults. H1a1 refers to the positive impact of facility accessibility on physical health, H1a2 refers to the positive impact of facility accessibility on mental health. H1b1 refers to the positive impact of mobility convenience on physical health, H1b2 refers to the positive impact of mobility convenience on mental health. H1c1 refers to the positive impact of spatial environmental safety on physical health, and H1c2 refers to the positive impact of spatial environment safety on mental health. H1d1 refers to the positive impact of facility layout safety on physical health, and H1d2 refers to the positive impact of facility layout safety on mental health. H1e1 refers to the positive impact of landscape environment comfort on physical health, and H1e2 refers to the positive impact of landscape environment comfort on mental health. H1f1 refers to the positive impact of site spatial comfort on physical health, and H1f2 refers to the positive impact of site spatial comfort on mental health.
H2: The community built environment has a significant positive impact on daily activities. H2a1 refers to the positive impact of facility accessibility on walking, H2a2 refers to the positive impact of facility accessibility on outdoor exercise. H2b1 refers to the positive impact of mobility convenience on walking, H2b2 refers to the positive impact of mobility convenience on outdoor exercise. H2c1 refers to the positive impact of spatial environmental safety on walking, H2c2 refers to the positive impact of spatial environmental safety on outdoor exercise. H2d1 refers to the positive impact of facility layout safety on walking, H2d2 refers to the positive impact of facility layout safety on outdoor exercise. H2e1 refers to the positive impact of landscape environment comfort on walking, H2e2 refers to the positive impact of landscape environment comfort on outdoor exercise. H2f1 refers to the positive impact of positive impact of site spatial comfort on walking; H2f2 refers to the positive impact of site spatial comfort on outdoor exercise.
H3: Daily activities have a significant positive impact on the health of older adults. H3a1 refers to the positive impact of walking on physical health, H3a2 refers to the positive impact of walking on mental health. H3b1 refers to the positive impact of outdoor exercise on physical health, H3b2 refers to the positive impact of outdoor exercise on mental health.
Fuzhou presents a compelling study area due to the pronounced conflict between high-density urban development and the urgent need for a healthy living environment for older adults within the community. The city’s unique geography, bordered by mountains on three sides and the sea on the fourth, creates a spatial configuration that simultaneously acts as a natural barrier and limits urban expansion. Fuzhou is currently undergoing a process of integrated development, resulting in constrained land availability for urban growth and a reduction in accessible living space for older adults. Moreover, in recent years, the Fuzhou municipal government has actively promoted the establishment of pedestrian-oriented urban systems and recreational spaces designed to support the health and mobility of older adults. Initiatives such as the creation of urban ecological trails, exemplified by the Jinniu Mountain Fudao, are not only supported by the government but also foster an environment conducive to community health and wellness.
Consequently, three urban districts in Fuzhou City—Gulou District, Taijiang District, and Jinan District—were selected as the study area. When selecting sample communities, communities that met the following three criteria were identified based on the evidence—based principles of gerontology and urban planning studies: a senior population exceeding 15% (40), the presence of a service station within the community (41), and at least one park located within 500 meters of the community (GB 50180–2018) (42, 43). This selection was informed by various factors, including the community support provided by the community council. Utilizing Baidu heat maps and on-site validation, twelve neighborhoods with high pedestrian traffic were identified as sample neighborhoods (Figure 2).
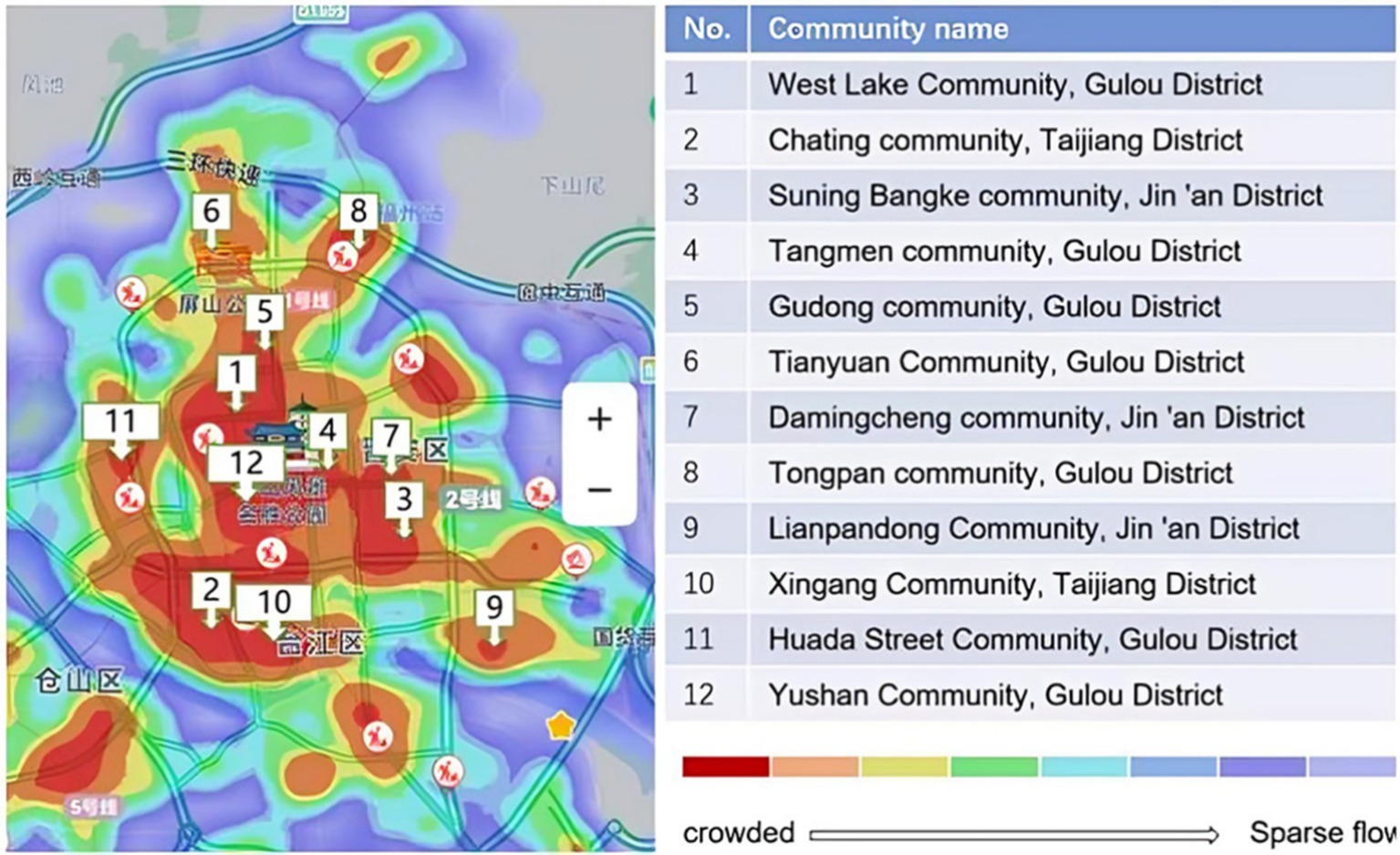
Figure 2. Heat map of sample neighborhoods.
The data obtained in this study were combined with data from preliminary research conducted for a settlement planning course in the urban and rural planning program at the College of Architecture and Urban Planning, Fujian University of Technology. The participants in the questionnaire survey were second-year undergraduate students (n = 24) of urban and rural planning. The trainers were members of the Fujian Provincial Natural Science Foundation (grant number 2022J05192) and teachers of the settlement planning course in the College of Architecture and Urban Planning, Fujian University of Technology. The trainers provided formal training to the data collectors consisting of three parts (Table 2). Twenty-four trained data collectors were divided into 12 groups to administer the questionnaire to residents of the 12 sample communities.
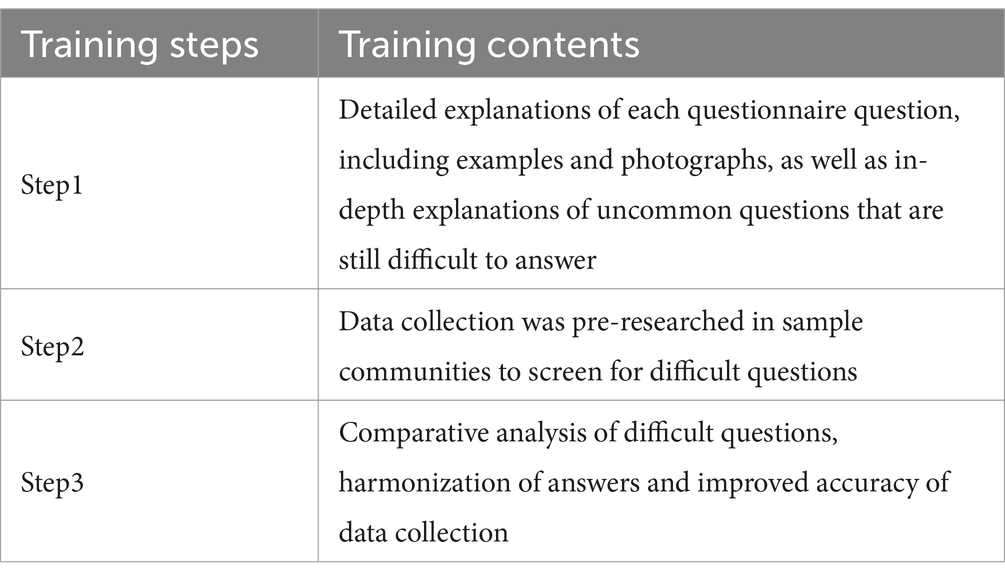
Table 2. Training steps.
The data for this study were categorized into three main areas: the community built environment, daily activities, and the health of older adults. Data collection involved a combination of online and offline questionnaires. A preliminary version of the questionnaire was developed, followed by a pilot study conducted in May 2022. A total of 120 questionnaires were distributed, with ten allocated to each sampled community. Of the distributed questionnaires, fifteen were returned, and 105 were deemed valid. Following the pilot study’s findings, adjustments were made to the questionnaire to include inquiries related to the community built environment, daily activities, and the health of older adults.
The formal questionnaire commenced on September 17, 2022, and was disseminated in the 12 selected communities using a combination of online and offline approaches. The community sampling survey was completed through the steps of preliminary preparation, pilot survey, formal investigation, and data processing (Table 3).
