 Skirmante Sauliune
Skirmante Sauliune Ramune Kalediene
Ramune Kalediene Vytenis Kalibatas
Vytenis Kalibatas Snieguole Kaseliene
Snieguole Kaseliene Olga Mesceriakova
Olga Mesceriakova- Department of Health Management, Faculty of Public Health, Lithuanian University of Health Sciences, Kaunas, Lithuania
The aim of this study: to analyze lifestyle changes among older adults during and after COVID-19 pandemic in Lithuania, with a particular focus on eating habits, physical activity, social engagement and harmful habits.
Methods: The representative sample of Lithuanian population over 65 years old (1,503 individuals) was involved in the questionnaire survey, performed in January 2024.
Results: Most of the eating habits and the body weight of the older adults did not change during the COVID-19 pandemic in Lithuania. Respondents noted that their physical activity decreased, face-to-face communication became rarer, while remote communication increased. During pandemic, the increased frequency of snacking was more often indicated by persons with lower than secondary education, working, receiving higher incomes, as well as increased snacking and body weight were more prevalent among younger, single or overweight persons; increased body weight during the pandemic was more often mentioned by the persons who assessed their health poorly. Physical activity decreased more often among rural residents and groups with higher or college education; face-to-face communication has become rarer among younger people, rural residents, pensioners, disabled, people with higher income and those with overweight, while remote communication has increased among women, respondents with a university education and those with an average income (p < 0.05). Nearly half of the respondents indicated that the changes in food consumption and smoking frequency that occurred during the pandemic remained after it. After the pandemic, the habits of consuming fast food, confectionery or other sweets and changes in body weight mostly remained, while the patterns of communication returned to the pre-pandemic level. Most of the healthy lifestyle habits formed during the pandemic persisted after the pandemic. The lifestyle habits formed during the pandemic remained more stable in the groups of older persons, residents of smaller towns, respondents with lower than secondary education, higher income, singles, disabled, obese, and those who assessed their health poorly (p < 0.05).
Conclusion: During the COVID-19 pandemic in Lithuania, there were various changes in eating habits, physical activity, communication patterns, and harmful habits. Certain habits formed during the pandemic continued afterward, particularly among specific groups of the older Lithuanian adults.
1 Introduction
The COVID-19 pandemic has had, and continues to have, various consequences for the health and lifestyle of people around the world, especially for the older adults. This unprecedented public health crisis necessitated widespread lifestyle changes due to the imposition of social distancing measures, lockdowns, and other preventive strategies aimed at mitigating virus transmission (1). Consequently, these measures have influenced the daily routines, physical activities, social interactions, and overall well-being of older adults, leading to significant lifestyle modifications during and after the pandemic (2–6).
Analyzing lifestyle, 65 aged and older people appeared to be among the most vulnerable groups during the pandemic and were given special attention. Social isolation during the COVID-19 pandemic has had a significant impact on lifestyle, especially sedentary lifestyle and resulting reduced physical activity, sleep and eating habits. Older adults were often unable to adapt to restraint/quarantine measures and suffered from depression and cognitive impairment (7). Spending more time at home was associated with eating more and sitting longer. The stress associated with fear and the constant media coverage of the pandemic has led to the consumption of so-called “convenience foods” (high in added sugar or fat) or increased snacking between meals, as well as alcohol consumption (8).
The COVID-19 pandemic significantly impacted alcohol consumption and smoking habits. In Germany, 35.5% of respondents reported increased drinking during quarantine, while 45.8% reported increased smoking, often due to heightened stress (9). In Italy, 9.1% of respondents reported increased cigarette consumption, with 9.0% starting, relapsing, or intensifying their smoking (10). In South Korea, 11.0% of current smokers increased smoking, whereas 12.8% decreased their smoking during the pandemic (11).
The aftermath of the pandemic presents a unique opportunity to examine the long-term effects of these lifestyle changes. Unfortunately, there are not many country-wide studies analyzing the lifestyle changes of the population aged 65 and older during the COVID-19 pandemic, they are fragmentary, often only incorporated in the larger studies. It is crucial to understand how the temporary adjustments made during the pandemic might influence the future behavior and health outcomes of older adults, especially for countries with an aging population. Lithuania is one of the countries with rapidly aging population, with a fifth of the population aged 65 and over (12). The aging population creates challenges both for health and social care services as well as older adults are characterized by different lifestyle and health problems compared to other age groups. Therefore, it is extremely important to analyze the current situation, respond to it, intervene early, and prevent further consequences of the pandemic. Therefore, the aim of this study was to analyze lifestyle changes among older adults during and after COVID-19 pandemic in Lithuania, with a particular focus on eating habits, physical activity, social engagement and harmful habits.
2 Materials and methods
2.1 Research organization
The study was conducted in January 5–17, 2024, in Lithuania. The study was conducted in January 5–17, 2024, in Lithuania. 1,503 Lithuanian residents 65 years of age and older were interviewed by means of an anonymous survey (the response rate was 36%; Table 1). The research was conducted in the form of face-to-face interviews at the respondent’s home by an independent institution of public opinion and market research “Vilmorus Ltd.” A team of professional interviewers collected the data. The duration of one interview was 25–40 min. The survey covered 34 municipalities - it took place in 26 cities and over 50 villages. All the participants were informed about the study. Participation was voluntary and anonymous. Verbal consent to participate in the study was received from all the participants.
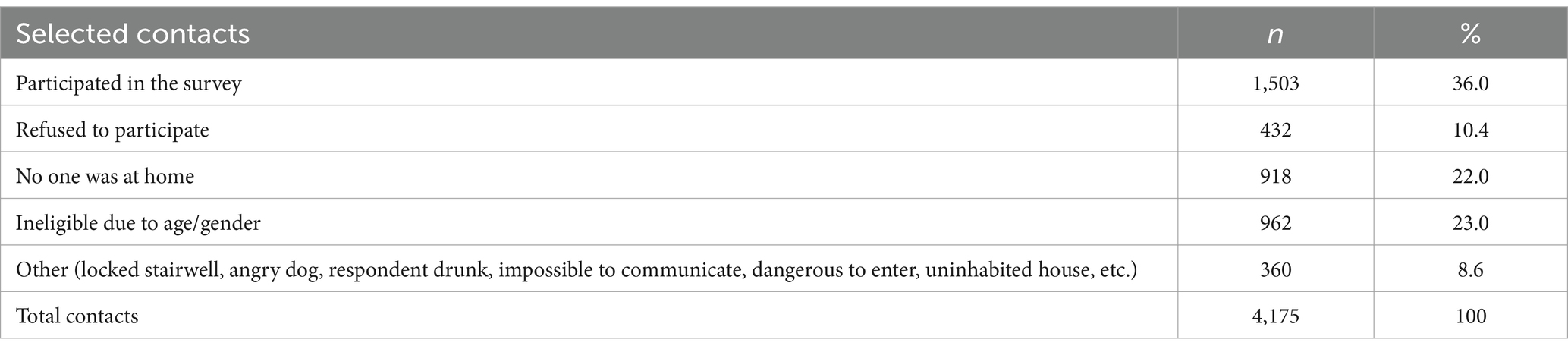
Table 1. Peculiarities of conducting the survey.
1,503 Lithuanian residents 65 years of age and older were interviewed by means of an anonymous survey (the response rate was 36%; Table 1) by the application of face-to-face interviews at the respondent’s home. The duration of one interview was 25–40 min. The survey covered 34 municipalities—it took place in 26 cities and over 50 villages.
2.2 Sampling
The study population of the survey is residents of Lithuanian households aged 65 and older selected using a multi-stage, probabilistic and proportional sampling technique. This method ensured equal opportunities for all Lithuanian residents, representing different places of residence and demographic groups, to participate in the study. The sample had to correspond to the demographic distribution of the Lithuanian population in terms gender and place of residence. The sample of Lithuanian residents older than 65 years was compiled based on the address register of the Republic of Lithuania managed by the state company Centre of Registers. A “route method” was used for further household selection. The survey was conducted in all ten administrative regions (counties) of Lithuania. The number of individuals interviewed in each county was proportional to its population size, as established using national statistical data. Within each county, the county center or another town and rural localities were chosen through random selection. Next, streets and the starting point of the route were randomly selected in each location. To ensure a representative respondent within each household, the ‘youngest male rule’ was applied. If the intended respondent was unavailable, a subsequent visit was arranged. Open Epi sample size calculator was used for the estimation of sample size using the following parameters: population size for each, gender and place of residence group, anticipated frequency 50%, probability of the mistake 5%, design effect 1 (estimated sample size was 1,536 participants).
