 Cristina Caramés1*†
Cristina Caramés1*† Ion Cristóbal
Ion Cristóbal- 1Quirónsalud Healthcare Network, Grupo Hospitalario Quirónsalud, Madrid, Spain
- 2Hospital Universitario Fundación Jiménez Díaz, Madrid, Spain
- 3Clinical and Organizational Innovations Unit, Hospital Universitario Fundación Jiménez Díaz, Madrid, Spain
Controversy surrounds the current debate regarding the effects of outsourcing health services, as recent studies claim that increased outsourcing leads to reduced costs at the expense of worse patient outcomes. The goal of the value-based model is to enable healthcare systems to create more value for patients, and evidence points to improvements in public health outcomes, patient experience, and health expenditure in systems incorporating components of value-based healthcare. Some emerging evidence indicates promising results for outsourced hospitals which follow a value-based model of healthcare delivery. Although additional future studies are still needed to confirm these benefits, value-based healthcare merits discussion as a new perspective on the public versus private management debate. In fact, we argue that outsourcing to value-based health providers could represent a valid alternative for public health management, encouraging greater competition within the healthcare sector while ensuring quality of care for both public and private sectors.
Introduction
European health systems currently fall under one of three co-existing management models: National Health Services, Social Insurance-based Systems or Mixed Model systems. These models differ regarding aspects such as financing, economic policies, and service delivery. In European countries with established National Health Services (United Kingdom, Spain, Italy, Portugal, and Denmark, among others), universal access to health care is guaranteed and financed through public taxation. A strong primary care network is at the core of National Health Services, with general practitioners acting as first port of call for the patients in their catchment area and as gatekeepers to specialist care. In this model, hospitals and other care facilities are owned by the state, but management may be delegated to non-profit or for-profit private organizations (1). Social Insurance-based systems rely on compulsory contributions from employers and employees to insurance funds used to reimburse healthcare providers. Healthcare providers can be either public or private (2). Examples of European countries following this model of healthcare include Germany, France, and the Netherlands (3–5), all of which provide universal access to healthcare. Finally, mixed systems, such as that of Bulgaria (6), involve a significant amount of private funding from voluntary insurance schemes or out-of-pocket reimbursement.
Over the last decade, there has been an evident shift in Europe toward outsourcing the management of publicly to private organizations, usually on the grounds of controlling national healthcare expenditure and increasing competitivity in the healthcare sector. However, while reversing this trend seems unlikely, largescale outsourcing has sparked concern that the financial interests of private organizations are undermining quality of care, leading to a heated debate in which defenders of healthcare outsourcing argue that increasing competition will improve healthcare service performance, while opponents contend that, although outsourcing seems to be an unavoidable consequence of financial pressure and increased demand for healthcare, it will surely lead to worse patient outcomes (7). As the Mixed model of healthcare is relatively uncommon in Europe, this article focuses mainly on potential effects of outsourcing in National Health Systems and Social Insurance-based models. While funding sources differ between models, both systems rely in lesser or greater measure on publicly owned entities to deliver care. In the National Health System blueprint, all resources are owned and managed by the state; Social Insurance-based models such as that of Germany own and manage around a third of national hospitals (8, 9). Strong national regulation of healthcare in both NHS and SI models means that healthcare is generally accessible to all residents. Both types of systems have increasingly turned to outsourcing publicly owned facilities and services since the early 2000s, citing similar reasons for this strategy: existence of financial constraints; need to improve system efficiency; need to incorporate new technologies; and the search for improved quality of care (7). Outsourcing can be performed on different scales, from contracting uncritical services such as laundry or catering, to outsourcing the management of medical facilities, to contracting highly critical services such as cardiology or intensive care (10, 11). Possible risks to data security, potential negative effects on the quality of care offered to patients, and cost-motivated staff reductions are concerns voiced by opponents of outsourcing in both systems (12).
This article aims to make a constructive contribution to the current “public versus private” healthcare debate by adding a new perspective which is currently gaining importance in countries with universal access to healthcare: value-based healthcare delivery. Although VBHC was conceived in the United States as a form of driving competition between healthcare providers, in Europe, where most countries grant universal access to care, VBHC is seen as driving cooperation between organizations to ensure patient-centered, high-quality care while reducing related costs. At the heart of VBHC is the objective of providing value to patients (patient-centered care) at the lowest possible cost, an objective that transcends ownership or management status (13). Thus, elements of VBHC have been successfully implemented in different models of healthcare, and in both privately and publicly managed facilities. Several successful case studies in VBHC in Europe include the private, non-profit Diabeter Network in the Netherlands, which provides integrated, person-centered care for people with Type 1 diabetes and has demonstrated improved clinical outcomes while reducing expenditure (14); the privately-owned Martini Klinik in Germany, which is an internationally recognized center for the treatment of prostate cancer (15); the Quirónsalud network in Spain, which manages both private and public hospitals (16–21); and the public-private Netherlands Heart Network (22, 23). In this article, we highlight legitimate concerns about outsourcing healthcare and summarize available evidence on outcomes in outsourced care, underlining the importance of taking different forms of care delivery into account when analyzing healthcare services and patient outcomes. We review the concept of value-based care and present recent examples of implementation of this model of care delivery. Finally, we summarize current evidence suggesting that value-based care may improve clinical outcomes and overall quality of care, indicating that how healthcare is managed may be even more important than who manages it.
Potential effects of outsourcing in countries with universal access to healthcare: an update
Several studies have evaluated the impact of healthcare outsourcing in countries with universal access to healthcare, using different perspectives and parameters (Table 1).
