
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 15 January 2025
Sec. Infectious Diseases: Epidemiology and Prevention
Volume 12 - 2024 | https://doi.org/10.3389/fpubh.2024.1485516
This article is part of the Research Topic The Global Phenotypic Diversity of HIV-1: Implications for Pathogenesis, Vaccine, and Cure View all 5 articles
 Jianxin Pei1†
Jianxin Pei1† Zhonglan Wu1,2†Bingqian Si3Chunhua Ma3Yichang Liu3Xiaofa Ma3Wenhe Kuai1Yinhao Zhang1Yong Li2*
Zhonglan Wu1,2†Bingqian Si3Chunhua Ma3Yichang Liu3Xiaofa Ma3Wenhe Kuai1Yinhao Zhang1Yong Li2*Background: Over the past decade, sexual transmission has become a dominant source of new HIV-1 infection in China. However, very few studies have been conducted to characterize the two sexual transmissions, homosexual and heterosexual transmission. This study was conducted to better understand the relationship between genotypes, drug resistance, and molecular transmission networks in two groups of sexually transmitted HIV-1 in Ningxia, China.
Methods: Plasma samples were collected from sexually transmitted HIV/AIDS patients in Ningxia between 2020 and 2021 for RNA extraction followed by HIV-1 genome sequencing, genotype and drug resistance analyses. The TN93 model in HyPhy2.2.4 with 1.25% as the threshold, was used to calculate the gene distance, and Cytoscape3.7.0 was used to generate a visual molecular transmission network.
Results: A total of 269 samples were successfully sequenced, and 10 HIV-1 subtypes were detected. The two most common subtypes were CRF07_BC and CRF01_AE. All 10 subtypes were detected in heterosexually transmitted patients, and 7 subtypes were found in homosexually transmitted patients who were exclusively men sex with men (MSM). The drug resistance rates of heterosexual individuals and MSMs were 45.34 and 33.33%, respectively. Sequences from 120 patients entered the molecular transmission network, forming 35 clusters. The clustering rate for MSM (52.78%) was higher than that of heterosexual individuals (39.13%). Some MSM and HSTs were involved in the same cluster and might act as bridges for transmission between the two populations.
Conclusion: Our data showed that heterosexually transmitted HIV-1 was more likely to be a drug-resistant virus, whereas MSM was more likely to contract viruses through network connection. It is strongly recommended that resistance testing be conducted before ART to improve effective treatment and reduce the spread of resistant viruses. Molecular networks can help to identify transmission clusters and provide more precise interventions.
Since the first case of AIDS was reported in the United States in 1981, human immunodeficiency virus type 1 (HIV-1) has spread worldwide through blood, mother-to-child vertical transmission, and sexual contact routes, posing a considerable threat to the economic and social development of societies (1). According to UNAIDS statistics, by the end of 2021, approximately 38.4 million people worldwide will be living with HIV, including 1,148,000 people living with HIV in China, and approximately 650,000 people will have died from HIV-related diseases in 2021 (2), making it one of the most important infectious diseases affecting public health. HIV was formerly spread mostly through blood transfusions and intravenous drug use in China; however, in recent years, the prevalence of sexually transmitted infections has greatly increased and has been considered the primary method of HIV transmission (3). The percentage of heterosexual and homosexual transmission in China has increased from 48.3 and 9.1% in 2009 to 74.2 and 23.3% in 2020, respectively (4). Due to unprotected sexual activity, multiple sexual partners, participation in commercial sex, bisexual sex, and other factors (5), men who have sex with men (MSM) have recently been identified as a high-risk population for HIV transmission. A study reported that MSM in China have a 19-fold higher risk of contracting HIV than the general population (6). However, heterosexual activities, such as its large population base, can spread HIV to the broader population, which presents substantial obstacles for HIV/AIDS prevention and treatment (7).
The National Free ART Program (NFATP) has greatly boosted the coverage of HIV/AIDS patients receiving antiviral therapy in China since its implementation in 2003 (8). Early antiretroviral therapy (ART) not only greatly reduces viral load but also leads to a significant reduction in the prevalence of risky sexual behaviors in different populations (9), thus greatly enhancing the effectiveness of HIV transmission prevention (10). However, with the increasing coverage of ART, the prevalence of drug resistance is increasing, which can substantially lessen the benefit of ART and may cause virological failure due to the high variation in the HIV gene and the pressure of drug selection (11). The reported data showed that 39% of patients for whom ART failed carried drug-resistant HIV-1, and the acquired drug resistance prevalence was 44.7% (12). HIV infections that are resistant to one or more antiviral drugs can spread via various routes. However, sexually transmitted individuals usually have poor treatment compliance, which could encourage the emergence and spread of drug resistance (13).
The Ningxia Hui Autonomous Region (Ningxia) is located in northwestern China and has a mixture of Han (64.05%) and Hui (35.04%) populations. The HIV-1 epidemic has been well controlled, but the case fatality rate has not shown a substantial downward trend, suggesting that the treatment of HIV-1 infection needs to be modified (14). It is also noted that the infections of HIV-1 are sexually spreading from high-risk populations to the general population in the region, indicating that the control measures for sexual transmission may not be very optimistic (14). Sexually transmitted HIV usually occurs through networks of closely connected groups. Building a molecular transmission network based on the genetic similarities of gene sequences of HIV-positive individuals is a useful approach to identify the transmission pathway and direct precise action against high-risk sources of infection (15). In this study, we combined drug resistance analysis and molecular transmission network technology to identify risk factors for HIV sexual transmission.
HIV-1/AIDS patients were recruited if they met the following criteria: (1) HIV positive screened by HIV-1/HIV-2 enzyme-linked immunosorbent assay and confirmed by HIV-1 Western blotting in the Ningxia Center for Disease Control and Prevention (CDC); (2) the route of infection was sexual transmission, including MSM and heterosexual transmission; (3) received antiviral therapy for more than 6 months; (4) the viral load was greater than 400 copies/mL; and (5) the individuals voluntarily participated in this study with verbal or written informed consent. Demographic characteristics (ethnicity, sex, age, and marital status) were obtained from the Ningxia Information System for Disease Control and Prevention. After eliminating duplicate samples, pol sequence (covering 1,060 base pairs, HXB2:2253–3,313) information was successfully exported from 269 people living with HIV (PLWH) in this study.
Plasma samples were separated from whole blood and preserved in a freezer at −80°C. RNA was extracted from 200 μL of plasma using an automatic nucleic acid extractor (Zhuhai Lizhu Reagent Co. LTD), which was performed in strict accordance with the manufacturer’s instructions. The HIV-1 pol gene was amplified by nested polymerase chain reaction (nPCR) using an in-house method (16), including the full-length protease gene (codon 1–99) and the first 300 amino acids of the reverse transcriptase gene (codon 1–300). The amplified product was approximately 1.1 kb. The amplified products were subjected to electrophoresis on 1% agarose gel, and the positive products were purified and sequenced by Beijing Nuosai Gene Sequencing Ltd.