2.3 Contingent
The distribution and grouping of respondents according to socio-demographic characteristics is presented in Table 2. Lithuanian residents aged 65–96 years participated in the study. The median age was 73 years, mean—74.04 years (standard deviation 6.37 years). The distribution of the research participants by age, gender and place of residence did not differ significantly from that of the whole population of Lithuania, so the study sample can be considered as a representative for the population of Lithuania.
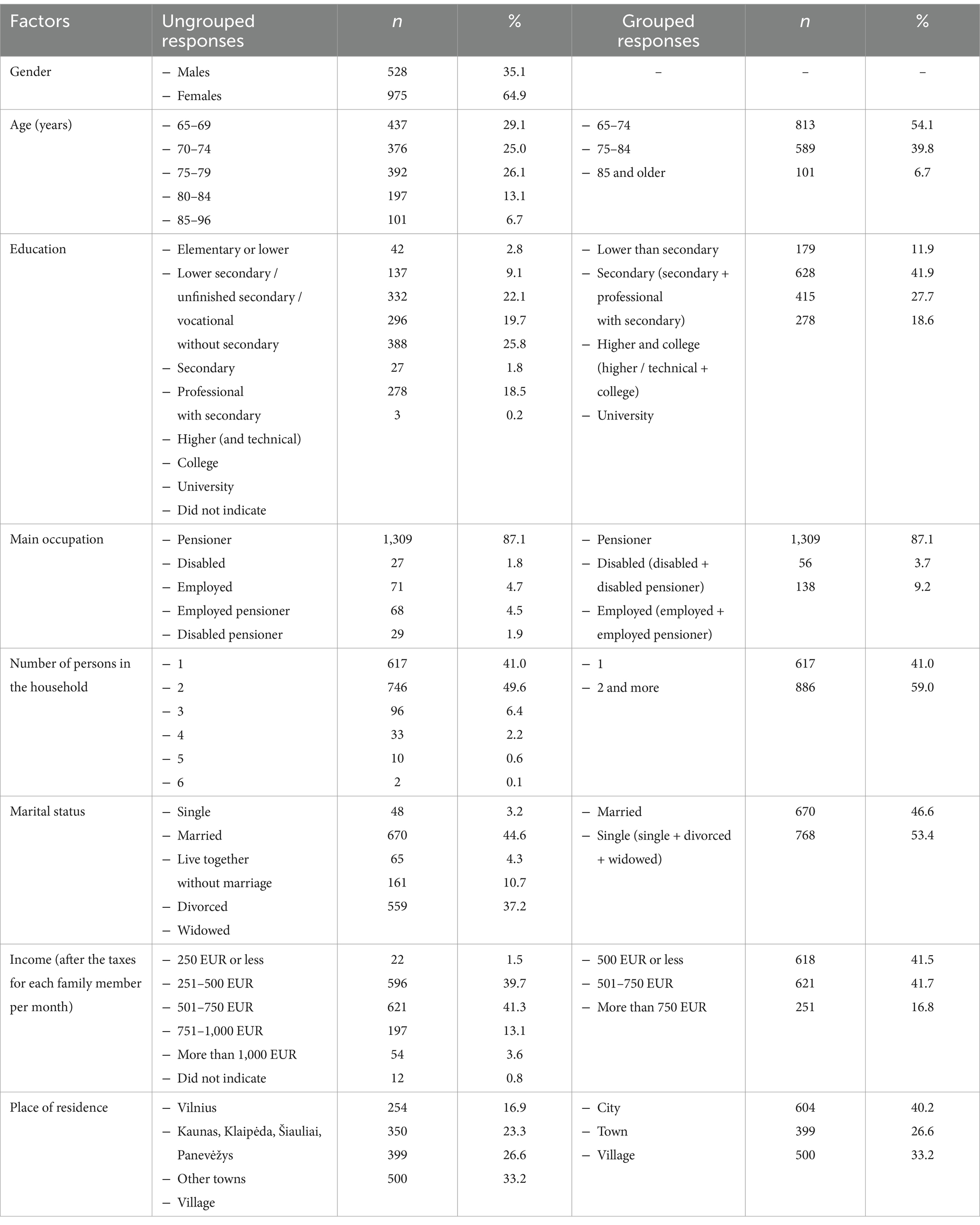
Table 2. Distribution of respondents according to socio-demographic characteristics.
The distribution of respondents according to certain health-related characteristics - body mass index (BMI), subjectively assessed health status was also rated. Study participants were also asked if they had a history of COVID-19. The distribution and grouping of respondents according to these health-related characteristics is presented in Table 3.
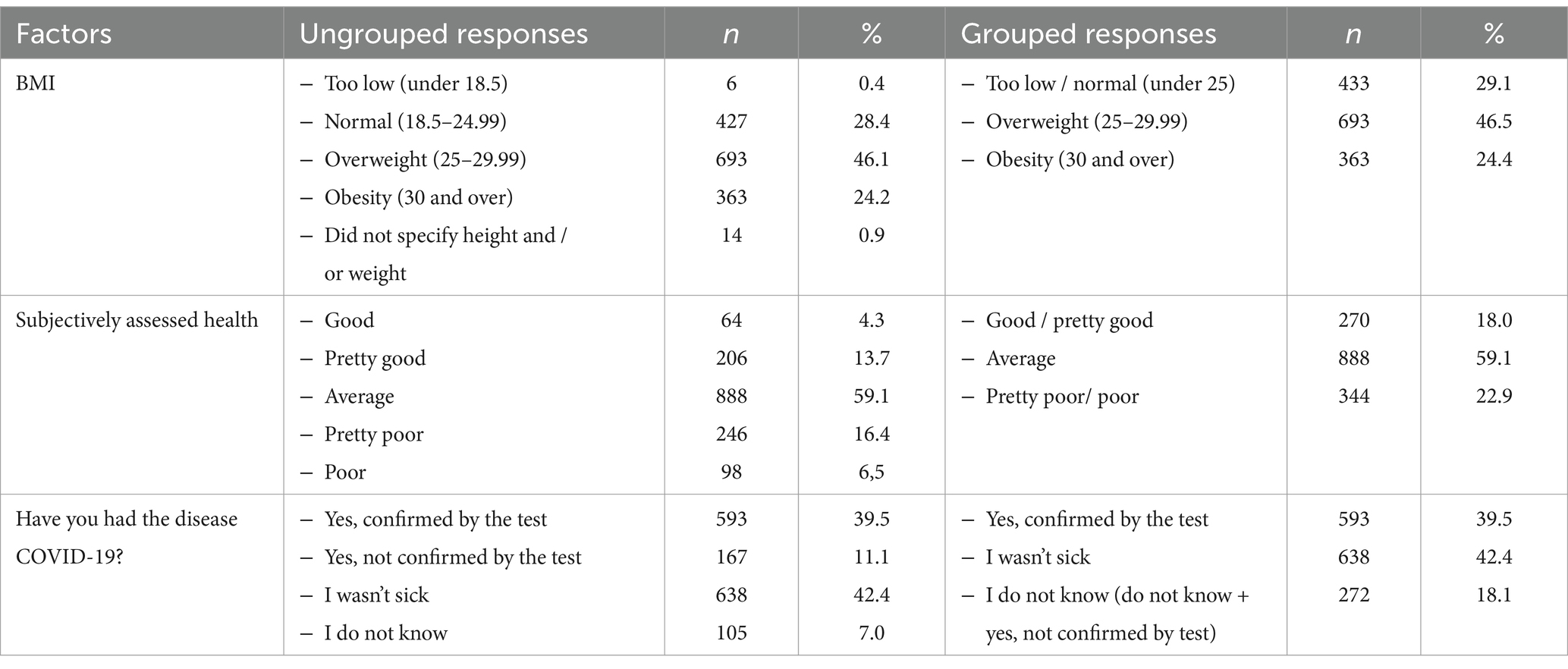
Table 3. Distribution of respondents according to health characteristics.
2.4 Research instrument
An original questionnaire of 74 questions was prepared for the study. The questionnaire consisted of 3 thematic sections (general information, lifestyle and its changes during and after the COVID-19 pandemic, and access to healthcare during and after the COVID-19 pandemic). This article analyses questions related to lifestyle changes during the COVID-19 pandemic (7 questions about changes in food consumption and 8 questions about changes in other lifestyle factors); lifestyle changes after the end of the pandemic (7 questions about changes in food consumption and 8 questions about changes in other lifestyle factors).
