 Mi Jung Rho
Mi Jung Rho Yong Hyun Park2*
Yong Hyun Park2* Jihwan Park
Jihwan Park
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 10 January 2025
Sec. Environmental Health and Exposome
Volume 12 - 2024 | https://doi.org/10.3389/fpubh.2024.1490458
This article is part of the Research TopicClimate Change, Air Pollution, and Health Inequality: Vulnerability of Marginalized PopulationsView all 9 articles
Introduction: Fine dust exposure has been reported to affect patients with prostate cancer, making it crucial to understand how environmental pollutants impact health. This study aimed to determine the risk of prostate cancer in South Korea associated with moderate levels of fine dust (PM10) exposure.
Methods: We analyzed data from 20,430 individuals in the National Health Insurance Sharing Service database from 2010 to 2020, comparing a new prostate cancer group (n = 4,071, 19.9%) with a non-prostate cancer group (n = 16,359, 80.1%). Using PM10 data from Air Korea's annual average air quality database, we conducted logistic regression analysis to assess the risk of prostate cancer.
Results: Our findings indicate that even moderate PM10 exposure is a risk factor for developing prostate cancer. Additionally, even at low levels of PM2.5, moderate PM10 exposure significantly impacts prostate cancer development, with lifestyle ha bits potentially lowering this risk.
Discussion: These results underscore the need for stricter environmental standards for PM10 and proactive policies to reduce public health and long-term social costs. Public awareness, including mask use and air quality management, is essential.
Environmental pollutants, particularly particulate matter (PM) air pollution, have been increasingly recognized for their significant impact on human health. Numerous studies have established a strong correlation between environmental pollution and various types of cancer, including lung, heart, brain, and respiratory diseases (1). Among these pollutants, fine dust, specifically PM10, has been implicated in a range of diseases such as chronic obstructive pulmonary disease (COPD), asthma, and lung cancer (2–6). Fine dust penetrates deep into the lungs, causing inflammation and increasing the risk of lung cancer. Additionally, emerging research suggests that fine dust exposure may also contribute to the development of urological cancers, including kidney cancer, urothelial cell carcinoma, and prostate cancer (PCa) (7, 8). Some study have also found that renal function and chronic urologic diseases are associated with PM10 (9, 10). There are also paper on the relationship between industrial pollution, including PM10, and the risk of PCa (11). However, research on PCa and PM10 is still needed, and diverse well-designed studies on PCa are needed. In addition, in Korea, there is a public DB on air quality (the Air Korea's annual average air quality database), so research using it is possible.
While various environmental standards for fine dust exist globally, these standards vary by country, reflecting local conditions. In Korea, the environmental standards for fine dust have adopted the second stage of the World Health Organization's (WHO) 2005 interim targets for air quality (12). According to the 2021 WHO recommendation, the PM10 standard levels is 15 μg/m2 for the annual average and 45 μg/m2 for the 24-h average (12). However, in Korea, the PM10 standard levels is 50 μg/m2 for the annual average and 100 μg/m2 for the 24-h average (13). Despite efforts to reduce fine dust levels through various policies, Korea's standard levels concentration remains high compared to that in developed countries.
PCa is a significant health concern, particularly in Korea, where it ranks third among cancers in men and sixth in overall cancer incidence as of 2021 (14). In Western countries such as Europe and the United States, it has been the number one cancer in men for a long time (15). PCa is rapidly increasing along with the increase in the aging population. Its importance is increasing in Korea, which is entering a super-aging society. PCa is a cancer with a good prognosis when detected early, with a high survival rate of more than 5 years. However, the social costs caused by PCa remain enormous.
Given the rising incidence of PCa and the ongoing concerns about environmental pollution, it is crucial to understand the potential role of fine dust exposure in the development of this cancer. Therefore, this study aimed to investigate the risk of PCa due to moderate level fine dust (31–80 μg/m2) concentration in Korea (13).
Previous research has established that PM10 is associated with various diseases, including respiratory illnesses, lung cancer, heart disease, brain disorders, chronic obstructive pulmonary disease, asthma, COPD exacerbation, esophageal cancer, and corpus uteri cancer (6, 16). Particulrly, PM10 is a risk factor for the development of urological cancers, including kidney cancer, PCa, and urothelial cell carcinoma (7, 17). This study hypothesized that even moderate exposure to PM10 could influence the risk of developing PCa. The specific hypothesis was as follows.
H1: Moderate level PM10 exposure has relationship with PCa.
We used customized health information data from the National Health Insurance Sharing Service (NHISS). In Korea, the NHISS discloses “customized health information data” to researchers (18). Customized health information refers to data provided by processing citizens' health information collected, held, and managed by the NHISS into customized data that can be used for policy and academic research purposes. The NHISS provides researchers with a sample cohort database (DB), health examination cohort DB and older adult cohort DB. The entire data period provided by the NHISS was from 2002 to 2020 (as of 2023, when this study was first conducted). This study used data from 2010 to 2020.
Participants were selected from the NHISS database, including individuals who underwent a baseline health examination in 2013 (n = 3,480,795). Exclusions were made as follows: participants diagnosed with cancer before the baseline examination (N = 232,019), those diagnosed with cancer in the 1st year (n = 66,322), participants with missing health examination data between 2015 and 2020 (n = 1,816,822), and those with no data on air pollution between 2010 and 2013 (n = 674,728). The final cohort consisted of 690,904 participants, with 5,935 cases (0.9%) in the PCa group and 684,969 (99.1%) in the non-PCa group. Propensity score matching (PSM) was applied to minimize selection bias, resulting in 29,674 matched participants. After excluding cases with missing data on weekly walking and drinking habits, 20,430 participants were included in the final analysis, divided into PCa (n = 4,071, 19.9%) and non-PCa groups (n = 16,359, 80.1%; Figure 1).
