 Maaidah Algamdi
Maaidah Algamdi- Community and Psychiatric Health Nursing Department, Faculty of Nursing, University of Tabuk, Tabuk, Saudi Arabia
Background: Self-esteem (SE) and obesity have been associated in various studies. This study investigates this relationship among adults in Saudi Arabia. The objectives of this study are to investigate the relationships between SE and body mass index (BMI) and to examine the interactions between sociodemographic-related factors.
Methods: We designed a cross-sectional study using an online survey that included sociodemographics, a BMI measure, and the Rosenberg Self-Esteem Scale.
Results: Levels of SE did not change substantially between the various age groups, as indicated by the Chi-Square test X2 (12, N = 332, = 5.278, p-value = 0.948). The results for males reveal that there is a variation in the levels of SE across the different BMI categories. This suggests that the BMI categories have a major influence on the levels of SE among males. In both genders, the results indicate a negative association between variables, with a higher BMI being associated with a lower level of SE. The significance of this association stands for both genders (p-value <0.001). For males, the association has a greater influence (Estimate = −0.110, p-value <0.001) than it does for females (Estimate = −0.099, p-value <0.001). In females, the negative link is larger for education (−0.273) and highly impactful (p-value <0.001) in comparison to men (Estimate = −0.157, p-value <0.001). Higher education levels are associated with a lower BMI (p-value = 0.018). For men, the indirect effects show that education (Estimate = 0.0173*) and marital status (Estimate = −0.0405*) significantly influence SE, with other factors mediating these effects. Both genders experience significant and detrimental impacts from BMI on SE, with males experiencing a more pronounced impact. There are considerable disparities in the ways in which these parameters impact SE in both genders, as revealed by the comparisons of the nested models.
Conclusion: There is a negative correlation between BMI and SE in both genders, with a more pronounced impact in men. Gender-specific differences in the relationship between BMI and SE underscore the importance of considering distinct pathways for males and females in future analyses.
Introduction
Recent years have seen the emergence of obesity as a disease that is both complicated and multifaceted, and it continues to have a broad influence on a worldwide scale. The prevalence of obesity has grown considerably over the last four decades, reaching approximately a third of the world’s population at present (1, 2). By 2040, more than 50% of people will be obese or overweight, and the global pandemic of obesity, known as ‘globesity’, has gained widespread recognition (3–5). Compared to men, women are more likely to be overweight or obese due to the unique physical changes associated with pregnancy and childbirth, as well as the fact that they lead more sedentary lifestyles and are thus more vulnerable to the harmful effects of obesity and overweight (4). Comorbidities, such as type 2 diabetes, certain types of cancer, hypertension, heart failure, stroke, and hypercholesterolemia, have all been linked to obesity (6–8) and have led to increased healthcare expenses (9). The net result is a poor quality of life for those who are struggling with excessive body weight (10).
In addition to these detrimental effects, people who are overweight or obese usually face prejudice and social stigma, which makes the already complex issue much more difficult to deal with (11). Accordingly, obese people typically exhibit lower levels of self-esteem (SE) than non-obese people (12–15), due to society’s negative opinion about them (16). Furthermore, a higher prevalence of negative body image in females compared to males relates to poor SE, as are many psychological problems, including behavioral disorders, melancholy moods, and unpleasant, uncontrollable emotions (17–19). The negative relationship between SE and obesity is well-documented (20, 21), and research in Jordan and Saudi Arabia further supports this inverse correlation (22, 23). Certain studies indicate a causal association, attributing the reason to inadequate diet and exercise (24). Additionally, a study in Sanandaj, Iran demonstrated that a lifestyle training program led to greater weight loss and improved SE, demonstrating the positive impact of weight loss on the mental health of obese individuals (25). In fact, a study in Esfahan, Iran reported significant improvements in SE and body mass index (BMI) following cognitive-behavior therapy, revealing that both lifestyle and cognitive interventions effectively reduced BMI and enhanced the quality of life in obese patients (26). Research has widely demonstrated that BMI, a negative biological component, contributes to negative body image and anxiety about unfavorable appraisal (19, 27–29). Higher levels of SE may also be linked to increased levels of physical activity, which improves weight status (30), as well as healthy eating habits, including a stronger adherence to a healthy diet, such as the Mediterranean diet (31), and a lower consumption of soft beverages. While several studies have found a possible correlation between SE and weight (32–34), no studies have found a definitive link between the two.
Despite the increasing amount of research on the various risk factors for weight gain, such as education, genetics, biology, sociodemographic factors, environment, and behavior (35, 36), the fundamental elements that could lead to an understanding of the interaction between men and women in Saudi Arabia remain unclear. As far as we are aware, there has not been any study looking at the probability of a correlation between weight changes and SE adjustments in a large adult population over time. This study examined SE, BMI, and other sociodemographic and lifestyle factors. With the following study questions, we intend to determine the extent to which there is a relationship between BMI and SE among people in Saudi Arabia: (1) What is the prevalence of obesity and SE among the studied sample? (2) Is there any relationship between the sociodemographic characteristics of the sample and the BMI and SE? What is the relationship between BMI and SE?
Methodology
Design
The study used an observational, cross-sectional approach. We collected data from individuals in Saudi Arabia to assess the relationship between BMI, SE, and the participants’ sociodemographic characteristics.
The research required a convenient sample of Saudi Arabian individuals aged 18 and above who possessed literacy skills. The sample size was determined utilizing the following formula: n = N * X/ (X + N – 1), where X was defined as Zα/2 * p * (1 - p) /MOE2. Here, Zα/2 represents the critical value of the normal distribution at α/2 (e.g., at a 95% confidence interval, α = 0.05 and c = 1.96), MOE denotes the margin of error, p indicates the sample percentage, N refers to the population size, and n = sample size. Given the indeterminacy of the prevalence percentage, we applied an estimate of 50%. This formula produced a sample size of 384. We collected data over 4 months using an online survey, completing a total of 332 surveys. The dependent variable was SE, while the independent variables included age, gender, marital status, education, occupation, weight, height, smoking, and chronic illness. The cross-sectional design examined the moderating effect of BMI.
Data collection method
We collected data using an online survey over a four-month period. We distributed the survey using various social media platforms to reach a diverse audience. This approach ensured wide accessibility and convenience for participants, enabling responses from individuals across different locations and demographics.
Instruments
In this study, we used three instruments to assess the variables: the sample’s sociodemographic characteristics, SE, and BMI. Sociodemographic characteristics included age, gender, marital status, education, occupation, weight, height, smoking, and chronic illness. We assessed self-esteem using the Rosenberg Self-Esteem Scale (RSES) (37), following the original manual’s scoring system that divided the scores into three categories: poor (0–14.9), average (15–25), and high (25.1–30). BMI was calculated according to the following formula: (weight in kilograms/square height) kg/m2. We categorize BMI as follows (38): underweight (15–19.9), normal weight (20–24.9), overweight (25–29.9), Class I (30–34.9), Class II (35–39.9), and Class III (≥ 40).
Data analysis
We used Analysis of Moment Structures (AMOS) for structural equation modelling (SEM) to evaluate the direct and indirect relationships between one or more independent latent variables and dependent variables, providing a more robust analysis than traditional multivariate methods like multiple regression. SEM enables the simultaneous simulation of multiple independent and dependent constructs. We coded the data in an Excel sheet, treated it for missing variables, and then transferred it into the Statistical Package for Social Science (SPSS) software. We performed the analysis using SPSS version 23.0 (IBM, Armonk, NY, USA) at a 95% confidence interval. We checked the data for completeness and correctness. Typically, we use normality tests to verify the normal distribution of a continuous variable. However, categorical variables, not being continuous, cannot conform to a normal distribution. Nominal data represent categories without a specific order or ranking, such as gender, marital status, occupation, etc. Unlike continuous or ordinal data, nominal data do not have a numerical relationship that allows for skewness or kurtosis analysis (39–42). As an example, it’s possible that answers in datasets like 1, 2, 3, and 4 are three times more likely to be in a higher category than the lowest category. We might treat them similarly to 1 or 2, assuming equal distances, which could lead to erroneous conclusions (43). Therefore, normality does not apply to nominal data in the same way as it does to interval or ratio data (44).
Ethical consideration
We obtained ethical approval # UT-120-15-2020 from the University of Tabuk Local Research Ethic Committee, attached informed consent to the beginning of the questionnaire, and allowed anyone who agreed to participate to fill it out without needing to sign a name or phone number. Participation in the study is entirely voluntary, and we maintain anonymity and confidentiality throughout all stages of the study. The principal investigator provided the participants with complete contact information for informed consent.