Initially, Sequencher 4.9 software was used to edit and assemble the sequences, followed by sequence alignment and arrangement using BioEdit 7.1.3. A phylogenetic tree was constructed using Mega7.0, using neighbor joining (Kimura two-parameter model, bootstrap samples = 1,000), and the HIV-1 subtypes were compared to international reference strains from the HIV gene database (LANL).1 If the sequence in which the genotype could not be confirmed by the phylogenetic tree or HIV BLAST database was considered a unique recombinant form (URF), recombination breakpoint analysis was performed using the SimPlot software.
The obtained nucleic acid sequence was submitted to the Stanford University Drug Resistance Gene Database 2for base-resistance mutation identification and drug sensitivity analysis (17). According to the score in the database system, the degree of drug resistance was divided into five levels: sensitive (S), potential low drug resistance (P), low drug resistance (L), moderate drug resistance (I), and high drug resistance (H). At least one low-to-high resistance mutation indicates drug resistance.
Pairwise gene distance of the sequence was calculated using the TN93 model in HyPhy2.2.4. The total number of transmission clusters in the molecular transmission network was considered to reach a maximum when the gene distance was less than 0.0125 (18). Therefore, gene distance was selected to construct the molecular transmission network, and Cytoscape 3.7.2 software was used to visualize the network. In molecular transmission networks, the number of edges connected to each node is a “degree” value.
The database was constructed using Excel 2010 software, and the differences in transmission routes under different characteristics were statistically analyzed using SPSS 22.0. The count data were described as the number of cases and constituent ratios, and the differences between groups were compared using the chi-square test or Fisher’s exact test. Logistic regression analysis was used to determine the factors affecting the molecular transmission networks. All tests were two-tailed, and a p value <0.05 was considered statistically significant.
A total of 3,524 patients received antiviral treatment between 2020 and 2021 in Ningxai and 332 of them had a viral load greater than 400 copies/mL. The intact pol sequence was successfully obtained from 269 patients that were included in this analysis.
108 patients were homosexual transmitted who were exclusively MSMs, while 161 infected individuals were heterosexual transmitted. The major characteristics of two group patients included (Table 1): (1) Heterosexual transmission occurred mainly among males, accounting for 75.78%; (2) The age range of MSM was 15–63 years, with the mean ± SD of 37.21 ± 10.87 years; and the age range of HSTs was 19–81 years and the mean ± SD of the age was 46.19 ± 15.63 years. The means of age of the two groups were statistically different. (3) The majority of patients in both groups lived in Yinchuan City, the capital city of Ningxia. (4) Of the MSM, 55.56% were unmarried, while only 26.72% of HSTs were unmarried. The difference in marital status in two group was statistically significant. (5) Approximately 80% of patients received first-line treatment, mainly lamivudine+efavirenz+tenofovir disoproxil fumarate (3TC + EFV + TDF) in both groups. (6) There was a trend that MSM had higher CD4+ T-cell counts than HSTs, and the mean CD4+ count in the two groups was statistically different. (7) 87.73% of patients had >10,000 copies/ml of viral load, and there was no statistically different between the two groups.
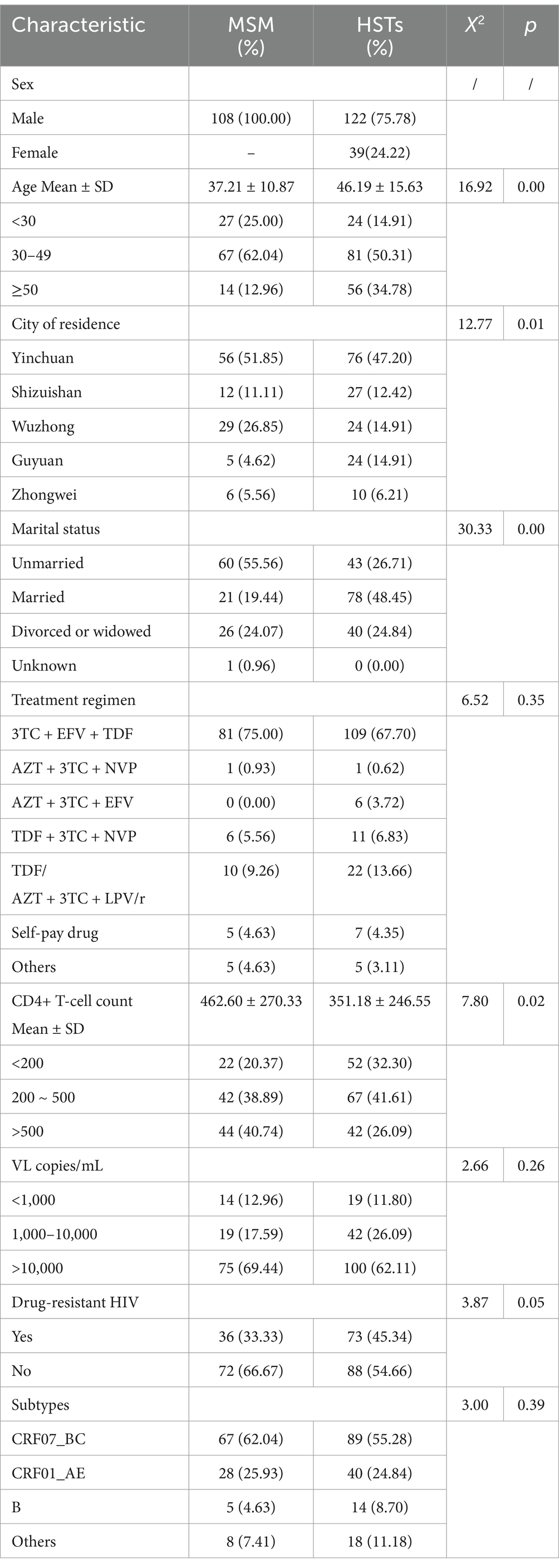
Table 1. Basic information of MSM and HSTs from 2020–2021 in Ningxia.
A total of 10 HIV-1 subtypes were detected, including CRF07_BC (156 cases (57.99%)) and CRF01_AE (68 cases (25.29%)), followed by B (19 cases (7.06%)), CRF08_BC (8 cases (2.97%)), C (4 cases (1.49%)), CRF55_ 01 B (4 cases (1.49%)), and CRF59_ 01 B (1 case (0.37%)). In addition, seven cases of URFs (2.60%) and one case of CRF79_0107 (0.37%) were detected in this study.