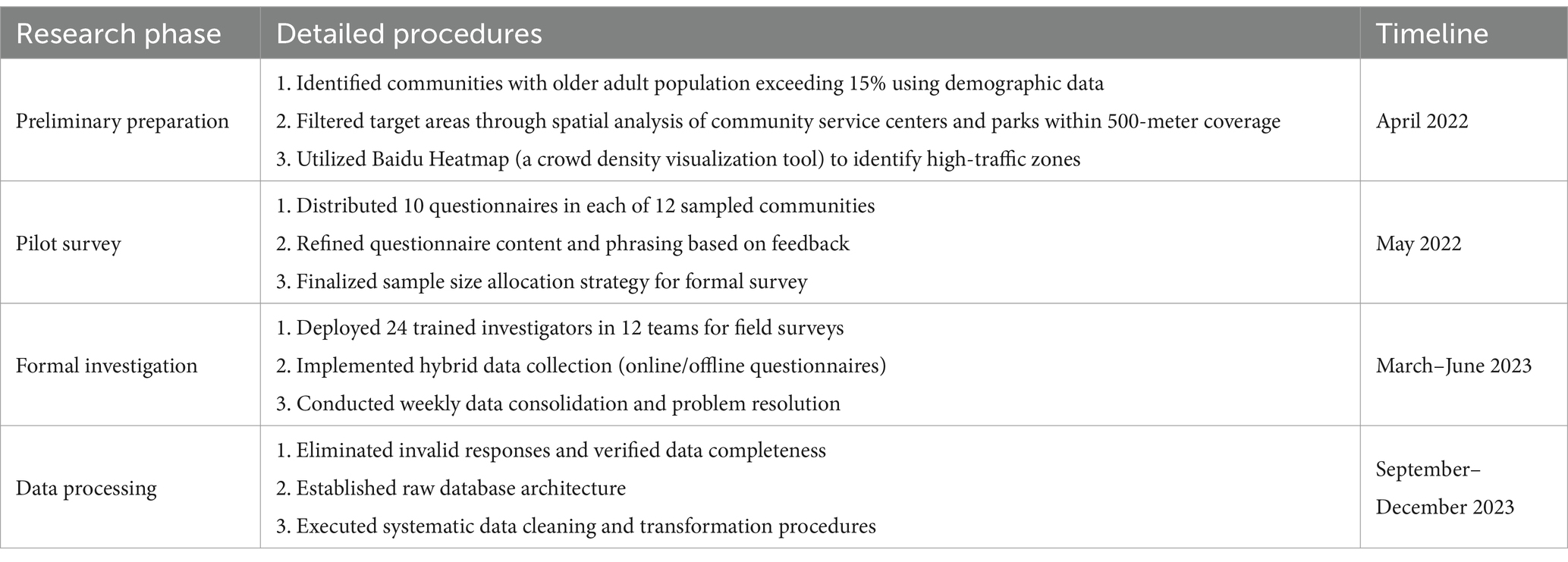
Table 3. Community sampling survey steps.
Older adults in the community were recruited to participate in the study by offering a carton of eggs valued at approximately 6 RMB as an incentive for completing the questionnaire. Upon questionnaire completion, participants received the voucher promptly. Inclusion criteria for participation were: (1) age 60 years or older; (2) permanent residence in the selected communities for at least one year; (3) ability to understand and respond to the questionnaire either independently or with assistance; and (4) willingness to provide informed consent. Exclusion criteria were: (1) severe cognitive impairment preventing reliable response to questionnaires; (2) acute illness or hospitalization during the survey period; (3) inability to communicate effectively; and (4) temporary residents or those who had lived in the community for less than one year (44–46).
The online survey was administered using the questionnaire tool Star1. This platform provided a user-friendly web interface that elaborated on each question option. The offline survey took place in high-traffic areas within the community. Data collectors were tasked with explaining the question options either online or in person. They utilized photo examples to aid older adults in comprehending the questions and accurately completing the questionnaire. In the 12 sample communities, we distributed 595 questionnaires, including 432 online and 163 offline. We collected 494 valid questionnaires, including 356 online and 138 offline (Table 4). The questionnaire recovery validity rate stood at 84.04%, with online recoveries at 82.40% and offline at 84.66%.
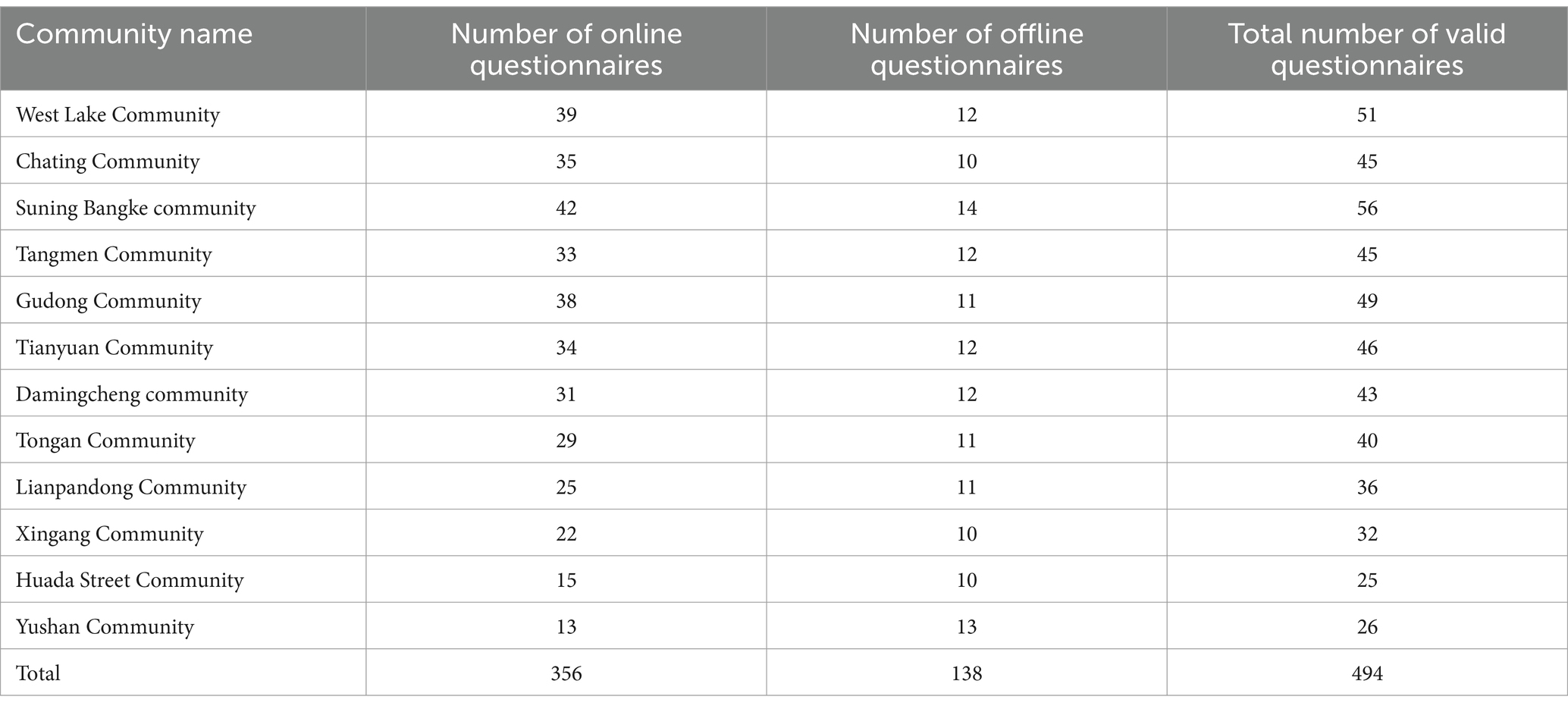
Table 4. Sample distribution in each sample community.
From the perspectives of age, personal economic condition, physical condition and education (47), the statistics are as follows (Table 5).
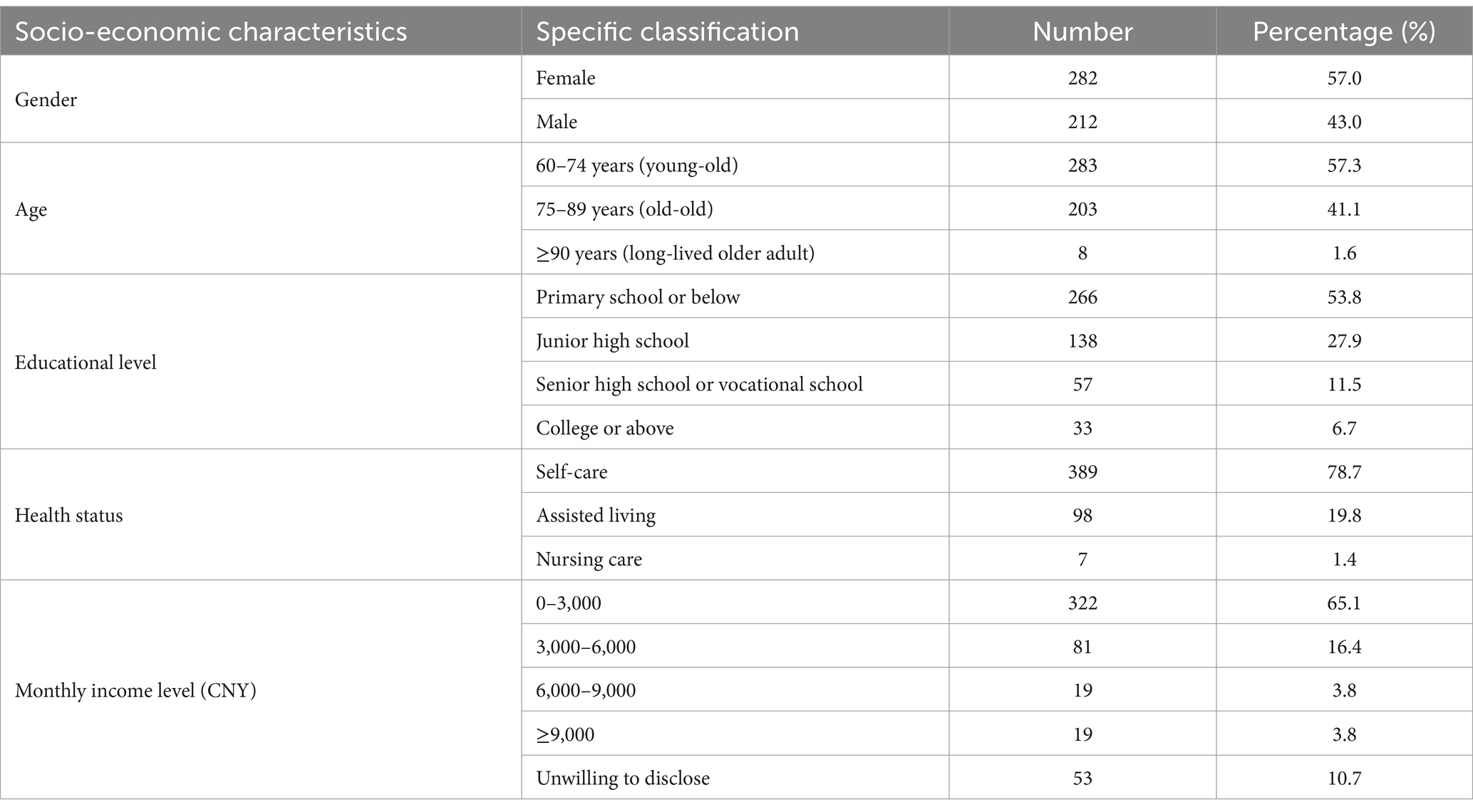
Table 5. Socio-economic characteristics of the older adults (n = 494).
For facility accessibility, the existing literature underscores the importance of accessibility to various facilities—such as cultural, sports, educational, healthcare, and commercial services—for older adults. For mobility convenience, the literature has examined the impact of pedestrian network connectivity, pedestrian crossing accessibility, and public transit accessibility on the well-being of older adults. The accessibility of entrances and exits is important for older adult residents traveling long distances, and this paper introduces the accessibility of entrances and exits into the study. Regarding the safety of the spatial environment, the literature has examined the safety of transportation environment, pavement quality, and the impact of noise on older adults. Concerning facility layout safety, studies have investigated the effects of barrier-free facilities and security monitoring. Interviews revealed that older adults often have the habit of walking after meals and express concerns about sudden health issues; thus, attention must be given to the coverage of nighttime lighting and the accessibility of emergency rescue systems. For the comfort of the landscape environment, the literature identifies several factors, including the ease of landscape vignettes, visual richness, corridor smoothness, green visibility, and tree shading rates. In terms of site spatial comfort, existing research has focused on the impacts of street cleanliness and the convenience of walking rest facilities, as well as the availability of rain and shade structures. Interviews indicated that a diverse range of functions along the street façade attracts older adults to go out, prompting this paper to introduce research on the functional richness of street facades. The community built environment data collection was based on six main dimensions (Table 6). Respondents were asked to evaluate the strengths and weaknesses of each factor on a five-point scale (1 = very poor, 2 = poor, 3 = normal, 4 = good, 5 = very good).