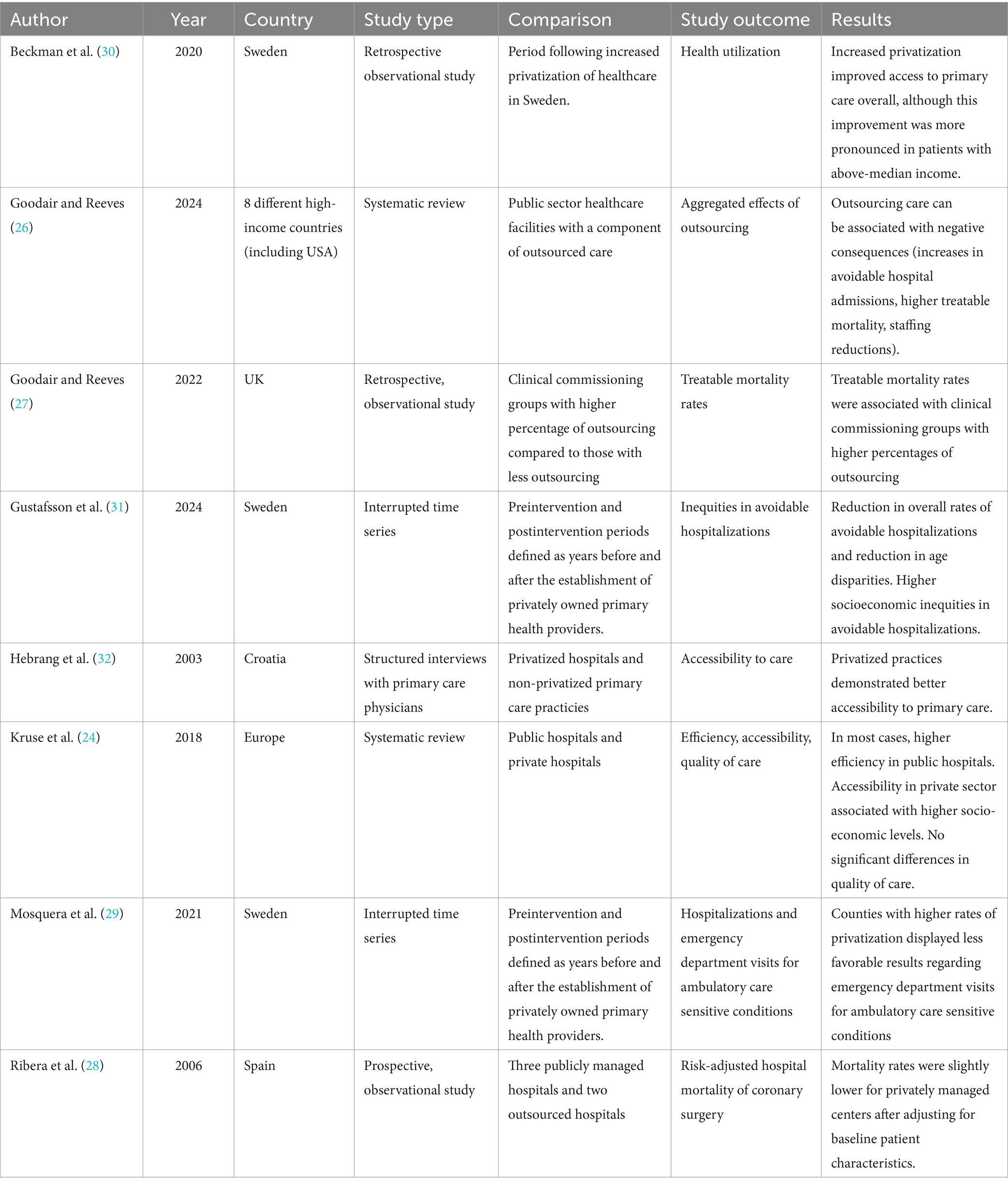
Table 1. Summary of cited studies on the effects of outsourcing healthcare services in high-income countries.
A systematic review comparing European public and private hospitals in terms of efficiency, accessibility, and quality of care (24) concluded that, with some exceptions, public hospitals were more efficient than their private counterparts. In this review, accessibility to private sector was associated with higher social-economic levels. Evidence for differences in quality of care between public and private hospitals was inconclusive. The review included studies published before June 2017 from countries with different healthcare management models. Individual studies used different indicators to measure efficiency, accessibility, and quality of care, making comparison between public and private hospitals difficult, and limiting the generalizability of these findings. This systematic review provides valuable information about the state of European public and private healthcare sectors before the COVID-19 pandemic.
A qualitative analysis of 24 different studies performed in the last decade examining the perspectives of both public and private social care providers (such as long-term geriatric and mental health facilities) highlighted that under austere financial conditions – such as ongoing budget cuts in the healthcare sector – it is a mistake to assume that trying to increase competency of public providers through outsourcing will improve quality in healthcare delivery (25). Notably, both public and private providers expressed similar issues with contracts, commenting that unstable regulation and insufficient prices led to deteriorated employment conditions and service quality in both sectors. A limitation of this study is that it focused exclusively on social care providers, without including the perspective of acute or primary care.
