 Hao Li1,2
Hao Li1,2 Weihong Zeng1,2*
Weihong Zeng1,2*- 1Jinhe Center for Economic Research, Xi’an Jiaotong University, Xi’an, Shaanxi, China
- 2Center for Aging Health Research, Xi’an Jiaotong University, Xi’an, Shaanxi, China
Objectives: The relationship between sedentary behaviors and elevated blood pressure remains inconclusive, and the socioeconomic mechanisms underlying the linkage are rarely discussed. Since retirement is often associated with behavioral changes that impact health, this study aims to provide evidence on changes in leisure sedentary time after the statutory retirement age on elevated blood pressure, along with the socioeconomic mechanisms.
Methods: We utilized data from five waves (2004–2015) of the China Health and Nutrition Survey (CHNS), focusing on males aged 55–65 employed in the formal sector. Leisure sedentary time, the independent variable, was measured based on self-reported data, while diastolic (DBP) and systolic (SBP) blood pressure were the dependent variables. Using statutory retirement policy as an exogenous variation, we employed a continuous difference-in-differences (DID) framework and a propensity score matching difference-in-differences (PSM-DID) approach to examine the relationship between changes in leisure sedentary time after the statutory retirement age and elevated blood pressure. The analysis was conducted using ordinary least squares (OLS). To address potential endogeneity, we applied the instrumental variable (IV) method via two-stage least squares (2SLS).
Results: Our findings indicate an increase in diastolic blood pressure after statutory retirement, attributed to increased leisure sedentary time. However, there was no significant increase in systolic blood pressure. Moreover, physical activity did not appear to offset this rise in blood pressure, while higher educational attainment and having family members employed in the medical field helped mitigate its negative effects.
Conclusion: This study highlights the potential adverse impact of increased leisure sedentary time on diastolic blood pressure among middle-aged men in the formal sector, while also exploring the socioeconomic factors that may alleviate these effects. These results provide a foundation for public health initiatives aimed at addressing the rising prevalence of sedentary behavior and its association with blood pressure issues.
1 Introduction
Elevated blood pressure is a leading modifiable risk factor of numerous health risks and is associated with 10.8 million deaths per year worldwide (1). In China, the prevalence of elevated blood pressure has risen significantly, now affecting approximately a quarter of all adults and about half of older adults (2, 3). It is widely recognized that elevated blood pressure is related to age, with the highest incidence occurring among older adults (4).
As the population ages, the baby boomers born in the 1950s and 1960s in China are gradually retiring. Retirement marks a significant turning point in an individual’s life (5), signifying the end of employment and the onset of aging. This transition prompts people to re-plan their lives, potentially altering their behaviors and impacting their health. On the one hand, retirement can negatively affect health, as some researchers have found associations with reduced physical activity, increased sedentary behaviors (e.g., TV watching), more frequent insomnia, and increased smoking and drinking (6). On the other hand, retirement can also positively impact health through increased exercise, sufficient sleep, and healthier meal preparation (7).
The etiology of elevated blood pressure is multifaceted, influenced by both genetic predispositions and lifestyle factors. Besides age, lifestyle changes such as smoking (8), alcohol consumption (9), and dietary imbalances (10) are primary contributors. However, the relationship between sedentary behavior and elevated blood pressure is often overlooked. Adults spend an alarming 9–10 h/day sedentary (11). Accordingly, the phrase “sitting is the new smoking” has been coined by popular press to describe a current epidemic of many nations (12). Sedentary behavior increased with age, and older adults are those who spend more time on sitting (13). Retirement means more leisure time; increased leisure time post-retirement may lead to more unhealthy behaviors such as sedentary activities, especially watching TV (14). However, studies on the association between sedentary behaviors and elevated blood pressure have reported mixed findings, which highlight the limitations of previous studies, especially confounding factors and measurement error (15). For example, one study found no significant link between sedentary behaviors and elevated blood pressure (16), while others, such as Guo et al. and Chauntry et al., established connections between total sedentary behavior and elevated blood pressure (17, 18).
Given the limitations of previous studies, this paper utilizes the statutory retirement policy as an exogenous variation to examine the effect of changes in leisure sedentary time (e.g., TV watching) before and after the statutory retirement age on elevated blood pressure using a continuous difference-in-differences (DID) framework combined with propensity score matching difference-in-differences (PSM-DID) approach. Additionally, to address concerns about the endogeneity, we use instrumental variable (IV) method. We also conduct several checks to ensure the validity of our method, including sample considerations, parallel trend tests, placebo tests, and robustness checks.
The statutory retirement age in China was established in the 1950s, mandating retirement in the formal sectors such as government, public services, state-owned, and collectively owned enterprises. The retirement age is set at 60 for men, 50 for female workers, and 55 for female cadres. This study focuses on men in the formal sector as research shows that many women opt for early retirement before reaching the standard retirement age (19), while men typically retire at the mandatory age of 60. One study observed a significant increase in the proportion of retired males at age 60, but not among females at ages 50 or 55 (20). Additionally, structural adjustments in state-owned and collectively owned enterprises from the mid-1990s altered urban employment patterns, particularly for women. Women over 40 experienced a sharp decline in labor force participation, with many reporting themselves as retired or permanently withdrawn from the workforce (19). For this reason, including women in this study would not provide reliable conclusions, so we limit our analysis to men in the formal sector (20–23). Moreover, to accurately assess the influence on elevated blood pressure, we focus on males aged 55–65 as elevated blood pressure is generally believed to be related to age, encompassing 5 years before and after the statutory retirement age (21, 24).
This study contributes to the literature in several ways. First, by employing a continuous DID design, PSM-DID approach, and IV method, we offer new evidence on the relationship between leisure sedentary time and elevated blood pressure before and after retirement, filling gaps in the current literature. Second, while most existing studies focus on risk factors such as smoking, drinking, and diet, our study emphasizes the impact of sedentary behavior on blood pressure, providing new insights into this underexplored area.
2 Literature review and hypothesis development
In this section, we review and summarize existing research from two perspectives: the relationships among retirement, sedentary behaviors, and elevated blood pressure, as well as the socioeconomic mechanisms.
Research suggests that retirement consists of three stages: the near-retirement phase, the transition period, and the retirement stability period (25). In most countries, the legal retirement age is fixed, making retirement life predictable. During the pre-retirement stage, workers have expectations or concerns about retirement and make preparations and psychological adjustments for the transition (26). The transition period includes the first few years of retirement. Continuity theory implies that the lifestyle during this period is consistent with the pre-retirement stage, as it takes time to form new habits (27). For example, a study found a greater increase in television viewing time after retirement among those who had less physically demanding jobs (28). Additionally, increased leisure time post-retirement may lead to more risky behaviors such as smoking, drinking, or sedentary activities. Several studies have found that sedentary time increases during the transition period (29–31), especially television viewing (28, 32, 33). For example, one study found that total sedentary time increased by 73 min per day during the transition period, with TV viewing time increasing by 28 min per day (30).
Sedentary behaviors are associated with modern lifestyles and lead to many adverse health outcomes, including elevated blood pressure. Previous literature has documented the correlation between high levels of sedentary time and elevated blood pressure (34). Contemporary evidence shows a strong association between occupational sedentary behavior and elevated blood pressure (35). Additionally, high levels of leisure sedentary time have been linked to elevated blood pressure (36). For instance, individuals who spent more than 3 h per day watching television had a significantly higher risk of elevated blood pressure compared to those who watched television for 0–1 h per day (37). Blood pressure is categorized into diastolic and systolic blood pressure. Some studies have found that increased sedentary time is associated with higher diastolic blood pressure (18, 38), with limited association to systolic blood pressure (39). Therefore, we propose the following hypothesis:
Hypothesis 1: Prolonged sedentary time after retirement is associated with higher diastolic blood pressure but not with higher systolic blood pressure.
Research on the underlying mechanisms is limited and mainly focuses on biological dimensions. For example, watching television often involves prolonged periods of uninterrupted sitting, especially after dinner (40). This increases the risk of elevated blood glucose and triglyceride levels (41). High blood sugar leads to chronic inflammation and oxidative stress, further contributing to elevated blood pressure (42). However, biological mechanisms limit the possibility of intervention. From a socioeconomic perspective, some literature has documented the moderating effect of physical activity on the association between sedentary behaviors and blood pressure (43), whereas most studies distinguish between sedentary behaviors and inactivity, suggesting that physical activity is unlikely to offset the adverse effects of sedentary behaviors on blood pressure changes (44, 45). For example, one person may engage in the recommended amount of physical activity every day (not physically inactive) but still spend a lot of time sitting. Conversely, a person may sit very little but not reach the recommended level of physical activity (physically inactive). Therefore, we propose the following hypothesis:
Hypothesis 2a: Physical activity is unlikely to offset the adverse effect of sedentary behaviors on elevated blood pressure.
Socioeconomic status (SES), traditionally measured through levels of education, income, and occupation, is considered the most fundamental cause of health disparities (46). Although SES indicators are powerful determinants of health, they do not impact health directly but serve as proxies for other determinants (47). Educational attainment is the most important dimension. People with higher levels of education generally have better access to and understanding of health information and adopt healthier lifestyles to promote their health. For example, more education is associated with an improved diet, moderate alcohol consumption, and less sedentary behaviors (47, 48). Additionally, a good education enhances self-care capabilities and increases the likelihood of accessing higher-quality healthcare. Higher educational attainment also leads to better job opportunities, higher wages, and better living standards, facilitating superior healthcare access (49).
Furthermore, health literacy, a key channel linking SES and health outcomes, relates to individuals’ knowledge, motivation, and competencies to access, understand, appraise, and apply health information, and to make appropriate decisions relevant to health promotion, disease prevention, and self-care management (50). Individuals with inadequate health literacy are more likely to report a sedentary lifestyle (51) and elevated blood pressure (52). Medical professionals, with higher health literacy, can provide more effective medical advice to promote health for both their patients and family members. Therefore, we propose the following hypothesis:
Hypothesis 2b: Educational attainment and having family members employed as medical workers are mechanisms through which prolonged sedentary time impacts elevated blood pressure.
3 Data discerption and empirical strategy
3.1 Data
The data used in this paper come from the China Health and Nutrition Survey (CHNS). The CHNS is an ongoing large-scale study aimed at determining how China’s social and economic development affects the health and nutritional status of the country’s population, with 10 rounds of collected data from 1989 to 2015 (i.e., 1989, 1991, 1993, 1997, 2000, 2004, 2006, 2009, 2011, and 2015). Jointly collected by the Chinese Center for Diseases Control and Prevention and the University of North Carolina at Chapel Hill, the CHNS survey randomly selected samples from 12 provinces, covering 12,522–20,878 individuals in each round.
3.2 Variables
3.2.1 Blood pressure
We utilize diastolic blood pressure (DBP) and systolic blood pressure (SBP) as main dependent variables. The CHNS dataset encompasses diastolic blood pressure and systolic blood pressure measurements conducted by professionally trained medical staff for each individual. Specifically, the medical staff measured both the DBP and SBP three times on three consecutive days for each individual (53). We calculate the average DBP and SBP as main dependent variables. In our robustness check, we use the average DBP and SBP from the last two measurements instead of all three, considering that the first measurement might be more susceptible to measurement errors and less reflective of the individual’s “true” underlying blood pressure due to stress or anxiety (54).