Different subtypes distributions were detected from patients of two different transmission routes. Seven subtypes were detected in the MSM group and 10 subtypes were detected in the HST group. CRF07_BC and CRF01_AE were the two major subtypes in both groups. The proportions of CRF07_BC and CRF01_AE subtypes in MSM were higher than those in HSTs, whereas subtypes CRF79_0107, CRF59_ 01 B, and A1 were only detected in HSTs (Figure 1).
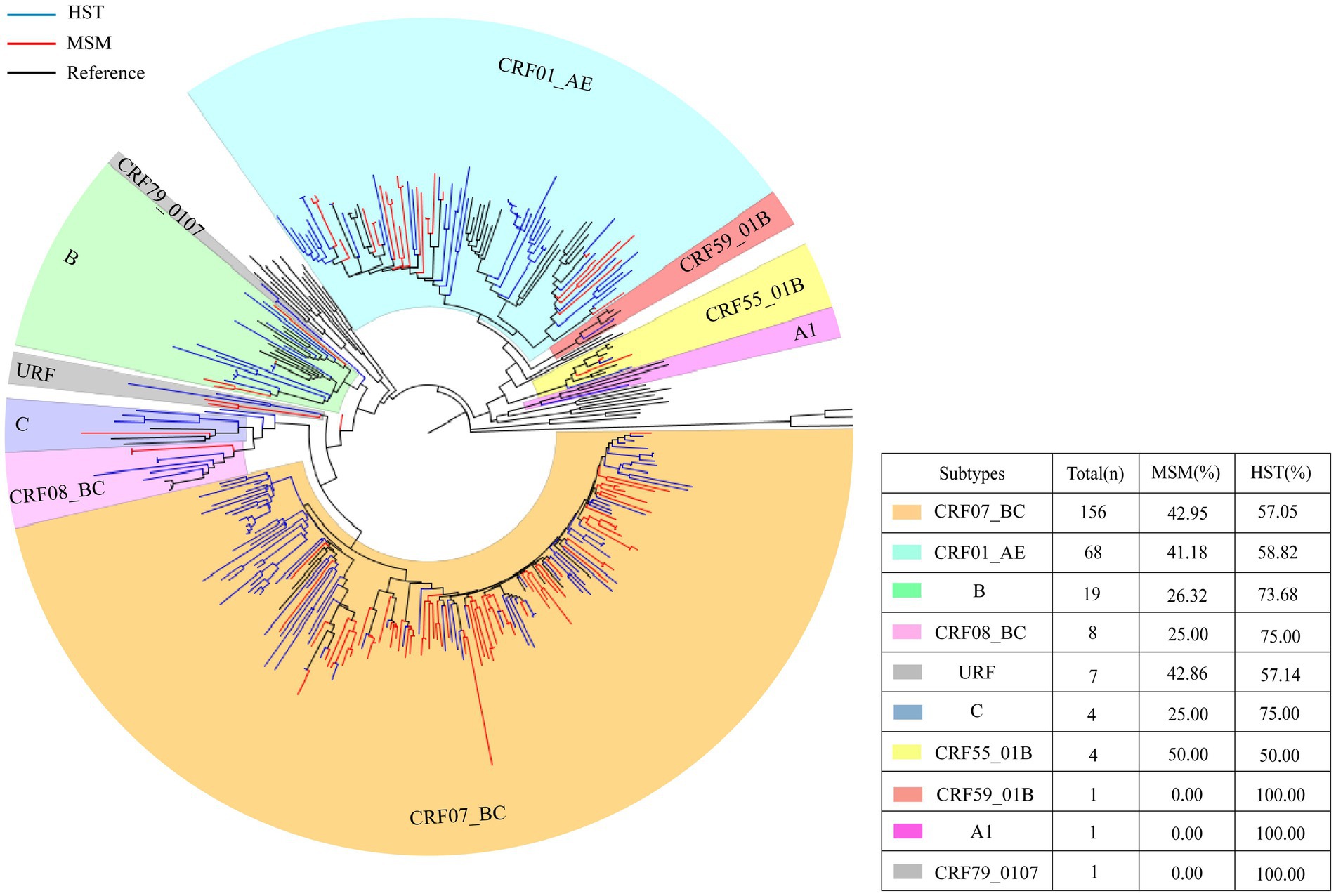
Figure 1. HIV-1 pol region phylogeny and gene subtype analysis of patients transmitted via MSM and HST. The blue branches indicate the sequences of HST, the red branches indicate the sequences from MSM, the black branches indicate reference sequences. A total of 156 sequences clustered with CRF07_BC, which HST making up 57.05% and MSM making up 42.95% (indicated by orange). 68 cases branched with CRF01_AE reference sequence, which HST accounted for 58.82% and MSM accounted for 41.18% (indicated by bluish green).19 cases of subtype B, with HST accounted for 73.68% and MSM accounted for 26.32% (indicated in grass green). 8 cases of CRF08_BC, which HST accounted for 75% and MSM accounted for 25% (indicated in light pink). 4 cases of subtype C, which HST accounted for 75% and MSM accounted for 25% (indicated in blue). 4 cases of CRF55_01B, with 50% of HST and MSM each (indicated in yellow).1 CRF59_01 B, only HST (indicated in red). 1 A1 detected in HST only (indicated in lavender).7 URF (HST 57.14%, MSM 42.86%) and 1 CRF 79 _ 0107 (HST detected only) (indicated in gray).
Among the 269 patients with successfully obtained sequences, HIV drug resistance mutations were detected in 109 individuals, and the resistance rate was 40.52% (109/269). The resistance rate in HST (45.34%, 73/161) was significantly higher than that in MSM (33.33%, 36/108), and there was a strong association between drug resistance and subtypes among the two groups (Figure 2A). Drug resistance to protease inhibitors (PIs), nucleoside reverse transcriptase inhibitors (NRTIs), and non-nucleoside reverse transcriptase inhibitors (NNRTIs) was found, and dual resistance to NRTIs/NNRTIs was dominant. The most common drug-resistant mutations in both MSMs and HSTs were NNRTI drugs, followed by NRTI drugs (Figures 2B,D). The sites and degrees of drug resistance were similar between the two groups (Figure 2C). There were four cases of PI-resistant mutations, and the most frequent mutation was Q58E, which was detected in both groups. The other PI-resistant mutations included I54V, V82A, M46I, and N88ND, which were detected only in HSTs (Figure 2B). All PI-resistant mutations showed low or intermediate resistance (Figure 2C). The main NRTI resistance mutation sites were M184V/I, K65R/KR/N, and K70E/R, and most were high resistance to 3TC, FTC, and abacavir (ABC). The main mutations responsible for NNRTI resistance were K103N/KN, V106M/A/I, and V179D/E/T, which were frequently detected in the CRF07_BC and CRF01_AE subtypes, and had the highest degree of resistance to NVP and EFV (Figures 2B–D).
