 Chandra Yogal1,2*
Chandra Yogal1,2* Astrid Kamilla Stunes1,3
Astrid Kamilla Stunes1,3 Sunila Shakya4
Sunila Shakya4 Biraj Karmarcharya2Rajendra Koju5
Biraj Karmarcharya2Rajendra Koju5 Mats P. Mosti1,6
Mats P. Mosti1,6 Miriam K. Gustafsson1,7Bjørn Olav Åsvold8,9Berit Schei10
Miriam K. Gustafsson1,7Bjørn Olav Åsvold8,9Berit Schei10 Unni Syversen1,9
Unni Syversen1,9- 1Department of Clinical and Molecular Medicine, Faculty of Medicine and Health Science, Norwegian University of Science and Technology, Trondheim, Norway
- 2Department of Community Program, Kathmandu University School of Medical Science, Dhulikhel Hospital, Kathmandu University Hospital, Dhulikhel, Nepal
- 3Center for Oral Health Services and Research, Mid-Norway (TkMidt), Trondheim, Norway
- 4Department of Gynecology and Obstetrics, Kathmandu University School of Medical Sciences, Dhulikhel Hospital, Kathmandu University Hospital, Dhulikhel, Nepal
- 5Department of Internal Medicine, Dhulikhel Hospital, Kathmandu University Hospital, Dhulikhel, Nepal
- 6Department of Research and Development, Clinic of Substance Use and Addiction Medicine, St. Olavs University Hospital, Trondheim, Norway
- 7Regional Education Center, Helse Midt-Norge, Trondheim, Norway
- 8HUNT Center for Molecular and Clinical Epidemiology, Department of Public Health and Nursing, Faculty of Medicine and Health Science, Norwegian University of Science and Technology, Trondheim, Norway
- 9Department of Endocrinology, Clinic of Medicine, St. Olavs University Hospital, Trondheim, Norway
- 10Department of Public Health and Nursing, Faculty of Medicine and Health Science, Norwegian University of Science and Technology, Trondheim, Norway
Background: The prevalence of overweight is rapidly escalating, especially in South-Asia. We aimed to estimate the prevalence of overweight/obesity and central obesity, and associated risk factors among women in a rural setting of Nepal.
Methods: A cross-sectional study addressing reproductive health and non-communicable diseases (NCDs) was conducted 2012–2013 in a rural district of Nepal. Married, non-pregnant women ≥15 years of age were included. Height, weight, and waist circumference (WC) were measured, and body mass index (BMI) calculated. WHO cut-offs for Asians were used to assess the prevalence of overweight (23.0–27.4 kg/m2), obesity (≥ 27.5 kg/m2) and central obesity (WC ≥ 80 cm). Data concerning socioeconomic and lifestyle factors were collected.
Results: Altogether, 1,391 women 43.1 ± 14.4 years of age were included. The majority belonged to the Adhivasi/Janajati ethnicity, were uneducated and worked in agriculture. Altogether, 30.5% were overweight, 12.0% obese, and 34.2% centrally obese; 25.7% were both overweight/obese and centrally obese. Underweight (< 18.5 kg/m2) was observed in 9.6%. Among women with normal weight or underweight, 14.9 and 15.3% had central obesity, respectively. Hypertension was observed in 13.4% and was associated with both overweight/obesity and central obesity. Instant noodle intake ≥2 times weekly was associated with increased prevalence of central obesity and overweight/obesity.
Conclusion: We observed a high prevalence of overweight/obesity and central obesity among women in a rural district of Nepal, which entails an increased risk of metabolic complications and NCDs. Our findings underscore the need for public health programs addressing nutritional patterns and physical activity to prevent obesity.
Introduction
The prevalence of overweight and obesity has doubled since 1980, affecting nearly a third of the population worldwide (1). The prevalence is now rapidly escalating in low- and middle-income countries (2). The most rapid rise in obesity is seen in South Asian countries like Maldives, Bhutan, Myanmar, Nepal, and Bangladesh (3). This rise is linked among others to dietary changes, increase in sedentary lifestyle, environmental contaminants, and epigenetic influences (4). Notably, the prevalence is somewhat higher among women than in their male counterparts (5, 6).
Nepal has witnessed a rapid change in social determinants, such as urbanization, nutritional transition, and economics (7). This is also accompanied by a dramatic rise in overweight and obesity, as demonstrated by the 2016 Nepal demographic and health survey (NDHS), including a total of 13,542 adults >18 years, of whom 61% were residing in urban areas (8). The overall prevalence of overweight/obesity using cut-offs for Asians (BMI ≥ 23.0 kg/m2) was 31.2%. When stratifying for sex, a higher prevalence of overweight or obesity was observed among women than men (8). Women of reproductive age are even more susceptible to overweight or obesity (9). Between 1996 and 2016, overweight/obesity (BMI ≥ 25.0 kg/m2) and obesity (BMI ≥ 30.0 kg/m2) increased from 1.8 to 19.7% and 0.2 to 4.1%, respectively, among non-pregnant Nepalese women (15–49 years) using cut-offs for the general population (10). In the same time period, the prevalence of underweight decreased from 24 to 17% (11). Socioeconomic factors, older age, female sex, married, education, watching television and high income have been shown to be positively associated with overweight/obesity prevalence in Nepal (10, 12–14).
The rise in obesity prevalence represents a major challenge as it is associated with increased risk of non-communicable diseases (NCDs), such as type 2 diabetes (T2D), hypertension and cardiovascular diseases (CVDs) (15, 16). NCDs are the main causes of death globally, accounting for 71% of deaths every year (17). Vasan et al., found that a weight increase by 5% promoted a 20–30% rise in the incidence of hypertension (18). Men display a higher prevalence of hypertension, but after the onset of menopause, women experience a more rapid increase in the prevalence (19). Maternal overweight/obesity during pregnancy is also associated with increased risk of metabolic diseases in the offspring later in life (20). In addition to the consequences for the individuals, the obesity epidemic represents a substantial economic burden on the society (21).
BMI is the most widely used measure of overweight and obesity. In Asian populations, the prevalence of CVDs has been observed to increase continuously with BMI (22). Central adiposity as assessed by waist circumference (WC) has, however, emerged as a better predictor of cardiometabolic risk than generalized adiposity (23) and is a significant predictor of obesity-related diseases and all-cause mortality (24, 25). Notably, South Asians, in general, have higher body fat and lower skeletal muscle mass at the same or lower BMIs compared to white people. Despite being generally less obese, they are also more prone to visceral fat accumulation and excess hepatic fat than western populations, which implies an increased risk for T2D and CVDs (26). This phenotype is even more pronounced in women. Consequently, lower cut-off values for BMI have been set by WHO for Asian than for White populations based on risk for CVDs and T2D (27, 28). The cut-off for WC used to define central obesity, is the same in Asian and European women (29).
Most previous studies in Nepal have addressed overweight and obesity by BMI. Thus, there is a knowledge gap concerning the prevalence of central obesity and the distribution of central obesity among individuals with different BMI categories, particularly among women in rural Nepal. In the present study, we therefore aimed to estimate the prevalence of both central obesity and overweight/obesity assessed by WC and BMI, respectively, among women in a rural setting of Nepal.
Materials and methods
Study design, study site and population
This is a cross-sectional population-based study conducted during February 2012 to May 2013 in five villages within the Kavre District, Nepal, as described previously (30, 31). The outcomes were prevalence of sexually transmitted infections (30, 31), and prevalence of overweight/obesity and diabetes. According to local tradition, never married and pregnant women, should not undergo gynecological examination (31). Therefore, the inclusion criteria were that the women should be married (including divorced and widowed) and ≥ 15 years of age. Exclusion criteria were pregnancy and mental and physical illness that made it difficult to attend the study site.
In each of the five villages there is a governmental primary health center and additionally, in Bolde Fediche there is an outreach health center run by Dhulikhel Hospital. According to the District Population Profile 2012, a total of 7,379 females were living in these five villages (32). The governmental household records showed that 2,674 married women aged ≥15 years were living in the villages during the study period. Of these, 258 were pregnant, thus, 2,416 women were eligible for participation in the study. Female community health volunteers (FCHVs) from the local community who were recruited by the government were involved in the implementation of the study. Prior to data collection, 45 FCHVs, health workers and local leaders in the study area were informed about the study. They thereafter conveyed this information to the eligible women and invited them to participate in the study. One-day screening sites were prepared at health centers, local schools, and village halls.