3.2.2 Leisure sedentary time
While TV watching is often the most common sedentary activity, sedentary behavior includes various activities, and measuring only TV watching may underestimate total sedentary time. In our study, leisure sedentary behavior was assessed through several questions. Participants were asked, “Do you engage in these sedentary activities?” The listed activities included watching TV, watching videos, and playing video games. Additional questions were asked to determine the time spent on these activities: “How much time do you spend on these activities from Monday to Friday?” and “How much time do you spend on Saturday and Sunday?” Based on these responses, we calculate total leisure sedentary time. Using non-exercise sitting behaviors, especially screen-based activities, is common in research. These measures have demonstrated acceptable reliability and validity (55), and have been widely employed in prior studies (56, 57).
We calculate the independent variable based on equation 1 and winsorize at the 1st and 99th percentiles of their respective sample distributions. The equation is as follows:
According to dependent variable and independent variable, we employ the CHNS from the 2004, 2006, 2009, 2011, and 2015 waves.
3.2.3 Control variables
In our specification, we control for a rich set of individual-, household-, and macro-level characteristics. First, we include individual and household factors such as sleep duration, physical activity, use of antihypertensive drugs, body mass index (BMI), smoking status, drinking status, marital status, and log-transformed annual household income. Second, as diet is linked to elevated blood pressure, we account for key nutritional elements, including average daily intake of dietary fat, carbohydrates, and protein (g/d) (58). We also control for taste preferences (e.g., a preference for salty food) and attitudes toward the relationship between salt intake and blood pressure to reduce omitted variable bias. A strong preference for salty food, combined with the belief that salt does not affect blood pressure, suggests a high-salt diet. Third, we control for mental health and other chronic diseases such as diabetes as they are associated with elevated blood pressure (59, 60). Mental health was assessed using the CHNS dataset, which includes three questions for individuals aged 55 and older: “Do you have as much energy as you did last year?” “Are you as happy now as you were when you were younger?” and “As you age, are things better than you expected?” Each question has five possible responses, scored from 1 to 5. A higher score indicates greater agreement with the statements, and the total score was used as a mental health measure. These questions are simplified versions of indicators from the Symptom Checklist-90 (SCL-90), reflecting the mental health of individuals (61). In addition, blood pressure status is strong associated with elevated blood pressure. Hypertensive population have greater variability in blood pressure than normotensive population (62), especially taking into account sedentary behaviors (63). We also control for occupational sedentary time, as it significantly influences blood pressure (64). Furthermore, we include macro-level variables such as Urbanization, Economic, Health, and House Scores, where higher scores indicate better development. We also account for individual, household, and year fixed effects to control for confounding factors, with age effects absorbed by the fixed effects.
Genetic predisposition can also affect blood pressure (65). Since the CHNS dataset does not provide family health history, we mitigate potential omitted variable bias through three strategies: (1) controlling for individual fixed effects, which capture time-invariant factors such as genetics that could affect both sedentary time and blood pressure; (2) employing an instrumental variable (IV) method; and (3) excluding individuals and regions with a strong preference for salty foods in our robustness checks, as taste preferences tend to be stable and are correlated with elevated blood pressure.
Table 1 presents descriptive statistics for the sample. The average diastolic blood pressure is 83 mmHg, while the average systolic blood pressure is 131 mmHg, indicating that most participants are normotensive. On average, participants engage in 154 min of leisure sedentary time per day and 1,026 min of occupational sedentary time per week before retirement. On average, participants sleep 7.76 h per day and have a mean BMI of 24, with values ranging from 17 to 32. Most people do not prefer salty food and believe that salty food raises blood pressure. The proportions of individuals who exercise, have diabetes, or take antihypertensive drugs are relatively low, with average values of 0.23, 0.08, and 0.20, respectively. About half of the sample smokes or drinks alcohol, and most are married. The average mental health score is 9, ranging from 3 to 15. The average daily intake of dietary fat, carbohydrates, and protein is 85.22 g, 280.73 g, and 74.84 g, respectively, similar to findings from a previous study (66). The average annual household income is 56,016 yuan.
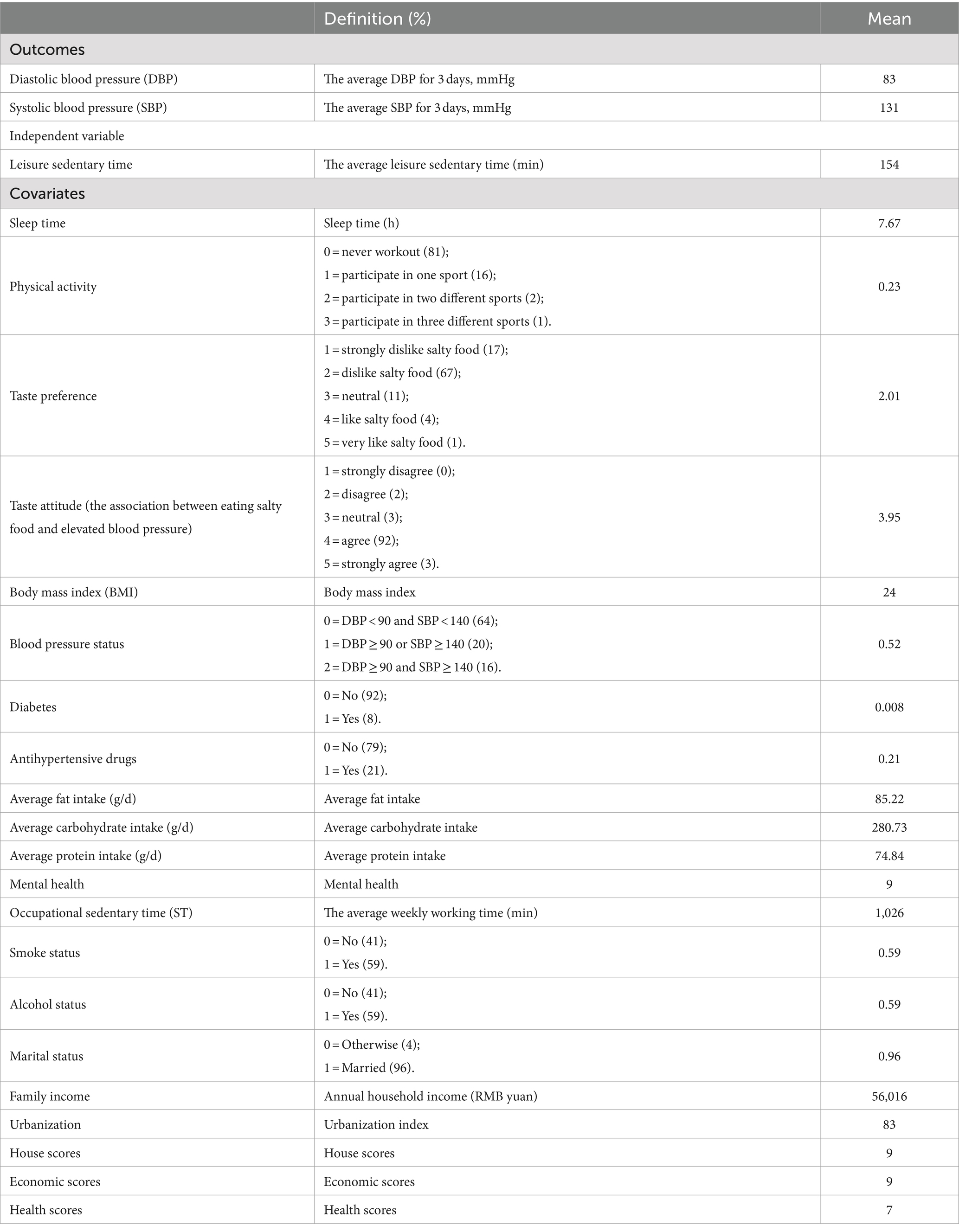
Table 1. Variables definition and descriptive statistics.
Additionally, we provide the evidence of the changes in retirement possibility and leisure sedentary time before and after retirement in Figure 1, and the changes in blood pressure before and after retirement in Figure 2. Figure 1 displays the relationships between the statutory retirement policy and retirement possibility on the left hand, and leisure sedentary time on the right hand. There is a clear positive discontinuity in both retirement possibility and leisure sedentary time before and after retirement. The fitted line in Figure 1 suggests that the discontinuity of retirement possibility is roughly 50 percentage points around the cut-off on the left hand, and the discontinuity of leisure sedentary time is roughly 40 min around the cut-off on the right hand. In sum, Figure 1 demonstrate that leisure sedentary time increases significantly after retirement.
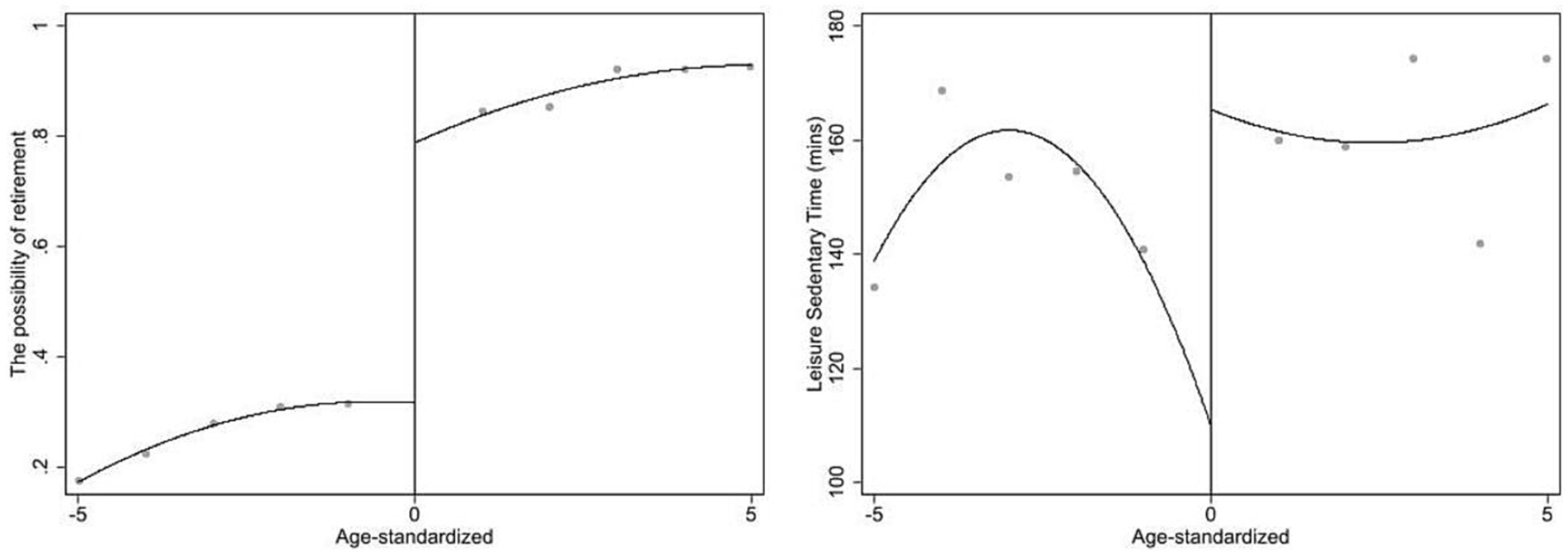
Figure 1. The possibility of retirement and leisure sedentary time before and after law-forced retirement policy.