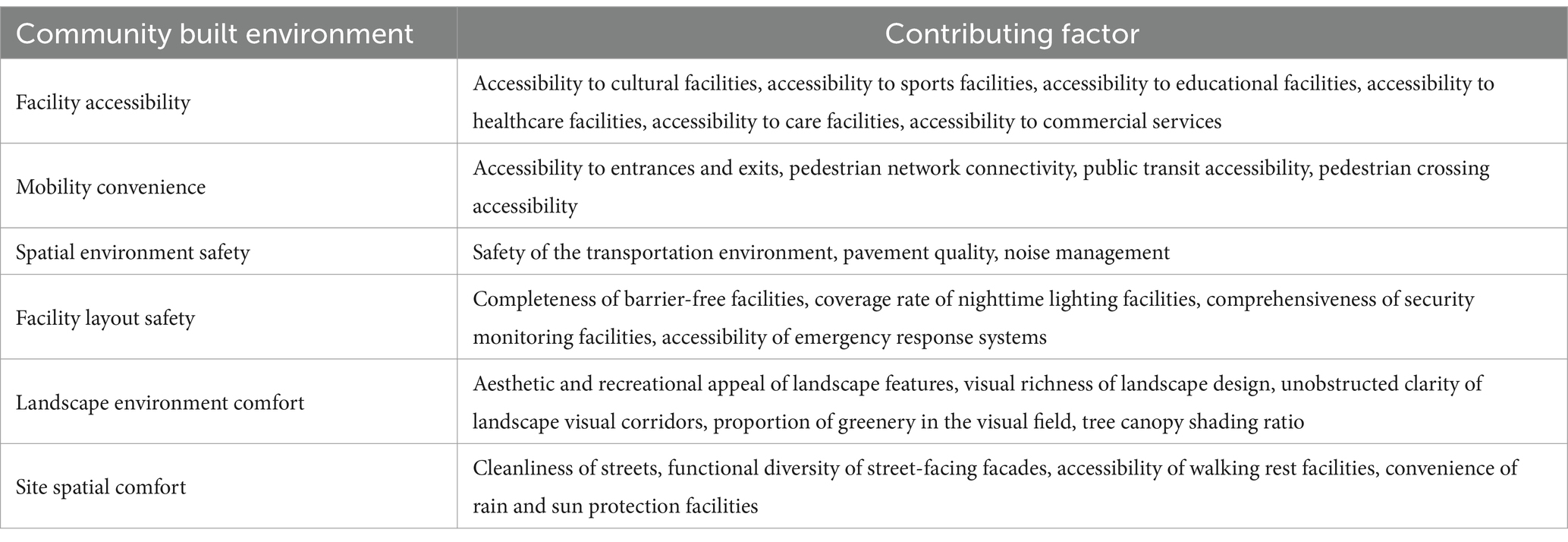
Table 6. Community built environment data collection.
Based on the aforementioned literature review, daily activities included walking and outdoor exercise, categorized by types of activities, daily frequency, and duration of each session (Table 7). Respondents were asked to select the duration of their participation (1 = 0–5 min per day, 2 = 5–15 min per day, 3 = 15–30 min per day, 4 = 30–60 min per day, 5 = 60 min per day and above).
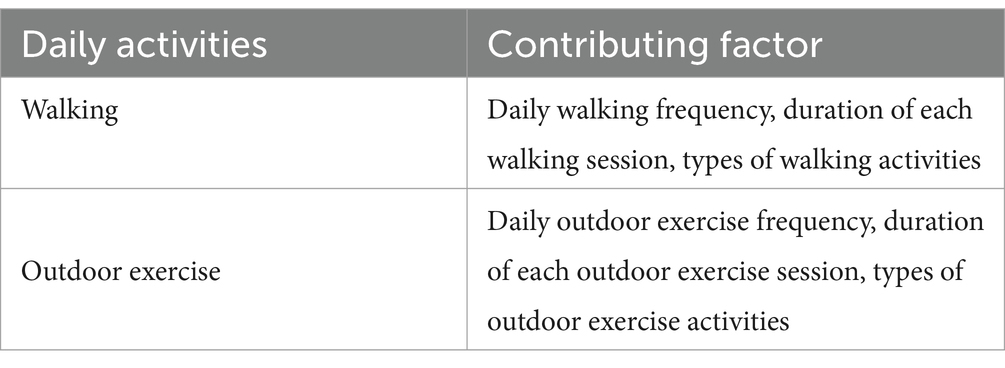
Table 7. Daily activities data collection.
According to the literature review, ease of mobility, quality of sleep, dietary habits, and chronic health conditions are associated with physical health (48–51), while cognitive health, emotional health, happiness and satisfaction, and psychological resilience are related to mental health (52–55) (Table 8). Consequently, the relevant factors pertaining to the health of the older adult have been summarized. Participants were requested to evaluate their physical condition (Table 9).
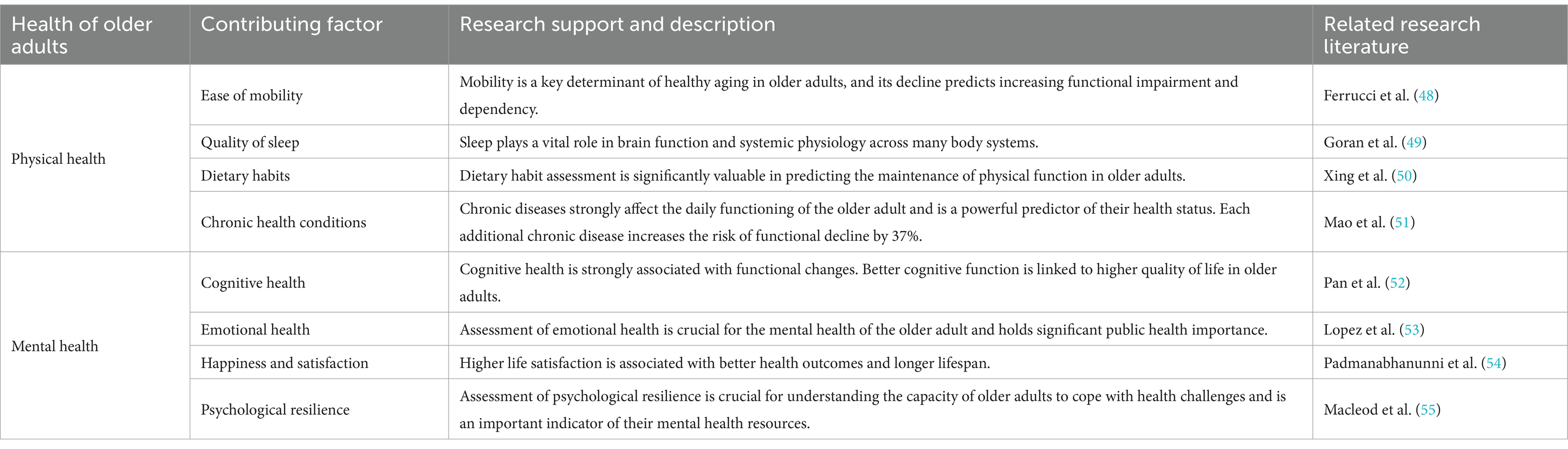
Table 8. Contributing factors to health of older adults and supporting research.
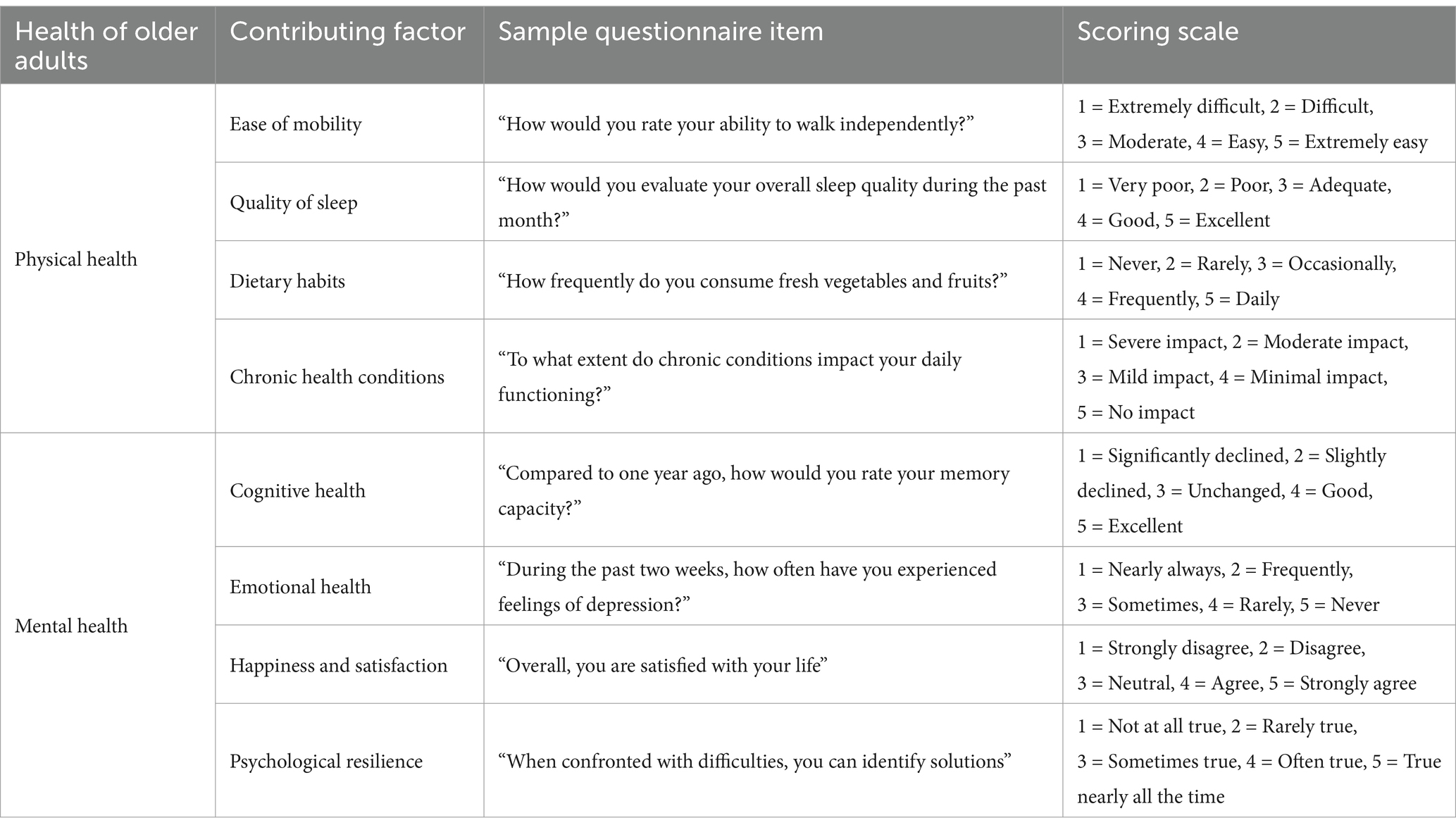
Table 9. Questionnaire items and scoring scales for health of older adults assessment.