Data collection
A questionnaire was administered by trained female interviewers. Data on socio-demographic characteristics were collected, including age, ethnicity, religion, occupation, education level, household income and number of children. In addition, information was obtained on smoking habits (previous, current, or never smoking), frequency of intake of instant noodles, milk and vegetarian diet, and family history of diabetes, hypertension, and CVDs. Intake of instant noodles and milk was categorized as intake more often or less often than 2 times weekly. Data on energy intake and physical activity were not collected. The questionnaire was not validated.
Measurement of anthropometric parameters and blood pressure
Height was measured in centimeters (cm) by a measuring tape attached on the wall. Participants were requested to remove any hair ties, take off their shoes, to stand on a flat surface and look straight ahead without tilting their head. Body weight was recorded in kilogram (kg) using a portable digital weighing scale. The participants were requested to remove their footwear and to have minimal clothing. WC was measured in a separate room by a female health worker, in standing position, at the end of a natural expiration, holding the arms relaxed at the sides and at the midpoint between the lower margin of the last palpable rib in the mid axillary line and the top of the iliac crest (hip bone). The measurement was recorded in centimeters. BMI was calculated as weight in kilogram per square of height in meter and categorized according to WHO cut-off values for Asians as underweight (< 18.5 kg/m2), normal weight (18.5–22.9 kg/m2), overweight (23.0–27.4 kg/m2) and obese (≥ 27.5 kg/m2) (27). For comparison with other studies, the prevalence of overweight/obesity was also calculated using cut-offs for the general population, overweight 25.0–29.9 kg/m2 and obesity ≥30 kg/m2. Central obesity was defined as WC ≥ 80 cm according to WHO’s cut-off for Asian and European women (27). Blood pressure (BP) was measured by a digital device (Omron-5 series digital BP monitor, Japan) on the left arm in sitting position at the end of the interview. Hypertension was defined as systolic BP ≥ 140 mmHg and/or diastolic BP ≥ 90 mmHg and/or self-report of hypertension. Prehypertension was defined as systolic BP 120–139 mmHg and/or diastolic BP 80–89 mmHg (33).
Statistical analysis
The descriptive data are presented as mean and standard deviation (SD) for continuous variables and as frequencies (n) and percentages (%) for categorical variables. One-way ANOVA test was used for continuous variables and Pearson’s χ2 test for categorical variables. The overall prevalence of obesity across the covariates was calculated through cross tabulation. Bivariate and multivariate binary logistic regression analyses were performed with overweight/obesity (BMI ≥ 23 kg/m2) and central obesity (WC ≥ 80 cm) as dependent variables. Independent variables used in the analyses were: age, sociodemographic and dietary characteristics and smoking status. Age was used as a continuous variable or categorized into four groups, 17–34 years, 34–44 years, 45–54 years and ≥ 55 years. Ethnicity was classified into three groups, Brahmin/Chhetri, Adhivasi/Janajati and Dalit. Educational status was divided into two groups, uneducated and educated. Household monthly income was categorized into < and ≥ 24,000 Nepali rupees. Number of children was categorized as zero, 1–3 children and > 3 children. Intake of instant noodles and milk was categorized into <2 times a week and ≥ 2 times a week, respectively. Smoking status was categorized into current smoker, former smoker and never smoker. Adjustment for age, education and household income was made based on previous studies (12, 34). Results are presented as odds ratios (OR) and adjusted odds ratios (AOR) with 95% confidence intervals (CIs). All analyses were performed using IBM SPSS (version 28.0.1.0, New York, NY, USA).
Ethical considerations
The study was approved by the Dhulikhel Hospital/Kathmandu University School of Medical Sciences Institutional Review Committee (Approval no. 38/2011), Nepal Health Research Council (Approval no. 124/2012), and the Regional Committee for Medical and Health Research Ethics, Central Norway (Ref. no 2011/2540). Informed consent in the form of a signature or thumb print was obtained from women who agreed to participate. The study was conducted according to the guidelines provided in the Declaration of Helsinki.
Results
Characteristics of the study population
Altogether, 1,391 women aged 17 to 86 years (43.1 ± 14.4 years) were finally included based on measurement of BMI. The characteristics of the study population are summarized in Table 1. The women belonged to three ethnic groups, Brahmin/Chhetri, Adhivasi/Janajati and Dalit, representing the advantaged cast, “middle class” and disadvantaged cast, respectively. The majority were part of the Adhivasi/Janajati ethnicity (69.5%). Most of the women were uneducated (85.8%), and agriculture was the main source of income (84.6%). Moreover, 556 (40.0%) reported any intake of instant noodles, and 22.0% reported intake ≥2 times weekly. Milk intake was reported by 819 (59.4%) participants and intake ≥2 times a week by 29.0% of the study participants. One fourth of the women (25.0%) were current smokers, and 7.0% were former smokers. Mean BMI and WC were 23.1 ± 4.6 kg/m2 and 77.1 ± 8.9 cm, respectively. Prehypertension and hypertension were observed in 506 (36.4%) and 184 (13.4%) women, respectively. Only 27 (2.0%) women reported that they had hypertension, however, we do not have data on medication.
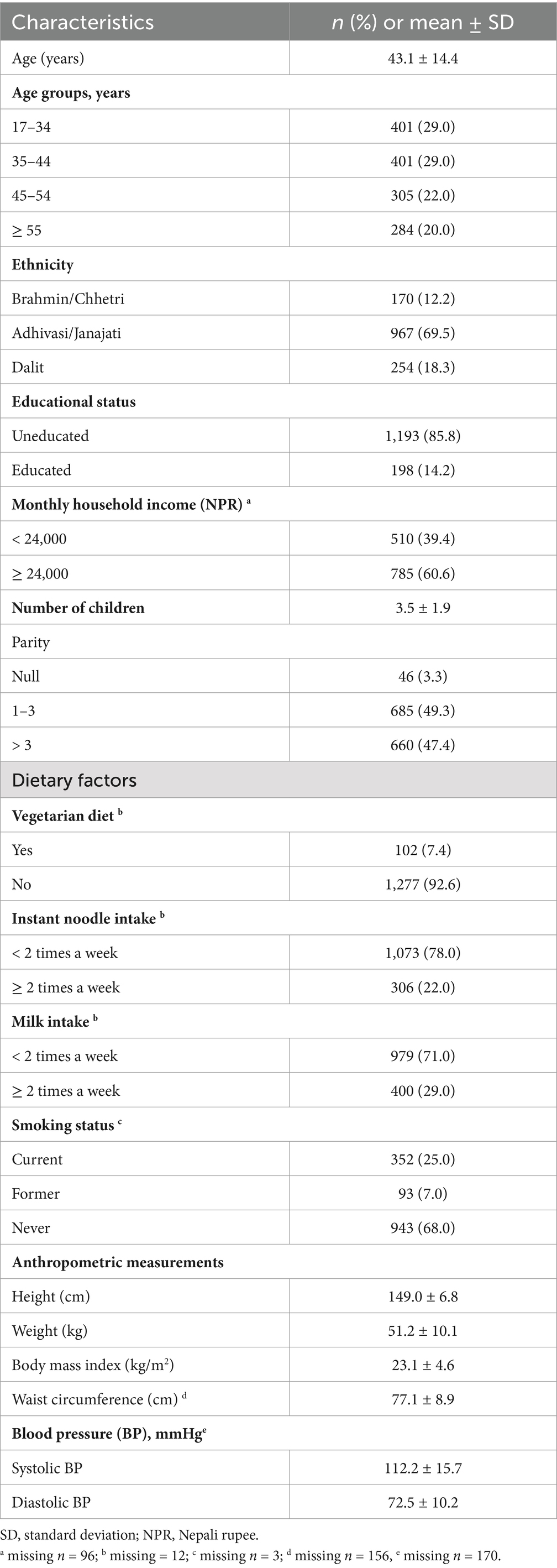
Table 1. Characteristics of the study population (n = 1,391).