Descriptive statistics of demographic variables
Table 1 provides a comprehensive overview of the distribution of various demographic factors among the research participants (N = 332). The variables consist of gender, marital status, education, employment, smoking status, chronic illness status (ChronicDx), BMI categories, and the RSES scores. The variable “Gender” categorizes the distribution of participants based on their gender in the research sample. Of the 332 participants, 62.35%, or 207 individuals, belong to the male gender. This indicates that a substantial majority of the individuals included in the study are male, underscoring a potential disparity in gender representation within the sample. Conversely, the data reveals that 125 individuals, comprising 37.65% of the entire sample, are female. The gender distribution in this study gives important contextual information on the representation of each gender within Saudi religious and cultural backgrounds. This information might have an impact on the generalizability and applicability of the study’s findings to larger groups. The chi-square test produced a significant outcome (Chi-Square = 20.253, df = 1, p-value = <0.001), signifying a statistically significant difference in gender distribution within the sample. The chi-square test results (Chi-Square = 240.072, df = 3, p-value = <0.001) demonstrate a considerable difference in the distribution of marital status among the research participants. There exists a substantial disparity in levels of education, occupational distribution among participants, smoking status, prevalence of chronic illness, and classifications of participants’ BMI. The RSES figures indicate that most participants had medium self-esteem, whereas a lesser percentage demonstrated negative SE.
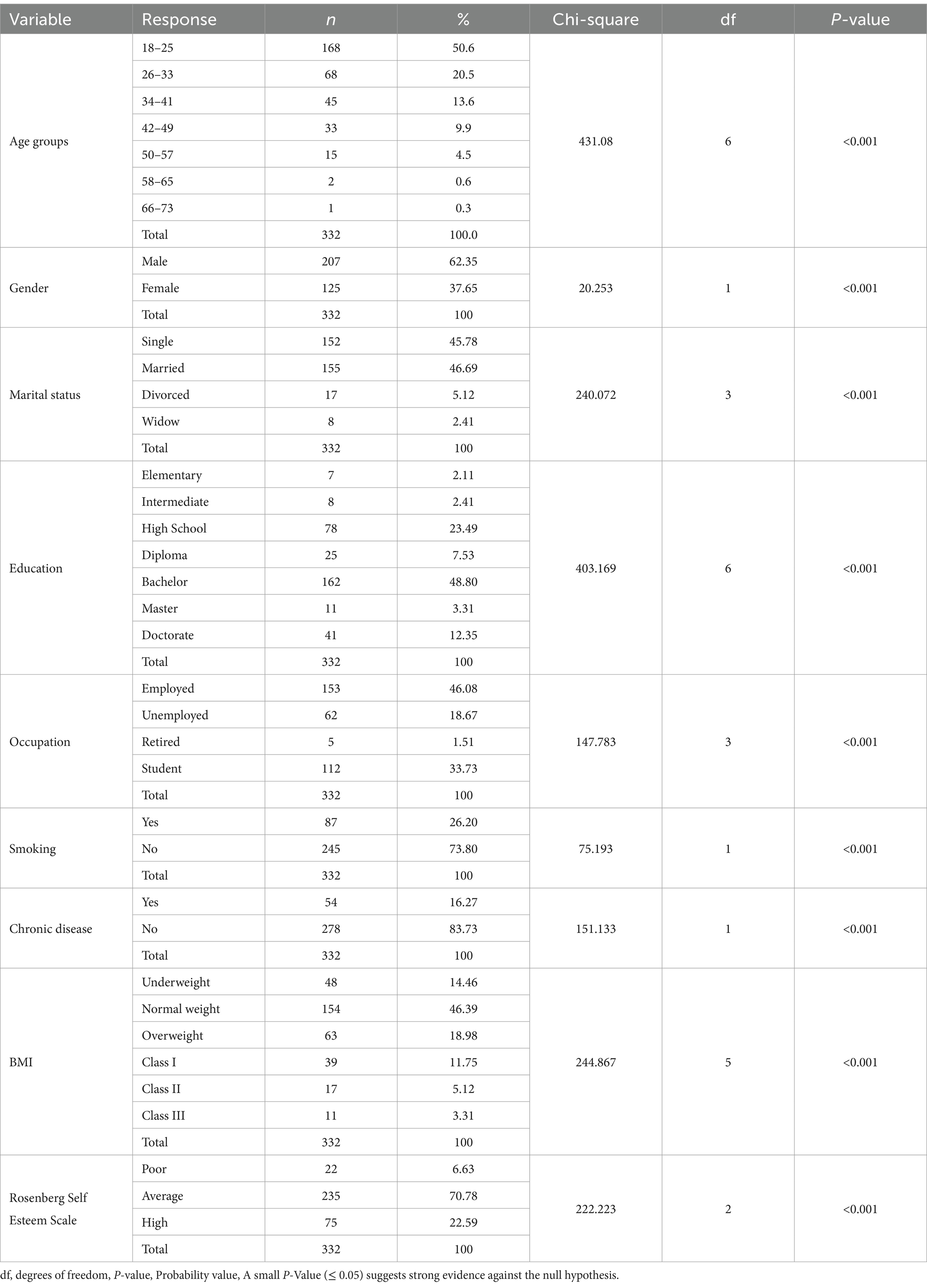
Table 1. Demographic and health variables with their chi-square tests.
Self-esteem scale by demographic and health variables
Table 2 presents the results of the RSES across various demographic and health variables, using chi-square tests for independence. The age groups ranged from 18 to 73 years. SE levels did not vary significantly across the different age groups (X2 [12, N = 332] = 5.278, p-value = 0.948). Both male and female participants had similar distributions of SE levels. No significant relationship between gender and SE levels was observed (X2 [2, N = 332] = 2.235, p-value = 0.327). The participants’ marital status significantly influenced SE levels by associating different marital statuses with varying levels of SE. We found a significant relationship between education level and SE, with higher educational attainment significantly influencing different levels of SE, suggesting that education significantly influences SE. The distribution of SE varied significantly across occupational statuses, which highlighted the impact of occupation on SE. Furthermore, the SE levels of smokers and non-smokers varied significantly, and the presence or absence of chronic diseases significantly correlated with SE, indicating that individuals with chronic diseases had different SE levels compared to those without. Figure 1 for males shows the distribution of SE levels across different BMI categories.
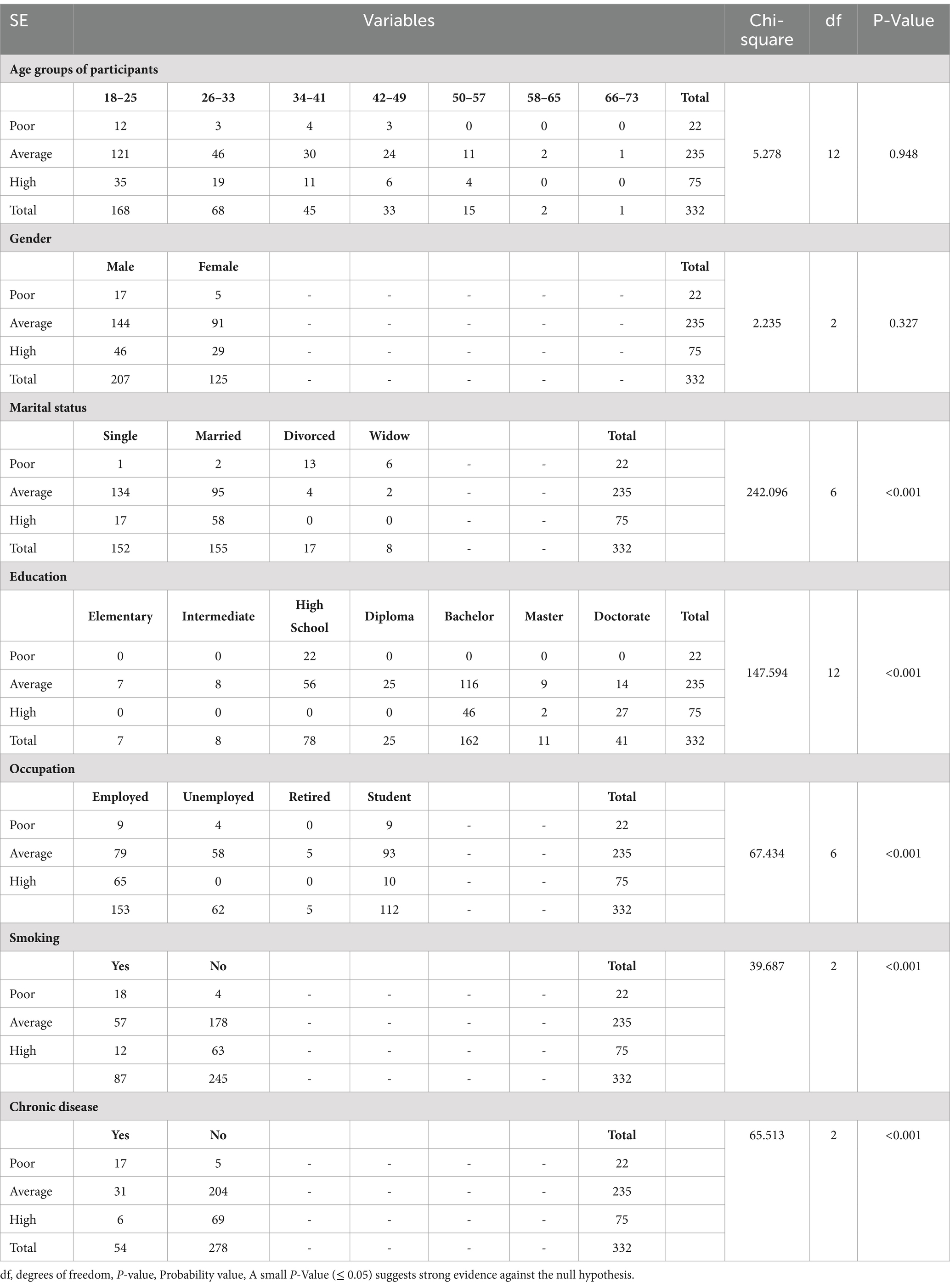
Table 2. SE scale by demographic and health variables.