Likert scales were employed to evaluate the data. Latent variables, including facility accessibility, mobility convenience, spatial environment safety, facility layout safety, landscape environment comfort, site spatial comfort, walking, outdoor exercise, and both physical and mental health, were considered, with their corresponding factors treated as observed variables (Table 10). These variables were inputted into SPSS 27.0 and AMOS 27.0 statistical software for structural equation modeling analysis.
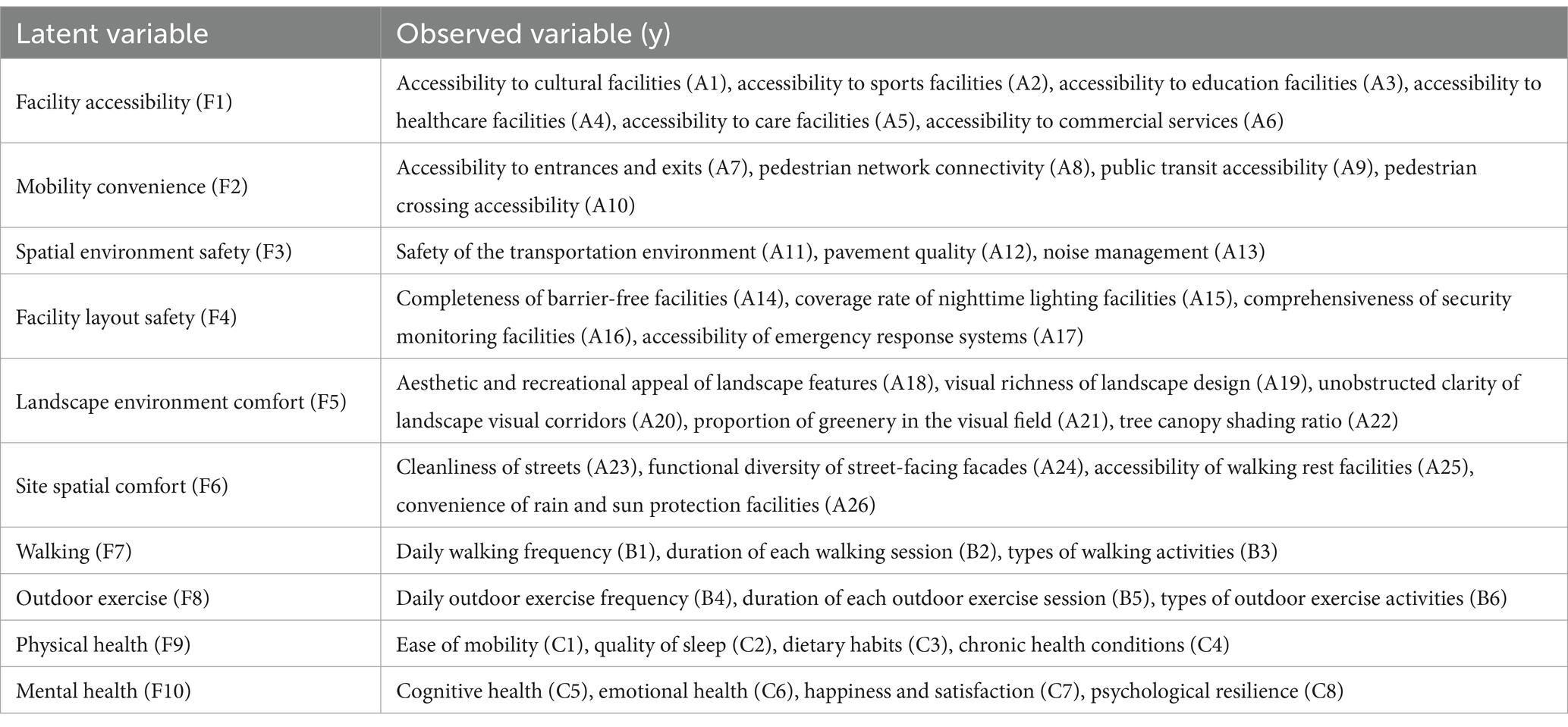
Table 10. Latent and observed variables.
Data analysis for reliability and validity was conducted using SPSS version 27.0. The study focused on assessing the reliability and validity of the grade level variables in the questionnaire. Reliability testing involved Cronbach’s alpha analysis and modified item-total correlation (CITC) analysis.
The results indicated a Cronbach’s alpha coefficient of 0.904 for the overall data, with coefficients above 0.8 for both latent and observed variables (56). The item correlation coefficients all exceeded 0.50, indicating strong relationships between variables and confirming good reliability according to established guidelines (57). Validity assessment utilized the KMO (Kaiser-Meyer-Olkin) test and Bartlett’s test of sphericity. The KMO value was 0.910, well above the 0.80 threshold considered “meritorious” for factor analysis (58). Additionally, Bartlett’s test of sphericity was statistically significant (p ≤ 0.001) (59).
Model testing and analysis were conducted subsequently. The study data underwent analysis utilizing AMOS software, and model testing was executed employing the maximum likelihood estimation (MLE) method for the estimation of model parameters. The chi-square degrees of freedom ratio (χ/df), goodness-of-fit index (GFI), root mean square error of approximation (RMSEA), comparative fit index (CFI), normal fit index (NFI), and adjusted GFI (AGFI) were utilized to assess the model fit (Table 11). The findings indicated that all the indices satisfied the standard range criteria, signifying a good fit and an ideal model.
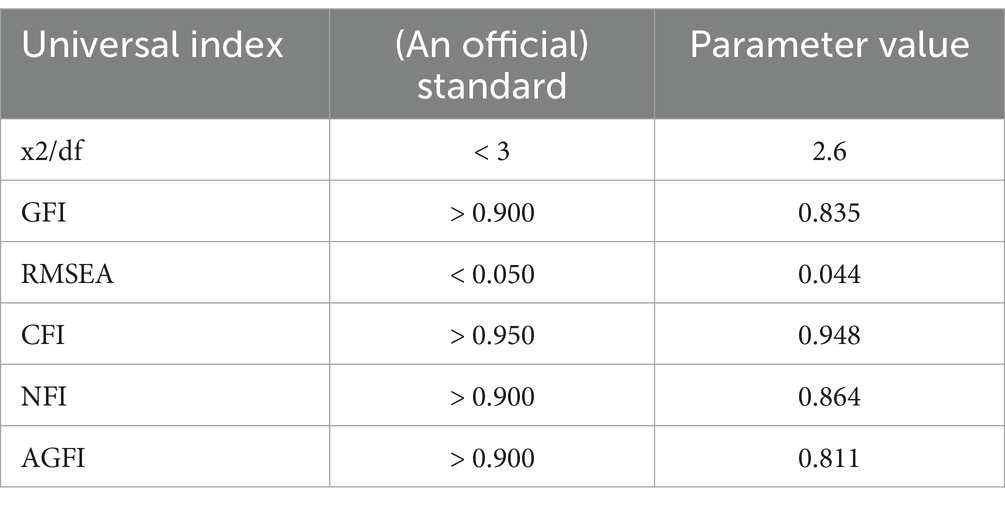
Table 11. Fitting index of the model.
Standardized path coefficients were examined for both observed and latent variables within the community health support environment. The results were statistically significant (p ≤ 0.05). All primary paths were statistically significant.
The findings from the structural equation modeling analysis indicated that all proposed hypothetical models were accepted (Figure 3).
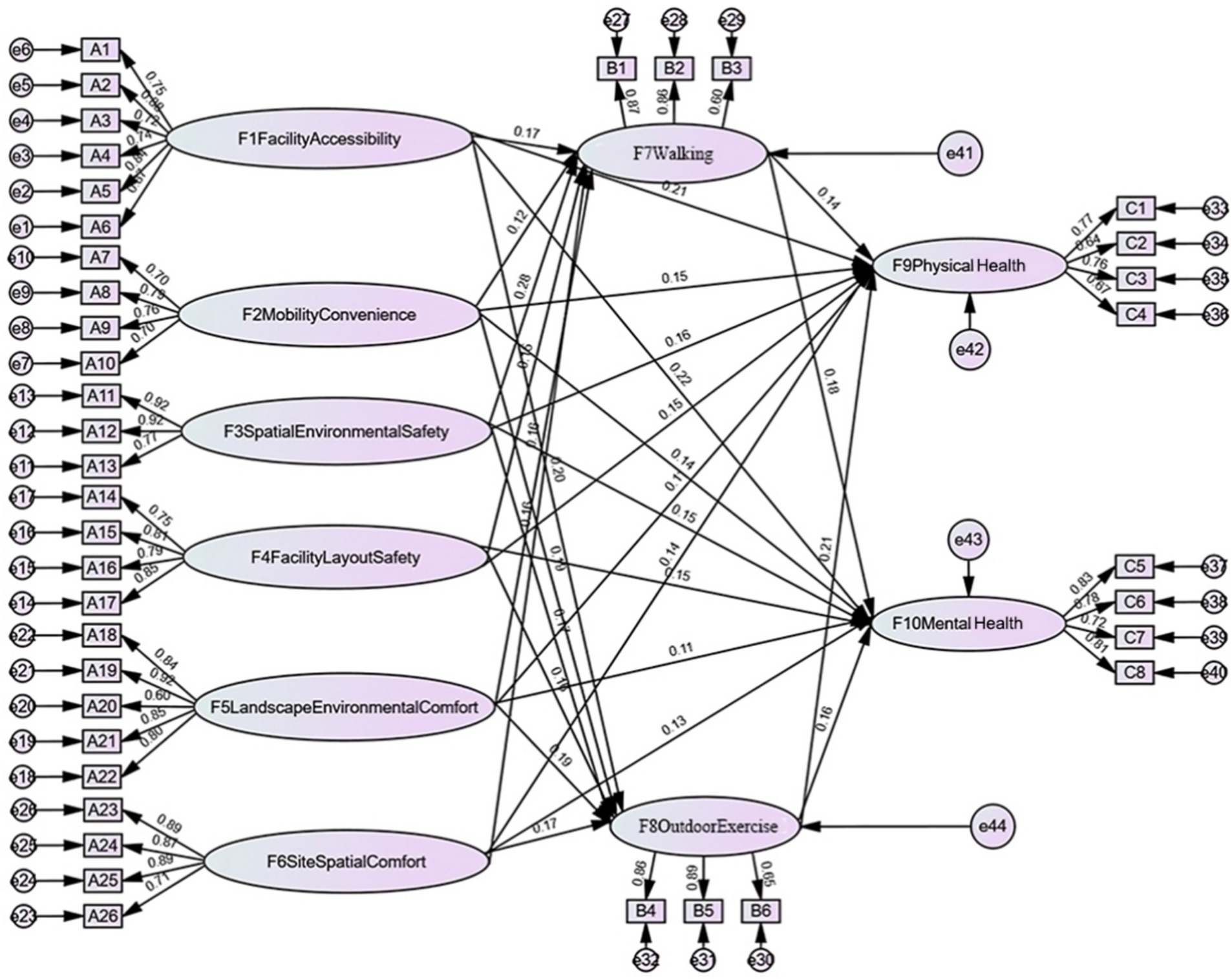
Figure 3. Pathways of influence of community built environment, daily activities and health of older adults.
