 Rok Čivljak1,2†Karla Draženović3†
Rok Čivljak1,2†Karla Draženović3† Iva Butić1,4*
Iva Butić1,4* Marina Kljaković Gašpić Batinjan5Eva Huljev1Ninoslava Vicković1Ivan Krešimir Lizatović1Borna Grgić1
Marina Kljaković Gašpić Batinjan5Eva Huljev1Ninoslava Vicković1Ivan Krešimir Lizatović1Borna Grgić1 Ana Budimir2,5Andrea Janeš6
Ana Budimir2,5Andrea Janeš6 Ana Nikić Hecer7
Ana Nikić Hecer7 Tajana Filipec Kanižaj2,8
Tajana Filipec Kanižaj2,8 Vanja Tešić9,10
Vanja Tešić9,10 Mirjana Lana Kosanović Ličina9
Mirjana Lana Kosanović Ličina9 Karolina Dobrović11
Karolina Dobrović11- 1University Hospital for Infectious Diseases “Dr. Fran Mihaljević”, Zagreb, Croatia
- 2University of Zagreb School of Medicine, Zagreb, Croatia
- 3Tajana Janja Lovnički – Kontent, Family Medicine Practice, Zagreb, Croatia
- 4University of Zagreb School of Dental Medicine, Zagreb, Croatia
- 5University Hospital Centre Zagreb, Zagreb, Croatia
- 6University Hospital “Sveti Duh”, Zagreb, Croatia
- 7University Hospital Center Sestre Milosrdnice, Zagreb, Croatia
- 8University Hospital Merkur, Zagreb, Croatia
- 9Andrija Štampar Teaching Institute of Public Health, Zagreb, Croatia
- 10University of Rijeka School of Medicine, Rijeka, Croatia
- 11University Hospital Dubrava, Zagreb, Croatia
Introduction: Invasive pneumococcal disease (IPD) is a severe form of illness caused by Streptococcus pneumoniae with high morbidity and mortality rate in the general population, particularly in children <5 years of age, adults ≥65 years of age and the immunocompromised. As known, pneumococcal vaccination lowers the risk of IPD so the aim of this study was to investigate whether the introduction of pneumococcal vaccination has influenced the incidence and mortality of IPD in adults in Croatia.
Materials and methods: A retrospective study was conducted among adult patients (aged ≥18 years) hospitalized due to IPD in the metropolitan area of Zagreb from 1st January 2010 to 31st December 2022. Number of vaccine doses distributed were obtained from the healthcare system.
Results: During the study period, 389 patients were hospitalized, of whom 214 (55.5%) were male. The annual incidence of IPD ranged from 0.6 to 4.1/100,000 population. A total of 185 (47.6%) patients were ≥ 65 years of age and 309 (79.4%) were ≥ 50 years of age. In 331 (85.1%) of the patients, at least one risk factor was identified, with age ≥ 65 years being the most common. Bacteremic pneumonia was the most frequent clinical presentation of IPD (66.3%). Indication for vaccination had 249 patients (64%) but only 11 patients (4.4%) were vaccinated. Also, 64 patients (16.5%) died. Serotype was determined in 233 (59.9%) of the isolates, with serotype 3 being the most frequent (49, 21%), followed by serotype 14 (38, 16.3%) and 19A (15, 6.4%). A total of 180 isolates (77.3%) were included in the 13-valent conjugate vaccine, 208 (89.3%) in the 20-valent conjugate vaccine and 212 (91%) in the 23-valent pneumococcal polysaccharide vaccine.
Discussion: The introduction of pneumococcal vaccination has led to a significant decrease in the incidence and mortality of IPD in adults. To further reduce morbidity and mortality from IPD, it is necessary to increase vaccine coverage in adults, particularly in individuals with risk factors. It may be beneficial to lower the recommended vaccination age from ≥65 to ≥50 years as the substantial difference in the incidence rates of IPD between these age groups was noticed.
Introduction
Streptococcus pneumoniae causes two groups of diseases in humans: invasive and noninvasive. While the noninvasive forms of disease (sinusitis, otitis media and non-bacteremic pneumonia) are more common, the invasive forms (bacteremic pneumonia, meningitis and primary bacteremia) are more severe and in such cases, pneumococcus can be identified in primary sterile body fluids, such as blood, cerebrospinal fluid (CSF) or pleural effusion (1). In the general population, IPD contributes significantly to morbidity and mortality, especially in children <5 years of age, adults ≥65 years of age and the immunocompromised, therefore representing a significant public health problem. According to data from the Centers for Disease Control and Prevention in the United States, over 31,000 cases of IPD were reported in 2017, an incidence of 9.4/100,000 population, of whom over 3,500 (11.3%) persons died (2). In 2018, 24,663 confirmed cases of IPD were reported in the EU/EEA, corresponding to a crude notification rate of 6.4 /100,000 population (3). Primary bacteremia (with no recognizable source) is the most common manifestation of IPD, especially in children ≤2 years of age, who account for approximately 40% of IPD cases (2). In the adult population, bacteremia usually accompanies invasive pneumonia or meningitis. According to a retrospective study conducted at the University Hospital for Infectious Diseases “Dr. Fran Mihaljević” in Zagreb, 9.2% of the adult patients hospitalized for IPD in 2010–2013, prior to the introduction of mandatory vaccination of children, had isolated bacteremia, while 58% of the patients had pneumonia (4).
The incidence of IPD in the population depends on many factors: patient age, comorbidities, vaccination status, serotype, season and geographical location. Incidence is higher in the extreme age groups (children <2 years of age and adults ≥65 years of age), as well as persons with comorbidities (5, 6). In the early 2000s, a study was conducted in Croatia to assess the incidence of IPD in children. According to the results of that study, the annual incidence of IPD in children aged <2 is 36.8/100,000, in children from 2 to 5 years of age 16.3/100,000, and in those >5 years of age 2.9/100,000 (7). However, the incidence of laboratory confirmed IPD cases among Croatian adults during a fifteen-year period (2005–2019) was 1.92/100,000, 2.68/100,000, and 4.45/100,000 in 20–49 year olds, 50–64 year olds, and ≥ 65 year olds, respectively (8).
The incidence of IPD depends on the pneumococcal serotype and vaccination status. With the introduction of the 7-valent pneumococcal conjugate vaccine (PCV7) in the year 2002 and the 13-valent PCV13 in 2010 into the mandatory vaccination program for children in Canada, a decreased incidence in the incidence of pneumococcal serotypes contained in the PCV7 and PCV13 vaccines was observed and as well as an increased incidence in the pneumococcal serotypes contained in the 23-valent pneumococcal polysaccharide vaccine (PPSV23) vaccine and non-vaccine pneumococcal serotypes (9). There is a consistent increase in pneumococcal resistance to beta-lactam antibiotics and macrolides worldwide. In Europe, between 8.4 and 20.7% of clinical isolates are resistant to penicillin and between 14.7 and 17.1% to erythromycin (10).
According to data from 2022, penicillin resistance in Croatia was low (5%) but percentage of isolates susceptible, increased exposure to penicillin were high (18%). Resistance to macrolides is continuously very high for more than 20 years, being highest in 2008 (40%) and lowest in 2022 (24%) (11). The future increase in the antibiotic resistance and treatment of IPD caused by resistant pneumococcal strains is an additional argument for the introduction of pneumococcal vaccination in all age groups, including adults. With the use of conjugated and polysaccharide vaccination throughout the world, a decrease in the incidence of IPD, as well as decreased colonization of the nasopharynx, was recorded (12, 13).
The first pneumococcal vaccine was licensed in 1977, which was replaced in 1983 by the PPSV23 currently in use. Since the polysaccharide vaccine is not sufficiently immunogenic in persons <2 years of age, in the early 2000s a conjugate vaccine was introduced worldwide that also stimulates mucosal immunity. Mucosal immunity prevents the colonization of the nasopharynx and thereby reduces the percentage of carriers, having an impact on collective immunity (12, 13). The first conjugate vaccine, PCV7, was licensed in the United States in 2000. In 2010, it was replaced by the PCV13, which is currently in use (2). In 2022, a new 20-valent PCV was registered, which contains 20 polysaccharides of the most common pneumococcal serotypes (serotypes 1, 3, 4, 5, 6A, 6B, 7F, 8, 9 V, 10A, 11A, 12F, 14, 15B, 18C, 19A, 19F, 22F, 23F and 33F) (14). Until 2019, pneumococcal vaccination was recommended and available for some categories, all persons over 2 months of age with functional or anatomical asplenia, immunocompromised persons and immunocompetent persons with cochlear implants or conditions that lead to the CSF leak and infection. Polysaccharide vaccine was recommended for all persons over 2 years of age with functional or anatomical asplenia, immunocompromised persons and immunocompetent persons with chronic heart, lung, kidney or liver disease, diabetes mellitus, alcoholism, cochlear implant and conditions that lead to CSF leak and infection (15).