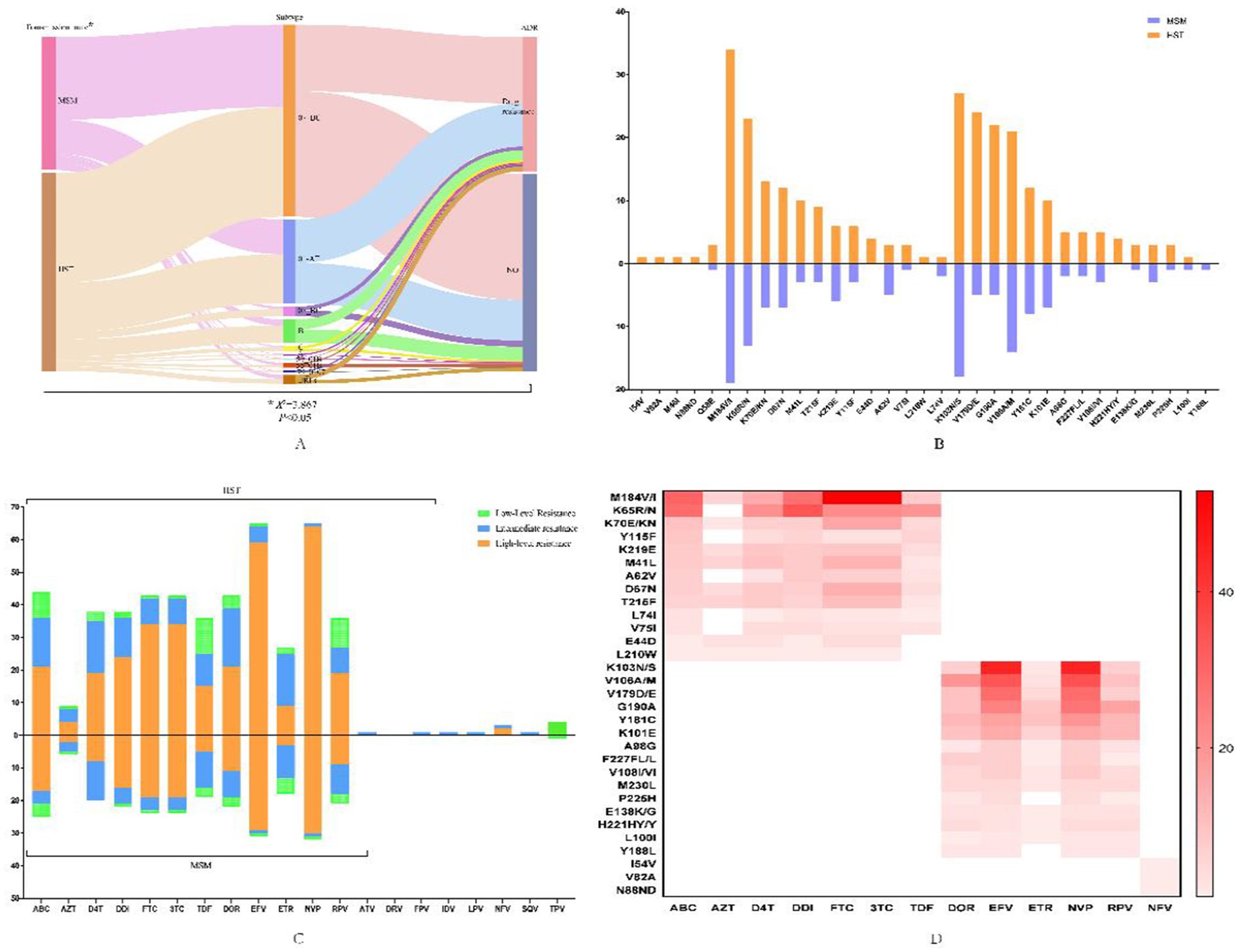
Figure 2. HIV-1 drug-resistant mutations and the profile of antiviral drug resistance in patients transmitted via MSM and HST. (A) Flow diagram of the relationship between infection routes, genotypes and drug resistance, which was analyzed by chi-square test. (B) Distribution of drug resistance sites in MSM and HST, in which the orange indicates HST and the blue indicates MSM. (C) Different antiviral drug resistance in MSM and HST, with the orange indicates high-level resistance, the blue indicates intermediate resistance and the green indicates low-level resistance. (D) Association of different antiviral drugs with major resistance sites that the darker color indicates greater effect of mutation sites on drugs. ABC, abacavir; AZT, zidovudine; D4T, stavudine; DDI, didanosine; FTC, emtricitabine; 3TC, lamivudine; TDF, tenofovir disoproxil fumarate; EFV, efavirenz; DOR, doravirine; NVP, nevirapine; RPV, Rilpivirine; ETR, etravirine; ATV/r, atazanavir/ritonavir; FPV/r, Fosamprenavir/ritonavir; IDV/r, indinavir/ritonavir; LPV/r, lopinavir/ritonavir, NFV, nelfinavir, SQV/r, saquinavir/ritonavir; TPV/r, tipranavir/ritonavir.
All 269 sequences were selected to construct a molecular network, and the total number of transmission clusters in the network peaked at 39.120 sequences entering the network, with a network entry rate of 44.61% under a gene distance threshold of 1.25%. Among the 120 sequences entered the network, 57 sequences were from MSM and 63 sequences were from HSTs. The clustering rate of MSM (52.78%) was higher than that of HST (39.13%). Among the most common HIV subtypes, the cluster rates of subtypes CRF07_BC, CRF01_AE, and CRF08_BC were 48.72, 42.65 and 50%, respectively. This difference was not statistically significant (Figure 3C). By taking a variable factor entered the HIV molecular transmission network as a dependent variable, logistic regression analysis (Table 2) showed that heterosexual transmission and drug resistance increased the risk of HIV infection entering the transmission network (adjusted odds ratio (AOR) > 1, p < 0. 05). Married and divorced or widowed patients, those taking lopinavir/ritonavir (LPV/r), non-drug resistance mutation, and those with VL > 10,000 copies/ml were the factors that were less likely to be included in the transmission network (AOR < 1, p < 0. 05).