The findings indicate that the research hypothesis models H1a1, H1a2, H1b1, H1b2, H1c1, H1c2, H1d1, H1d2, H1e1, H1e2, H1f1, and H1f2 (Figures 1, 3) were supported. The community built environment was shown to have a significant direct impact on the physical and mental health of older adults (Table 12). Among these factors, facility accessibility exerted the greatest combined impact on older adult health (effect coefficient: 0.43). This encompassed direct effects on physical health (impact coefficient: 0.21) and mental health (impact coefficient: 0.22). High-quality facility accessibility enables older adults to participate more conveniently in cultural and sports activities and healthcare services, thereby effectively delaying chronic diseases and enhancing well-being. The safety of spatial environment and the safety of facility layout, also significantly affect the health of older adults (combined impact coefficients of 0.31 and 0.30, respectively). Safety reduces the risk of falls and transportation accidents, providing an important safeguard for the physical and mental health of the older adults.
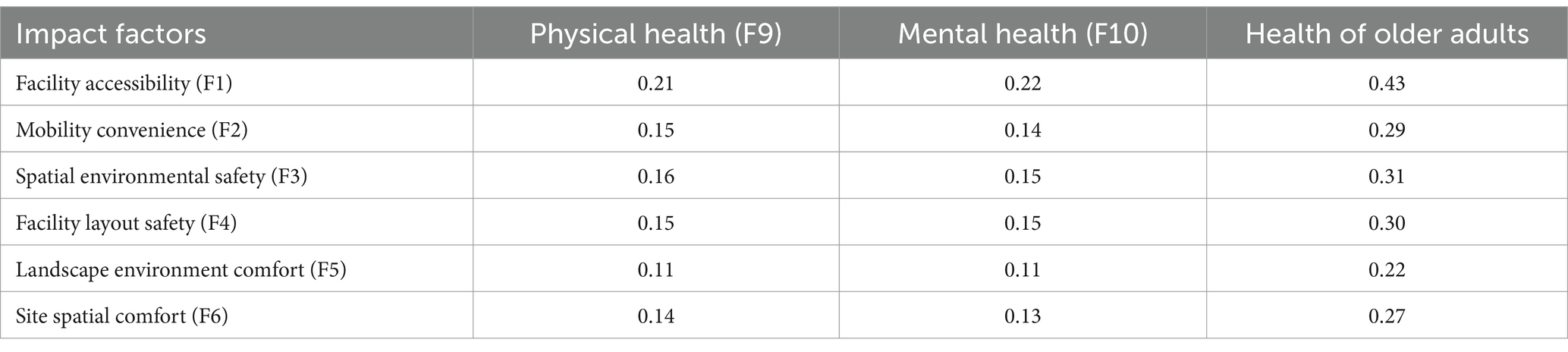
Table 12. Coefficient of direct effect of community built environment on health of older adults.
The hypothetical models H2a1, H2a2, H2b1, H2b2, H2c1, H2c2, H2d1, H2d2, H2e1, H2e2, H2f1, and H2f2 were validated (Figures 1, 3). Key factors of the built environment—including facility accessibility, mobility convenience, spatial environmental safety, facility layout safety, landscape environmental comfort, and site spatial comfort—were found to have significant positive effects on walking and outdoor exercise (Table 13). Among these factors, spatial environmental safety had the most pronounced impact on daily activities (impact coefficient: 0.45), Walking was particularly affected by the safety of the spatial environment (impact coefficient of 0.28). Facility accessibility had the most significant impact on outdoor activities (impact coefficient of 0.20). This result suggests that optimizing the built environment of a community can significantly improve the quality of daily activities for older adults.
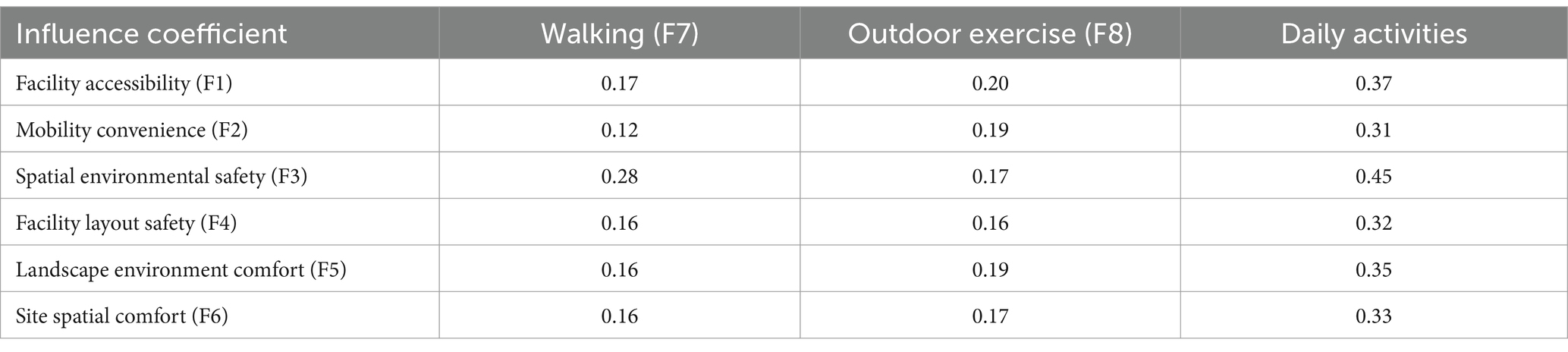
Table 13. The influence coefficient of community built environment on daily activities.
Hypothesized models H3a1, H3a2, H3b1 and H3b2 were supported (Figures 1, 3). Daily activities played a crucial mediating role between the community built environment and the health of older adults (Table 14). Walking was particularly effective in enhancing mental health (impact coefficient of 0.18), and outdoor exercise emerged as the strongest contributor to physical health (impact coefficient of 0.21). These findings suggest that both physical and mental health can be significantly improved by enhancing the community built environment to promote daily activities among older adults.
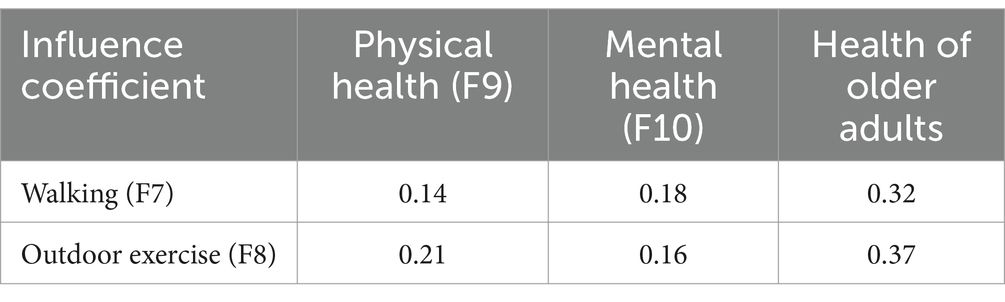
Table 14. The influence coefficient of daily activities on health of older adults.
Among the three observed variables of walking the frequency of daily walking and the duration of each walking had the most significant impact on the health of older adults (Table 15). In community planning, it is essential to arrange suitable activity sites and prioritize the construction of community walking paths to enhance the walking environment. Among the additional three activity variables observed, daily outdoor exercise frequency and daily outdoor exercise time had the greatest influence on the health of older adults (Table 16). Community planning should focus on improving exercise areas and equipment to the fullest extent possible.
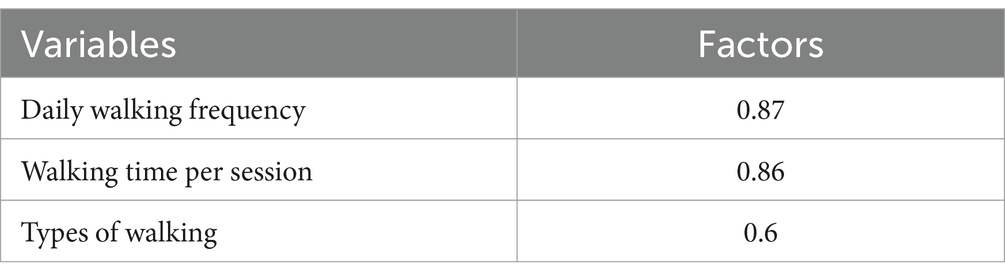
Table 15. Factors influencing walking.
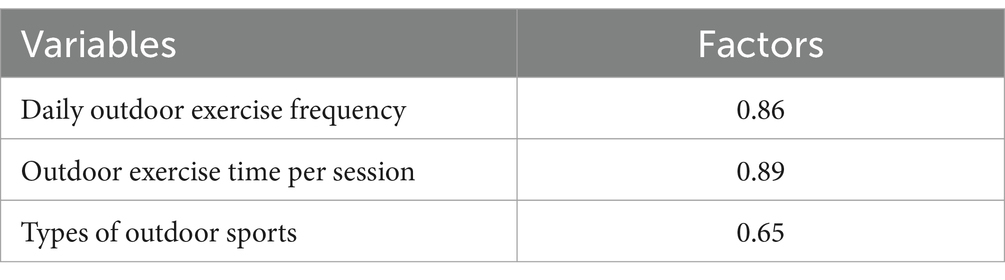
Table 16. Factors influencing outdoor exercise.
The community built environment indirectly influences the health of older adults through daily activities (Table 17). These daily activities play a crucial mediating role in the relationship between the community built environment and the health of older adults. Facility accessibility indirectly affects physical health (0.0658 [0.17*0.14 + 0.20*0.21]) and mental health (0.0626 [0.17*0.18 + 0.20*0.16]) through walking and outdoor exercise. Mobility convenience indirectly affects physical health (0.0567 [0.12*0.14 + 0.19*0.21]) and mental health (0.052 [0.12*0.18 + 0.19*0.16]) through walking and outdoor exercise. Spatial environment safety indirectly affects physical health (0.0749 [0.28*0.14 + 0.17*0.21]) and mental health (0.0776 [0.28*0.18 + 0.17*0.16]) through walking and outdoor exercise. Facility layout safety indirectly affects physical health (0.056 [0.16*0.14 + 0.16*0.21]) and mental health (0.0544 [0.16*0.18 + 0.16*0.16]) through walking and outdoor exercise. Landscape environmental comfort indirectly affects physical health (0.0623 [0.16*0.14 + 0.19*0.21]) and mental health (0.0592 [0.16*0.18 + 0.19*0.16]) through walking and outdoor exercise. Site spatial comfort indirectly affects physical health (0.0581 [0.16*0.14 + 0.17*0.21]) and mental health (0.056 [0.16*0.18 + 0.17*0.16]) through walking and outdoor exercise. Overall, spatial environmental safety had the strongest mediating effect in indirectly promoting the health of older residents.