Since 2019, mandatory pneumococcal vaccination with PCV10 has been implemented in the Croatian National Immunization Program, but only for children <18 years of age (16). According to the Croatian Health Statistics Yearbook for 2023, primary pneumococcal vaccination coverage in children was 92.4% and revaccination coverage was 90.4% (17). In 2021, the Croatian Institute of Public Health revised the recommendations for the pneumococcal vaccination of the adult population. It is recommended for immunocompetent persons to receive only PPSV23, while immunocompromised and asplenic patients should additionally receive PCV13 (18). For now, there is neither data on the overall national vaccination coverage in adults not the impact of the introduction of vaccination against pneumococcal disease on adults in the Republic of Croatia. The aim of this study was to examine whether the introduction of nonmandatory pneumococcal vaccination until 2019 and the introduction of mandatory vaccination for children from 2019 affected the incidence and mortality of IPD in adults.
Materials and methods
A cohort retrospective study of adult patients hospitalized for IPD in all the hospitals of the metropolitan area of Zagreb from 1st January 2010, to 31st December 2022, was conducted. The analysis included all the adult patients ≥18 years of age whose disease was etiologically confirmed by the presence of S. pneumoniae in primary sterile body fluids. Neither persons younger than 18 years of age nor patients with evidence of pneumococci from nonsterile body fluids were included in the study. Demographic data (age, sex), epidemiological data and risk factors for IPD (excessive alcohol consumption, smoking, cardiovascular disease, diabetes, cerebrovascular diseases, respiratory diseases, autoimmune diseases, malignant diseases, immunodeficiency), data on vaccination status, clinical data and pneumococcal serotypes responsible for IPD were collected from hospital medical records.
Serotyping was done using the Quellung method (Statens Serum Institute, Denmark) (19). Antibiotic susceptibility testing was performed following the EUCAST standard. The antimicrobial susceptibility of S. pneumoniae strains was tested using the disk diffusion and gradient test methods. In the pneumococcal strains that were positive on the oxacillin screening disc, minimal inhibitory concentrations (MIC) for penicillin and ceftriaxone were determined using gradient test (E-test, Biomerieux, France). S. pneumoniae ATCC 49619 was used as a control strain (20).
The data on the number and types of vaccines used were obtained from the Dr. Andrija Štampar Teaching Institute for Public Health in Zagreb. Statistical analysis was performed using Fisher’s exact test to compare in which of the mentioned variables there are significant differences at the bivariate level (two tailed p-value <0.001). All the variables that had a significance level of p < 0.100 were entered in a binary logistic regression model for vaccination prediction. All the statistical procedures were performed using the IBM SPSS Statistics version 27.0.1.
The study was approved by the ethics committees of all the participating hospitals, as well as the ethics committee of the School of Medicine, University of Zagreb.
Results
During the study period, 389 patients with confirmed IPD were hospitalized in the metropolitan area of Zagreb. The annual incidences of IPD in adults during the 2010–2022 period are shown in Figure 1. The highest incidence was recorded in 2011 (4.1/100,000 population), and the lowest in 2022 (0.6/100,000 population). The total number of 214 (55.5%) patients were male. The distribution of the subjects according to age group is presented in Table 1. There were 185 (47.6%) persons in the age group of ≥65 years, and in the age group of ≥50 years there were 309 (79.4%). The median age was 63 years (range 25–105 years).
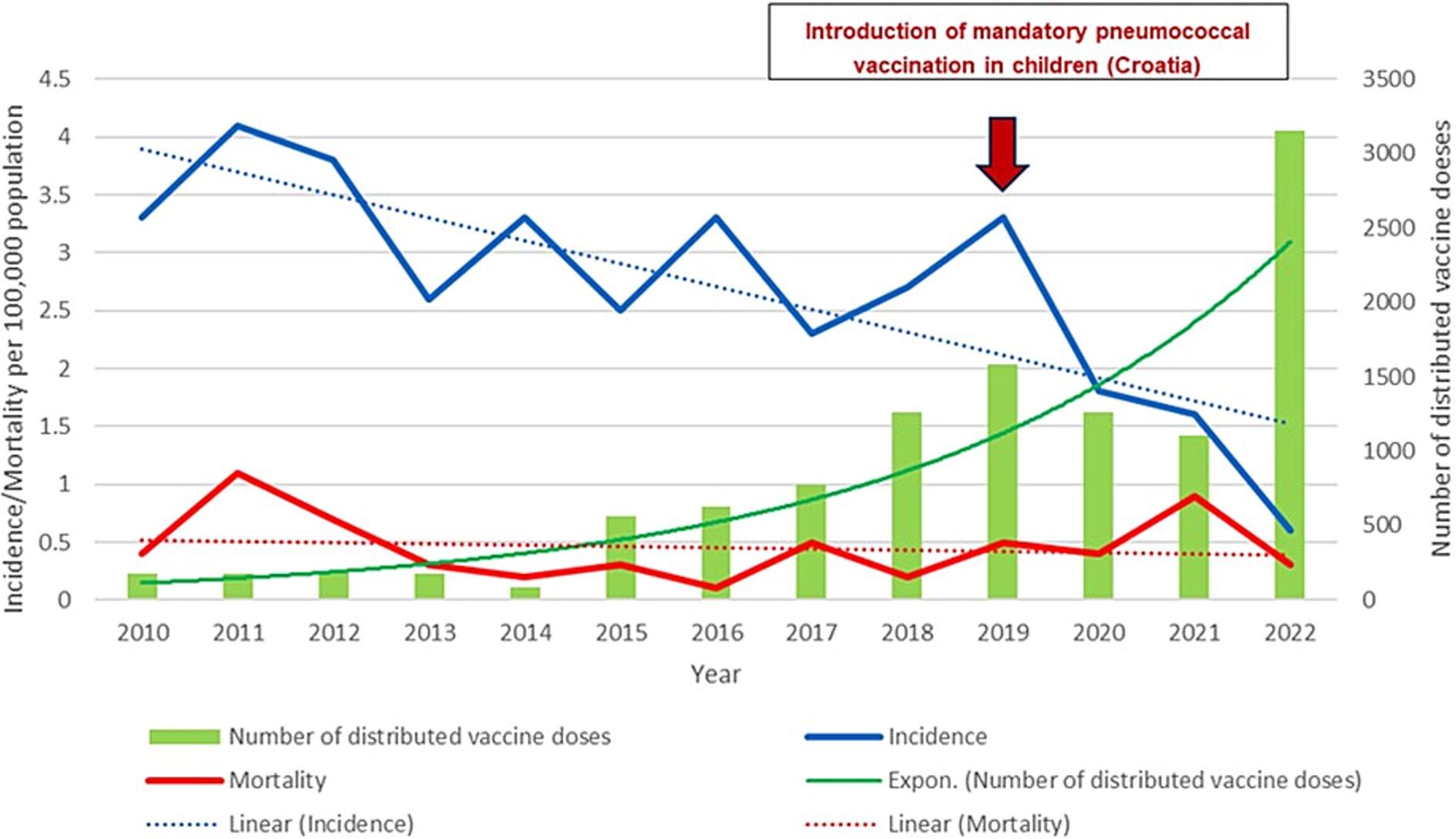
Figure 1. Graphic representation of the annual incidence and mortality of invasive pneumococcal diseases in adult patients in relation to the number of distributed pneumococcal vaccines in the metropolitan area of Zagreb (2010–2022); Linear (Incidence) – Incidence trend; Linear (Mortality) – Mortality trend.