2.5 Statistical analysis
Statistical data analysis was performed using the IBM SPSS Statistics 29 statistical package. Data was weighted by gender and age. To identify the most vulnerable older adults population groups, study participants’ answers to questionnaire questions were compared according to socio-demographic factors and health characteristics using the Chi-square (χ2) criterion, and the z criterion for pairwise comparison of frequencies. Associations were considered statistically significant when the probability of the mistake (p) was <0.05.
3 Results
3.1 Lifestyle changes during a COVID-19 pandemic
Most of the respondents indicated that their eating habits did not change during the COVID-19 pandemic, and only 7.3% mentioned that they consumed more confectionery or other sweets, 7.0%—fresh vegetables, fruits or berries, every tenth study participant consumed less fast food (10.7%), meat and its products (10.4%) and confectionery or other sweets (9.4%), (Figure 1).
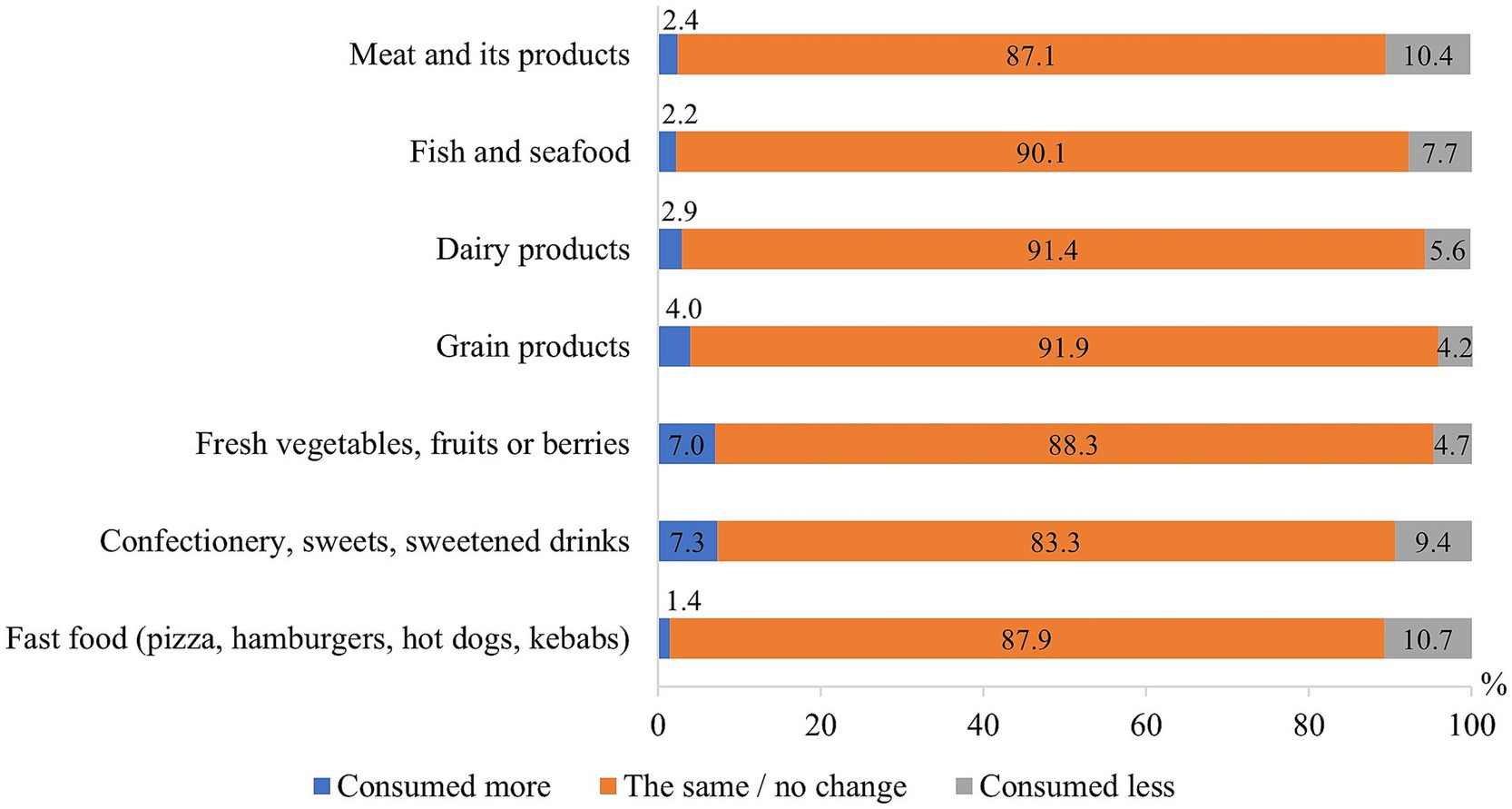
Figure 1. Changes of eating habits during the COVID-19 pandemic.
Also, most respondents indicated that the frequency and intensity of their smoking (94.4%), the frequency and amount of alcohol consumption (92.8%), the amount of food eaten (80.5%), snacking frequency (75.8%), and body mass (76.6%) did not change during the COVID-19 pandemic. However, a considerable number of study participants noted that their communication with their relatives “live” by meeting has become rare (62.0%) and distance communication has increased (i.e., by phone, e-mail or social networks; 26.8%), 33.9% indicated that their physical activity has decreased, 16.1% - snacking has increased, and 15% observed an increased body mass (Figure 2).
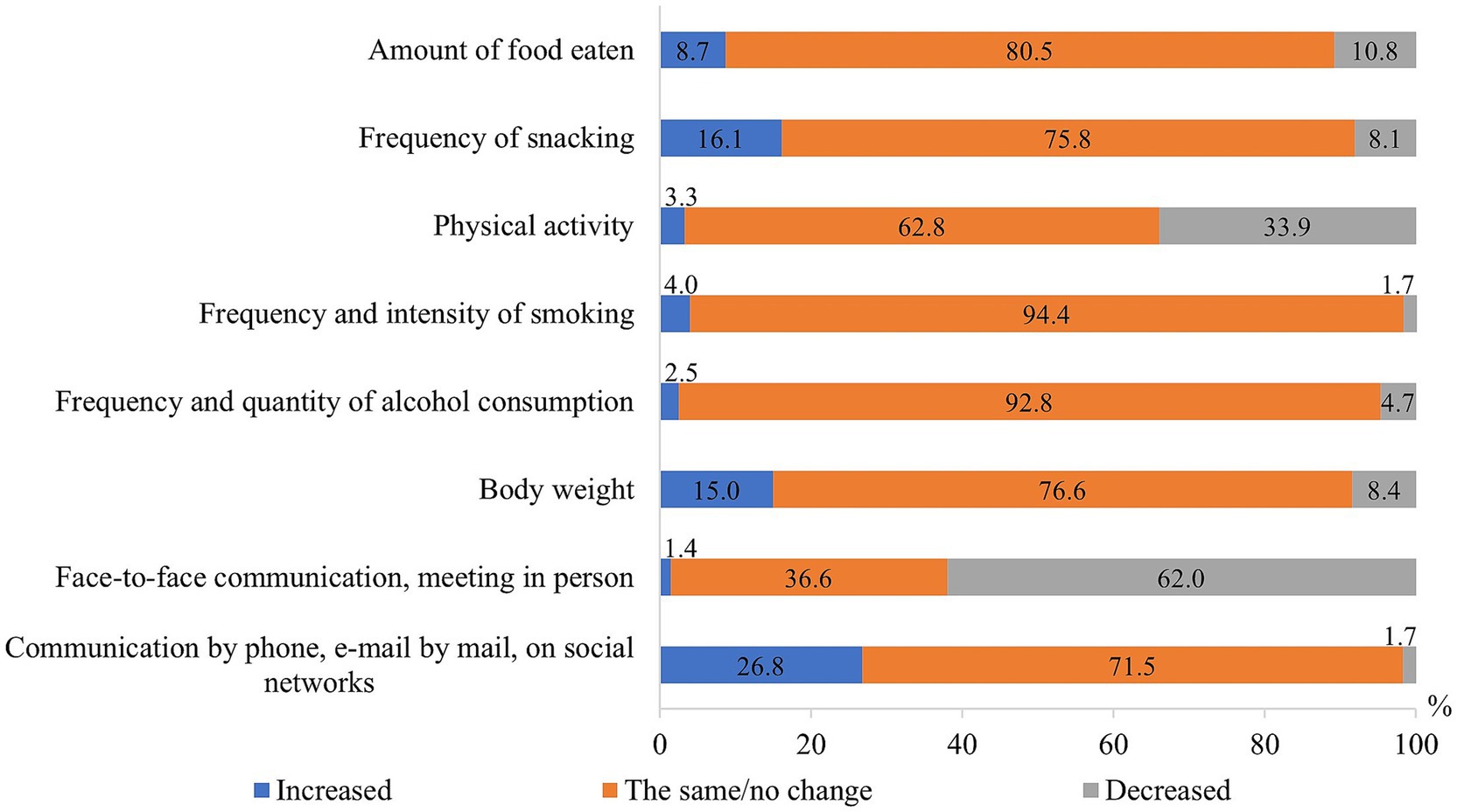
Figure 2. Changes of some of the lifestyle factors during the COVID-19 pandemic.