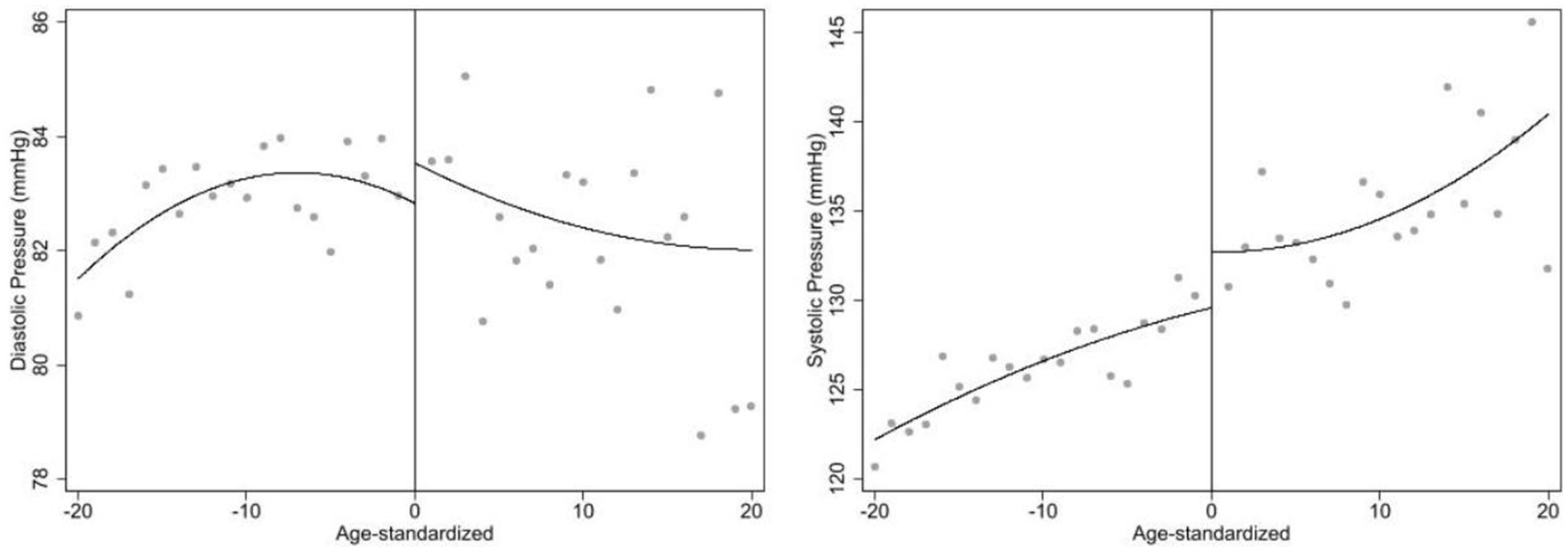
Figure 2. The changes of diastolic blood pressure and systolic blood pressure before and after law-forced retirement policy.
Figure 2 shows changes in blood pressure before and after retirement. Diastolic blood pressure increases on the right, while systolic blood pressure shows a similar increase on the left. After retirement, diastolic blood pressure tends to decline with age, while systolic blood pressure continues to rise, consistent with previous studies that found diastolic blood pressure increases with age until about 55, then declines, while systolic blood pressure continues to rise at least until age 80 (67).
3.3 Empirical strategy
3.3.1 DID framework
This paper uses the statutory retirement policy as an exogenous variation to examine the effect of changes in leisure sedentary time before and after retirement on elevated blood pressure under the continuous difference-in-differences (DID) framework, based on males aged between 55 and 65 who worked in the formal sector.
There are three common ways to define retirement (68): (1) self-reported retirement status. This is not ideal in this study because some people still work for pay after retirement. (2) The statutory retirement policy. This is not ideal because some people may manipulate their retirement status, such as those who are either unhealthy or senior cadres. The former group may retire early (69), while the latter group may delay retirement (70). Thus, we adopt the third definition using the statutory retirement policy as an exogenous variation and excluding the individuals who still work for pay after retirement, and who may manipulate their retirement status.
The regression framework of the continuous DID design is typical written as equation 2 as follows.
Where is dependent variables (the average DBP and the average SBP) for individual at wave , and represents individual leisure sedentary time at wave . is a dummy variable which equals 1 if the subject is from the treatment group, 0 if from the control group. is a set of control variables, and , and represents individual fixed effect, household fixed effect, and year fixed effect. The coefficient of interest is . If retirees who spend more leisure time on sitting elevates blood pressure, we should expect .
3.3.2 PSM-DID framework
DID estimation is most appropriate when the treatment is randomly assigned or at least when observable characteristics can be used to control for the treatment. Although the statutory retirement policy is an exogenous variation, the DID results may be biased by possible unobservable and unchangeable intergroup differences between the treatment and control groups. Therefore, a comparable control group is often constructed using matching techniques. Rosenbaum and Rubin suggest matching on the propensity score (PSM) (71). The PSM can find the most similar samples in the treatment group and the control group for comparison; after matching the samples, both groups do not differ significantly in the observable control variables. Therefore, we employ the propensity score matching difference-in-differences (PSM-DID) framework to further ensure our results’ robustness.
3.3.3 Instrumental variable method
To further improve the validity of our results, we employ instrumental variable (IV) method to address the endogenous concern of leisure sedentary time. While the fixed effect model is generally known to be effective in addressing omitted variable bias, measurement error is main endogeneity in our study, because our independent variable was collected by questionnaires, which is inevitably underestimating leisure sedentary time (72). Therefore, will underestimate if is positive.
To alleviate the endogeneity problem, this paper uses external instrumental variable method and higher moment instruments approach proposed by Lewbel for further regressions (73).
For the external instrumental variable method, we use “Do you like watching TV?” as an instrumental variable. Responses ranged from “dislike very much” as 1 to “like very much” as 5, with higher scores representing greater preference. An ideal instrumental variable must satisfy the following two conditions: relevance and exogeneity (exclusion restriction). In terms of relevance, screen use preference is strongly associated with screen use time. For example, a study in China showed that the screen preference was significantly positively associated with TV viewing time (74). As for exogeneity, screen use preference is a subjective attitude unrelated to health outcomes, satisfying the exclusion restriction.
Moreover, we adopt higher moment instruments approach proposed by Lewbel to construct an internal instrumental variable as the method without relying on external factors. Lewbel suggests using the cubic relationship between independent variables and the mean value of their higher moments. This approach, originally designed for measurement error models, has proven useful in dealing with general correlated-regressor errors and multilevel models. For example, one study examining the effects of TV viewing on children’s cognitive outcomes used Lewbel’s IV to correct for measurement error bias (75). Following this framework, we take the cubic between the individual’s leisure sedentary time and the mean value of their family’s leisure sedentary time as the instrumental variable. This construction is strongly correlated with leisure sedentary time but is highly unlikely to be correlated with elevated blood pressure, thus addressing endogeneity concerns (75).
3.3.4 Moderating effect
Physical activity has been defined as “any bodily movement produced by skeletal muscles that results in energy expenditure (76).” It can be classified into three intensities: light (1.6–2.9 MET (metabolic equivalent of task), such as slow walking or household chores); moderate (3.0–6.0 MET, such as jogging, golfing, light cycling, or dancing); and vigorous (>6.0 MET, such as football, tennis, running, or boxing) (77). Based on these classifications, we explore the moderating effect of physical activity by examining both moderate physical activities (MPA), like walking, jogging, and dancing, and vigorous physical activities (VPA), like football, tennis, basketball, and badminton. Specifically, we use interaction terms between physical activity time and the independent variable to assess these moderating effects.
Socioeconomic status (SES) is defined as an individual’s or group’s position within a hierarchical social structure, reflecting social class and status (78). In this study, we focus on families with low educational attainment and family members who are not employed as medical workers for two key reasons. First, there are relatively few individuals in our dataset with high educational attainment or who work as medical professionals, which could lead to unstable results for this group (less than 5% of individuals are medical professionals). Second, these individuals likely have more accurate health perceptions, and focusing solely on them may yield insignificant findings. Instead, we aim to show that individuals with low educational attainment and families without medical workers experience more pronounced changes in blood pressure.
4 Empirical results
4.1 DID and PSM-DID framework
Table 2 presents the estimates of the effect of leisure sedentary time on elevated blood pressure. The first two columns use the continuous DID model, while the last two columns use the PSM-DID model. Columns (1) and (3) indicate significant positive effects of increased leisure sedentary time after retirement on diastolic blood pressure, passing the 1% significance tests. Specifically, the results show an average increase of 0.011 mmHg in diastolic blood pressure in column (1) and (3). A back-of-the-envelope calculation suggests that each additional hour of sedentary behavior per day significantly increase in diastolic blood pressure by 0.66 mmHg on average. Our work is similar to Lee and Wong, who found that each hour increase in self-reported sedentary behavior was associated with increase in diastolic blood pressure of 0.20 mmHg (79). In contrast, columns (2) and (4) show that increased leisure sedentary time is unlikely to affect systolic blood pressure after retirement. These findings support Hypothesis 1.