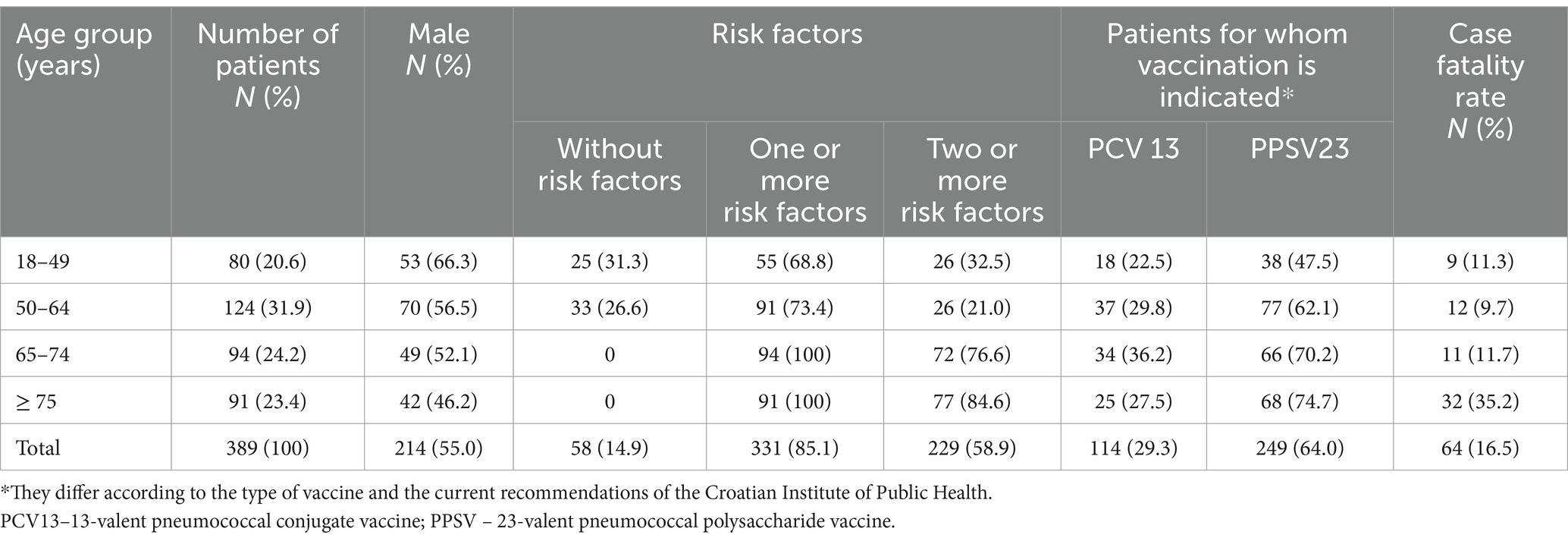
Table 1. Basic demographic, epidemiological and clinical data on patients.
Table 2. presents the patient distribution with regard to the presence of individual comorbidities and risk factors. No risk factor was identified in 58 (14.9%) of the patients, while at least one risk factor was identified in 331 patients (85.1%).
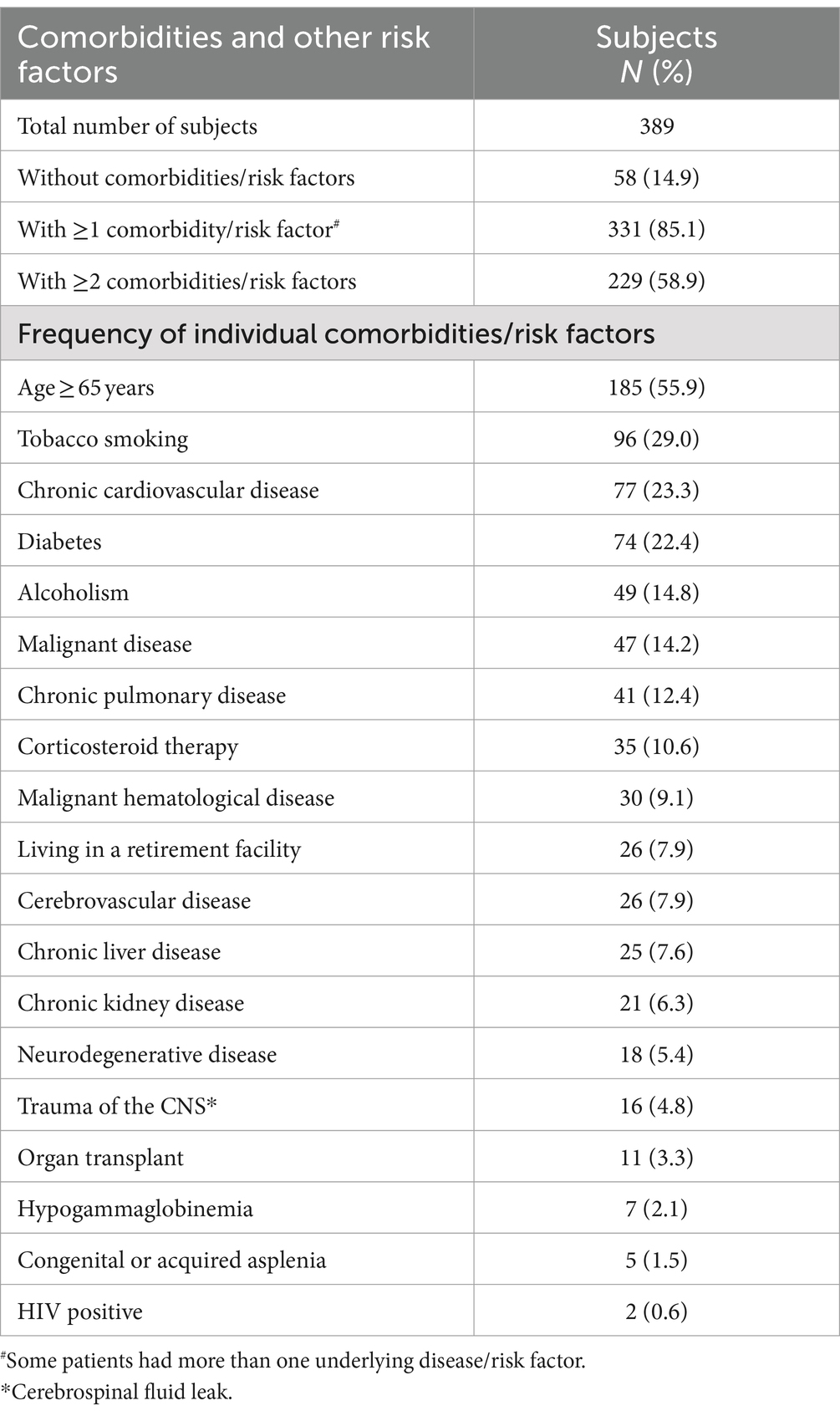
Table 2. Individual comorbidities and risk factors in adult patients hospitalized for invasive pneumococcal disease in the metropolitan area of Zagreb (2010–2022).
Data on the antibiotic susceptibility testing was available for 326 out of 389 strains (84% of all isolates). Resistance to penicillin was low, <1% (detected in only two of isolates with MIC 3.0 mg/L) while 17% of strains were penicillin susceptible, increased exposure. Susceptibility to ceftriaxone was high, 98% while three isolates were susceptible, increased exposure while three isolates were resistant to ceftriaxone. Resistance to macrolides was high, 24%.
With regard to the clinical presentation of the IPD, 258 (66.3%) had bacteremic pneumonia, 79 (20.3%) had meningitis and 52 (13.4%) had primary bacteremia. The average duration of IPD prior to hospitalization was four days (median 3, range 1–21 days). The patients with isolated bacteremia and those with meningitis were hospitalized on average on the third day of illness, while patients with pneumonia were hospitalized on average on the fourth day of illness. The average duration of hospitalization for patients with IPD was 19 (median 14, range 1–195) days; for patients with primary bacteremia 13.9 days, for patients with bacteremic pneumonia 14.8 days, while for patients with meningitis 33.8 days.
Empiric antimicrobial therapy during hospitalization was initiated with third-generation cephalosporins in 107 (27.5%) of the patients, co-amoxiclav in 48 (12.3%), penicillin in 19 (4.9%) and carbapenems in 11 (2.8%). Combination therapy was started in 204 (52.4%) patients. The most common therapy was combination of third-generation cephalosporin and azithromycin in 87 (22.4%) of the patients, followed by third-generation cephalosporin and vancomycin in 25 (6.4%) and a combination of third-generation cephalosporin and penicillin in 18 (4.6%) The average duration of antimicrobial therapy in patients with IPD was 15 (median 13, range 1–195) days. Due to the severity of IPD, 148 (38%) of the patients were treated in an intensive care unit, of whom 64 (24.8%) had pneumonia, 14 (31.1%) primary bacteremia and 70 (88.6%) had meningitis.