A recent publication by Goodair and Reeves (26) investigated the aggregated effects of outsourcing in high-income countries, including studies from 2009 to 2022. Notably, this systematic review highlighted that outsourcing care can cause negative consequences due to the development of cost reduction strategies leading to reductions in staffing, increases in avoidable hospital admissions as reported by one study, and higher treatable mortality as observed in three studies. The authors conclude that outsourcing may indeed reduce costs, but potentially at the expense of quality of care. However, it is important to consider that only 13 studies from eight different healthcare systems were included in the analysis, less than half of which focused on health outcomes. A small sample size, heterogeneities among included healthcare systems, and lack of evidence from the majority of European countries entail that these conclusions must be taken cautiously.
In a previous work, the same authors performed an observational study analyzing the effects of outsourcing healthcare on treatable mortality rates between 2013 and 2020 in England (27). Interestingly, they found that the increase in the percentage of outsourcing was significantly associated with an increase in treatable mortality, hypothesizing that this finding was caused by lower quality of the healthcare services offered by for-profit providers. As in the previous case, this study presents some key limitations, such as the lack of data on the complexity of the population attended or information on the specific services provided by the supplier. In fact, the authors stated that a causal relationship cannot be established between increased mortality and the outsourcing of health care. Their findings contrast with a study from Spain, in which patients undergoing coronary bypass surgery in outsourced hospitals presented significantly lower mortality rates than in publicly managed hospitals, after adjusting for surgical risk and comorbidities (28).
A series of studies focusing on the effects of increased outsourcing of primary care in Sweden found that overall higher levels of outsourcing were associated with lower rates of avoidable hospital admissions across the country (although with higher rates of avoidable admissions in regions with more outsourced care), as well as with increased overall access to primary care and lower disparities in access to care across age groups, although with higher rates of emergency care use and disparities in hospitalizations and access to care across socioeconomic groups (29–31). The effects of increased outsourcing in primary care were also examined in a study from the Croatian healthcare system, which found that outsourcing was associated with an increase in access to care (32).
Altogether, bearing in mind the complexity of healthcare scenario and the increasing prevalence of outsourcing in Europe, we believe that policymakers should analyze different models of healthcare delivery in privately managed care in order to determine which strategies can effectively increase quality of care.
Value-based care delivery as a novel optimal strategy for healthcare management
At the end of the 20th century, a revolutionary new concept – evidence-based medicine – emphasized the need for clinical decisions to be based on the best available scientific evidence along with the best clinical expertise (33). Moreover, decisions should integrate patient’s preferences to ensure the highest possible quality of life at lower costs (34). In 2006, emergence of value-based healthcare in the United States of America marked a milestone in the evolution of evidence-based medicine as a form of healthcare delivery.
The value-based model of healthcare delivery challenges the traditional model of healthcare by incorporating changes geared toward improving outcomes that truly matter to patients, and in the most sustainable way (13, 35). Redesigning health systems to focus on value for patients involves not only measuring clinician reported outcomes (CROMs), but also incorporating patient-reported outcomes and experience measures (PROMs and PREMs). In the value-based model of care delivery, capitation-based payment is exchanged for pay-for-performance which aligns reimbursement with value to incentivize “quality of care” over “quantity of care.” Value-based care promotes the organization of care around medical conditions through integrated practice units, thus promoting truly patient-centered care, as well as harnessing information technology, optimizing the geography of care, and ensuring systems integration to improve equity and sustainability in access to healthcare by streamlining the logistics of care delivery.
When analyzing the effect of value-based healthcare, it is important to consider that the potential applications of this model could differ across healthcare systems. However, the objective of value-based care – to enable healthcare systems to create more value for patients – remains the same (36). Various studies have examined the effectiveness of the different components of value-based healthcare on quality of care. The importance of measuring patient-reported outcomes is indisputable, and many studies have demonstrated that patients participating in PROMs initiatives from a range of clinical specialties present better outcomes (including improved symptom control, quality of life, and patient-provider communication) than non-participants (37–39). Evidence for pay-for-performance comes mostly from US and UK studies which show heterogeneous effects on quality of care, with results varying widely among centers (40, 41). Several studies suggest that pay-for-performance is associated with better clinical outcomes including immunization rates and control of risk factors for cardiovascular disease (42–44). A recent study from France demonstrated overall improvement in public health outcomes for primary care centers participating in a pay-for-performance program, including higher rates of chronic disease follow-up and cancer prevention, as well as lower rates of iatrogenesis and inappropriate antibiotic use (45). Healthcare-related expenditure also improved over the three-year study period. The implementation of integrated practice units has been associated with decreased complications of treatment and hospital readmission rates (19, 46), increased access to care even for uninsured patients (47, 48), improved patient experience (19), and reductions in healthcare costs. Finally, few studies focus on the other components of value-based care (systems integration, optimizing geography of care through national centers of excellence to provide care for exceedingly complex patients, and developing a robust information technology platform) and more research is necessary to confirm the effect of these components on quality of care and clinical outcomes (49).