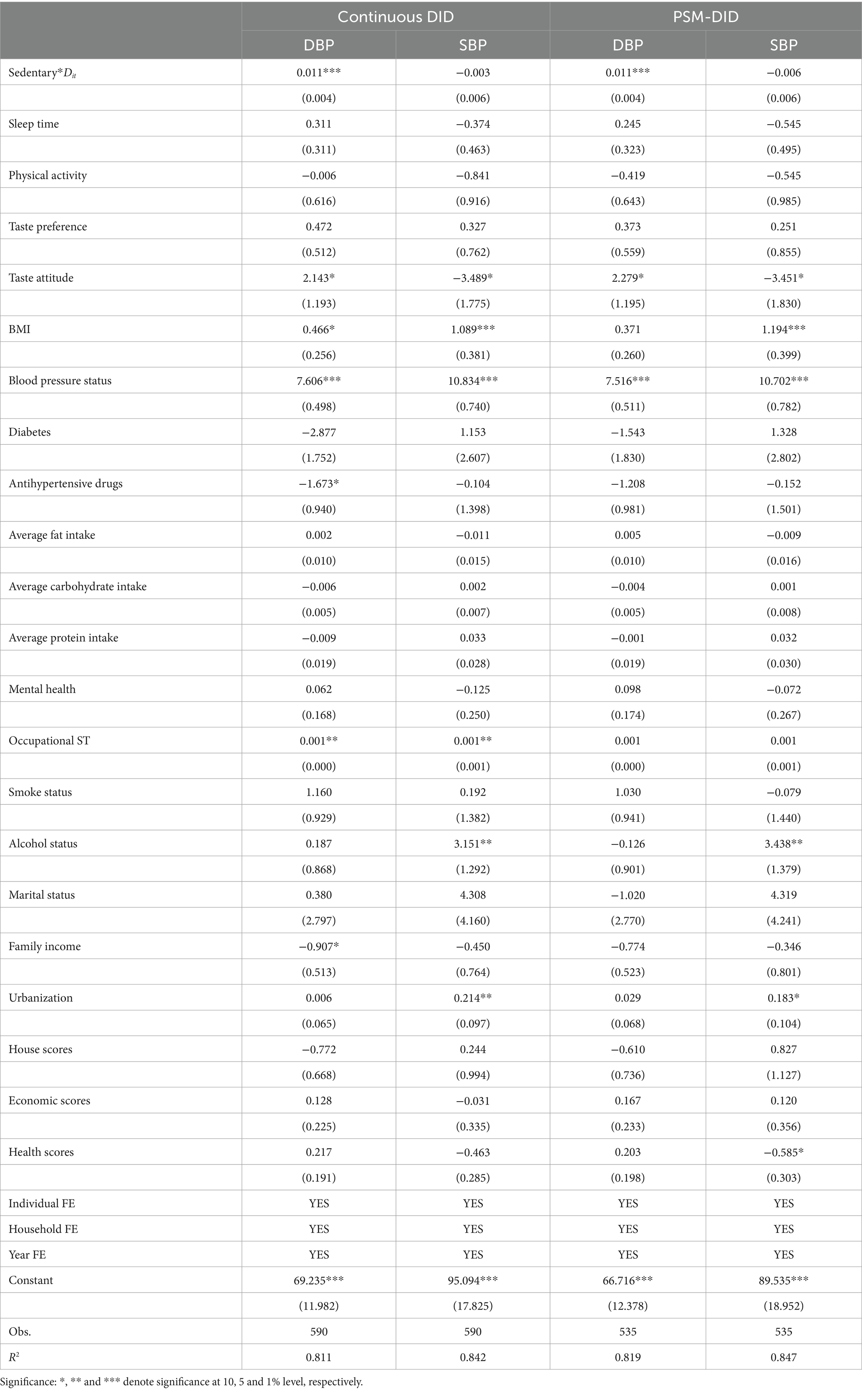
Table 2. The effect of leisure sedentary time on elevated blood pressure.
Additionally, two assumptions must be met when using the propensity score matching: the balance assumption and the common support assumption. The balance assumption requires that the matching variables balance the data well, meaning no significant difference exists between the treatment and control groups after matching. The common support assumption ensures sufficient overlap between the treatment and control group samples, allowing for adequate matching.
Figure 3 provides the results of these assumption tests. The balance assumption test, shown on the left, indicates that standardized biases are largely reduced, with all selection biases below 10%, suggesting effective elimination of selection bias by matching. Our balance assumption test excludes occupational sedentary time and family income, as the former is zero after retirement and the latter significantly reduces after retirement. The common support assumption test, shown on the right, demonstrates that most samples fall within the common value range, indicating minimal sample loss after matching and that the common support assumption is met.
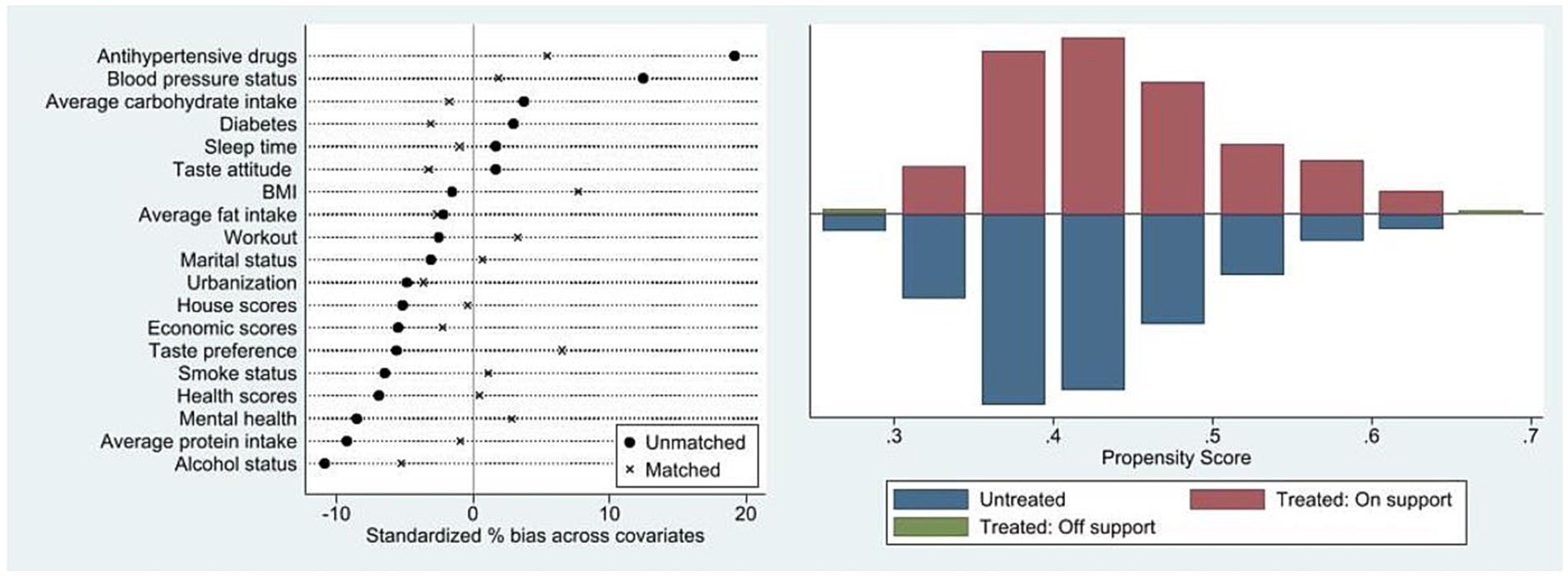
Figure 3. Results of the balance assumption test & results of the common assumption test.
4.2 Instrumental variable method
Possible endogeneity may arise from measurement error bias. To alleviate this issue, this paper uses three additional checks to ensure the robustness, including external instrumental variable method (by using Preference for watching TV), higher moment instruments approach (by using Lewbel’s IV), and a combination of both methods.
Table 3 presents the results from the external instrumental variable method. Column (3) shows the first-stage IV estimates, indicating a significant positive relationship between the instrument (preference for watching TV) and the endogenous independent variable (leisure sedentary time). The first-stage F-test yields an F-statistic of 14.40, which exceeds the threshold for weak instruments, as suggested by Stock and Yogo (80). Additionally, the p-value of the Kleibergen-Paap rk LM statistic is 0.00, rejecting the null hypothesis and confirming the validity of the instrument. The second-stage results, shown in columns (1) and (2), demonstrate that increased leisure sedentary time after retirement has a significant positive effect on diastolic blood pressure (column 1). The effect on systolic blood pressure (column 2), while positive, is not statistically significant. Specially, the coefficient in column (1) is larger than those in columns (1) and (3) of Table 2, suggesting a potential downward bias in the estimates when endogeneity is not addressed. Then, the positive coefficient in column (2) implies that increased leisure sedentary time also affects systolic blood pressure after adjusting for endogeneity, consistent with the trend shown in Figure 2.
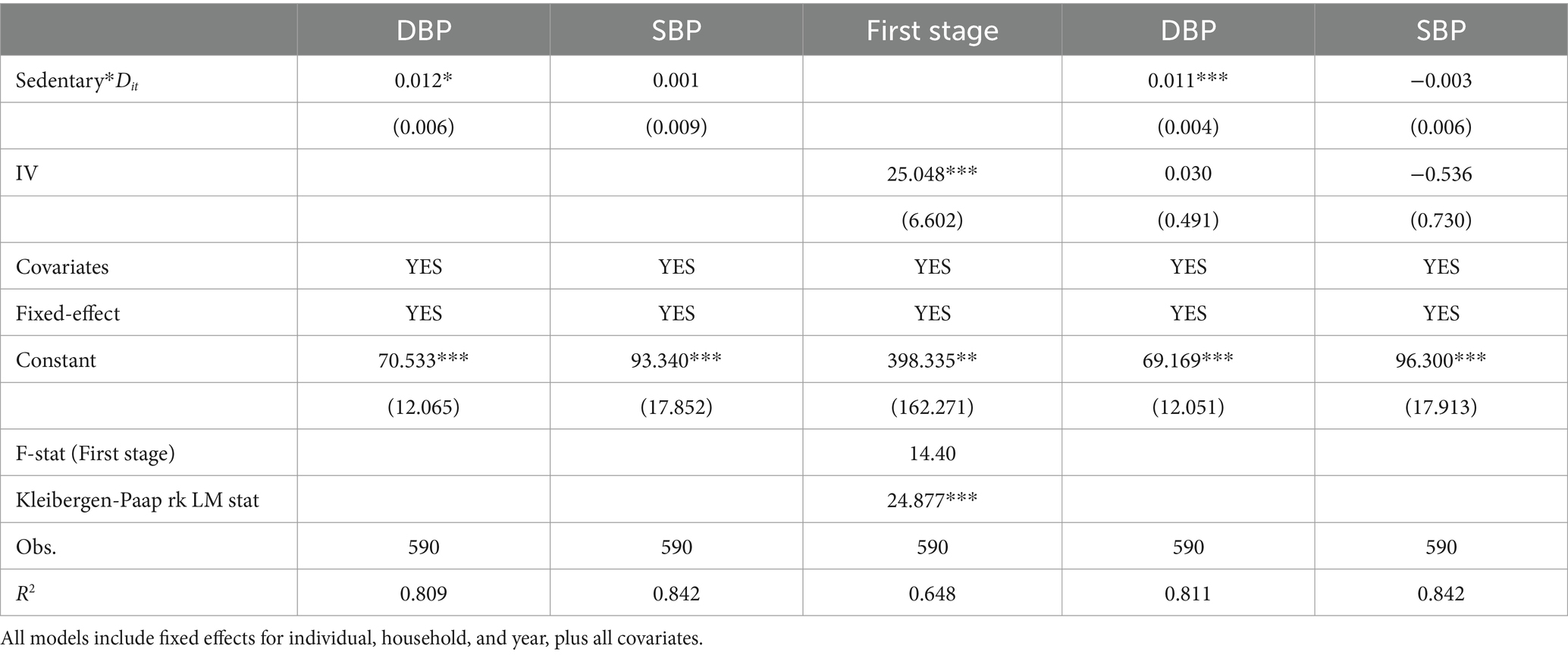
Table 3. Endogenous test of the effect of leisure sedentary time on elevated blood pressure (preference for watching TV).
To further validate the instrumental variable’s effectiveness, we conduct a reduced form regression, following the approach of Acemoglu et al. (81). Columns (4) and (5) include both the independent variable and the instrumental variable in the model. We find that the coefficient of IV is insignificant after controlling for the independent variable, which, to some extent, supports that the IV will not directly affect dependent variable in ways other than independent variable.