Three hundred twenty-five (83.5%) of the patients with IPD survived, and 64 (16.5%) died. There were 8/79 (10.1%) deaths among the patients with meningitis, 40/258 (15.5%) among the patients with pneumonia, and 16/52 (30.8%) among the patients with primary bacteremia. The largest number of patients hospitalized with IPD (45) was recorded in 2011, while the smallest number (6) was recorded in 2022. The largest number of deaths from IPD (12) was recorded in 2011, while the smallest number (1) was recorded in 2016. There was a decrease in the number of adult patients with IPD according to age, as well as a decrease in the number of deaths during the study period (Figure 1).
The etiological diagnosis of IPD was confirmed by a positive blood culture in 347 (85.1%) of the patients, positive culture from the CSF in 52 (13.4%) patients, positive PCR in the CSF in 38 (9.8%), and a positive culture from pleural effusions in 3 (0.8%) patients. The serotype was determined in 233 (59.9%) of the patients. The frequency of the individual serotypes is presented in Table 3. Of the pneumococcal serotypes confirmed as the causative agent of IPD, 180 (77.3%) were included in the PCV13, 212 (91%) in the PPSV23, and 208 (89.3%) in the 20-valent conjugate pneumococcal (PCV20) (Table 3). The percentages of the individual pneumococcal serotypes were not the same during the period studied. Figure 2 presents the percentages of isolated pneumococcal serotypes according to year. The serotypes are divided into non-vaccine serotypes (NVT), and serotypes contained in the PCV13 and PPSV23. The percentages of the serotypes included in the PCV13 and PPSV23 had a decreasing trend, while the percentages of NVT was unchanged. Table 4. presents the number of patients who died and in whom the pneumococcal serotype had been confirmed. The highest mortality was in patients in whom the serotype 19F (44.4%) and serotype 11A (33.3%) were isolated, followed by patients with the serotype 19A and 11A in whom mortality was 26.7 and 25%, respectively. Figure 1. presents the annual incidence and mortality of IPD in adults hospitalized in the metropolitan area of Zagreb (2010–2022) in relation to the number of people vaccinated with pneumococcal vaccine in said territory during the study period.

Table 3. Distribution of individual serotypes of isolated Streptococcus pneumoniae in patients with IPD (according to frequency and representation in the PCV13, PPSV23 and PCV20 vaccines).
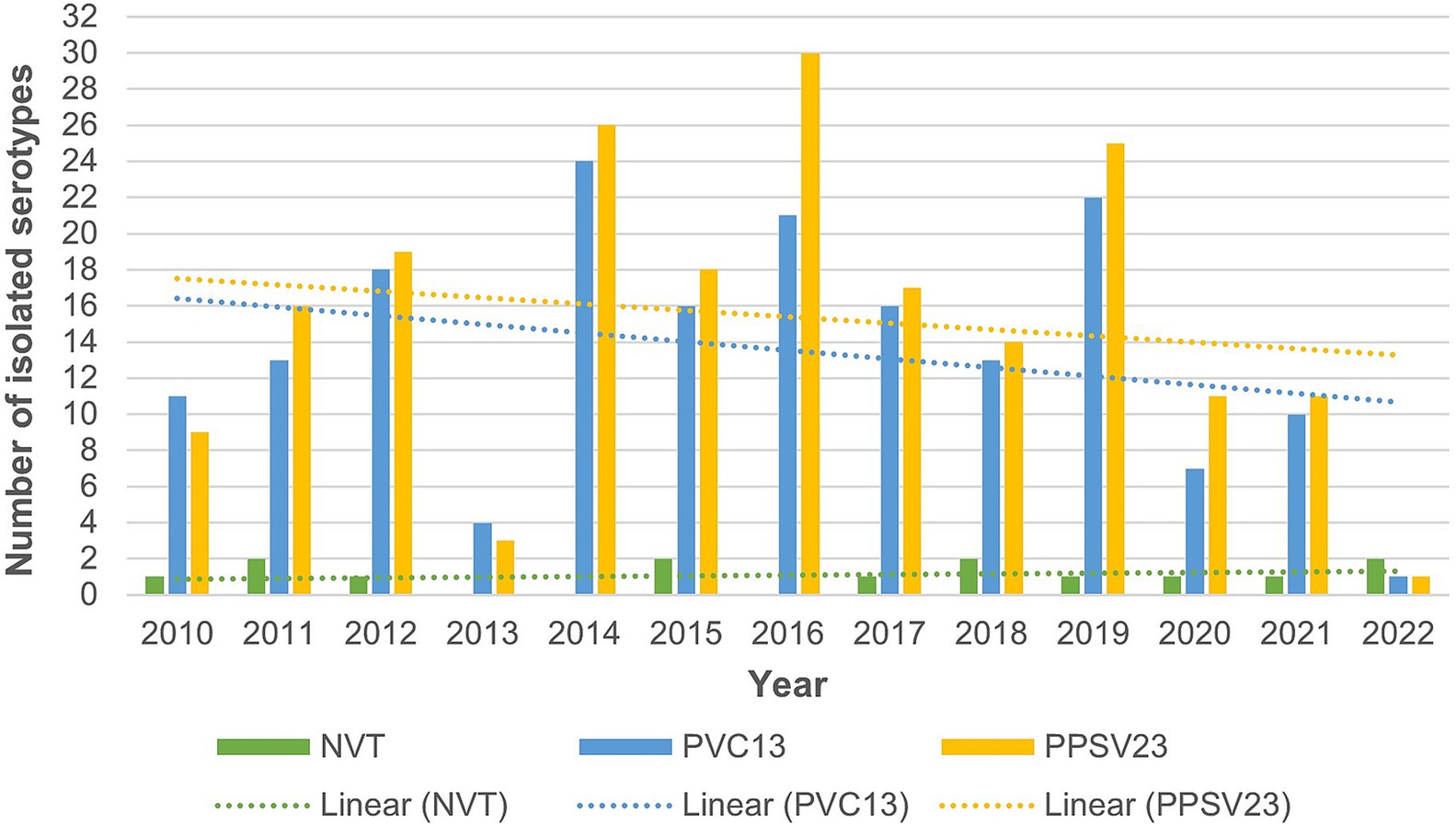
Figure 2. Graphic representation of the distribution of isolated serotypes of pneumococci in adult patients hospitalized due to invasive pneumococcal disease in the metropolitan area of Zagreb according to year (NVT – non-vaccine serotype; PVC13–13-valent pneumococcal conjugate vaccines; PPSV23–23-valent pneumococcal polysaccharide vaccine).
