 Edward Mundy1,2
Edward Mundy1,2 Alexander Carter3
Alexander Carter3 Tom Nadarzynski4†Christopher Whiteley5Richard O. de Visser3†
Tom Nadarzynski4†Christopher Whiteley5Richard O. de Visser3† Carrie D. Llewellyn3*†
Carrie D. Llewellyn3*†- 1School of Psychology, University of Kent, Canterbury, United Kingdom
- 2Sussex Partnership NHS Foundation Trust, Worthing, West Sussex, United Kingdom
- 3Department of Primary Care and Public Health, Brighton & Sussex Medical School, University of Sussex, Falmer, United Kingdom
- 4School of Social Sciences, University of Westminster, London, United Kingdom
- 5Central and North West London NHS Foundation Trust, London, United Kingdom
Introduction: Chemsex’ is the sexualised use of drugs among men who have sex with men (MSM). Past systematic reviews have primarily focussed on quantitative research exploring the key characteristics and health consequences of chemsex. However, a large body of qualitative literature exists, drawing on different theoretical frameworks.
Methods: A systematic review and thematic synthesis of the qualitative research on chemsex was conducted with the aim of exploring the chemsex experiences of MSM in the context of substance misuse and addictions, and to reviewing their underlying theoretical frameworks. Six databases were searched, and 43 papers were included in the review.
Results: The thematic synthesis resulted in four key themes: ‘characterising chemsex’, ‘the context around chemsex’, ‘the chemsex experience’, and ‘harms, saying safe, and stopping chemsex’. Only nine papers explicitly drew on theoretical frameworks, which were broadly divided into two categories: those which drew on psychological theories, and those that framed chemsex as a social and cultural phenomenon.
Discussion: The results of the thematic synthesis add further understanding of the key characteristics of chemsex as well as some of the complex social and psychological drivers which may shape why people have chemsex. Finally, the review highlights the clinical implications and inherent complexities in providing clinical services for those reporting chemsex and the need for greater application of theory to advance our understanding of chemsex and continue to develop appropriate forms of therapeutic support.
Systematic review registration: https://osf.io/j6k9r/.
Introduction
‘Chemsex’ has been defined as the sexualised use of drugs, in particular mephedrone, γ-hydroxybutyrate (GHB)/γ-butyrolactone (GBL) and crystallised methamphetamine, most commonly associated with men who have sex with men (MSM) (1, 2). Since the mid-2010s academic interest has increased in response to the emergence of chemsex among MSM (2) and its potential role in increasing rates of sexually transmitted infections (STIs) (3). Previous systematic reviews initially focussed on characterising chemsex as a phenomena and quantifying the health outcomes of people who engaged in chemsex, culminating in several reviews documenting which drugs were used, proximal antecedents to chemsex, motives for chemsex, and the health consequences, particularly in relation to HIV/STIs, other blood born viruses, illicit drug use, and psychological distress (4–6).
In addition to the quantitative research into chemsex, a body of qualitative research has emerged (3, 7–13). This research has explored the experiences of MSM who engage in chemsex, to understand the psychological, social, and cultural, factors that influence chemsex among some MSM. In doing so, this literature has sought to expand the focus beyond a narrow health and risk paradigm (8, 11, 14, 15, 65). Various theoretical and disciplinary approaches have been applied to the study of chemsex, drawing on sociological, cultural, public health, and psychological theory and methods.
There has been no review of the now substantial body of qualitative research into the experiences of MSM who engage in chemsex. Understanding the chemsex experiences of MSM (we use the term MSM to refer to men’s behaviour, and therefore include people who identify as gay, bisexual, heterosexual, or any other way) may contribute to our understanding of how, when, why, and what happens when people engage in this activity. Although previous systematic reviews (4–6, 66) have incorporated qualitative research, they have been limited in their depth of analysis and narrower focus on health consequences associated with chemsex. Furthermore, they have not integrated how different theoretical perspectives have conceptualised chemsex as a phenomenon.
A systematic review and thematic synthesis of the qualitative research on chemsex was conducted. The aims were to explore the chemsex experiences of MSM in the context of substance misuse and addictions, and to review their underlying theoretical frameworks.
Methods
The study protocol for this systematic review and narrative synthesis of qualitative studies of chemsex experiences of MSM followed PRISMA guidelines, and was registered on Open Science Framework (osf.io/j6k9r).
Search strategy
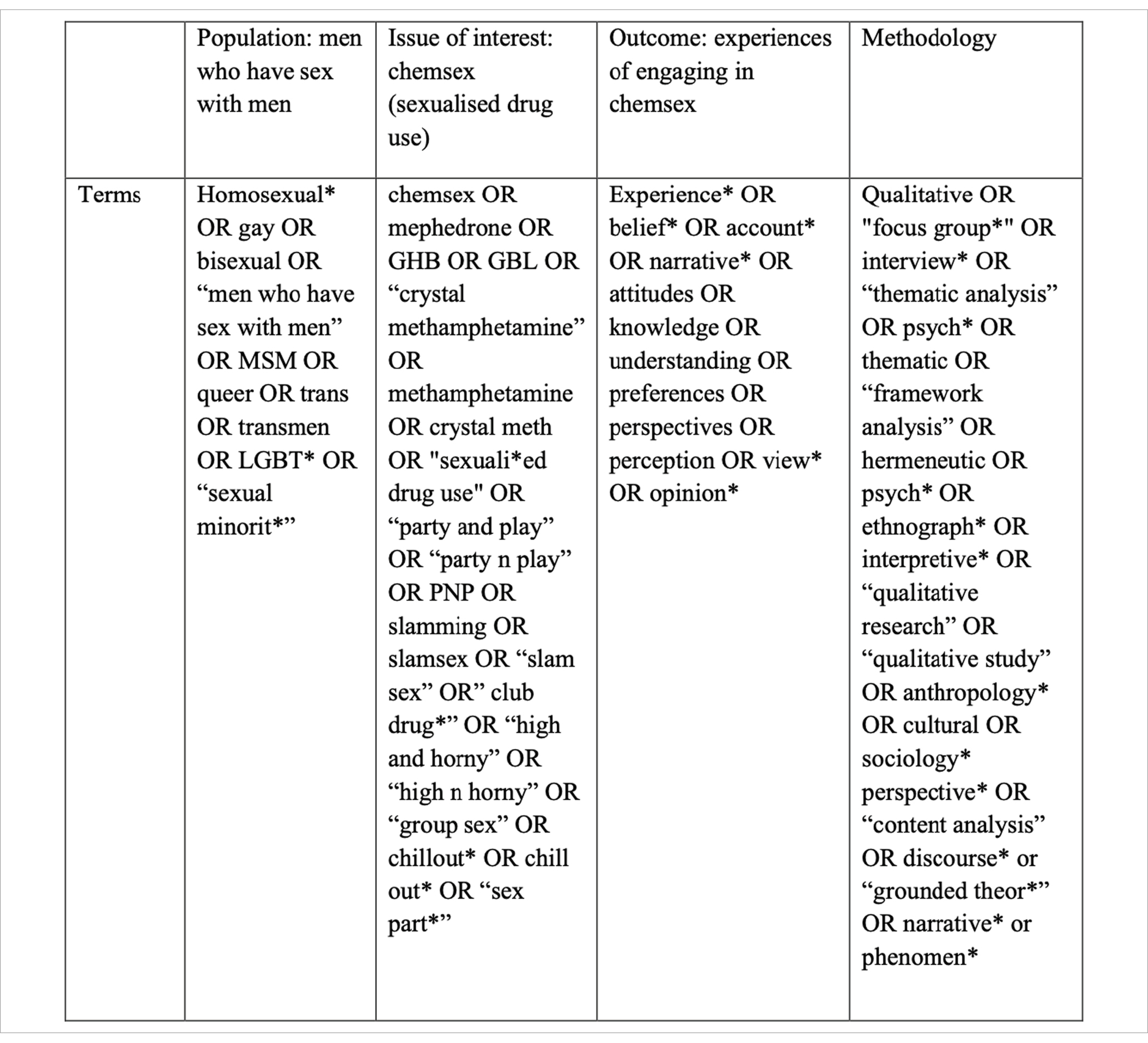
Web of Science, ASSIA, Pubmed, PsycINFO, SCOPUS, and EMBASE, were searched using a comprehensive search strategy. Searches of Google Scholar were also undertaken using the terms ‘chemsex’ and ‘qualitative’, alongside citation tracking and hand searching the reference lists of relevant literature. Databases were searched from 2000 onwards, as the early 2000s was when the term ‘chemsex’ is argued to have emerged (2, 16, 17). Databases were searched in March 2021 (by EM), with an updated search in November 2022 (by AC) to identify new papers.
