 Jin Young Nam
Jin Young Nam
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 28 March 2025
Sec. Health Economics
Volume 13 - 2025 | https://doi.org/10.3389/fpubh.2025.1411534
Objective: This study aims to examine the association between maternal mortality and childbirth-related medical costs using both unadjusted and adjusted models and to assess the potential reduction in delivery-related medical costs associated with maternal mortality in South Korea.
Methods: This retrospective cohort study used data from the National Health Insurance Service Delivery Cohort Database of South Korea. A total of 7,171,578 participants were included. The outcome measured was delivery-related medical costs associated with maternal mortality. A Generalized Estimating Equation model with a log link and gamma distribution was used to estimate delivery-related medical costs.
Results: The maternal death rates were 9.7 per 100,000 births. The adjusted mean delivery-related medical costs were approximately six times higher in cases with maternal death than in those without ($2,802 vs. $480, p < 0.0001). The total delivery-related medical costs for all women with maternal mortality were approximately $2 million, accounting for 0.06% of total delivery-related medical costs. Although this proportion is relatively small, 83% of the direct medical costs associated with maternal mortality among South Korean women were potentially reducible.
Conclusion: This study found that maternal mortality is associated with significantly higher delivery-related medical costs, nearly six times those of non-maternal mortality cases. Therefore, policymakers should consider reducing costs and improving maternal health outcomes, expanding access to prenatal care for early risk detection and strengthen nationwide maternal health monitoring systems.
Maternal mortality remains a critical public health issue worldwide, despite substantial advancements in medical care. Most cases of maternal mortality are preventable and reducing maternal deaths has been a global health priority for decades (1, 2). However, maternal mortality rates have remained high in several high-income countries. For instance, in 2020, the maternal mortality ratio (MMR) in the United States and South Korea was 23.8 and 11.8 per 100,000 live births, respectively, ranking among the highest in high-income nations (3–6). Although maternal mortality is a relatively rare event in high-income countries, it imposes significant economic and social burdens on individuals and healthcare systems.
Among these burdens, the economic impact of maternal mortality is a crucial yet understudied aspect. The financial burden associated with maternal deaths affects not only the healthcare system but also the families and society at large. Despite this, studies on the economic costs of maternal mortality are scarce due to several limitations: (1) low maternal mortality rates in high-income countries leading to data scarcity (7), (2) a predominant focus on chronic diseases in medical cost research (8), (3) challenges in establishing a causal relationship between maternal mortality and medical costs, (4) a preventive approach in public health research (7), and (5) difficulties in cost comparisons across differences in healthcare systems (9).
While some studies have explored the indirect economic costs of maternal mortality, they were primarily conducted in low-and middle-income countries, such as those examining the household financial burden of maternal deaths in rural areas (10, 11). In high-income countries, a few studies have investigated the economic burden associated with severe maternal morbidity (SMM) (12, 13) or pregnancy-related complication such as preeclampsia, gestational diabetes, and ICU admissions (14–17). These studies have consistently demonstrated that women with SMM or pregnancy-related complications incur significantly higher medical costs compared to those without those. However, very few studies have directly examined the economic burden of maternal mortality itself, particularly in high-income setting.
Despite increasing recognition of this issue, limited research has quantified the direct medical costs of maternal mortality. One study estimated the economic impact of maternal mortality in the United States in 2019 at $30.8 million (8, 14), but no study has comprehensively analyzed the direct medical costs of maternal mortality using long-term, nationwide data in high-income countries.
Therefore, this study aims to examine the association between maternal mortality and childbirth-related medical costs using both unadjusted and adjusted models and to assess the potential reduction in delivery-related medical costs associated with maternal mortality in South Korea, based on a nationwide, 19-year population-based delivery cohort database.
This population-based study used the database of the Korean National Health Insurance Service (NHIS), a single insurer of the entire country’s population, to which approximately 98% of all South Koreans are enrolled (18). The NHIS database retains data on the following: sociodemographic characteristics; healthcare utilization (received services and treatment costs); clinically determined diagnostic codes from the International Classification of Diseases, 10th revision (ICD-10); prescriptions with drug codes; days of prescription; daily dosages (18). The database uses de-identified join keys to link databases while ensuring patient anonymity (18). The study design was reviewed and approved by the Institutional Review Board of Eulji University (IRB Number: EU22-27). The requirement for informed consent was waived as the data did not contain identifiable information.