Prevalence of overweight/obesity and central obesity stratified by the participants’ characteristics
The prevalence of overweight (BMI 23.0–27.4 kg/m2) and obesity (BMI ≥ 27.5 kg/m2) was 30.5 and 12.0%, respectively (Table 2). When applying WHO’s BMI cut-offs for the general population, the prevalence of overweight (BMI 25.0–29.9 kg/m2) and obesity (BMI ≥ 30.0 kg/m2) was 17.0 and 6.7%, respectively. The prevalence of obesity was highest in the age groups 35–44 and 45–54 years, 14.4 and 12.4%, respectively. Underweight (BMI < 18.5 kg/m2) was observed in 9.6% of the study population, one third of these were in the age group 35–44 years. Hypertension was most frequent in the age group 45–54 years.
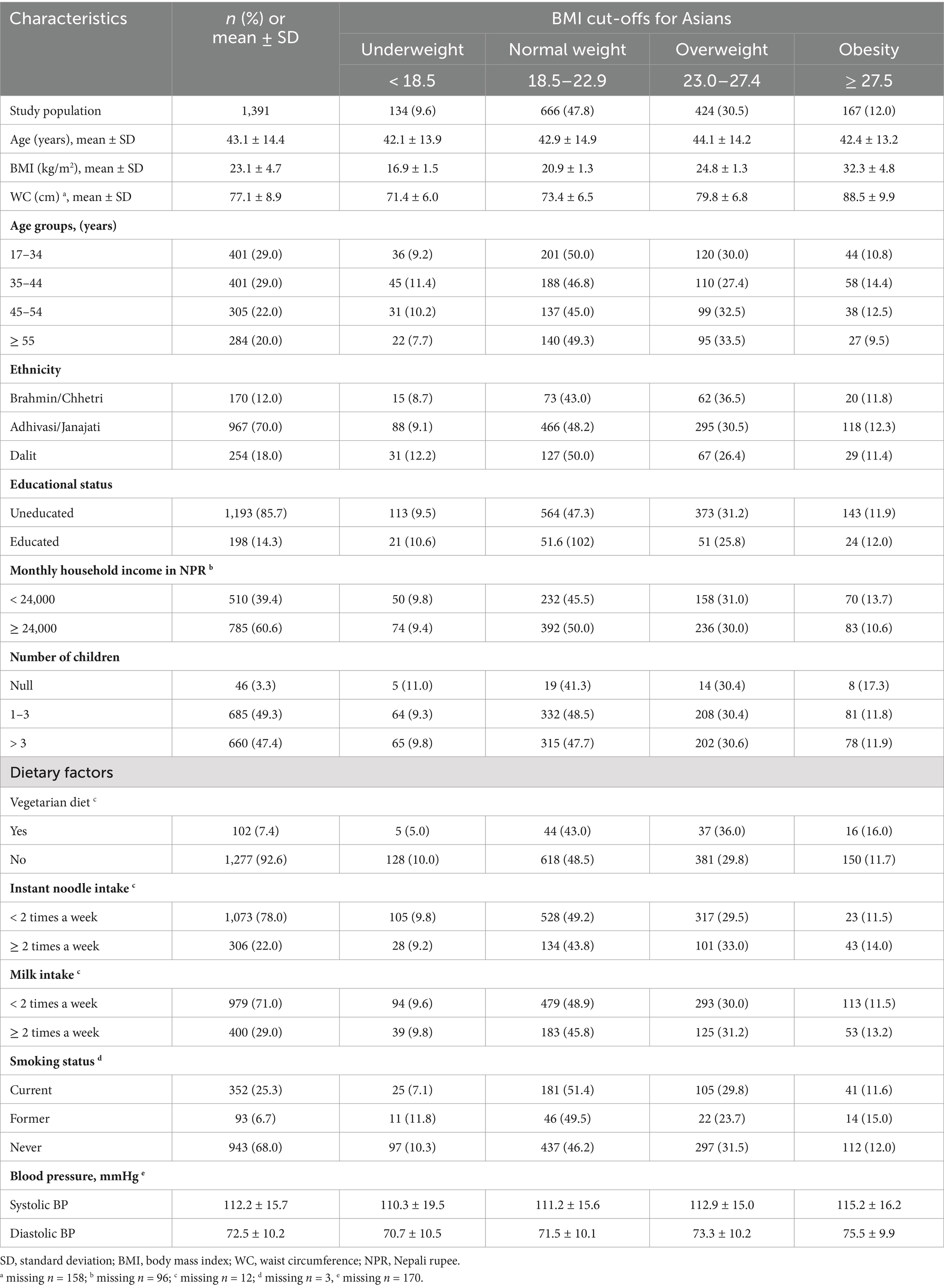
Table 2. Characteristics of the participants stratified by different BMI categories.
The prevalence of central obesity by selected characteristics is shown in Table 3. Central obesity (WC ≥ 80 cm) was observed in 34.2% of the participants and occurred frequently in all age groups. Women with intake of instant noodles ≥2 times per week displayed a higher prevalence of central obesity than those with intake <2 times weekly. Mean systolic and diastolic BP were higher in individuals with WC ≥ 80 cm than in those with WC < 80 cm. Figure 1 shows the percentage of the population with overweight/obesity, central obesity, and combination of the two. Altogether, 25.7% displayed both overweight/obesity and central obesity. Central obesity was also found in 14.9 and 15.3% of those with normal weight and underweight, respectively.
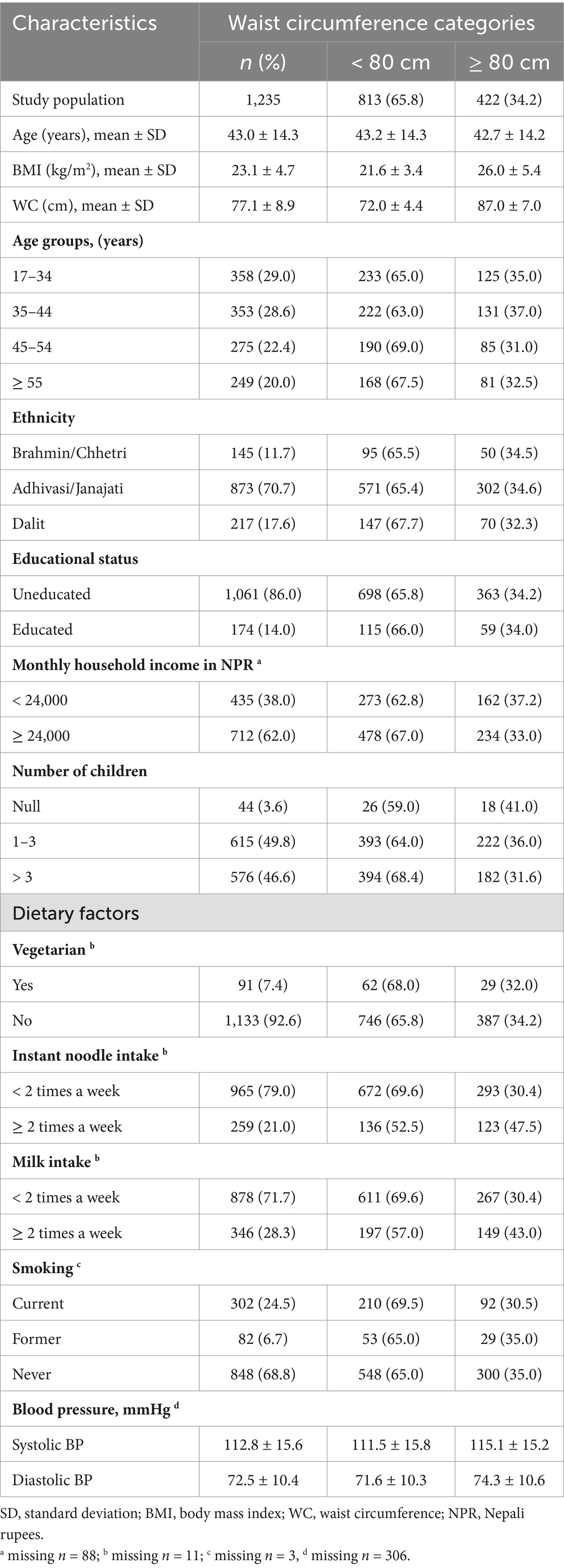
Table 3. Characteristics of the participants stratified by waist circumference below or above 80 cm.