Inclusion criteria
The review included peer-reviewed studies that explored the experiences of MSM who engage in chemsex. Participants were aged 16+, male, trans or of diverse gender identity, and had engaged in chemsex with other males, trans or people with diverse gender identities. Chemsex was defined as the use of illegal substances, in particular mephedrone, GHB/GBL, and crystallised methamphetamine, for sexual purposes or concurrently with sexual behaviour. However, given the lack of agreed terminology within the literature and geographic and cultural differences in the use of language around sexualised drug use, the review included studies which used a range of terminology, including chemsex, sexualised drug use, party’n’play, slam sex, and ‘chill out’. Furthermore, although chemsex is associated with other substances, such as alcohol, cannabis, amyl nitrate, or sildenafil, studies which reported on these substances were only included if they were used in addition to the focal chemsex substances listed previously. Studies were included if they provided qualitative data from either mixed-methods or qualitative studies and were published in English in peer-reviewed journals.
Exclusion criteria
Studies were excluded if they did not contain primary data, explored drug use among MSM outside of a sexualised context (i.e., general drug use in MSM); or studied chemsex in non-MSM populations. Studies which adopted a purely quantitative methodology, did not allow meaningful extraction of qualitative data, or were non-peer reviewed (i.e., grey literature) were also excluded.
Screening procedure
All studies identified from the search strategy were imported into Mendeley with duplicates removed. The database was then shared with each member of the research team. From there, study selection occurred over two phases for each search. During stage one, EM independently screened articles by title and abstract, guided by the eligibility criteria. At the same time, the database was divided equally between TN, CW, and CL who then independently screened articles by title and abstract, guided by the eligibility criteria. Independent evaluations of whether to include papers were shared with the whole team; discrepancies or disagreements were discussed until consensus was reached.
The second stage was independent full-text review of the included studies against the eligibility criteria by EM, TN, CW, and CL. Independent evaluations of whether to include papers were shared with the whole team; discrepancies or disagreements were discussed until consensus was reached. When the updated searches were conducted, the same stepwise procedure was followed with AC carrying out the initial screening. Figure 1 presents a flow diagram.

Figure 1. Prisma diagram.
Data extraction
Data from eligible studies was extracted and entered into a customised template. Data included key descriptive information (authors, study year, location), study aims and objectives, participants and contextual information (demographic and descriptive information about participants), theoretical framework, methodological information (recruitment, data collection and analysis methods), and results (key findings, main themes and sub-themes, illustrative quotes, and interpretive codes). Data were then imported into NVivo 12 Pro (QSR International Pty Ltd., 2018) for data analyses.
Data analysis
Data were analysed following the three stages of thematic synthesis described by Thomas and Harden (18). Although these stages are described linearly, this was an iterative process, with stages one and two beginning concurrently, with greater differentiation as the analysis continued and themes were created. Stage one consisted of the systematic line-by-line coding of data (i.e., main themes, sub-themes, illustrative participant quotes) and ascribing meaning to sections of text. The cumulative process of line-by-line coding led to categorisation of findings which were felt to be similar in content into preliminary themes, stage two. Finally, these themes were hierarchically ordered to present the final themes.
Quality appraisal
Studies were assessed using the Joanna Briggs Institute (JBI) quality appraisal tool for qualitative research (67). The JBI checklist is a widely-used tool that allows researchers to assess the quality of qualitative studies (19). All papers were assessed by AC and their quality was considered when describing and interpreting the results.
Results
We initially identified 2,040 papers. Following the removal of duplicates and the exclusion of papers that did not meet inclusion criteria on the basis of screening their titles and abstract, 72 papers were retrieved and a full text review was undertaken. Of those, 29 were not included (Figure 1), leaving a final 43 papers for inclusion in the review.
Study characteristics
Table 1 provides a summary of studies. Most were conducted in the USA (10), the UK (9), Western Europe (11), and Canada (5), alongside studies in Australia (3), South Africa (1), Singapore (1), China (1), Thailand (1) and Malaysia (1). In total, 1,295 participants were included, with sample sizes ranging from 6 to 89. Participants were aged 18–74 and were either engaging in chemsex at the time of the study, or had done so previously. Studies predominantly employed individual interviews and used various analytic approaches: Thematic Analysis (21), Interpretive Phenomenological Analysis (2), Critical Discourse Analysis (2), Content Analysis (4), Grounded Theory (6), Labovian Narrative Analysis (1), Conjectural analysis (1), Ethnography (1), Framework Analysis (1). Four studies contained insufficient detail to allow categorisation of their data analysis (20–22, 23). Four studies used focus groups alongside individual interviews (7, 9, 21, 23).

Table 1. Summary of included studies.
Risk of bias assessment
All studies were of a high quality. The majority fell down on reporting their theoretical perspective and failing to address the effect that the researcher may have on the participant responses and vice versa. All studies scored highly (ranging from 7 to 9 out of 10) for their methodology and reporting of results, as well as accurate representation of participant voices (Table 2).
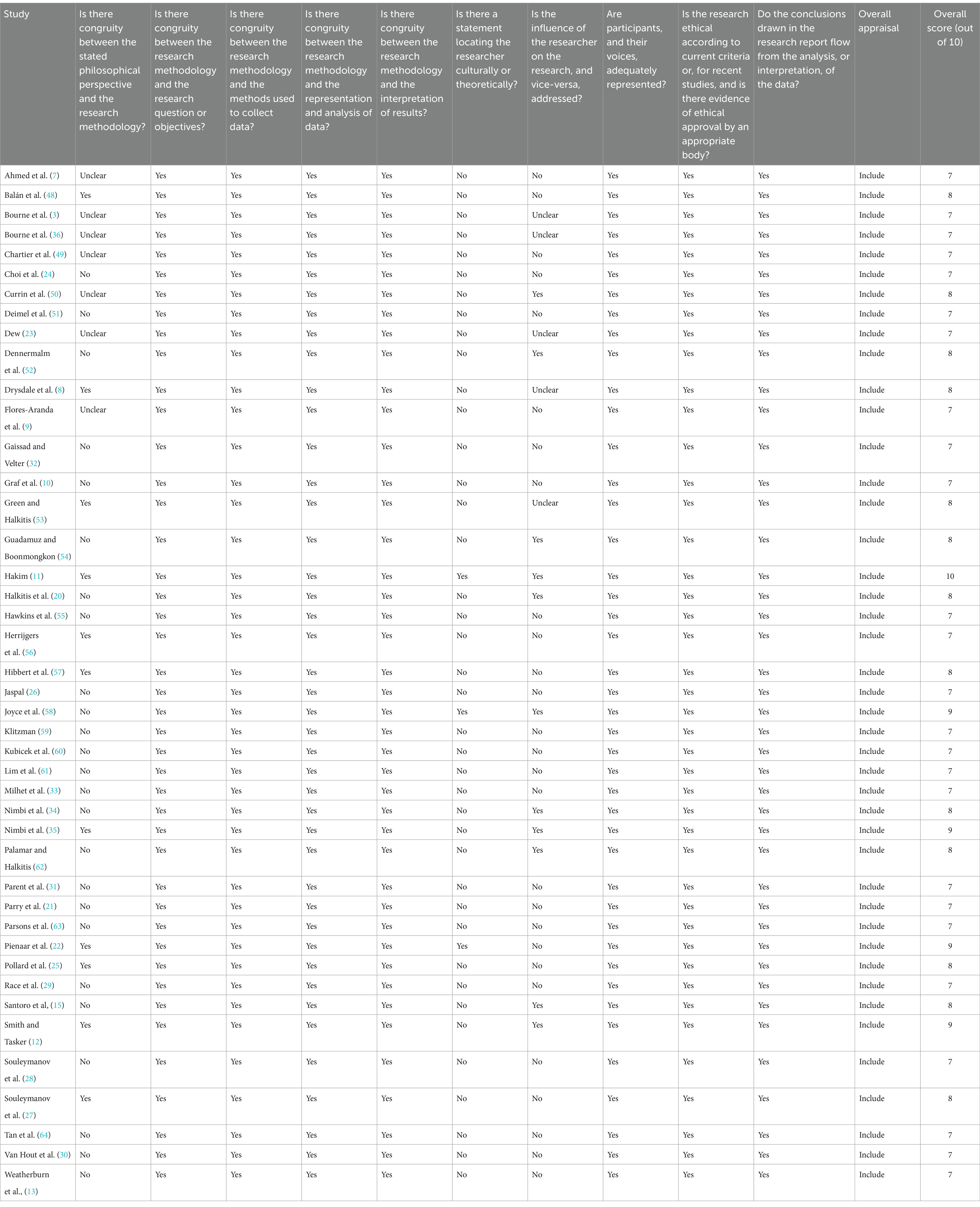
Table 2. Summary of JBI checklist quality appraisal.
Theoretical frameworks
Only nine studies framed their understanding of and approach to chemsex within an explicit theoretical framework (Table 3). These papers were broadly divided into two categories: those which drew on psychological theories, and those that framed chemsex as a social and cultural phenomenon.