Similarly, Table 4 reports the results from the higher moment instruments approach, which align with the earlier findings. Table 5 combines the external instrumental variable method with the higher moment instruments approach, and the results remain consistent. Thus, our primary conclusion—that increased leisure sedentary time raises diastolic blood pressure—is robust after addressing endogeneity.
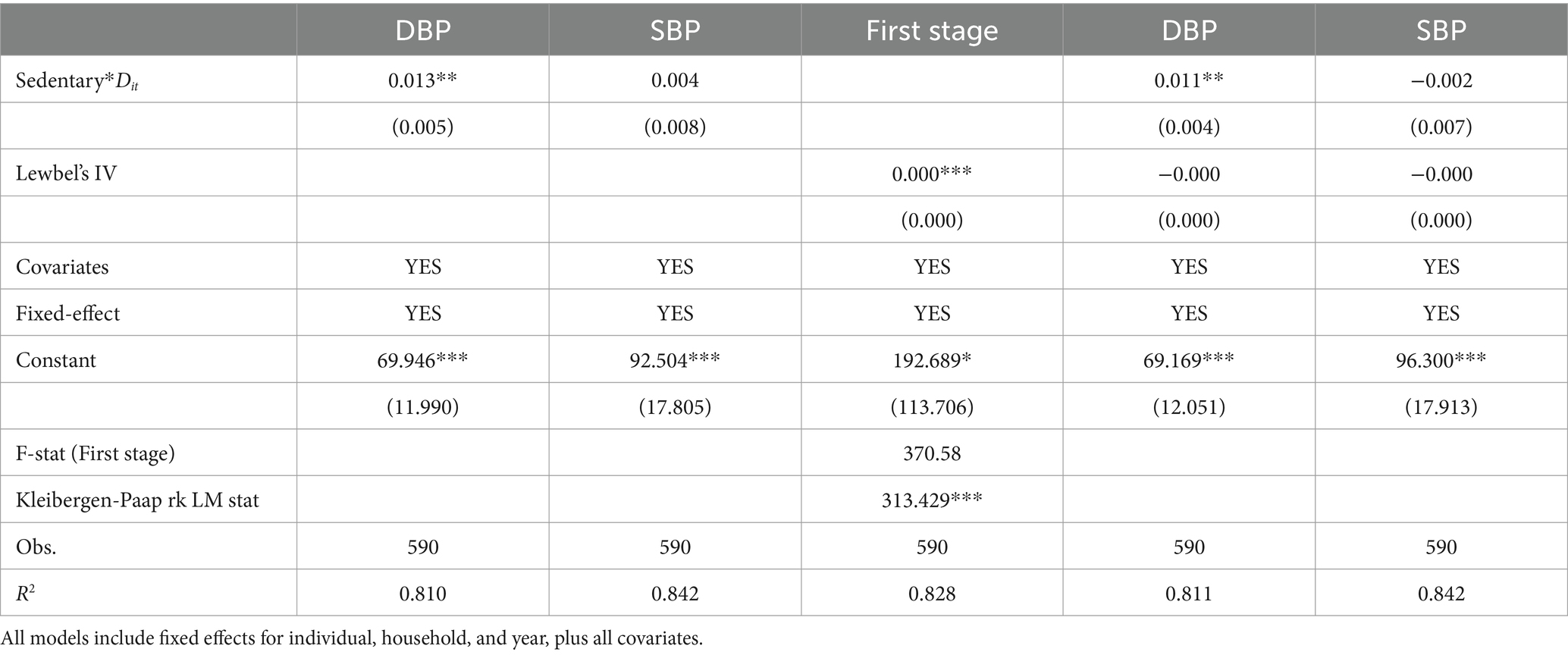
Table 4. Endogenous test of the effect of leisure sedentary time on elevated blood pressure (Lewbel’s IV).
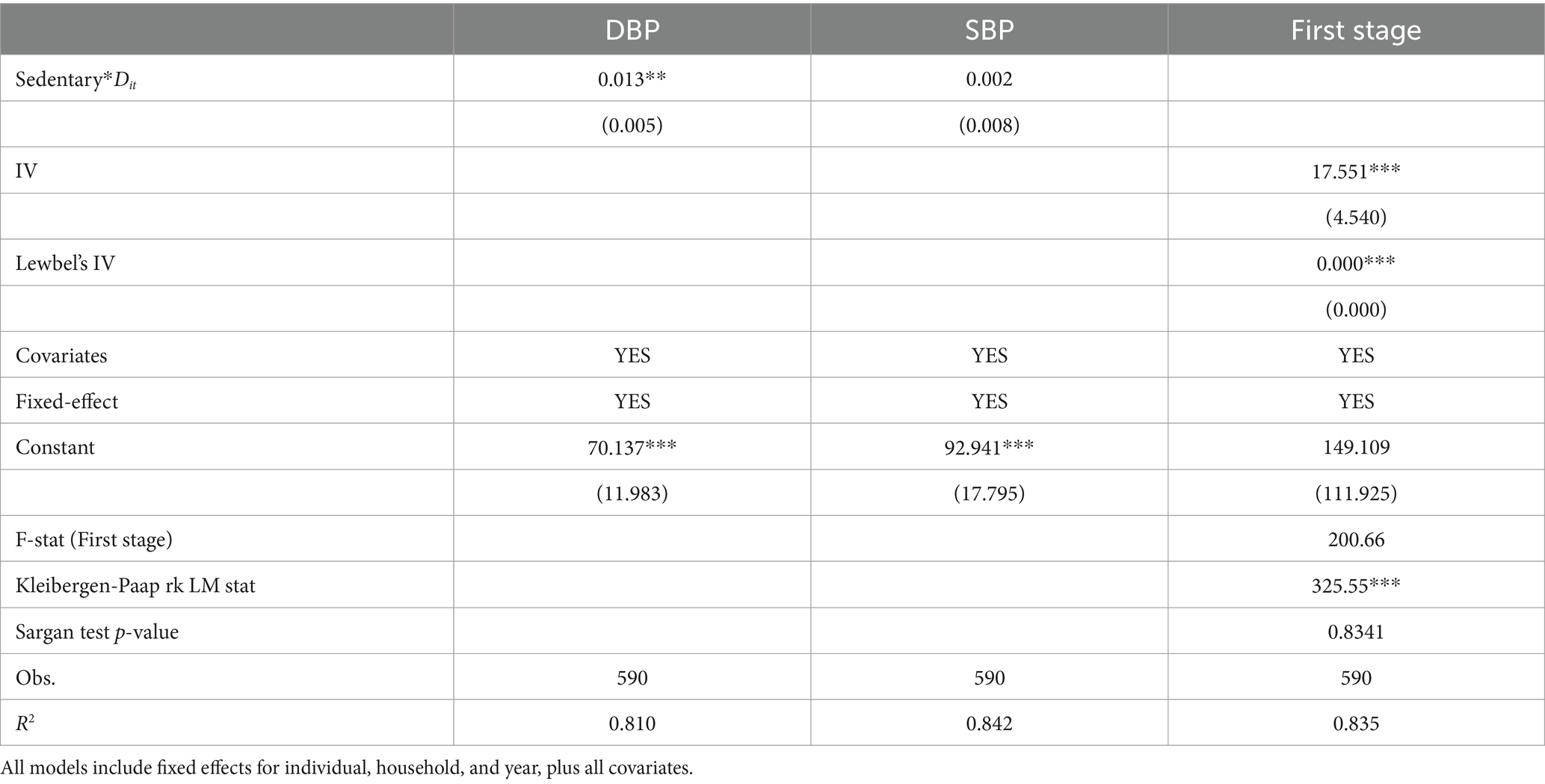
Table 5. Endogenous test of the effect of leisure sedentary time on elevated blood pressure (preference for watching TV + Lewbel’s IV).
Moving to column (3) of Table 5, we provide the tests regarding relevance and exogeneity. The first stage estimates show that we reject the hypothesis of the instruments are weak. Concurrently, Sargan test p-values exceed 0.1, confirming the exogeneity of the instrumental variables. Hence, our instrumental variable selection is reasonable.
4.3 Validity of DID model
We then perform a series of checks to bolster the validity of our methods. First, we address potential concerns about sample composition. We limit our analysis to white-collar male workers, identified as those in senior professional/technical, junior professional/technical, administrative/executive/managerial, or office staff roles. We also exclude individuals living in rural areas, as urban statutory retirement policies are more stringent. The first two columns of Table 6 present results for white-collar male workers, while the last two columns show results for individuals living in urban areas. Our findings remain consistent with our expectations.
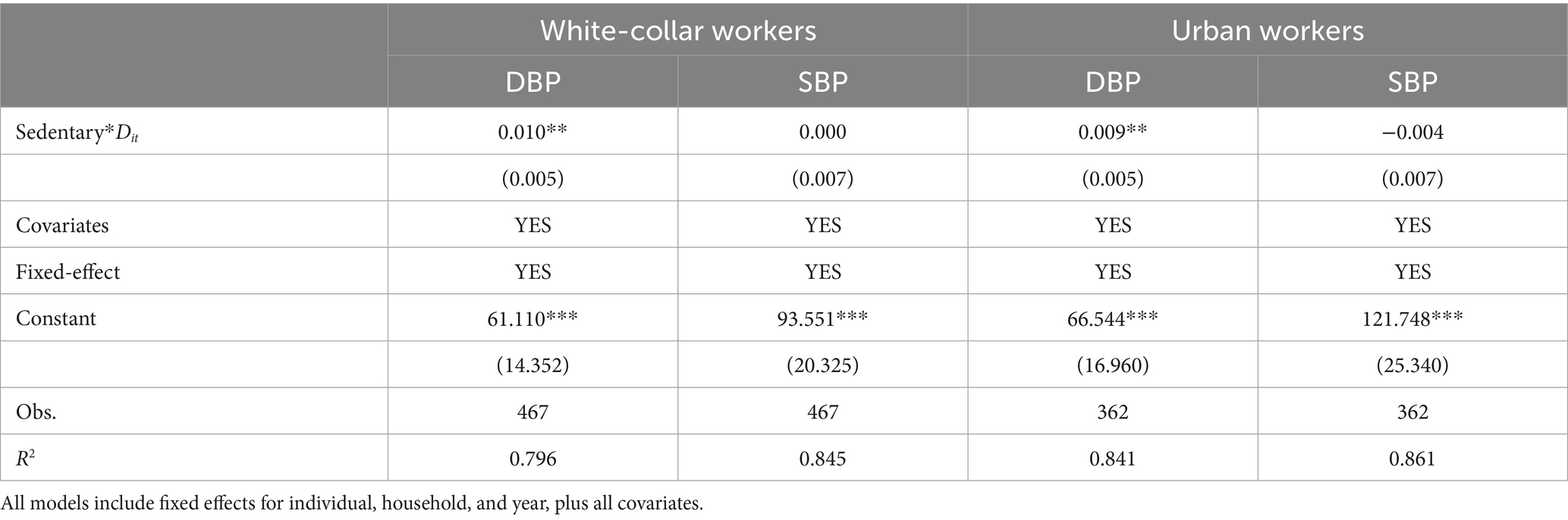
Table 6. DID results-address the sample issue.