We extracted data from the NHIS claims databases for all women who delivered in medical institutions in South Korea between 1 January 2003, and 31 December 2021. Childbirth was identified using all inpatient records, including pregnancy-related diagnoses and vaginal or cesarean delivery procedures. The study population included women aged 15–49 years and those who gave birth between 1 January 2003, and 19 November 2021, so that the data on childbirth within 6 weeks postpartum could be analyzed. The study population comprised 7,203,924 deliveries. Notably, we excluded women who gave birth after November 19, 2021 (n = 7,415), had no healthcare institution delivery data (n = 7,836), or had no information due to missing data (n = 17,095). A total of 7,171,578 deliveries were included in this study.
Delivery-related medical costs were calculated from the claimed total direct medical costs during delivery hospitalization and the 6-week postpartum period. As the NHIS database does not include outpatient drug costs or uncovered healthcare service costs (such as uncovered treatments, medical administrations and injections, and nonstandard accommodations), the costs reported herein do not include those of the uncovered services.
To compare prices from different calendar years, costs were inflated to 2020 values using the South Korea Consumer Price Index for healthcare from the Bank of Korea by multiplying them by a year-specific inflation factor (19). To express costs in US dollars, they were converted from Korean won to US dollars using the annual exchange rates of the Ministry of Economy and Finance for each year (20).
Maternal mortality was defined as the death of a woman during pregnancy or within 6 weeks postpartum (21). Maternal mortality included all-cause mortality because the cause of death was not available in the database.
The covariates included maternal sociodemographic and clinical factors. Sociodemographic factors included maternal age (<19, 19–24, 25–29, 30–34, 35–39, 40–44, or > 45 years), income level (quartile), type of insurance (self-employed insurance, employee insurance, or medical aid), and residential area (Seoul, metropolitan areas, small cities, or rural areas). Maternal clinical factors included the following: mode of delivery (spontaneous vaginal delivery, instrumental delivery, or cesarean section delivery); preterm birth (delivered at <37 vs. ≥37 weeks); parity (nulliparous or multiparous); multiple birth status (singleton vs. twin or more); adequacy of prenatal care (estimated by the Kessner Adequacy of Prenatal Care Index (22), which categorized adequate vs. inadequate, including intermediate, prenatal care); obstetric comorbidity [assessed by Bateman’s obstetric comorbidity index (23)]; type of hospital (general hospital with more than 500 beds, general hospital with 100–499 beds, hospital with 30–99 beds, and clinics with less than 30 beds); delivery year.
We analyzed the distribution of maternal mortality and SMM according to maternal sociodemographic and clinical factors using descriptive statistics. We calculated the unadjusted mean delivery-related total medical costs and their 95% confidence intervals (CIs) to test their differences for childbirth with and without maternal mortality and SMM and all variables using the Kruskal–Wallis test. We used a generalized estimating equation (GEE) model with a log link, gamma distribution, and robust standard errors to estimate the mean delivery-related medical costs of maternal mortality and other variables, adjusted for covariates. We performed a stratified analysis using the GEE model to calculate the association between the adjusted delivery-related medical costs and maternal mortality by residential area. All statistical analysis was conducted using SAS 9.4 (SAS Institute, Inc., Cary, NC, United States). The level of significance was set at p < 0.05.
In total, 7,171,578 deliveries were included in this study. The maternal mortality rate was 9.7 per 100,000 deliveries. Women aged 35 years and older had a higher proportion of maternal death (35–39 years: 32.8%; 40–44 years: 6.1%; 45 years and older, 0.1%). Maternal mortality gradually decreased from 7.5% in 2003 to 3.2% in 2021 (Table 1).