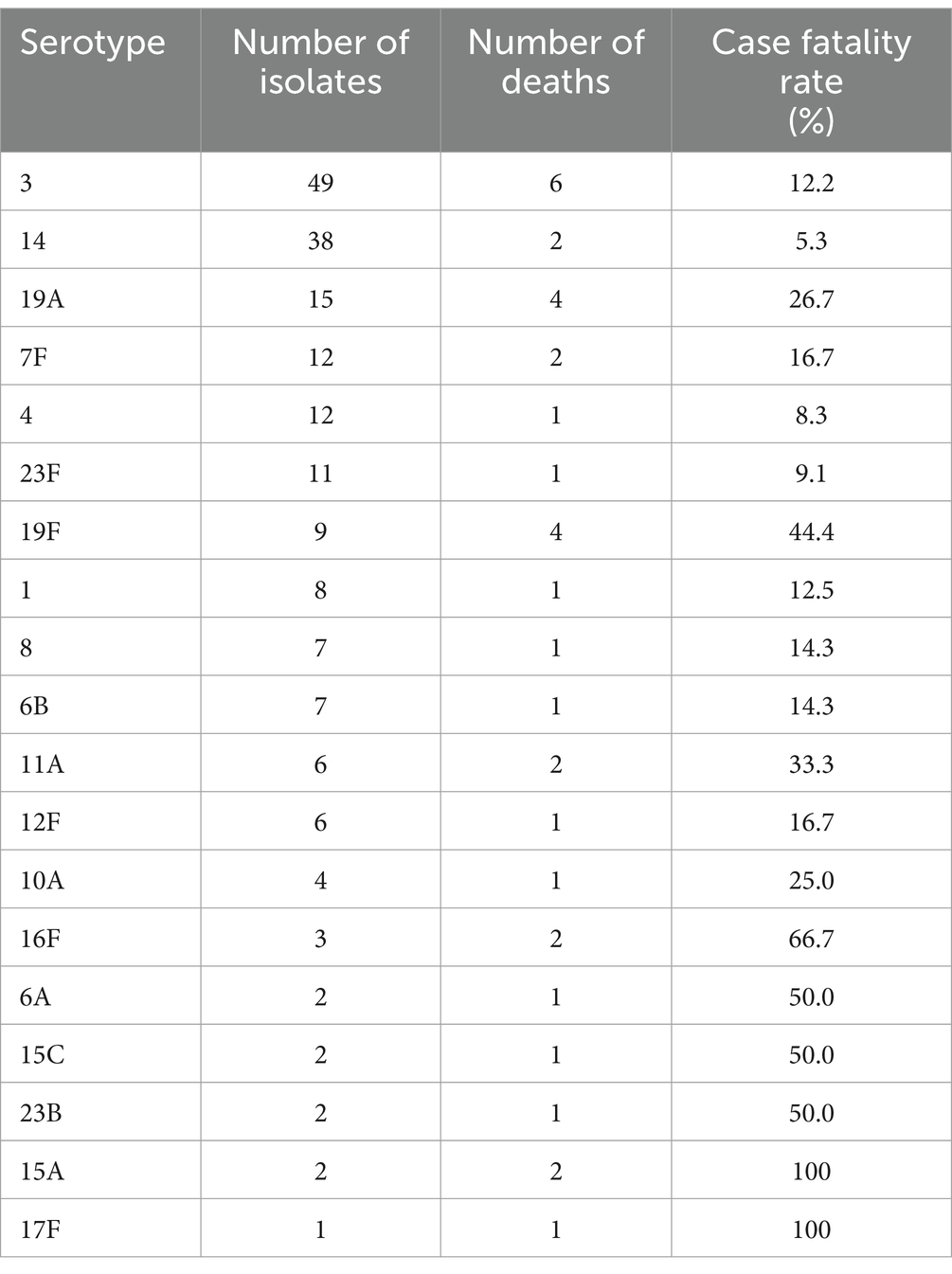
Table 4. Distribution of fatal outcomes in patients with invasive pneumococcal disease according to the confirmed serotypes of the Streptococcus pneumoniae isolates.
Of the 389 patients hospitalized for IPD, 249 (64%) had an indication for pneumococcal vaccination, although only 11 (4.4%) were vaccinated (Table 1).
The polysaccharide vaccine was predominant and the largest number of persons vaccinated, 3,151 (2,910 with PPSV23 vaccine and 241 with PCV13 vaccine) was recorded in the year 2022. Table 5 shows differences in the comorbidities and risk factors among patients hospitalized for invasive pneumococcal disease in the metropolitan area of Zagreb (2010–2022) regarding their pneumococcal vaccination status. Using Fisher’s exact test to detect any significant differences among the variables at the bivariate level, variables whose p value was less than 0.100 were used in a binary logistic model to predict of belonging to the group of patients who were vaccinated against pneumococci (Table 6). This regression model is statistically significant (p < 0.001) and explains 26.6% of the variance of the dependent variable (vaccination) and correctly classifies 97.4% of the respondents. Statistically significant higher vaccination coverage was shown in a group of patients with hypogammaglobulinemia (OR 15.42; 95% CI 1.70–139.73), congenital or acquired asplenia (OR 76.32; 95% CI 9.45–616.37) and CNS trauma (OR 10.29; 95% CI 1.83–57.76).
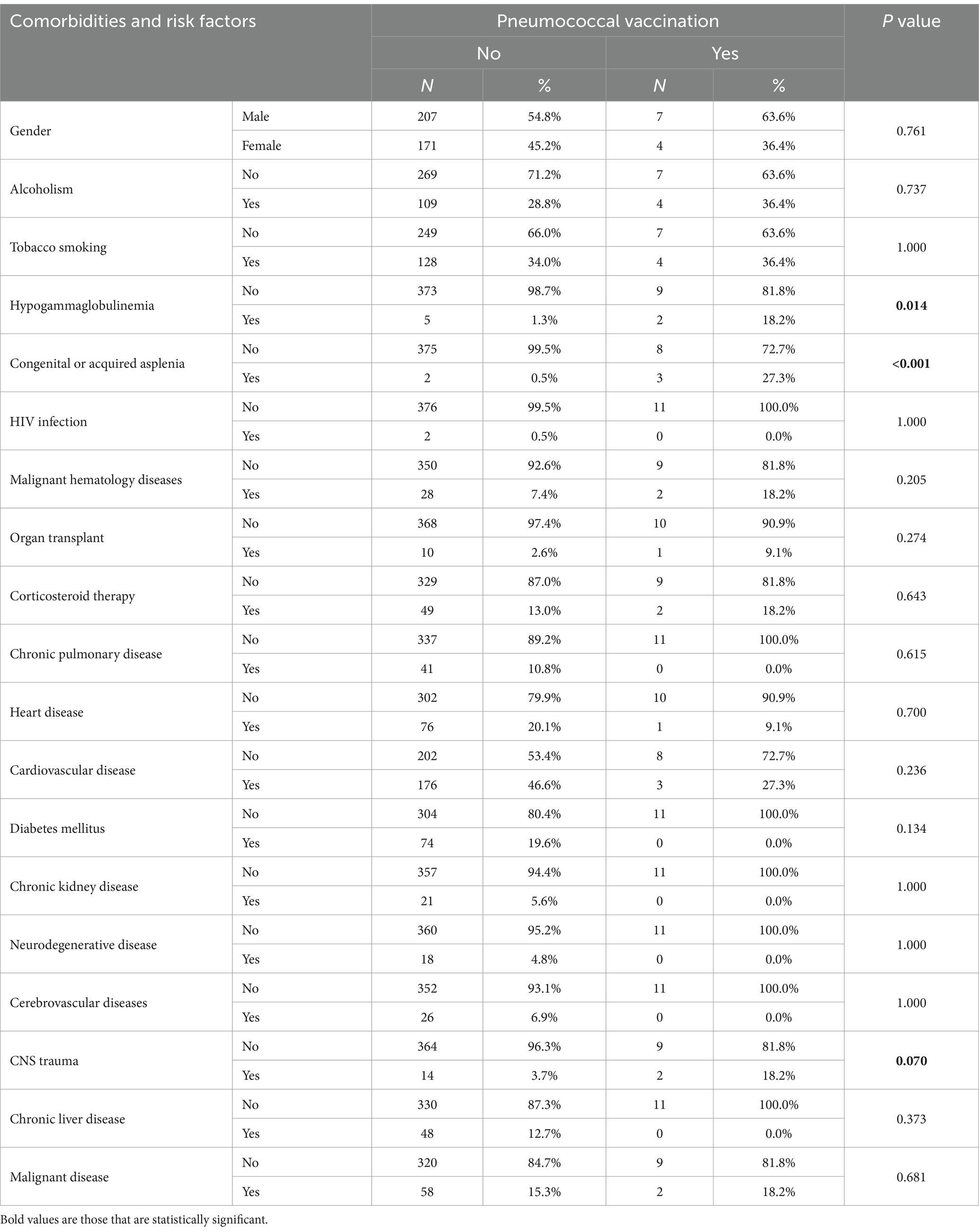
Table 5. Differences in comorbidities and risk factors among hospitalized patients for invasive pneumococcal disease in the metropolitan area of Zagreb (2010–2022) regarding their pneumoccocal vaccination status.
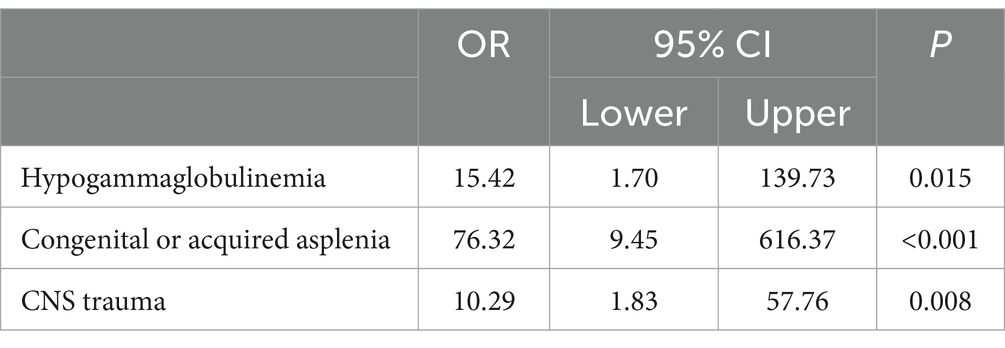
Table 6. Binary logistic regression model of pneumococcal vaccination prediction.