Changes in respondents’ lifestyle factors during the COVID-19 pandemic were statistically significantly (p < 0.05) associated with their sociodemographic characteristics (Figure 3). Women more often than men indicated that their distance/online communication improved. Younger respondents more often indicated more frequent snacking and an increase in body weight compared to older ones. They also reported more frequent communication with relatives at a distance and less frequent communication by “in person” meetings. Those living in the countryside more often than the inhabitants of the cities noted that their physical activity decreased and communication during meetings became less frequent, while the inhabitants of smaller towns more often than those living in the countryside stated that their snacking frequency and body weight increased. Respondents with lower than secondary education more seldom reported that their frequency of snacking had increased compared to the respondents of other educational groups. Physical activity of those with higher or college education more often decreased in comparison to those with secondary education. Respondents in the university education group more often than persons with lower education reported increased communication by phone or the Internet. Married respondents or those living in the household with other person, more often noticed that their snacking frequency and body weight increased as compared to the single ones. In the group of working persons, snacking became more frequent than among others, and pensioners more often than disabled persons complained that their communication with relatives “live meeting,” became less frequent. As the income of the respondents increased, the frequency of their snacking also increased; those with an income of EUR 750 or less more often than those with a higher income indicated that their communication with relatives by meeting became rare, and those whose income reached EUR 501–750 more often than those with a lower income indicated that their communication over a distance has increased.
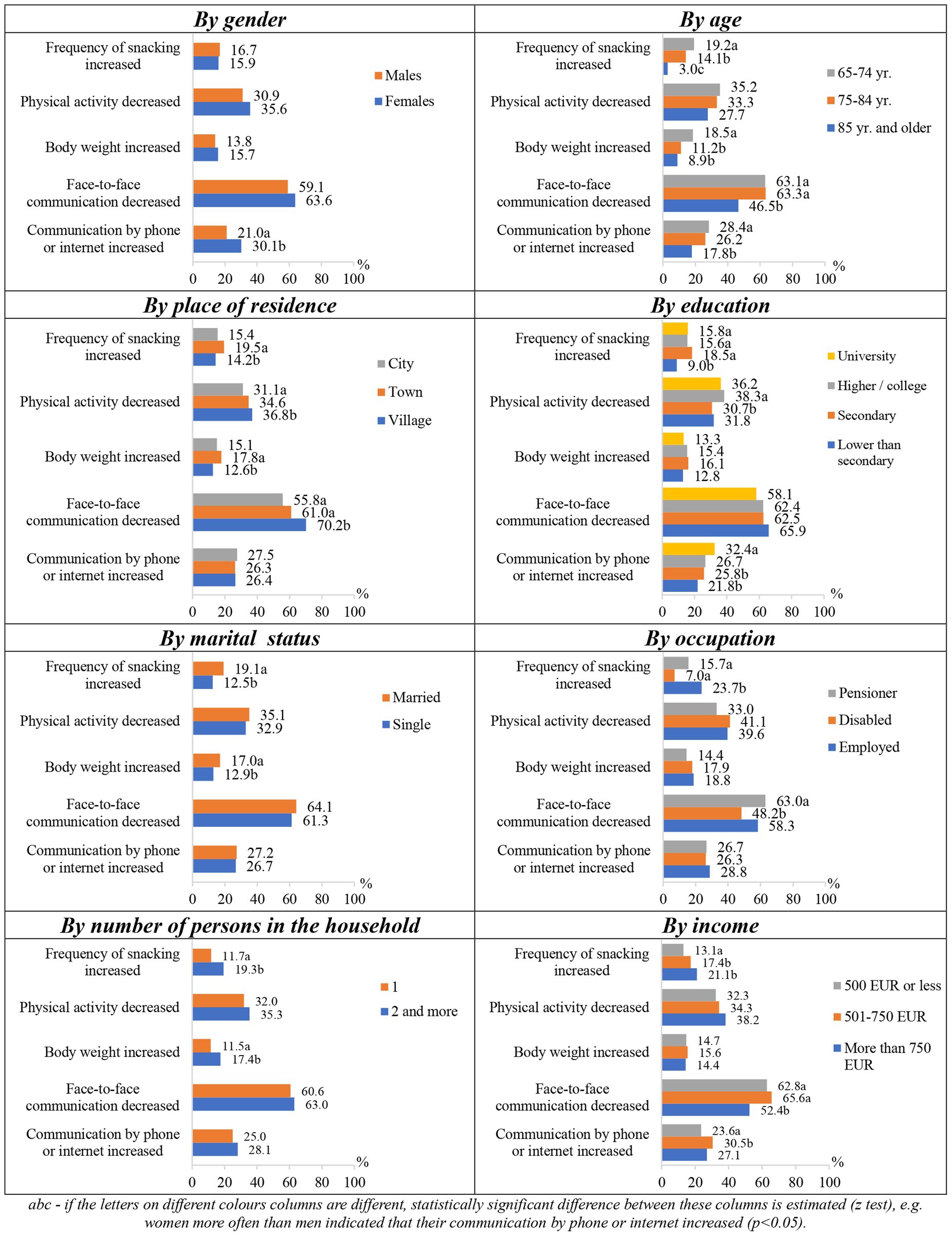
Figure 3. Changes in lifestyle factors during the COVID-19 pandemic depending on socio-demographic factors.
Overweight respondents more often stated that their frequency of snacking increased, in comparison to those with too low/normal weight respondents (18.0% vs. 13.4%); they also more often stated that their “live” communication, when meeting, became less frequent compared to low/normal weight and obese respondents (66.4% vs. 60.3% vs. 55.8%). The higher the respondents’ BMI was, the more often they reported that their body weight increased during the pandemic. According to the subjectively assessed health status, respondents who rated their health poorly complained of increased body weight the most compared to those who assessed their health average and pretty good/good (20.9% vs. 13.5% vs. 12.2%).
3.2 Lifestyle changes after the COVID-19 pandemic
Nearly half of the respondents reported that the changes in food consumption that occurred during the COVID-19 pandemic remained, while the other half said that their food consumption returned to the pre-pandemic level (Figure 4). The largest number of respondents indicated that their habits of consuming fast food (65.6%) and confectionery and other sweets (54.4%) remained, while meat and its products (41.7%) as well as fish and seafood remained the least common (44.6%).