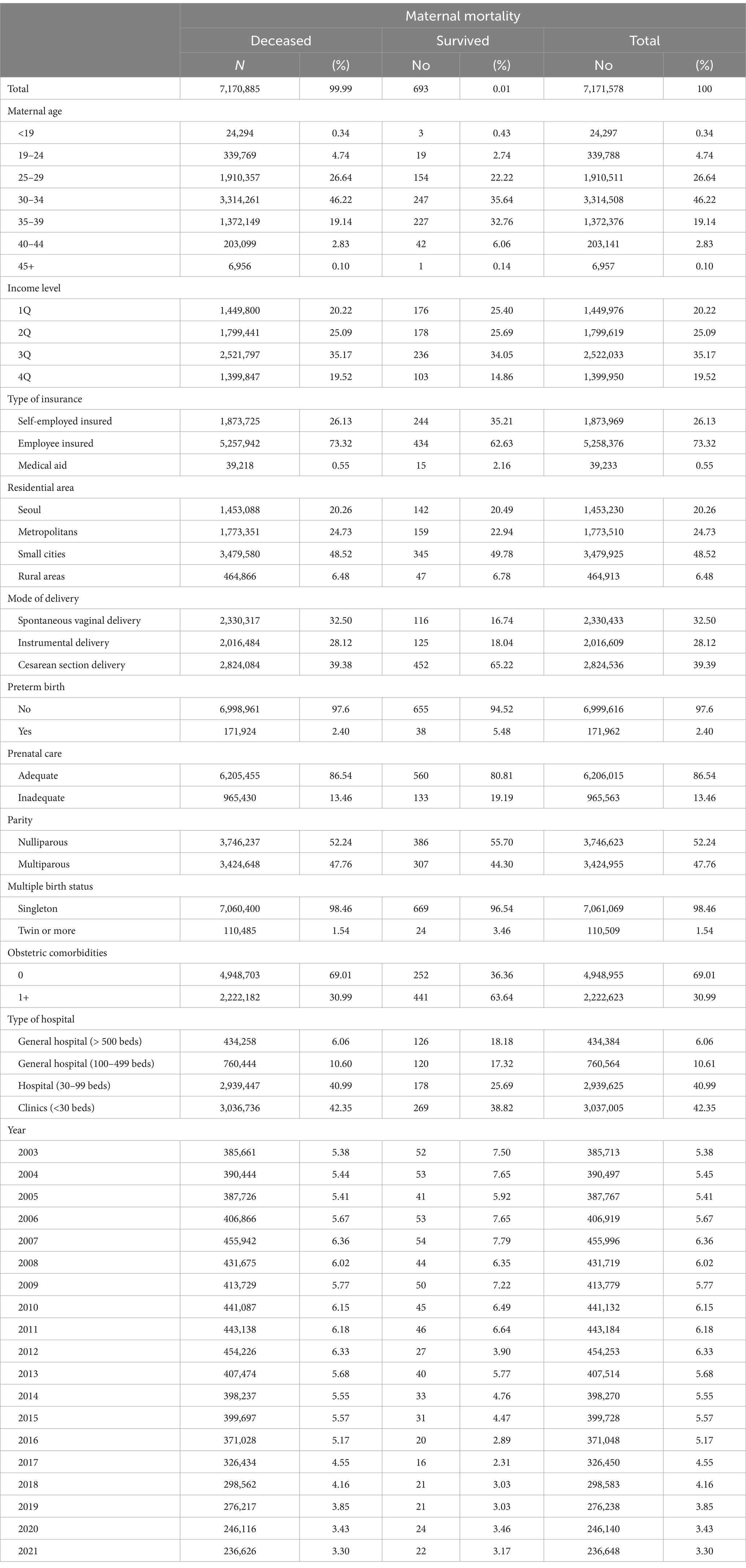
Table 1. General characteristics of study population.
The average total delivery-related medical costs with unadjusted all covariates for all participants were $1,157 (95% CI $1,156–$1,157); the costs in cases with maternal mortality were $7,634 (95% CI, $6,717–$8,551) and those in cases without maternal mortality were $1,156 (95% CI $1,156–$1,157) over 19 years (Table 2). The average medical costs varied significantly based on the covariates (p < 0.0001 for each) (Table 2).