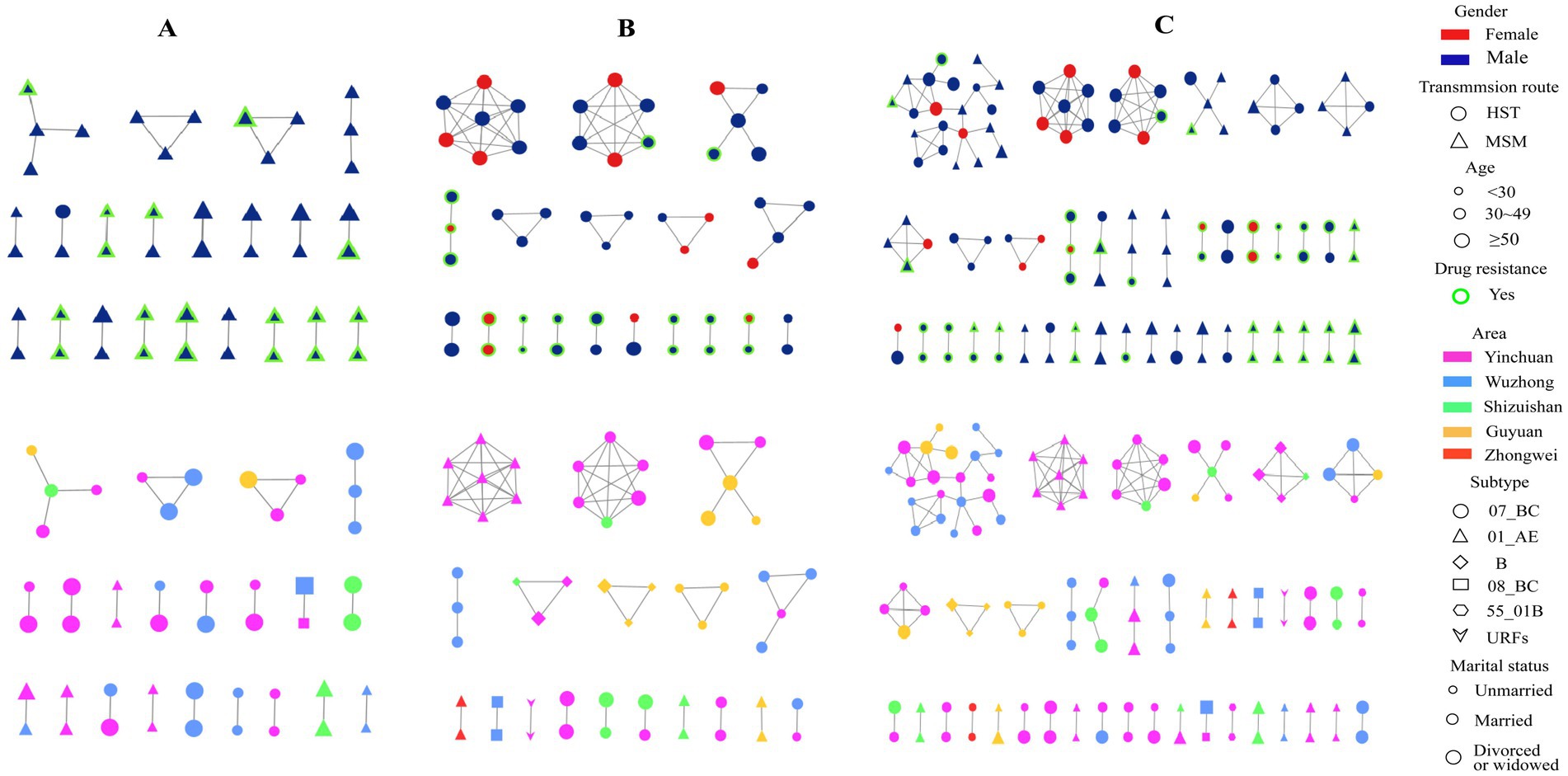
Figure 3. HIV-1 molecular transmission networks diagram. Top half: Molecular transmission network by gender, transmission route, age, and drug resistance, bottom half: Network by region, subtype, and marital status in MSM (A), HST (B) and combined MSM and HST populations (C).
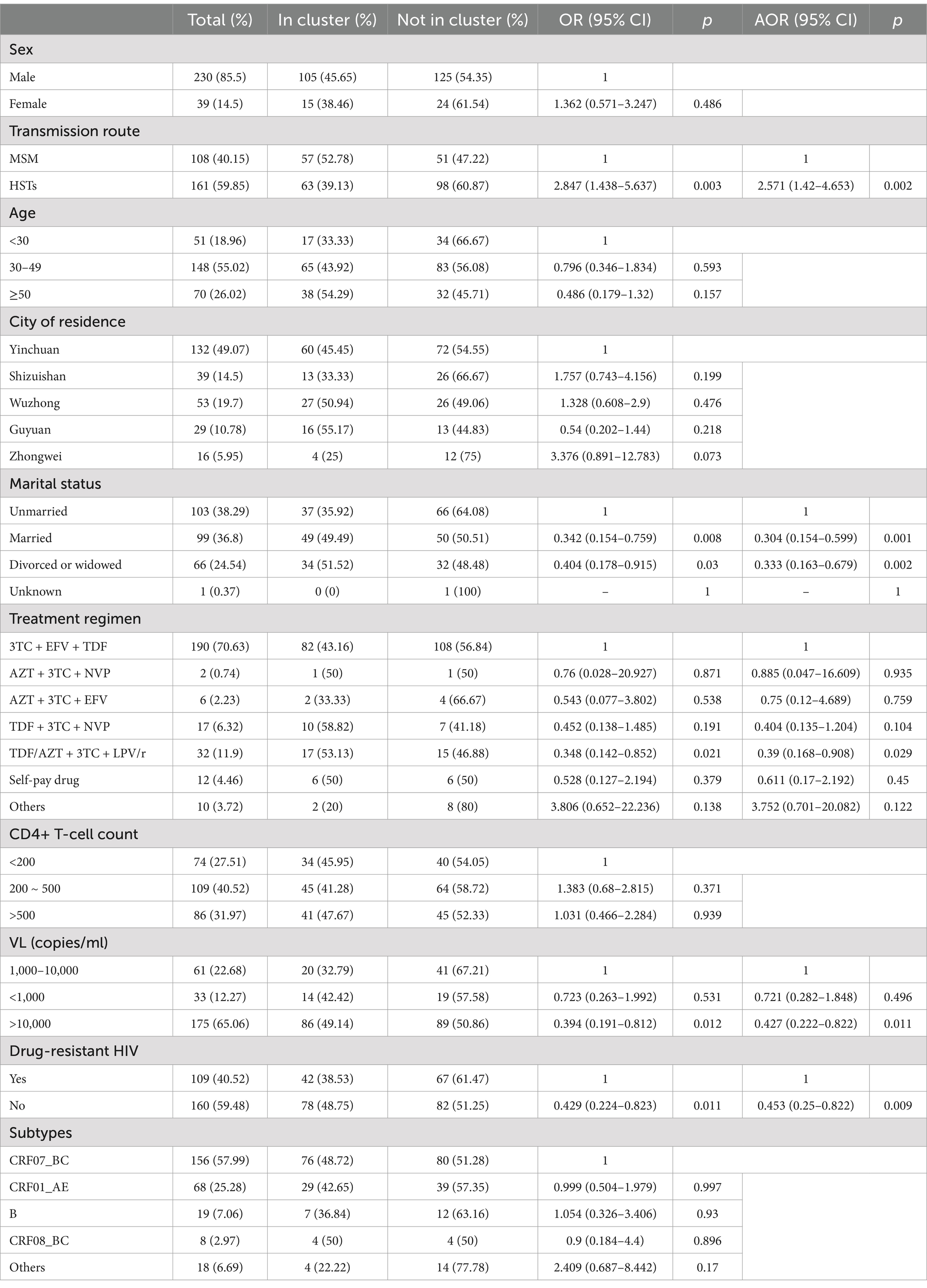
Table 2. Factors influencing HIV-1 molecular transmission networks via MSM and HSTs in 2020–2021.
