 David Major1*
David Major1* Márton Falus1
Márton Falus1 Dorottya Árva1,2,3Daniel Eorsi2András Terebessy1
Dorottya Árva1,2,3Daniel Eorsi2András Terebessy1 Adam G. Tabak1,4,5†
Adam G. Tabak1,4,5† Vince Fazekas-Pongor1†
Vince Fazekas-Pongor1†- 1Institute of Preventive Medicine and Public Health, Faculty of Medicine, Semmelweis University, Budapest, Hungary
- 2Doctoral College of Semmelweis University, Budapest, Hungary
- 3MTA-PTE Innovative Health Pedagogy Research Group, University of Pécs, Pécs, Hungary
- 4Department of Internal Medicine and Oncology, Faculty of Medicine, Semmelweis University, Budapest, Hungary
- 5UCL Brain Sciences, University College London, London, United Kingdom
Introduction: The COVID-19 pandemic affected adolescents’ mental health diversely.
Methods: Our objective was to examine the one-year change in well-being (WHO-5 well-being index) and self-esteem (Rosenberg self-esteem scale) among secondary school students affected by school lockdown (lockdown group) compared to control students unaffected by the pandemic (pre-pandemic group), utilizing data from a longitudinal survey study conducted in Hungary. We used linear mixed models stratified by sex and adjusted for family structure and family communication.
Results: Two hundred twenty seven pre-pandemic (128 girls, 99 boys) and 240 lockdown (118 girls, 122 boys) students were included. Both boys’ and girls’ well-being declined in the pre-pandemic group but remained stable in the lockdown group. Post-hoc analyses on WHO-5 items revealed that the pre-pandemic and lockdown groups differed significantly on Item 4 (waking up feeling fresh and relaxed). Boys’ self-esteem did not change over the observation period in neither groups. As for girls, self-esteem of girls during lockdown increased over the observation period, while it did not change in the pre-pandemic group. Better family communication was consistently associated with higher well-being and self-esteem scores for both sexes.
Discussion: Our results suggested that students may have benefitted from altered academic circumstances due to lockdown (e.g., more sleep) and students struggling with waking up early benefitted the most from lockdown (as shown in our post hoc analysis). Additionally, our results also indicate that families should be involved in mental health promotion interventions, especially in time of adversities. This study underscores the multifaceted effects of pandemic-related factors on adolescent mental health and highlights the need to also investigate the unexpected benefits of pandemic-related restrictions to incorporate this knowledge in health promotion programs targeting the well-being of students.
1 Introduction
Since 2020 when COVID-19 was declared a pandemic, a total of 703 million people were infected by Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and COVID-19 was responsible for 7 million deaths worldwide (1). To decrease disease burden, governments launched vaccination campaigns (2) and implemented social restrictions that severely impacted people’s life (3). Among these restrictions, school closures are notable as these restrictions forced adolescents to learn online from home and severely changed the life of affected families (4–7).
Several studies confirmed the negative impact of pandemic-related factors on adolescents’ mental health (8–10). An increasing trend of depressive symptoms, anxiety, stress and loneliness were described in the literature (8, 11). According to a systematic review of 156 observational studies, a worsening of adolescents’ well-being and self-esteem was reported in most studies during the pandemic with some reporting null-findings (12). Furthermore, it was observed that young females (age ≤ 25) were affected more harshly than males (12). The negative effects on well-being and self-esteem were explained partly by the pandemic itself (loss of control and an increase in fear, insecurity, and anger) and partly by the pandemic related social restrictions, such as school closures and social distancing that led to the social isolation of adolescents (12). Even though the majority of studies reported deteriorating mental health among the youths during the pandemic, some studies reported no change or an improvement in both well-being [defined as “the combination of feeling good and functioning well” (13)] and self-esteem [defined as “one’s perception of their own worth and value” (14)], especially at the beginning of the pandemic (15, 16).
Studies focusing on changes of well-being among adolescents often found that certain factors, such as family togetherness, better family functioning, and better quality of family relationships may counterbalance the adverse effects of the pandemic (12). Conversely, dysfunctional parenting, negative familial coping strategies, irritability of parents, and conflicts between parents and children were identified as risk factors related to worse mental health outcomes (12). For self-esteem, similar family-related factors were identified with better family relationship and communication being protective factors and familial conflict and harsh parenting being risk factors for worse self-esteem measured during the pandemic (16).
Understanding the effects of the COVID-19 pandemic on adolescents’ mental health is essential for identifying long-term psychological needs, examining the cohort effect on this generation, and improving preparedness for future public health crises. Given the low number of longitudinal studies and the mixed results regarding the association between the pandemic and well-being and self-esteem of adolescents, we aimed to compare the one-year changes in well-being and self-esteem of secondary school students affected by school lockdown to control students not affected by the pandemic using data from a longitudinal study conducted in Hungary. Our hypothesis was that well-being and self-esteem of students affected by school lockdown would show negative trends compared to the trends of control students not affected by the pandemic. As the effect of school lockdown on mental health was modulated by sex (12, 15) and family functioning (12, 17), we decided to stratify our analysis by sex and adjust for measures of family communication and family structure.
2 Materials and methods
2.1 Study design
The present study is a secondary analysis of data derived from the Balassagyarmat Health Education Program (BEP) (6, 18). BEP was a school-based health education project that focused on measuring and improving various health aspects, including sexual health, substance use, basic life support, infection control, nutrition, physical activity, and mental health of ninth-grade students from all secondary schools (three grammar schools and two vocational schools) in Balassagyarmat. Balassagyarmat is the capital of a northern Hungarian district with around 40,000 inhabitants. BEP operated between 2018 and 2021. Ninth-grade students underwent an online baseline survey before engaging in the one-year long health education program. Following the program, students completed an online follow-up survey in their 10th grade, approximately 1 year after the baseline survey.
For the current analysis, we specifically chose students with a baseline assessment in 2018 or 2020 (excluding 2019). Students with a baseline assessment in 2018 were considered the pre-pandemic group (controls) because they were not affected by the COVID-19 pandemic. This group filled in both baseline and follow-up surveys at school during teaching hours under the supervision of a research assistant without the presence of teachers. Students with a baseline assessment in 2020 were considered the lockdown group because they experienced school lockdowns due to the COVID-19 pandemic. Their baseline assessment happened similarly to the pre-pandemic group before the pandemic, the follow-up survey, however, was filled out at home during the lockdowns. Students were instructed to complete the survey during designated school hours, with the option to contact a research assistant online for any queries. We decided to exclude students enrolled in 2019 because school lockdown was undergoing an early adaptation period in Hungary at the time of their follow-up survey (March 2020). Ethical approval was obtained from the Institutional Review Board of Semmelweis University (SE TUKEB: 276/2017). Passive parental approval (opt-out) consent was sought for every participant.
2.2 Participants
All ninth-graders in Balassagyarmat were invited to participate. Out of 454 eligible ninth-grade students in pre-pandemic classes, 332 (73.1%) completed the baseline survey in February 2018. Of these 98 students were lost to follow-up, thus 234 completed the follow-up survey in March 2019. As for the lockdown group, out of 446 ninth-grade students, 334 participated (74.9%) at the baseline investigation in February 2020, approximately 1 month before the COVID-19-related school lockdowns. The follow-up survey was completed by 251 students in March 2021 (Figure 1). It should be noted that all items on the full questionnaire were compulsory to fill in, so no missing individual outcomes or covariates were in the database. We further excluded overage students (mean + 3SD, n = 7) and participants reporting living with no parents from the analyses (n = 11) leaving to a final analytical sample of 227 students in the pre-pandemic group (128 girls and 99 boys) and 240 students in the lockdown group (118 girls and 122 boys) (Figure 1).