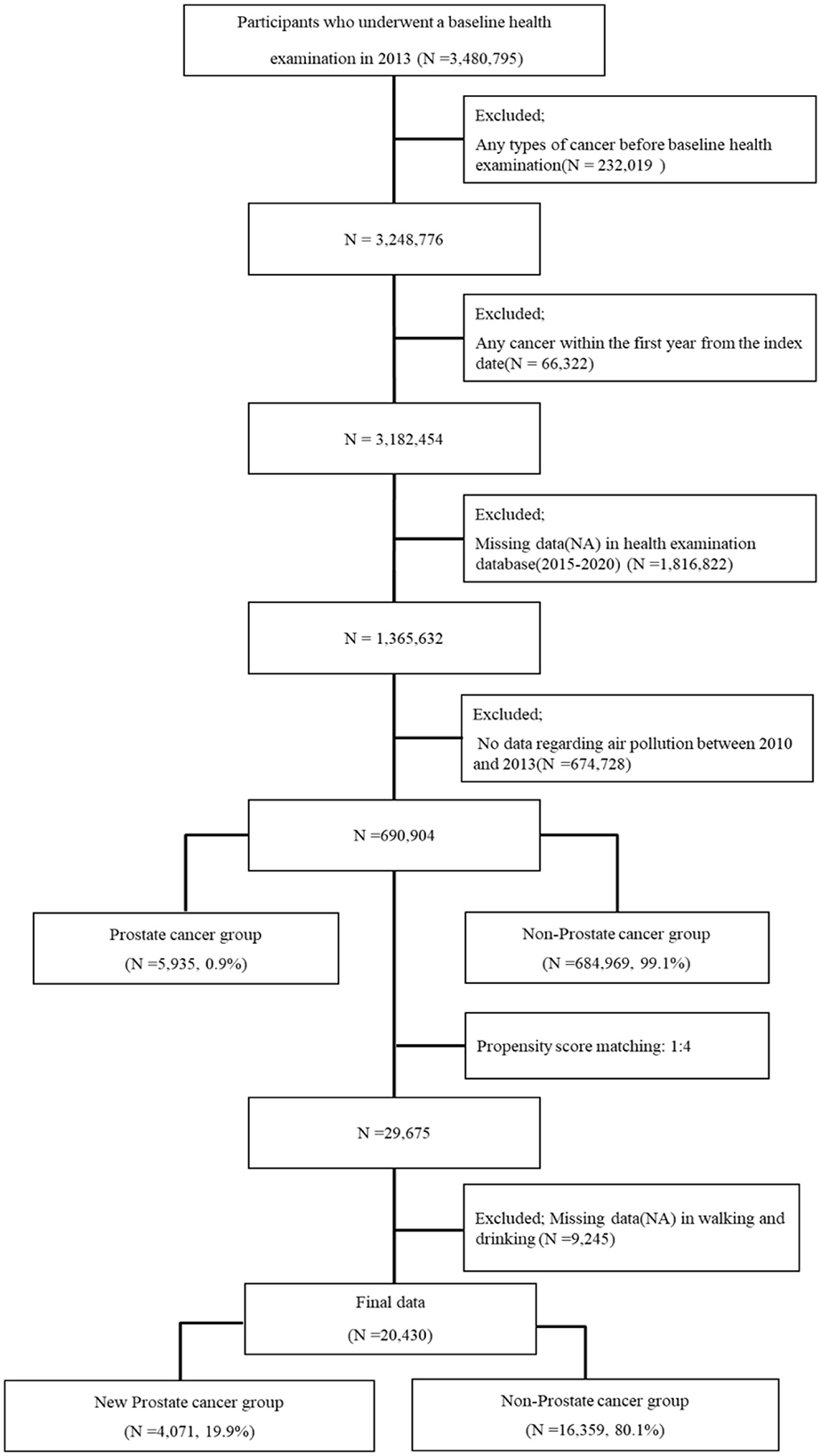
Figure 1. Flowchart of participant inclusion.
The period of PM10 exposure covered 3 years, from 2010 to 2012 (Figure 2). A 1-year washout period followed. The follow-up period for the target data spanned 6 years, from 2015 to 2020.
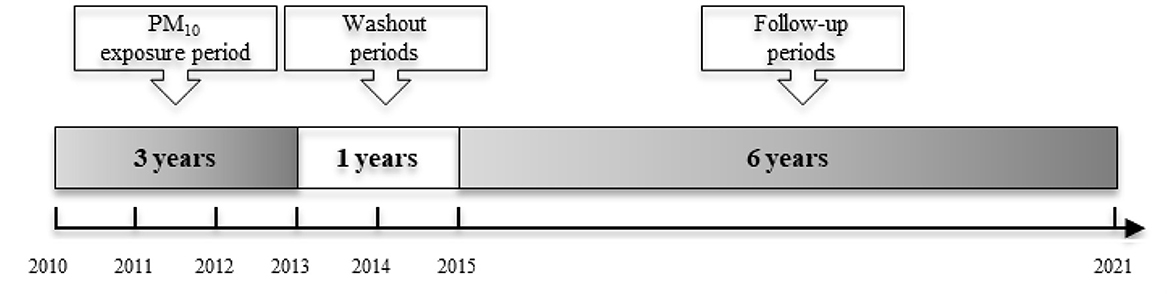
Figure 2. Participants' timeline.
PCa was classified under ICD-10 code C61. In this study, PCa cases were identified based on this classification, with a total of 4,071 patients diagnosed with PCa.
PM10 exposure data were obtained from the Air Korea's annual average air quality database, which monitors air quality across various administrative districts in Korea. The Air Korea's annual average air quality database is categorized by area code. It was used by matching the area code of the subject in the NHISS database. PM10 refers to particulate matter with a diameter of 10 μm or less (19). In Korea, fine dust forecast grades are divided into four levels: good (0–30 μg/m3), moderate (31–80 μg/m3), bad (81–150 μg/m3), and very bad (over 151 μg/m3) (13).