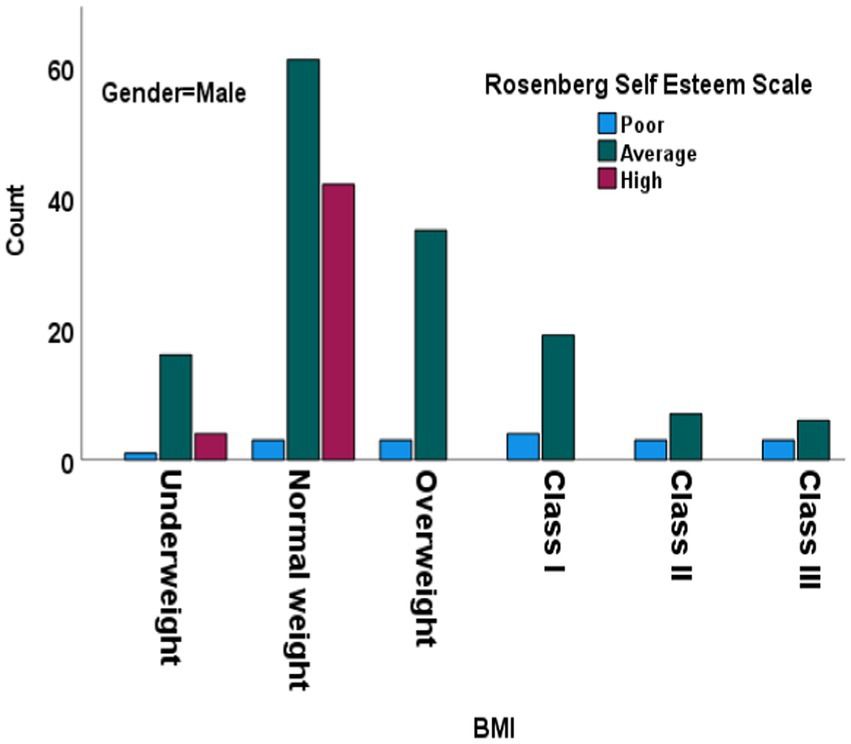
Figure 1. Chi-square test results for Rosenberg Self-Esteem Scale across BMI categories in males. BMI: body mass index. Df, degree of freedom.
We categorized SE levels into three categories: poor, average, and high. Most underweight males fell into the average SE category (16), with fewer in the high (4) and poor (1) categories. Only three members of the normal-weight group fell into the poor category, compared to a higher number of members in the average (61) and high (42) categories. This suggests a positive correlation between normal weight and higher SE. Notably, there were no members from the Overweight, Class I Obesity, Class II Obesity, and Class III Obesity groups who were in the high SE category. Furthermore, the chi-square test for males showed a significant difference in SE levels across BMI categories, indicating that BMI categories significantly impact SE levels among males. Most normal-weight females (Figure 2) were in the average (29) and high (19) categories, with none in the poor category, suggesting a strong correlation between normal weight and higher SE (p-value <0.001). Both males and females had a majority in the average SE category, but females had a higher count in the high SE category compared to males. Both genders exhibited higher SE among members of the normal-weight category, with males having a slightly higher count in the high SE category. The chi-square test results reinforce the observation that BMI categories significantly impact SE levels for both genders, with normal-weight individuals generally exhibiting higher SE compared to those in higher BMI categories. This underscores the relationship between BMI and SE and highlights the psychological implications of weight categories on self-perception and confidence levels in both males and females.
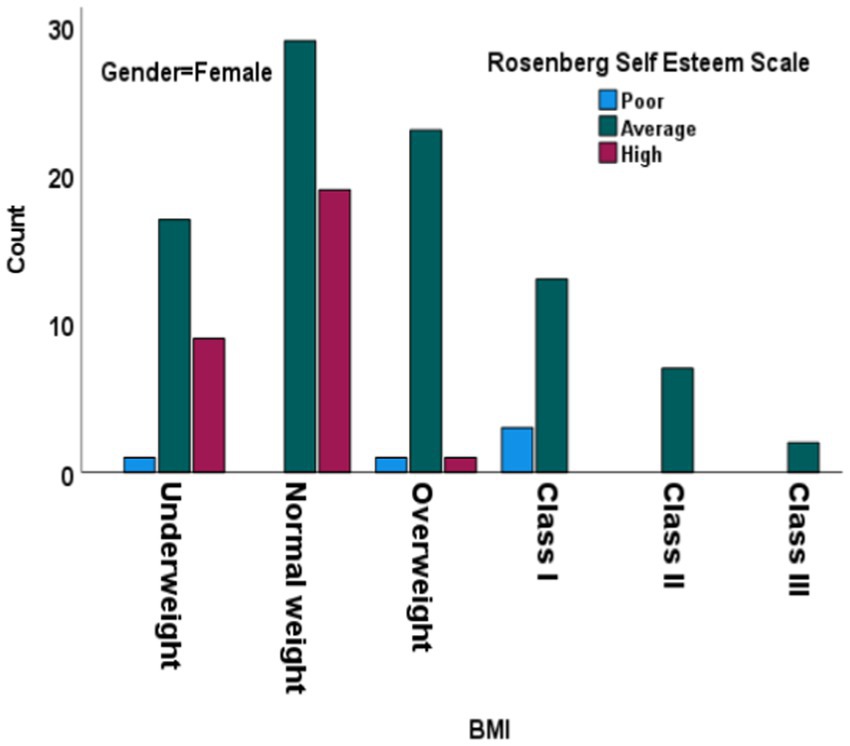
Figure 2. Chi-square test results for Rosenberg Self-Esteem Scale across BMI categories in females. BMI: body mass index. Df, degree of freedom.
Model fit diagnostics for unconstrained and constrained model
Table 3 contrasts the model fit indices for the unconstrained and constrained (male vs. female groups) models. Table 3 contrasts the reported indices. The indices include the Tucker-Lewis index (TLI), comparative fit index (CFI), root mean square error of approximation (RMSEA), root mean square residual (RMR), normed fit index (NFI), relative fit index (FRI), incremental fit index (IFI), goodness of fit index (GFI), adjusted goodness of fit index (AGFI), and chi-square value (CMIN). The male vs. female model had a CMIN/DF ratio of 2.1243, whereas the unconstrained model had a CMIN/DF ratio of 2.1388. Furthermore, the unconstrained model had an RMR of 0.0197, a GFI of 0.9957, and an AGFI of 0.9105 in the RMR and GFI sections. The RMR, GFI, and AGFI for the male vs. female models were 0.0449, 0.9775, and 0.9141, respectively. The Baseline Comparisons section displays the fit indices for both models—NFI, RFI, IFI, TLI, and CFI. Each of these indices showed a strong match. The unconstrained model had an RMSEA of 0.0587, while the male vs. female model had an RMSEA of 0.0584. Thus, all metrics followed the threshold values (45).