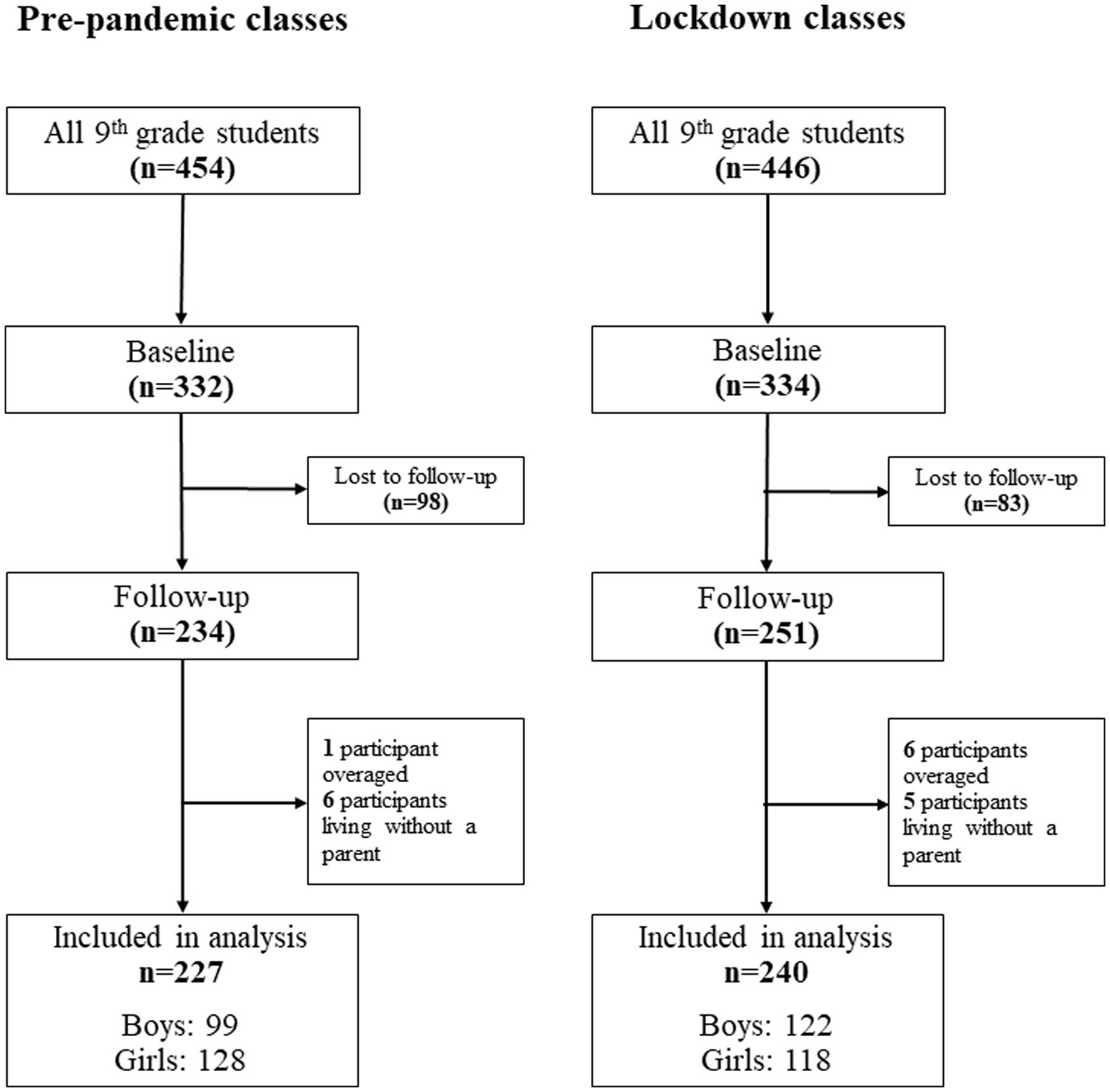
Figure 1. Flowchart of participants.
Secondary schools in Hungary were affected by the lockdowns twice during the pandemic. The first period began on 16 March 2020 and ended on 2 June 2020, while the second began on 11 November 2020 and was still ongoing at the end of our study. Excluding school holidays, public holidays, and weekends, Hungarian schools were closed for a total of 164 days between 1 January 2020 and 20 May 2021 (19).
2.3 Outcomes
Well-being was measured by the validated Hungarian version of the WHO-5 Well-being Index (WBI) (20, 21). This instrument consists of five items, each with a Likert scale ranging from 0 (at no time) to 3 points (all of the time). The items assess whether the participants (1) ‘have felt cheerful in good spirits’, (2) ‘have felt calm and relaxed’, (3) ‘have felt active and vigorous’, (4) ‘woke up feeling fresh and rested’ or (5) daily life has been filled with things that interest them in the last 2 weeks. The maximal score is 15. A higher score indicates better well-being.
Self-esteem was measured by the validated Hungarian version of the Rosenberg Self-esteem Scale (RSS) (14, 22), which has 10 items (5 of these with reverse scoring) with 4-point Likert scales (ranging from strongly agree to strongly disagree). The maximal score is 30. RSS is a unidimensional construct reflecting global self-esteem. A higher score is associated with higher self-esteem. The items read (1) ‘On the whole, I am satisfied with myself’; (2) ‘At times, I think I am no good at all’; (3) ‘I feel that I have a number of good qualities’; (4) ‘I am able to do things as well as most other people’; (5) ‘I feel I do not have much to be proud of’; (6) ‘I certainly feel useless at times’; (7) ‘I feel that I’m a person of worth, at least on an equal plane with others’; (8) ‘I wish I could have more respect for myself’; (9) ‘All in all, I am inclined to feel that I am a failure’; (10) ‘I take a positive attitude toward myself’.
2.4 Covariates
As family plays a significant role in children’s development, distress, well-being (23, 24), and self-esteem (16), our analysis was adjusted for family structure and family communication measures based on the recommendations from the Health Behavior in School-aged Children Study (25). Family structure was characterized by the participants’ response to the question with whom they lived together. Answers were collapsed into three categories: living with both parents, with one parent, or in a stepfamily (one biological parent and his/her new partner who lives in the same household).
Family communication was assessed by the Hungarian short version of the Clear Communication Scale from Family Dynamics Measure II (FDMII) (25, 26). The questionnaire has four items with a Likert scale ranging from 1 to 5 (strongly disagree to strongly agree) with a maximum score of 20. A higher score indicates a more positive assessment of family communication. The items assess whether in the family (1) ‘I think the important things are talked about’; (2) ‘When I speak someone listens to what I say’; (3) ‘We ask questions when we do not understand each other’; (4) ‘When there is misunderstanding, we talk it over until it’s clear’.
2.5 Statistical analysis
All analyses used a ‘full case’ design and were stratified by sex. Chi-squared tests for the categorical variable family structure and independent samples t-tests for the continuous variables (age and family communication) were used to compare baseline data of pre-pandemic vs. lockdown classes as well as follow-up data of pre-pandemic vs. lockdown classes, respectively.
Marginal homogeneity tests for the categorical variable family structure and paired t-tests for continuous variables (age and family communication) were used to compare baseline vs. follow-up data within pre-pandemic and lockdown groups.
Linear mixed models were used to assess changes associated with COVID-19-related school lockdowns in well-being (WHO-5 WBI) and self-esteem (RSS). Model 1 includes group status (pre-pandemic/lockdown) as the sole predictor, while Model 2 is adjusted for time-varying family structure and family communication. Both models include a random slope and a random intercept with an unstructured covariance matrix.
To further clarify the possible causes of the unexpected improvement in well-being during the pandemic, we run separate models for each question of the WHO-5 WBI using similar linear mixed models with group status as the only predictor (Model 1). These models showed that the only significant difference between the pre-pandemic and the lockdown groups was in the change in the score on Item 4 (waking up feeling fresh and rested) over follow-up. Thus, we hypothesized that those adolescents who struggled with waking up early profited the most from the lockdowns. To test this hypothesis, first we divided the students into two subgroups: those with a low score on Item 4 (0 and 1) vs. those with a high score (2 or 3) at baseline. Then we extended Model 1 with the previous grouping variable (including the main effect, its interaction with pandemic status, with follow-up, and a 3-way interaction with pandemic status and follow-up). This parameterization allowed us to test whether the subgroups based on Item 4 showed different behaviors before and during the pandemic.
Given that RSS has a unidimensional structure (14, 27), we decided against conducting any post-hoc analyses on RSS questions.
All statistical analyses were performed using IBM SPSS Statistics version 29.0.1.0. Statistical significance was set at 2-tailed p < 0.05.
3 Results
3.1 Baseline characteristics of the participants
Table 1 presents the descriptives for the study sample by sex, group status (pre-pandemic/lockdown), and timepoint (baseline/follow-up).
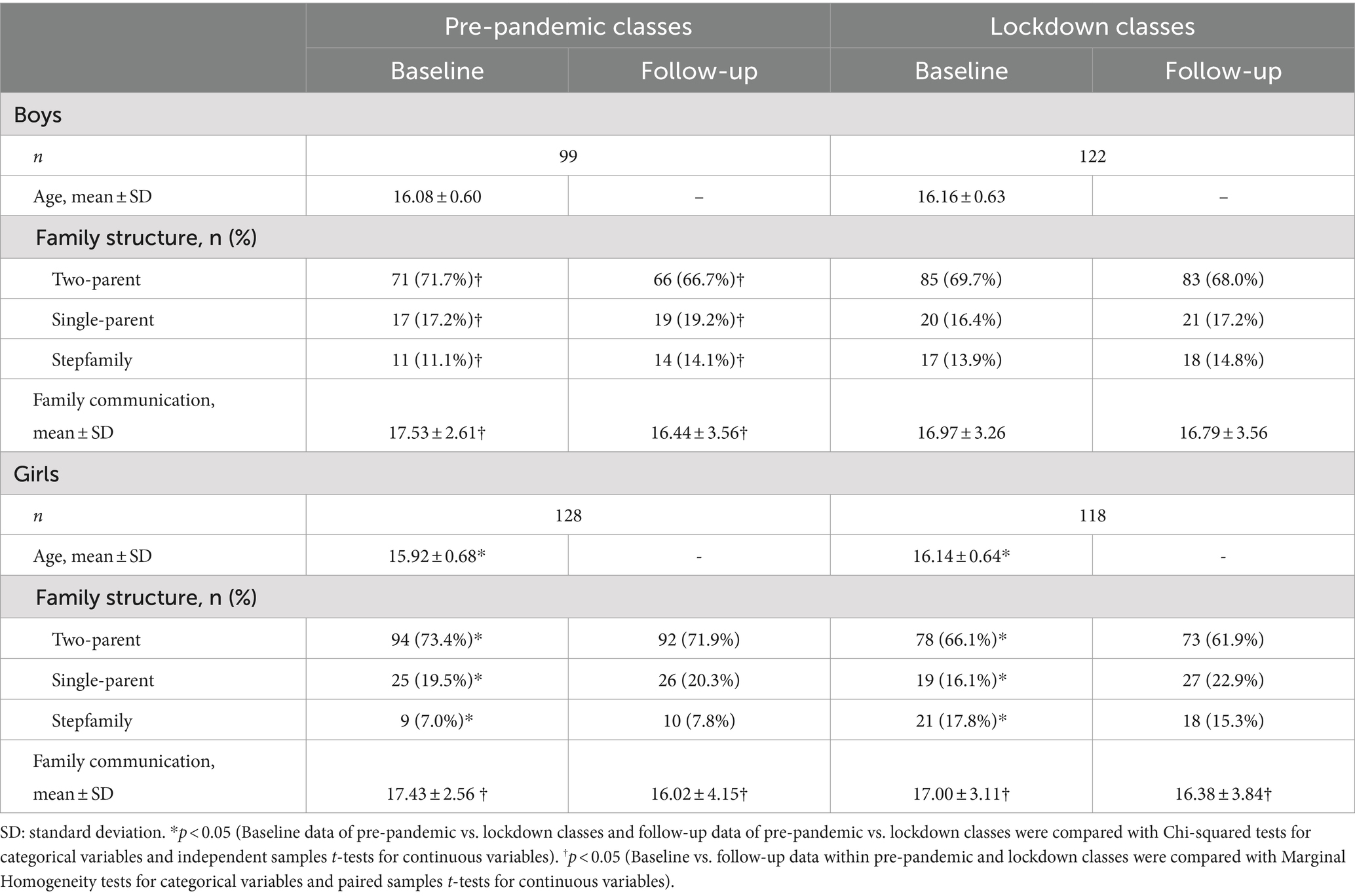
Table 1. Characteristics of pre-pandemic and lockdown classes.