Eight covariates were assessed: weekly walking frequency, alcohol consumption, smoking status, hypertension, diabetes mellitus, hyperlipidemia, body mass index (BMI), and PM2.5 exposure. These variables were categorized as follows: Walking per week: (1) no walking, (2) 1–2 times per week, (3) 3–4 times per week, and (4) 5–7 times per week. Drinking: (1) no drinking, (2) ~2–3 times a month, (3) ~1–2 times a week, (4) 3–4 times a week, and (5) almost daily. Smoking status: (1) non-smokers, (2) ex-smokers, and (3) smokers. Hypertension was classified into three types based on systolic blood pressure and diastolic blood pressure values: (1) normal group [systolic blood pressure (sbp): <120 and diastolic blood pressure (dbp): <80], (2) normal border group (sbp: 120–139 or dbp: 80–89), and (3) group suspected of hypertension (sbp: ≥140 or dbp: ≥90) (20). Diabetes mellitus was divided into three types based on fasting blood sugar: (1) normal (<100 mg/dL), (2) prediabetes (100–125 mg/dL), and (3) diabetes (≥126 mg/dL) (21). Hyperlipidemia was divided into three types based on total cholesterol: (1) low (under 200), (2) middle (200–239), and (3) high (≥240) (22). BMI was divided into three types: (1) normal weights (18.5–24.9), (2) normal weight-border (<18.5 or 25–29.9), and (3) obesity (BMI of 30 or greater) (23). PM2.5 exposure was classified into two groups based on 25 μg/m3: (1) low exposure group (Under 25 μg/m3) and (2) high exposure group (Under 25 μg/m3). The average value of PM2.5 was 25.48 μg/m3 and the median value was 24.79 μg/m3. Therefore, the groups were divided based on the value of 25 μg/m3.
Statistical analysis was conducted using R software for data preprocessing and Propensity Score Matching (PSM), and SPSS for basic statistical analysis, chi-square tests, and multivariate logistic regression. The chi-square test was used to compare demographic characteristics by PM10 exposure levels, and logistic regression analysis was used to assess the risk of PCa associated with PM10 exposure. All statistical tests were two-tailed, and the significance level was set at P-values < 0.05. The analyses were performed using R version 4.0.4 (2020-10-10) and IBM Statistical Package for the Social Sciences (SPSS) Statistics (version 25.0; SPSS Inc.).
The study included 20,430 participants, with 67.4% aged under 65 years and 32.6% over 65 years (Table 1). The average age was 60.76 years, and the median age was 61 years. Regarding physical activity, 22.3% of participants did not engage in any walking, while 32.5% walked more than 5 times per week. Overall, 77.7% of participants walked at least once per week. Additionally, 30.8% of participants consumed alcohol two to three times per month, and 12.4% abstained from drinking entirely. The analysis also revealed that 39.9% of participants were ex-smokers, and 29.1% were non-smokers. Hypertension was suspected in 19.5% of the participants, which aligns with the global variation in hypertension prevalence, reported to be 18% in America and 27% in Africa (20). The majority (51.4%) had a total cholesterol level below 200 mg/dL, and 58.9% had fasting blood sugar levels under 100 mg/dL. A total of 63.4 63.4% of participants were classified within the normal BMI range (18.5 to 24.9). A total of 80.1% belonged to the No PCa group and 19.9% belonged to the PCa group.
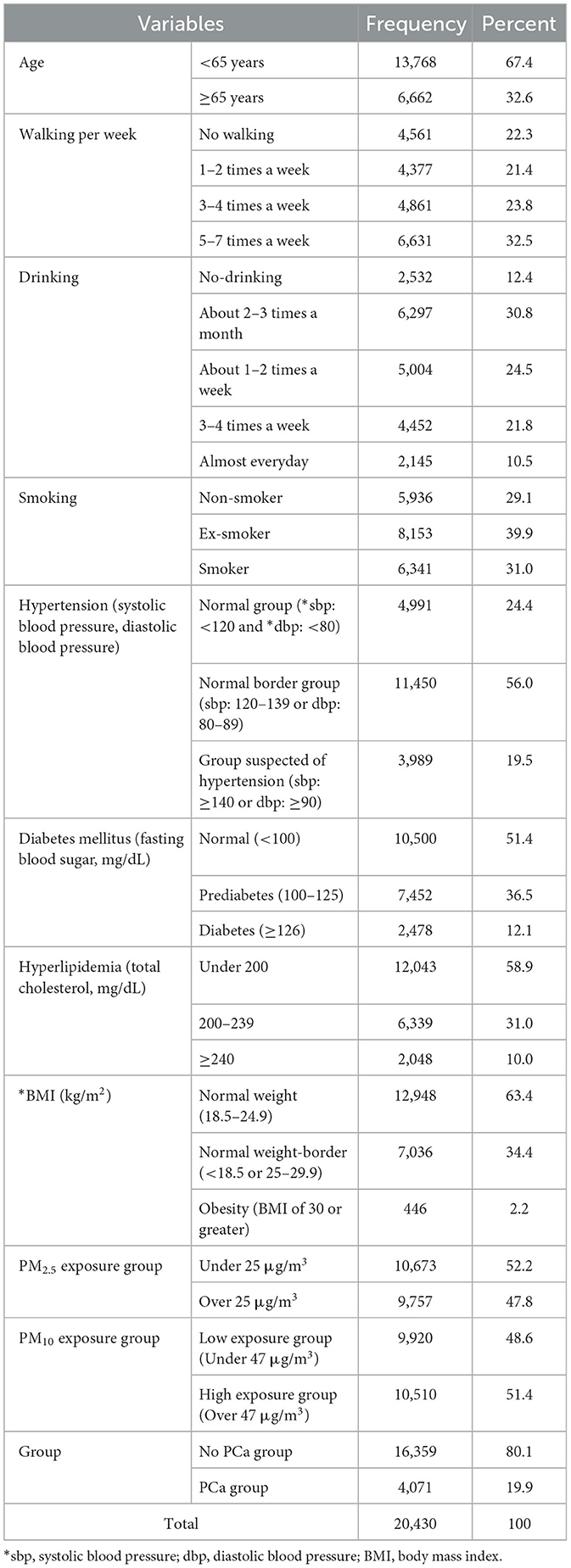
Table 1. Characteristics of the participants.
The average PM10 exposure level was 47.48 μg/m3, with a median of 47.49 μg/m3. Participants were categorized into low and high PM10 exposure groups based on a threshold of 47 μg/m3. The minimum exposure level recorded was 32.44 μg/m3, and the maximum was 62.92 μg/m3. The skewness and kurtosis values were 0.345 and 0.851, respectively, indicating a relatively normal distribution. According to Korea's air quality classification, these values correspond to an “average” level of PM10 exposure (31–80 μg/m3) (Figure 3).