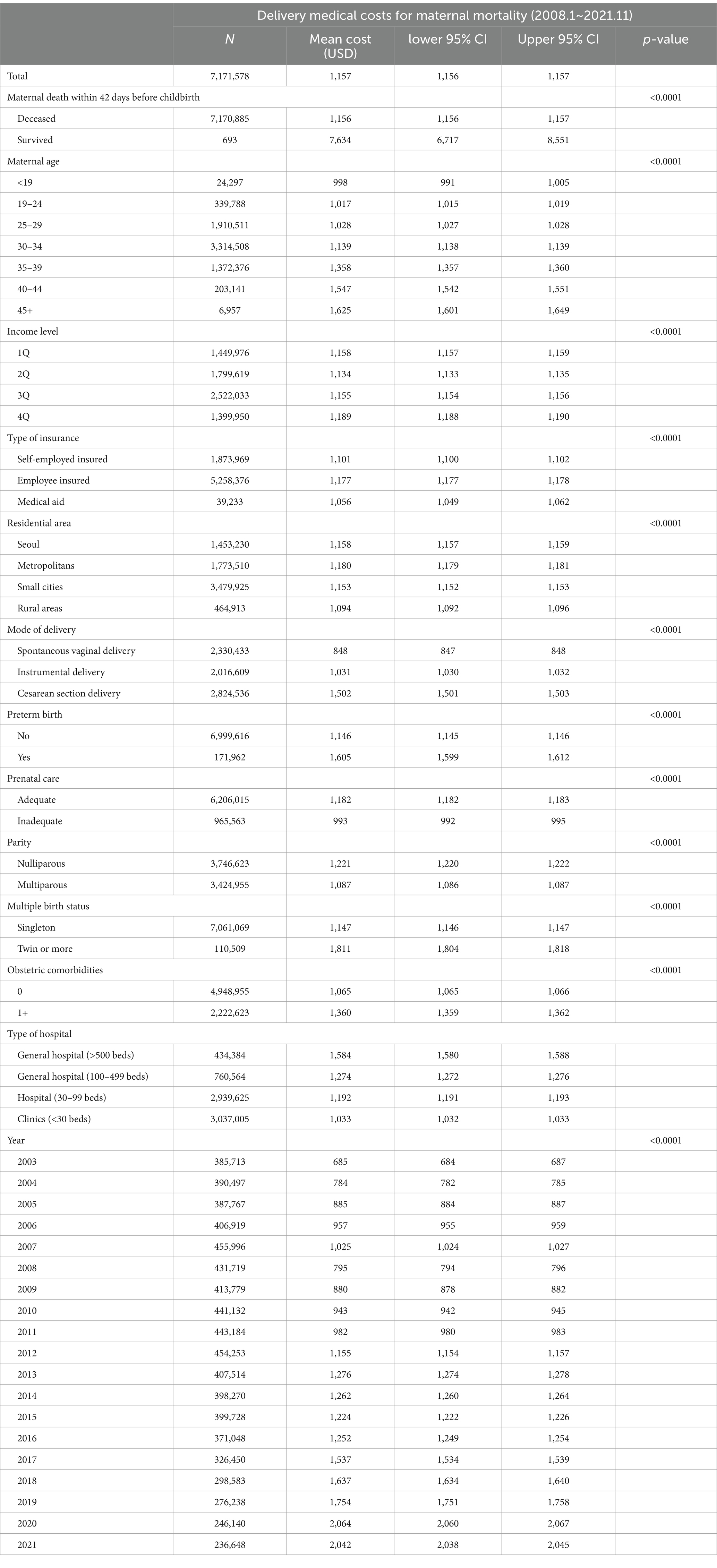
Table 2. Unadjusted model for delivery costs on maternal mortality.
The mean delivery-related total medical costs were adjusted for all covariates, and the association between the adjusted costs and maternal mortality was analyzed (Table 3). Patients with maternal mortality incurred significantly higher medical costs than those without. The adjusted mean (CI) delivery-related costs were $2,802 (95% CI $2,717–$2,889), which was 5.8-fold higher with maternal mortality than without maternal mortality. The total delivery-related medical cost for all women with maternal mortality {number with maternal mortality (n = 693) × adjusted mean cost of maternal mortality ($2,802)} was approximately $1.94 million, representing 0.06% of the total delivery-related medical costs. Moreover, maternal mortality-related costs have significantly increased in recent years, from $546 (95% CI $544–$548) in 2003 to $1,352 (95% CI $1,347–1,357) in 2021.