Regarding boys, age, family structure, and family communication results were similar in the pre-pandemic and the lockdown classes at both timepoints (all p > 0.05).
Girls in lockdown classes were 0.22 years older compared to the pre-pandemic group. Furthermore, the baseline family structure of the pre-pandemic and lockdown classes differed significantly for girls with a higher proportion of stepfamilies in the lockdown group. However, we found no significant differences in family structure or family communication at follow-up.
3.2 Changes in family structure and communication over follow-up
When comparing baseline and follow-up characteristics within groups, we found that the distribution of family structure changed (less two-parent families at follow-up) and family communication worsened significantly from baseline to follow-up in the pre-pandemic group for boys. No other significant changes were found in any of the groups from baseline to follow-up (Table 1).
3.3 Changes in the WHO-5 well-being score
According to the unadjusted model (Model 1), WHO-5 well-being scores were similar in the pre-pandemic and lockdown groups of boys at baseline. The pre-pandemic boys’ score declined by 1.05 (95% confidence intervals [CI]: −1.72 to −0.38) points over 1 year of follow-up. In contrast, the lockdown group showed a significantly smaller decline during follow-up, leading to a non-significant but positive point estimate of change. Adjustment for family structure and family communication (Model 2) did not materially change this pattern. Furthermore, family communication showed a significant positive association with the WHO well-being score cross-sectionally: better communication within the family was associated with higher score on well-being of boys (Table 2; Figure 2).
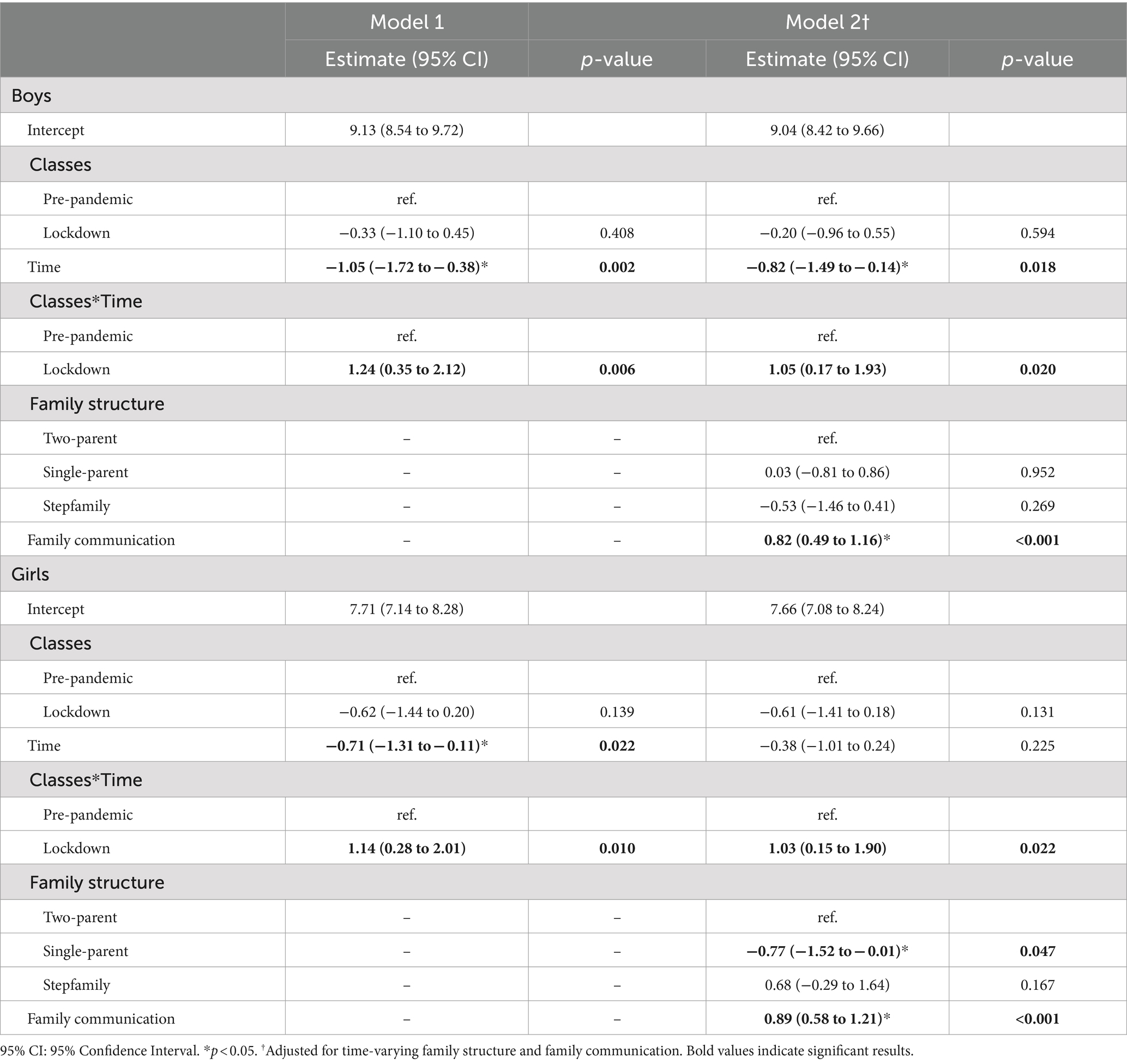
Table 2. Results of linear mixed models for WHO well-being score.
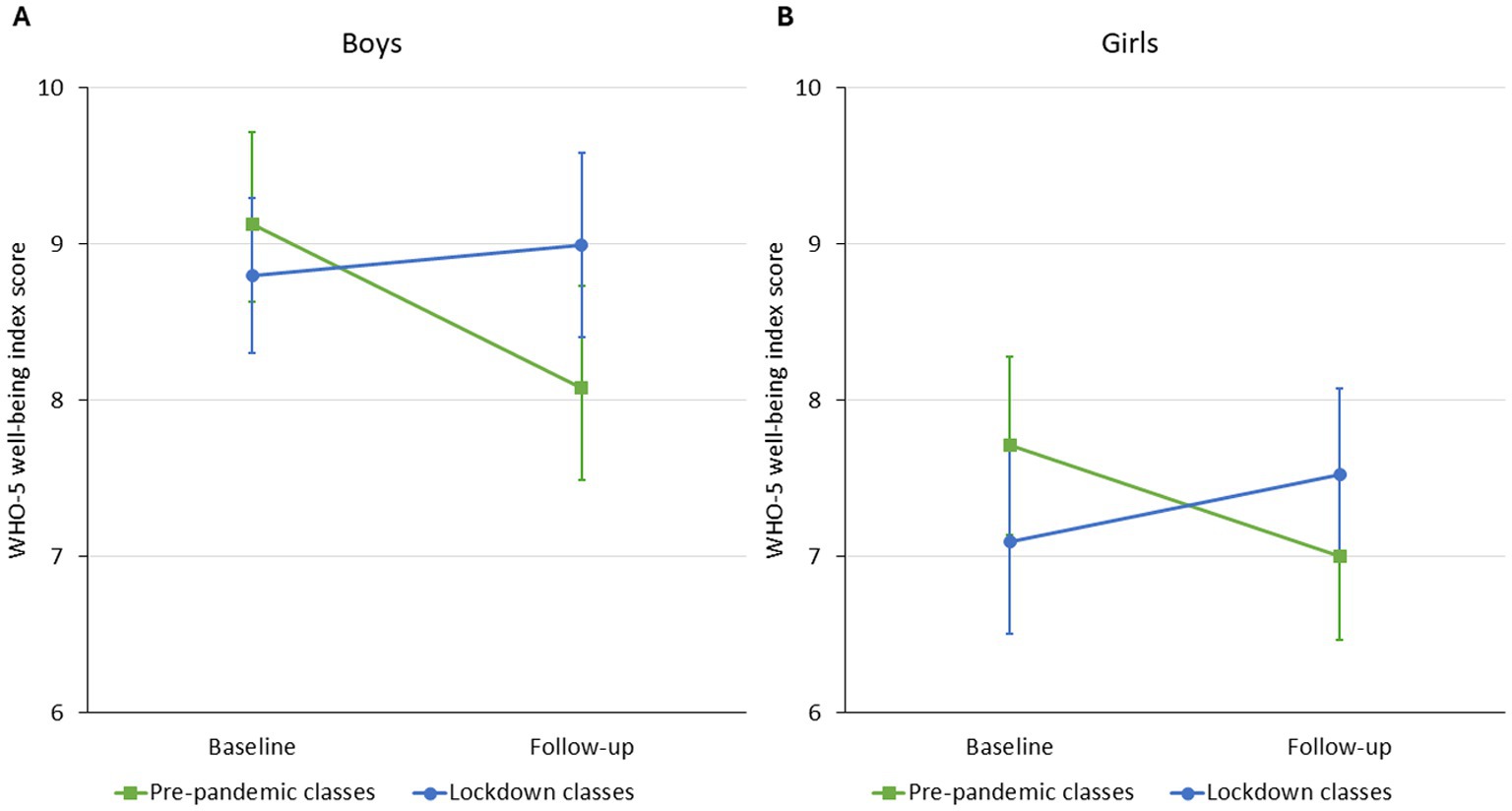
Figure 2. Estimated marginal means (Model 1) of boys’ (Panel A) and girls’ (Panel B) WHO-5 well-being index score of pre-pandemic and lockdown classes from baseline to follow-up.