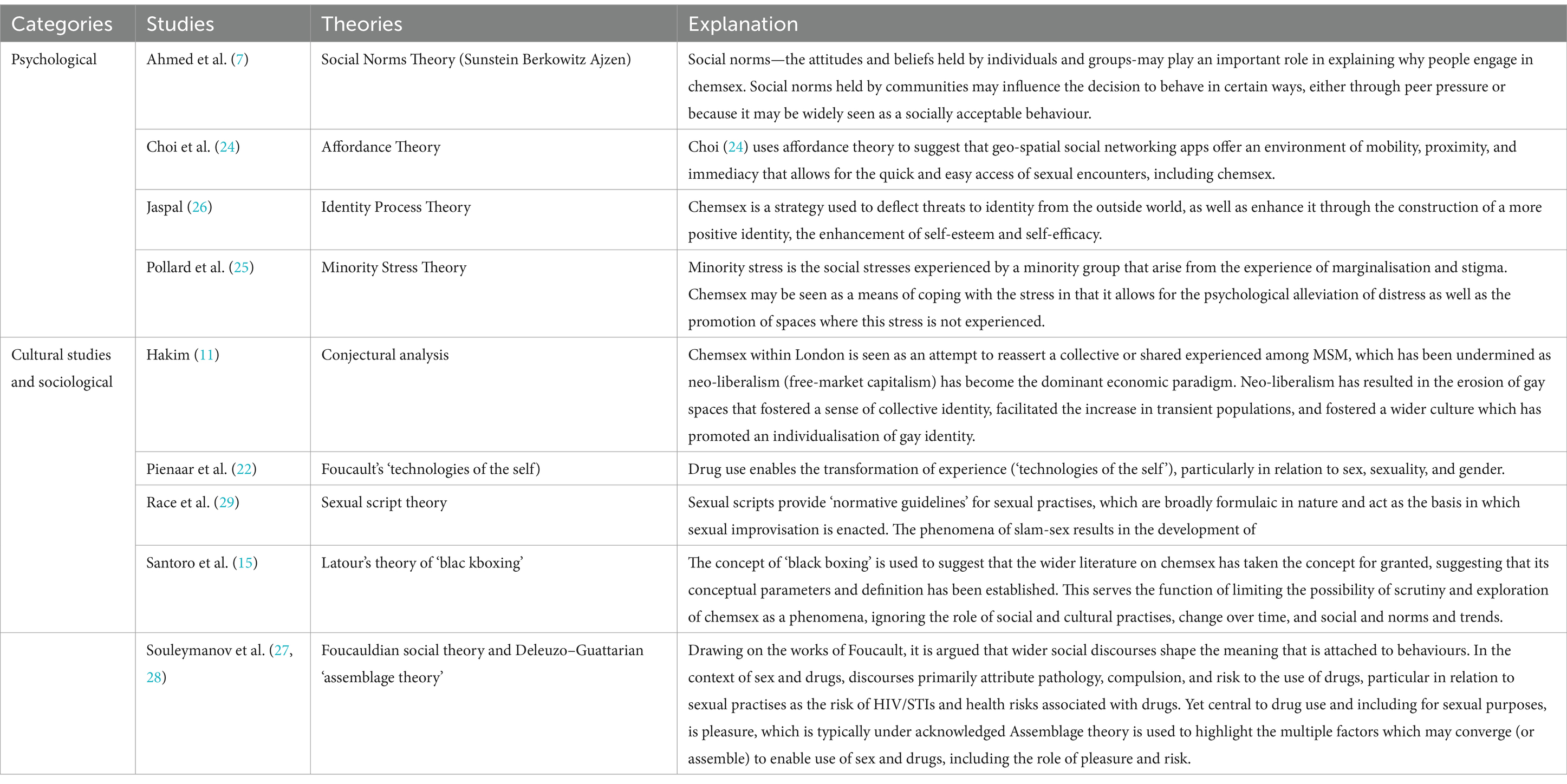
Table 3. Theoretical frameworks of studies.
Papers which explicitly drew on psychological theory used Affordance Theory (24), Syndemic and Minority Stress theories (25), Social Norm Theory (7), and Identity Process Theory (26). In drawing on Affordance Theory (68), Choi et al. (24) view chemsex as emerging through the proliferation and use of digital technology, in particular geo-spatial dating apps, among MSM. Technology allows for the creation of a digital environment which offers users three unique ‘affordances’: (1) mobility in that smart phones can be used at anytime and anywhere by users; (2) proximity both physically and digitally to others who are using the app; and (3) immediacy in terms of ease in arranging sexual encounters. These affordances are given greater salience in the context of ongoing discrimination and stigmatisation as a sexual minority. Pollard et al. (25) extend the significance of the role of discrimination and marginalisation by viewing chemsex through the prism of syndemic and minority stress theories. MSM experience unique marginalisation as Chemsex is situated within three contexts of adversity: (1) prevailing homophobic culture, (2) pressurised and hedonistic gay-subcultures, and (3) interpersonal invalidation. Jaspal (26) also places emphasis on the role of stress which can arise as a member of a sexual minority, but emphasises how these stressors exert themselves through a person’s sense of identity. Drawing on Identity Process Theory, Jaspal (26) argues that sexual-minority stressors harm a person’s sense of self-esteem and efficacy, with chemsex acting as a means by which MSM manage the distress which can result. Ahmed et al. (7) also highlight the social context, but argue that it influences chemsex through social norms - attitudes and beliefs that groups hold, or individuals perceive the group to hold, about appropriate or inappropriate behaviour. Ahmed et al. (7) draw on Social Norm Theory to argue that chemsex emerged in the context of MSM viewing it as normalised among other MSM, how sex was perceived to be different when under the influence of drugs, and in the context of pre-existing social norms around the ubiquity of drug use among MSM.
The second collection of papers applying an explicit theory were predominantly critical of most academic approaches to studying chemsex, which were seen to pathologise sexualised drug use through a focus on health risks. Souleymanov et al. (27, 28) drew on Foucaludian social theory and assemblage theory to highlight how social discourses shape the meaning attached to chemsex, with discourses primarily highlighting pathology, compulsion, and health risks (especially HIV). For Pienaar et al. (22) chemsex is an inherently transformative experience and uses Foucault’s idea of the technologies of the self to argue that drugs are a ‘technology’ that individuals use to transcend themselves and facilitate new subjective experiences. This has particular relevance for gender and sexual minorities where drugs enable the expansion of experiences, possibilities, and pleasure in relation to sexual and gender identity transcending restrictive binary understandings. Similarly, Race et al. (29) highlight the way in which drugs enable a transformation of experience through the transcending of sexual-scripts that structure sexual encounters. Santoro et al. (15) draw on Latour’s theory of ‘black boxing’ to argue that the literature on chemsex has taken the concept for granted, without sufficient scrutiny or discussion around its conceptual parameters. The focus on public health risks potentially downplays the role of important social and cultural dynamics which underpin chemsex. Hakim (11) uses conjectural theory to conceptualise chemsex as an attempt by marginalised communities to experience a sense of collectively which has been undermined through various social, cultural, and historical forces, predominantly a neo-liberal economic paradigm which has eroded queer spaces and emphasised individualism.
Papers that did not use an explicit theoretical framework often framed or positioned chemsex in two distinct ways. The first drew primarily on literature highlighting the health risks or concerns around chemsex, particularly increased risk of STIs, or risks associated with drug use, including addiction and poor mental health. The second approach, however, was often critical of approaches that framed chemsex primarily as a health risk. Instead, these papers explored the social, psychological, and cultural meanings of sex and drugs, as well as how risk was navigated by those who engaged in chemsex.
Understanding the chemsex experiences of MSM
The search highlighted a range of different themes across the papers, which were broadly divided into four main areas.
Theme 1: Characterising chemsex: frequency, settings, drugs, and sexual partners
The first major theme related to characterising chemsex, this included the places and settings that people engage in chemsex, the types of drugs used, the frequency and length of chemsex sessions, the diversity of chemsex experiences. Participants reported using chemsex in the context of group sex, sex with multiple partners, and with individual partners. The length of chemsex sessions varied from hours through to multiple days, and the frequency of engaging in chemsex varied from once or twice yearly (often around large LGBT events), to 1–2 per month or per week, and more frequently.
People who engaged in chemsex reported using a range of drugs. Although crystal methamphetamine, mephedrone, and GHB were the most commonly cited, people also reported using Ecstasy/MDMA, cocaine, cannabis, ketamine, and heroin. Polysubstance use was reported. People also reported using other substances in the context of chemsex, including alcohol and nicotine, amyl nitrate (‘poppers’) and Sildenafil (‘Viagra’). People reported consuming drugs in a variety of ways including injecting, snorting, smoking, and as part of sex acts.
People reported engaging in sexualised drug use in private settings, particularly people’s homes, as well as sex on premised sites, and public spaces, however, it is important to note that some people described chemsex taking place across multiple settings and reported a progression of events. Typically, people described taking drugs for recreational and social reasons in a social setting, such as a club, but as the time progressed and commercial spaces closed, participants would either seek out chemsex, or there would be a progression of going to a private home which developed into chemsex.
Theme 2: the context around chemsex
Many participants discussed their experience of chemsex with reference to the wider social and cultural context in which they lived. Reference was made to wider queer culture and the expectations and norms that are perceived by some to be present; the perceived prevalence of drug use generally, and wider social and geographic determinants of gay life; as well as the role of discrimination and minority stress that MSM can experience.