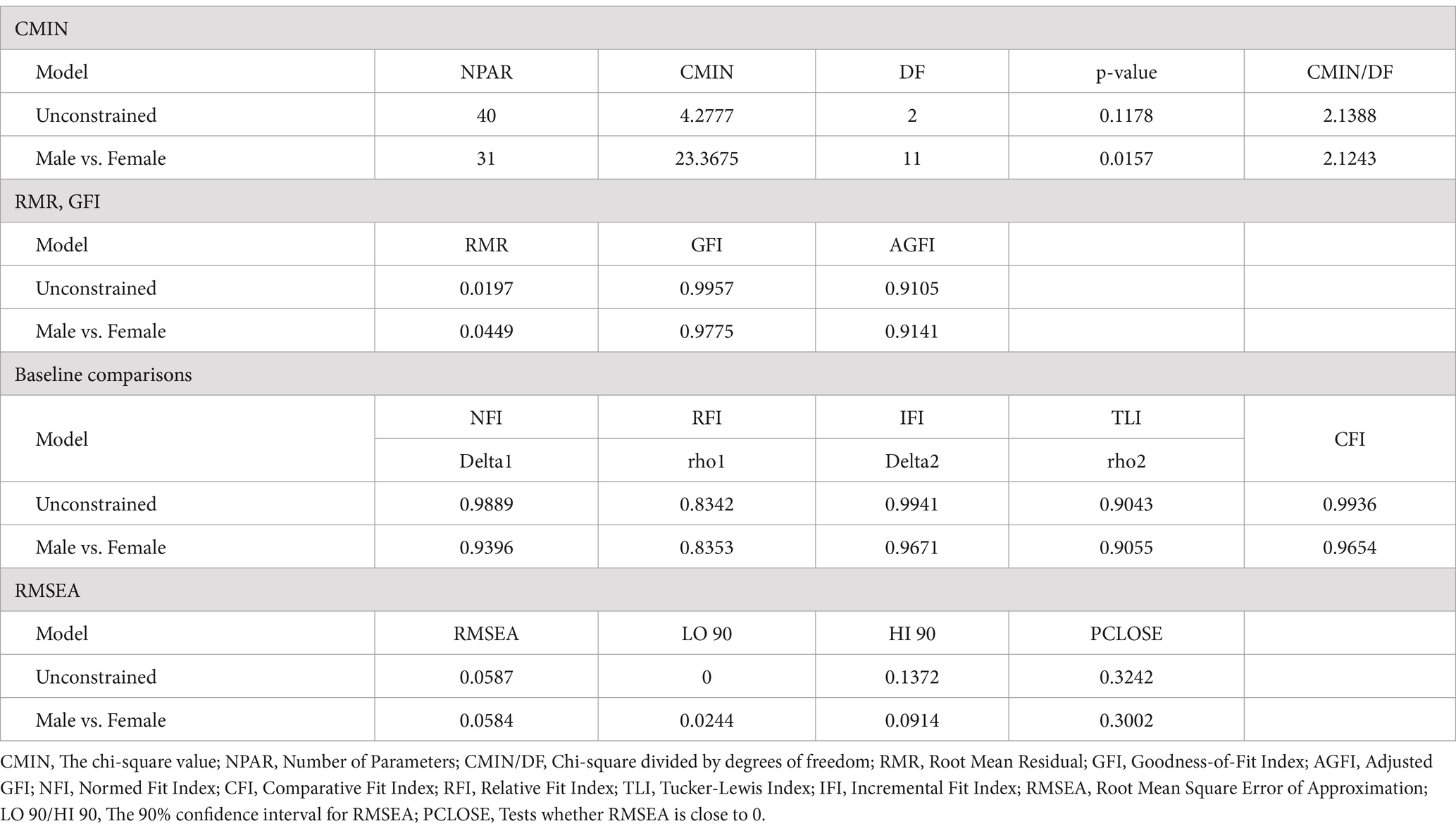
Table 3. Model fit summary of unconstrained vs constrained (Male vs Female) models.
Impact analysis
The analysis indicates that for both genders, a higher BMI is associated with lower SE, demonstrating a negative relationship (Table 4). This relationship is statistically significant for both males and females (p-value <0.001). However, the impact of BMI on SE is slightly more pronounced for males, with an estimate of −0.110, compared to an estimate of −0.099 for females. While both genders link increased BMI to decreased SE, the effect is marginally stronger in males, suggesting that BMI may play a more critical role in influencing SE in men than in women. For both genders, a negative relationship suggests that higher BMI decreases SE. The relationship is more impactful for males (Estimate = −0.110, p-value <0.001) than for females (Estimate = −0.099, p-value <0.001).
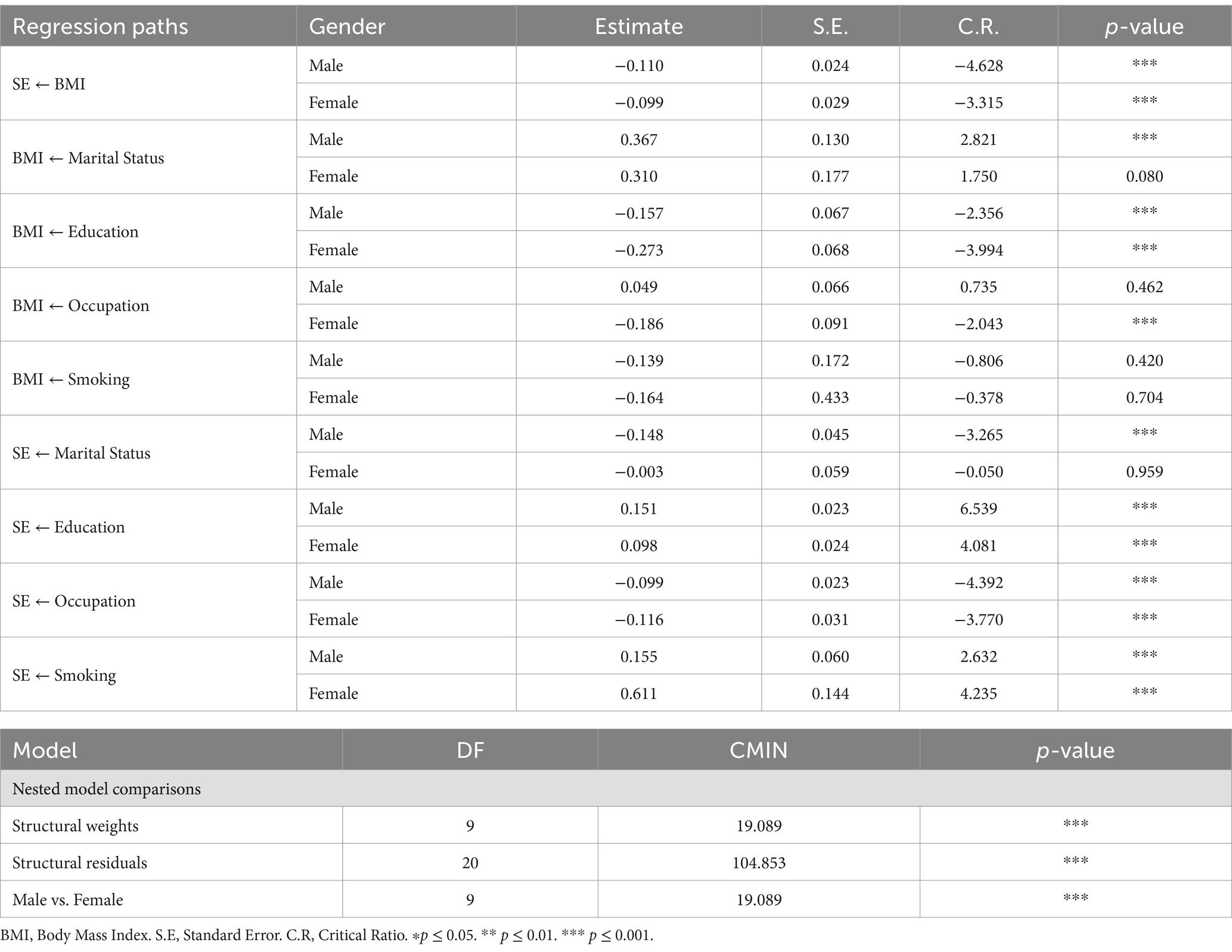
Table 4. Gender-based differences in regression paths and nested model comparisons.
For males, a positive relationship (Estimate = 0.367) indicates that being married or having a certain marital status increases BMI (p-value = 0.004). For females, the relationship is also positive (Estimate = 0.3095), but not statistically significant (p-value = 0.080). For males, a negative relationship (Estimate = −0.157) suggests that higher education levels are associated with lower BMI (p-value = 0.018). For females, the negative relationship is stronger (estimate = −0.273) and highly impactful (p-value <0.001). For females, a negative relationship (Estimate = −0.186) suggests certain occupations are associated with lower BMI (p-value = 0.040). For males, the relationship is not significant (Estimate = 0.049, p-value = 0.462). Regarding smoking, the relationship is not significant for both males (Estimate = −0.139, p-value = 0.420) and females (Estimate = −0.164, p-value = 0.704). For males, a negative relationship (Estimate = −0.148) indicates that being married or having a certain marital status decreases SE (p-value = 0.001). For females, the relationship is not significant (Estimate = −0.003, p-value = 0.959).
For both genders, a positive relationship indicates that higher education levels increase SE. The relationship is highly impactful for males (Estimate = 0.151, p-value <0.001) than females (Estimate = 0.098, p-value <0.001). For both genders, a negative relationship suggests that certain occupations decrease SE. The relationship is significant both for males (Estimate = −0.099, p-value <0.001) and females (Estimate = −0.116, p-value <0.001). For both genders, a positive relationship indicates that smoking increases SE. The relationship is significant for males (Estimate = 0.155, p-value = 0.008) and highly significant for females (Estimate = 0.611, p-value <0.001). For both genders, a positive relationship indicates that smoking increases SE. The relationship is stronger for females (Estimate = 0.611, p-value <0.001) than for males (Estimate = 0.155, p-value = 0.008). The nested model comparisons indicate significant differences in the structural weights and residuals between the male and female models. The chi-square values (CMIN) for structural weights and the overall model comparison are significant (p-value <0.05), which means that gender seems to change how the predictors and outcomes are related. Thus, higher education and smoking are positively associated with SE for both genders, while a higher BMI is negatively associated with it. The impact of marital status and occupation on BMI and SE varies between males and females.