In general, girls had lower WHO-5 well-being scores than boys. The overall pattern of change in girls was similar to boys in the unadjusted model (Model 1): similar scores in the pre-pandemic and the lockdown groups at baseline with a significant decline in the pre-pandemic group (mean difference [MD]: 0.71, 95%CI: −1.31 to −0.11), and a significantly different change leading to a non-significant improvement in the lockdown group. After adjustment for time-varying family communication and structure (Model 2), the decline in the pre-pandemic group hugely attenuated and became non-significant, while the difference in the change between the groups remained leading to an actual improvement in well-being in the lockdown group (MD: 0.64, 95%CI: 0.01 to 1.72). Living in a single-parent family was associated with a worse well-being score (−0.77 [95%CI: −1.52 to −0.01]) compared to two-parent families and stepfamilies cross-sectionally. Family communication had a positive effect of on well-being with a similar effect size as it did in boys (Table 2; Figure 2).
3.4 Changes in the individual items of the WHO-5 well-being index during follow-up
After experiencing an unexpected improvement in well-being during the pandemic, we decided to clarify the reason by running separate models for the individual items of the WHO-5 WBI using similar linear mixed models with group status as the only predictor. When analyzing individual items of the WHO-5 WBI questionnaire, the boys’ lockdown group had slightly higher scores at baseline for Item 1 (feeling cheerful in good spirits; 0.32 [95%CI: 0.09 to 0.54]) and Item 3 (feeling active and vigorous; 0.27 [95%CI: 0.03 to 0.50]) compared to the pre-pandemic group. No significant change for the group of pre-pandemic boys was found during the follow-up period. As for the lockdown group, no change in Items 1, 2, 3, and 5 was found, however, the change over time was significantly different for Item 4 (waking up feeling fresh and relaxed) between the pre-pandemic and lockdown groups, showing an improvement in the lockdown group from baseline to follow-up (Table 3).
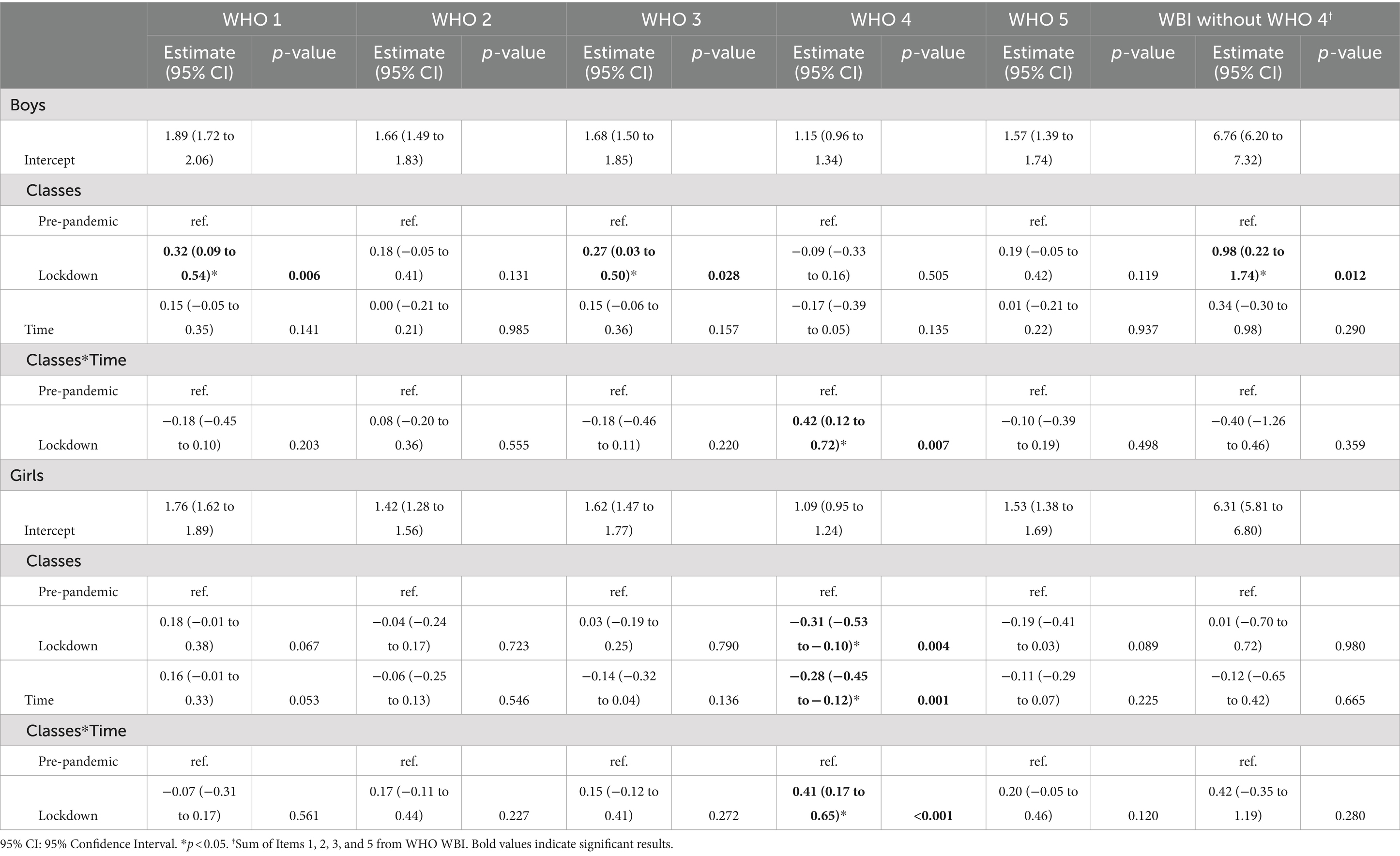
Table 3. Results of linear mixed models for WHO-5 WBI items.
As for girls, baseline differences were detected only for Item 4 with lockdown girls having a lower score (−0.31 95%CI: −0.53 to −0.10). The score of Item 4 declined in pre-pandemic girls during the follow-up period, while (similarly to boys) the lockdown girls’ score changed in the opposite direction with a similar effect size observed in boys (Table 3).
3.5 Changes in the WHO-5 well-being score in subgroups based on item 4 at baseline
Since the only significant difference between the pre-pandemic and the lockdown groups was in the change in the score on Item 4 (waking up feeling fresh and rested), we hypothesized that adolescents who struggled with waking up early may have profited the most from the lockdowns. To test this, we compared the changes in the WHO-5 well-being score in subgroups based on Item 4 at baseline. The WHO-5 WBI score of boys waking up feeling fresh and relaxed (Item 4 score ≥ 2) declined similarly in the pre-pandemic and the lockdown classes (MD of changes: 0.33 [95%CI: −1.10 to 1.77]). In contrast, boys with lower scores on Item 4 at baseline behaved differently in pre-pandemic and lockdown groups: total WHO-5 WBI score of the pre-pandemic group declined, while the score of lockdown group increased (MD of changes: 1.20 [95%CI: 0.15 to 2.25]) (Figure 3).