Discussion
The results of the study demonstrate that the incidence of IPD in the metropolitan area of Zagreb during the study period decreased from 4.1/100,000 population in 2011 to 0.6/100,000 population in 2022. Since 2019 more significant decline in number of IPD was observed what can be explained with introduction of mandatory pneumococcal vaccination into the childhood immunization program (16). Also, during COVID-19 pandemic decrease of IPD was observed in Croatia as reported in other European countries (11). The introduction of the mandatory pneumococcal vaccination of children led to a decrease in the incidence of IPD in other European countries and elsewhere (12, 21). Moreover, the greater vaccination of children resulted in a decrease in the incidence of IPD in the general population (22, 23).
In addition, there was greater vaccination coverage among adults in the period from 2010 to 2022. One of the reasons for the increase in pneumococcal vaccination rates may be the campaign React and Prevent, which was launched in Croatia, with the aim of educating the public about pneumococcal vaccination (24). Generally, developed nations, including the UK, Canada, France, and Germany, have started recommending PCV20 (25–28) However, during the study period PCV20 was not available in Croatia.
Several interventions were associated with increased pneumococcal vaccination coverage in adults, with prioritization of vaccination schemes, primary care interventions and awareness campaigns being the most effective (29). The results of several studies concluded that combining interventions was found to be more successful, but barriers and interventions could vary for certain population subgroups which should be take into account while tailoring programs (30).
Our results demonstrate that during the period studied, the number of deaths due to IPD decreased (from 12 in 2011 to 3 in 2022) as well as mortality (from 0.4/100,000 population in 2010 to 0.3/100,000 population in 2022). A study conducted in Denmark also showed a reduction in mortality (from 3.4/100,000 population prior to the introduction of PCV to 2.4/100,000 after the introduction of PCV13), especially among the unvaccinated population (22). Age is one of the known risk factors for IPD. This study only included adult patients (≥ 18 years of age) but not children, in whose age group the incidence of IPD is also high, especially those under 5 years of age (7). Among our patients, 47.6% were ≥ 65 years of age, but as many as 79.4% were ≥ 50 years of age. This demonstrates that persons younger than 65 years of age also belong to the risk population, due to which perhaps the recommended age for the vaccination of adults should be lowered from 65 to 50 years of age (31–34).
The majority of the subjects (85.1%) had at least one risk factor for developing IPD, while as many as 58.9% had two or more. The highest number of patients with confirmed risk factors were ≥ 65 years of age. A similar finding was recorded in a study conducted in Columbia, where 80.5% of the patients had at least one risk factor, while 37.3% had two or more. Furthermore, the largest number of patients with confirmed risk factors were ≥ 65 years of age (31). In a study conducted in Croatia in 2013, 68.9% of the patients had at least one risk factor (4). Among our study subjects, 64% had indications for pneumococcal vaccination, although only 4.4% were vaccinated. According to the current recommendations of the Croatian Institute of Public Health, among our subjects 64% of the patients had indications for the PPSV23 vaccine and 29.3% for the PCV13. The vaccination of subjects with indications for vaccination against pneumococcal disease varies among countries. According to the results of a study involving nine European countries, including Croatia, the highest pneumococcal vaccination rate (30.5%) was in Spain and the lowest (0.7%) was in Croatia (6). Subjects ≥4 years of age were included in the study. The vaccination rate in the United States is 23.3% among those 19–64 years of age with increased risk for IPD, while there is a somewhat higher (69%) pneumococcal vaccination rate in those ≥65 years of age (35).
Death occurred in 16.5% of the patients: 10.1% among patients with meningitis, 15.5% among patients with bacteremic pneumonia and 30.8% in patients with primary bacteremia. By comparison, in a study conducted in Sweden, death occurred in 9.9% of the participants: 13% among patients with meningitis, 8.3% among patients with pneumonia and 21% among patients with primary bacteremia (36). The most common serotype was serotype 3 detected in 21% of the patients followed by serotype 14 (16.3%) and serotype 19A (6.4%). Among the serotypes detected, 77.3% belonged to the serotypes covered by the PCV13 vaccine, 89.3% were covered by the PCV20 vaccine and 91% by the PPSV23 vaccine. These results demonstrate that the pneumococcal serotypes that caused disease in our patients are well covered by the available vaccines.
In numerous studies, it was stated that the introduction of the PCV7, and later also PCV13, led to a decrease in the number of serotypes covered by the vaccines used but also to an increase in IPD due to NVT. Therefore, there is a need for the constant development of new vaccines that will cover as many pneumococcal serotypes as possible (6, 12, 37). Since 2022 new PCV20 vaccine was available in Croatia. This vaccine contains the pneumococcal serotypes in the PCV13 vaccine plus an additional seven serotypes. Of the 233 pneumococcal isolates serotyped in our study, as many as 89.3% belong to the serotypes contained in the PCV20 vaccine, which would mean that the use of this vaccine in the Republic of Croatia could prevent a large percentage of IPD in adult patients. According to the Centers for Disease Control and Prevention, the PCV20 vaccine is currently recommended for children <5 years of age, adults ≥65 years of age as well as adults 19–64 years of age who have a risk factor (38). If the PCV20 vaccine is administered, neither prior administration of the PPSV23 vaccine nor a booster is needed. As previously mentioned, according to the latest the Centers for Disease Control and Prevention guidelines, vaccination with only the PCV20 vaccine is recommended (38). In Denmark, a study was conducted to compare the benefits of the PCV20 vaccine with those of the PPSV23 vaccine. According to the study results, approximately 75% of the strains are covered by the PPSV23 vaccine, while 65% are covered by the PCV20 vaccine. Through further analysis, they concluded that the administration of the PCV20 vaccine, together with the PPSV23 vaccine or alone, leads to a decreased incidence of IPD and reduced mortality. Moreover, the inclusion of PCV20 vaccine instead of PPSV23 in the National Vaccination Program will also lower the costs (39). Nowadays, more than 100 pneumococcal serotypes have been described, of which 8–10 serotypes are the most common causes of pneumococcal diseases in humans (2). In our study, it was possible to determine the serotype in 59.9% of the isolates with serotypes 3, 14, 19A and 9 V being the most common. In a study conducted during 2010–2013, the serotypes most represented were 3, 1, 19A and 6B (4). In a study conducted among children in Croatia, the most frequently represented serotypes were 14, 6B, 18C and 23F (7). According to other studies, these serotypes are given as the most common in adults and children. All these serotypes are included in all three pneumococcal vaccines for adults (PCV13, PCV20 and PPSV23) currently available in Croatia. The pneumococcal serotype can also affect mortality. In a study conducted in Switzerland, it was demonstrated that mortality from IPD is greater if the infection is caused by the serotypes 3, 19A or 19F (5). In our study, mortality among the most common serotypes 3, 14 and 19A was 12.2, 5.3 and 26.7%, respectively, while serotype 19F had high mortality of 44.4% (4 out 9 patients). In some countries, there has been an increase in the incidence of IPD caused by NVT following the introduction of PCV vaccine in the mandatory children’s vaccination programs (9, 37). According to our research, during the study period there was no increase in the NVT among the causes of IPD in Croatia.
Antibiotic resistance in Streptococcus pneumoniae, mainly to penicillin, macrolides and recently flouroquinolones, is recognized as a global health problem. The Croatian network of microbiological laboratories has a tradition of over 25 years in the antibiotic resistance surveillance of the most important human pathogens including Streptococcus pneumoniae. Based on our national data, resistance to macrolides and penicillin non-wild type has decreasing trends since 2019 (11). Our study confirms that the main problem regarding resistance in Croatia is high resistance to macrolides and the high percentage of penicillin non-wild type isolates but resistance to penicillin is continuously very low. Therefore, macrolides are not suitable for the treatment of pneumococcal infections in Croatia while amoxicillin is identified as the best choice, which is in line with the European and Croatian guidelines (40, 41).