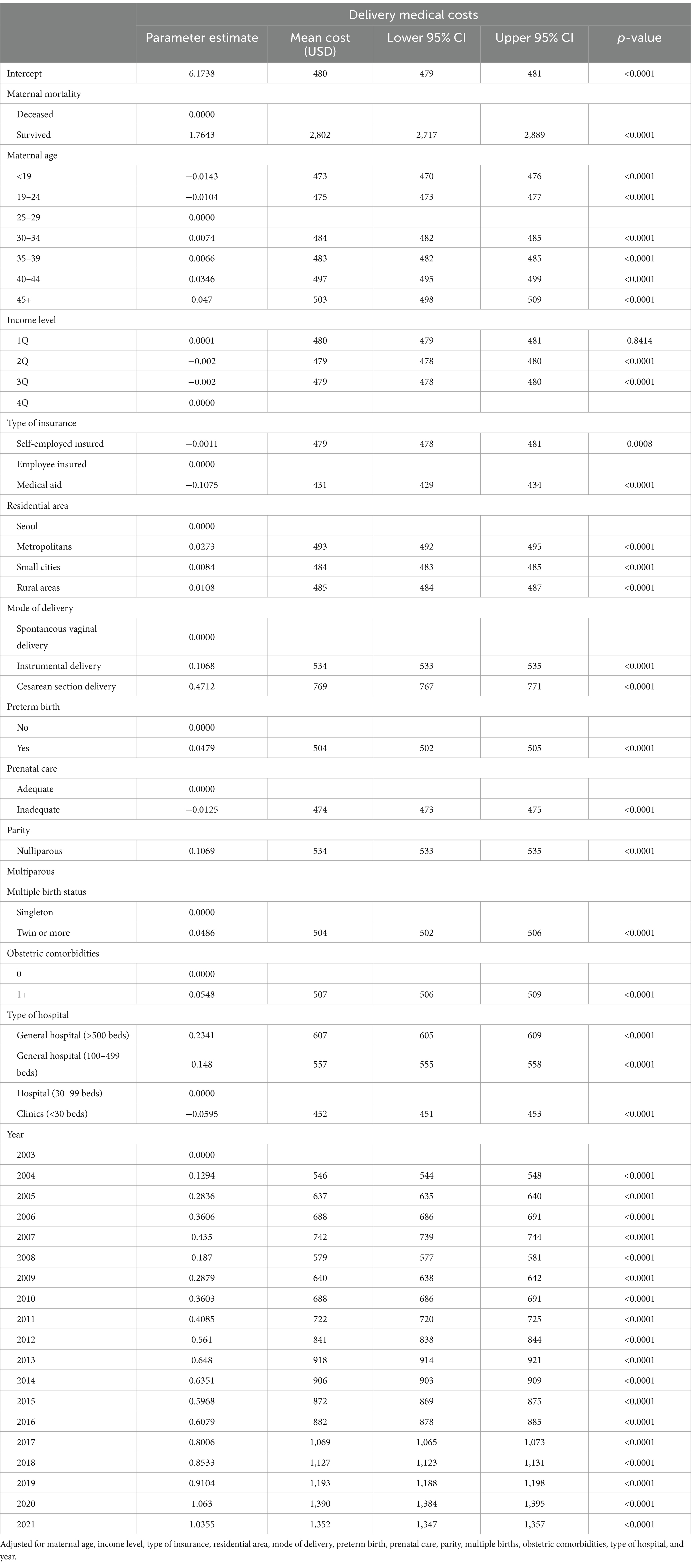
Table 3. Adjusted model for delivery medical costs on maternal mortality.
This study demonstrated a strong association between maternal mortality and delivery-related medical costs, with a nearly six-fold increase in costs among women who experienced maternal mortality. The results provide a detailed breakdown of these costs, highlighting that maternal mortality cases incurred significantly higher expenses across all periods. These findings align with previous studies on severe maternal morbidity (SMM), which have shown increased medical costs associated with adverse maternal outcomes (12). Consequently, over $1.6 million was spent from 2003 to 2021 on excess delivery-related medical costs due to maternal death, as calculated using adjusted cost estimates (693 cases × $2802 – 693 cases × $480). Importantly, approximately 83% ($1.6 million of $1.94 million) of the maternal mortality delivery-related medical costs could have been avoided through the prevention of mortality-related complications.
While the association between maternal mortality and medical costs is clear, the cause of the high cost is insufficiently understood, perhaps because maternal mortality is demographically rare and difficult to study. Consistent with this, a World Health Organization (WHO) study on maternal mortality did not estimate direct medical costs and included only low-income countries (24).
At 0.06% of the overall delivery-related medical costs, the proportion of the total delivery medical costs attributable to maternal mortality may seem small. This relates to the absolute number of maternal deaths, which is relatively low in South Korea because of its total fertility rate, which, at 0.81 children per woman, is the lowest in the world (25). Therefore, although the MMR in South Korea in 2022 is higher than that of the Organization for Economic Co-operation and Development (OECD) members (12 vs. 9 deaths per 100,000 live births in South Korea vs. OECD countries) (26), the absolute number of maternal deaths is extremely small. Furthermore, the burden of maternal mortality extends beyond direct medical costs to include the potential years of lost life, the statistical value of those years, and their impact on surviving family members. Thus, further studies are required to estimate the total burden of maternal mortality. As 83% of the direct medical costs associated with maternal mortality in South Korean women were potentially reducible, maternal health promotion can potentially improve maternal health outcomes and prevent tragic events.