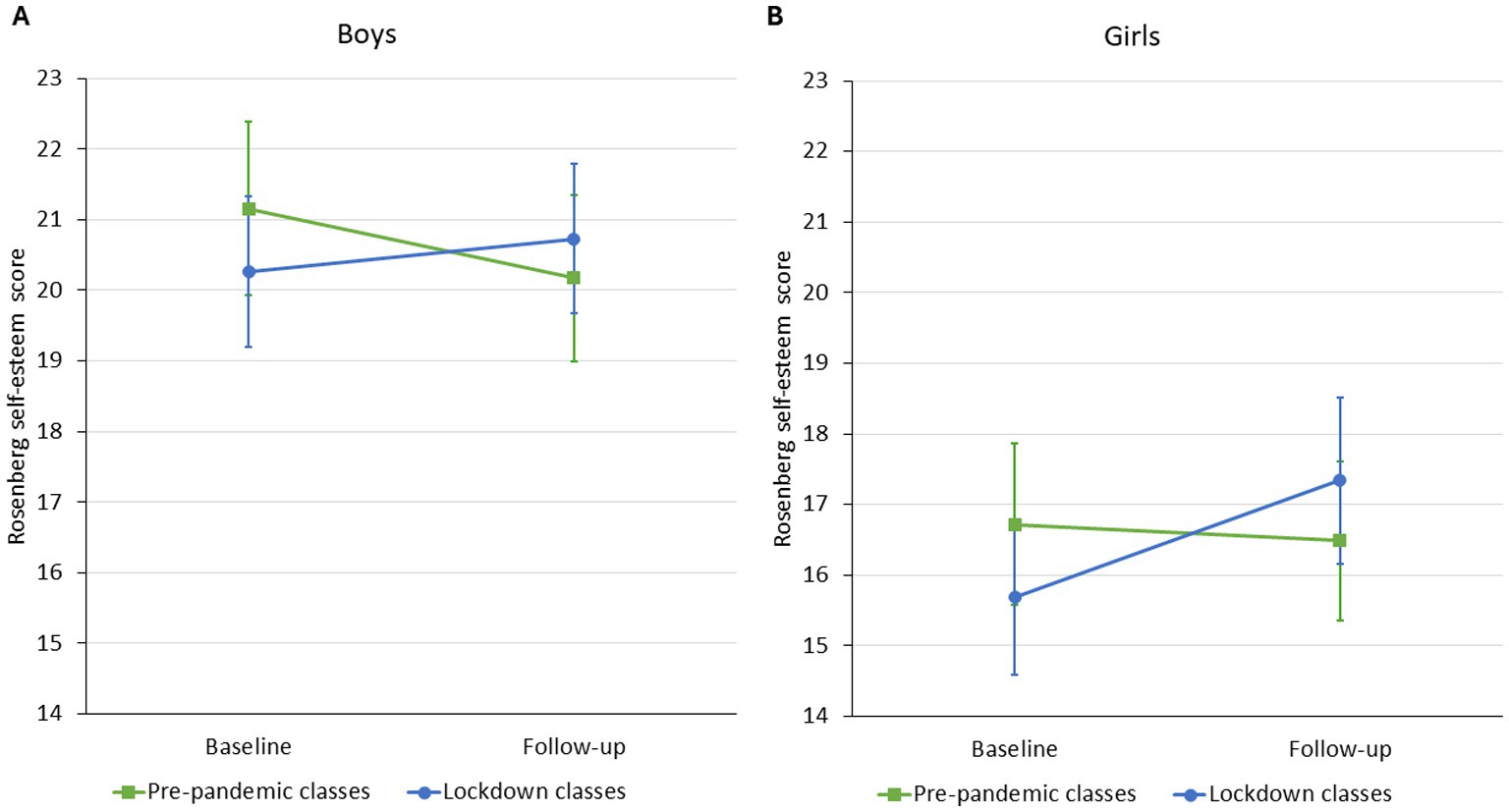
Figure 3. Estimated marginal means (Model 1) of boys’ (Panel A) and girls’ (Panel B) WHO-5 well-being index score by subgroups based on WHO-5 Item 4.
The changes observed in girls were similar to boys. The WHO-5 WBI score of girls waking up feeling fresh and relaxed (Item 4 score ≥ 2) declined similarly in the pre-pandemic and the lockdown classes (MD of changes: -0.31 [95%CI: −2.02 to 1.41]). In contrast, girls with lower scores on Item 4 at baseline behaved differently in the pre-pandemic and the lockdown groups: total WHO-5 WBI score of the pre-pandemic group declined, while the score of the lockdown group increased (MD of changes: 1.20 [95%CI: 0.23 to 2.17]) (Figure 3).
3.6 Changes in the Rosenberg self-esteem scale
The average score on the Rosenberg self-esteem scale was similar for boys in the pre-pandemic and the lockdown groups without a significant change in unadjusted models (Model 1) during the one-year follow-up. The model adjusted for family structure and communication (Model 2) yielded similar results. Furthermore, this model also found that living in a stepfamily was associated with a 2.26 (95%CI: 0.35 to 4.16) point lower score on the self-esteem scale, as well as better family communication was associated with significantly higher self-esteem (Table 4; Figure 4).
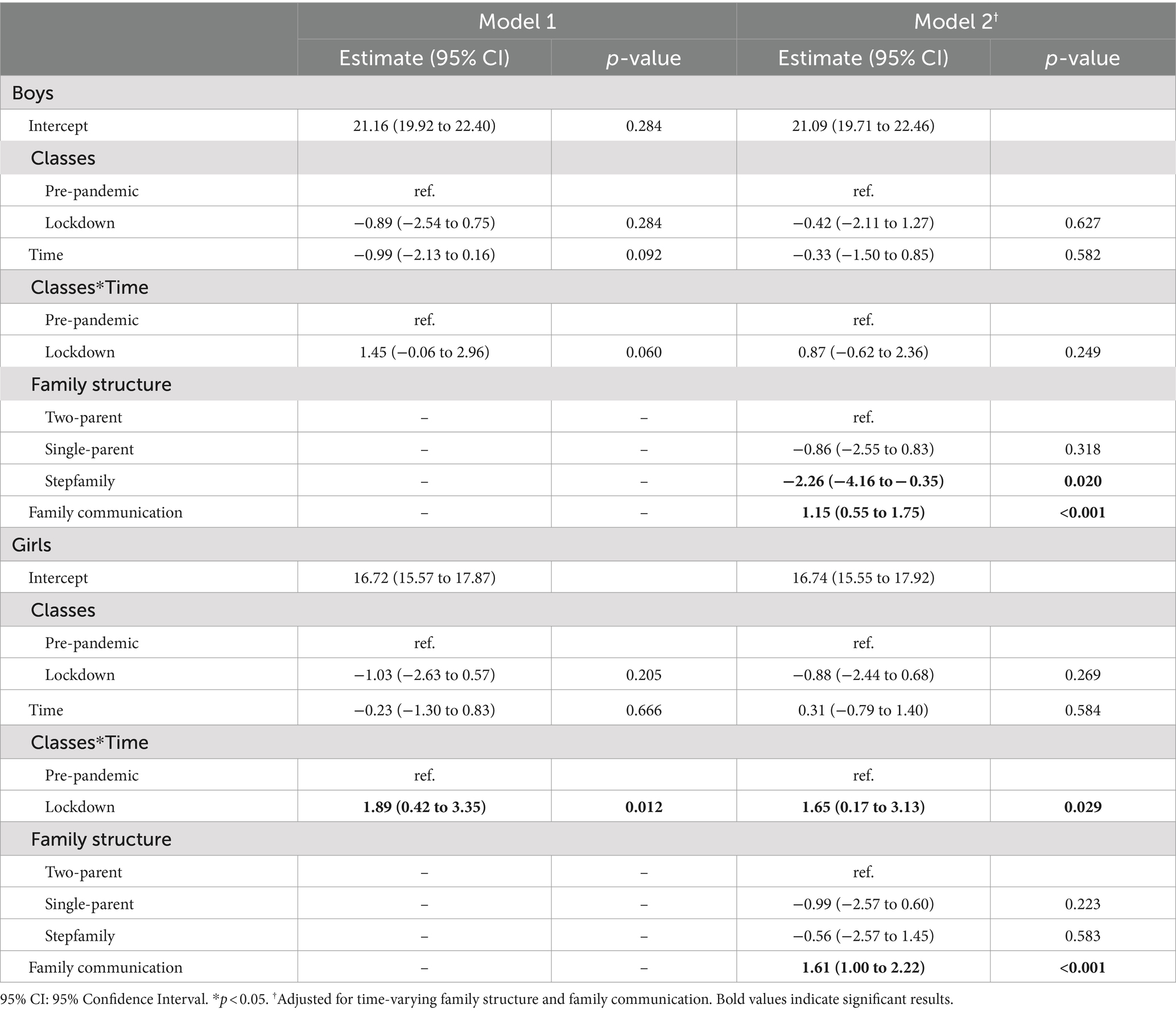
Table 4. Results of linear mixed models for score on Rosenberg self-esteem scale.