The identification assumption of the continuous DID method requires comparability between the treatment group and the control group. Therefore, to address a potential concern about the parallel trend assumption, we conduct an event study analysis and the empirical model (see Equation 3) used for this analysis is:
The results, visualized in Figure 4, show that prolonged sedentary time during the transition period of retirement elevates diastolic blood pressure. However, there is no significant effect on systolic blood pressure changes before and after retirement, supporting the parallel trend assumption.
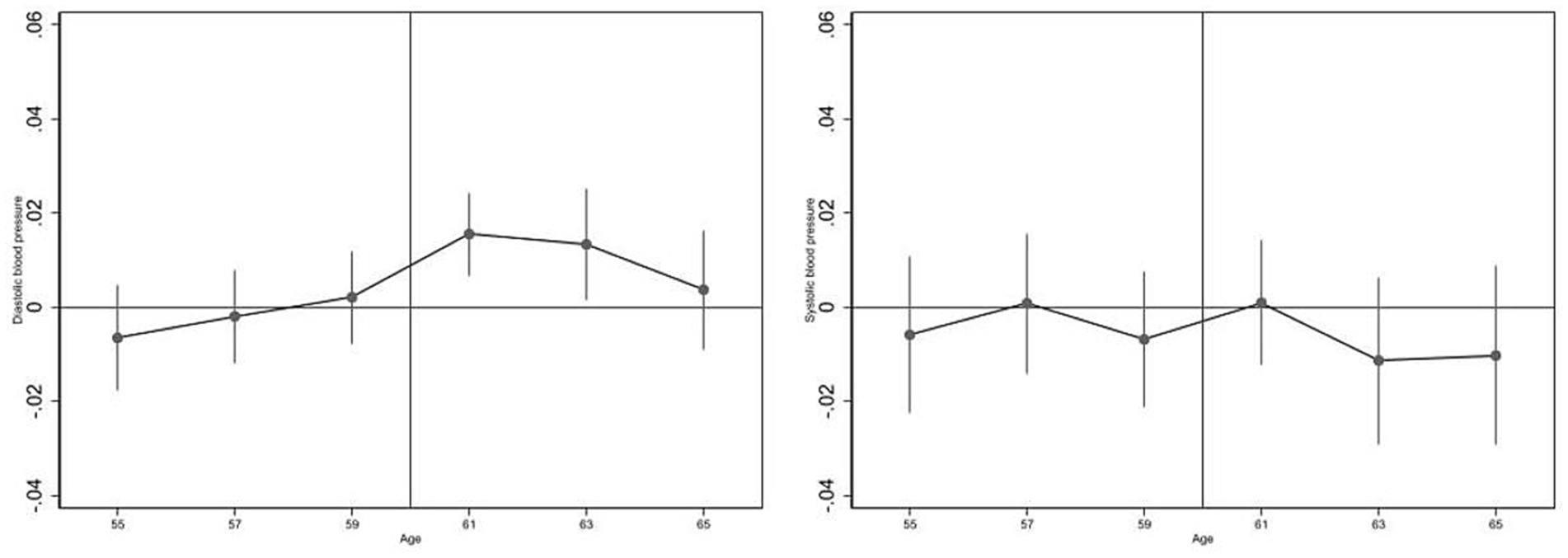
Figure 4. Event-study analyses of parallel trend tests.
Finally, we examine our identification assumption using placebo tests. One placebo cut-off sets the retirement age for males in the formal sectors at 55 instead of 60, and another sets the retirement age for males in the informal sectors at 60. The results in Table 7 indicate no significant blood pressure changes from leisure sedentary time among “retirees,” specifically 55-year-old males in the formal sectors and 60-year-old males in the informal sectors.
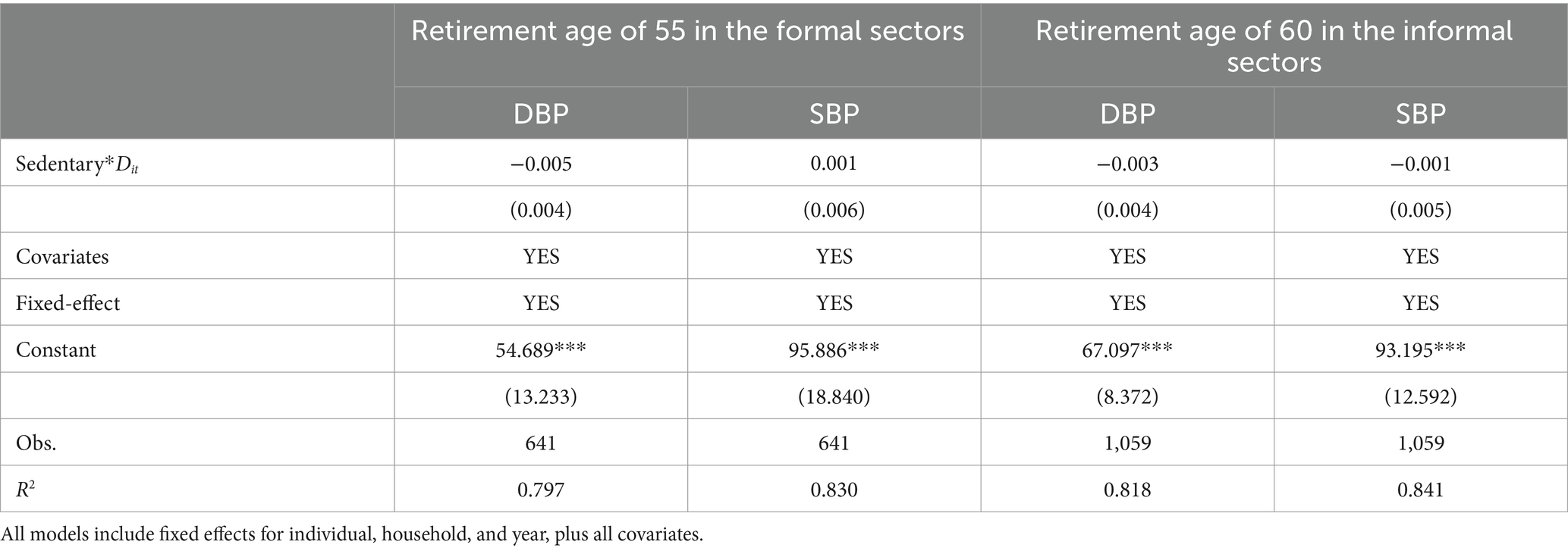
Table 7. DID results-placebo tests.
5 Moderating effect
We explore the mechanisms through which leisure sedentary time may lead to elevated blood pressure. First, we assess the role of physical activity. If increased physical activity effectively reduces elevated blood pressure, we would expect the interaction terms to be negative and statistically significant. However, Table 8 shows no significant moderating effect, supporting Hypothesis 2a. Our findings align with a systematic review that concluded sedentary behavior is not mediated by time spent in physical activity (82). Next, we examine the moderating effect of SES, focusing on individuals with low educational attainment and those whose family members do not work in the medical field. According to Hypothesis 2b, we predict that the effect on diastolic blood pressure in Table 9 will be greater than in Table 2. As expected, Table 9 demonstrates that educational attainment and support from medical professionals can mitigate elevated blood pressure. These findings support the view that SES is a “fundamental cause” of health (83).
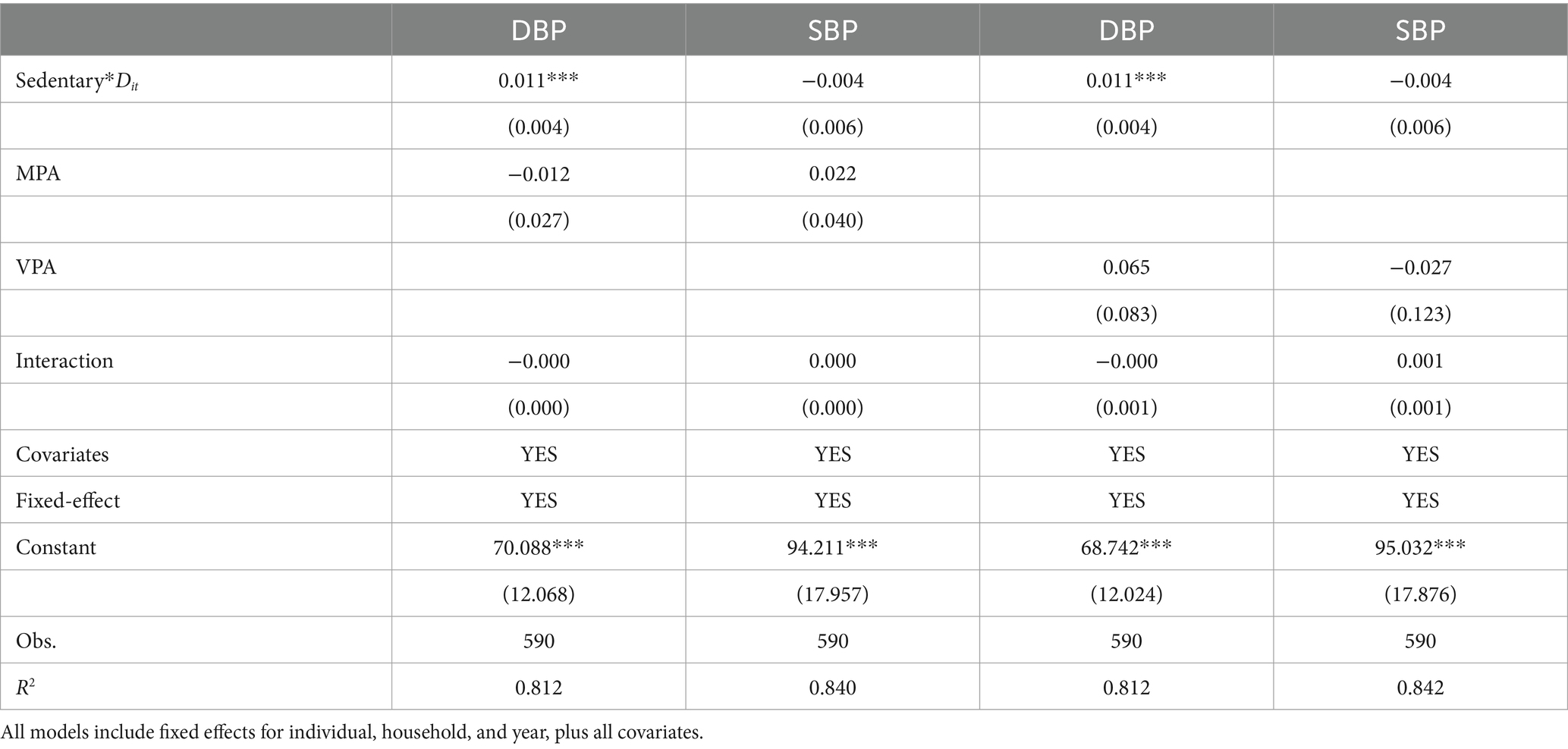
Table 8. Moderating effect-physical activities as moderators.