Interestingly, the medical costs associated with maternal mortality have increased significantly in recent years. Although the reasons for this remain unknown, several mechanisms have been proposed. First, delivery-related medical costs may have been changed by the new fee-for-service policies. The Korean government supported several fertility-related policies to encourage the expansion of healthcare coverage. Since January 2005, spontaneous vaginal delivery has been free of charge. In the 4 years from its universal adoption for prospective payment in July 2012 to June 2016, cesarean section delivery accounted for 20% of the total out-of-pocket costs paid. Since July 2016, it has accounted for 5% of the total delivery-related costs. When the South Korean government implemented a financial support policy, out-of-pocket medical costs for cesarean section delivery dropped from 100 to 5%, reducing the financial burden on maternities. Therefore, pregnancies and obstetricians might choose their delivery by cesarean section more easily if needed. Nevertheless, total costs were not reduced but increased with respect to the consumer price inflation rate.
Moreover, the rate of cesarean section deliveries in South Korea has gradually increased, which is related to the medical costs of childbirth. According to OECD statistics, the rate of cesarean section deliveries from 2003 to 2020 dramatically increased from 36.5 to 53.8% in South Korea, the second-highest rate of cesarean section delivery in 2020 among OECD countries (27). A previous study showed that cesarean delivery is a high-risk factor for maternal mortality, and a report from a WHO Health Organization global survey involving nine Asian countries showed higher rates of cesarean section to be associated with a higher MMR (28). A similar finding was reported in a high-income country (29). Therefore, these numbers indicate that delivery-related medical costs may increase due to increasing C-section deliveries.
Finally, the South Korean government implemented several childbirth encouragement policies, including financial and service support measures such as iron supplementation (2008), vouchers for prenatal care and childbirth (2011), reduced out-of-pocket (OOP) medical costs for high-risk pregnancies (2015), and insured coverage of assisted reproductive technology. Direct or indirect improvement in maternal health and reduced financial burdens may have led to reduced OOP costs associated with maternal mortality in recent years. However, increasing new policies related to encouraging pregnancy may raise total medical costs because the utilization of healthcare services and accessibility to obstetricians may be better.
This study has several strengths. First, to the best of our knowledge, no other investigation has estimated the association between maternal mortality and delivery-related direct medical costs using a nationally representative database that includes all women who delivered in South Korea during an extended 19-year period. While several studies have examined the relationship between delivery costs and one of these conditions, none have estimated the costs regarding maternal mortality. Second, the endpoints were adjusted for numerous covarying demographic and obstetric factors, allowing for the detection of significant differences in the diverse case mix. Third, this study provides considerable data to support future studies on the association between maternal health outcomes and medical costs and the disease burden of maternal mortality and morbidity in various segments of the delivery population.
This study has some limitations. First, as the NHIS delivery cohort database does not include information on healthcare services not covered by insurance and policies affecting covered services that changed during the 19-year span of the study, some costs were inconsistently captured. For instance, the coverage of specialist medical service fees changed in January 2018, and the coverage of some non-standard hospital accommodations changed in July 2019. Consequently, total medical costs may have been underestimated. Second, maternal death included all-cause mortality within 42 days of childbirth. Thus, as the NHIS Delivery Cohort database did not include information on cause-specific mortality, it may have included incident- or accident-caused mortality. Further studies are necessary to link the government’s cause-specific mortality database with the NHIS Delivery Cohort database. Third, as the NHIS Delivery Cohort database uses revised ICD-10 codes that do not include procedure codes, we converted the ICD-10 codes for procedures, which may have made the identification of procedural cases less accurate.
This study found that maternal mortality is associated with significantly higher delivery-related medical costs, nearly six times those of non-maternal mortality cases. Approximately 83% of these costs ($1.6 million) were potentially reducible, emphasizing the need for improved maternal health interventions. This study provides the first nationwide, long-term analysis of the direct medical costs of maternal mortality in a high-income country, highlighting its economic burden on both individuals and the healthcare system. To reduce costs and improve maternal health outcomes, policymakers should expand access to prenatal care for early risk detection and strengthen nationwide maternal health monitoring systems. Additionally, further research is needed to explore the broader economic impact of maternal mortality. By implementing these measures, maternal deaths can be reduced, and healthcare expenditures can be optimized, benefiting both individuals and society.