Figure 1. Venn diagram showing the prevalence of overweight/obesity, central obesity and the combination of both.
Characteristics associated with overweight/obesity
Characteristics associated with overweight/obesity (cut-offs for Asians) are presented in Table 4. The prevalence of overweight/obesity did not convincingly differ by ethnicity. Women reporting consumption of instant noodles ≥2 times weekly exhibited a higher prevalence than those reporting intake <2 times weekly (OR 1.3, 95% CI: 0.99, 1.68; p = 0.062), however, borderline significant. Non-vegetarian diet was associated with a non-significant lower prevalence (OR 0.7, 95% CI: 0.47, 1.08; p = 0.112). Hypertension was associated with overweight/obesity (OR 1.5, 95% CI: 1.09, 2.13; p = 0.013).
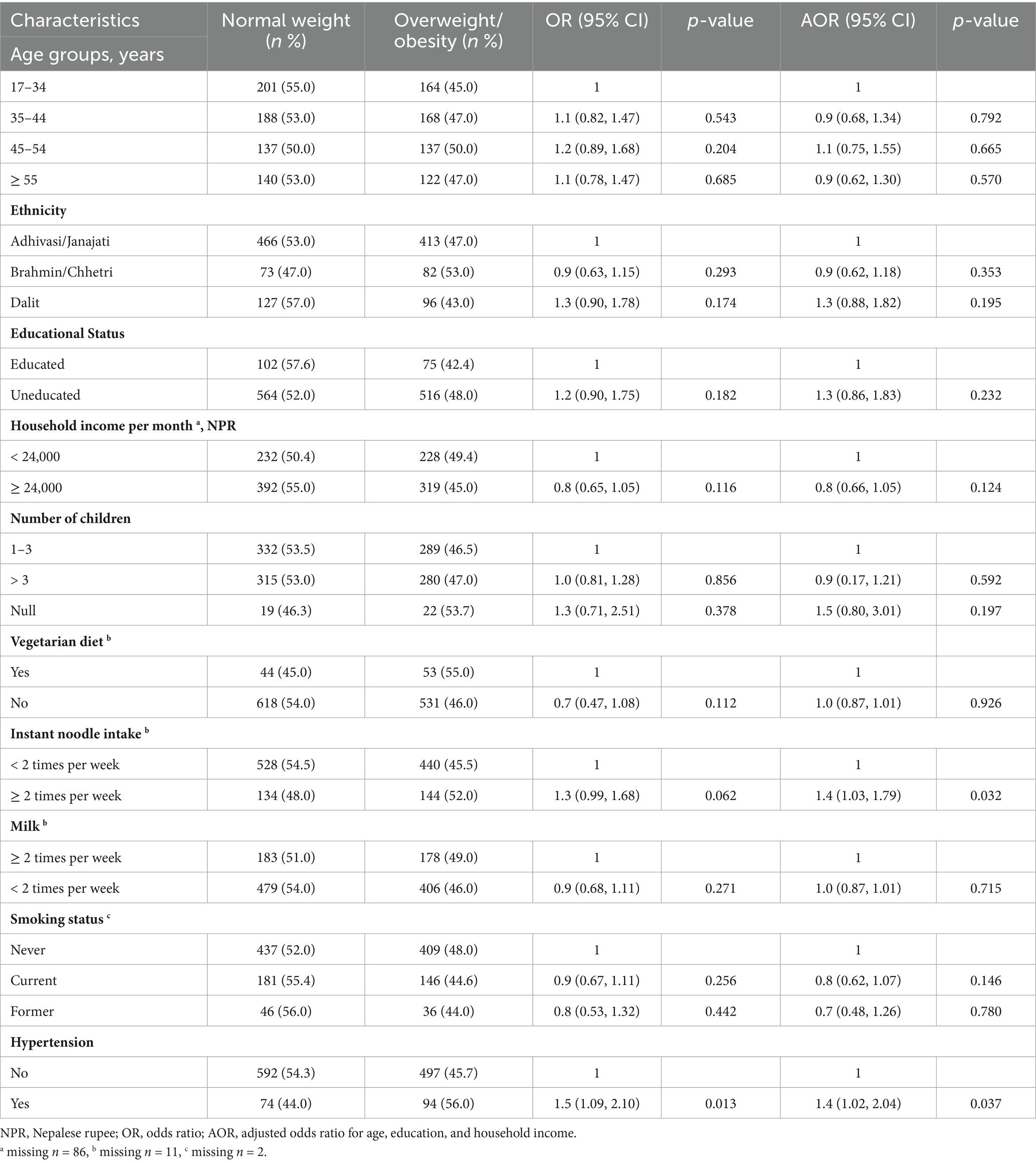
Table 4. Characteristics associated with overweight/obesity (n = 1,257).
Characteristics associated with central obesity
Characteristics associated with central obesity are presented in Table 5. Women with more than 3 children tended to have a lower prevalence (OR 0.8, 95% CI: 0.64, 1.04; p = 0.131), however, not statistically significant. Women consuming instant noodles ≥2 times a week displayed a higher prevalence of central obesity compared to those with intake <2 times weekly, (OR 2.1, 95% CI: 1.57, 2.74; p < 0.001). Women with milk intake <2 times a week were less likely to have central obesity than those with intake ≥2 times a week, (OR 0.6, 95% CI: 0.45, 0.75; p < 0.001). Given that concomitant intake of instant noodles and milk was common, we regarded instant noodles as a potential confounder. Accordingly, when adjusting milk intake for instant noodle consumption, the association was attenuated (OR 0.8, 95% CI: 0.56, 1.03; p = 0.08). Central obesity was less prevalent in those with non-vegetarian diet and in current smokers (OR 0.7, 95% CI: 0.47, 1.08; p = 0.112) and (OR 0.8 95% CI: 0.60, 1.06; p = 0.122), respectively, however, not significant. Women with central obesity exhibited a higher prevalence of hypertension (OR 1.5, 95% CI: 1.11–2.13; p = 0.009).