When only the MSM population was selected to construct a molecular network, a total of 21 transmission clusters (47 cases) were found, with a clustering rate of 43.52% (47/108) under the 1.25% gene distance threshold, in which only four were spread clusters with more than three nodes. All CRF 08_BC subtypes in the MSM population were included in the network, followed by a higher proportion of CRF07_BC and CRF01_AE. None of the other subtypes were included in the network (Figure 3A). When only HSTs were selected to construct the transmission network, a total of 18 transmission clusters (53 cases) were found, with a clustering rate of 32.92% (53/161) under the 1.25% threshold, in which eight transmission clusters had more than three nodes. The highest clustering rate of subtypes in the HSTs was 50% for URFs, followed by subtype B (42.86%), CRF07_BC (34.83%), CRF08_BC (33.33%), and CRF01_AE (30%) (Figure 3B).
Since China adopted Free ART Program in 2003 and ‘Treat for all’ policy in 2016, free of charge virus load test were implemented for all patients of the PLWHA receiving ART once per year. By analyzing the characteristics of HIV subtypes, drug resistance, and molecular transmission networks of homosexually and heterosexually transmitted infections in Ningxia, this study explored the general characteristics and risk factors of sexual transmission and provided useful information for improving control measures in different populations.
The results of this study confirmed the trends and main characteristics of HIV-1 infection that have been reported previously in Ningxia, which include the following: (1) men aged 30–49 were a high-risk population; (2) heterosexual transmission was the major sexual transmission route; (3) the majority of patients (79.93%) were taking first-line antiviral drugs; and (4) the primary gene subtypes were CRF07_BC and CRF01_AE. Compared with transmission among heterosexual individuals, MSM are younger, unmarried, and better-educated (19). However, MSMs are more likely to conceal their sexual orientation, which can cause intrafamily transmission and spread HIV to the general population (20).
There are reports showing different distribution of HIV-1 subtypes among different populations and regions (21, 22). Although a total of 10 HIV-1 subtypes were detected in the subjects of this study, CRF07_BC and CRF01_AE were the two dominant subtypes, which is consistent with the findings in other regions of China (23, 24). These two subtypes are the most prevalent strains of sexually transmitted HIV-1 in most regions. Subtype B is another major viral strain that spreads through sexual transmission, but it is usually overshadowed by the increasing prevalence of CRF01_AE (25). HIV-1 subtypes in Ningxia have recently become more diverse, with the feature of increasing detections of URFs. The study also found that the subtypes of heterosexually transmitted HIV were more diverse than those in MSM because subtypes A1, CRF79_0107, and CRF59_ 01 B were detected only in heterosexual individuals.
With increasing ART coverage, drug resistance mutations accumulate gradually, which may lead to treatment failure and further spread of HIV resistance (26). Some studies have shown that the incidence of drug resistance among MSM is higher than that among the general population (27). In this study, the drug resistance rate of individuals with sexually transmitted HIV was 40.52%, which was lower than the overall acquired drug resistance rate of 51.33%, which was calculated by a meta-analysis of results reported in China (28), indicating a regional difference in HIV-1 prevalence. The most common drug resistance in this study was NNRTIs, followed by NRTIs and PIs, which is consistent with previous reports (29). Among the drug resistance mutations in NRTIs, M184V/I, K65R/KR/N, and K70E/R were the main drug resistance sites. The M184V/I mutations have high and medium levels of resistance to 3TC and FTC, respectively, and the K65R mutation can reduce sensitivity to TDF (30). Among the drug resistant NNRTIs, K103N/KN, V106M/A/I, and V179D/E/T were the main mutations. Among them, the K103N caused a high level of resistance to the drugs NVP and EFV in patients receiving ART (31, 32).
In this study, under a gene threshold of 1.25%, the total clustering rate of sexual transmission in Ningxia was 44.61%. Heterosexual transmission and drug resistance increased the risk of HIV entering the transmission network (AOR > 1, p < 0.05), indicating that these two factors increased the risk of HIV transmission by the network (33, 34). These results are similar to those of a study conducted in the Eastern China Province, Jiangsu (35), Married, divorced, or widowed patients were less likely to be included in the transmission network. In other words, unmarried people usually have more social connections and are more likely to get HIV infection through their networks. The study also found that the patients who took LPV/r-containing medications and had a VL >10,000/mm3 were less likely to be included in the transmission network, which can be explained by the fact that LPV/r-containing medication had a lower chance of drug resistance (Figure 2) and high VL may limit individual social activities. The clustering rate of CRF08_BC was higher than that of CRF07_BC and CRF01_AE in our study, and all MSMs infected with the CRF08_BC subtype were included in the cluster. CRF08_BC has been reported to spread among different high-risk groups (injecting drug users and heterosexual individuals) to men who have sex with men (36, 37). Therefore, real-time monitoring of CRF08_BC subtype is necessary to prevent HIV-1 transmission (38).
Our analysis also found that MSMs and HSTs were involved in the same cluster (Figure 3C), indicating that some individuals acted as bridges for transmission between the two populations. Identification and control of these “bridge individuals, “who may have a bi-sexual orientation, are very important to curb the spread of HIV in different populations.