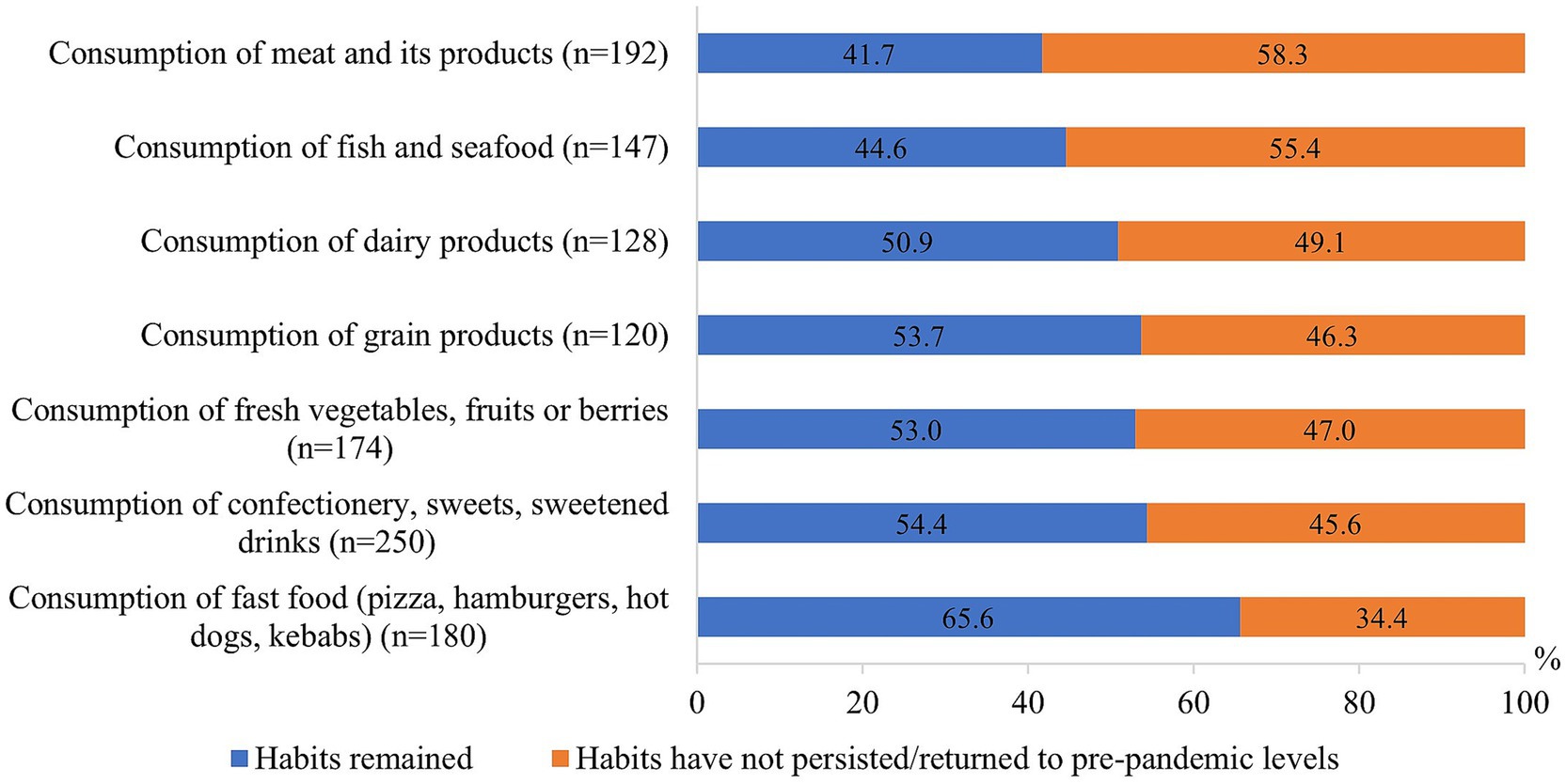
Figure 4. Changes of eating habits after the COVID-19 pandemic.
The consumption of fish and seafood, dairy and grain products, fresh vegetables, fruits and berries remained more frequent after the pandemic among those who had increased it during the pandemic, while the consumption of meat and its products, confectionery and other sweets, and fast food remained more frequent for those who used them less during the pandemic than before it (Figure 5).
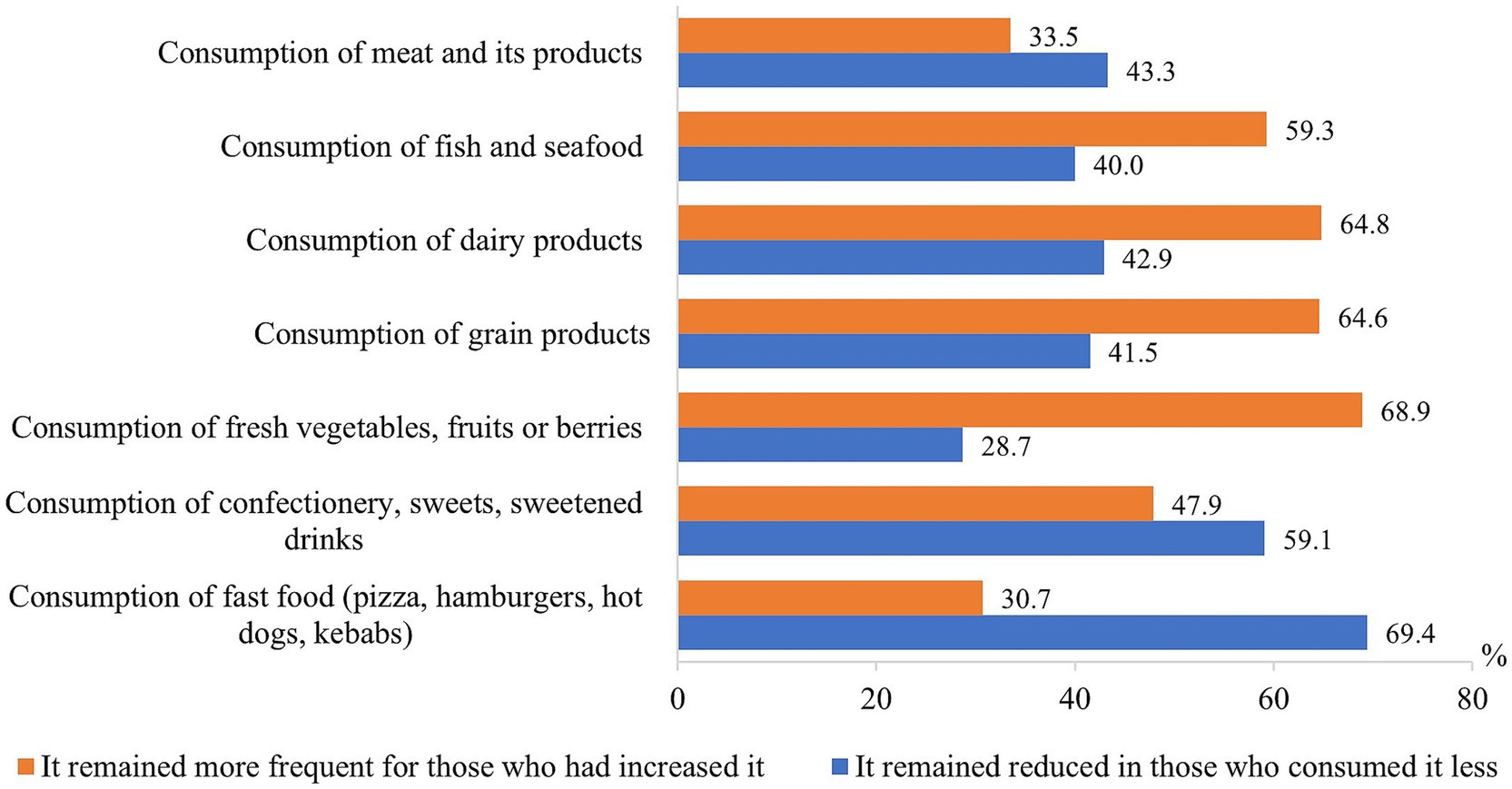
Figure 5. Proportion of respondents who maintained changes formed during the pandemic in eating habits after the end of the COVID-19 pandemic.
Changes in eating habits after the pandemic were statistically significantly (p < 0.05) dependent on the sociodemographic characteristics (Figure 6). The tendencies were observed that the eating habits formed during the COVID-19 pandemic mostly remained in smaller cities, in groups of people with lower than secondary education, the singles, disabled persons and people with income above 750 EUR.