This study has several limitations. It includes only participants from the metropolitan area of Zagreb, although it covers almost one fourth of the total population of Croatia. Only adult subjects are included in the study, although in order to speak more clearly about the effects of the introduction of mandatory pneumococcal vaccination it would be necessary to include subjects <18 years of age, for whom mandatory pneumococcal vaccination has already been introduced. Due to the facts that pneumococcal conjugate vaccine was introduced in to the Croatian national childhood immunization program in 2019 and our study period included the COVID-19 pandemic period when the incidence of IPD was low, our study did not show a post-vaccinal increase of IPD caused by NVT due to the short follow up period. Therefore, longer monitoring of IPD and serotypes is need for to drawing more thorough conclusions.
In conclusion, the introduction of pneumococcal vaccination led to a decrease in the incidence and mortality from IPD in adults. In order to achieve a further decrease in morbidity and mortality from IPD, it is necessary to increase vaccination coverage among adults, especially in persons with risk factors and also lower the recommended age for vaccination from the existing 65 to 50 years of age. Therefore, prioritization of vaccination schemes, primary care interventions, awareness campaigns and combinations with other preventive interventions are needed to achieve this goal. It is necessary to continue this study and in the coming period analyze the effects of the mandatory vaccination of children on the adult population and the effects of the recommendations for the pneumococcal vaccination of adults.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by the University Hospital for Infectious Diseases “Dr. Fran Mihaljević”, University Hospital Centre Zagreb, University Hospital Merkur, University Hospital “Sveti Duh”, University Hospital Dubrava, University Hospital Center Sestre Milosrdnice, as well as the ethics committee of the University of Zagreb School of Medicine. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
RČ: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Supervision, KDr: Writing – original draft, Conceptualization, Investigation, Methodology, Data curation, Formal analysis, Supervision, Validation, Visualization, Writing – review & editing. Validation, Visualization, Writing – original draft, Writing – review & editing, Project administration. IB: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing, Project administration, Resources. MKGB: Data curation, Formal analysis, Methodology, Writing – original draft. EH: Data curation, Formal analysis, Methodology, Writing – original draft. NV: Data curation, Formal analysis, Methodology, Writing – original draft. IKL: Data curation, Formal analysis, Methodology, Writing – original draft. BG: Data curation, Formal analysis, Methodology, Writing – original draft. AB: Data curation, Formal analysis, Methodology, Writing – original draft. AJ: Data curation, Formal analysis, Methodology, Writing – original draft. ANH: Data curation, Formal analysis, Methodology, Writing – original draft. TFK: Data curation, Formal analysis, Methodology, Writing – original draft. VT: Data curation, Formal analysis, Methodology, Writing – original draft. MLKL: Data curation, Formal analysis, Methodology, Writing – original draft. KDo: Data curation, Formal analysis, Methodology, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Weycker, D, Strutton, D, Edelsberg, J, Sato, R, and Jackson, LA. Clinical and economic burden of pneumococcal disease in older US adults. Vaccine. (2010) 28:4955–60. doi: 10.1016/j.vaccine.2010.05.030
2. Centers for Disease Control and Prevention . Active Bacterial Core Surveillance (ABCs) Report Emerging Infections Program Network: Streptococcus pneumoniae, 2017. (2019). Available at: https://stacks.cdc.gov/view/cdc/78826 [Accessed July 15, 2024].
3. European Centre for Disease Prevention and Control . Stockholm: ECDC; (2020). Invasive pneumococcal disease - Annual epidemiological report for 2018. Available at: https://www.ecdc.europa.eu/en/publications-data/invasive-pneumococcal-disease-annual-epidemiological-report-2018 (Accessed September 8, 2020).
4. Turalija, I, Kljakovic Gaspic, M, Civljak, R, Kuzman, I, Butic, I, Tambic Andrasevic, A, et al. Invasive pneumococcal disease in adults before the introduction of mandatory vaccination in Croatia: a retrospective study, 2010 - 2013. CROCMID 2013: Proceedings of the 10th Croatian Congress of Clinical Microbiology and the 7th Croatian Congress on Infectious Diseases with international participation; 2013 October 24–27; Rovinj, Croatia. Zagreb: Croatian Medical Association. p. 238–239.
5. Meichtry, J, Born, R, Küffer, M, Zwahlen, M, Albrich, WC, Brugger, SD, et al. Serotype epidemiology of invasive pneumococcal disease in Swiss adults: a nationwide population-based study. Vaccine. (2014) 32:5185–91. doi: 10.1016/j.vaccine.2014.07.060
6. Yahiaoui, RY, Bootsma, HJ, den Heijer, CDJ, Pluister, GN, John Paget, W, Spreeuwenberg, P, et al. Distribution of serotypes and patterns of antimicrobial resistance among commensal Streptococcus pneumoniae in nine European countries. BMC Infect Dis. (2018) 18:440. doi: 10.1186/s12879-018-3341-0
7. Guzvinec, M, Tesovic, G, Tambic-Andrasevic, A, Zidovec-Lepej, S, Vukic, BT, and Begovac, J. The epidemiology of invasive Streptococcus pneumoniae disease in Croatian children. Med Sci Monit. (2008) 14:PH59–64.
8. Butić, I, Gužvinec, M, Jelić, M, Groš, I, Lucić, S, Bošnjak, M, et al. Working Group for Invasive Isolates of the Croatian Committee for Antibiotic Resistance Surveillance. Serotype distribution and antimicrobial resistance of invasive Streptococcus pneumoniae isolates among Croatian adults during a fifteen-year period (2005–2019). Croat Med J. (2022) 63:156–65. doi: 10.3325/cmj.2022.63.156
9. Nasreen, S, Wang, J, Kwong, JC, Crowcroft, NS, Sadarangani, M, Wilson, SE, et al. Population-based incidence of invasive pneumococcal disease in children and adults in Ontario and British Columbia, 2002-2018: a Canadian immunization research network (CIRN) study. Vaccine. (2021) 39:7545–53. doi: 10.1016/j.vaccine.2021.11.032
10. Torres, A, Blasi, F, Peetermans, WE, Viegi, G, and Welte, T. The aetiology and antibiotic management of community-acquired pneumonia in adults in Europe: a literature review. Eur J Clin Microbiol Infect Dis. (2014) 33:1065–79. doi: 10.1007/s10096-014-2067-1
11. Tambic Andrasevic, A, Lj, Z, Obrovac, M, Hunjak, B, Babic-Erceg, A, Unukic, T, et al. Antibiotic resistance in Croatia, 2022. Zagreb: Croatian Academy of Medical Sciences (2022).
12. Chapman, KE, Wilson, D, and Gorton, R. Serotype dynamics of invasive pneumococcal disease post-PCV7 and pre-PCV13 introduction in north East England. Epidemiol Infect. (2013) 141:344–52. doi: 10.1017/S0950268812000763
13. Bogaert, D, De Groot, R, and Hermans, PW. Streptococcus pneumoniae colonisation: the key to pneumococcal disease. Lancet Infect Dis. (2004) 4:144–54. doi: 10.1016/S1473-3099(04)00938-7
14. European medicines agency . Prevenar 20 (previously Apexxnar). (2022). Available at: https://www.ema.europa.eu/en/medicines/human/EPAR/apexxnar [Accessed April 26, 2024].
15. Hrvatski zavod za javno zdravstvo . Program cijepljenja u Hrvatskoj u 2017. godini (2017). Available at: https://www.hzjz.hr/sluzba-epidemiologija-zarazne-bolesti/program-cijepljenja-u-hrvatskoj-u-2017-godini/ [Accessed May 5, 2024].
16. Hrvatski zavod za javno zdravstvo. Trogodišnji program obaveznog cijepljenja u Republici Hrvatskoj od 2019. do 2021. godine (Program 1). (2018). Available at: https://www.hzjz.hr/wp-content/uploads/2018/07/TROGODI%C5%A0NJI-PROGRAM-OBVEZNOG-CIJEPLJENJA.pdf [Accessed May 5, 2024].
17. Croatian Institute for Public Health . Croatian Health Statistics Yearbook 2022. R Stevanović, K Capak, and T Benjak, editors. (2023). https://www.hzjz.hr/wp-content/uploads/2024/03/HZSLj-2022.pdf.