Effect evaluation
Total effects
For males (Table 5), smoking has a positive total effect on SE (Estimate = 0.1702*), while education (Estimate = 0.1684*) and marital status (Estimate = −0.1885*) also significantly influence SE. However, BMI negatively impacts SE (Estimate = −0.1104*). For females, smoking has a much larger positive total effect on SE (Estimate = 0.6279*) compared to males. Education (Estimate = 0.1259*) also has a positive total effect on SE, while occupation (Estimate = −0.0981 ns) and marital status (Estimate = −0.0337 ns) are not significant. BMI negatively impacts SE (Estimate = −0.0991*).
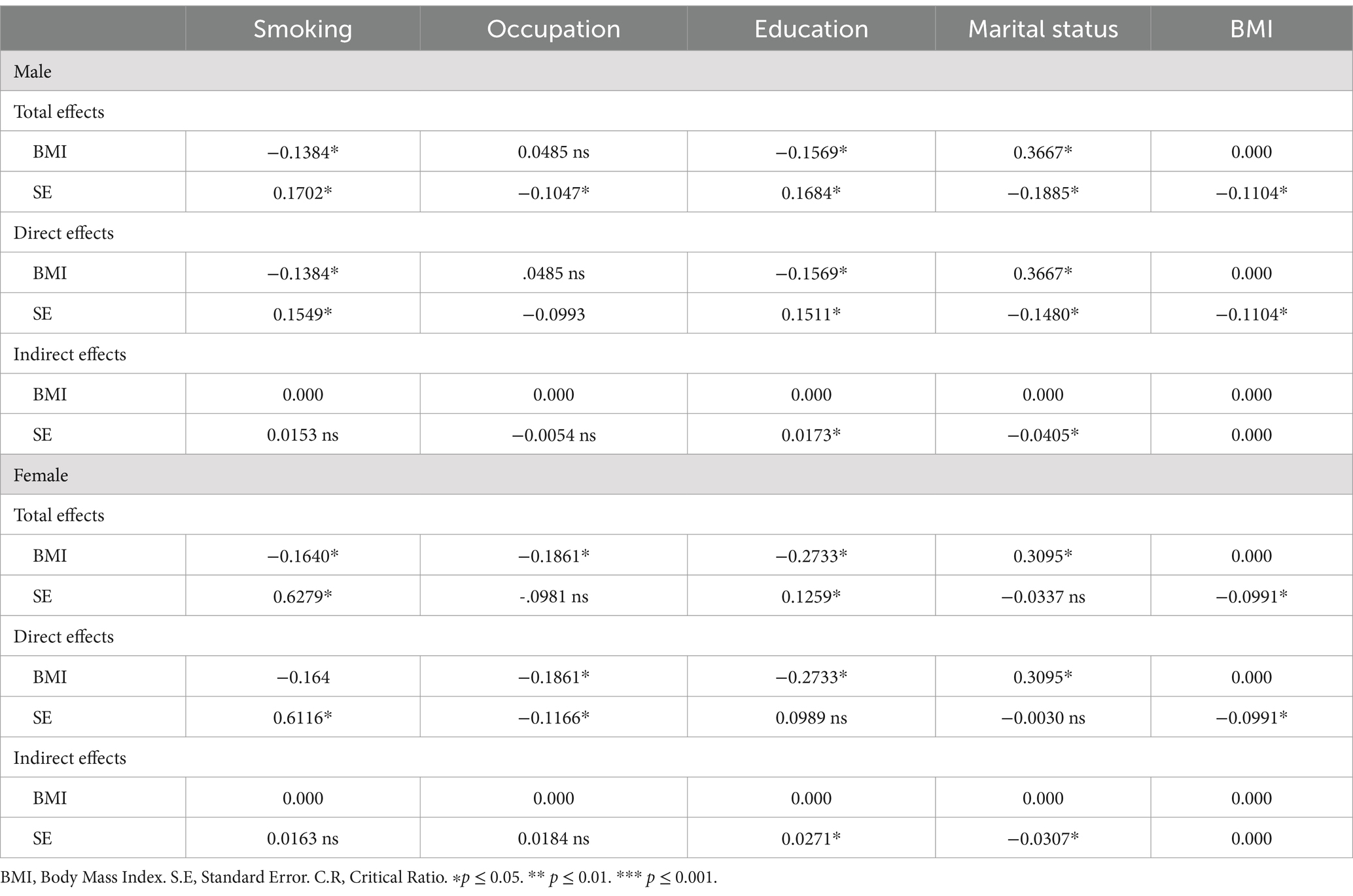
Table 5. Gender-based breakdown of total, direct, and indirect effects of BMI on SE.
Direct effects
For males, the direct effects show that smoking (Estimate = 0.1549*) positively impacts SE, while education (Estimate = 0.1511*) and marital status (Estimate = −0.1480*) are significant influencers. BMI continues to have a negative direct effect on SE (Estimate = −0.1104*). For females, smoking has a strong positive direct effect on SE (Estimate = 0.6116*), while occupation (Estimate = −0.1166*) is negatively significant. Education (Estimate = 0.0989 ns) and marital status (Estimate = −0.0030 ns) do not have significant direct effects. BMI negatively impacts SE (Estimate = −0.0991*).
Indirect effects
For males, indirect effects show that education (Estimate = 0.0173*) and marital status (Estimate = −0.0405*) have significant impacts on SE, mediated by other variables. Smoking and occupation do not have significant indirect effects on SE. For females, education (Estimate = 0.0271*) and marital status (Estimate = −0.0307*) have significant indirect effects on SE, while smoking and occupation do not have significant indirect effects. The analysis indicates that both the total and direct effects of BMI on SE are negative and significant for both genders, though the impact is slightly more pronounced for men. Smoking has a significant positive impact on SE for both genders, with a stronger effect in females. Education positively influences SE in both genders, while occupation and marital status show varying impacts. The nested model comparisons reveal significant differences in how these factors influence SE between males and females, emphasizing the importance of considering gender-specific pathways when understanding the relationship between BMI and SE. Figure 3 visualizes the gender-specific demographic impacts on SE.
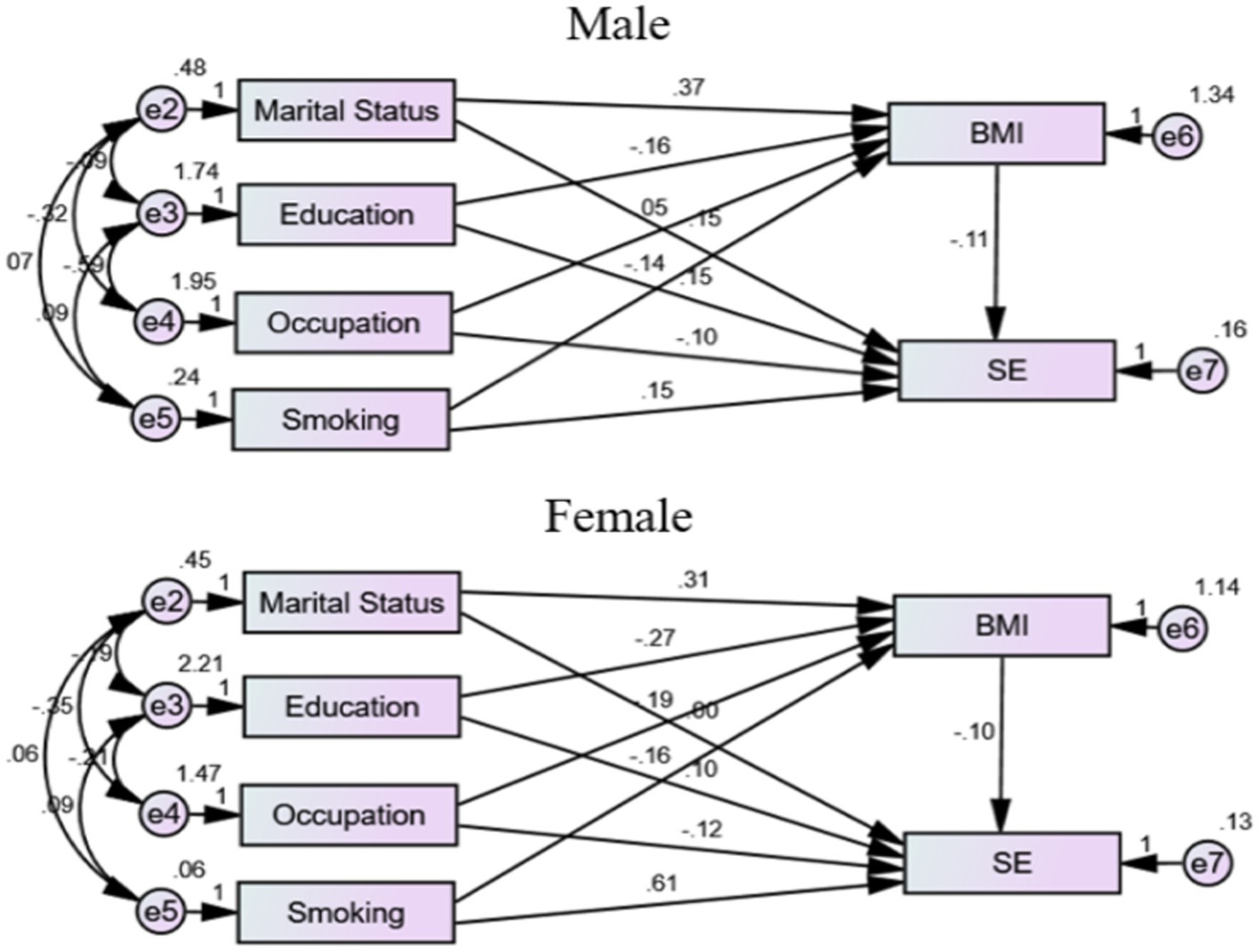
Figure 3. Gender-specific demographic impacts on SE. BMI: body mass index. SE: self-esteem.