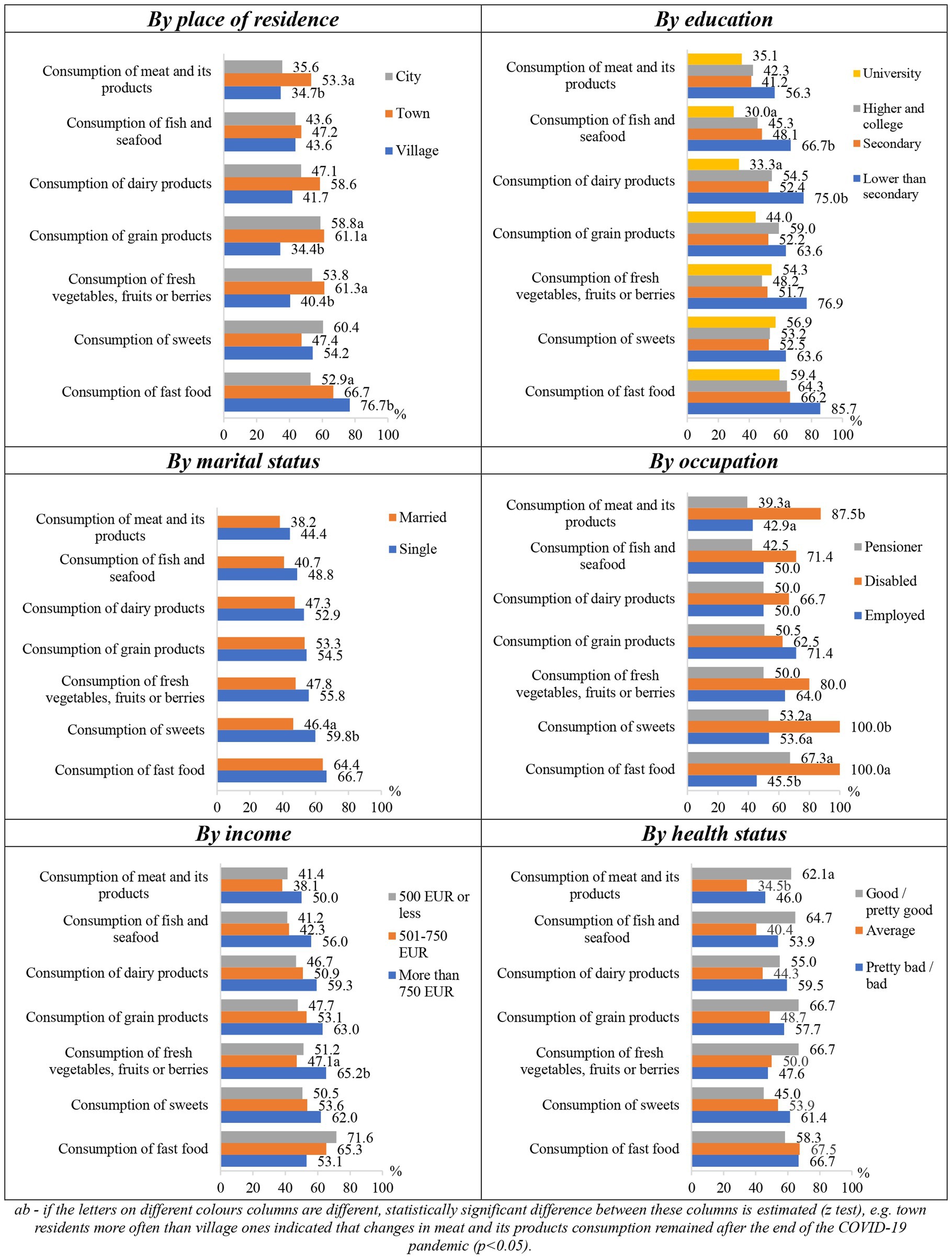
Figure 6. Changes in eating habits that remained after the end of the COVID-19 pandemic depending on socio-demographic factors.
When evaluating the changes in other lifestyle factors after the end of the COVID-19 pandemic, it was observed that changes in body weight (60.4%) as well as smoking frequency and intensity (52.3%) that occurred during the pandemic mostly remained. After the end of the pandemic, communication by “live” meeting (90.0%) and communication by phone, e-mail or on social networks (66.8%), as well as the amount of food eaten (67.8%), frequency of snacking (65.9%), physical activity (62.1%) and frequency of alcohol consumption and quantity (61.5%) mostly returned to the pre-pandemic level (Figure 7).

Figure 7. Changes of other lifestyle factors after the COVID-19 pandemic.
Physical activity, body weight, and face-to-face communication were more likely to be maintained after the pandemic in those who reported it increased during the pandemic, while the amount of food eaten, frequency of snacking, smoking and alcohol consumption, and communication with relatives remotely were more likely to be maintained in those who reported it decreased during the pandemic (Figure 8).
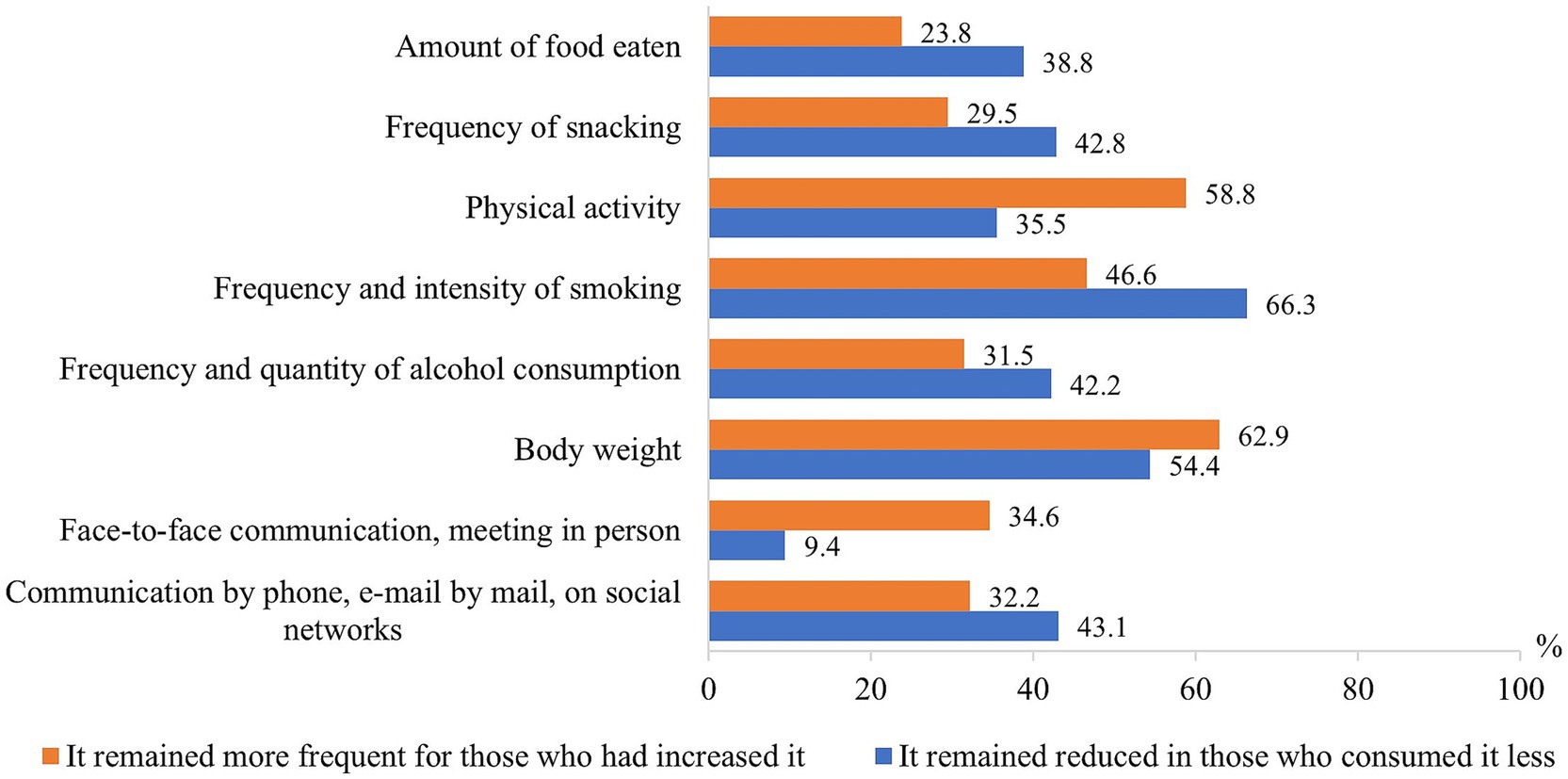
Figure 8. Proportion of respondents who maintained changes formed during the pandemic in other lifestyle factors after the end of the COVID-19 pandemic.
Changes in lifestyle factors after the COVID-19 pandemic depended statistically significantly (p < 0.05) on various sociodemographic factors (Figure 9). The lifestyle habits formed during the pandemic mostly remained in groups of older, having less than secondary education, single, and disabled persons. Residents of smaller cities statistically significantly more often indicated that the changes in physical activity remained after the pandemic, compared to those living in big cities, as well as the residents of smaller cities differed from other groups in stating that the habits of communication formed over a distance remained. People with an income of more than 500 EUR more often reported that the amount of food eaten remained unchanged.