Queer culture
This theme captured the wider norms, experiences, and expectations that participants discussed in relation to wider queer culture in which chemsex took place.
Apps and hook up culture
When discussing their experience of chemsex, and arranging chemsex, there was an implied normalisation of a wider ‘hook up culture’ which involved meeting people for sex, and the role that digital technology, particularly apps, played in facilitating hooking up and chemsex:
‘This is the gay life on social media—you are only ever two sentences away from sex or to getting sex.’ ( 30 )
Pressures of the ‘gay scene’. Often when discussing their experience of online hook ups, there was a recognition by some that it came with pressures and anxieties that could act as stressors in their lives. This often related to fears around participants perceived attractiveness and sexual desirability:
‘There’s a lot of anxiety that comes with […] dating on Grindr, at least for myself. Dating apps […] can shatter your self-esteem because we all look better in photos than we do in real life.’ ( 31 )
Not only was this discussed in relation to online hook ups or dating, but as a more pervasive pressure and fear of negative judgement that existed within queer. There was a perception by some around how current ‘homonormative’ codes of masculinity acted as a distal pressure that was crystalised when participants entered queer space, either physical or online.
Minority stress
Participants also discussed external sources of stress that could be characterised as minority stress. Some participants spoke of how they continued to experience stigma and discrimination because of their sexuality. Whilst the gay scene could come with its challenges, there was a recognition that it offered a space where people could express themselves and their sexuality in a way that was not possible in a heteronormative world.
Changing nature of gay spaces and ways of socialising
Many participants spoke about the changing nature of queer spaces and the ways in which MSM socialise. Participants reflected on a shift from clubs and public spaces toward meeting in private settings, such as people’s homes, often facilitated through use of apps, leading to a sense of the diminishing relevance of clubs, bars, and pubs as spaces for MSM to meet:
‘… people don’t need to go out to meet people. […] because we’re all living in Lambeth so we all fucking know each other. We can all get each other on [app]. There’s a dealer there, there, there and there. We don’t need the clubs.’ ( 7 )
Geography
Implicit within some people’s accounts of their chemsex use was the role of geography, and in particular the importance of the city and gay spaces within it, as either the context in which chemsex happens or as a distal driver behind people’s use. These gay spaces seemed important in attracting a large collection of MSM people, as well as bars, pubs, clubs, and sex-on-premises venues, which facilitated access to other MSM people, improved access to drugs, as well as fostered the cultural context in which drugs and sex was commonplace and accepted.
‘… then you come to Vauxhall and you’re just hanging out, there’s just so much temptation, and you go on Grindr and there’s a really good-looking guy inviting you over and you just kind of fall into the circle of people and behaviour. It becomes something you enjoy and then it becomes hard to get out.’ ( 25 )
General drug use
Whilst drug use was predominantly discussed in relation to sex, some participants also spoke about their use of drugs more generally, including the changing and varied nature of their drug use, and how their use of drugs was not solely in relation to sex.
‘I suppose I've grown up on a culture of ecstasy and, obviously, speed and acid and that, so that was back in the day. That's the reason why I would take it, you know, because of the lights and the music and people and then it, sort of, just gradually over the years been into a sort of sexual thing.’ ( 8 )
Participants spoke about the use of different drugs in different settings for different reasons, such as using cocaine or MDMA when going to nightclubs so that people could dance or stay awake for longer, or at friends’ homes to enhance social interactions. For some, the setting influenced the experience of the drug itself, such that the use of methamphetamine in a club rarely led to sexual activity as well as shaping what drugs were seen as acceptable and how they were taken, for example ecstasy/MDMA or cocaine were seen as more socially acceptable in a club compared to injecting crystal methamphetamine. There was also a sense that preferences for drugs naturally changed over time, with some discussing how there was a shift from alcohol as the dominant substance to ecstasy/MDMA and cocaine to GBH/GHB through to mephedrone and methamphetamine. The introduction of new drugs intersected with or contributed to the changing motivations for drug use:
‘Before, we used to go out, and we’d take drugs to keep going at after-parties. It was for partying. Sex wasn’t the main reason.’ (32).
Theme 3: the chemsex experience
Enhanced sexual experiences
There was an overwhelming sense that the sex was better when using drugs –it lasted longer, felt better, and there was a sense of the overall experience as more intense, physically, psychologically, and sexually. For some, the pleasure was almost indescribable and meant that chemsex was somehow inherently different or unique compared to sober sex
‘[on mephedrone] It was the best sex I ever had. Really the best orgasm I’d had. I used to say it was like the heavens opened and it was like the light came down when I had an orgasm. Because it was that intense on drugs, it really was, I’ve never experienced that sober’. ( 13 )
Physiological aspects of chemsex
In describing the increase in pleasure and satisfaction with sex, participants mainly spoke of the ability to perform better physically and having significantly increased libido
‘you feel you want to have sex all the time, you like that. With no effort, you have a great libido, you want to fuck everyone.’ ( 32 )
Physical performance related to how drugs improved stamina and increased energy levels, helped delay orgasms as well as the ability to have multiple orgasms. The improved physical performance and increase in libido were not simply convenient by-products of drug taking, but for many was greatly valued and an important reason behind their drug use:
‘[I use crystal methamphetamine] for sex… Definitely you can go longer—definitely I have had 11–15 hours sessions—and it makes you want more and you are turned on totally. Or at least I am…I use it definitely for sex!’ ( 20 )
For a minority, the drugs enabled them to overcome health-related challenges that impaired their sex lives, including loss of libido, pain and fatigue, the effects of aging, and to counteract the side effects of HIV medication.
‘I don’t have a sex drive any longer. It’s one of the reasons why I started slamming chems because when I slam, I get horny.’ ( 13 )
Psychological aspects of chemsex
Many participants described how the use of drugs allowed them to ‘let go’ and push their limits sexually
‘I had a crazy good time with slam [injecting drugs, typically crystal methamphetamine]. Even in regard to my sexual practices, there’s no more barriers, you always want to push your limits further, but there are no limits.’ ( 9 )
Participants described how they were more able to explore their sexuality in an almost completely unimpeded way. Participants reported that they felt sexually less inhibited and able to engage in more diversified sexual practices, which for many would not have felt possible sober People also reported an improved sense of sexual and psychological self-confidence.
The psychological advantages that drugs conferred also meant that the relational aspects of sex and romantic experiences were intensified. Chemsex allowed for the intensification of romantic experiences and shared intimacy between people:
‘Having him in my arms, suddenly I was comforted and I felt so light. It was a feeling of complete well-being. He was cute, and thoughtful. I was too. We pleasured each other and we only wanted the best for one another. It was a special moment.’ ( 33 )
Psychological motivators for chemsex
Many participants revealed that they carried some sexual, inter, and intrapersonal insecurity. In particular, how low self-esteem and insecurity about their body and perceived desirability had a significant negative effect on their ability to initiate and enjoy sex:
‘I think when I was using drugs I did not have body issues. I did not think, I am feeling a bit too fat or feeling that I do not really feel that attractive so it reduces inhibitions physically and psychologically in terms of having sex and with people you would not feel comfortable, like, having sex with normally.’ ( 13 )
These anxieties could become crystalised or brought to the forefront when navigating hookups (sex) with people they had not met before, and drugs allowed for the management of these concerns:
‘there’s a lot of anxiety that comes with actually meeting the person and, you know, expectations. At least for me, I worried a lot with, like, “Oh, what if they don’t think I look like I’m the same person?” Or, like—and I know my friends also have gotten really bad comments. Like, “Oh, you’re bigger in person,” or things like that […] I think I would need help from … some substances […] to get over those anxieties […] about the sex […] because when you talk about trust and you … I think alcohol and I think weed and stuff like that, it kind of just skirts those problems away. […] It’s not an issue anymore.’ ( 31 )
Some participants recognised that chemsex was a type of escapism, allowing them to escape from the pressures and banality of life At the more extreme end, participants recognised that chemsex was used as a means of managing or overcoming psychological distress The nature and cause of the psychological distress varied, with participants reflecting on their sense of loneliness, depression, the emotional consequences of ending a relationships, work and family stresses, and managing the long-term consequences of trauma and marginalisation as a sexual minority.
Perceptions, experiences, and expectations
Perceived prevalence
Many participants reflected on how widespread they believed chemsex was within MSM communities. Whilst the perceived prevalence was not universally shared, some people perceived chemsex as normalised, with some even perceiving it as an inherent part of what MSM men do.
‘It is a kind of gay men aggregation rite involving sex and drugs.’ ( 34 )
Initiation into chemsex
Participants spoke about the variety of ways that they started using drugs when having sex A common narrative related to the offer of drugs through sexual partners, but also friendships, and being in situations, such as saunas or parties, where they were offered drugs with the intention of having sex. Many participants also described a sense of curiosity around chemsex, with the decision to try it either a conscious decision or more opportunistic in nature, often as a result of being offered drugs by a sexual partner. Some participants spoke of more significant personal stressors or events, such as the end of relationships, or moving to a new city. People’s relationships with drugs before chemsex varied, some had not used drugs at all, whilst others had much more developed drug histories and saw new chemsex-related drugs as the evolution of their drug use.