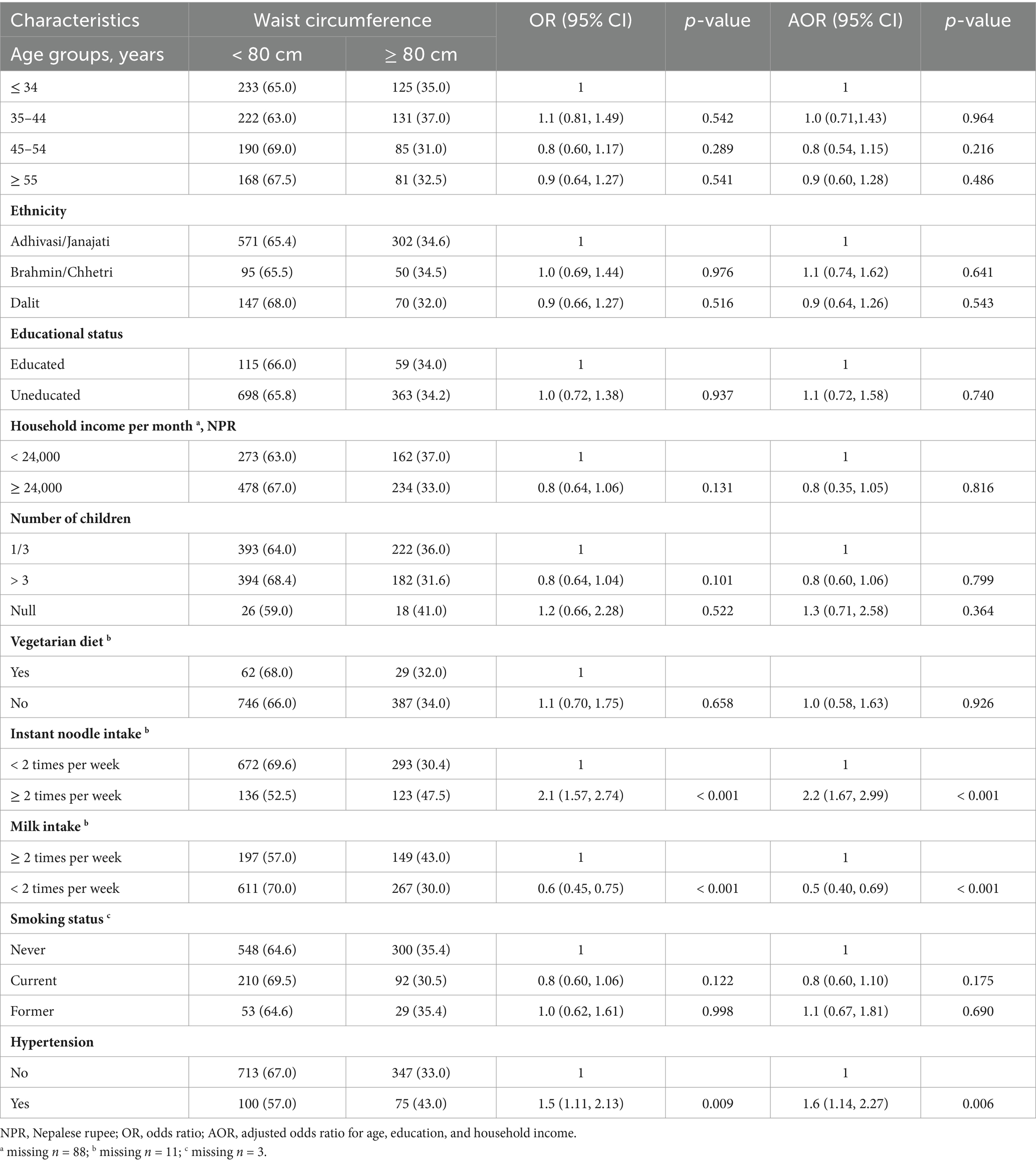
Table 5. Characteristics associated with central obesity in the study population (n = 1,235).
Discussion
In this large, cross-sectional study we observed a high prevalence of overweight/obesity, as well as central obesity among women in a rural district of Nepal. We applied cut-offs for Asians as recommended by WHO, both for BMI and WC. The prevalence of overweight and obesity in the study population was 30.5 and 12.0%, respectively, whereas central obesity was observed in 34.2%. Moreover, 9.8% of the women were underweight. To our knowledge, this is the first report on assessment of both overweight/obesity and central obesity among women specifically in rural Nepal. This approach enabled identification of central obesity among subjects in different BMI categories. Central obesity was observed in 15.3, 14.9 and 25.7% of those with underweight, normal body weight and overweight/obesity, respectively. Hypertension was observed in 13.4% and was associated with both overweight/obesity and central obesity. Women reporting intake of instant noodles more than two times weekly had a higher prevalence of central obesity.
The high prevalence of overweight and obesity observed among women in rural Nepal complies with the alarmingly high prevalence worldwide. Women are more susceptible to be overweight/obese, both in high-income and low-income countries (5, 25). We observed a higher prevalence of overweight/obesity than reported by Rawal et al., among women from the NDHS 2016, using cut-offs for Asians, 42.5% versus 32.9% (8). Mothers in a semi-urban region of Nepal displayed a prevalence of 57% (≥ 23.0 kg/m2) (35). The majority of the participants in the NDHS resided in urban areas (64.6%), where the prevalence of overweight and obesity is anticipated to be higher than in rural districts (11). However, Rawal et al., observed no significant difference in prevalence of overweight/obesity by ecological regions and place of residence (urban vs. rural) (8). In the NDHS, women in the age 36–45 years were more likely to be overweight or obese (8).
BMI is easy to obtain and is the most widely used measure of obesity and of the association between obesity and morbidity/mortality. However, it has been questioned whether BMI is an appropriate indicator of obesity (36). BMI does not distinguish between fat and lean mass and does not give information about fat accumulation (37). A novelty of the present study is that we applied both BMI and WC to assess the prevalence of overweight/obesity and central obesity, respectively, among women specifically in a rural district of Nepal. We used a WC cut-off of ≥80 cm as recommended by WHO for Asian and European women and found that 34.2% of the women displayed central obesity. The highest prevalence was seen in the age group 35–44 years (37%), followed by women <34 years. In a secondary analysis of NCDs risk factor 2013, addressing metabolic syndrome in 3,729 Nepalese adults, 27.5% had high WC (38). When stratifying for sex, central obesity was observed in 36.5% of the women (38), which is in line with the prevalence in our study. A report from “Non-communicable disease risk factors: STEPS survey Nepal 2019” showed a somewhat higher prevalence among the women, 39.7% versus 34.2% in the present study (39). Both studies applied cut-offs for Asians to measure WC (38, 39).
The high prevalence of overweight/obesity and central obesity in our study population is of concern, as these conditions are associated with increased risk of NCDs like T2D, hypertension, CVDs and cancer, giving rise to excess morbidity and mortality (16, 40, 41). High BMI has been associated with a wide range of cancers, and the combination of high BMI and WC with all-cause cancer (40, 41). Notably, a fourth of the women in the present study had both overweight/obesity and central obesity. Moreover, 14.9 and 15.3% of those with normal weight and underweight, respectively, displayed central obesity. There is increasing evidence that individuals with normal-weight central obesity are at increased risk for T2D due to excessive accumulation of abdominal fat (36, 42). Furthermore, subjects with central obesity at normal BMI have been shown to exhibit a similar or higher mortality risk as those with central obesity who are overweight or obese (43). They have, however, received little clinical attention, and are overlooked when it comes to development of preventive strategies. There are no reports on the significance of the combination of underweight and central obesity, but it is reasonable that these individuals have a similar risk profile as normal-weight subjects with central obesity. The American Obesity Society recommends routine measurement of WC in overweight people, but not in subjects with normal weight as the evidence of harmful effects of central obesity in individuals with a normal BMI is considered to be limited (44). Given the rise in central obesity over the last decades, the proportion of individuals with normal-weight and underweight central obesity is anticipated to rise. Accordingly, identification of these individuals and assessment of their health risks are clinically important.
Underweight was also prevalent in our study population, affecting 9.8% of the women, but was lower than reported by Rawal et al., from the NDHS 2016, where a prevalence of 18% was observed among women (8). This could possibly reflect differences between urban and rural districts. In the present study, underweight was most common in the age group 35–44 years, whereas Rawal et al., observed that older adult (≥ 65 years), and adults of the poorest wealth quintile were more likely to be underweight (8).
The high prevalence of overweight/obesity and central obesity as observed in the present and previous studies is postulated to be attributed to the rapid urbanization and industrialization. This has caused a dramatic shift in dietary patterns from traditional to western diet with energy-dense foods, accompanied by a decline in physical activity levels. The Nepalese diet has been reported to change from agricultural staple-based foods to modern processed foods with higher total energy, total fat, and sugar. The most pronounced increase was observed in consumption of plant oils with a seven-fold rise from 10 g/capita/day in 1970 to 65 g/capita/day in 2010 (45). Instant noodles were introduced in Nepal about 30 years ago. In 2019, South Korea had the highest consumption of instant noodles per capita with 75 servings per year, followed by Nepal and Indonesia with 58 and 56 servings, respectively (46). Notably, instant noodles have a high concentration of refined carbohydrates, fats and sodium and a high calorie content (47), and may thus contribute to an increased risk of metabolic disease. In a recent study, Park et al. showed that noodle intake had a causal association with metabolic syndrome in Asian adults (48). Moreover, they found that individuals in the high-noodle intake group had lower intake of calcium, vitamin D, and flavonoids, indicating a poorer diet quality. Additionally, the glycemic index and glycemic load of their daily meals were significantly higher compared to those in the low-noodle intake group (48). A South Korean study including 10,711 subjects, 19–64 years of age, also showed that women who consumed instant noodles ≥2 times a week, were 68% more likely to develop metabolic syndrome (49). These studies comply with our findings showing that intake of instant noodles ≥2 times a week was associated with central obesity and overweight/obesity, although borderline significant for the latter.