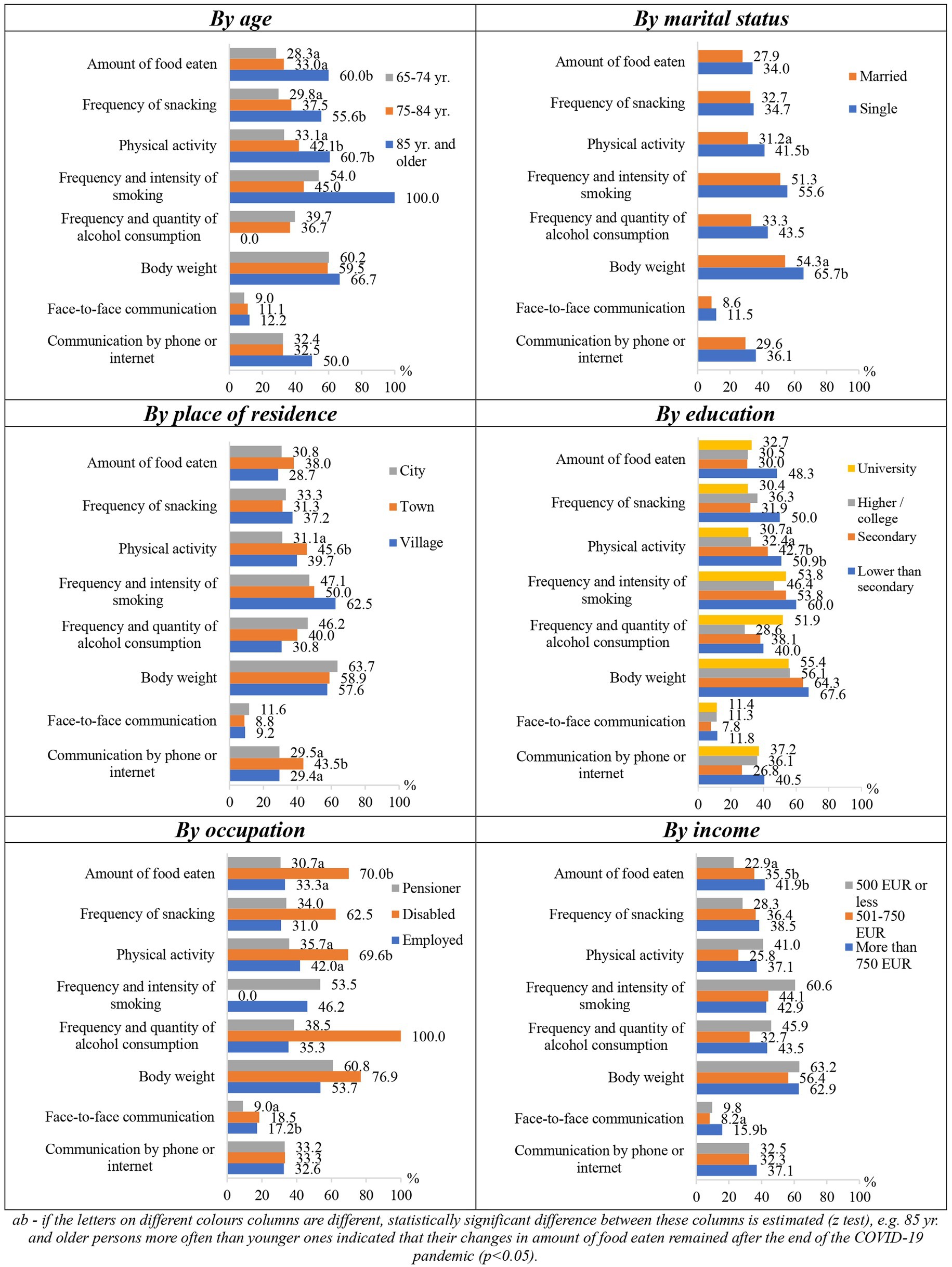
Figure 9. Changes in other lifestyle factors that remained after the end of the COVID-19 pandemic depending on socio-demographic factors.
Obese people, as compared to overweight or low/normal weight ones, more often indicated that changes in their physical activity (48.6% vs. 34.6% vs. 34.0%) and body weight (71.1% vs. 54.7% vs. 56.9%) remained after the pandemic. Also, the respondents, who rated their health as pretty poor/poor, more often indicated that the lifestyle habits formed during the pandemic remained in the post-pandemic period.
4 Discussion
Coronavirus was a major health threat for older adults during the period of pandemics. It is well reported that mortality from COVID-19 was strongly associated with the high prevalence of chronic non-communicable diseases among the older adults (13). Therefore, lifestyle factors contributing to the development of chronic non-communicable diseases must be seriously considered in this age group of population.
A healthy diet is an important health-enhancing factor. A balanced diet strengthens the immune system both through the consumption of anti-inflammatory nutrients and the consumption of fermented foods by the gut microbiota, which provide metabolic compounds involved in the homeostasis of the inflammatory process. Therefore, it is very important to understand whether the period of COVID-19 quarantines may have affected the quality of nutrition and to what extent such changes may have had a long-term effect on the health of the population. An unhealthy diet combined with a concomitant decrease in physical activity can negatively affect health status, leading to an increased prevalence of obesity and other risk factors, which in turn can increase the risk of complications from COVID-19. Fifty-nine studies analyzed changes in eating habits as reflected by the amount of food eaten, cooking at home, snacking, and consumption of takeaway or home delivery. Most of the survey respondents indicated that they increased the number of meals per day and the amount of food eaten during the COVID-19 quarantine. In addition, during the quarantine, cooking at home increased, home-cooked food was eaten more often, and at the same time eating out decreased. Analysis by geographic region revealed substantial similarities in changes in eating patterns across the world, although increases in daily meals were less pronounced in Asian studies than in other regions (14). During a cross-sectional survey conducted in the United Kingdom, 79% of the participants suggested that at least one of the five lifestyle factors studied (healthy diet, overeating, exercise, sleep, alcohol consumption) had worsened. Subjects diagnosed with mental illness or obesity were particularly at increased risk of weight gain during the COVID-19 crisis (15). A similar study in Spain found an increase in emotional eating, “cravings” (the desire to consume certain foods) and eating to compensate for boredom or anxiety after weight gain (16).
Among the sudden changes in public life associated with the impact of the COVID-19 pandemic, a significant decrease in physical activity and a prolonged sedentary lifestyle can be observed. Restrictions on physical activity resulted from closed sports centers and limited social mobility. Social distancing and telecommuting may have contributed to sedentary lifestyles and increased sitting time during the day, as well as shorter periods of vigorous physical activity during leisure time and reduced physical activity, adverse changes in motivation, and individual perceptions of fatigue (17). A population-based survey, conducted in suburban Japan, revealed that due to the COVID-19 pandemic regular/daily exercise decreased – it was reported by the 30% of study participants. The health-related quality of life of these older adults deteriorated independently of their age, gender, body mass index, baseline status of activities of daily living, and musculoskeletal symptoms (18). Many studies have shown that regular physical activity helps prevent the most common chronic diseases, such as diabetes, hypertension, cardiovascular disease, cancer, chronic kidney disease, obesity, osteoarthritis, etc. (19). There is evidence that older adults who engaged in regular physical activity during COVID-19 quarantines had higher stress resilience scores and less symptoms of depression and anxiety (20). The findings from other countries are somewhat like the Lithuanian, nevertheless our study disclosed some specific peculiarities, particularly related to sociodemographic inequalities among older adults of the country.
4.1 Limitations of the study
We collected data about the lifestyle factors among the older adults during and after the COVID-19 pandemic. One of the potential limitations of the current study could be related to the challenges in remembering precisely about their lifestyle factors during the COVID-19 pandemic, because it happened a few years ago. However, this type of limitation could be seen in many survey-based studies where past events are examined.
4.2 Advantages of the study
The important advantage of this study is that it is population-based survey, involving a representative sample of Lithuanian population over 65 years old, therefore the conclusions can be generalized to the entire older adults population of Lithuania. Also, it is important to note, that it examines not only lifestyle factors during the COVID-19 pandemic, but also after the pandemic, which helps to evaluate lifestyle changes related to the COVID-19 pandemic and look at the perspectives in lifestyle of the older adults.
5 Conclusion
Most of the eating habits, e.g., the amount of food eaten, the frequency of snacking, and the body weight of the older adults did not change during the COVID-19 pandemic in Lithuania. Respondents noted that their physical activity decreased, face-to-face communication with relatives became rarer, while communication by phone, Internet or social networks increased. During COVID-19 pandemic, the increased frequency of snacking was more often indicated by the persons with lower than secondary education, working people, and those receiving higher income. An increased snacking and body weight were more prevalent among younger, single or overweight persons; increased weight during the pandemic was also more often mentioned by persons who assessed their health poorly. Physical activity decreased more often among rural residents and groups with higher or college education; face-to-face communication has become rarer among younger people, rural residents, pensioners, the disabled, people with an income of more than 750 EUR and those who are overweight. Remote communication has increased among women, residents with a university education and people with an income of 501–750 EUR (p < 0.05).