Organising chemsex
Many people discussed how chemsex was organised. In particular, participants discussed the role of digital technology, including using geo-spacial networking apps as a means of accessing drugs and sexual partners. Alternatively, participants would go to saunas, and some people discussed how chemsex was organised through existing social networks
‘Right now I probably have a network of around 30 people in Madrid who I can meet to practise chemsex with, and they're guys I've known for three years, and in turn we have other people we know in common.’ ( 15 )
Relationship between sex and drugs
Within some participant narratives, a distinction was made between those whose use of drugs was primarily sexual and those whose sexual effects were secondary or only one reason for why they used drugs.
‘Like, I had sex on gear, but it was never like “let's have sex and gear”.’ ( 8 )
Although some participants clearly saw drugs and sex as inextricably linked, this was not universally shared, and participants described a more fluctuating and variable relationship between their use of drugs and its relationship with sex. Some spoke of a gradual transition in their desire to use drugs for sex, this was expressed both longer-term as well as over the course of a single evening. For some they derived pleasure in taking drugs and this was a more primary motivator behind their drug use, for others, it is a means of enhancing social situations, improving concentration, and maintaining energy levels.
Social aspects of chemsex experiences
Within the narratives of participants was the importance of the social aspects to chemsex, where MSM men could meet, develop or continue friendships, dance, and relax together. Central to this was the idea that chemsex settings often offered people a space of acceptance, safety, belonging, and community.
‘The feeling of sharing, of coming together with others, belonging to a group that recognises itself as a group.’ ( 32 )
Theme 4: harms, saying safe, and stopping chemsex
Harms and risks
Within the narratives of participants, there was a recognition that chemsex came with potential risks as well as acknowledging that it had caused harm to themselves and/or others. Differing recognition of needs and outcomes. For many participants, there was recognition that the potential risks or harms associated with chemsex varied and severity. Harm and risk were complicated ideas that, for participants, were predicated by a range of factors, such as the types, frequency, and quantities of drugs used and the method of drug delivery, how actively ‘in control’ they were over their use, and the types of sex that they engaged in.
Coercion, consent, and sexual assault
A major theme within the narratives of participants related to witnessing examples of coercion, ambiguities around establishing consent, and sexual assault Reports of coercion often relate to subtle use of power to encourage people to acquiesce to sexual practises and to take drugs. For some there was an ‘economy of drug use’ where people would engage in certain sexual acts with others in exchange for drugs. The extent to which this was an equal decision by two people was not clear, but came with an implied sense of subtle coercion. Establishing and withdrawing consent during chemsex could be complicated by the effects of drug use on cognition and decision making.
Loss of control
Participants spoke of the potential for or experience of loss of control over chemsex. This loss of control was often characterised in relation to escalating and excessive drug use and chemsex to the point that it either dominated their lives or negatively impacted multiple aspects of their lives. For some, chemsex could become ‘all-consuming’ to the point that it was difficult to stop or remain in control. Some participants reported how drugs could lead to a loss of consciousness, which would vary in how long it would last.
Physical, psychological, social, and occupational harms
In discussing the negative psychological consequences of their drug use, participants reported a range of problems including difficulties associated with the aftermath of drug use (‘comedowns’) including low mood, lethargy, feeling run down, vulnerable, and questioning their decision, along with feeling on edge, highly anxious, depressed, suicidal, as well as paranoia, auditory and visual hallucinations, and psychosis
‘The after … the sense of guilt and emptiness … I had thoughts of death…’ (28yo, predominantly gay) ( 35 )
Some participants also felt that their use of chems had a negative effect on their relationships, both friendships and romantic, this could include the loss of relationships, the end of romantic relationships, and difficulties establishing a romantic relationship. Problematic chemsex could also have a negative effect on people’s work, such that they struggled to concentrate and missed work or education. Participants also discussed the negative effect that chemsex had on their physical health. Some of this was related to the cumulative effects of heavy drug use, but more typically it was related to physical damage due to of sex and drug use. Participants reported rectal trauma or penile abrasions and drug-related damage included collapsed veins and muscle damage.
Sexual health and satisfaction
The negative consequences of chemsex in relation to participants sexual lives varied considerably from bad, painful or unsatisfactory sex to engaging in risky sexual practises, contracting STIs, and sexual dysfunction. Some participants spoke of how bad, painful, and unsatisfactory sex could be while on drugs. Participants spoke of a type of ‘sexual selfishness’ that meant the qualities of sex that they valued, such as heightened relational and emotional connection, were not obtained. Instead, some participants reported experiences where the desire for gratification was at the expense of heightened emotional intimacy that was a key motivator for engaging in chemsex. Many participants discussed how drugs could result in sexual dysfunction, particularly difficulties in getting or maintaining an erection.
Although some reported regret or concerns about engaging in riskier sexual behaviours when having chemsex, this was not universally shared. Some participants reported how their perception of risk and what they were willing to do changed over time, such that they had made the decision to not use condoms, which was unrelated to their drug use. In addition to this, others were of the belief that contracting STIs was not a significant concern. This took on added significance in the context of the use of pre- (PREP) and post-exposure prophylaxis (PEP) for preventing HIV.
Staying safe
Individual harm reduction strategies in relation to drugs
Participants reported a range of strategies that they engaged in to reduce the risk to themselves. By far the most common strategies related to limiting the frequency and timing of chemsex and setting limits on their drug use, including limiting the type and/or quantity of drugs they used. Participants also reported a range of safe drug practises, including using clean needles, not sharing needs, or use of individual straws to snort drugs.
Shared responsibility when taking drugs
Participants also spoke about a shared sense of responsibility and mutual help when it came to drug use. This often involved looking out and caring for those who had perhaps taken too many drugs, having people more experienced with certain drugs supporting those who were more novice users, as well as having shared responsibility and awareness of what drugs people had taken, when, and in what quantity through a written or electronic document that recorded the names, times, and quantity of drugs taken by individuals.
Sexual health
Participants reported using condoms when having sex, having open discussions about their sexual health status which drugs sometimes facilitated, as well as using PREP and PEP to limit the risk of contracting HIV. Whilst participants were aware that the drugs could influence how stringently these practises were adhered to, participants reported being able to stick to their boundaries around what types of sex they wanted and doing it in a way that they felt limited their risk
‘He said, “Listen, you can’t fuck me with that dick because it’s got a condom on it.” […] And I said, “I’m always going to wear this condom, no matter what.”’ ( 36 )
Stopping chemsex
When it came to stopping chemsex, participants reflected on how challenging this could be. There was an awareness of how much they liked having chemsex alongside the harms that it could cause, meaning that for some, they were unsure if they could, or wanted, to stop. While there was little research into relapse, a few participants spoke of how they would have a period of deliberate abstinence, but this would not be sustained, and they would relapse. Whilst there was no substantial literature around life after stopping chemsex, there was a narrative of needing to mourn what was lost from stopping. In particular, participants spoke of mourning their sexuality and the difficulty of having sober sex, which could not match the intensity of chemsex sessions. Stopping chemsex also required a significant change to, potential loss of, and need to rebuild romantic relationships and friendships that were not connected with chemsex.
Seeking professional support
When discussing chemsex, some participants discussed their experience of seeking professional support and/or the type of support they felt they needed. In discussing their experience of seeking support around chemsex, some participants discussed issues with struggling to access services. For some, this was related to simply not knowing where to go for support. While some participants mentioned mental health and drug addiction services, there were concerns about whether these services were appropriate for their needs. The most consistent concern reported by participants was that traditional services lacked cultural awareness around both MSM health needs and sexualised drug use, which could result in some feeling judged either for their drug use or sexuality, or needing to explain chemsex to professionals who lacked an understanding of the interaction between drugs, sex, and MSM health needs.
When discussing the type of support required, participants recognised the need for more support that was culturally appropriate and integrated spanning sexual, physical, and mental health as well as drug addiction, offered clear and accessible information, recognised the varying health needs of those who engage in chemsex, and was delivered in a non-judgemental manner. Whilst professional support was valued, there was a sense from some participants that support also came outside health services, including community-based organisations.
Discussion
This is the first systematic review of qualitative studies of chemsex experiences of MSM and the theoretical frameworks that have been used to conceptualise chemsex. Past reviews (4–6) have primarily focused on quantitative research, with an emphasis on understanding key characteristics and health consequences of chemsex. Although Maxwell et al. (5) review explored the chemsex participants’ expectations, this focused on proximal expectations, particularly in relation to the effect of drugs on sex. A mixed-methods systematic review by Lafortune et al. (66) examined qualitative research, but was limited to psychological and interpersonal factors around chemsex and only included a limited number of studies.