Noticeably, milk intake more than twice weekly was associated with increased prevalence of central obesity in our study population. This contrasts with the majority of studies showing a protective effect of dairy products both against central obesity and overweight/obesity (50, 51). The milk consumed in rural Nepal is not reduced in fat content, however, based on previous studies, this is not associated with an increased prevalence of obesity (52, 53). The association could possibly be attributed to the fact that a large proportion of women reporting milk intake ≥2 times weekly also consumed instant noodles. When adjusting milk intake ≥2 times weekly for intake of instant noodles twice weekly, the association was attenuated.
A decrease in physical activity has been recognized as an important contributor to obesity and NCDs. A nationwide cross-sectional study among 4,143 Nepalese adults (66.5% females) aged 15–69 years showed that around 97% of men and 98% of women met the recommended levels of physical activity. The Global Physical Activity Questionnaire (GPAQ) was applied and both rural and urban populations were included. Very few were engaged in any leisure-time activity, whereas both men and women reported high occupational physical activity. Moreover, a multiple regression analysis showed that less self-reported total physical was inversely associated with older age, higher level of education, urban place of residence, never been married, being underweight, and smoking in both sexes, and with overweight and obesity in males (54). Unfortunately, we did not collect data on physical activity, however, given that the majority of our study subjects were farmers, it is reasonable that the pattern of physical activity was similar.
In the NDHS 2016, adults who had no education except for preschool, had reduced prevalence of overweight/obesity (8), which contrasts with our results. Adults who never married also displayed reduced risk of overweight/obesity (8). We did not have the possibility to explore whether married women displayed a higher prevalence than never married, as only married women were included. Most studies show that increasing number of children is associated with obesity (55). Weng et al., observed a 7% increase in risk of obesity among women for each additional child after adjustment for multiple factors (56). In the present study, those with more than three children tended to have a lower prevalence of central obesity, whereas no association with BMI-defined obesity was observed.
There is emerging evidence for a role of environmental pollution in the development of obesity (57). These pollutants are referred to as obesogens, and they include among others bisphenol A (BPA), which is added to plastics and widely used, as well as some pesticides and air pollution (58–60). Notably, in 2019 Nepal was ranked as number 2 among countries with the highest emission of outdoor particulate matter 2.5 (PM2.5), which is the major air pollution globally (61). Kathmandu has topped the global ranks of the most polluted city for the last few years (62). We do not have data on air pollution at our study site in 2012–13. The study site is, however, located not so far from Kathmandu.
In the present study, overweight/obesity and central obesity were frequent in all age groups, thus affecting a large proportion of women in fertile age. Both women who are underweight and overweight/obese are at risk for adverse pregnancy outcomes, among others maternal anemia, gestational diabetes, miscarriage, preterm deliveries, intrauterine growth retardation and low birth weight (63–65). Furthermore, the offspring’s future health may be affected negatively, as children born to obese mothers are at increased risk of obesity and T2D (20, 66). This may be attributed to epigenetic mechanisms, genetic predisposition, or a shared family environment (20, 66). This may contribute to acceleration of the obesity and diabetes epidemics in Asia. Our study underscores the need for urgent preventive and curative strategies to combat these epidemics.
The high prevalence of both communicable diseases and NCDs in Nepal is a significant public health concern and poses a substantial burden on the society. The Multisectoral Action Plan for Prevention and Control of NCDs 2014–2020 was formulated with the goal to reduce preventable morbidity, avoidable disability, and premature mortality due to NCDs in Nepal (67). In a recent report by Dhimal et al., it was stated that implementation of this plan has been challenging, with limited participation from non-health sectors (68). It was concluded that multisectoral action plans beyond 2020, should engage stakeholders from federal, provincial, and local governments and develop costed action plans with specific roles and responsibilities for each sector.
A strength of the present study is the large study sample and the acceptable participation rate of 62% (31). Moreover, assessment of both BMI and WC allows identification of individuals that may have increased cardiometabolic risk. The study has some limitations. Due to the cross-sectional design of the study, a cause-and-effect relationship cannot be established. We do not have data on the women who did not participate, and cannot exclude that these women differed from those who took part in the study. Thus, selection bias at that level cannot be ruled out. The findings of the present study may not be generalizable to women in all rural districts of Nepal or to men. Data on the intake of different food items were based on reported frequency and not amount. Moreover, the information collected from the questionnaire relies on self-report and may be influenced by recall and social desirability bias. Finally, the questionnaire was not validated.
Conclusion
In conclusion, we observed a high prevalence of overweight/obesity and central obesity among women in a rural district of Nepal. The prevalence was high in all age groups. Central obesity was also found among women with normal weight and underweight. Intake of instant noodles ≥2 times weekly was associated with a higher prevalence of overweight/obesity and central obesity. Our results underscore that measurement of WC should be implemented in addition to BMI in assessment of obesity. Moreover, our findings illustrate the need for increased awareness and development of preventive health strategies to combat the obesity epidemic.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Nepal Health Research Council, the Dhulikhel Hospital/Kathmandu University School of Medical Sciences Institutional Review Committee and the Regional Committee for Medical and Health Research Ethics, Central Norway. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
CY: Formal analysis, Writing – original draft, Writing – review & editing, Data curation, Visualization, Software. AS: Formal analysis, Writing – review & editing, Visualization. SS: Investigation, Methodology, Project administration, Conceptualization, Writing – review & editing. BK: Conceptualization, Writing – review & editing. RK: Conceptualization, Methodology, Project administration, Writing – review & editing. MM: Formal analysis, Visualization, Writing – review & editing. MG: Formal analysis, Visualization, Writing – review & editing. BÅ: Writing – review & editing, Visualization. BS: Supervision, Writing – review & editing. US: Conceptualization, Funding acquisition, Resources, Supervision, Visualization, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This study was supported by a Global Health Research Fund from the Norwegian University of Science and Technology, Trondheim, Norway (grant number 81771136).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. World Health Organization. (2024). Obesity and overweight: key facts. Available at: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (Accessed April 24, 2024).
2. Templin, T, Hashiguchi, TCO, Thomson, B, Dieleman, J, and Bendavid, E. The overweight and obesity transition from the wealthy to the poor in low- and middle-income countries: a survey of household data from 103 countries. PLoS One. (2019) 16:e1002968. doi: 10.1371/journal.pmed.1002968
3. Awasthi, A, Panduranga, AB, and Deshpande, A. Prevalence of overweight/obesity in South Asia: a narrative review. Clin Epidemiol Glob Health. (2023) 22:101316. doi: 10.1016/j.cegh.2023.101316
4. Ford, ND, Patel, SA, and Narayan, KM. Obesity in low- and middle-income countries: burden, drivers, and emerging challenges. Annu Rev Public Health. (2017) 38:145–64. doi: 10.1146/annurev-publhealth-031816-044604
5. Bhurosy, T, and Jeewon, R. Overweight and obesity epidemic in developing countries: a problem with diet, physical activity, or socioeconomic status? ScientificWorldJournal. (2014) 2014:964236. doi: 10.1155/2014/964236
6. NCD Risk Factor Collaboration (NCD-RisC). Trends in adult body-mass index in 200 countries from 1975 to 2014: a pooled analysis of 1698 population-based measurement studies with 19·2 million participants. Lancet. (2016) 387:1377–96. doi: 10.1016/S0140-6736(16)30054-X
7. Shakya, S, Shrestha, V, and Neupane, D. Social determinants of health and cardiometabolic risk factors in Nepal: a scoping review. Nutr Metab Cardiovasc Dis. (2023) 33:2308–16. doi: 10.1016/j.numecd.2023.08.001
8. Rawal, LB, Kanda, K, Mahumud, RA, Joshi, D, Mehata, S, Shrestha, N, et al. Prevalence of underweight, overweight and obesity and their associated risk factors in Nepalese adults: data from a Nationwide survey, 2016. PLoS One. (2018) 13:e0205912. doi: 10.1371/journal.pone.0205912
9. Ogunwole, SM, Zera, CA, and Stanford, FC. Obesity Management in Women of reproductive age. JAMA. (2021) 325:433–4. doi: 10.1001/jama.2020.21096
10. Rana, K, Ghimire, P, Chimoriya, R, and Chimoriya, R. Trends in the prevalence of overweight and obesity and associated socioeconomic and household environmental factors among women in Nepal: findings from the Nepal demographic and health surveys. Obesities. (2021) 1:113–35. doi: 10.3390/Obesities1020011
11. Ministry of Health Nepal, New ERA, ICF. Nepal demographic and health Survery 2016. Kathmandu, Nepal: Ministry of Health, Nepal (2017).