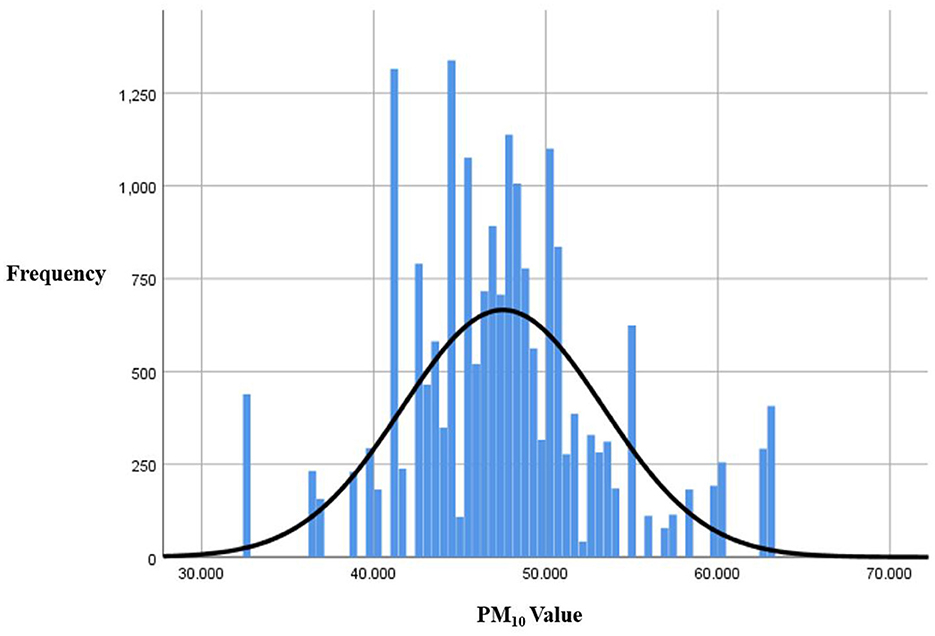
Figure 3. Particulate matter distribution (PM10).
Table 2 shows the demographics according to PM10 exposure. The PCa and non-PCa groups were divided into two groups according to PM10 exposure. In the non-PCa group, significant differences were observed in weekly walking (P = 0.002), drinking (P < 0.001), smoking (P = 0.009), BMI (P = 0.034), and PM2.5 exposure (P < 0.001). In the PCa group, there were significant differences in walking per week (P = 0.002) and PM2.5 exposure (P < 0.001) between low PM10 exposure and high PM10 exposure.
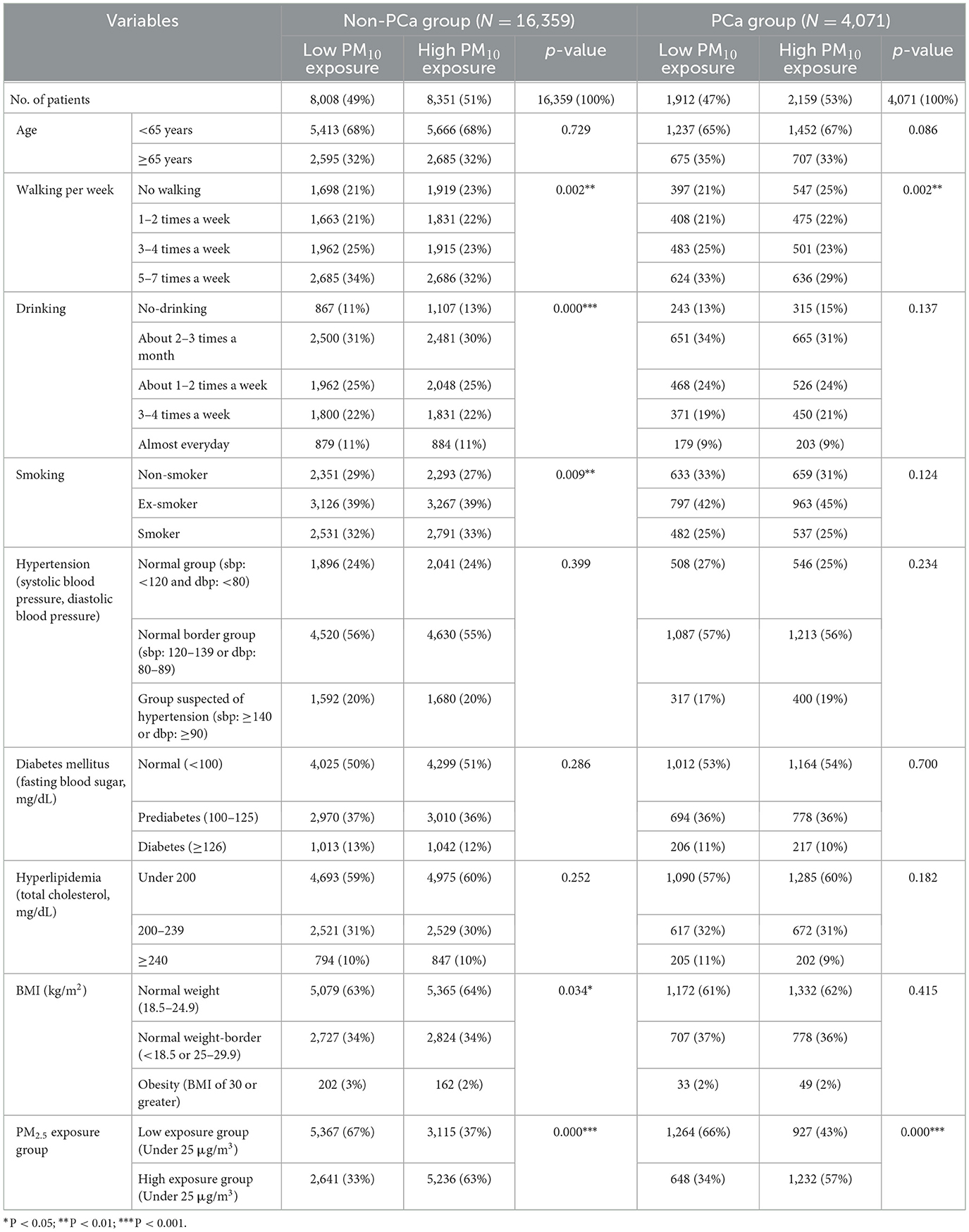
Table 2. Demographics according to the PM10 exposure.