Some of the results confirm findings from previous systematic reviews. In understanding the emergence of chemsex as a phenomenon, research focused on characterising chemsex in relation to the types of drugs use, how they are consumed, where chemsex takes place, the number of sexual partners, and the role of technology in facilitating chemsex. However, the key findings from our review also highlight the importance of situating chemsex within a wider social, cultural, and geographic context. This includes distal factors such as the changing nature of gay or queer spaces and the evolution of the means by which MSM communicate, socialise and congregate. The emergence of digital technologies has intersected with other cultural factors within queer culture, including casual sex (‘hook up culture’), general drug use, and for some, repudiation of hetero-and homo-normative expectations (11, 37). Although chemsex has been seen as a distinct phenomenon, it is important to situated its emergence within pre-existing social and cultural dynamics.
The results of this review add evidence to the claim that a central proximal motivator for chemsex is the effects that drugs have on perceptions of sex, both physically and psychologically (5). However, our results also suggest that there are complex and multiple psychosocial factors that may directly and indirectly influence why a person may have chemsex, which go beyond the immediate effects of drugs on perceptions of sex. Psychologically, some people who have chemsex reported how it helped overcome low self-esteem, insecurity about their body and perceived desirability, anxieties about sex, and psychological distress. This was also in the context of need for acceptance and belonging from both within and outside of the queer community, highlighting the complex struggles for some of navigating life as someone from a sexual minority and the potential role of structural social issues including marginalisation and homophobia. Importantly, there is an absence of research which explores these issues from an intersectional lens, including research among gender and ethnically diverse populations given the unique challenges these populations can face (38). At present, there is limited research beyond qualitative studies (66) that explore a broad range of psychological factors that may confer greater risk, either as a risk factor for problematic chemsex and/or negative health outcomes, or act as protective against such consequences. Research has predominantly focused on the relationship between mental health problems, particularly anxiety and depression, and chemsex (39), but there is a need to broaden the focus to look at a range of other psychological factors, including issues with body image, self-esteem, community and belonging, sexual insecurities, and strategies for managing psychological distress. There is emerging evidence that for some people, chemsex is a strategy for managing emotional dysregulation that arises in the context of adverse childhood experiences (40, 41). Our findings, combined with this fledgling literature, suggest that there are complex and multifaceted psychological drivers behind chemsex, which require further exploration. Furthermore, given that not all chemsex is problematic, identifying the individual psychological differences between those with problematic versus non-problematic use would help to identify areas of resilience that may be protective against negative consequences.
The findings also help to broaden the perspective on supporting the health needs of those who report chemsex. Consistent with previous reviews, we found that there can be negative health consequences of problematic chemsex in relation to mental health, substance misuse and loss of control, increased risk of STIs, dependence on drugs, and negative physical effects from cumulative heavy drug use (4–6). However, our findings highlight that people adopt a range of individual and collective strategies to reduce harm and risk in relation to drugs. Furthermore, risk in relation to drugs and sex had different meanings for different participants, and perceptions could change over time. This has added significance in relation to the prevalence of pre-pre-exposure prophylaxis (PREP) and post-exposure prophylaxis (PEP) for HIV. Understanding the individual experiences and decision making of people in relation to ‘health risks’ has important implications for how people who have chemsex are supported. There is a recognition within the wider chemsex literature to move beyond a ‘risk and health outcomes paradigm’ (8, 41, 65) and adopt an approach that recognises the resilience of those who engage in chemsex (69), including recognising and promoting the strategies used to reduce potential harm. Finally, this review brings together qualitative research on how people stop using chemsex and seek professional support for their use, which remains an under-researched aspect of chemsex. Supporting people to stop or move toward safer chemsex needs to consider a broad and holistic understanding of needs (42), including issues of wellbeing, psychosexual factors given the potential challenges of sober-sex for some people, and help to develop social networks that foster a sense of belonging outside of chemsex (43). Health services and communities that may work directly with or encounter people who engage in chemsex need to be supported in their understanding of the needs of this population, with suitable cultural understanding and awareness. This highlights the need for further research into how this was achieved and what interventions could be developed to support people who wish to stop or to practise chemsex more safely (44).
The second aim of this review was to explore the conceptual and theoretical paradigms adopted in exploration of chemsex. Although chemsex can be viewed through different disciplinary and methodological lenses, much of the qualitative literature omitted reference to underlying theoretical perspectives that informed their conceptualisation of chemsex as a phenomenon. Nevertheless, many of these papers framed chemsex within a health and risk paradigm, raising concerns about the potential negative health consequences. While acknowledgment of the potential health implications of problematic chemsex is required, it is important that a theoretical understanding of who, when, and how chemsex may become problematic is incorporated. Furthermore, a more sophisticated theoretical understanding of chemsex, which incorporates a range of social, cultural, and psychological factors, is needed to guide research and inform the response to chemsex.
Implications
The findings of this review have implications for those working with people who engage in chemsex. There is now substantial evidence that a primary motivator for having chemsex is how it enhances sex, yet the motivation to have chemsex is influenced by other psychological, social, and cultural factors. This necessitates a comprehensive assessment of people’s needs that includes an individualised assessment of the perceived benefits, drivers, and consequences, that can come with chemsex. This review suggests that important psychological factors - namely concerns around body image and self-perception, often in the context of ongoing marginalisation as a sexual minority group - may reflect important areas of assessment, and potentially intervention, drawing on evidence-based interventions at both the individual and public health levels. Participants highlighted the challenges that came with accessing support, principally confusion about where to seek help, and feeling that services were not fully able to meet their needs. This raises important questions about how best to develop services for people seeking help related to chemsex. There is now a recognition of the need for chemsex-specific services to be developed, either as standalone services or embedded within existing services, that offer comprehensive and tailored services that can meet the psycho-sexual, mental health, substance misuse and sexual health needs of people who have chemsex (45, 46); this includes the need for co-production of service design and delivery, often in tandem with existing charity and third sector organisation that have a trusted reputation amongst the community (45). Future research should focus on understanding pathways into chemsex, how and when it becomes problematic, and how best to support people when chemsex is associated with problems typically associated with polysubstance misuse (47). Finally, there is a long history of using a range of theories, in particular those from the behavioural sciences, to understand and support MSM with regard to their health and wellbeing, yet chemsex remains an area of under theorised.
Strengths and limitations
One strength of this review is the narrative synthesis using qualitative literature only. This is important because understanding the theoretical frameworks that conceptualise chemsex provides a basis for consistency across future research and can be utilised for designing training to provide to professionals. At present, there is a notable absence of a theoretical understanding of chemsex, as highlighted by the small number of studies that explicitly stated their theoretical framework.
One potential limitation is that the review included literature in English only. This reduces the scope of the review and the impact and reach that it may have. The review only included MSM, thus limiting the transferability to other people who engage in chemsex.