Publicly available datasets were analyzed in this study. This data can be found at: https://nhiss.nhis.or.kr/.
The studies involving humans were approved by the Institutional Review Board of Eulji University (IRB Number: EU22-27). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
JN: Conceptualization, Data curation, Formal analysis, Funding acquisition, Methodology, Project administration, Resources, Validation, Visualization, Writing – original draft, Writing – review & editing.
The author(s) declare that financial support was received for the research and/or publication of this article. This research was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Science, ICT and Future Planning (No. 2020R1C1C1013668).
The author would like to thank the National Health Insurance Service for the using database of this study.
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Trost, S, Beauregard, J, Chandra, G, Njie, F, Berry, J, Harvey, A, et al. Pregnancy-related deaths: Data from maternal mortality review committees in 36 US States, 2017–2019. Atlanta, GA: Centers for Disease Control and Prevention, US Department of Health and Human Services. (2022). Available from: https://www.cdc.gov/maternal-mortality/php/data-research/mmrc-2017-2019.html.
2. Kassebaum, NJ, Bertozzi-Villa, A, Coggeshall, MS, Shackelford, KA, Steiner, C, Heuton, KR, et al. Global, regional, and national levels and causes of maternal mortality during 1990-2013: a systematic analysis for the global burden of disease study 2013. Lancet. (2014) 384:980–1004. doi: 10.1016/S0140-6736(14)60696-6
3. Hoyert, DL. Maternal mortality rates in the United States 2020. NCHS Health E-Stats. (2022). doi: 10.15620/cdc:113967
4. Mariotto, AB, Enewold, L, Zhao, J, Zeruto, CA, and Yabroff, KR. Medical care costs associated with cancer survivorship in the United States. Cancer Epidemiol Biomarkers Prev. (2020) 29:1304–12. doi: 10.1158/1055-9965.EPI-19-1534
5. Wang, Y, Zhang, P, Shao, H, Andes, LJ, and Imperatore, G. Medical costs associated with diabetes complications in Medicare beneficiaries aged 65 years or older with type 1 diabetes. Diabetes Care. (2023) 46:149–55. doi: 10.2337/dc21-2538
6. Gunja, MZ, Gumas, ED, and Williams, RD. US health care from a global perspective, 2022: accelerating spending, worsening outcomes. Commonwealth Fund. (2023) 1:1–24. doi: 10.26099/8ejy-yc74
7. World Health Organization. Maternal mortality Geneva. Switzerland: World Health Organization (2024).
8. O'Neil, SS, Platt, I, Vohra, D, Pendl-Robinson, E, Dehus, E, Zephyrin, L, et al. Societal cost of nine selected maternal morbidities in the United States. PLoS One. (2022) 17:e0275656. doi: 10.1371/journal.pone.0275656
9. Tikkanen, R, Gunja, MZ, FitzGerald, M, and Zephyrin, L. Maternal mortality and maternity care in the United States compared to 10 other developed countries. Commonwealth Fund. (2020) 10:22. doi: 10.26099/411v-9255
10. Kes, A, Ogwang, S, Pande, RP, Douglas, Z, Karuga, R, Odhiambo, FO, et al. The economic burden of maternal mortality on households: evidence from three sub-counties in rural western Kenya. Reprod Health. (2015) 12:1–10. doi: 10.1186/1742-4755-12-S1-S3
11. Ye, F, Wang, H, Huntington, D, Zhou, H, Li, Y, You, F, et al. The immediate economic impact of maternal deaths on rural Chinese households. PLoS One. (2012) 7:e38467. doi: 10.1371/journal.pone.0038467
12. Howland, RE, Angley, M, Won, SH, Wilcox, W, Searing, H, and Tsao, T-Y. Estimating the hospital delivery costs associated with severe maternal morbidity in new York City, 2008–2012. Obstet Gynecol. (2018) 131:242–52. doi: 10.1097/AOG.0000000000002432
13. Callaghan, WM, Creanga, AA, and Kuklina, EV. Severe maternal morbidity among delivery and postpartum hospitalizations in the United States. Obstet Gynecol. (2012) 120:1029–36. doi: 10.1097/AOG.0b013e31826d60c5