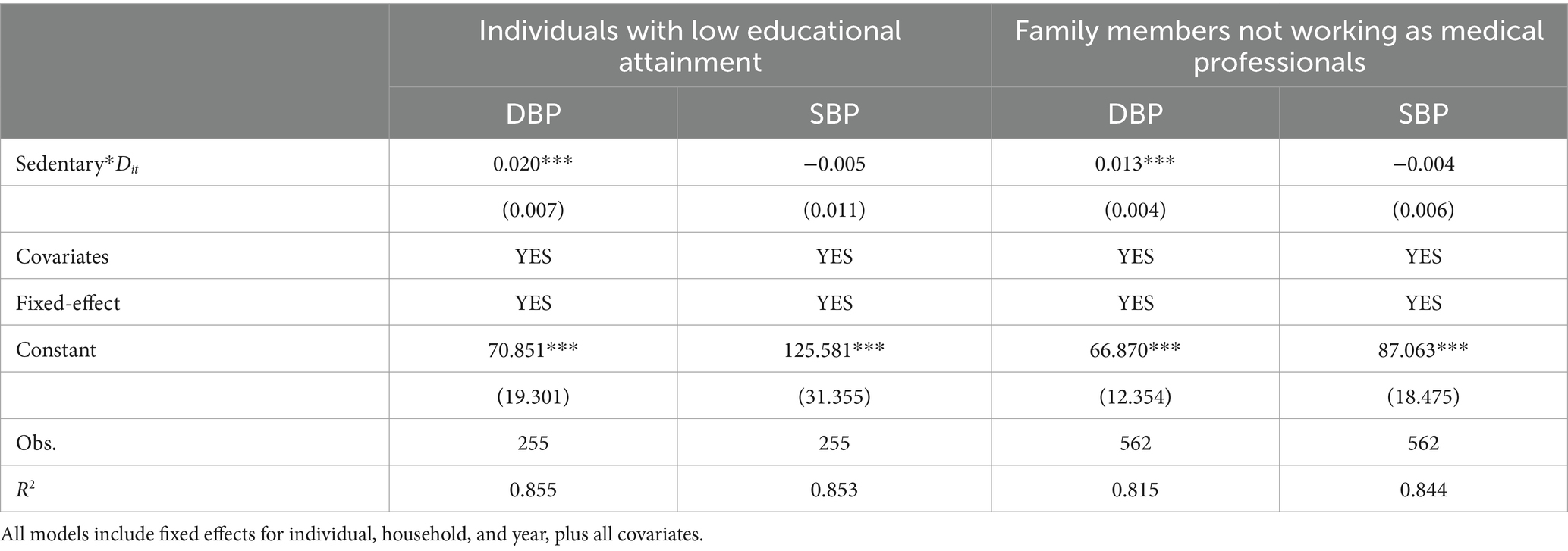
Table 9. Moderating effect-SES as moderators.
6 Robustness checks
6.1 Subsample
One limitation of this paper is we lack the blood pressure information of agents’ family members, which may underestimate our result. To alleviate this concern, we rule out individuals who (1) live in Beijing and Shanghai (the highest hypertension prevalence provinces), and Guizhou (the lowest hypertension awareness province) (84), and Heilongjiang and Liaoning (traditional high salt intake provinces), and strongly like and like salty food; (2) are obesity (BMI over 28); (3) are diagnosed with diabetes. Table 10 reports the results of subsample. Panel A reports the findings for individuals living in the excluded provinces and those with a preference for non-salty food (first two columns). The last two columns of panel A report the results individuals who are not obese. Moving to panel B, the first two columns reveal the results of individuals who are not diagnosed with diabetes. All results are consistent with baseline model.
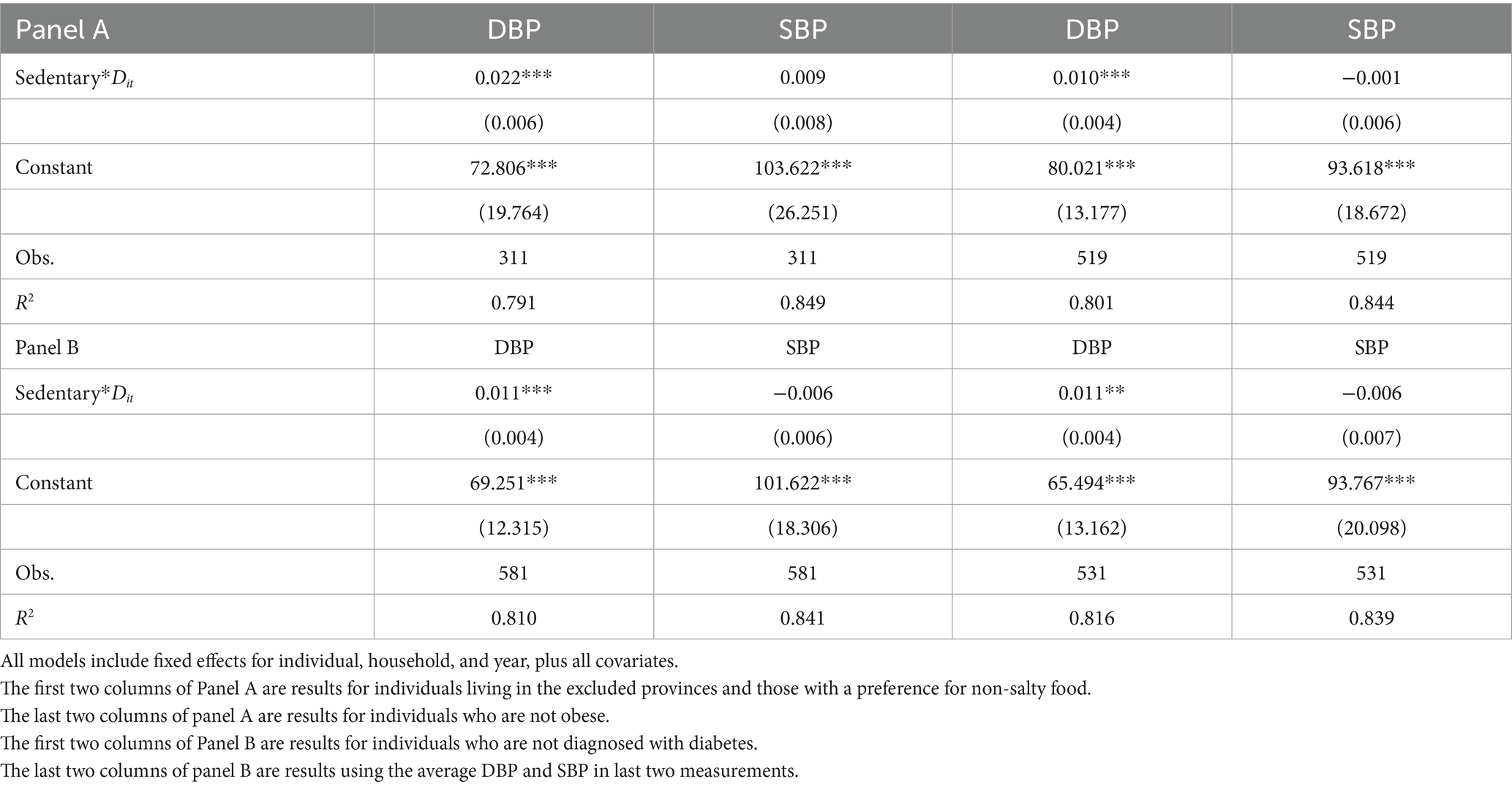
Table 10. Robustness checks.
6.2 Alternative measurement of blood pressure
We also use the average DBP and SBP in last two measurements instead of the three we have at hand. The results are shown in the last two columns of Panel B of Table 10, which in line with our baseline results.
7 Discussion
As baby boomers born in the 1950s and 1960s reach retirement age and leave the labor market, the healthcare system faces significant challenges. Elevated blood pressure is a leading cause of mortality and disease burden worldwide (85), especially among the older adults. Meanwhile, older adults, a vulnerable group, tend to spend more time sitting daily. Leading health authorities, including the World Health Organization, emphasize the importance of reducing sedentary behavior (86). The 2018 Physical Activity Guidelines Advisory Committee graded the evidence linking sedentary behavior with mortality and cardiovascular disease as strong (87) and included the recommendation to “sit less and move more” in the 2018 federal Physical Activity Guidelines (88).
This paper utilizes the statutory retirement policy as an exogenous variation and employs the continuous difference-in-differences (DID) framework, propensity score matching difference-in-differences (PSM-DID) approach and instrumental variable (IV) method to explore the relationship between post-retirement leisure sedentary time and elevated blood pressure. Our analysis yielded two main findings. First, we observed an increase in diastolic blood pressure after retirement due to increased leisure sedentary time, while no significant increase in systolic blood pressure was noted. Second, while physical activity did not mitigate the rise in blood pressure, educational attainment and having family members employed as healthcare workers appeared to reduce its negative impact.
Regarding the first finding, our results align with previous studies and support the link between increased sedentary time and higher DBP (18, 38), confirming Hypothesis 1. Previous studies have found that elevated DBP is significantly related to male sex (89–91) and unhealthy lifestyle such as sedentary behaviors (89), smoking (90), and alcohol consumption (91). In terms of magnitude, each additional hour of sedentary behavior per day results in a statistically significant but modest increase in DBP of 0.66 mmHg on average. This finding holds clinical importance, as elevated DBP is independently linked to a higher risk of heart failure and cardiovascular mortality compared to normal blood pressure (92, 93). As such, highlighting the association between prolonged leisure sedentary time and elevated DBP could help prevent these conditions. Additionally, it remains unclear, however, why significant effects were observed for DBP but not for SBP, a pattern noted in other studies (94). One study conducted between May 2019 and December 2020 found that higher sedentary behavior was linked to increased DBP and total peripheral resistance, suggesting that sedentary behavior may primarily affect vascular stress reactivity rather than cardiac stress (18).
To better inform health interventions, our study revealed two socioeconomic mechanisms. The first mechanism found that engaging in physical activities is unlikely to alleviate the increase in blood pressure (Hypothesis 2a), aligning with literature highlighting the distinction between inactivity and sedentary behavior (44, 45). Therefore, reducing sedentary behaviors, rather than merely promoting physical activities, may be more effective in counteracting the negative impact on blood pressure. The second mechanism hypothesized that educational attainment and having family members employed as medical workers might alleviate the negative impact on blood pressure (Hypothesis 2b). This aligns with studies showing that SES is inversely related to blood pressure (95) and underscores the importance of the social gradient in health (96).
Due to data limitations, we did not explore biological pathways in detail. However, previous studies have proposed several pathways. One suggests that television viewing, often linked to unhealthy eating habits, can lead to obesity and diabetes, which increase hypertension risk (97). Another pathway relates to the suppression of skeletal muscle lipoprotein lipase (LPL) activity during prolonged sitting, which can lead to elevated levels of glucose, triglycerides, and free fatty acids. This can trigger inflammation, endothelial dysfunction, and increased sympathetic activity, potentially raising blood pressure over time (98, 99). Finally, a smaller strand of the literature has suggested that leisure sedentary time may increase DBP through pathways such as increased sympathetic activity, vagal withdrawal, and vascular resistance (34, 100, 101).