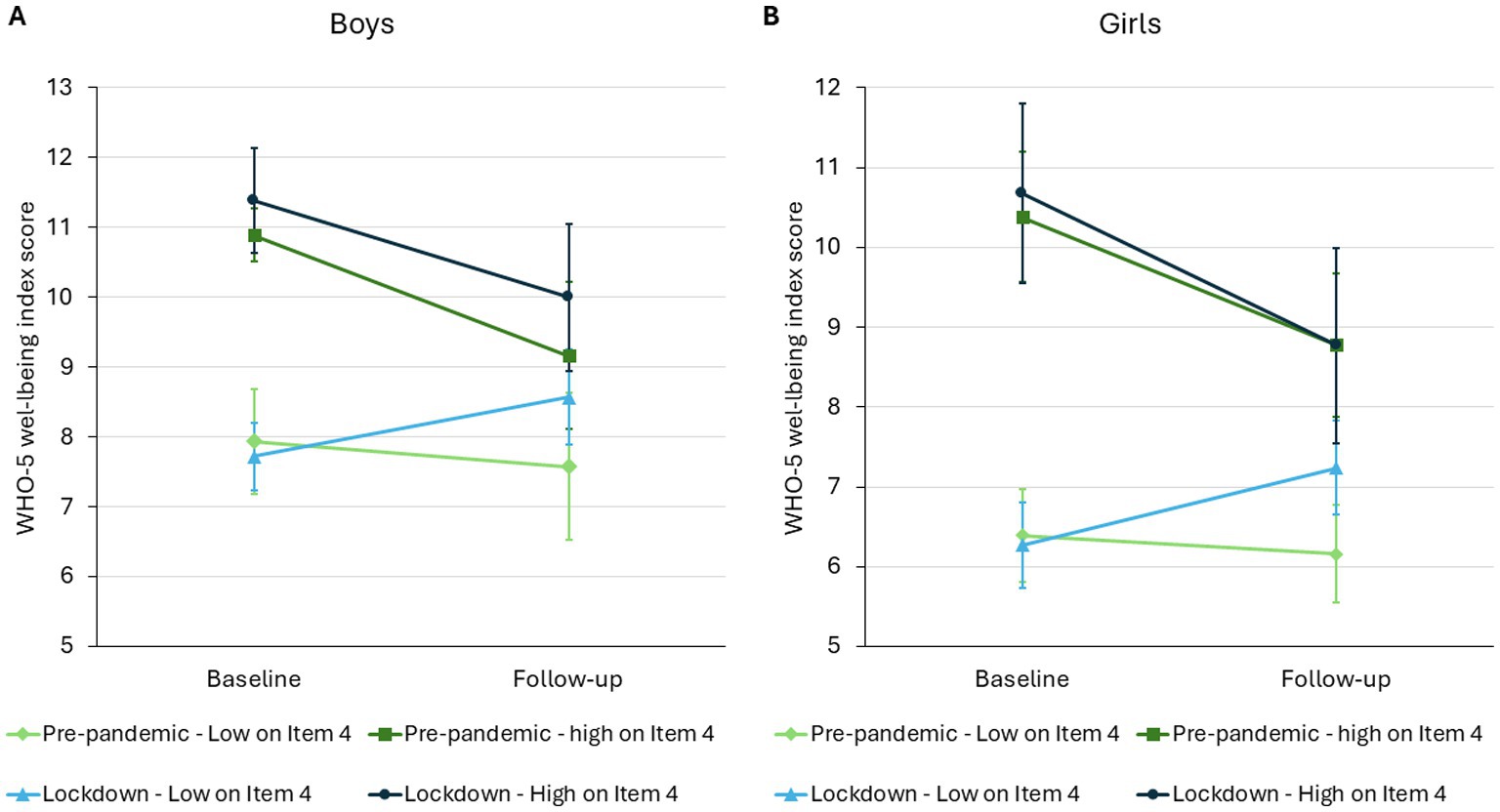
Figure 4. Estimated marginal means (Model 1) of boys’ (Panel A) and girls’ (Panel B) Rosenberg self-esteem score of pre-pandemic and lockdown classes from baseline to follow-up.
Girls had a lower score on the Rosenberg self-esteem scale compared to boys. There was no difference in the self-esteem scores either in the unadjusted or the adjusted models between pre-pandemic and lockdown groups at baseline. We found no significant change in the self-esteem score in the pre-pandemic classes during the one-year follow-up, while the change in the lockdown classes was significantly larger, leading to an increase over time. Model 2 confirmed this finding. Furthermore, we found that better family communication was associated with higher self-esteem score in girls, while family structure was not related to self-esteem (Table 4; Figure 4).
4 Discussion
4.1 Short summary
In a secondary epidemiological analysis of an intervention program of 9th grade secondary school students in a Hungarian city, we compared changes in well-being and self-esteem before and during the COVID-19 pandemic over a one-year period.
Our results showed that adolescents’ well-being declined under ordinary circumstances over 1 year, but this decline was significantly smaller (even showing positive point estimates) during the COVID-19 pandemic. This finding disproved our hypothesis. The differences between the changes in the pre-pandemic vs. the lockdown cohorts remained significant even after adjusting for family communication and structure. When we looked for a potential explanation of this observation, we found that 4 of the 5 WHO-5 WBI items changed similarly before and during the pandemic, while there was a significant difference in the change of Item 4 (waking up feeling fresh and relaxed) between the cohorts over follow-up. Based on this, we tested for an interaction between item 4 scores at baseline and lockdown status over time. This analysis showed that the total WHO-5 WBI score declined in those with a high baseline score on item 4 irrespective of sex and lockdown status over time. For those with a low baseline score on item 4, it remained stable in those not affected by the lockdown, while it improved significantly in those adolescents affected by the pandemic.
While the self-esteem of boys changed similarly in the cohorts over follow-up, self-esteem of girls affected by the pandemic increased compared to the pre-pandemic classes over follow-up. Again, adjustment for family structure and communication had no major effect on these observations.
Finally, our study also revealed that better family communication was consistently associated with higher well-being and higher self-esteem for both boys and girls.
4.2 Results in context of the literature
4.2.1 Sex differences in well-being and self-esteem
Our study showed that girls overall had a lower well-being and self-esteem than boys, which correlates with the literature (28–30). Girls tend to have more depressive symptoms and exhibit stronger anxiety than boys, which may translate to lower well-being (31, 32). As for self-esteem, girls tend to evaluate their own physical appearance and intellectual abilities more negatively than boys, potentially explaining why girls have a lower self-esteem in adolescence than boys (33). Furthermore, the observed sex differences may be related to sex-related variations in changes related to puberty or differences in the roles of sexes, their responsibilities, and the support system (31).
4.2.2 Changes in well-being associated with the pandemic
Our study revealed a decrease in well-being of pre-pandemic adolescents over a one-year period, which is in line with the results of the latest Health Behavior in School-aged Children Study of the WHO (28). Surprisingly, this decline was not observed in the pandemic cohort despite several studies demonstrating negative effects of school lockdowns on mental health (34–37). According to our post-hoc analysis, changes in 4 of the 5 items of the WHO-5 WBI were similar before and during the pandemic, while Item 4 that investigates feelings after waking up, sleeping more and feeling more rested decreased significantly less during the pandemic. Based on these findings we suspect that the overall change in well-being is linked to more sleep time and/or later wake-up time among those students that had a low response on Item 4 at baseline, as students attended class from home and did not have to commute to school in the early hours (38, 39). A study performed in Austrian supports our findings, as it also revealed an improvement in the WHO-5 WBI score during remote schooling compared to a period when schools were reopened. However, they did not look for an explanation of this counterintuitive observation (40). Furthermore, a qualitative study on Scottish adolescents claimed the disruption to schooling had positive impact on their mental health and well-being due to reduced school-related difficulties and workload (41).
4.2.3 Changes in self-esteem during the pandemic
In our study, self-esteem remained broadly stable in in the pre-pandemic cohorts over follow-up, which is in line with the results of other studies (42, 43). In contrast, girls’ self-esteem improved during the pandemic compared to the pre-pandemic group. Unlike our finding, other studies reported no change (44) or a slight decrease (15) in self-esteem, however the latter used different instrument. Furthermore, studies on the effect of COVID-19 school lockdowns on self-esteem are scarce. Self-esteem reflects one’s perception of their own worth and value (14) and is affected by several factors among which school expectations and academic achievement seem to play an important role (30, 45, 46). Since girls are more concerned about academic achievement (47), lower academic expectations may explain the observed improvement of the girls’ self-esteem during the pandemic.
4.2.4 Cross-sectional determinants of well-being and self-esteem
Better family communication was cross-sectionally related to higher well-being and self-esteem both in boys and girls in our study that well corresponds to the literature (48, 49). In addition family communication has a mediating effect between family resilience and family functioning (50) and could also lead to better mental health of adolescents (51). Our results showed that both boys and girls with better family communication independent of the presence of adversities, such as the COVID-19 pandemic, as better family communication incorporating elements of approach coaching may decrease distress (23). Approach coaching is defined as “any behavioral, cognitive, or emotional activity that is directed toward a threat (e.g., problem solving or seeking information)” (52) and is in contrast to avoidance of the situation, which is linked to an increase of distress in time of adversities (23).
4.3 Strengths and limitations
Our study benefits from several strengths. First, our participants from a deprived Central-European region well represent adolescents from similar circumstances giving some external validity to our findings. Given that we collected data on within person changes over time, we have sufficient power to investigate relatively small absolute changes in well-being and self-esteem. Furthermore, the fact that the pre-pandemic and the lockdown cohorts came from the same source population and had similar baseline characteristics, the bias resulting from cohort effect may be minimal. The longitudinal design of our study is also notable because most studies investigating similar questions had a cross-sectional design or did not have adequate control groups.
Our study has some limitations that has to be acknowledged. First, neither the participation rate, nor the capture of participants at follow-up were perfect that limits external validity. Similarly, our participants represent an ethnically homogenous group, thus extrapolation to non-white adolescents is limited. Our outcomes are based on short versions of the well-being and the self-esteem questionnaires that may limit their sensitivity. Furthermore, the WHO-5 questionnaire may be prone to an ‘influential question’: given that students were not required to get up early during the pandemic, Item 4 of the WHO-5 WBI questionnaire showed a significant improvement. However, we think that this does not necessarily reflect an improvement in overall well-being. This observation highlights the importance to investigate the effect of an intervention or changing circumstance on each item of the questionnaire and shows limited generalizability of this measure. Furthermore, even though the WHO-5 WBI is widely used to measure well-being in different phases of life, the definition of well-being and the factors affecting it may differ between adults and adolescents (53). For instance, while the WHO-5 well-being index was shown to be associated with psychosocial working factors among adults (54), its association with school environment or academic pressure have not been investigated as extensively, which factors can be relevant regarding the well-being of adolescents. Moreover, our questionnaire did not include questions and instruments that measured certain feelings related to the pandemic either, such as fear and anxiety of the pandemic (55), that may also have a great impact on the well-being of adolescents. The main reason for this is that our questionnaire was developed before the pandemic. Similarly, other determinants of well-being and self-esteem (such as, social connections (56), teacher-student relationship (57), or environmental factors (56)) were not captured in our study, and these and other unmeasured confounders could have biased our findings. Given this and the fact that ours is a post hoc analysis of health promotion program precludes determining causal relationships and our results are only for hypothesis generation.