This study had some limitations. First, patients with sexually transmitted HIV who received ART were selected and other routes of transmission were not included. As a result, the findings may not be generalizable to the entire population. Selection of patients with high viral loads and unsuccessful extraction of sequences from some samples can also generate bias. Follow-up studies should consider including all HIV/AIDS patients to better explain and analyze the characteristics of HIV transmission and improve sample processing and sequencing. This was a cross-sectional study and active transmission clusters could not be identified. A real-time dynamic network analysis will be more meaningful to trace the transmission source and improve the credibility of the molecular network.
Sexual transmission is the predominant source of new HIV-1 infection in Ningxia, and both heterosexual and homosexual (exclusively MSMs) transmissions play roles. Our study showed that heterosexual transmission has more diverse genotypes and a higher risk of drug resistance than homosexual transmission. The molecular transmission network analysis found an increased cluster rate when combined the sequences of MSMs and HSTs than the analysis of separately, indicating the transmission of HIV-1 between the two populations, to which should pay extra attention. To achieve more effective and precise HIV-1 prevention and patient care, it is important to strengthen genetic monitoring and real-time network analyses.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Ningxia Centre of Disease Control and Prevention. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
JP: Validation, Funding acquisition, Writing - review & editing. ZW: Funding acquisition, Supervision, Writing - review & editing, Writing - original draft. BS: Data curation, Formal analysis, Software, Writing - original draft, Writing - review & editing. CM: Data curation, Formal analysis, Software, Writing - review & editing. YiL: Data curation, Formal analysis, Software, Writing - review & editing. XM: Data curation, Formal analysis, Software, Writing - review & editing. WK: Data curation, Writing - review & editing, YZ: Data curation, Writing - review & editing. YoL: Supervision, Validation, Writing - review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research was supported by grants from the Public Health Leaders Program in China and Ningxia Natural Science Foundation (No:2024AAC03734).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2024.1485516/full#supplementary-material.
1. de, K, Jaffe, H, and Curran, J. The evolving epidemiology of HIV/AIDS. J AIDS. (2012) 26:1205–13. doi: 10.1097/QAD.0b013e328354622a
2. UNAIDS Global Issues: AIDS, (2021). Available at: https://www.un.org/en/global-issues/aids
3. Wu, Z, Chen, J, Scott, SR, and JM, MG. History of the HIV epidemic in China. J Curr HIV/AIDS Rep. (2019) 16:458–66. doi: 10.1007/s11904-019-00471-4
4. Na, H. Research Progress in the epidemiology of HIV/AIDS in China. J China CDC weekly. (2021) 3:1022–30. doi: 10.46234/ccdcw2021.249
5. He, H, Lv, F, Zhang, NN, Wu, Z, Liao, Q, Chang, Z, et al. Look into the HIV epidemic of gay Community with a socio-cultural perspective: a qualitative study in China, 2015-2016. PLoS One. (2017) 12:e0170457. doi: 10.1371/journal.pone.0170457
6. Yin, Y, Liu, Y, Zhu, J, Hong, X, Yuan, R, Fu, G, et al. The prevalence, temporal trends, and geographical distribution of HIV-1 subtypes among men who have sex with men in China: a systematic review and meta-analysis. Epidemiol Infect. (2019) 147:e83. doi: 10.1017/s0950268818003400
7. Xiao, P, Li, J, Fu, G, Zhou, Y, Huan, X, and Yang, H. Geographic distribution and temporal trends of HIV-1 subtypes through heterosexual transmission in China: a systematic review and Meta-analysis. Int J Environ Res Public Health. (2017) 14:830. doi: 10.3390/ijerph14070830
8. Cao, W, Hsieh, E, and Li, T. Optimizing treatment for adults with HIV/AIDS in China: successes over two decades and remaining challenges. Curr HIV/AIDS Rep. (2020) 17:26–34. doi: 10.1007/s11904-019-00478-x
9. Lampe, FC, Rodger, AJ, Burman, W, Grulich, A, Friedland, G, Sadr, WE, et al. Impact of early antiretroviral treatment on sexual behaviour: a randomised comparison. AIDS (London, England). (2019) 33:2337–50. doi: 10.1097/qad.0000000000002359
10. Zhao, Y, Han, MJ, Gan, XM, Ma, Y, and Zhao, DC. Characteristics and viral suppression among people living with HIV from the National Free Antiretroviral Therapy Programme, 2019. HIV Med. (2020) 21:701–7. doi: 10.1111/hiv.13020
11. Zuo, Z, Liang, S, Sun, X, Bussell, S, Yan, J, Kan, W, et al. Drug resistance and Virological failure among HIV-infected patients after a decade of antiretroviral treatment expansion in eight provinces of China. PLoS One. (2016) 11:e0166661. doi: 10.1371/journal.pone.0166661
12. Zuo, L, Liu, K, Liu, H, Hu, Y, Zhang, Z, Qin, J, et al. Corrigendum to “trend of HIV-1 drug resistance in China: a systematic review and meta-analysis of data accumulated over 17 years (2001-2017)” [EClinicalMedicine 18 (2020) 100238]. J EClinicalMedicine. (2021) 33:100696–6. doi: 10.1016/j.eclinm.2020.100696
13. Van Vaerenbergh, K. Study of the impact of HIV genotypic drug resistance testing on therapy efficacy. Verhandelingen - Koninklijke Academie voor Geneeskunde van Belgie. (2001) 63:447–73.
14. LiHua, Z, YunHui, Z, Ling, S, and JianHua, Z. Analysis of surveillance data on HIV/AlDS antiviral therapy in Ningxia from 2005 to 2018. Journal of l of Ningxia Medical, (2020) 42:917–9. doi: 10.13621/j.1001-5949.2020.10.0917
15. Prevention, C. C. f. D. C. a. Technical guidelines for HIV transmission network monitoring and intervention. (2019).
16. Prevention, C. C. f. D. C. a. Guidelines for drug resistance testing and quality assurance of HIV-1 genotypes. Beijing: The People’s Health Publishing House, 12–16 (2013).