Although many European countries are embracing VBHC as a solution to the current state of healthcare, many obstacles exist. One of the greatest challenges to VBHC is that current healthcare systems have been around for many decades and cannot be redesigned “from scratch”; in fact, healthcare provider and payer resistance is one of the greatest barriers to VBHC implementation. The initial costs of implementing VBHC – for example, expenditure on enabling IT platforms – can be problematic, especially in underfunded countries. However, in the long run, studies point to cost savings due to improved patient outcomes and care-related costs (50). While the original concept of VBHC includes six components which should be implemented simultaneously, most successful real-life implementations of VBHC in Europe focus on one or two components, such as measuring costs and outcomes for every patient, or organizing care into integrated practice units. Many studies cite legal barriers and adherence to traditional, “pay for service” payment models as a major challenge toward implementing VBHC, as healthcare providers are not incentivized to provide higher value care and multiple obstacles exist impeding reorganization of care (51). The concept of “bundled payment” and “pay for performance,” too, have its potential drawbacks. In systems that are highly dependent on private insurance without strong government regulation, such as the USA, patients with risk factors are prone to being “lemon dropped,” while in systems with a majority of publicly owned facilities and tighter government regulation (such as most European countries), hospitals in socially deprived areas or with a greater complexity case-mix could be unjustly penalized for worse outcomes (52). One of the pillars of VBHC – measuring costs and outcomes for every patient – can be burdensome to both patients and healthcare providers, pointing to the need to implement strategies to reduce survey fatigue and increased paperwork, especially in understaffed healthcare settings (53, 54). The organization of care into Integrated Practice Units, while often applicable in the USA setting, is often deemed unpractical in the European setting (55); however, advocates of VBHC have proposed developing standardized patient pathways as an alternative to IPUs to achieve better, patient-centered organization of care (56).
Does VBHC transcend the public-private debate by improving healthcare outcomes independently of hospital ownership/management status?
Current indicators used to compare public and private healthcare outcomes include clinical outcomes (such as mortality rates and hospital-acquired infection), efficiency metrics (such as average length of hospital stay and surgical waiting lists), patient satisfaction metrics, and cost analyses. To determine if VBHC can transcend the public-private debate by improving these outcomes independently of hospital ownership/management status, we performed a scoping review of the literature, focusing on studies published since 2020 in European countries. We included only those studies describing already-implemented VBHC solutions, excluding theoretical or pilot studies. Included studies followed a quantitative research design, excluding mixed-methods and qualitative approaches. Included endpoints were clinical outcomes (including patient-reported outcomes), efficiency metrics, patient satisfaction outcomes and/or cost analysis.
We used the following query to search MedLine via PubMed: (“Value-Based Health Insurance”[MeSH Terms] OR “value-based care”[Text Word] OR “value-based healthcare”[Text Word] OR “value-based health care”[Text Word] OR “valuebased care”[Text Word] OR “value-based care”[Text Word] OR “value-based healthcare”[Text Word] OR “value-based health care”[Text Word] OR “VBHC”[Text Word]) AND (2020:2024[pdat]).
Our query returned 1770 results. After screening 176 articles, we finally included 11 studies were included in the review. The results of our review are presented in Supplementary Table S1. According to our findings, the initial, quantitative evidence on VBHC in Europe demonstrates that adopting a value-based attitude to healthcare and implementing components of VBHC can, in fact, improve outcomes in both public and private settings, Interestingly, two of the 11 examples included large-scale initiatives in which both public and private providers participated, highlighting the potential of VBHC to drive value-based collaboration in European healthcare. Also, the studies focusing on VBHC in private centers demonstrated improvements not only in efficiency metrics such as overall length of stay (57) and increased productivity (57, 58), but also increased quality of life for patients (58), improved clinical outcomes (59), and improved perception of quality of care (60), underlining the potential of VBHC to ensure quality of care and patient-centeredness in outsourced and privatized services.
This literature review has several limitations. Firstly, the published studies may be subject to selection bias. The search query did not include specific search terms for each of the components of VBHC, and so we may have excluded some studies focusing on individual components of the value-based framework. Secondly, we only included studies during the last 5 years as the healthcare landscape has changed significantly since the COVID-19 pandemic. However, this approach may have excluded several reports. Finally, although we differentiated between VBHC in private and public healthcare, we did not identify any studies comparing outcomes of VBHC between public and outsourced services. Although our findings point to VBHC as a potential solution to the theoretical drawbacks of outsourcing, further research is necessary to confirm this hypothesis.
Discussion
This article summarizes several studies which analyze effects derived from healthcare outsourcing. A shared limitation is that these studies fail to mention the potential impact of alternative models of health-care delivery, such as value-based healthcare, on quality of care when choosing to outsource. This issue is probably caused by lack of available data at the time of publication. However, an increasing amount of evidence on the positive effects of value-based care on private and public healthcare has been published in recent years, and this data should be analyzed and considered as a new perspective on the current “public versus private” debate.
It has been claimed that, for private companies, reducing costs is easier than improving quality of care, but recent data suggest that implementing value-based healthcare leads to improved clinical outcomes, better patient experience, and more sustainable care – regardless of management type. Kaiser Permanente, a major US private health system with a value-based model of care delivery, has demonstrated better patient outcomes and lower use of resources than German Social Insurance hospitals operating on a traditional care model (61). Among countries with National Health Services, official data from the Regional Outcomes Observatory of Madrid (Spain) (62) show that four publicly owned hospitals outsourced to a value-based, for-profit healthcare provider and covering a population of close to 1 million patients present lower-than-average inpatient mortality and medical and surgical complications, as well as lower surgical backlogs and higher patient experience scores than their publicly managed counterparts.
Irrespectively of differing characteristics of national health systems regarding funding, payer and provider status, European healthcare is highly regulated by state and local government. Thus, government authorities have an important role in facilitating VBHC in privatized settings, for example, by designing contracting policies not only based on cost-effectiveness but also on clinical and patient-reported outcomes. Bundled payment or pay-for-performance can also incentivize private providers to improve quality of care. A typical argument against bundled payment in the privatized setting is the risk of “lemon dropping,” that is, avoiding patients whose social or health profile could influence outcomes negatively. However, in European healthcare, this scenario is highly mitigated by government regulation and medical ethics. In fact, yearly audit data from outsourced hospitals in Spain shows a higher-complexity case mix than publicly managed counterparts (62), while data from Germany show that public and privately run hospitals make similar losses from caring for uninsured patients (63).