Table 3 presents the odds ratios (95% CI) for PCa according to moderate PM10 exposure, categorized into low (9,920 participants) and high (10,510 participants) exposure groups. Moderate PM10 exposure was identified as a significant predictor of PCa in all models: Model 1 (OR = 1.118), Model 2 (OR = 1.119), and Model 3 (OR = 1.121). These models were adjusted for various factors, including age, PM2.5, drinking habits, walking frequency, smoking status, hypertension, diabetes, hyperlipidemia, and BMI.
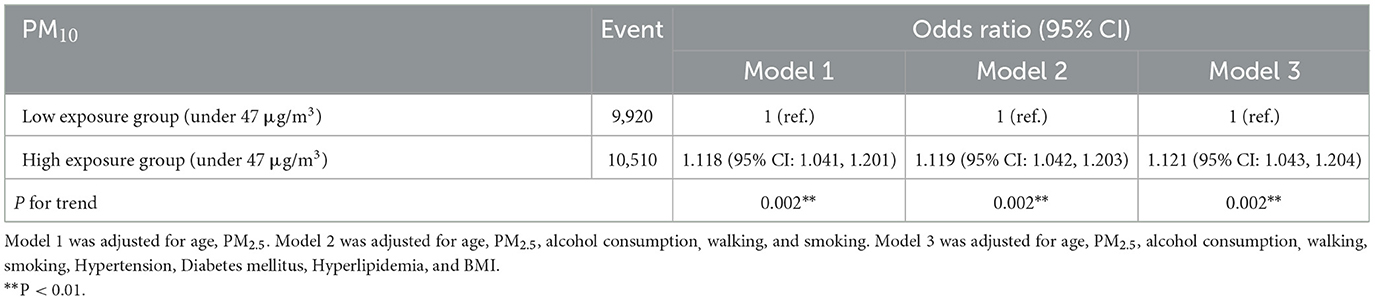
Table 3. Odds ratio of PCa according to the moderate PM10 exposure.
The subgroup results according to moderate exposure to PM10 are as follows: Not all the sub-variables were vulnerable to moderate PM10 exposure (Table 4). However, some subgroups were found to be vulnerable to even moderate exposure to PM10: under 65 years group (OR =1.121), under 25 μg/m3 group (OR = 1.264), no walking group (OR = 1.219), ex-smoker group (OR = 1.156), group suspected of hypertension (OR = 1.196), under 200 of hyperlipidemia (OR = 1.112), obesity group (BMI of 30 or greater) (OR = 1.851), and drinking group 3–4 times a week (OR = 1.192).
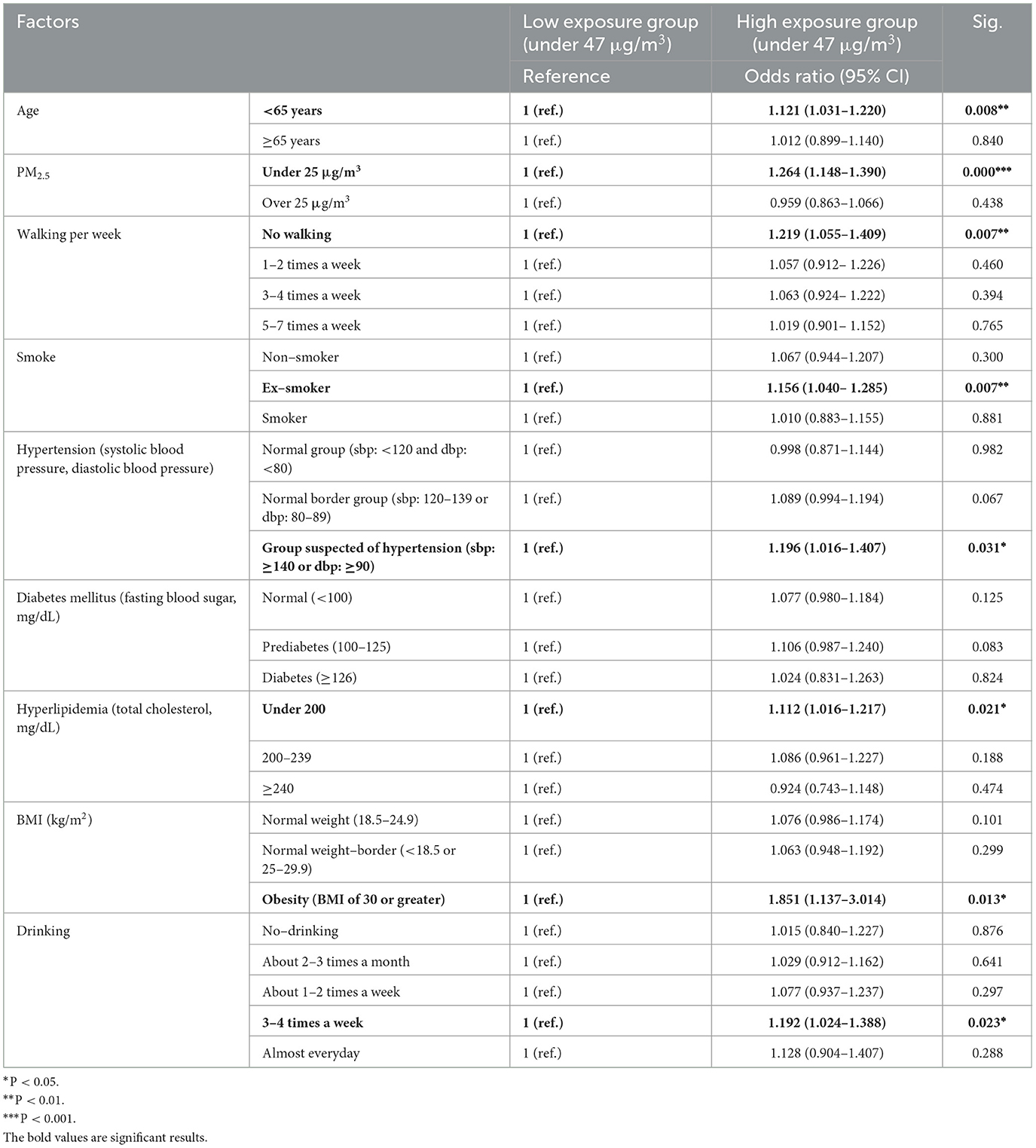
Table 4. Odds ratio of PCa in relevant subgroups.