17. Shafer, RW, Rhee, SY, Pillay, D, Miller, V, Sandstrom, P, Schapiro, JM, et al. HIV-1 protease and reverse transcriptase mutations for drug resistance surveillance. AIDS (London, England). (2007) 21:215–23. doi: 10.1097/QAD.0b013e328011e691
18. Little, SJ, Kosakovsky Pond, SL, Anderson, CM, Young, JA, Wertheim, JO, Mehta, SR, et al. Using HIV networks to inform real time prevention interventions. PLoS One. (2014) 9:e98443. doi: 10.1371/journal.pone.0098443
19. Qiao, S, Zhou, G, and Li, X. Disclosure of same-sex behaviors to health-care providers and uptake of HIV testing for men who have sex with men: a systematic review. Am J Mens Health. (2018) 12:1197–214. doi: 10.1177/1557988318784149
20. Zhuoma, L, Zhang, Y, Yan, T, Kang, F, Hou, X, Chen, J, et al. Non-disclosed men who have sex with men within local MSM HIV-1 genetic transmission networks in Guangyuan, China. Front Public Health. (2022) 10:956217. doi: 10.3389/fpubh.2022.956217
21. Thomson, MM, Pérez-Alvarez, L, and Nájera, R. Molecular epidemiology of HIV-1 genetic forms and its significance for vaccine development and therapy. Lancet Infect Dis. (2002) 2:461–71. doi: 10.1016/s1473-3099(02)00343-2
22. Li, X, Li, W, Zhong, P, Fang, K, Zhu, K, Musa, TH, et al. Nationwide trends in molecular epidemiology of HIV-1 in China. AIDS Res Hum Retrovir. (2016) 32:851–9. doi: 10.1089/aid.2016.0029
23. Yuan, D, Zhong, X, Li, Y, He, Q, Li, N, Li, H, et al. Molecular Transmission Network of Newly Reported HIV Infections in Pengzhou, Sichuan Province: A Study Based on Genomics and Spatial Epidemiology. in J Environ Res Public Health. (2023) 20:2523. doi: 10.3390/ijerph20032523
24. Zhou, PP, Yu, G, Kuang, YQ, Huang, XH, Li, Y, Fu, X, et al. Rapid and complicated HIV genotype expansion among high-risk groups in Guangdong Province, China. BMC Infect Dis. (2019) 19:185. doi: 10.1186/s12879-019-3788-7
25. He, X, Xing, H, Ruan, Y, Hong, K, Cheng, C, Hu, Y, et al. A comprehensive mapping of HIV-1 genotypes in various risk groups and regions across China based on a nationwide molecular epidemiologic survey. PLoS One. (2012) 7:e47289. doi: 10.1371/journal.pone.0047289
26. Hecht, FM, Grant, RM, Petropoulos, CJ, Dillon, B, Chesney, MA, Tian, H, et al. Sexual transmission of an HIV-1 variant resistant to multiple reverse-transcriptase and protease inhibitors. N Engl J Med. (1998) 339:307–11. doi: 10.1056/nejm199807303390504
27. Defu, Y, Yueqi, Y, Jianshuang, C, Ying, Z, Jing, L, Gengfeng, F, et al. Drug resistance in naive HIV/AIDS virological treatment-failed population in China:a Meta-analysis. Journal of l of Ningxia Medical. (2022) 28:162–7. doi: 10.13419/j.cnki.aids.2022.02.07
28. Yuan, D, Liu, Y, Zhou, Y, Shi, L, Chen, J, Lu, J, et al. Men who have sex with men is the high-risk drug resistance population: a meta-analysis of HIV-1 drug resistance profiles and trends in China. J Clin Pharm Ther. (2022) 47:1729–37. doi: 10.1111/jcpt.13772
29. Obasa, AE, Engelbrecht, S, and Jacobs, GB. Near full-length HIV-1 subtype B sequences from the early south African epidemic, detecting a BD unique recombinant form (URF) from a sample in 1985. Sci Rep. (2019) 9:6227. doi: 10.1038/s41598-019-42417-1
30. Obasa, AE, Mikasi, SG, Brado, D, Cloete, R, Singh, K, Neogi, U, et al. Drug resistance mutations against protease, reverse transcriptase and integrase inhibitors in people living with HIV-1 receiving boosted protease inhibitors in South Africa. Front Microbiol. (2020) 11:438. doi: 10.3389/fmicb.2020.00438
31. Zhihui, X, XueRong, Y, and Zefeng, D. Characteristics of drug resistance among HIV-1 infected patients with failed antiviral treatment in Suzhou city from 2017 to 2018. Int J Virol. (2022) 1:8. doi: 10.3760/cma.j.issn.1673-4092.2022.01.008
32. Ávila-Ríos, S, García-Morales, C, Matías-Florentino, M, Romero-Mora, KA, Tapia-Trejo, D, Quiroz-Morales, VS, et al. Pretreatment HIV-drug resistance in Mexico and its impact on the effectiveness of first-line antiretroviral therapy: a nationally representative 2015 WHO survey. Lancet HIV. (2016) 3:e579–91. doi: 10.1016/s2352-3018(16)30119-9
33. Gilks, CF, Crowley, S, Ekpini, R, Gove, S, Perriens, J, Souteyrand, Y, et al. The WHO public-health approach to antiretroviral treatment against HIV in resource-limited settings. Lancet (London, England). (2006) 368:505–10. doi: 10.1016/s0140-6736(06)69158-7
34. Zuo, L, Liu, K, Liu, H, Hu, Y, Zhang, Z, Qin, J, et al. Trend of HIV-1 drug resistance in China: a systematic review and meta-analysis of data accumulated over 17 years (2001–2017). J EClinicalMedicine. (2020) 18:100238. doi: 10.1016/j.eclinm.2019.100238
35. Dennis, AM, Volz, E, Frost, ASMSDW, Hossain, M, Poon, AFY, Rebeiro, PF, et al. HIV-1 transmission clustering and Phylodynamics highlight the important role of Young men who have sex with men. AIDS Res Hum Retrovir. (2018) 34:879–88. doi: 10.1089/aid.2018.0039
36. Li, X, Gao, R, Zhu, K, Wei, F, Fang, K, Li, W, et al. Genetic transmission networks reveal the transmission patterns of HIV-1 CRF01_AE in China. Sex Transm Infect. (2018) 94:111–6. doi: 10.1136/sextrans-2016-053085
37. Zhou, Y, Lu, J, Zhang, Z, Sun, Q, Xu, X, and Hu, H. Characteristics of the different HIV-1 risk populations based on the genetic transmission network of the newly diagnosed HIV cases in Jiangsu, Eastern China. Heliyon. (2023) 9:e22927. doi: 10.1016/j.heliyon.2023.e22927
Keywords: China, HIV - human immunodeficiency virus, art, sexually transmitted, genetic transmission networks
Citation: Pei J, Wu Z, Si B, Ma C, Liu Y, Ma X, Kuai W, Zhang Y and Li Y (2025) HIV-1 drug resistance and genetic transmission networks among patients with sexually transmitted HIV in Ningxia, China. Front. Public Health. 12:1485516. doi: 10.3389/fpubh.2024.1485516
Edited by:
Hongshuo Song, University of Maryland, United StatesReviewed by:
Adetayo Emmanuel Obasa, Stellenbosch University, South AfricaCopyright © 2025 Pei, Wu, Si, Ma, Liu, Ma, Kuai, Zhang and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yong Li, bGl5b25nNzczMkBueHUuZWR1LmNu
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.