Conclusion
This is the first systematic review of the qualitative literature on the chemsex experiences of MSM and the first to explore theoretical frameworks that have been used to conceptualise chemsex. The results add further understanding of some of the key characteristics of chemsex, while highlighting important psycho-social factors that inform why people engage in chemsex, as well as addressing specific healthcare care needs that may need to be met. Further research is needed to better understand the psychosocial factors that may shape why people have chemsex, their experiences, and outcomes.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
EM: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. AC: Formal analysis, Investigation, Writing – review & editing, Writing – original draft. TN: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. CW: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. RV: Investigation, Supervision, Writing – review & editing, Writing – original draft. CL: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Giorgetti, R, Tagliabracci, A, Schifano, F, Zaami, S, Marinelli, E, and Busardò, FP. When "Chems" meet sex: a rising phenomenon called "ChemSex". Curr Neuropharmacol. (2017) 15:762–70. doi: 10.2174/1570159X15666161117151148
2. McCall, H, Adams, N, Mason, D, and Willis, J. What is chemsex and why does it matter? BMJ. (2015) 351:h5790. doi: 10.1136/BMJ.H5790
3. Bourne, A, Reid, D, Hickson, F, Torres-Rueda, S, Steinberg, P, and Weatherburn, P. “Chemsex” and harm reduction need among gay men in South London. Int J Drug Policy. (2015) 26:1171–6. doi: 10.1016/j.drugpo.2015.07.013
4. Edmundson, C, Heinsbroek, E, Glass, R, Hope, V, Mohammed, H, White, M, et al. Sexualised drug use in the United Kingdom (UK): a review of the literature. Int J Drug Policy. (2018) 55:131–48. doi: 10.1016/J.DRUGPO.2018.02.002
5. Maxwell, S, Shahmanesh, M, and Gafos, M. Chemsex behaviours among men who have sex with men: a systematic review of the literature. Int J Drug Policy. (2019) 63:74–89. doi: 10.1016/J.DRUGPO.2018.11.014
6. Tomkins, A, George, R, and Kliner, M. Sexualised drug taking among men who have sex with men: a systematic review. Perspect Public Health. (2019) 139:23–33. doi: 10.1177/1757913918778872
7. Ahmed, AK, Weatherburn, P, Reid, D, Hickson, F, Torres-Rueda, S, Steinberg, P, et al. Social norms related to combining drugs and sex (“chemsex”) among gay men in South London. Int J Drug Policy. (2016) 38:29–35. doi: 10.1016/j.drugpo.2016.10.007
8. Drysdale, K, Bryant, J, Holt, M, Hopwood, M, Dowsett, GW, Aggleton, P, et al. Destabilising the ‘problem’ of chemsex: diversity in settings, relations and practices revealed in Australian gay and bisexual men’s crystal methamphetamine use. Int J Drug Policy. (2020) 78:102697. doi: 10.1016/j.drugpo.2020.102697
9. Flores-Aranda, J, Goyette, M, Aubut, V, Blanchette, M, and Pronovost, F. Let’s talk about chemsex and pleasure: the missing link in chemsex services. Drugs Alcohol Today. (2019) 19:189–96. doi: 10.1108/DAT-10-2018-0045
10. Graf, N, Dichtl, A, Deimel, D, Sander, D, and Stöver, H. Chemsex among men who have sex with men in Germany: motives, consequences and the response of the support system. Sex Health. (2018) 15:151–6. doi: 10.1071/SH17142
11. Hakim, J. The rise of chemsex: queering collective intimacy in neoliberal London. Cult Stud. (2019) 33:249–75. doi: 10.1080/09502386.2018.1435702
12. Smith, V, and Tasker, F. Gay men’s chemsex survival stories. Sex Health. (2017) 15:116–22. doi: 10.1071/SH17122
13. Weatherburn, P, Hickson, F, Reid, D, Torres-Rueda, S, and Bourne, A. Motivations and values associated with combining sex and illicit drugs (chemsex) among gay men in South London: findings from a qualitative study. Sex Transm Infect. (2016) 93:203–6. doi: 10.1136/sextrans-2016-052695
14. Bryant, J, Hopwood, M, Dowsett, GW, Aggleton, P, Holt, M, Lea, T, et al. The rush to risk when interrogating the relationship between methamphetamine use and sexual practice among gay and bisexual men. Int J Drug Policy. (2018) 55:242–8. doi: 10.1016/J.DRUGPO.2017.12.010
15. Santoro, P, Rodríguez, R, Morales, P, Morano, A, and Morán, M. One “chemsex” or many? Types of chemsex sessions among gay and other men who have sex with men in Madrid, Spain: findings from a qualitative study. Int J Drug Policy. (2020) 82:102790. doi: 10.1016/j.drugpo.2020.102790
16. Halkitis, PN, Parsons, JT, and Stirratt, MJ. A double epidemic: crystal methamphetamine drug use in relation to HIV transmission among gay men. J Homosex. (2001) 41:17–35. doi: 10.1300/J082V41N02_02
17. Stuart, D. Chemsex: origins of the word, a history of the phenomenon and a respect to the culture. Drugs and Alcohol Today. (2019) 19:3–10. doi: 10.1108/DAT-10-2018-0058
18. Thomas, J, and Harden, A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol. (2008) 8:45. doi: 10.1186/1471-2288-8-45
19. Pearson, A. Balancing the evidence: incorporating the synthesis of qualitative data into systematic reviews. JBI Reports. (2004) 2:45–64. doi: 10.1111/j.1479-6988.2004.00008.x
20. Halkitis, PN, Fischgrund, BN, and Parsons, JT. Explanations for methamphetamine use among gay and bisexual men in new York City. Subst Use Misuse. (2005) 40:1331–45. doi: 10.1081/JA-200066900
21. Parry, C, Petersen, P, Dewing, S, Carney, T, Needle, R, Kroeger, K, et al. Rapid assessment of drug-related HIV risk among men who have sex with men in three South African cities. Drug Alcohol Depend. (2008) 95:45–53. doi: 10.1016/j.drugalcdep.2007.12.005
22. Pienaar, K, Murphy, DA, Race, K, and Lea, T. Drugs as technologies of the self: enhancement and transformation in LGBTQ cultures. Int J Drug Policy. (2020) 78:102673. doi: 10.1016/j.drugpo.2020.102673
23. Dew, BJ. Toward a better understanding of non-addicted, methamphetamine-using, men who have sex with men (MSM) in Atlanta. Open AIDS J. (2010) 4:141–7. doi: 10.2174/1874613601004030141
24. Choi, KWY, Choi, EPH, Chow, EPF, Wan, EYF, Wong, WCW, Wong, JYH, et al. The experience of using dating applications for sexual hook-ups: a qualitative exploration among HIV-negative men who have sex with men in Hong Kong. J Sex Res. (2021) 58:785–94. doi: 10.1080/00224499.2021.1886227
25. Pollard, A, Nadarzynski, T, and Llewellyn, C. Syndemics of stigma, minority-stress, maladaptive coping, risk environments and littoral spaces among men who have sex with men using chemsex. Cult Health Sex. (2018) 20:411–27. doi: 10.1080/13691058.2017.1350751
26. Jaspal, R. Chemsex, identity processes and coping among gay and bisexual men. Drugs Alcohol Today. (2021) 21:345–55. doi: 10.1108/DAT-12-2020-0083
27. Souleymanov, R, Brennan, DJ, Logie, CH, Allman, D, Craig, SL, and Halkitis, PN. Party-n-play and online information and communication technologies: a socio-linguistic perspective. Sexualities. (2020) 24:388–408. doi: 10.1177/1363460720932379
28. Souleymanov, R, Brennan, DJ, Logie, C, Allman, D, Craig, SL, and Halkitis, PN. Pleasure and HIV biomedical discourse: the structuring of sexual and drug-related risks for gay and bisexual men who party-n-play. Int J Drug Policy. (2019) 74:181–90. doi: 10.1016/j.drugpo.2019.09.015
29. Race, K, Murphy, D, Pienaar, K, and Lea, T. Injecting as a sexual practice: cultural formations of ‘slamsex.’. Sexualities. (2021) 26:1–18. doi: 10.1177/1363460720986924
30. Van Hout, MC, Crowley, D, O’Dea, S, and Clarke, S. Chasing the rainbow: pleasure, sex-based sociality and consumerism in navigating and exiting the Irish Chemsex scene. Cult Health Sex. (2019) 21:1074–86. doi: 10.1080/13691058.2018.1529336
31. Parent, N, Ferlatte, O, Milloy, MJ, Fast, D, and Knight, R. The sexualised use of cannabis among young sexual minority men: “I’m actually enjoying this for the first time.”. Cult Health Sex. (2020) 23:883–98. doi: 10.1080/13691058.2020.1736634
32. Gaissad, L, and Velter, A. Getting high to get laid.” drugs and gay sex under influence. Theol Sex. (2019) 28:e48–53. doi: 10.1016/j.sexol.2019.06.007
33. Milhet, M, Shah, J, Madesclaire, T, and Gaissad, L. Chemsex experiences: narratives of pleasure. Drugs Alcohol Today. (2019) 19:11–22. doi: 10.1108/DAT-09-2018-0043
34. Nimbi, FM, Rosati, F, Esposito, RM, Stuart, D, Simonelli, C, and Tambelli, R. Chemsex in Italy: experiences of men who have sex with men consuming illicit drugs to enhance and prolong their sexual activity. J Sex Med. (2020) 17:1875–84. doi: 10.1016/j.jsxm.2020.07.001
35. Nimbi, FM, Rosati, F, Esposito, RM, Stuart, D, Simonelli, C, and Tambelli, R. Sex in Chemsex: sexual response, motivations, and sober sex in a Group of Italian men who Have sex with men with Sexualized Drug use. J Sex Med. (2021) 18:1955–69. doi: 10.1016/j.jsxm.2021.09.013
36. Bourne, A, Reid, D, Hickson, F, Torres-Rueda, S, Steinberg, P, and Weatherburn, P. Illicit drug use in sexual settings ('chemsex’) and HIV/STI transmission risk behaviour among gay men in South London: findings from a qualitative study. Sex Transm Infect. (2015b) 91:564–8. doi: 10.1136/sextrans-2015-052052
37. Mowlabocus, S. Fucking with homonormativity: the ambiguous politics of chemsex. Sexualities. (2021) 26:585–603. doi: 10.1177/1363460721999267
38. Hibbert, MP, Hillis, A, Brett, CE, Porcellato, LA, and Hope, VD. A narrative systematic review of sexualised drug use and sexual health outcomes among LGBT people. Int J Drug Policy. (2021) 93:103187. doi: 10.1016/j.drugpo.2021.103187
39. Íncera-Fernández, D, Gámez-Guadix, M, and Moreno-Guillén, S. Mental health symptoms associated with sexualized drug use (Chemsex) among men who have sex with men: a systematic review. Int J Environ Res Public Health. (2021) 18:13299. doi: 10.3390/ijerph182413299
40. González-Baeza, A, Barrio-Fernández, P, Curto-Ramos, J, Ibarguchi, L, Dolengevich-Segal, H, Cano-Smith, J, et al. Understanding attachment, emotional regulation, and childhood adversity and their link to Chemsex. Subst Use Misuse. (2023) 58:94–102. doi: 10.1080/10826084.2022.2148482
41. Tan, RKJ, Phua, K, Tan, A, Gan, DCJ, Ho, LPP, Ong, EJ, et al. Exploring the role of trauma in underpinning sexualised drug use (‘chemsex’) among gay, bisexual and other men who have sex with men in Singapore. Int J Drug Policy. (2021) 97:103333. doi: 10.1016/j.drugpo.2021.103333
42. Bakker, I, and Knoops, L. Towards a continuum of care concerning chemsex issues. Sex Health. (2018) 15:173–5. doi: 10.1071/SH17139
43. Nagington, M, and King, S. Support, care and peer support for gay and bi men engaging in chemsex. Health Soc Care Community. (2022) 30:e6396–403. doi: 10.1111/hsc.14081
44. Strong, C, Huang, P, Li, CW, Ku, SWW, Wu, HJ, and Bourne, A. HIV, chemsex, and the need for harm-reduction interventions to support gay, bisexual, and other men who have sex with men. Lancet HIV. (2022) 9:e717–25. doi: 10.1016/S2352-3018(22)00124-2
45. Campbell, T, Gurreri, N, Margetts, A, Mundy, E, and Rutter, S. Developing chemsex intervention services: guidance for psychological care provision. Leicester: British Psychological Society (2024).