This study aimed to determine the risks associated with moderate levels of PM10 exposure for the development of PCa, based on the fine dust standards of the Korean Ministry of Environment (13). The findings reveal several important insights.
First, we observed that even moderate levels (31–80 μg/m3, Korea standard) (13) of PM10 exposure are significant risk factors for the development of PCa. According to the Korean air-quality classifications, a PM10 level of 47 μg/m3 is considered moderate level, a level at which masks are typically not worn by the public (13). However, our findings suggest that even at these moderate levels, PM10 exposure can influence the development of urological cancers such as PCa. This aligns with previous studies that have highlighted detrimental effects of PM10 on cancer risk (7, 24). There is little research on moderate level PM10, so in-depth discussion on it is limited. However, it is very meaningful that disease risks were predicted even for moderate level fine dust, even based on Korean standards.
In Korea, days with poor air quality have increased since 2012 due to an increase in PM, and various measures have been sought along with public concerns (9). Since 2015, air quality alerts have increased nationwide (25). Nevertheless, as described in the introduction, Korea PM10 standards are less stringent than those in other countries. The PM10 standard levels of 2021 WHO recommendation is 15 μg/m3 for the annual average and 45 μg/m3 for the 24-h average (12). The PM10 standard levels is 50 μg/m3 for the annual average and 100 μg/m3 for the 24-h average in Korea (13). This study emphasizes that Korea should further strengthen air quality standards for PM10.
In addition, it is critical to implement more detailed guidelines and actively promote the use of masks and air purification strategies when air quality deteriorates to hazardous levels. Prior research has demonstrated that education about the health risks associated with fine dust can influence public perceptions of susceptibility and severity (26). Our findings support the need for robust awareness campaigns to mitigate these risks.
Second, the study highlights the importance of individual physical characteristics in the relationship between PM10 exposure and PCa development. We found that the risk of PCa due PM10 exposure is higher in patients under 65 years of age, in those with suspected hypertension, in individuals with total cholesterol levels below 200 mg/dL, and in obese individuals. These findings contribute to the ongoing debate on the association between obesity, air pollution, and cancer risk (27). Previous research continues to explore the relationship between local environment factors and cancer incidence (28). Many studies have suggested that air pollution may negatively contribute to body weight status in adults (29–33), our results also indicate that in obesity, PM10 exposure is a significant risk factor for PCa. Thus, identifying high-risk groups based on major factors such as underlying health conditions is crucial, and targeted mid- to long-term support for these groups should be prioritized.
Third, lifestyle habits also play a crucial role in the relationship between PM10 exposure and PCa. Our study found that the risk of developing PCa due to PM10 exposure is elevated in individuals who do not engage in regular exercise, in ex-smokers, and in those who consume alcohol three to four times a week. These results are consistent with previous research indicating that lifestyle management can help mitigate the incidence of cancer related to air pollution (7, 28, 34, 35). In order to reduce the social cost of cancer, a comprehensive solution approach is needed that addresses environmental issues such as air pollution and actively corrects people's lifestyle habits.
Finally, we observed that the risk of developing PCa due to PM10 exposure was higher even in the presence of low PM2.5. This result was very interesting because even when PM2.5 is low, increased PM10 exposure increases the risk of developing PCa. Both PM10 and PM2.5 are air quality measurements, and although they are very important air quality measurement factors and global challenge issues (36–40), they should be viewed separately. Depending on the disease, PM2.5 and PM10 exposure often affect the disease at the same time (40). In fact, there are days when PM2.5 levels are low but PM10 levels are high. Although it is important to understand the impact of the integrated air quality index or multiple pollutants together in some cases (41), the fact that PM10 alone still increases the risk of disease is very significant.
Despite these significant findings, our study has several limitations. First, air pollution encompasses a range of pollutants, including PM10, NO2, and PM2.5 (42), and the incidence of various cancers has been consistently linked to PM2.5 exposure (43, 44). However, our study focused mainly on the relationship between PM10 exposure and PCa. Future research should consider a broader range of air pollutants to provide a more comprehensive understanding of their combined effects. Second, the study limited the period of PM10 exposure to 3 years (2010–2012). We used PM10 exposure data from Air Korea's annual average air quality database. The Air Korea's annual average air quality database has been providing air quality data since 2009, we identified appropriate data for the study and used air quality data from 2010 to 2012, which provided the longest follow-up period. Therefore, we used only 3 years of data to select data with as many area codes as possible that can be matched with NHISS customized health information data and with PM10 values that can be used in research. Additional research with longer exposure periods is needed to fully assess the long-term risks associated with fine dust exposure. Third, this study considered some lifestyle factors such as alcohol consumption, smoking, and physical activity. However, there may be other lifestyle factors, such as diet and occupational exposure, which could also influence the risk of prostate cancer. However, the customized health information data from NHISS does not provide additional lifestyle data (such as diet and occupational exposure), so it could not be utilized. Future research is needed to derive risk factors by including various lifestyles. Fourth, this study is based on Korea's environmental standards (13), and since environmental standards may differ from country to country, there may be limitations in the global applicability of the research results. Future research needs to be conducted based on global standards. Fifth, there is research that shows a relationship between air pollution and temperature (45). If we can secure data on temperature in the future, it would be desirable to analyze various environmental factors such as temperature in addition to air quality.
Despite these limitations, this study provides important insights into the relationship between moderate PM10 exposure and increased PCa risk. The findings also underscore the need for more stringent and detailed environmental standards for PM10. Reducing the disease risk from fine dust requires a mid- to long-term, comprehensive solution approach to identify high-risk groups and reduce social costs. In addition, public health should emphasize the importance of wearing masks and managing air quality, and managing lifestyle habits to protect the negative health effects of fine dust exposure.
The national health insurance sharing service requires approval of institutional review board. Requests to access these datasets should be directed to NHISS bigdata service, MDA3NTAzMEBuaGlzLm9yLmtyLg==
We used the public data set from the National Health Insurance System that is not individually identifiable after approval by the Institutional Review Board of Dankook University (DKU2022-06-002).