While the use of PROMs and PREMs to motivate clinical decisions can give patients a voice in healthcare delivery, some concerns have been voiced regarding potential disparities. Socially disadvantaged groups are often less health-literate and may not participate equally in PROMs and PREMs programs (64). Breast cancer researchers observed that non-responders in a PROM program were more frequently of older age, non-English speaking, and non-white, pointing to the need for addressing the digital divide and language barriers in patient-reported data collection programs (65). Although risk selection could theoretically hamper the potential of VBHC (66), emerging evidence suggests that participation in value-based payment models reduces race and economic disparities (67, 68). Further studies are necessary to confirm the effects of VBHC on healthcare disparities in European countries.
In our opinion, European healthcare policy makers should bear in mind that the “public versus private” debate is not the only factor to consider when trying to solve the current discussion about which is the best healthcare system for our society. In fact, one of the advantages of the private sector is that changes occur faster, allowing new initiatives to be tested in a limited environment before being adopted by the public sector. In this sense, initial evidence from Europe points to the effectiveness of the value-based model of healthcare delivery (34). Meanwhile, preliminary data shows that outsourcing to providers with a value-based strategy may have advantages both in terms of profitability, health outcomes and patient experience compared to the traditional model and may represent an optimal form of contracting.
In conclusion, further research is necessary to fully elucidate the effects of different models of health-care delivery on quality of care when transitioning from public to private management. Furthermore, the progressive adoption of emerging health policies in European countries to encourage “value-based” decision-making represents an essential strategy that must be analyzed within a constructive debate on the impact and consequences of health-care outsourcing. In the meantime, we agree that “quantity over quality” is not an option when health-care outsourcing is concerned.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding authors.
Author contributions
CC: Conceptualization, Writing – original draft. JA: Supervision, Writing – review & editing. BP: Conceptualization, Writing – original draft. IC: Conceptualization, Writing – original draft. JAÁ: Supervision, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
All authors are employees of the Quirónsalud Healthcare Network and JA, JAÁ, and CC hold management roles at the company.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2024.1484709/full#supplementary-material
References
1. Gaeta, M, Campanella, F, Capasso, L, Schifino, GM, Gentile, L, Banfi, G, et al. An overview of different health indicators used in the European health systems. J Prev Med Hyg. (2017) 58:E114–20.
2. Tulchinsky, TH. Bismarck and the long road to universal health coverage. Case Stud Public Health. (2018) 131:8. doi: 10.1016/B978-0-12-804571-8.00031-7
3. Birault, F, Mignot, S, Caunes, N, Boutin, P, Bouquet, E, Pérault-Pochat, MC, et al. The characteristics of care provided to population(s) in precarious situations in 2015. A preliminary study on the universal health cover in France. Int J Environ Res Public Health. (2020) 17:3305. doi: 10.3390/ijerph17093305
4. Busse, R, Blümel, M, Knieps, F, and Bärnighausen, T. Statutory health insurance in Germany: a health system shaped by 135 years of solidarity, self-governance, and competition. Lancet. (2017) 390:882–97. doi: 10.1016/S0140-6736(17)31280-1
5. Kuipers, T, van de Pas, R, and Krumeich, A. Is the healthcare provision in the Netherlands compliant with universal health coverage based on the right to health? A narrative literature review. Glob Health. (2022) 18:1–11. doi: 10.1186/s12992-022-00831-7
6. Dimova, A, Rohova, M, Moutafova, E, Atanasova, E, Koeva, S, Panteli, D, et al. Bulgaria health system review. Health Syst Transit. (2012) 14:1–186.
7. Goodair, B. ‘Accident and emergency?’ Exploring the reasons for increased privatisation in England’s NHS. Health Policy. (2023) 138:104941. doi: 10.1016/J.HEALTHPOL.2023.104941
8. Tiemann, O, and Schreyögg, J. Effects of ownership on hospital efficiency in Germany. Bus Res. (2009) 2:115–45. doi: 10.1007/BF03342707
9. Klenk, T. Ownership change and the rise of a for-profit hospital industry in Germany. Policy Stud. (2011) 32:263–75. doi: 10.1080/01442872.2011.561694
10. Lorence, DP, and Spink, A. Healthcare information systems outsourcing. Int J Inf Manag. (2004) 24:131–45. doi: 10.1016/j.ijinfomgt.2003.12.011
11. Roberts, J, Henderson, J, Olive, L, and Obaka, D. A review of outsourcing of services in health care organizations. J Outsourc Organizat Informat Manag. (2013):1–10. doi: 10.5171/2013.985197
12. Augurzky, B, and Scheuer, M. Outsourcing in the German hospital sector. Serv Ind J. (2007) 27:263–77. doi: 10.1080/02642060701207080
14. Steinbeck, V, Fresemann, ML, and Busse, R. Value-based healthcare as an opportunity for patient management at the individual and system level. Inn Med (Heidelb) (2024). 890–8.