18. Hrvatski zavod za javno zdravstvo . Zagreb: HZJZ; c2021. Preporuke za cijepljenje odraslih osoba protiv pneumokoka; (2021). Available at: https://www.hzjz.hr/sluzba-epidemiologija-zarazne-bolesti/preporuke-za-cijepljenje-odraslih-osoba-protiv-pneumokoka//
19. Habib, M, Porter, BD, and Satzke, C. Capsular serotyping of Streptococcus pneumoniae using the Quellung reaction. J Vis Exp JoVE. (2014). doi: 10.3791/51208-v
20. The European Committee on Antimicrobial Susceptibility Testing - EUCAST Available at: https://www.eucast.org/ [Accessed May 15, 2024].
21. Rodrigo, C, Bewick, T, Sheppard, C, Greenwood, S, Mckeever, TM, Trotter, CL, et al. Impact of infant 13-valent pneumococcal conjugate vaccine on serotypes in adult pneumonia. Eur Respir J. (2015) 45:1632–41. doi: 10.1183/09031936.00183614
22. Harboe, ZB, Dalby, T, Weinberger, DM, Benfield, T, Mølbak, K, Slotved, HC, et al. Impact of 13-valent pneumococcal conjugate vaccination in invasive pneumococcal disease incidence and mortality. Clin Infect Dis. (2014) 59:1066–73. doi: 10.1093/cid/ciu524 [Accessed May 5, 2024].
23. HSE Health Protection Surveillance Centre . Dublin: HSE HPSC; (2024). Streptococcus pneumoniae (invasive) in Ireland, 2023; 2024. Available at: https://www.hpsc.ie/a-z/vaccinepreventable/pneumococcaldisease/epidemiologicaldata/annualreportsoninvasivepneumococcaldisease/Streptococcus%20Pneumoniae%20(invasive)%20in%20Ireland,%202023.pdf
24. Nastavak kampanje “Reagiram i preveniram” u borbi protiv pneumokokne bolesti. Medix (2023);29:34.
25. Kobayashi, M, Pilishvili, T, Farrar, JL, Leidner, AJ, Gierke, R, Prasad, N, et al. Pneumococcal vaccine for adults aged ≥19 years: recommendations of the advisory committee on immunization practices, United States, 2023. MMWR Recomm Rep. (2023) 72:1–39. doi: 10.15585/mmwr.rr7203a1
26. Joint Committee on Vaccination and Immunisation . (2024). Minute of the meeting held on 07 June 2023. Available at: https://app.box.com/s/iddfb4ppwkmtjusir2tc/file/1262409204637 (Accessed January 7, 2024).
27. Wierzbowski, A, Pless, R, and Hildebrand, KJ. Summary of the NACI statement on public health level recommendations on the use of pneumococcal vaccines in adults, including the use of 15-valent and 20-valent conjugate vaccines. Can Commun Dis Rep. (2023) 49:81–6. doi: 10.14745/ccdr.v49i23a08
28. Haute Autorité de Santé. Stratégie de vaccination contre les infections à pneumocoque - Place du vaccin pneumococcique polyosidique conjugué (20-valent, adsorbé) chez l’adulte. Available at: https://www.has-sante.fr/jcms/p_3457419/fr/strategie-de-vaccination-contre-les-infections-a-pneumocoque-place-du-vaccin-pneumococcique-polyosidique-conjugue-20-valent-adsorbe-chez-l-adulte#ancreDocAss (Accessed January 25, 2024).
29. Kirubarajan, A, Lynch, M, Nasreen, S, Gebretekle, GB, Fadel, SA, Crowcroft, NS, et al. Increasing pneumococcal vaccine uptake in older adults: a scoping review of interventions in high-income countries. BMC Geriatr. (2023) 23:2. doi: 10.1186/s12877-022-03653-9
30. Eiden, AL, Barratt, J, and Nyaku, MK. A review of factors influencing vaccination policies and programs for older adults globally. Hum Vaccin Immunother. (2023) 19:2157164. doi: 10.1080/21645515.2022.2157164
31. Castro, ALL, Camacho-Moreno, G, Montañez-Ayala, A, Varón-Vega, F, Alvarez-Rodríguez, JC, Valderrama-Beltrán, S, et al. Invasive pneumococcal disease characterization in adults and subgroups aged < 60 years and ≥ 60 years in Bogota, Colombia. IJID Reg. (2022) 3:293–9. doi: 10.1016/j.ijregi.2022.04.007
32. Arya, S, Norton, N, Kaushik, P, Brandtmüller, A, and Tsoumani, E. Recent changes to adult national immunization programs for pneumococcal vaccination in Europe and how they impact coverage: a systematic review of published and grey literature. Hum Vaccin Immunother. (2023) 19:2279394. doi: 10.1080/21645515.2023.2279394
33. Birck, AM, Nordin Christensen, L, Pedersen, MH, Olsen, J, Johnson, KD, Bencina, G, et al. Health economic evaluation of introducing a PPSV23-based vaccination programme to adults aged 65 and above, and an extension to the 60-64 age group in Denmark. Expert Rev Vaccines. (2021) 20:1327–37. doi: 10.1080/14760584.2021.1977627
34. Kuchenbecker, U, Chase, D, Reichert, A, Schiffner-Rohe, J, and Atwood, M. Estimating the cost-effectiveness of a sequential pneumococcal vaccination program for adults in Germany. PLoS One. (2018) 13:e0197905. doi: 10.1371/journal.pone.0197905
35. Walensky, RP, Schuchat, A, Jernigan, D, Bunnell, R, Layden, J, Kent, CK, et al. Surveillance of vaccination coverage among adult populations-United States, 2018. MMWR Surveill Summ. (2021) 70:1–26. doi: 10.15585/mmwr.ss7003a1
36. Backhaus, E, Berg, S, Andersson, R, Ockborn, G, Malmström, P, Dahl, M, et al. Epidemiology of invasive pneumococcal infections: manifestations, incidence and case fatality rate correlated to age, gender and risk factors. BMC Infect Dis. (2016) 16:367. doi: 10.1186/s12879-016-1648-2
37. Waight, PA, Andrews, NJ, Ladhani, SN, Sheppard, CL, Slack, MP, and Miller, E. Effect of the 13-valent pneumococcal conjugate vaccine on invasive pneumococcal disease in England and Wales 4 years after its introduction: an observational cohort study. Lancet Infect Dis. (2015) 15:535–43. doi: 10.1016/S1473-3099(15)70044-7
38. Centers for Disease Control and Prevention . Geneve: CDC; c2019. Pneumococcal Vaccination. (2024). Available at: https://www.cdc.gov/vaccines/vpd/pneumo/index.html
39. Olsen, J, Schnack, H, Skovdal, M, Vietri, J, Mikkelsen, MB, and Poulsen, PB. Cost-effectiveness of 20-valent pneumococcal conjugate vaccine in Denmark compared with PPV23. J Med Econ. (2022) 25:1240–54. doi: 10.1080/13696998.2022.2152235
40. Pneumonia (community-acquired): antibiotic prescribing, NICE guideline Available at: https://www.nice.org.uk/guidance/ng138
Keywords: invasive pneumococcal disease, pneumonia, meningitis, primary bacteremia, incidence, mortality, adults, vaccination
Citation: Čivljak R, Draženović K, Butić I, Kljaković Gašpić Batinjan M, Huljev E, Vicković N, Lizatović IK, Grgić B, Budimir A, Janeš A, Nikić Hecer A, Filipec Kanižaj T, Tešić V, Kosanović Ličina ML and Dobrović K (2024) Invasive pneumococcal disease in adults after the introduction of pneumococcal vaccination: a retrospective study in the metropolitan area of Zagreb, Croatia (2010–2022). Front. Public Health. 12:1480348. doi: 10.3389/fpubh.2024.1480348
Edited by:
Miguel Angel Sanchez-Aleman, National Institute of Public Health, MexicoReviewed by:
Barbara Camilloni, University of Perugia, ItalyAngelo Salzo, U.O.C. Igiene e Sanità Pubblica, Dipartimento Unico di Prevenzione, Italy
Copyright © 2024 Čivljak, Draženović, Butić, Kljaković Gašpić Batinjan, Huljev, Vicković, Lizatović, Grgić, Budimir, Janeš, Nikić Hecer, Filipec Kanižaj, Tešić, Kosanović Ličina and Dobrović. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Iva Butić, aWJ1dGljQGJmbS5ocg==
†These authors have contributed equally to this work and share first authorship