MJR: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Validation, Visualization, Writing – original draft, Writing – review & editing. YP: Conceptualization, Data curation, Investigation, Validation, Writing – original draft, Writing – review & editing. JP: Conceptualization, Data curation, Funding acquisition, Investigation, Project administration, Supervision, Validation, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea Government (MSIT; No. NRF-2022R1G1A1011635).
This study was performed using the database from the National Health Insurance System (NHIS-2023-1-160) and the results do not necessarily represent the opinion of the National Health Insurance Corporation.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Huang Y, Zhu M, Ji M, Fan J, Xie J, Wei X, et al. Air pollution, genetic factors, and the risk of lung cancer: a prospective study in the UK Biobank. Am J Respir Crit Care Med. (2021) 204:817–25. doi: 10.1164/rccm.202011-4063OC
2. Badyda A, Gayer A, Czechowski PO, Majewski G, Dabrowiecki P. Pulmonary function and incidence of selected respiratory diseases depending on the exposure to ambient PM10. Int J Mol Sci. (2016) 17:1954. doi: 10.3390/ijms17111954
3. Misiukiewicz-Stepien P, Paplinska-Goryca M. Biological effect of PM10 on airway epithelium-focus on obstructive lung diseases. Clin Immunol. (2021) 227:108754. doi: 10.1016/j.clim.2021.108754
4. Tahery N, Geravandi S, Goudarzi G, Shahriyari HA, Jalali S, Mohammadi MJ. Estimation of PM10 pollutant and its effect on total mortality (TM), hospitalizations due to cardiovascular diseases (HACD), and respiratory disease (HARD) outcome. Environ Sci Pollut Res. (2021) 28:22123–30. doi: 10.1007/s11356-020-12052-9
5. Zhang Q, Sun S, Sui X, Ding L, Yang M, Li C, et al. Associations between weekly air pollution exposure and congenital heart disease. Sci Tot Environ. (2021) 757:143821. doi: 10.1016/j.scitotenv.2020.143821
6. Ciabattini M, Rizzello E, Lucaroni F, Palombi L, Boffetta P. Systematic review and meta-analysis of recent high-quality studies on exposure to particulate matter and risk of lung cancer. Environ Res. (2021) 196:110440. doi: 10.1016/j.envres.2020.110440
7. Park J, Rho MJ, Park YH. Ambient particulate matter exposure and urologic cancer: a longitudinal nationwide cohort study. Am J Cancer Res. (2023) 13:4755.
8. Winkelstein Jr W, Kantor S. Prostatic cancer: relationship to suspended particulate air pollution. Am J Publ Health Nations Health. (1969) 59:1134–8. doi: 10.2105/AJPH.59.7.1134
9. Kim E-A. Particulate matter (fine particle) and urologic diseases. Int Neurourol J. (2017) 21:155. doi: 10.5213/inj.1734954.477
10. Yang Y-R, Chen Y-M, Chen S-Y, Chan C-C. Associations between long-term particulate matter exposure and adult renal function in the Taipei metropolis. Environ Health Perspect. (2017) 125:602–7. doi: 10.1289/EHP302
11. Ramis R, Diggle P, Cambra K, López-Abente G. Prostate cancer and industrial pollution: risk around putative focus in a multi-source scenario. Environ Int. (2011) 37:577–85. doi: 10.1016/j.envint.2010.12.001
12. WHO. What Are the WHO Air Quality Guidelines? (2021). p. 3–10. Available at: https://www.who.int/news-room/feature-stories/detail/what-are-the-who-air-quality-guidelines (accessed September 22, 2021).
13. Korea A. Comprehensive Air-Quality Index. (2022). Available at: https://www.airkorea.or.kr/eng/khaiInfo?pMENU_NO=166 (accessed June 30, 2024).
15. Siegel RL, Giaquinto AN, Jemal A. Cancer statistics, 2024. CA Cancer J Clin. (2024) 74:12–49. doi: 10.3322/caac.21820
16. Li W, Wang W. Causal effects of exposure to ambient air pollution on cancer risk: insights from genetic evidence. Sci Tot Environ. (2024) 912:168843. doi: 10.1016/j.scitotenv.2023.168843
17. Wang A, Tseng C-c, Rose H, Cheng I, Wu AH, Haiman CA. Ambient air pollution and risk of prostate cancer: the multiethnic cohort study. Cancer Res. (2022) 82(12_Suppl.):1437. doi: 10.1158/1538-7445.AM2022-1437
18. Service NHI. Customized DB: What Is Customized Health Information Data? (2019). Available at: https://nhiss.nhis.or.kr/bd/ab/bdaba032eng.do (accessed March 13, 2019).
19. Environmental Standards. Enforcement Decree of the Framework Act on Environmental Policy [Appendix 1]<Amended May 12, 2020> (related to Article 2). Republic of Korea (2020).
20. WHO. Hypertension. (2023). Available at: https://www.who.int/news-room/fact-sheets/detail/hypertension (accessed May 21, 2023).
21. WHO. Mean Fasting Blood Glucose. (2024). Available at: https://www.who.int/data/gho/indicator-metadata-registry/imr-details/2380 (accessed May 20, 2024).
22. Jeong SM, Choi S, Kim K, Kim SM, Lee G, Park SY, et al. Effect of change in total cholesterol levels on cardiovascular disease among young adults. J Am Heart Assoc. (2018) 7:e008819. doi: 10.1161/JAHA.118.008819
23. Organization WH. Obesity: Preventing and Managing the Global Epidemic: Report of a WHO Consultation. Geneva: Organization WH (2000).