15. Würnschimmel, C, Maurer, T, Knipper, S, von Breunig, F, Zoellner, C, Thederan, I, et al. Martini-Klinik experience of prostate cancer surgery during the early phase of the COVID-19 pandemic. BJU Int. (2020) 126:252–5. doi: 10.1111/bju.15115
16. del Olmo, M, Córdoba, R, Gómez-Meana, Á, Herrero, A, Pascual, A, Cabello, Á, et al. Implementing a broad digital framework to drive network strategy through PROMs and PREMs. NEJM Catal Innov Care Deliv. (2023) 4:83. doi: 10.1056/CAT.23.0083
17. Short Apellaniz, J, Álvaro de la Parra, JA, Gomez-Meana, A, Carabias, L, Cordoba, R, Arcos, J, et al. Leveraging telemedicine to reduce ED overcrowding: the Quirónsalud virtual urgent care program. NEJM Catal Innov Care Deliv. (2023) 4:422. doi: 10.1056/CAT.22.0422
18. Álvaro de la Parra, JA, del Olmo Rodríguez, M, Caramés Sánchez, C, Blanco, Á, Pfang, B, Mayoralas-Alises, S, et al. Effect of an algorithm for automatic placing of standardised test order sets on low-value appointments and attendance rates at four Spanish teaching hospitals: an interrupted time series analysis. BMJ Open. (2024) 14:e081158. doi: 10.1136/bmjopen-2023-081158
19. del Olmo, M, Córdoba, R, Gómez-Meana, Á, Herrero, A, Pascual, A, Cabello, A, et al. The HOPE project: improving Cancer patient experience and clinical outcomes through an integrated practice unit and digital transformation. NEJM Catal. (2023) 4:414. doi: 10.1056/CAT.22.0414
20. Flores-Balado, Á, Castresana Méndez, C, Herrero González, A, Mesón Gutierrez, R, de las Casas Cámara, G, Vila Cordero, B, et al. Using artificial intelligence to reduce orthopedic surgical site infection surveillance workload: Algorithm design, validation, and implementation in 4 Spanish hospitals. Am. J. Infect. Control. (2023) 51:1225–1229. doi: 10.1016/J.AJIC.2023.04.165
21. Guadalajara, H, Lopez-Fernandez, O, León Arellano, M, Domínguez-Prieto, V, Caramés, C, and Garcia-Olmo, D. The Role of Shared Decision-Making in Personalised Medicine: Opening the Debate. Pharmac. (2022) 15:215. doi: 10.3390/PH15020215
22. Theunissen, L, Cremers, HP, Dekker, L, Janssen, H, Burg, M, Huijbers, E, et al. Implementing value-based health care principles in the full cycle of care: the pragmatic evolution of the Netherlands heart network. Circ Cardiovasc Qual Outcomes. (2023) 16:E009054. doi: 10.1161/CIRCOUTCOMES.122.009054
23. Wyffels, E, Beles, M, Baeyens, A, Croeckaert, K, de Potter, T, van Camp, G, et al. Same day discharge strategy by default in a tertiary catheterization Laboratory in Belgium: value based healthcare-change in practice. Health Policy. (2023) 132:104826. doi: 10.1016/J.HEALTHPOL.2023.104826
24. Kruse, FM, Stadhouders, NW, Adang, EM, Groenewoud, S, and Jeurissen, PPT. Do private hospitals outperform public hospitals regarding efficiency, accessibility, and quality of care in the European Union? A literature review. Int J Health Plann Manag. (2018) 33:e434–53. doi: 10.1002/hpm.2502
25. Bach-Mortensen, AM, and Barlow, J. Outsourced austerity or improved services? A systematic review and thematic synthesis of the experiences of social care providers and commissioners in quasi-markets. Soc Sci Med. (2021) 276:113844. doi: 10.1016/J.SOCSCIMED.2021.113844
26. Goodair, B, and Reeves, A. The effect of health-care privatisation on the quality of care. Lancet Public Health. (2024) 9:e199–206. doi: 10.1016/S2468-2667(24)00003-3
27. Goodair, B, and Reeves, A. Outsourcing health-care services to the private sector and treatable mortality rates in England, 2013-20: an observational study of NHS privatisation. Lancet Public Health. (2022) 7:e638–46. doi: 10.1016/S2468-2667(22)00133-5
28. Ribera, A, Ferreira-González, I, Cascant, P, Pons, JMV, and Permanyer-Miralda, G. Evaluation of risk-adjusted hospital mortality after coronary artery bypass graft surgery in the Catalan public healthcare system. Influence of hospital management type (ARCA study). Rev Esp Cardiol. (2006) 59:431–40. doi: 10.1016/S1885-5857(06)60791-3
29. Mosquera, PA, San Sebastian, M, Burström, B, Hurtig, AK, and Gustafsson, PE. Performing through privatization: an ecological natural experiment of the impact of the Swedish free choice reform on ambulatory care sensitive conditions. Front Public Health. (2021) 9:4998. doi: 10.3389/FPUBH.2021.504998
30. Beckman, A, and Anell, A. Changes in health care utilisation following a reform involving choice and privatisation in Swedish primary care: a five-year follow-up of GP-visits. BMC Health Serv Res. (2013) 13:452. doi: 10.1186/1472-6963-13-452
31. Gustafsson, PE, Fonseca-Rodríguez, O, Castel Feced, S, San Sebastián, M, Bastos, JL, and Mosquera, PA. A novel application of interrupted time series analysis to identify the impact of a primary health care reform on intersectional inequities in avoidable hospitalizations in the adult Swedish population. Soc Sci Med. (2024) 343:116589. doi: 10.1016/J.SOCSCIMED.2024.116589
32. Hebrang, A, Henigsberg, N, Erdeljic, V, Foro, S, Vidjak, V, Grga, A, et al. Privatization in the health care system of Croatia: effects on general practice accessibility. Health Policy Plan. (2003) 18:421–8. doi: 10.1093/heapol/czg050