Discussion
This study explored SE levels across various demographic, socioeconomic, and health-related factors. Age ranged from 18 to 73 years, with SE levels remaining consistent across age groups, suggesting stability of SE throughout adulthood. Research on SE stability across adulthood indicates fluctuations depending on life stages. According to Trzesniewski et al. (46) SE stability is quite low during childhood, improves throughout adolescence and early adulthood, and then starts to decline during midlife and older age. Orth et al. (47) observed that SE tends to increase from adolescence to middle adulthood, peaking around ages 50 to 60, before declining into old age. Gender analysis revealed similar SE distributions for males and females, with no significant associations, supporting the idea that gender may not critically influence SE (25). Marital status emerged as a significant factor, with different marital statuses linked to varying SE levels, possibly reflecting the social and emotional dimensions of relationships attributed to the emotional support and social validation inherent in marital relationships (48). Education level showed a strong positive correlation with SE, emphasizing its role in enhancing SE and societal standing, which is in line with a study that found that SE positively predicted academic engagement, which is closely linked to educational attainment (36). Similarly, occupational status significantly influences SE; individuals who are employed tend to report higher SE compared to those who are unemployed; this is due to the positive identity and social validation that employment provides. Employment reinforces worker identity, enhancing self-confidence as a component of SE (49), highlighting the psychological benefits of professional engagement.
Health factors also played a role, with smokers exhibiting distinct SE levels compared to non-smokers. However, studies revealed that smokers often have lower SE, which may influence their smoking behaviors. For instance, Barros et al. discovered that smokers exhibited lower levels of mindfulness and subjective well-being, closely associated with SE, in comparison to non-smokers (50). Additionally, Carter and Byrne reported that people with low SE, particularly in areas such as academics and relationships with parents, were more likely to engage in smoking compared to their peers with higher SE (51). The significant positive correlation between smoking and SE illustrates a paradoxical trend, suggesting that individuals may view smoking as a socially empowering or stress-relieving activity, potentially boosting their self-confidence. The relationship between smoking and SE is complex and varies across different studies. While many studies have found a negative association between smoking and SE, some research suggests that, in certain contexts, smoking may be associated with higher SE, particularly among females. For instance, a Tabriz, Iran study revealed that SE had no conceptual effect on smoking among males. However, the study found that smoking among females decreased with decreasing SE, suggesting that higher SE may be associated with increased smoking behavior among females (52). Additionally, chronic disease presence significantly impacted SE, indicating the influence of physical health on psychological well-being. Ji et al. found that middle-aged and older patients with chronic illnesses exhibited lower SE, which adversely affected their quality of life (53).
The study’s findings for both genders indicate a negative association between a greater BMI and a lower level of SE. The statistical significance of this association was high (p-value <0.001) for both males and females. Male BMI had a greater effect on SE than female BMI, with an estimate of −0.110 versus −0.099. Because of this, it appears that, although an increasing BMI is associated with a drop in SE for both males and females, the impact is somewhat stronger in males. This shows that BMI may play a more significant role in determining SE in males than in females.
An existing study showed a larger negative link between BMI and body image among individuals with lower levels of SE (54). These findings are consistent with the results of the current study, which highlight the considerable influence that BMI has on one’s sense of self-worth. There is a negative correlation between a higher BMI and a decrease in the RSES scores for both genders.
In a different study, researchers surveyed 410 teenagers, 51.2% of whom were female and 55.1% of whom were between the ages of 13 and 15 (15). Girls showed a considerably lower SE score than boys did when it came to the categories of obesity and overweight. However, in the overweight group, there was no significant relationship between SE scores based on BMI categories and eating habits, particularly with regard to eating meals with family. This was the case despite the fact that females had a lower mean SE score compared to boys. These findings are consistent with the results of the current study, which highlight the subtle distinctions in the ways that gender and BMI categories affect SE.
One study (23) found that the prevalence of poor SE among Saudi undergraduate women was just 6.1%. However, this percentage was much higher (9.8%) among individuals who were overweight or obese. This conclusion is also consistent with the findings of the current study, which highlight the detrimental effect that a greater BMI has on the SE of females.
Using path analyses to test for mediation, Skorek et al. (55) discovered that self-worth mediated the association between the three personality qualities and body esteem in both men and women. This was the case regardless of whether the individuals were male or female. We found a connection between higher degrees of extraversion, emotional stability, and conscientiousness and higher levels of SE, which in turn led to higher levels of body esteem. However, the model’s incorporation of SE found the associations between personality characteristics and body esteem to be insignificant, indicating the presence of complete mediation. This study lends credence to the notion that SE plays a significant part in mediating the relationship between BMI and general contentment with one’s body image.
In another study, Satwik et al. (56) discovered that factors such as education level, BMI, social support system, diagnosis of mental illness, and perception of menopause were significant predictors of negative body image. The frequency of negative body image among women in their middle years was 17.4%, and this variable had a high correlation with both low SE and mood disorders. Factors such as having a lower education status, a higher BMI, a negative impression of menopause, a weak social support network, and a history of mental health diagnosis enhanced the likelihood of having a bad body image among middle-aged women. Likewise, according to the findings of this study, BMI is one of the numerous essential variables that contribute to body image and SE.
Among pregnant Saudi women, Ghamri et al. (57) discovered a significant positive link between SE and the degree to which they were satisfied with their bodies. The study specifically demonstrated a variable degree of correlation between body image satisfaction, SE, and socioeconomic characteristics, including level of education and income, smoking, and psychiatric and medical comorbidities. Furthermore, the study revealed that the respondents experienced higher levels of Self-Esteem (SE) during the initial weeks of their pregnancies. These studies reveal a strong relationship between body satisfaction and SE, with various elements, including BMI, having an impact.
In their study, Shahzadi and Rasheed investigated the association between gender and SE in obese young girls and boys in Punjab, Pakistan (58). Specifically, they were interested in determining the relationship between body image, BMI, body form dissatisfaction, and body dimensions. In this case, there was a significant correlation between gender, BMI, body shape dissatisfaction, and SE. However, the researchers discovered that there were significant variations between girls and boys in terms of their SE and body image. In comparison to males, girls exhibited significantly higher mean scores for body image dissatisfaction, which resulted in a decrease in their individual SE. This study recommends using the media to increase awareness about the importance of maintaining a positive body image to protect and enhance individuals’ mental and physical health.
Another study conducted by Gómez-Díaz et al. (59) with a total of 55 participants, consisting of 25 males and 30 females, revealed a weight loss of 11 kilograms for females and 16.3 kilograms for males. The study revealed an increase in positive body image perception by 65.2% for women and 76.1% for males, respectively. In addition, there was a rise of 51.4% in the level of SE among women and a rise of 60.3% among males. According to these findings, both men and women can experience considerable changes in their perceptions of their bodies and their levels of SE as a result of weight loss; however, males showed slightly greater benefits.
The present study provides evidence that supports the findings of previous research by indicating that there is a strong negative link between BMI and SE for both males and females. However, the impact was slightly more pronounced in men, indicating the need to tailor interventions aimed at enhancing SE to the specific gender of the target audience. One limitation of the current study is its cross-sectional design and relatively small sample size, which could potentially limit the study’s generalizability. Also, self-reported online surveys might be a potential source of bias. In addition to the cultural and religious nature of society, Saudi Arabia could play a confounding role in the relationship between the studied variables. When conducting research in the future, it will be important to continue investigating these gender disparities and to take into account additional characteristics, such as socioeconomic position, psychiatric comorbidities, and cultural and social factors that have the potential to alter the association between BMI and SE. For people with a higher BMI, it is possible to establish more successful ways to improve their SE and general well-being if they have better knowledge of these complicated relationships. The study’s findings are critical for understanding the participants’ general health and psychological well-being, and they can help inspire future statistical studies to investigate potential relationships and impacts between BMI, SE, and other variables in future studies. Variations in SE across BMI categories for males point to potential connections between physical health and SE, warranting further study. These findings emphasize the multifaceted nature of SE and the significant influence of socio-economic, educational, occupational, and health-related factors. The intricate interplay between socio-economic factors, cultural norms, and personal coping strategies underscores the need for targeted interventions that address these fundamental dynamics, promoting healthier lifestyle choices and enhancing SE through constructive and non-harmful methods.