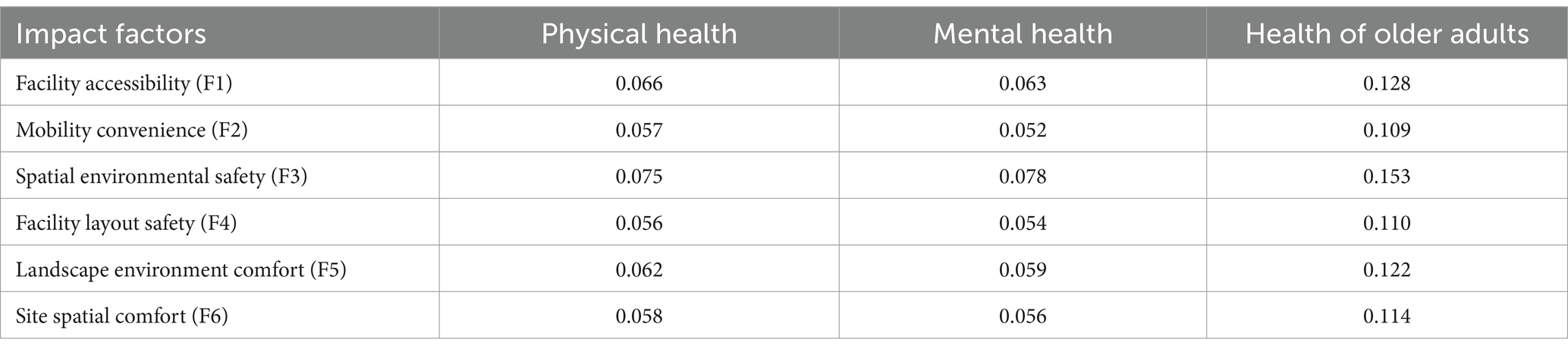
Table 17. Coefficient of indirect effect of community built environment on health of older adults.
The relationship between the community built environment and the health of older adults can be interpreted through a social-ecological theory, which posits that health outcomes emerge from dynamic interactions across multiple levels, including individual behaviors, community resources, and broader environmental contexts (60, 61). Our findings align with this framework, revealing that the built environment serves as a critical meso-level system that both directly shapes health and indirectly facilitates health-promoting behaviors through daily activities. These direct and indirect impacts together constitute the overall influence of the community built environment on the health of older adults (Table 18).
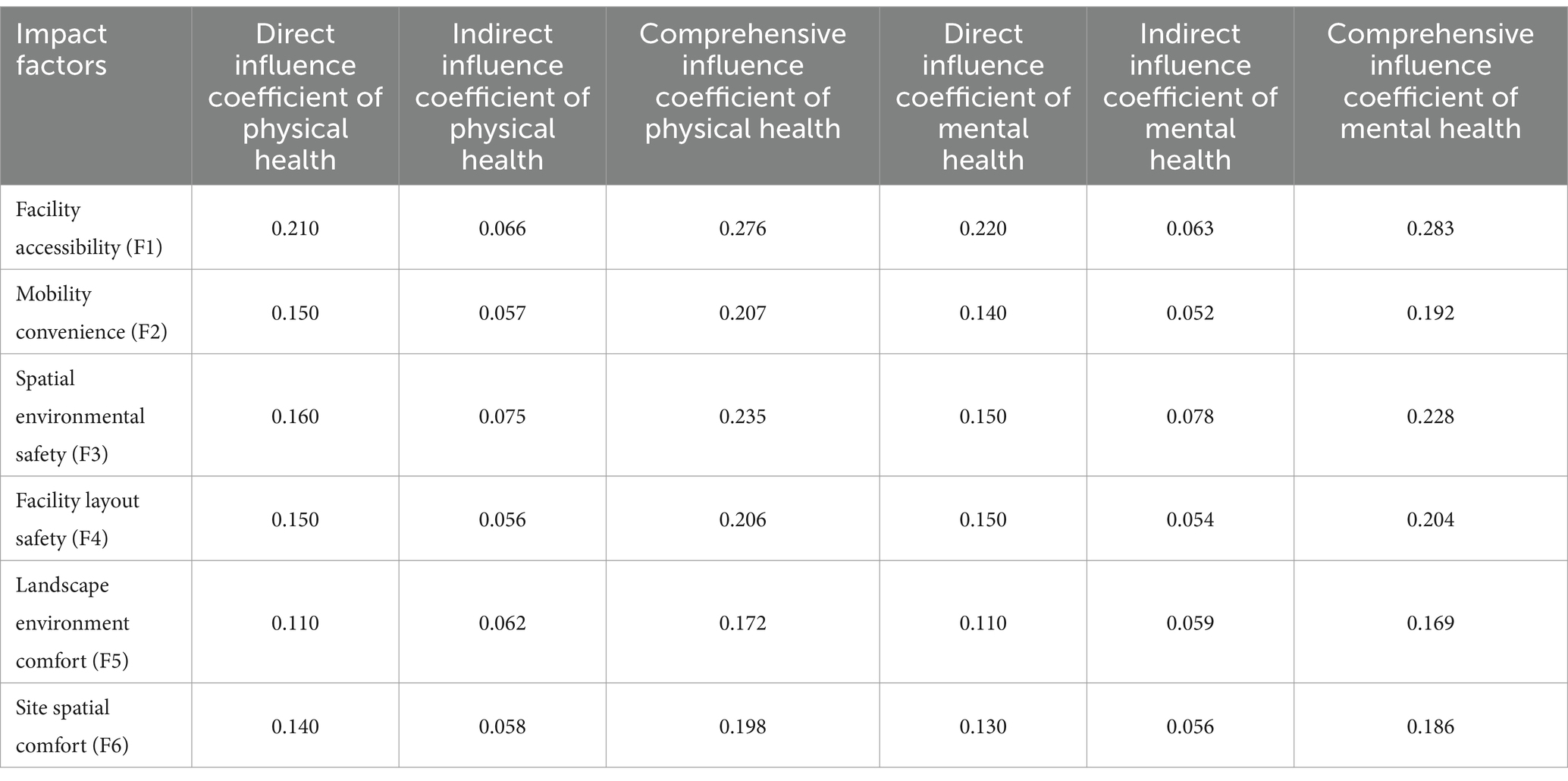
Table 18. Coefficient of influence of the community built environment on the health of older adults.
The combined impact coefficient of facility accessibility on the health of older adults is 0.5584, comprising a coefficient of 0.2758 for physical health and 0.2826 for mental health. This indicates that a one-unit improvement in facility accessibility corresponds to a 0.5584-unit enhancement in the overall health of older adults. The combined impact coefficient of mobility convenience on the health of older adults is 0.3987, comprising a coefficient of 0.2067 for physical health and 0.192 for mental health. This indicates that a one-unit improvement in mobility convenience results in a 0.3987-unit enhancement in the health of older adults. The combined impact coefficient of spatial environment safety on the health of older adults is 0.4625, comprising coefficients of 0.2349 for physical health and 0.2276 for mental health. This indicates that a one-unit improvement in spatial environment safety leads to a 0.4625-unit enhancement in the health of older adults. The combined impact coefficient of facility layout safety on the health of older adults is 0.4104, with a coefficient of 0.206 for physical health and 0.2044 for mental health. This indicates that a one-unit increase in facility layout safety contributes to a 0.4104-unit enhancement in the health of older adults. The combined impact coefficient of landscape environmental comfort on the health of older adults is 0.3415, comprising coefficients of 0.1723 for physical health and 0.1692 for mental health. This indicates that a one-unit improvement in landscape environmental comfort corresponds to a 0.3415-unit enhancement in the health of older adults. The combined impact coefficient of site spatial comfort on the health of older adults is 0.3841, with coefficients of 0.1981 for physical health and 0.186 for mental health. This indicates that a one-unit improvement in site spatial comfort results in a 0.3841-unit enhancement in the health of older adults (Table 19).
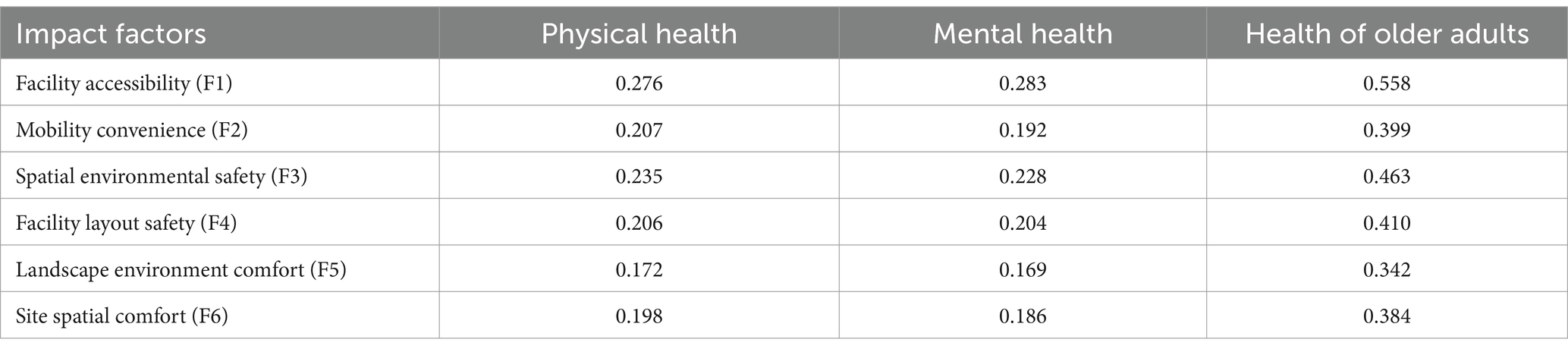
Table 19. Combined impact coefficient of community built environment on the health of older adults.
The findings of the study clearly indicate that the community built environment plays a crucial role in maintaining and enhancing the health of older adults. Facility accessibility is particularly significant for the physical and mental health of older adults and should be a primary focus in community built environment planning. This aligns with previous research emphasizing the role of environmental affordances as a driving force for agency in older adults (62). Emphasis should be placed on optimizing the distribution and functional design of these facilities (63).
In terms of facility accessibility, prioritizing the equitable distribution of amenities is critical to meet the diverse needs of older residents in every building within the community. Establishing centralized older adult activity centers in core areas can function as key hubs, promoting social interaction and enhancing participation in activities.
Regarding mobility convenience, implementing community shuttle services to connect key residential areas with community entrances and exits can significantly improve mobility. Enhancing the internal pedestrian network will boost connectivity, while optimizing bus routes and constructing pedestrian bridges or gently sloped ramps at major crossings can ensure safer and more convenient street crossings for older residents.
For spatial environment safety, measures should prioritize the safety of transportation systems. Installing dividers to separate pedestrian and vehicular traffic, ensuring smooth road surfaces, and maintaining obstacle-free walking paths and activity sites are essential. Additionally, installing noise monitoring devices can help manage and reduce noise pollution effectively.
With respect to the safety of facility layout, improving barrier-free facilities is imperative. Introducing night-time induction lighting systems along walking paths and activity areas can enhance the safety of evening activities. High-definition surveillance systems should be installed in critical locations, such as entrances and activity plazas, to strengthen security. Furthermore, first aid stations or emergency alarm systems should be established in activity venues and along main access routes to ensure rapid response in emergencies.
In terms of landscape environmental comfort, increasing green spaces and flowerbeds can enhance the visual appeal of walking corridors. Small-scale natural interaction points, such as water features or fountains, can create relaxing environments, while designing themed landscape areas can offer diverse recreational opportunities tailored to the preferences of older residents.
For site spatial comfort, installing awnings and pavilions along major roads and rest areas can provide shade and shelter. Benches placed at 200-meter intervals in walking corridors, fitness areas, and public plazas can ensure sufficient resting spaces for older residents during their activities. Additionally, regular cleaning and maintenance of streets and pathways should be undertaken to keep them clear of clutter, prevent haphazard parking, and enhance the overall walking experience.