Nearly half of the respondents indicated that the changes in food consumption, smoking frequency and intensity that occurred during the COVID-19 pandemic remained after the pandemic, while the other half indicated that they returned to the pre-pandemic level. After the pandemic, the habits of consuming fast food, confectionery or other sweets, as well as the changes in body weight mostly remained, while the characteristics of communication with the close relatives, friends and family members mostly returned to the pre-pandemic level. Most of the healthy lifestyle habits, formed during the pandemic, persisted after it ended. The lifestyle habits, formed during the COVID-19 pandemic, more often remained in the groups of older persons, residents of smaller cities, those with lower than secondary education, higher income, single, disabled, obese people, and those with poorly self-perceived health (p < 0.05).
The current study adds to the research, confirming the impact of pandemics on the lifestyle of older adults, disclosing sociodemographic and spatial inequalities. Identification of the vulnerable groups of older adults is essential for further prediction and development of preventive measures for the future, to improve preparedness for the possible health disasters.
This study is considered as having high practical significance, since the most vulnerable groups among older adults of Lithuania have been detected in terms of lifestyles. Health care providers should pay particular attention to those living in rural areas, the disabled, single persons, as well as those with already prevalent lifestyle risk factors, such as overweight and obesity. Disease prevention and health promotion programs, delivered by primary health care centers and municipality public health bureaus are the key players in reducing inequalities in health care and improving health for older adults of Lithuania.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
Lithuanian University of Health Sciences Bioethics Center permission was received to conduct the study (14.09.2023, No BEC-M-06).
Author contributions
SS: Conceptualization, Writing – original draft. RK: Writing – original draft, Writing – review & editing. VK: Writing – original draft. SK: Formal analysis, Writing – original draft. OM: Writing – original draft.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This research was conducted within the project Impact of the COVID-19 Pandemic on the Health and Lifestyle of the Lithuanian Population aged 65 Years and Older and Development of Recommendations for Health Promotion of the Elderly. The project was financed by the State Fund for Public Health Promotion in 2023, carried out in the framework of the Priority 2, Activity 3.2, Action 3.2.2, Measure 3.2.3.2, The Impact of the Pandemic of the Coronavirus (COVID-19) Disease on the Health and Lifestyle of the Lithuanian Population” (Funding Contract No 2023-PRO-00089).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. World Health Organization. (2020). Coronavirus disease (COVID-19) pandemic. Available at: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (Accessed August 27, 2024).
2. Park, AH, Zhong, S, Yang, H, Jeong, J, and Lee, C. Impact of COVID-19 on physical activity: a rapid review. J Glob Health. (2022) 12:05003. doi: 10.7189/jogh.12.05003
3. Long, E, Patterson, S, Maxwell, K, Blake, C, Bosó Pérez, R, Lewis, R, et al. COVID-19 pandemic and its impact on social relationships and health. J Epidemiol Community Health. (2022) 76:128–32. doi: 10.1136/jech-2021-216690
4. Lebrasseur, A, Fortin-Bédard, N, Lettre, J, Raymond, E, Bussières, EL, Lapierre, N, et al. Impact of the COVID-19 pandemic on older adults: rapid review. JMIR Aging. (2021) 4:e26474. doi: 10.2196/26474
5. Hauner, H, Blanken, CPS, and Holzapfel, C. Long-lasting effects of the COVID-19 pandemic on lifestyle and body weight: results of representative cross-sectional surveys in adults in Germany. BMC Public Health. (2024) 24:1199. doi: 10.1186/s12889-024-18680-x
6. Shinohara, T, Saida, K, Tanaka, S, Murayama, A, and Higuchi, D. Changes in frailty and lifestyle among community-dwelling older adults: a two-point cross-sectional study during and after the COVID-19 pandemic in Japan. Geriatr Nurs. (2024) 58:208–14. doi: 10.1016/j.gerinurse.2024.05.014
7. Caroppo, E, Mazza, M, Sannella, A, Marano, G, Avallone, C, Claro, AE, et al. Will nothing be the same again?: changes in lifestyle during COVID-19 pandemic and consequences on mental health. Int J Environ Res Public Health. (2021) 18:8433. doi: 10.3390/ijerph18168433
8. Alfawaz, H, Yakout, SM, Wani, K, Aljumah, GA, Ansari, MGA, Khattak, MNK, et al. Dietary intake and mental health among Saudi adults during COVID-19 lockdown. Int J Environ Res Public Health. (2021) 18:1653. doi: 10.3390/ijerph18041653
9. Koopmann, A, Georgiadou, E, Reinhard, I, Müller, A, Lemenager, T, Kiefer, F, et al. The effects of the lockdown during the COVID-19 pandemic on alcohol and tobacco consumption behavior in Germany. Eur Addict Res. (2021) 27:242–56. doi: 10.1159/000515438
10. Carreras, G, Lugo, A, Stival, C, Amerio, A, Odone, A, Pacifici, R, et al. Impact of COVID-19 lockdown on smoking consumption in a large representative sample of Italian adults. Tob Control. (2022) 31:615–22. doi: 10.1136/tobaccocontrol-2020-056440
11. Han, MA, and Kim, HR. Smoking behavior changes during COVID-19 among Korean adults. Am J Health Behav. (2021) 45:1031–40. doi: 10.5993/AJHB.45.6.7
12. Health Statistics of Lithuania (2022). Health Information Centre of Institute of Hygiene. Available at: https://www.hi.lt/uploads/Institutas/leidiniai/Statistikos/LT_sveik_stat_health/la_2022.pdf (Accessed August 28, 2024).
13. Grasselli, G, Zangrillo, A, Zanella, A, Antonelli, M, Cabrini, L, Castelli, A, et al. COVID-19 Lombardy ICU network. Baseline characteristics and outcomes of 1591 patients infected with SARS-CoV-2 admitted to ICUs of the Lombardy region, Italy. JAMA. (2020) 323:1574–81. doi: 10.1001/jama.2020.5394
14. Mignogna, C, Costanzo, S, Ghulam, A, Cerletti, C, Donati, MB, de Gaetano, G, et al. Impact of Nationwide lockdowns resulting from the first wave of the COVID-19 pandemic on food intake, eating behaviors, and diet quality: a systematic review. Adv Nutr. (2022) 13:388–423. doi: 10.1093/advances/nmab130
15. Robinson, E, Gillespie, S, and Jones, A. Weight-related lifestyle behaviours and the COVID-19 crisis: an online survey study of UK adults during social lockdown. Obes Sci Pract. (2020) 6:735–40. doi: 10.1002/osp4.442
16. López-Moreno, M, López, M, Miguel, M, and Garcés-Rimón, M. Physical and psychological effects related to food habits and lifestyle changes derived from Covid-19 home confinement in the Spanish population. Nutrients. (2020) 12:3445. doi: 10.3390/nu12113445
17. Koohsari, MJ, Nakaya, T, McCormack, GR, Shibata, A, Ishii, K, and Oka, K. Changes in workers’ sedentary and physical activity behaviors in response to the COVID-19 pandemic and their relationships with fatigue: longitudinal online study. JMIR Public Health Surveill. (2021) 7:e26293. doi: 10.2196/26293
18. Tamai, K, Terai, H, Takahashi, S, Katsuda, H, Shimada, N, Habibi, H, et al. Decreased daily exercise since the COVID-19 pandemic and the deterioration of health-related quality of life in the elderly population: a population-based cross-sectional study. BMC Geriatr. (2022) 22:678. doi: 10.1186/s12877-022-03316-9
19. Parameshwar, A, Maiya, GA, Kamath, SU, and Shastry, BA. Ravishankar lifestyle modification with physical activity promotion on leptin resistance and quality of life in metabolic syndrome - a systematic review with Meta-analysis. Curr Diabetes Rev. (2021) 17:345–55. doi: 10.2174/1573399816666200211102917
Keywords: COVID-19, pandemic, lifestyle, eating habits, physical activity, social engagement, smoking, alcohol consumption
Citation: Sauliune S, Kalediene R, Kalibatas V, Kaseliene S and Mesceriakova O (2025) Lifestyle changes among older adults during and after COVID-19 pandemic in Lithuania. Front. Public Health. 12:1504193. doi: 10.3389/fpubh.2024.1504193
Edited by:
Antonio Sarría-Santamera, Nazarbayev University, KazakhstanReviewed by:
Carlos Navarro, Alfonso X el Sabio University, SpainBalnur Omarova, Ahmet Yesevi University, Kazakhstan
Copyright © 2025 Sauliune, Kalediene, Kalibatas, Kaseliene and Mesceriakova. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Skirmante Sauliune, c2tpcm1hbnRlLnNhdWxpdW5lQGxzbXUubHQ=