33. Sackett, DL, and Rosenberg, WMC. The need for evidence-based medicine. J R Soc Med. (1995) 88:330–4.
34. Sackett, DL, Rosenberg, WMC, Gray, JAM, Haynes, RB, and Richardson, WS. Evidence based medicine: what it is and what it isn’t. BMJ. (1996) 312:71–2. doi: 10.1136/bmj.312.7023.71
35. Marzorati, C, and Pravettoni, G. Value as the key concept in the health care system: how it has influenced medical practice and clinical decision-making processes. J Multidiscip Healthc. (2017) 10:101–6. doi: 10.2147/JMDH.S122383
36. Teisberg, E, Wallace, S, and O’Hara, S. Defining and implementing value-based health care: a strategic framework. Acad Med. (2020) 95:682–5. doi: 10.1097/ACM.0000000000003122
37. Bele, S, Chugh, A, Mohamed, B, Teela, L, Haverman, L, and Santana, MJ. Patient-reported outcome measures in routine pediatric clinical care: a systematic review. Front Pediatr. (2020) 8:364. doi: 10.3389/FPED.2020.00364
38. Graupner, C, Kimman, ML, Mul, S, Slok, AHM, Claessens, D, Kleijnen, J, et al. Patient outcomes, patient experiences and process indicators associated with the routine use of patient-reported outcome measures (PROMs) in cancer care: a systematic review. Support Care Cancer. (2021) 29:573–93. doi: 10.1007/s00520-020-05695-4
39. Steinbeck, V, Langenberger, B, Schöner, L, Wittich, L, Klauser, W, Mayer, M, et al. Electronic patient-reported outcome monitoring to improve quality of life after joint replacement: secondary analysis of a randomized clinical trial. JAMA Netw Open. (2023) 6:E2331301. doi: 10.1001/jamanetworkopen.2023.31301
40. Wagenschieber, E, and Blunck, D. Impact of reimbursement systems on patient care – a systematic review of systematic reviews. Health Econ Rev. (2024) 14:22. doi: 10.1186/S13561-024-00487-6
41. Slawomirski, L, Hensher, M, Campbell, J, and deGraaff, B. Pay-for-performance and patient safety in acute care: a systematic review. Health Policy. (2024) 143:105051. doi: 10.1016/J.HEALTHPOL.2024.105051
42. Huang, J, Yin, S, Lin, Y, Jiang, Q, He, Y, and du, L. Impact of pay-for-performance on management of diabetes: a systematic review. J Evid Based Med. (2013) 6:173–84. doi: 10.1111/jebm.12052
43. Jia, L, Meng, Q, Scott, A, Yuan, B, and Zhang, L. Payment methods for healthcare providers working in outpatient healthcare settings. Cochrane Database Syst Rev. (2021) 2021:CD011865. doi: 10.1002/14651858.CD011865.PUB2
44. Langdown, C, and Peckham, S. The use of financial incentives to help improve health outcomes: is the quality and outcomes framework fit for purpose? A systematic review. J Public Health (Oxf). (2014) 36:251–8. doi: 10.1093/pubmed/fdt077
45. Sanchez, MA, Sanchez, S, Bouazzi, L, Peillard, L, Ohl-Hurtaud, A, and Quantin, C. Does the implementation of pay-for-performance indicators improve the quality of healthcare? First results in France. Front. Public Health. (2023) 11:3806. doi: 10.3389/FPUBH.2023.1063806
46. Low, LL, Tan, SY, Ng, MJM, Tay, WY, Ng, LB, Balasubramaniam, K, et al. Applying the integrated practice unit concept to a modified virtual Ward model of Care for Patients at highest risk of readmission: a randomized controlled trial. PLoS One. (2017) 12:e0168757. doi: 10.1371/JOURNAL.PONE.0168757
47. Borde, D, Agana-Norman, DFG, Leverence, R, Photos, L, Shuster, J, Lukose, K, et al. Outcomes of an integrated practice unit for vulnerable emergency department patients. BMC Health Serv Res. (2023) 23:1449. doi: 10.1186/S12913-023-10067-9
48. Williams, DV, Liu, TC, Zywiel, MG, Hoff, MK, Ward, L, Bozic, KJ, et al. Impact of an integrated practice unit on the value of musculoskeletal care for uninsured and underinsured patients. Healthc. (2019) 7:16–20. doi: 10.1016/j.hjdsi.2018.10.001
49. van Staalduinen, DJ, van den Bekerom, P, Groeneveld, S, Kidanemariam, M, Stiggelbout, AM, and van den Akker-van Marle, ME. The implementation of value-based healthcare: a scoping review. BMC Health Serv Res. (2022) 22:270. doi: 10.1186/S12913-022-07489-2
50. Islam, MK, Ruths, S, Jansen, K, Falck, R, Mölken, MRV, and Askildsen, JE. Evaluating an integrated care pathway for frail elderly patients in Norway using multi-criteria decision analysis. BMC Health Serv Res. (2021) 21:884. doi: 10.1186/S12913-021-06805-6
51. Bandurska, E, Ciećko, W, Olszewska-Karaban, M, Damps-Konstańska, I, Szalewska, D, Janowiak, P, et al. Value-based integrated care (VBIC) concept implementation in a real-world setting-problem-based analysis of barriers and challenges. Healthcare. (2023) 11:1110. doi: 10.3390/HEALTHCARE11081110
52. Bohler, F, Garden, A, Brock, C, and Bohler, L. Value-based healthcare payment models: a wolf in sheep’s clothing for patients and clinicians. Ann Med. (2024). 56:2948. doi: 10.1080/07853890.2024.2382948