Particular emphasis should be placed on designing accessible facilities. Increasing the number of small fitness areas and outdoor activity spaces, especially along major walking corridors, ensures equitable access for older adults across different residential zones. The density of community clinics and health education points should also be increased to provide health counseling and basic diagnostic services. Facilities such as daycare centers and community canteens should be conveniently located within community centers and designed with barrier-free access. Small commercial service points, including supermarkets and food markets, should be rationally distributed to ensure accessibility within a 5–10 min walk (Table 20).
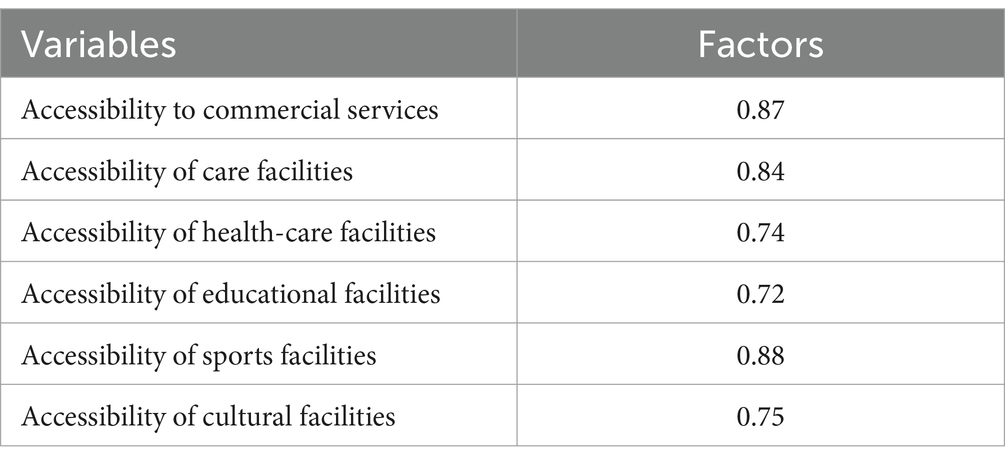
Table 20. Factors influencing facility accessibility.
The mediating effect of daily activities highlights the indirect influence of community design on health outcomes. Outdoor exercise and walking are not only essential forms of community engagement for older adults but also crucial contributors to their overall health. Walking, in particular, has been shown to significantly enhance mental health, while outdoor exercise is particularly effective in improving physical function. These findings indicate that creating suitable activity spaces and pedestrian networks can greatly enhance the health of older adults.
This study collected data through questionnaires; however, this method has limitations, primarily due to the small sample size and the uncertainty associated with relying on a single data source. Future research should implement a multi-channel data collection and integration strategy to enhance the comprehensiveness and accuracy of the data. Specific recommendations include: first, fostering cross-sectoral collaboration with public transportation departments, community hospitals, and social networking platforms to gather data related to the community environment, daily activities, and health status. Second, diversifying data integration by utilizing remote sensing technology, geo-tagged time-series data, street view images, and residents’ activity trajectories, in conjunction with hospital patient information and personal health reports, to provide a comprehensive overview of the health behavior characteristics of older community residents. Finally, innovative analytical tools should be employed to examine the correlations among multi-source data by adopting cross-modal data integration technology, thereby enabling a thorough exploration of the comprehensive impact of the community built environment on the health of the older adults. This approach aims to provide a high-precision foundation for policy formulation.
Current research primarily focuses on the older adult, often neglecting the health needs of residents from various age groups within the community concerning the built environment. To develop a more inclusive model that addresses the health implications of the built environment, the following considerations should be taken into account: First, broaden the scope of research to comprehensively analyze the diverse needs of young, middle-aged, and older adult residents in community health services, while also exploring their interactions with the environment. Second, optimize the functional layout of the community and dynamically adjust the configuration of public facilities based on the needs of residents across multiple age groups, ensuring that all individuals can benefit. Finally, establish an intergenerational co-construction model that encourages the active participation of residents from different age groups in shaping the community built environment through intergenerational interaction programs, thereby enhancing the overall health of the community.
Since the regional sample of this study is limited to Fuzhou City, it is challenging to generalize the findings to other cities or regions. Therefore, future research should focus on the following: First, expanding the scope of the study to include similar investigations in various cities, regions, and countries to examine the impact of geographic differences on the health needs of older adult residents in the community. Second, conducting a differentiation analysis to facilitate in-depth comparisons of cultural backgrounds, economic conditions, and community planning across different regions, thereby refining replicable and scalable strategies for building healthy communities. Finally, establishing a data-sharing platform will promote the accessibility and sharing of community health research data through international and inter-regional collaboration, supporting cross-regional comparative research.
A meticulously designed community environment is instrumental in promoting the physical and mental well-being of older adults. Such an environment can significantly enhance their levels of physical activity, mitigate mental stress, decrease fatigue, and cultivate a sense of belonging within the community. This study seeks to investigate the daily routines of older adult individuals to elucidate the relationships among the community environment, daily activities, and the health of older adults, as well as the mechanisms through which these factors interact.
Research indicates that the physical infrastructure of a community can significantly influence the well-being of older adults. Firstly, the built environment can directly enhance the health of older adults, with accessibility identified as the most critical factor. Secondly, the built environment can indirectly affect the health of older adults by facilitating their daily activities, in which spatial environmental safety plays a pivotal role. Thirdly, the daily routines of older adults act as a mediator in the relationship between the built environment and their health. This mediation is particularly pronounced when the physical environment impacts the health of older adults who participate in outdoor exercise. Finally, the accessibility of facilities has the most substantial cumulative effect on the health of older adults.
It is imperative to prioritize the strategic placement of diverse facilities within the framework of community planning and development to encourage older individuals to utilize and engage with these resources, thereby enhancing their overall well-being. Additionally, community recreational areas and pathways should be meticulously designed to motivate older adults to engage in regular physical activities. The referenced study offers a coherent framework for improving the health of older populations and proposes practical initiatives and strategies for the creation of a health-promoting environment.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
The studies involving humans were reviewed and approved by Science and Technology Ethics Committee of Fujian University of Technology. The studies were conducted in accordance with local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
JY: Funding acquisition, Project administration, Supervision, Writing – review & editing. YS: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Writing – original draft, Writing – review & editing. FC: Funding acquisition, Supervision, Writing – review & editing. HY: Investigation, Writing – review & editing. YL: Investigation, Writing – review & editing.
The author(s) declare that financial support was received for the research and/or publication of this article. This study was supported by the Natural Science Foundation of Fujian Province (nos. 2022J05192 and 2022J01937) and the Talent Construction Fund of Fujian University of Science and Technology (nos. GY-Z21178 and GY-Z21177).
We sincerely appreciate all the authors who participated in this study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1478337/full#supplementary-material
1. ^www.wjx.cn
1. Tine, B, and Chris, P. Can global cities be 'Age-friendly Cities'? Urban development and ageing populations. Cities. (2016) 55:94–100. doi: 10.1016/j.cities.2016.03.016
2. Poganik, JR, and Gladyshev, VN. We need to shift the focus of aging research to aging itself. Proc Natl Acad Sci USA. (2023) 120:e2307449120. doi: 10.1073/pnas.2307449120
3. Liljas, AEM, Walters, K, Jovicic, A, Iliffe, S, Manthorpe, J, Goodman, C, et al. Strategies to improve engagement of 'Hard to Reach' older people in research on health promotion: a systematic review. BMC Public Health. (2017) 17:349–61. doi: 10.1186/s12889-017-4241-8
4. Song, Y, Wang, Y, Zhou, M, Suo, Z, Wang, X, Li, C, et al. Association between the perceived built environment and health behaviors in older adults: a cross-sectional study from Beijing, China. BMC Geriatrics. (2024) 24:1–9. doi: 10.1186/s12877-024-05285-7
5. Organisation WH. Constitution of World Health Organisation. Geneva: World Health Organisation. (1948). Available online at: https://www.who.int/about/governance/constitution
6. Xu, Y, Pan, C, Yu, H, and Zhan, B. Correlation analysis of the Urban Community environment and health promotion among adults aged ≥ 55 years: the mediating role of physical activity. BMC Public Health. (2024) 24:2790. doi: 10.1186/s12889-024-20303-4
7. Zheng, Z, Liu, W, Lu, Y, Sun, N, Chu, Y, and Chen, H. The influence mechanism of community-built environment on the health of older adults: from the perspective of low-income groups. BMC Geriatr. (2022) 22:590. doi: 10.1186/s12877-022-03278-y
8. Vahabi, S, Lak, A, and Panahi, N. Driving the determinants of older People’s mental health in the context of urban resilience: a scoping review. BMC Geriatr. (2023) 23:711. doi: 10.1186/s12877-023-04387-y
9. Lyu, X, and Fan, Y. The impact of home-and community-based services on the health of older adults: a Meta-analysis. SAGE Open. (2024) 14:787–95. doi: 10.1177/21582440241285674
10. Bonaccorsi, G, Milani, C, Giorgetti, D, Setola, N, Naldi, E, Manzi, F, et al. Impact of built environment and neighborhood on promoting mental health, well-being, and social participation in older people: an umbrella review. Ann Ig. (2022) 35:213–39. doi: 10.7416/ai.2022.2534
11. Niculita-Hirzel, H, Hirzel, AH, and Wild, P. A Gis-based approach to assess the influence of the urban built environment on cardiac and respiratory outcomes in older adults. Build Environ. (2024) 253:111362. doi: 10.1016/j.buildenv.2024.111362
12. Liu, Y, Guo, Y, Lu, S, Chan, O, Chui, C, Ho, H, et al. Understanding the long-term effects of public open space on older Adults' functional ability and mental health. Build Environ. (2023) 234:110126. doi: 10.1016/j.buildenv.2023.110126
13. Xiao, Y, Chen, S, Miao, S, and Yu, Y. Exploring the mediating effect of physical activities on built environment and obesity for elderly people: evidence from Shanghai, China. Front Public Health. (2022) 10:853292. doi: 10.3389/fpubh.2022.853292
14. Andersen, AMJ, Jervelund, SS, Maindal, HT, and Hempler, NF. Acquisition, application, and distribution of health literacy from culturally sensitive type 2 diabetes education among Arabic-speaking migrants in Denmark: a longitudinal qualitative analysis. Scand J Caring Sci. (2024) 38:523–35. doi: 10.1111/scs.13228