14. White, RS, Lui, B, Bryant-Huppert, J, Chaturvedi, R, Hoyler, M, and Aaronson, J. Economic burden of maternal mortality in the USA, 2018–2020. J Compar Effective Res. (2022) 11:927–33. doi: 10.2217/cer-2022-0056
15. Khosla, K, Jin, Y, Espinoza, J, Kent, M, Gencay, M, Kunz, LH, et al. Signs or symptoms of suspected preeclampsia–a retrospective national database study of prevalence, costs, and outcomes. Pregnancy Hypertens. (2024) 36:101124. doi: 10.1016/j.preghy.2024.101124
16. Riestenberg, C, Jagasia, A, Markovic, D, Buyalos, RP, and Azziz, R. Health care-related economic burden of polycystic ovary syndrome in the United States: pregnancy-related and long-term health consequences. J Clin Endocrinol Metabol. (2022) 107:575–85. doi: 10.1210/clinem/dgab613
17. Margiotta, C, Gao, J, O’Neil, S, Vohra, D, and Zivin, K. The economic impact of untreated maternal mental health conditions in Texas. BMC Pregnancy Childbirth. (2022) 22:700. doi: 10.1186/s12884-022-05001-6
18. Lee, J, Lee, JS, Park, S-H, Shin, SA, and Kim, K. Cohort profile: the national health insurance service–national sample cohort (NHIS-NSC), South Korea. Int J Epidemiol. (2017) 46:dyv319. doi: 10.1093/ije/dyv319
20. Korean Government. Trends of currency exchange. (2022). Available online at: https://www.index.go.kr/unity/potal/main/EachDtlPageDetail.do?idx_cd=1068 (Accessed August 15, 2023).
21. World Health Organization. Trends in maternal mortality 2000 to 2020: estimates by WHO, UNICEF, UNFPA, World Bank Group and UNDESA/Population Division. Geneva: World Health Organization. (2023).
22. Kessner, DM, Singer, J, and Kalk, CW. Infant death: An analysis by maternal risk and health care. Vol. 1. Washington DC: Institute of Medicine Natiolnal Academy of Sciences. (1973).
23. Bateman, BT, Mhyre, JM, Hernandez-Diaz, S, Huybrechts, KF, Fischer, MA, Creanga, AA, et al. Development of a comorbidity index for use in obstetric patients. Obstet Gynecol. (2013) 122:957–65. doi: 10.1097/AOG.0b013e3182a603bb
24. Islam, MK, and Gerdtham, UGWorld Health Organization. The costs of maternal-newborn illness and mortality. Geneva: World Health Organization (2006). Available from: https://iris.who.int/handle/10665/43516
25. Organization for Economic Co-operation and Development. Fertility rates. (2023) Available from: https://data.oecd.org/pop/fertility-rates.htm (Accessed October 2, 2023).
26. Organisation for Economic Co-operation and Development WHO. Health at a glance: Asia/Pacific 2022: Measuring Progress towards universal health coverage. Paris: Organisation for Economic Co-operation and Development WHO (2022).
27. Organization for Economic Co-operation and Development. Caesarean sections (indicator). (2024). Available from https://www.oecd.org/en/data/indicators/caesarean-sections.html. (Accessed October 2, 2023).
28. Lumbiganon, P, Laopaiboon, M, Gülmezoglu, AM, Souza, JP, Taneepanichskul, S, Ruyan, P, et al. Method of delivery and pregnancy outcomes in Asia: the WHO global survey on maternal and perinatal health 2007-08. Lancet. (2010) 375:490–9. doi: 10.1016/S0140-6736(09)61870-5
Keywords: maternal mortality, maternal death, medical costs, NHIS delivery cohort, pregnancy-related medical costs
Citation: Nam JY (2025) How much can we reduce delivery-related medical costs associated with maternal mortality? A nationwide cohort study from 2003 to 2021. Front. Public Health. 13:1411534. doi: 10.3389/fpubh.2025.1411534
Edited by:
Chhabi Lal Ranabhat, Eastern Scientific LLC, United StatesReviewed by:
Myung-Bae Park, Yonsei University Mirae Campus, Republic of KoreaCopyright © 2025 Nam. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jin Young Nam, anluYW1AZXVsamkuYWMua3I=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.