53. Amini, M, Oemrawsingh, A, Verweij, LM, Lingsma, HF, Hazelzet, JA, Eijkenaar, F, et al. Facilitators and barriers for implementing patient-reported outcome measures in clinical care: an academic center’s initial experience. Health Policy. (2021) 125:1247–55. doi: 10.1016/j.healthpol.2021.07.001
54. Nguyen, H, Butow, P, Dhillon, H, and Sundaresan, P. A review of the barriers to using patient-reported outcomes (PROs) and patient-reported outcome measures (PROMs) in routine cancer care. J Med Radiat Sci. (2021) 68:186–95. doi: 10.1002/jmrs.421
55. Lewis, S. Value-based healthcare: is it the way forward? Future Healthc J. (2022) 9:211. doi: 10.7861/fhj.2022-0099
56. Cossio-Gil, Y, Omara, M, Watson, C, Casey, J, Chakhunashvili, A, Gutiérrez-San Miguel, M, et al. The roadmap for implementing value-based healthcare in European university hospitals—consensus report and recommendations. Value Health. (2022) 25:1148–56. doi: 10.1016/j.jval.2021.11.1355
57. Cecconi, M, Goretti, G, Pradella, A, Meroni, P, Pisarra, M, Torzilli, G, et al. Value-based preoperative assessment in a large academic hospital. J Anesth Analg Crit Care. (2024) 4:42. doi: 10.1186/S44158-024-00161-7
58. Goretti, G, Marinari, GM, Vanni, E, and Ferrari, C. Value-based healthcare and enhanced recovery after surgery implementation in a high-volume bariatric Center in Italy. Obes Surg. (2020) 30:2519–27. doi: 10.1007/s11695-020-04464-w
59. Van Dam, VS, Van Zijl, FVWJ, Kremer, B, and Datema, FR. The rhinoplasty healthcare monitor: an update on the practical and clinical benefits after 10 years of prospective outcome measurements. Facial Plast Surg. (2023) 40:539–45. doi: 10.1055/a-2218-7189
60. Van Veghel, D, Soliman-Hamad, M, Schulz, DN, Cost, B, Simmers, TA, Dekker, LRC, et al. Improving clinical outcomes and patient satisfaction among patients with coronary artery disease: an example of enhancing regional integration between a cardiac Centre and a referring hospital. BMC Health Serv Res. (2020) 20:1–8. doi: 10.1186/s12913-020-05352-w
61. Simon, B, Navarro, R, Reddy, NC, Convissar, JL, Rabrenovich, V, Paxton, E, et al. Patient pathway comparison for Total hip replacement in the United States and Germany — why the payment model matters. NEJM Catal. (2023) 4:456. doi: 10.1056/CAT.22.0456
62. Observatorio de resultados del Servicio Madrileño de Salud|Comunidad de Madrid. Available at: https://www.comunidad.madrid/servicios/salud/observatorio-resultados-servicio-madrileno-salud (accessed May 17, 2024).
63. Zimmer, M. Refusal of patients: care for people without health insurance in German emergency departments. BMC Med Ethics. (2024) 25:56. doi: 10.1186/S12910-024-01059-3
64. Shapiro, LM, Katz, P, Stern, BZ, and Kamal, RN. Equitable integration of patient-reported outcomes into clinical practice – opportunities, challenges, and a roadmap for implementation. J Am Acad Orthop Surg. (2024) 32:187–95. doi: 10.5435/JAAOS-D-23-00798
65. Srour, MK, Tadros, AB, Sevilimedu, V, Nelson, JA, Cracchiolo, JR, McCready, TM, et al. Who are we missing: does engagement in patient-reported outcome measures for breast Cancer vary by age, race, or disease stage? Ann Surg Oncol. (2022) 29:7964–73. doi: 10.1245/s10434-022-12477-1
66. Leao, DLL, Pavlova, M, and Groot, W. Risk selection reduces efficiency of value-based healthcare. Int J Health Plann Manag. (2023) 38:1088–96. doi: 10.1002/hpm.3648
67. Kilaru, AS, Liao, JM, Wang, E, Zhao, Y, Zhu, J, Ng, G, et al. Association between mandatory bundled payments and changes in socioeconomic disparities for joint replacement outcomes. Health Serv Res. (2024) 59:4369. doi: 10.1111/1475-6773.14369
Keywords: healthcare quality, outsourcing, value-based healthcare, patient outcomes, clinical management, patient experience
Citation: Caramés C, Arcos J, Pfang B, Cristóbal I and Álvaro de la Parra JA (2024) Value-based care as a solution to resolve the open debate on public healthcare outsourcing in Europe: What do the available data say? Front. Public Health. 12:1484709. doi: 10.3389/fpubh.2024.1484709
Edited by:
Alexandre Morais Nunes, University of Lisbon, PortugalReviewed by:
Le Khanh Ngan Nguyen, University of Strathclyde, United KingdomRicardo De Moraes E. Soares, Instituto Politécnico de Setúbal (IPS), Portugal
Copyright © 2024 Caramés, Arcos, Pfang, Cristóbal and Álvaro de la Parra. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Cristina Caramés, Y2NhcmFtZXNAcXVpcm9uc2FsdWQuZXM=; Ion CristóbalaW9uLmNyaXN0b2JhbEBxdWlyb25zYWx1ZC5lcw==
†ORCID: Cristina Caramés, https://orcid.org/0000-0002-5748-7628
Ion Cristóbal, https://orcid.org/0000-0003-0234-4213