24. Turner MC, Krewski D, Diver WR, Pope III CA, Burnett RT, Jerrett M, et al. Ambient air pollution and cancer mortality in the cancer prevention study II. Environ Health Perspect. (2017) 125:087013. doi: 10.1289/EHP1249
25. Kim D, Han H, Wang W, Kang Y, Lee H, Kim HS. Application of deep learning models and network method for comprehensive air-quality index prediction. Appl Sci. (2022) 12:6699. doi: 10.3390/app12136699
26. Kim J, Kim Y. What predicts Korean citizens' mask-wearing behaviors? health beliefs and protective behaviors against particulate matter. Int J Environ Res Public Health. (2021) 18:2791. doi: 10.3390/ijerph18062791
27. An R, Ji M, Yan H, Guan C. Impact of ambient air pollution on obesity: a systematic review. Int J Obes. (2018) 42:1112–26. doi: 10.1038/s41366-018-0089-y
28. Felici A, Peduzzi G, Giorgolo F, Spinelli A, Calderisi M, Monreale A, et al. The local environment and germline genetic variation predict cancer risk in the UK Biobank prospective cohort. Environ Res. (2024) 241:117562. doi: 10.1016/j.envres.2023.117562
29. Huang S, Zhang X, Huang J, Lu X, Liu F, Gu D. Ambient air pollution and body weight status in adults: a systematic review and meta-analysis. Environ Pollut. (2020) 265:114999. doi: 10.1016/j.envpol.2020.114999
30. Chaparro MP, Benzeval M, Richardson E, Mitchell R. Neighborhood deprivation and biomarkers of health in Britain: the mediating role of the physical environment. BMC Public Health. (2018) 18:1–13. doi: 10.1186/s12889-018-5667-3
31. Eze IC, Schaffner E, Foraster M, Imboden M, von Eckardstein A, Gerbase MW, et al. Long-term exposure to ambient air pollution and metabolic syndrome in adults. PLoS ONE. (2015) 10:e0130337. doi: 10.1371/journal.pone.0130337
32. Li M, Qian Z, Vaughn M, Boutwell B, Ward P, Lu T, et al. Sex-specific difference of the association between ambient air pollution and the prevalence of obesity in Chinese adults from a high pollution range area: 33 communities Chinese health study. Atmos Environ. (2015) 117:227–33. doi: 10.1016/j.atmosenv.2015.07.029
33. Shamy M, Alghamdi M, Khoder MI, Mohorjy AM, Alkhatim AA, Alkhalaf AK, et al. Association between exposure to ambient air particulates and metabolic syndrome components in a Saudi Arabian population. Int J Environ Res Public Health. (2018) 15:27. doi: 10.3390/ijerph15010027
34. Zhu Y, Wu Y, Cheng J, Liang H, Chang Q, Lin F, et al. Ambient air pollution, lifestyle, and genetic predisposition on all-cause and cause-specific mortality: a prospective cohort study. Sci Tot Environ. (2024) 2024:173120. doi: 10.1016/j.scitotenv.2024.173120
35. Tainio M, Andersen ZJ, Nieuwenhuijsen MJ, Hu L, De Nazelle A, An R, et al. Air pollution, physical activity and health: a mapping review of the evidence. Environ Int. (2021) 147:105954. doi: 10.1016/j.envint.2020.105954
36. Lim C-H, Ryu J, Choi Y, Jeon SW, Lee W-K. Understanding global PM2.5 concentrations and their drivers in recent decades (1998–2016). Environ Int. (2020) 144:106011. doi: 10.1016/j.envint.2020.106011
37. Wathanavasin W, Banjongjit A, Phannajit J, Eiam-Ong S, Susantitaphong P. Association of fine particulate matter (PM2.5) exposure and chronic kidney disease outcomes: a systematic review and meta-analysis. Sci Rep. (2024) 14:1048. doi: 10.1038/s41598-024-51554-1
38. Yue H, He C, Huang Q, Zhang D, Shi P, Moallemi EA, et al. Substantially reducing global PM2.5-related deaths under SDG3 9 requires better air pollution control and healthcare. Nat Commun. (2024) 15:2729. doi: 10.1038/s41467-024-46969-3
39. Li B, Ma Y, Zhou Y, Chai E. Research progress of different components of PM2.5 and ischemic stroke. Sci Rep. (2023) 13:15965. doi: 10.1038/s41598-023-43119-5
40. Azizi S, Hadi Dehghani M, Nabizadeh R. Ambient air fine particulate matter (PM10 and PM2.5) and risk of type 2 diabetes mellitus and mechanisms of effects: a global systematic review and meta-analysis. Int J Environ Health Res. (2024) 2024:1–20. doi: 10.1080/09603123.2024.2391993
41. Mentese S, Mirici NA, Elbir T, Tuygun GT, Bakar C, Otkun MT, et al. A comprehensive assessment of ambient air quality in Çanakkale city: emission inventory, air quality monitoring, source apportionment, and respiratory health indicators. Atmos Pollut Res. (2020) 11:2282–96. doi: 10.1016/j.apr.2020.07.005
42. Su S-Y, Liaw Y-P, Jhuang J-R, Hsu S-Y, Chiang C-J, Yang Y-W, et al. Associations between ambient air pollution and cancer incidence in Taiwan: an ecological study of geographical variations. BMC Public Health. (2019) 19:1–8. doi: 10.1186/s12889-019-7849-z
43. Coleman NC, Burnett RT, Ezzati M, Marshall JD, Robinson AL, Pope III CA. Fine particulate matter exposure and cancer incidence: analysis of SEER cancer registry data from 1992–2016. Environ Health Perspect. (2020) 128:107004. doi: 10.1289/EHP7246
44. Li P, Guo X, Jing J, Hu W, Wei W-Q, Qi X, et al. The lag effect of exposure to PM2.5 on esophageal cancer in urban-rural areas across China. Environ Sci Pollut Res. (2022) 29:4390–400. doi: 10.1007/s11356-021-15942-8
Keywords: particulate matter exposure, prostate cancer, PM10, the National Health Insurance Sharing Service, national cohort study
Citation: Rho MJ, Park YH and Park J (2025) Moderate PM10 exposure increases prostate cancer: a longitudinal nationwide cohort study (2010–2020). Front. Public Health 12:1490458. doi: 10.3389/fpubh.2024.1490458
Received: 03 September 2024; Accepted: 23 December 2024;
Published: 10 January 2025.
Edited by:
Nurzawani Md Sofwan, Universiti Teknologi MARA Sarawak Branch, MalaysiaReviewed by:
Yuzhu Liu, Nanjing University of Information Science and Technology, ChinaCopyright © 2025 Rho, Park and Park. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yong Hyun Park, bGVzdGF0MDRAY2F0aG9saWMuYWMua3I=; Jihwan Park, amlod2FucGFya0BkYW5rb29rLmFjLmty
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.