46. Mundy, E, Margetts, A, Vosper, J, Zetler, S, Revez, A, Hilton, S, et al. ‘Sex, drugs and clinical psychology: Developing chemsex services’, Clinical Psychology Forum. British Psychological Society. 382:70–77. doi: 10.53841/bpscpf.2024.1.382.70
47. Rinaldi, R, Bersani, G, Marinelli, E, and Zaami, S. The rise of new psychoactive substances and psychiatric implications: a wide-ranging, multifaceted challenge that needs far-reaching common legislative strategies. Hum Psychopharmacol. (2020) 35:e2727. doi: 10.1002/hup.2727
48. Balán, IC, Carballo-Diéguez, A, Ventuneac, A, and Remien, RH. Intentional condomless anal intercourse among Latino MSM who meet sexual partners on the internet. AIDS Educ Prevent. (2009) 21:14–24. doi: 10.1521/AEAP.2009.21.1.14
49. Chartier, M, Araneta, A, Duca, L, McGlynn, LM, Gore-Felton, C, Goldblum, P, et al. Personal values and meaning in the use of methamphetamine among HIV-positive men who have sex with men. Qual Health Res. (2009) 19:504–18. doi: 10.1177/1049732309333018
50. Currin, JM, Hubach, RD, and Croff, JM. Sex, drugs, & rurality: a brief qualitative analysis of rural gay and bisexual men’s substance use sex expectancies. J Subst Abus. (2019) 24:381–7. doi: 10.1080/14659891.2019.1581284
51. Deimel, D, Stöver, H, Hößelbarth, S, Dichtl, A, Graf, N, and Gebhardt, V. Drug use and health behaviour among German men who have sex with men: results of a qualitative, multi-Centre study. Harm Reduct J. (2016) 13:36–11. doi: 10.1186/s12954-016-0125-y
52. Dennermalm, N, Scarlett, J, Thomsen, S, Persson, KI, and Alvesson, HM. Sex, drugs and techno – a qualitative study on finding the balance between risk, safety and pleasure among men who have sex with men engaging in recreational and sexualised drug use. BMC Public Health. (2021) 21:863–12. doi: 10.1186/s12889-021-10906-6
53. Green, AI, and Halkitis, PN. Crystal methamphetamine and sexual sociality in an urban gay subculture: an elective affinity. Cult Health Sex. (2006) 8:317–33. doi: 10.1080/13691050600783320
54. Guadamuz, TE, and Boonmongkon, P. Ice parties among young men who have sex with men in Thailand: pleasures, secrecy and risks. Int J Drug Policy. (2018) 55:249–55. doi: 10.1016/j.drugpo.2018.04.005
55. Hawkins, B, Armstrong, HL, Kesselring, S, Rich, AJ, Cui, Z, Sereda, P, et al. Substance us as a mechanism for social inclusion amoung gay, bisexual and other men who have sex with men in Vancouver, Canada. Substa Use Misuse. (2019) 54:1945–55. doi: 10.1080/10826084.2019.1621901
56. Herrijgers, C, Poels, K, Vandebosch, H, Platteau, T, van Lankveld, J, and Florence, E. Harm reduction practices and needs in a belgian chemsex context: findings from a qualitative study. Int J Environ Res Public Health. (2021) 17:1–18. doi: 10.3390/ijerph17239081
57. Hibbert, MP, Germain, JS, Brett, CE, Van Hout, MC, Hope, VD, and Porcellato, LA. Service provision and barriers to care for men who have sex with men engaging in chemsex and sexualised drug use in England. Int J Drug Policy. (2021) 92:103090. doi: 10.1016/j.drugpo.2020.103090
58. Joyce, N, MacNeela, P, Sarma, K, Ryall, G, and Keenan, E. The experience and meaning of problematic ‘G’ (GHB/GBL) use in an Irish context: an interpretative phenomenological analysis. Int J Ment Heal Addict. (2018) 16:1033–54. doi: 10.1007/s11469-017-9851-y
59. Klitzman, R. From “male bonding rituals” to “suicide tuesday”: a qualitative study of issues faced by gay male ecstasy (MDMA) users. J Homosex. (2006) 51:7–32. doi: 10.1300/J082v51n03_02
60. Kubicek, K, McDavitt, B, Carpineto, J, Weiss, G, Iverson, EF, and Kipke, M. Making informed decisions: how attitudes and perceptions affect the use of crystal, cocaine and ecstasy among young men who have sex with men. J Drug Issues. (2007) 37:643–72. doi: 10.1177/002204260703700308
61. Lim, SH, Akbar, M, Wickersham, JA, Kamarulzaman, A, and Altice, FL. The management of methamphetamine use in sexual settings among men who have sex with men in Malaysia. Int J Drug Policy. (2018) 55:256–62. doi: 10.1016/J.DRUGPO.2018.02.019
62. Palamar, JJ, and Halkitis, PN. A qualitative analysis of GHB use among gay men: reasons for use despite potential adverse outcomes. Int J Drug Policy. (2006) 17:23–8. doi: 10.1016/J.DRUGPO.2005.11.002
63. Parsons, JT, Kelly, BC, and Weiser, JD. Initiation into methamphetamine use for young gay and bisexual men. Drug Alcohol Depend. (2007) 90:135–44. doi: 10.1016/J.DRUGALCDEP.2007.02.017
64. Tan, RKJ, Wong, CM, Chen, MIC, Chan, YY, Bin Ibrahim, MA, Lim, OZ, et al. Chemsex among gay, bisexual, and other men who have sex with men in Singapore and the challenges ahead: a qualitative study. Int J Drug Policy. (2018) 61:31–7. doi: 10.1016/j.drugpo.2018.10.002
65. Møller, K, and Hakim, J. Critical chemsex studies: Interrogating cultures of sexualized drug use beyond the risk paradigm. Sexualities, (2023). 26:547–555. doi: 10.1177/13634607211026223
66. Lafortune, D, Blais, M, Mille, G, et al. Psychological and Interpersonal Factors Associated with Sexualized Drug Use Among Men Who Have Sex with Men: A Mixed-Methods Systematic Review. Arch Sex Behav (2021) 50:427–460. doi: 10.1007/s10508-020-01741-8
67. Joanna Briggs Institute. Critical Appraisal Checklist for Systematic Reviews and Research Syntheses. (2017). Available at: https://jbi.global/sites/default/files/2019-05/JBI_Critical_Appraisal-Checklist_for_Systematic_Reviews2017_0.pdf
68. Gibson, JJ. The Theory of Affordances, The Ecological Approach to Visual Perception. Boston: Houghton Mifflin, (1979). Print.
69. Halkitis, PN, and Singer, SN. Chemsex and mental health as part of syndemic in gay and bisexual men. Int J Drug Policy. (2018) 55:180–182. doi: 10.1016/j.drugpo.2018.04.002
Appendix
Keywords: chemsex, sexualised drug use, polydrug use, substance use, men who have sex with men, qualitative, systematic review
Citation: Mundy E, Carter A, Nadarzynski T, Whiteley C, de Visser RO and Llewellyn CD (2025) The complex social, cultural and psychological drivers of the ‘chemsex’ experiences of men who have sex with men: a systematic review and conceptual thematic synthesis of qualitative studies. Front. Public Health. 13:1422775. doi: 10.3389/fpubh.2025.1422775
Edited by:
Yi-lang Tang, Emory University, United StatesReviewed by:
Simona Zaami, Sapienza University of Rome, ItalyBradley Luke Hillier, West London Mental Health NHS Trust, United Kingdom
Copyright © 2025 Mundy, Carter, Nadarzynski, Whiteley, de Visser and Llewellyn. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Carrie D. Llewellyn, Yy5kLmxsZXdlbGx5bkBic21zLmFjLnVr
†ORCID: Tom Nadarzynski, orcid.org/0000-0001-7010-5308
Richard O. de Visser, orcid.org/0000-0003-1174-1499
Carrie Llewellyn, orcid.org/0000-0002-9107-8473