12. Bhattarai, S, Nerhus Larsen, R, Shrestha, A, Karmacharya, B, and Sen, A. Association between socioeconomic positions and overweight/obesity in rural Nepal. Frontiers. Nutrition. (2022) 9:9. doi: 10.3389/fnut.2022.952665
13. Paudel, S, Owen, AJ, Owen, N, and Smith, BJ. Trends in television viewing and overweight /obesity among Nepalese women: findings from 2006, 2011 and 2016 Nepal demographic and health surveys. Nutr Metab Cardiovasc Dis. (2022) 32:382–92. doi: 10.1016/j.numecd.2021.10.023
14. Shakya, S, Absetz, P, and Neupane, S. Two-decade trends and factors associated with overweight and obesity among young adults in Nepal. PLOS Glob Public Health. (2023) 3:e0002522. doi: 10.1371/journal.pgph.0002522
15. Chu, D-T, and Singh, V. Obesity and hypertension in Asia: current status and challenges. Lancet Reg Health West Pac. (2021) 15:100243. doi: 10.1016/j.lanwpc.2021.100243
16. The GBD. 2015 obesity collaborators. Health effects of overweight and obesity in 195 countries over 25 years. N Engl J Med. (2017) 377:13–27. doi: 10.1056/NEJMoa1614362
17. World Health Organization. (2022). Noncommunicable diseases 2021. Available at: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (Accessed July 20, 2022).
18. Vasan, RS, Larson, MG, Leip, EP, Kannel, WB, and Levy, D. Assessment of frequency of progression to hypertension in non-hypertensive participants in the Framingham heart study: a cohort study. Lancet. (2001) 358:1682–6. doi: 10.1016/S0140-6736(01)06710-1
19. Tikhonoff, V, Casiglia, E, Gasparotti, F, and Spinella, P. The uncertain effect of menopause on blood pressure. J Hum Hypertens. (2019) 33:421–8. doi: 10.1038/s41371-019-0194-y
20. Godfrey, KM, Reynolds, RM, Prescott, SL, Nyirenda, M, Jaddoe, VWV, Eriksson, JG, et al. Influence of maternal obesity on the long-term health of offspring. Lancet Diabetes Endocrinol. (2017) 5:53–64. doi: 10.1016/S2213-8587(16)30107-3
21. Tremmel, M, Gerdtham, UG, Nilsson, PM, and Saha, S. Economic burden of obesity: a systematic literature review. Int J Environ Res Public Health. (2017) 14:435. doi: 10.3390/ijerph14040435
22. Ni Mhurchu, C, Rodgers, A, Pan, WH, Gu, DF, and Woodward, M. Body mass index and cardiovascular disease in the Asia-Pacific region: an overview of 33 cohorts involving 310 000 participants. Int J Epidemiol. (2004) 33:751–8. doi: 10.1093/ije/dyh163
23. Robson, E, Norris, T, Costa, S, Kivimäki, M, Hamer, M, and Johnson, W. Contribution of 20-year body mass index and waist circumference history to poor cardiometabolic health in overweight/obese and normal weight adults: a cohort study. Nutr Metab Cardiovasc Dis. (2021) 31:2851–9. doi: 10.1016/j.numecd.2021.06.005
24. Blüher, M. Obesity: global epidemiology and pathogenesis. Nat Rev Endocrinol. (2019) 15:288–98. doi: 10.1038/s41574-019-0176-8
25. Dai, H, Alsalhe, TA, Chalghaf, N, Riccò, M, Bragazzi, NL, and Wu, J. The global burden of disease attributable to high body mass index in 195 countries and territories, 1990–2017: an analysis of the global burden of disease study. PLoS One. (2020) 17:17(e1003198). doi: 10.1371/journal.pmed.1003198
26. Lim, U, Ernst, TM, Buchthal, S, Latch, M, Albright, CL, Wilkens, L, et al. Asian women have greater abdominal and visceral adiposity than Caucasian women with similar body mass index. Nutr Diabetes. (2011) 1:1. doi: 10.1038/nutd.2011.2
27. WHO Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet. (2004) 363:157–63. doi: 10.1016/S0140-6736(03)15268-3
28. World Health Organization. Wasit circumference and waist-hip ratio: Report of a WHO expert consultation. Geneva: World Health Organization (2008).
29. Lear, SA, James, PT, Ko, GT, and Kumanyika, S. Appropriateness of waist circumference and waist-to-hip ratio cutoffs for different ethnic groups. Eur J Clin Nutr. (2010) 64:42–61. doi: 10.1038/ejcn.2009.70
30. Shakya, S, Syversen, U, Åsvold, BO, Bofin, AM, Aune, G, Nordbø, SA, et al. Prevalence of human papillomavirus infection among women in rural Nepal. Acta Obstet Gynecol Scand. (2017) 96:29–38. doi: 10.1111/aogs.13036
31. Shakya, S, Thingulstad, S, Syversen, U, Nordbø, SA, Madhup, S, Vaidya, K, et al. Prevalence of sexually transmitted infections among married women in rural Nepal. Infect Dis Obstet Gynecol. (2018) 2018:1–9. doi: 10.1155/2018/4980396
32. Central Bureau of Statistics. National Population and Housing Census 2011 (National Report). Kathmandu: Central Bureau of Statistics (2012).
33. Chobanian, AV, Bakris, GL, Black, HR, Cushman, WC, Green, LA, Izzo, J, et al. The seventh report of the joint National Committee on prevention, detection, evaluation, and treatment of high blood Pressure the JNC 7 report. JAMA. (2003) 289:2560–71. doi: 10.1001/jama.289.19.2560
34. Shrestha, N, Mishra, SR, Ghimire, S, Gyawali, B, Pradhan, PMS, and Schwarz, D. Application of single-level and multi-level modeling approach to examine geographic and socioeconomic variation in underweight, overweight and obesity in Nepal: findings from NDHS 2016. Sci Rep. (2020) 10:2406. doi: 10.1038/s41598-019-56318-w
35. Schwinger, C, Chandyo, RK, Ulak, M, Hysing, M, Shrestha, M, Ranjitkar, S, et al. Prevalence of underweight, overweight, and obesity in adults in Bhaktapur, Nepal in 2015–2017. Front Nutr. (2020) 7:567164. doi: 10.3389/fnut.2020.567164
36. Jin, X, Liu, J, Cao, Q, Lin, J, Wu, G, Liu, L, et al. Normal-weight central obesity: implications for diabetes mellitus. Front Nutr. (2023) 10:1239493. doi: 10.3389/fnut.2023.1239493
37. Tuttle, MS, Montoye, AHK, and Kaminsky, LA. The benefits of body mass index and waist circumference in the assessment of health risk. ACSMs Health Fit J. (2016) 20:15–20. doi: 10.1249/FIT.0000000000000217
38. Mehata, S, Shrestha, N, Mehta, RK, Bista, B, Pandey, AR, and Mishra, SR. Prevalence of the metabolic syndrome and its determinants among Nepalese adults: findings from a nationally representative cross-sectional study. Sci Rep. (2018) 8:14995. doi: 10.1038/s41598-018-33177-5
39. Dhimal, M, Bista, B, Bhattarai, S, Dixit, LP, Hyder, MK, Agrawal, N, et al. Non-communicable disease risk factors: STEPS survey Nepal 2019. Kathmandu, Nepal: Nepal Health Research Council (2019).