5 Conclusion
In conclusion, our study shows that adolescents’ well-being and self-esteem changed differently during the COVID-19 lockdowns compared to the pre-pandemic period. While it is expected that the fear of an unknown pandemic and social distancing can raise anxiety and depression in populations, certain aspects of life may unexpectedly improve. For instance, our study showed that adolescents felt more rested during the lockdown period of the pandemic that had a positive effect on their WHO-5 well-being scores. Similarly, we found a robust improvement in the self-esteem of girls during the pandemic potentially related to a less intensive feedback from peers and teachers. If our results reflect a causal relationship between longer sleep and well-being, schools could consider starting teaching at later hours for adolescents.
In addition to this, our results strongly support the beneficial role of good family communication in adolescents’ well-being and self-esteem, as well as other mental health issues.
Another important conclusion relates to the limitation of general well-being questionnaires and especially short versions of them in measuring well-being in special circumstances. We think that these questionnaires should be supplemented with other instruments that evaluate other aspects of well-being and also aspects of the circumstances we intend to investigate.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Institutional Review Board of Semmelweis University (SE TUKEB: 276/2017). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
DM: Formal analysis, Investigation, Visualization, Writing – original draft. MF: Formal analysis, Investigation, Writing – original draft. DÁ: Investigation, Writing – original draft. DE: Conceptualization, Investigation, Writing – review & editing. AT: Conceptualization, Writing – review & editing. AGT: Supervision, Writing – review & editing. VF-P: Formal analysis, Writing – original draft.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. The Balassagyarmat Health Education Program was supported by the European Union and the Hungarian State (grant number: EFOP-3.4.3-16-2016-00007). AGT was supported by project no. TKP2021-NKTA-47, implemented with the support provided by the Ministry of Innovation and Technology of Hungary from the National Research, Development and Innovation Fund, financed under the TKP2021-NKTA funding scheme. Funding for the project through the National Cardiovascular Laboratory Program (RRF-2.3.1-21-2022-00003) was provided by the Ministry of Innovation and Technology of Hungary from the National Research, Development and Innovation Fund. This work was also supported by European University for Well-Being (EUniWell) program (grant agreement number: 101004093/ EUniWell/EAC-A02-2019 / EAC-A02-2019-1). The funding sources had no role in the interpretation of data, the writing of the report, and the decision to submit the article for publication.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Worldometer. Worldometer COVID-19 data. Avaliable at: https://www.worldometers.info/coronavirus/about/ (Accessed March 04, 2024).
2. Fazekas-Pongor, V, Szarvas, Z, Nagy, ND, Péterfi, A, Ungvári, Z, Horváth, VJ, et al. Different patterns of excess all-cause mortality by age and sex in Hungary during the 2(nd) and 3(rd) waves of the COVID-19 pandemic. Geroscience. (2022) 44:2361–9. doi: 10.1007/s11357-022-00622-3
3. Talic, S, Shah, S, Wild, H, Gasevic, D, Maharaj, A, Ademi, Z, et al. Effectiveness of public health measures in reducing the incidence of covid-19, SARS-CoV-2 transmission, and covid-19 mortality: systematic review and meta-analysis. BMJ. (2021) 375:e068302. doi: 10.1136/bmj-2021-068302
4. Janssens, JJ, Achterhof, R, Lafit, G, Bamps, E, Hagemann, N, Hiekkaranta, AP, et al. The impact of COVID-19 on Adolescents' daily lives: the role of Parent-child relationship quality. J Res Adolesc. (2021) 31:623–44. doi: 10.1111/jora.12657
5. Canzi, E, Danioni, FV, Parise, M, Lopez, G, Ferrari, L, Ranieri, S, et al. Perceived changes in family life during COVID-19: the role of family size. Fam Relat. (2021) 70:1303–11. doi: 10.1111/fare.12579
6. Major, D, Fazekas-Pongor, V, Pártos, K, Tabák, AG, Ungvari, ZI, Eörsi, D, et al. Effect of school lockdown due to the COVID-19 pandemic on screen time among adolescents in Hungary: a longitudinal analysis. Front Public Health. (2023) 11:24. doi: 10.3389/fpubh.2023.1233024
7. Biroli, P, Bosworth, S, Della Giusta, M, Di Girolamo, A, Jaworska, S, and Vollen, J. Family life in lockdown. Front Psychol. (2021) 12:12. doi: 10.3389/fpsyg.2021.687570
8. Pepe, A, and Farina, E. A mixed-method study on adolescents' well-being during the COVID-19 syndemic emergency. Sci Rep. (2023) 13:871. doi: 10.1038/s41598-022-24007-w
9. Richard, V, Dumont, R, and Lorthe, E. Impact of the COVID-19 pandemic on children and adolescents: determinants and association with quality of life and mental health-a cross-sectional study. Child Adol Psych Men. (2023) 17:563. doi: 10.1186/s13034-023-00563-5
10. Farrell, AH, Vitoroulis, I, Eriksson, M, and Vaillancourt, T. Loneliness and well-being in children and adolescents during the COVID-19 pandemic: a systematic review. Children Basel. (2023) 10:279. doi: 10.3390/children10020279
11. Cochran, G, Cohen, ZP, Paulus, MP, Tsuchiyagaito, A, and Kirlic, N. Sustained increase in depression and anxiety among psychiatrically healthy adolescents during late stage COVID-19 pandemic. Front Psych. (2023) 14:1137842. doi: 10.3389/fpsyt.2023.1137842
12. Zolopa, C, Burack, JA, and O'Connor, RM. Changes in youth mental health, psychological wellbeing, and substance use during the COVID-19 pandemic: a rapid review. Adolesc Res Rev. (2022) 7:161–77. doi: 10.1007/s40894-022-00185-6
13. Ruggeri, K, Garcia-Garzon, E, Maguire, A, Matz, S, and Huppert, FA. Well-being is more than happiness and life satisfaction: a multidimensional analysis of 21 countries. Health Qual Life Out. (2020) 18:423. doi: 10.1186/s12955-020-01423-y
14. Rosenberg, M. Society and the adolescent self-image. Princeton: Princeton University Press (1965).
15. Goto, R, Piedvache, A, Hangai, M, Yamaoka, Y, Sampei, M, Sawada, N, et al. Time trends in emotional well-being and self-esteem in children and adolescents during the COVID-19 pandemic. Child Adolesc Psychiatry Ment Health. (2022) 16:89. doi: 10.1186/s13034-022-00525-3
16. Maruyama, JM, Tovo-Rodrigues, L, Santos, IS, Murray, J, and Matijasevich, A. Changes and predictors of adolescent emotion regulation, selfesteem, and locus of control during the COVID-19 pandemic: the 2004 Pelotas birth cohort. Braz J Psychiatry. (2023) 45:389–96. doi: 10.47626/1516-4446-2023-3169
17. Wong, RS, Tung, KTS, Li, X, Chui, CS, Tso, WWY, Lee, TMC, et al. Examining family pre-pandemic influences on adolescent psychosocial wellbeing during the COVID-19 pandemic. Curr Psychol. (2022) 43:12034–44. doi: 10.1007/s12144-022-02736-5
18. Eörsi, D, Árva, D, Herczeg, V, and Terebessy, A. Komplex iskolai egészségfejlesztő program a COM-B modell tükrében [introduction to a complex school-based health education program from the COM-B model’s perspective]. Egészségfejlesztés. (2020) 61:36–47. doi: 10.24365/ef.v60i2.540
19. OECD. The state of global education: 18 months into the pandemic. Paris: OECD Publishing (2021). doi: 10.1787/1a23bb23-en
20. Susánszky, É, Konkoly Thege, B, Stauder, A, and Kopp, M. Validation of the short (5-item) version of the WHO well-being scale based on a Hungarian representative health survey (Hungarostudy 2002). Mentálhigiéné Pszichoszomatika. (2006) 7:247–55. doi: 10.1556/mental.7.2006.3.8
21. Topp, CW, Ostergaard, SD, Sondergaard, S, and Bech, P. The WHO-5 well-being index: a systematic review of the literature. Psychother Psychosom. (2015) 84:167–76. doi: 10.1159/000376585
22. Sallay, V, Martos, T, Földvári, M, Szabó, T, and Ittzés, A. Hungarian version of the Rosenberg self-esteem scale (RSES-H): an alternative translation, structural invariance, and validity. Mentálhigiéné Pszichoszomatika. (2014) 15:259–75. doi: 10.1556/mental.15.2014.3.7
23. Gecer, E, and Yildirim, M. Family communication and psychological distress in the era of COVID-19 pandemic: mediating role of coping. J Fam Issues. (2023) 44:203–19. doi: 10.1177/0192513X211044489
24. Han, M. Influence of family structure on Children’s well-being—challenges and pathways to promote positive development. SHS Web Conf. (2023) 180:02008. doi: 10.1051/shsconf/202318002008
25. Németh, Á, and Költő, A. Egészség És Egészségmagatartás Iskoláskorban, 2014; Az Iskoláskorú Gyermekek Egészségmagatartása Elnevezésű, Az Egészségügyi Világszervezettel Együttműködésben Megvalósuló Nemzetközi Kutatás 2014. Évi Felméréséről Készült Nemzeti Jelentés; Health Behaviour In School-Aged Children (Hbsc): A Who-Collaborative Cross-National Study National Report 2014. Budapest: Nemzeti Egészségfejlesztési Intézet (2016).