15. Zhao, Z, Zhehao, Y, and Yihua, M. Effect of the establishment of age-friendly communities on the life satisfaction levels of the elderly in Beijing. J Tsinghua Univ. (2024):1–10. doi: 10.16511/j.cnki.qhdxxb.2024.22.051
16. Yafei, Y, Dongfeng, Y, Dan, X, and Jinxin, L. How built environment affects the mental health of urban older adults: contrasting perspective based on observation and perception. China City Plan Rev. (2022) 31:26–37. doi: 10.20113/j.ccpr.2022.03.003
17. Barnett, DW, Barnett, A, Nathan, A, Cauwenberg, JV, and Cerin, E. Built environmental correlates of older Adults' Total physical activity and walking: a systematic review and Meta-analysis. The. Int J Behav Nutr Phys Act. (2017) 14:103–27. doi: 10.1186/s12966-017-0558-z
18. Zhang, Z, Tang, X, Shen, ZY, and Yang, L. Built-environment determinants of active travel behavior of older adults in Xiamen, China. Int Rev Spat Plan Sust Dev. (2022) 10:130–45. doi: 10.14246/irspsd.10.4_130
19. Shrivastava, RB, Shrivastava, PS, and Joshi, A. Use of technology to promote road safety: public health perspective. J Pharm Bioal Sci. (2024) 16:S2941–3. doi: 10.4103/jpbs.jpbs_1244_23
20. Sallis, JF, Cerin, E, Kerr, J, Adams, MA, and Owen, N. Built environment, physical activity, and obesity: findings from the international physical activity and environment network (Ipen) adult study. Annu Rev Public Health. (2020) 41:119–39. doi: 10.1146/annurev-publhealth-040218-043657
21. Anrooij, VV, Koks-Leensen, MCJ, Cruijsen, AVD, Jansen, H, Velden, KVD, Leusink, G, et al. How can care settings for people with intellectual disabilities embed health promotion? J Appl Res Intell Dis. (2020) 33:1489–99. doi: 10.1111/jar.12776
22. Wang, L, and Kang, J. Acoustic demands and influencing factors in facilities for the elderly. Appl Acoust. (2020) 170:107470. doi: 10.1016/j.apacoust.2020.107470
23. Rosenberg, DE, Huang, DL, Simonovich, SD, and Basia, B. Outdoor built environment barriers and facilitators to activity among midlife and older adults with mobility disabilities. Gerontologist. (2013) 53:268–79. doi: 10.1093/geront/gns119
24. Liu, Q, He, H, Yang, J, Feng, X, and Lyu, J. Changes in the global burden of depression from 1990 to 2017: findings from the global burden of disease study. J Psychiatr Res. (2019) 126:134–40. doi: 10.1016/j.jpsychires.2019.08.002
25. Shouyi, W, Xian, L, and Hua, F. Research on the prediction model of night lighting environment of college gymnasium based on visual comfort. Urban Arch. (2021) 12:29–31. doi: 10.19892/j.cnki.csjz.2021.07.06
26. Padeiro, M, de Sao Jose, J, Amado, C, Sousa, L, Roma Oliveira, C, Esteves, A, et al. Neighborhood attributes and well-being among older adults in urban areas: a mixed-methods systematic review. Res Aging. (2022) 44:351–68. doi: 10.1177/0164027521999980
27. Pan, Z, Liu, Y, and Li, Z. Can living in an age-friendly Neighbourhood protect older Adults' mental health against functional decline in China? Landsc Urban Plan. (2023) 240:104897. doi: 10.1016/j.landurbplan.2023.104897
28. Yaoqiong, Z, and Zhenwei, L. Optimization strategy of public space in old community based on health promotion of the elderly. Chin Landsc Architect. (2021) 37:56–61. doi: 10.19775/j.cla.2021.S2.0056
29. Grey, T, Xidous, D, O'Neill, D, and Collier, M. Growing older urbanism: exploring the Nexus between ageing, the built environment, and urban ecosystems. Urban Transform. (2023) 5:1–13. doi: 10.1186/s42854-023-00053-z
30. Hassan, A, and Deshun, Z. Psychophysiological impact of touching landscape grass among older adults. J Urban Health. (2024) 101:792–803. doi: 10.1007/s11524-024-00875-7
31. Leigh, G, and Leigh, A. Leafy localities, longer lives: a cross-sectional and spatial analysis. Landsc Urban Plan. (2024) 242:104947. doi: 10.1016/j.landurbplan.2023.104947
32. Yang, L, Tang, X, and Liu, MJ. Using a system of equations to assess the determinants of the walking behavior of older adults. Transact GIS TG. (2022) 26:1339–54. doi: 10.1111/tgis.12916
33. Booth, FW, Roberts, CK, and Laye, MJ. Lack of exercise is a major cause of chronic diseases. Compr Physiol. (2012) 2:1143. doi: 10.1002/cphy.c110025
34. Wang, L, Li, S, Wei, L, Ren, B, and Zhao, M. The effects of exercise interventions on mental health in Chinese older adults. J Environ Public Health. (2022) 2022:2–11. doi: 10.1155/2022/7265718
35. Parra-Rizo, MA, Díaz-Toro, F, Hadrya, F, Pavón-León, P, and Cigarroa, I. Association of co-Living and age on the type of sports practiced by older people. Sports. (2022) 10:200. doi: 10.3390/sports10120200
36. Li, L, Li, W, and Fan, T. Baduanjin exercise improves cognitive function in older adults with mild cognitive impairment. J Nerv Ment Dis. (2024) 212:500–6. doi: 10.1097/NMD.00000000000001796
37. Voss, MW, Sutterer, M, Weng, TB, Burzynska, AZ, Fanning, J, Salerno, E, et al. Nutritional supplementation boosts aerobic exercise effects on functional brain systems. Am Physiol Soc. (2019) 126:77–87. doi: 10.1152/JAPPLPHYSIOL.00917.2017
38. Toth, EE, Ihász, F, and Szabo, RR-B. Physical activity and psychological resilience in older adults: a systematic review of the literature. J Aging Phys Act. (2024) 32:276–86. doi: 10.1123/japa.2022-0427
39. Monnaatsie, M, Biddle, SJH, and Kolbe-Alexander, T. Feasibility of ecological momentary assessment in measuring physical activity and sedentary behaviour in shift and non-shift workers. J Act Sedent Sleep Behav. (2024) 3:24. doi: 10.1186/s44167-024-00063-7
40. Cheng, Y, Wang, JE, and Rosenberg, MW. Spatial access to residential care resources in Beijing, China. Int J Health Geogr. (2012) 11:32. doi: 10.1186/1476-072X-11-32
41. Yen, IH, Michael, YL, and Perdue, L. Neighborhood environment in studies of health of older adults: a systematic review. Am J Prev Med. (2009) 37:455–63. doi: 10.1016/j.amepre.2009.06.022
42. Gong, Y, Palmer, S, Gallacher, J, Marsden, T, and Fone, D. A systematic review of the relationship between objective measurements of the urban environment and psychological distress. Environ Int. (2016) 96:48–57. doi: 10.1016/j.envint.2016.08.019
43. Development CMoHaU-R. Urban residential area planning and design standard (Gb 50180-2018). Beijing, China: China Architecture & Building Press. (2018).
44. Hoogendijk, EO, Deeg, DJH, Poppelaars, J, Marleen, VDH, Broese, VG, Marjolein, I, et al. The longitudinal aging study Amsterdam: cohort update 2016 and major findings. Eur J Epidemiol. (2016) 31:927–45. doi: 10.1007/s10654-016-0192-0
45. Rajasi, RS, Mathew, T, Nujum, Z, Anish, TS, and Lawrence, T. Quality of life and sociodemographic factors associated with poor quality of life in elderly women in Thiruvananthapuram, Kerala. Indian J Public Health. (2016) 60:210–5. doi: 10.4103/0019-557X.189016
46. Fernández-Mayoralas, G, Rojo-Pérez, F, Martínez-Martín, P, Prieto-Flores, ME, and Forjaz, MJ. Active ageing and quality of life: factors associated with participation in leisure activities among institutionalized older adults, with and without dementia. Aging Ment Health. (2015) 19:1031–41. doi: 10.1080/13607863.2014.996734
47. Gottschalk, S, Knig, HH, Werner, C, Fleiner, T, Thiel, C, Büchele, G, et al. Association between physical activity and costs in very mild to moderately frail community-dwelling older adults: a cross-sectional study. BMC Public Health. (2024) 24:1–9. doi: 10.1186/s12889-024-20253-x
48. Ferrucci, L, Cooper, R, Shardell, M, Simonsick, EM, Schrack, JA, and Kuh, D. Age-related change in mobility: perspectives from life course epidemiology and Geroscience. J Gerontol. (2016) 71:1184–94. doi: 10.1093/gerona/glw043
49. Goran, M, Micheline, W, and Michiel, H. Short-and long-term health consequences of sleep disruption. Nat Sci Sleep. (2017) 9:151–61. doi: 10.2147/NSS.S134864
50. Xing, L, Zhengwei, J, Jiaxin, T, Lei, W, Helang, H, and Zhifeng, W. Study on anti-aging factors and patterns of dietary types and structure of middle-aged and elderly people. Chongqing Med J. (2022) 51:3421–7. doi: 10.3969/j.issn.1671-8348.2022.20.01
51. Mao, D, Li, G, Liang, M, Wang, S, and Ren, X. Dietary patterns and multiple chronic diseases in older adults. Nutr Metabol. (2024) 21:36. doi: 10.1186/s12986-024-00814-y
52. Pan, CW, Wang, X, Ma, Q, Sun, HP, Xu, Y, and Wang, P. Cognitive dysfunction and health-related quality of life among older Chinese. Sci Rep. (2015) 5:17301. doi: 10.1038/srep17301
53. Lopez, J, Perez-Rojo, G, Noriega, C, Sánchez-Cabaco, A, Sitges, E, and Bonete, B. Quality-of-life in older adults: its association with emotional distress and psychological wellbeing. BMC Geriatr. (2024) 24:1–6. doi: 10.1186/s12877-024-05401-7
54. Padmanabhanunni, A, Pretorius, TB, and Isaacs, SA. Satisfied with life? The protective function of life satisfaction in the relationship between perceived stress and negative mental health outcomes. Int J Environ Res Public Health. (2023) 20:11. doi: 10.3390/ijerph20186777
55. Macleod, S, Musich, S, Hawkins, K, Alsgaard, K, and Wicker, ER. The impact of resilience among older adults. Geriatr Nurs. (2016) 37:266–72. doi: 10.1016/j.gerinurse.2016.02.014
56. Lance, CE, Butts, MM, and Michels, LC. The sources of four commonly reported cutoff criteria: what did they really say? Organ Res Methods. (2006) 9:202–20. doi: 10.1177/1094428105284919
57. Cohen, J. Statistical power analysis for the behavioral sciences (2nd Ed): statistical power analysis for the behavioral sciences. 2nd edn. Hillsdale, New Jersey (Hillsdale, NJ): Lawrence Erlbaum Associates. (1988).
58. Kaiser, HF. An index of factorial simplicity. Psychometrika. (1974) 39:31–6. doi: 10.1007/BF02291575
59. Williams, B, Brown, T, and Onsman, A. Exploratory factor analysis: a five-step guide for novices. Austral J Paramed. (2010) 8:1–13. doi: 10.33151/ajp.8.3.93
61. Mcleroy, KR, Bibeau, D, Steckler, A, and Glanz, K. An ecological perspective on health promotion programs. Health Educ Q. (1988) 15:351–77. doi: 10.1177/109019818801500401
62. Gallardo-Peralta, LP, Raymond, M, and Gálvez-Nieto, JL. Ageing in context: an ecological model to understand social participation among indigenous adults in Chile. Res Aging. (2023) 45:332–46. doi: 10.1177/01640275221108502
Keywords: the community built environment, indirect impacts and direct impacts, structural equation modeling, older adults, health outcomes
Citation: Yang J, Shang Y, Cao F, Ying H and Luo Y (2025) Identify the direct and indirect impacts of the community built environment on the health of older adults. Front. Public Health. 13:1478337. doi: 10.3389/fpubh.2025.1478337
Edited by:
Orazio Valerio Giannico, Local Health Authority of Taranto, ItalyReviewed by:
Rongrong Zhang, Zhengzhou University of Light Industry, ChinaCopyright © 2025 Yang, Shang, Cao, Ying and Luo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fengxiao Cao, Y2FvZnhAZmp1dC5lZHUuY24=
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.