Conclusion
While the impact was marginally stronger in men, the results showed that there was a statistically significant negative relationship between BMI and SE for both sexes. This indicates that both men and women experience a decline in SE when their BMI rises, with men feeling the effects to a somewhat greater extent. A man’s BMI increases with marriage or a specific marital status, while a lower BMI is associated with more education. Higher education levels and specific vocations are associated with a lower BMI in women. Neither gender showed a statistically significant relationship between smoking and BMI. Marriage lowered SE in men, but had no effect on women. Higher levels of education positively correlated with SE for both genders, with men experiencing a more pronounced effect. Some jobs reduced SE for both genders, but women felt the impact more acutely. Although the effect was larger in women, smoking had a favorable impact on SE in both genders.
Implications
• To successfully treat SE concerns connected to body weight, therapies that target specific genders may be required, as the negative influence of BMI on SE is more noticeable in men. When it comes to enhancing SE, it may be more useful for men to focus on decreasing BMI than for women.
• Given the positive association between higher levels of education and SE in both sexes, it is plausible that educational initiatives aimed at enhancing SE could be widely applicable. Nevertheless, given the more pronounced effect in men, this finding suggests that educational programs may work wonders in raising SE in this demographic.
• Particularly in women, the favorable link between smoking and SE emphasizes the need for focused anti-smoking initiatives addressing the alleged SE benefits of smoking. The development of more successful quitting programs depends on an awareness of the fundamental causes of smoking-related increased SE.
• Occupational health programs should include mental health and SE elements, as some jobs negatively affect SE and help reduce these impacts. Given the greater detrimental impact on women, tailoring these programs to meet their unique needs could be particularly beneficial.
• Given that men’s marital status has a negative effect on SE, it is possible that married men who are experiencing problems with their SE might benefit from marital therapy or support groups. Alternative support systems are necessary, as marital status has minimal impact on SE in females.
• Future studies should investigate these gender disparities further and consider additional factors, such as socioeconomic position and mental comorbidities, as potential factors that could impact the association between BMI and SE. Those persons who have a higher BMI can benefit from greater knowledge of these intricate relationships, which will help in the development of more effective measures to improve their SE and general well-being.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Local Research Ethics Committee (University of Tabuk). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
MA: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
I wish to express my gratitude to each and every person that supports the study in the Community and Psychiatric Health Nursing Department at the Faculty of Nursing, University of Tabuk, Tabuk, Saudi Arabia.
Conflict of interest
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Chooi, YC, Ding, C, and Magkos, F. The epidemiology of obesity. Metabolism. (2019) 92:6–10. doi: 10.1016/j.metabol.2018.09.005
2. Jaacks, LM, Vandevijvere, S, Pan, A, McGowan, CJ, Wallace, C, Imamura, F, et al. The obesity transition: stages of the global epidemic. Lancet Diabet Endocrinol. (2019) 7:231–40. doi: 10.1016/S2213-8587(19)30026-9
3. Templin, T, Cravo Oliveira Hashiguchi, T, Thomson, B, Dieleman, J, and Bendavid, E. The overweight and obesity transition from the wealthy to the poor in low-and middle-income countries: a survey of household data from 103 countries. PLoS Med. (2019) 16:e1002968. doi: 10.1371/journal.pmed.1002968
4. Chowdhury, MA, Adnan, MM, and Hassan, MZ. Prevalence and risk factors of overweight and obesity among women of reproductive age in Bangladesh: a pooled analysis of five national cross-sectional surveys. BMJ Open. (2018) 8:e018468. doi: 10.1136/bmjopen-2017-018468
5. Castelnuovo, G, Pietrabissa, G, Manzoni, GM, Corti, S, Ceccarini, M, Borrello, M, et al. Chronic care management of globesity: promoting healthier lifestyles in traditional and mHealth based settings. Front Psychol. (2015) 6:1557. doi: 10.3389/fpsyg.2015.01557
6. Tomiyama, AJ. Stress and obesity. Annu Rev Psychol. (2019) 70:703–18. doi: 10.1146/annurev-psych-010418-102936
7. Tune, JD, Goodwill, AG, and Sassoon, DJ. Cardiovascular consequences of metabolic syndrome. Transl Res. (2017) 183:57–70. doi: 10.1016/j.trsl.2017.01.001
8. Blüher, M. Obesity: global epidemiology and pathogenesis. Nat Rev Endocrinol. (2019) 15:288–98. doi: 10.1038/s41574-019-0176-8
9. Kim, DD, and Basu, A. Estimating the medical care costs of obesity in the United States: systematic review, meta-analysis, and empirical analysis. Value Health. (2016) 5:602–13. doi: 10.1016/j.jval.2016.02.008
10. Cheng, HL, Medlow, S, and Steinbeck, K. The health consequences of obesity in young adulthood. Curr Obes Rep. (2016) 5:30–7. doi: 10.1007/s13679-016-0190-2
11. Puhl, RM, and Heuer, CA. The stigma of obesity: a review and update. Obesity. (2009) 17:941–64. doi: 10.1038/oby.2008.636
12. Moradi, M, Mozaffari, H, and Askari, M. Association between overweight/obesity with depression, anxiety, low self-esteem, and body dissatisfaction in children and adolescents: a systematic review and meta-analysis of observational studies. Crit Rev Food Sci Nutr. (2021) 2:555–70. doi: 10.1080/10408398.2020.1823813
13. Unlu, S, Aykut, M, Borlu, A, and Kaner, G. Are low self-esteem and body image dissatisfaction related with body mass index? Prog Nutr. (2019) 21, (1-S):94–103. doi: 10.23751/pn.v21i1-S.5552
14. Benton, PM, Skouteris, H, and Hayden, M. Does maternal psychopathology increase the risk of pre-schooler obesity? A systematic review. Appetite. (2015) 87:259–82. doi: 10.1016/j.appet.2014.12.227
15. Fathi, F, Choujaa, H, and Abidli, Z. Overweight, obesity and psychological correlates in a Moroccan adolescent sample. Bangladesh J Med Sci. (2024) 23:798–807. doi: 10.3329/bjms.v23i3.75112
16. Murray, M, Dordevic, AL, and Bonham, MP. Systematic review and meta-analysis: the impact of multicomponent weight management interventions on self-esteem in overweight and obese adolescents. J Pediatr Psychol. (2017) 42:379–94. doi: 10.1093/jpepsy/jsw101
17. Farsani, ZK, and Khabazi, M. The psychological consequences of obesity in adolescent girls: a causal-comparative study. J Kermanshah Univ Med Sci. (2020) 2:e102339. doi: 10.5812/jkums.102339
18. Yates, A, Edman, J, and Aruguete, M. Ethnic differences in BMI and body/self-dissatisfaction among whites, Asian subgroups, Pacific islanders, and African-Americans. J Adolesc Health. (2004) 34:300–7. doi: 10.1016/S1054-139X(03)00305-7
19. Kaminsky, LA, and Dewey, D. The association between body mass index and physical activity, and body image, self esteem and social support in adolescents with type 1 diabetes. Can J Diabetes. (2014) 38:244–9. doi: 10.1016/j.jcjd.2014.04.005
20. Youssef, M, Shariff, S, and Albalawi, R. Impact of obesity on self-esteem and academic performance among medical students in Al-Rayan colleges, Al-Madinah. Dubai Med J. (2023) 6:188–94. doi: 10.1159/000531086
21. Mir Hadi, M, Sadrzadeh Yeganeh, H, and Jazayeri, SA. Relationship between self-esteem and obesity, and some lifestyle factors in employed women. Koomesh. (2024) 2:172–80.
22. Alghawrien, DA, Al-Hussami, M, and Ayaad, O. The impact of obesity on self-esteem and academic achievement among university students. Int J Adolesc Med Health. (2022) 34:20190137. doi: 10.1515/ijamh-2019-0137
23. Al Ahmari, T, Alomar, AZ, and Al Beeybe, J. Associations of self-esteem with body mass index and body image among Saudi college-age females. Eat Weight Disord Stud Anorexia Bulimia. (2019) 24:1199–207. doi: 10.1007/s40519-017-0471-0
24. Byth, S, Frijters, P, and Beatton, T. The relationship between obesity and self-esteem: longitudinal evidence from Australian adults. Oxford open. Economics. (2022) 1:odac009. doi: 10.1093/ooec/odac009
25. Abdi, S, Ahmadian, H, and Saed, L. Investigating the effect of life style change-based training on the improvement in self-esteem and decrease BMI among obese women. Rooyesh Ravanshenasi J. (2019) 11:1–6.