26. Lasky, P, Buckwalter, KC, Whall, A, Lederman, R, Speer, J, McLane, A, et al. Developing an instrument for the assessment of family dynamics. West J Nurs Res. (1985) 7:40–57. doi: 10.1177/0092055X8500700105
27. Aluja, A, Rolland, JP, Garcia, LF, and Rossier, J. Dimensionality of the Rosenberg self-esteem scale and its relationships with the three-and the five-factor personality models. J Pers Assess. (2007) 88:246–9. doi: 10.1080/00223890701268116
28. Cosma, A, Abdrakhmanova, S, Taut, D, Schrijvers, K, Catunda, C, and Schnohr, C. A focus on adolescent mental health and wellbeing in Europe, Central Asia and Canada. Health behaviour in school-aged children international report from the 2021/2022 survey. World Health Organization; (2023).
29. Bleidorn, W, Arslan, RC, and Denissen, JJ. Age and gender differences in self-esteem-a cross-cultural window. J Pers Soc Psychol. (2016) 111:396–410. doi: 10.1037/pspp0000078
30. Kiviruusu, O, Huurre, T, Aro, H, Marttunen, M, and Haukkala, A. Self-esteem growth trajectory from adolescence to mid-adulthood and its predictors in adolescence. Adv Life Course Res. (2015) 23:29–43. doi: 10.1016/j.alcr.2014.12.003
31. Moksnes, UK, and Espnes, GA. Self-esteem and emotional health in adolescents – gender and age as potential moderators. Scand J Psychol. (2012) 53:483–9. doi: 10.1111/sjop.12021
32. Yoon, Y, Eisenstadt, M, Lereya, ST, and Deighton, J. Gender difference in the change of adolescents' mental health and subjective wellbeing trajectories. Eur Child Adolesc Psychiatry. (2023) 32:1569–78. doi: 10.1007/s00787-022-01961-4
34. Singh, S, Roy, D, Sinha, K, Parveen, S, Sharma, G, and Joshi, G. Impact of COVID-19 and lockdown on mental health of children and adolescents: a narrative review with recommendations. Psychiatry Res. (2020) 293:113429. doi: 10.1016/j.psychres.2020.113429
35. Chadi, N, Ryan, NC, and Geoffroy, MC. COVID-19 and the impacts on youth mental health: emerging evidence from longitudinal studies. Can J Public Health. (2022) 113:44–52. Les impacts de la pandemie de la COVID-19 sur la sante mentale des jeunes: donnees emergeantes des etudes longitudinales. doi: 10.17269/s41997-021-00567-8
36. Mazrekaj, D, and De Witte, K. The impact of school closures on learning and mental health of children: lessons from the COVID-19 pandemic. Perspect Psychol Sci. (2023) 19:686–93. doi: 10.1177/17456916231181108
37. Orban, E, Li, LY, Gilbert, M, Napp, AK, Kaman, A, Topf, S, et al. Mental health and quality of life in children and adolescents during the COVID-19 pandemic: a systematic review of longitudinal studies. Front Public Health. (2023) 11:1275917. doi: 10.3389/fpubh.2023.1275917
38. Widnall, E, Adams, EA, Plackett, R, Winstone, L, Haworth, CMA, Mars, B, et al. Adolescent experiences of the COVID-19 pandemic and school closures and implications for mental health, peer relationships and learning: a qualitative study in south-West England. Int J Environ Res Public Health. (2022) 19:163. doi: 10.3390/ijerph19127163
39. Lukoševičiūtė, J, and Šmigelskas, K. Mental health during COVID-19 pandemic: qualitative perceptions among Lithuanian adolescents. Int J Environ Res Public Health. (2022) 19:86. doi: 10.3390/ijerph19127086
40. Dale, R, Jesser, A, Pieh, C, O'Rourke, T, Probst, T, and Humer, E. Mental health burden of high school students, and suggestions for psychosocial support, 1.5 years into the COVID-19 pandemic in Austria. Eur Child Adolesc Psychiatry. (2023) 32:1015–24. doi: 10.1007/s00787-022-02032-4
41. Stewart, TM, Fry, D, Wilson, J, McAra, L, Hamilton, S, King, A, et al. Adolescent mental health priorities during the Covid-19 pandemic. School Ment Health. (2023) 15:247–59. doi: 10.1007/s12310-022-09547-w
42. Orth, U, Erol, RY, and Luciano, EC. Development of self-esteem from age 4 to 94 years: a meta-analysis of longitudinal studies. Psychol Bull. (2018) 144:1045–80. doi: 10.1037/bul0000161
43. Huang, C. Mean-level change in self-esteem from childhood through adulthood: Meta-analysis of longitudinal studies. Rev Gen Psychol. (2010) 14:251–60. doi: 10.1037/a0020543
44. Ozer, S. Social support, self-efficacy, self-esteem, and well-being during COVID-19 lockdown: a two-wave study of Danish students. Scand J Psychol. (2024) 65:42–52. doi: 10.1111/sjop.12952
45. Metsäpelto, R-L, Zimmermann, F, Pakarinen, E, Poikkeus, A-M, and Lerkkanen, M-K. School grades as predictors of self-esteem and changes in internalizing problems: a longitudinal study from fourth through seventh grade. Learn Individ Differ. (2020) 77:101807. doi: 10.1016/j.lindif.2019.101807
46. Lepp, L, Aaviku, T, Leijen, A, Pedaste, M, and Saks, K. Teaching during COVID-19: the decisions made in teaching. Educ Sci. (2021) 11:47. doi: 10.3390/educsci11020047
47. Stentiford, L, Koutsouris, G, and Allan, A. Girls, mental health and academic achievement: a qualitative systematic review. Educ Rev. (2023) 75:1224–54. doi: 10.1080/00131911.2021.2007052
48. Birndorf, S, Ryan, S, Auinger, P, and Aten, M. High self-esteem among adolescents: longitudinal trends, sex differences, and protective factors. J Adolesc Health. (2005) 37:194–201. doi: 10.1016/j.jadohealth.2004.08.012
49. Kaveh Farsani, Z, Kelishadi, R, and Beshlideh, K. Study of the effect of family communication and function, and satisfaction with body image, on psychological well-being of obese girls: the mediating role of self-esteem and depression. Child Adolesc Psychiatry Ment Health. (2020) 14:39. doi: 10.1186/s13034-020-00345-3
50. Sabah, A, Aljaberi, MA, Hajji, J, Fang, C-Y, Lai, Y-C, and Lin, C-Y. Family communication as a mediator between family resilience and family functioning under the quarantine and COVID-19 pandemic in Arabic countries. Children. (2023) 10:742. doi: 10.3390/children10111742
51. Zapf, H, Boettcher, J, Haukeland, Y, Orm, S, Coslar, S, and Fjermestad, K. A systematic review of the association between parent-child communication and adolescent mental health. JCPP Adv. (2023) 4:205. doi: 10.1002/jcv2.12205
52. Dubow, EF, and Rubinlicht, M. Coping In: BB Brown and MJ Prinstein, editors. Encyclopedia of adolescence. New York: Academic Press (2011). 109–18.
53. Cormier, A-A, and Rossi, M. Is children’s wellbeing different from adults’ wellbeing? Can J Philos. (2019) 49:1146–68. doi: 10.1080/00455091.2019.1619354
54. Schutte, S, Chastang, JF, Malard, L, Parent-Thirion, A, Vermeylen, G, and Niedhammer, I. Psychosocial working conditions and psychological well-being among employees in 34 European countries. Int Arch Occup Environ Health. (2014) 87:897–907. doi: 10.1007/s00420-014-0930-0
55. Voitsidis, P, Kerasidou, MD, Nikopoulou, AV, Tsalikidis, P, Parlapani, E, Holeva, V, et al. A systematic review of questionnaires assessing the psychological impact of COVID-19. Psychiatry Res. (2021) 305:114183. doi: 10.1016/j.psychres.2021.114183
56. Ross, DA, Hinton, R, Melles-Brewer, M, Engel, D, Zeck, W, Fagan, L, et al. Adolescent well-being: a definition and conceptual framework. J Adolesc Health. (2020) 67:472–6. doi: 10.1016/j.jadohealth.2020.06.042
Keywords: well-being, self-esteem, adolescent, COVID-19, school lockdown
Citation: Major D, Falus M, Árva D, Eorsi D, Terebessy A, Tabak AG and Fazekas-Pongor V (2024) The effect of school lockdown on well-being and self-esteem of adolescents during the COVID-19 pandemic in Hungary. Front. Public Health. 12:1474893. doi: 10.3389/fpubh.2024.1474893
Edited by:
Mosad Zineldin, Linnaeus University, SwedenReviewed by:
Aleksandar Višnjić, University of Niš, SerbiaNazanin Azmi-Naei, Shahroud University of Medical Sciences, Iran
Copyright © 2024 Major, Falus, Árva, Eorsi, Terebessy, Tabak and Fazekas-Pongor. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: David Major, bWFqb3IuZGF2aWRAc2VtbWVsd2Vpcy5odQ==
†These authors have contributed equally to this work and share last authorship