40. Global BMI Mortality Collaboration. Body-mass index and all-cause mortality: individual-participant-data meta-analysis of 239 prospective studies in four continents. Lancet. (2016) 388:776–86. doi: 10.1016/S0140-6736(16)30175-1
41. Abdelaal, M, le Roux, CW, and Docherty, NG. Morbidity and mortality associated with obesity. Ann Transl Med. (2017) 5:161. doi: 10.21037/atm.2017.03.107
42. Shirasawa, T, Ochiai, H, Yoshimoto, T, Nagahama, S, Kobayashi, M, Ohtsu, I, et al. Associations between normal weight central obesity and cardiovascular disease risk factors in Japanese middle-aged adults: a cross-sectional study. J Health Popul Nutr. (2019) 38:46. doi: 10.1186/s41043-019-0201-5
43. Sun, Y, Liu, B, Snetselaar, LG, Wallace, RB, Caan, BJ, Rohan, TE, et al. Association of Normal-Weight Central Obesity with all-Cause and Cause-Specific Mortality among Postmenopausal Women. JAMA Netw Open. (2019) 2:e197337. doi: 10.1001/jamanetworkopen.2019.7337
44. Jensen, MD, Ryan, DH, Apovian, CM, Ard, JD, Comuzzie, AG, Donato, KA, et al. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: a report of the American College of Cardiology/American Heart Association task force on practice guidelines and the Obesity Society. Circulation. (2014) 129:S102–38. doi: 10.1161/01.cir.0000437739.71477.ee
45. Subedi, YP, Marais, B, and Newlands, D. Where is Nepal in the nutrition transition? Asia Pac J Clin Nutr. (2017) 26:358–67. doi: 10.6133/apjcn.112015.10
46. Buchholz, K. (2017). Oodles of noodles: instant noodle consumpiton around the world 2020. Available at: https://www.statista.com/chart/22865/instant-noodle-consumption-by-country/ (Accessed December 15, 2022).
47. Khanal, TR. (2021). Nutritional and health aspects of instant nooldes 2021. Available at: https://www.linkedin.com/pulse/nutritional-health-aspects-instant-noodles-tulsi-ram-khanal/?trackingId=%2B4OzK9RdR%2F%2BTDoqbx%2B%2FsFg%3D%3D (Accessed February 25, 2023).
48. Park, S, and Liu, M. A positive causal relationship between noodle intake and metabolic syndrome: a two-sample Mendelian randomization study. Nutrients. (2023) 15:2091. doi: 10.3390/nu15092091
49. Shin, HJ, Cho, E, Lee, HJ, Fung, TT, Rimm, E, Rosner, B, et al. Instant noodle intake and dietary patterns are associated with distinct cardiometabolic risk factors in Korea. J Nutr. (2014) 144:1247–55. doi: 10.3945/jn.113.188441
50. Rautiainen, S, Wang, L, Lee, IM, Manson, JE, Buring, JE, and Sesso, HD. Dairy consumption in association with weight change and risk of becoming overweight or obese in middle-aged and older women: a prospective cohort study. Am J Clin Nutr. (2016) 103:979–88. doi: 10.3945/ajcn.115.118406
51. Chen, M, Pan, A, Malik, VS, and Hu, FB. Effects of dairy intake on body weight and fat: a meta-analysis of randomized controlled trials. Am J Clin Nutr. (2012) 96:735–47. doi: 10.3945/ajcn.112.037119
52. Louie, JCY, Flood, VM, Hector, DJ, Rangan, AM, and Gill, TP. Dairy consumption and overweight and obesity: a systematic review of prospective cohort studies. Obes Rev. (2011) 12:e582–92. doi: 10.1111/j.1467-789X.2011.00881.x
53. Babio, N, Becerra-Tomás, N, Nishi, SK, López-González, L, Paz-Graniel, I, García-Gavilán, J, et al. Total dairy consumption in relation to overweight and obesity in children and adolescents: a systematic review and meta-analysis. Obes Rev. (2022) 23:e13400. doi: 10.1111/obr.13400
54. Pedisic, Z, Shrestha, N, Loprinzi, PD, Mehata, S, and Mishra, SR. Prevalence, patterns, and correlates of physical activity in Nepal: findings from a nationally representative study using the global physical activity questionnaire (GPAQ). BMC Public Health. (2019) 19:864. doi: 10.1186/s12889-019-7215-1
55. Van den Broek, T, and Fleischmann, M. The causal effect of number of children on later-life overweight and obesity in parous women. An instrumental variable study. Prev Med Rep. (2021) 24:101528. doi: 10.1016/j.pmedr.2021.101528
56. Haoling, H, Weng, LAB, Taylor, DH Jr, Moser, BK, and Ostbye, T. Number of children associated with obesity in middle-aged women and men: results from the health and retirement study. J Women's Health. (2004) 13:85–91. doi: 10.1089/154099904322836492
57. Wang, Y, Hollis-Hansen, K, Ren, X, Qiu, Y, and Qu, W. Do environmental pollutants increase obesity risk in humans? Obes Rev. (2016) 17:1179–97. doi: 10.1111/obr.12463
58. Nadal, A. Fat from plastics? Linking bisphenol a exposure and obesity. Nat Rev Endocrinol. (2013) 9:9–10. doi: 10.1038/nrendo.2012.205
59. Noppakun, K, and Juntarawijit, C. Association between pesticide exposure and obesity: a cross-sectional study of 20,295 farmers in Thailand. F1000Res. (2021) 10:445. doi: 10.12688/f1000research.53261.1
60. Deschenes, O, Wang, H, Wang, S, and Zhang, P. The effect of air pollution on body weight and obesity: evidence from China. J Dev Econ. (2020) 145:102461. doi: 10.1016/j.jdeveco.2020.102461
61. Health Effects Institute. State of global air 2020. Boston, MA: Health Effects Institute (2020).
63. Ghimire, PR, Akombi-Inyang, BJ, Tannous, C, and Agho, KE. Association between obesity and miscarriage among women of reproductive age in Nepal. PLoS One. (2020) 15:6435. doi: 10.1371/journal.pone.0236435
64. Sebire, NJ, Jolly, M, Harris, JP, Wadsworth, J, Joffe, M, Beard, RW, et al. Maternal obesity and pregnancy outcome: a study of 287 213 pregnancies in London. Int J Obes. (2001) 25:1175–82. doi: 10.1038/sj.ijo.0801670
65. Slack, E, Rankin, J, Jones, D, and Heslehurst, N. Effects of maternal anthropometrics on pregnancy outcomes in south Asian women: a systematic review. Obes Rev. (2018) 19:485–500. doi: 10.1111/obr.12636
66. Dalrymple, KV, Flynn, AC, Seed, PT, Briley, AL, O'Keeffe, M, Godfrey, KM, et al. Modifiable early life exposures associated with adiposity and obesity in 3-year old children born to mothers with obesity. Pediatr Obes. (2021) 16:e12801. doi: 10.1111/ijpo.12801
67. Government of Nepal. Multisectoral action plan for the prevention and control of non-communicable diseases (2014–2020). Nepal: Government of Nepal (2014).
68. Dhimal, M, Dhimal, ML, Dahal, S, Shrestha, MP, Gyanwali, P, Shao, R, et al. Barriers and facilitators to the implementation of a national multisectoral action plan for the prevention and control of noncommunicable diseases in Nepal: perspectives of stakeholders. Glob Health Action. (2021) 14:1963069. doi: 10.1080/16549716.2021.1963069
Keywords: overweight/obesity, central obesity, instant noodles, milk intake, women, rural Nepal, prevalence
Citation: Yogal C, Stunes AK, Shakya S, Karmarcharya B, Koju R, Mosti MP, Gustafsson MK, Åsvold BO, Schei B and Syversen U (2025) High prevalence of overweight/obesity and central obesity among women in a rural district of Nepal in 2012–2013: a population-based study. Front. Public Health. 13:1455940. doi: 10.3389/fpubh.2025.1455940
Edited by:
Robert Newton, Pennington Biomedical Research Center, United StatesReviewed by:
Ronny Westerman, Bundesinstitut für Bevölkerungsforschung, GermanyCairo Bruce Ntimana, University of Limpopo, South Africa
Copyright © 2025 Yogal, Stunes, Shakya, Karmarcharya, Koju, Mosti, Gustafsson, Åsvold, Schei and Syversen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Chandra Yogal, Y2hhbmRyYS5tLnlvZ2FsQG50bnUubm8=