26. Agah Heris, M, Alipour, A, and Janbozorgi, M. A comparative study of effectiveness on life-style modification and cognitive group therapy to weight management and quality of life enhancement. Health Psychol. (2012) 1:68–80.
27. Claes, L, Hart, TA, and Smits, D. Validation of the social appearance anxiety scale in female eating disorder patients. Eur Eat Disord Rev. (2012) 20:406–9. doi: 10.1002/erv.1147
28. Kantanista, A, Król-Zielińska, M, and Borowiec, J. Is underweight associated with more positive body image? Results of a cross-sectional study in adolescent girls and boys. Span J Psychol. (2017) 20:E8. doi: 10.1017/sjp.2017.4
29. Seifrabiei, MA, Ahmadpanah, M, Kazemzadeh, M, and Ebrahimi, S. Effects of educational program based on self-esteem enhancement on weight status in obese women. Iran J Nurs Midwifery Res. (2024) 29:486–90. doi: 10.4103/ijnmr.ijnmr_160_23
30. Zamani Sani, SH, Fathirezaie, Z, Brand, S, Pühse, U, Holsboer-Trachsler, E, Gerber, M, et al. Physical activity and self-esteem: testing direct and indirect relationships associated with psychological and physical mechanisms. Neuropsychiatr Dis Treat. (2016) 12:2617–25. doi: 10.2147/NDT.S116811
31. Muros, JJ, Cofre-Bolados, C, Arriscado, D, Zurita, F, and Knox, E. Mediterranean diet adherence is associated with lifestyle, physical fitness, and mental wellness among 10-y-olds in Chile. Nutrition. (2017) 35:87–92. doi: 10.1016/j.nut.2016.11.002
32. Pervaiz, H, Tariq, MH, and Lela, U. The relationship between social support and self-esteem with the mediating role of stigmatization among obese individuals. Al-NASR. (2024) 3:159–76. doi: 10.53762/alnasr.03.01.e10
33. Alvani, SR, Hosseini, SM, and Kimura, LW. Relationship between body weight and self-esteem: a study of young men and women in Iran. J Obes Overweig. (2016) 2:16–25. doi: 10.15744/2455-7633.2.202
34. Robert, M, Allès, B, Gisch, UA, Shankland, R, Hercberg, S, Touvier, M, et al. Cross-sectional and longitudinal associations between self-esteem and BMI depends on baseline BMI category in a population-based study. BMC Public Health. (2024) 24:230. doi: 10.1186/s12889-024-17755-z
35. Malik, VS, Willett, WC, and Hu, FB. Global obesity: trends, risk factors and policy implications. Nat Rev Endocrinol. (2013) 9:13–27. doi: 10.1038/nrendo.2012.199
36. Zhao, Y, Zheng, Z, Pan, C, and Zhou, L. Self-esteem and academic engagement among adolescents: a moderated mediation model. Front Psychol. (2921) 12:690828. doi: 10.3389/fpsyg.2021.690828
37. Rosenberg, M. Rosenberg self-esteem scale (RSE). Acceptance and commitment therapy/Measures package. (1965). Available at: https://integrativehealthpartners.org/downloads/ACTmeasures.pdf#page=61
38. Nuttall, FQ. Body mass index: obesity, BMI, and health: a critical review. Nutr Today. (2015) 50:117–28. doi: 10.1097/NT.0000000000000092
39. Liddell, TM, and Kruschke, JK. Analyzing ordinal data with metric models: what could possibly go wrong? J Exp Soc Psychol. (2018) 79:328–48. doi: 10.1016/j.jesp.2018.08.009
40. Kampen, J, and Swyngedouw, M. The ordinal controversy revisited. Qual Quant. (2000) 34:87–102. doi: 10.1023/A:1004785723554
41. Bovaird, JA, and Koziol, NA. Measurement models for ordered-categorical indicators In: RH Hoyle, editor. Handbook of structural equation modeling. New York City: The Guilford press (2012). 495–511.
42. Bürkner, PC, and Vuorre, M. Ordinal regression models in psychology: a tutorial. Adv Methods Pract Psychol Sci. (2019) 2:77–101. doi: 10.1177/2515245918823199
43. Williams, RA, and Quiroz, C. Ordinal Regression Models. Thousand Oaks, CA: SAGE Publications Limited (2020).
44. Nevill, AM, and Lane, AM. Why self-report ‘Likert’ scale data should not be log-transformed. J Sports Sci. (2007) 25:1–2. doi: 10.1080/02640410601111183
45. Sathyanarayana, S, and Mohanasundaram, T. Fit indices in structural equation modeling and confirmatory factor analysis: reporting guidelines. Asian J Econ Bus Account. (2024) 7:561–77. doi: 10.9734/ajeba/2024/v24i71430
46. Trzesniewski, KH, Donnellan, MB, and Robins, RW. Stability of self-esteem across the life span. J Pers Soc Psychol. (2003) 84:205–20. doi: 10.1037/0022-3514.84.1.205
47. Orth, U, Robins, RW, and Widaman, KF. Life-span development of self-esteem and its effects on important life outcomes. J Pers Soc Psychol. (2010) 98:645–58. doi: 10.1037/a0018769
48. Robles, TF, and Kiecolt-Glaser, JK. The physiology of marriage: pathways to health. Physiol Behav. (2003) 79:409–16. doi: 10.1016/S0031-9384(03)00160-4
49. Harrod, MM, and Serpe, RT. Identity, attribution, and self-esteem: when employment status matters. Ident Act. (2021) 6:201–22. doi: 10.1007/978-3-030-76966-6_10
50. Barros, VV, Kozasa, EH, Formagini, TDB, Pereira, LH, and Ronzani, TM. Smokers show lower levels of psychological well-being and mindfulness than non-smokers. PLoS One. (2015) 10:e0135377. doi: 10.1371/journal.pone.0135377
51. Carter, B, and Byrne, G. The role of stress and area-specific self-esteem in adolescent smoking. Aust J Psychol. (2013) 65:180–7. doi: 10.1111/ajpy.12019
52. Khodayari, MT, Abadi, A, Baghestani, AR, Asghari Jafarabadi, M, Mohammad, A, and Nadrian, H. Gender-based differences in associations between attitude and self-esteem with smoking behavior among adolescents: A secondary analysis applying Bayesian nonparametric functional latent variable model. J Pediatr Perspect. (2018) 6:7081–94. doi: 10.22038/ijp.2017.27232.2344
53. Ji, P, Zhang, L, Gao, Z, Ji, Q, Xu, J, Chen, Y, et al. Relationship between self-esteem and quality of life in middle-aged and older patients with chronic diseases: mediating effects of death anxiety. BMC Psychiatry. (2024) 24:7. doi: 10.1186/s12888-023-05459-4
54. Ahadzadeh, AS, Rafik-Galea, S, Alavi, M, and Amini, M. Relationship between body mass index, body image, and fear of negative evaluation: moderating role of self-esteem. Health Psychol Open. (2018) 5:2055102918774251. doi: 10.1177/2055102918774251
55. Skorek, M, Song, AV, and Dunham, Y. Self-esteem as a mediator between personality traits and body esteem: path analyses across gender and race/ethnicity. PLoS One. (2014) 9:e112086. doi: 10.1371/journal.pone.0112086
56. Satwik, R, Sinha, D, and Tiwari, B. Prevalence of poor body image and its correlation with self-esteem and depression in middle-aged women. Climacteric. (2024) 27:202–9. doi: 10.1080/13697137.2023.2297876
57. Ghamri, RA, Sadi, RK, and Eissa, GA. Body image perception and self-esteem among pregnant women in Saudi Arabia: a cross-sectional study. Clin Exp Obstet Gynecol. (2024) 51:125. doi: 10.31083/j.ceog5105125
58. Shahzadi, A, and Rasheed, A. The role of body image, body mass index, body shape dissatisfaction and gender on self-esteem among obese young boys and girls. J Psikol Int. (2024) 1:20–31. doi: 10.14421/jpsi.v11i1.3000
Keywords: body mass index, self-esteem, obesity, sociodemographic variables, gender-specific pathway
Citation: Algamdi M (2025) Exploring body mass index and gender-based self-esteem differences in Saudi Arabia. Front. Public Health. 12:1495973. doi: 10.3389/fpubh.2024.1495973
Edited by:
Charalampia Amerikanou, Harokopio University, GreeceReviewed by:
Stamatia Angeliki Kleftaki, Harokopio University, GreeceEfstratios Christodoulou, University of the Aegean, Greece
Copyright © 2025 Algamdi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maaidah Algamdi, aWFsZ2hhbWRpQHV0LmVkdS5zYQ==