Our findings suggest three policy implications. First, while physical activity alone may not counteract the negative effects of sedentary behavior, several studies show that reducing or interrupting prolonged sitting time can lower both DBP and SBP (102). For example, short breaks every 30 min have been shown to improve blood pressure (35). A 12-month workplace-based intervention targeting Australian state government workers significantly reduced SBP by 1.0 to 3.4 mmHg (p < 0.01) during the first 9 months and DBP by 4–5 mmHg over the full 12 months (p < 0.01) (103). In practice, the Chinese government held its highest-level national health conference and subsequently announced the Outline of the Healthy China 2030 Plan in 2016, including the aim of reducing sedentary. Effective promotion of this policy could contribute to achieving these goals. Additionally, local governments should also provide affordable fitness equipment to encourage reduced sedentary time and increased physical activity. For instance, the construction of urban greenways has been shown to significantly reduce sedentary time among participants (104). Second, as habits persist post-retirement, it is crucial to help individuals establish good habits before and after retirement. This includes ensuring easy access to and understanding of health information to promote a healthy lifestyle and providing more convenient community medical services. For example, an educational intervention targeting close-to-retirement employees, including health, leisure time, and financial needs, have showed that feelings of helplessness and failure and oldness and idleness significantly decreased after the educational intervention, and feelings of effort and a new direction significantly increased (105). Third, with rapid development, urbanization, and technological advancements have led to a significant increase in sedentary behavior. According to a 2021 report, Chinese employees have an average daily sitting time of 9.4 h, with 73.9% engaging in more than 8 h sitting per day. Therefore, policymakers should consider the broader social and economic costs associated with sedentary behavior and its impact on blood pressure.
However, our study has limitations. We relied on self-reported sedentary time, which may underestimate actual sedentary behavior. Although self-reported measures are commonly used and show acceptable validity, future studies should combine them with accelerometer-assessed data for a more comprehensive assessment. Additionally, due to China’s unique retirement policy, our study focuses only on males in the formal sector. Future research should include other demographic groups to provide a broader perspective.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
CHNS was approved by the Institutional Review Board at the University of North Carolina at Chapel Hill and local IRB (institutional review board or ethics committee). The patients/participants provided their written informed consent to participate in this study.
Author contributions
HL: Conceptualization, Formal analysis, Writing – original draft. WZ: Supervision, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This study was supported by the Social Sciences Funds of Shannxi Province in China under Grant numbers 2020D004.
Acknowledgments
We are grateful to the CHNS study, which provided the data in this research.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Roth, GA, Mensah, GA, Johnson, CO, Addolorato, G, Ammirati, E, Baddour, LM, et al. Global burden of cardiovascular diseases and risk factors, 1990-2019: update from the GBD 2019 study. J Am Coll Cardiol. (2020) 76:2982–3021. doi: 10.1016/j.jacc.2020.11.010
2. Lu, J, Lu, Y, Wang, X, Li, X, Linderman, GC, Wu, C, et al. Prevalence, awareness, treatment, and control of hypertension in China: data from 1·7 million adults in a population-based screening study (China PEACE million persons project). Lancet. (2017) 390:2549–58. doi: 10.1016/S0140-6736(17)32478-9
3. Wang, Z, Chen, Z, Zhang, L, Wang, X, Hao, G, Zhang, Z, et al. Status of hypertension in China: results from the China hypertension survey, 2012-2015. Circulation. (2018) 137:2344–56. doi: 10.1161/CIRCULATIONAHA.117.032380
4. Buford, TW. Hypertension and aging. Ageing Res Rev. (2016) 26:96–111. doi: 10.1016/j.arr.2016.01.007
5. King, DE, Mainous, AG 3rd, and Geesey, ME. Turning back the clock: adopting a healthy lifestyle in middle age. Am J Med. (2007) 120:598–603. doi: 10.1016/j.amjmed.2006.09.020
6. Yan, Z, Xiang, N, Meng, J, Liang, H, and Yue, Z. Understanding the effect of retirement on health behaviors in China: causality, heterogeneity and time-varying effect. Front Public Health. (2022) 10:952072. doi: 10.3389/fpubh.2022.952072
7. Gorry, D, and Slavov, SN. The effect of retirement on health behaviors. Health Econ. (2023) 32:2234–59. doi: 10.1002/hec.4723
8. Aldoori, MI, and Rahman, SH. Smoking and stroke: a causative role. Heavy smokers with hypertension benefit most from stopping. BMJ. (1998) 317:962–3. doi: 10.1136/bmj.317.7164.962
9. Rehm, J, Anderson, P, Prieto, JAA, Armstrong, I, Aubin, HJ, Bachmann, M, et al. Towards new recommendations to reduce the burden of alcohol-induced hypertension in the European Union. BMC Med. (2017) 15:173. doi: 10.1186/s12916-017-0934-1
10. Marques, FZ, Nelson, E, Chu, PY, Horlock, D, Fiedler, A, Ziemann, M, et al. High-fiber diet and acetate supplementation change the gut microbiota and prevent the development of hypertension and heart failure in hypertensive mice. Circulation. (2017) 135:964–77. doi: 10.1161/CIRCULATIONAHA.116.024545
11. Dunstan, DW, Howard, B, Healy, GN, and Owen, N. Too much sitting--a health hazard. Diabetes Res Clin Pract. (2012) 97:368–76. doi: 10.1016/j.diabres.2012.05.020
12. Diaz, KM, Howard, VJ, Hutto, B, Colabianchi, N, Vena, JE, Safford, MM, et al. Patterns of sedentary behavior and mortality in U.S. middle-aged and older adults: a national cohort study. Ann Intern Med. (2017) 167:465–75. doi: 10.7326/M17-0212
13. Harvey, JA, Chastin, SF, and Skelton, DA. Prevalence of sedentary behavior in older adults: a systematic review. Int J Environ Res Public Health. (2013) 10:6645–61. doi: 10.3390/ijerph10126645
14. Van Dyck, D, Cardon, G, and De Bourdeaudhuij, I. Longitudinal changes in physical activity and sedentary time in adults around retirement age: what is the moderating role of retirement status, gender and educational level? BMC Public Health. (2016) 16:1125. doi: 10.1186/s12889-016-3792-4
15. van der Ploeg, HP, and Hillsdon, M. Is sedentary behaviour just physical inactivity by another name? Int J Behav Nutr Phys Act. (2017) 14:142. doi: 10.1186/s12966-017-0601-0
16. Beunza, JJ, Martínez-González, MA, Ebrahim, S, Bes-Rastrollo, M, Núñez, J, Martínez, JA, et al. Sedentary behaviors and the risk of incident hypertension: the SUN cohort. Am J Hypertens. (2007) 20:1156–62. doi: 10.1016/j.amjhyper.2007.06.007
17. Guo, C, Zhou, Q, Zhang, D, Qin, P, Li, Q, Tian, G, et al. Association of total sedentary behaviour and television viewing with risk of overweight/obesity, type 2 diabetes and hypertension: a dose-response meta-analysis. Diabetes Obes Metab. (2020) 22:79–90. doi: 10.1111/dom.13867
18. Chauntry, AJ, Bishop, NC, Hamer, M, Kingsnorth, AP, Chen, YL, and Paine, NJ. Sedentary behaviour is associated with heightened cardiovascular, inflammatory and cortisol reactivity to acute psychological stress. Psychoneuroendocrinology. (2022) 141:105756. doi: 10.1016/j.psyneuen.2022.105756
19. Hare, D. Examining the timing of women's retirement in urban China: a discrete time hazard rate approach. Contemp Econ Policy. (2018) 36:451–66. doi: 10.1111/coep.12269
20. Chen, Q, Deng, T, Bai, J, and He, X. Understanding the retirement-consumption puzzle through the lens of food consumption-fuzzy regression-discontinuity evidence from urban China. Food Policy. (2017) 73:45–61. doi: 10.1016/j.foodpol.2017.09.006
21. Yi, C, and Xin, L. Retirement and health: evidence from China. China Econ Rev. (2018) 49:84–95. doi: 10.1016/j.chieco.2018.01.005
22. Zhang, A. Zhang Y and Tao Y does retirement make people happier? Evidence from China. Front Public Health. (2022) 10:874500. doi: 10.3389/fpubh.2022.874500
23. Wu, Y, Pang, J, and Yang, H. Effect of retirement on medical reimbursement expenses—evidence from China. Health Econ Rev. (2023) 13:22. doi: 10.1186/s13561-023-00434-x
24. Li, H, Shi, X, and Binzhen, W. The retirement consumption puzzle revisited: evidence from the mandatory retirement policy in China. J Comp Econ. (2016) 44:623–37. doi: 10.1016/j.jce.2015.06.001
25. Li, YH, and Ye, JT. Successful retirement transition process of the elders: an empirical study in Taiwan. J Educ Stud. (2013) 9:78–91. doi: 10.14082/j.cnki.1673-1298.2013.01.004
26. Vigezzi, GP, Gaetti, G, Gianfredi, V, Frascella, B, Gentile, L, Errico, A, et al. Transition to retirement impact on health and lifestyle habits: analysis from a nationwide Italian cohort. BMC Public Health. (2021) 21:1670–10. doi: 10.1186/s12889-021-11670-3
27. Atchley, RC. Retirement and leisure participation: continuity or crisis? Gerontologist. (1971) 11:13–7. doi: 10.1093/geront/11.1_Part_1.13
28. Touvier, M, Bertrais, S, Charreire, H, Vergnaud, AC, Hercberg, S, and Oppert, JM. Changes in leisure-time physical activity and sedentary behaviour at retirement: a prospective study in middle-aged French subjects. Int J Behav Nutr Phys Act. (2010) 7:14. doi: 10.1186/1479-5868-7-14
29. Sprod, J, Ferrar, K, Olds, T, and Maher, C. Changes in sedentary behaviours across the retirement transition: a systematic review. Age Ageing. (2015) 44:918–25. doi: 10.1093/ageing/afv140
30. Leskinen, T, Pulakka, A, Heinonen, OJ, Pentti, J, Kivimäki, M, Vahtera, J, et al. Changes in non-occupational sedentary behaviours across the retirement transition: the Finnish retirement and aging (FIREA) study. J Epidemiol Community Health. (2018) 72:695–701. doi: 10.1136/jech-2017-209958
31. Suorsa, K, Pulakka, A, Leskinen, T, Pentti, J, Vahtera, J, and Stenholm, S. Changes in prolonged sedentary behaviour across the transition to retirement. Occup Environ Med. (2020) 78:409–12. doi: 10.1136/oemed-2020-106532
32. Bossé, R, and Ekerdt, DJ. Change in self-perception of leisure activities with retirement. Gerontologist. (1981) 21:650–4. doi: 10.1093/geront/21.6.650
33. Evenson, KR, Rosamond, WD, Cai, J, Diez-Roux, AV, and Brancati, FLAtherosclerosis Risk in Communities Study Investigators. Influence of retirement on leisure-time physical activity: the atherosclerosis risk in communities study. Am J Epidemiol. (2002) 155:692–9. doi: 10.1093/aje/155.8.692
34. Dempsey, PC, Larsen, RN, Dunstan, DW, Owen, N, and Kingwell, BA. Sitting less and moving more: implications for hypertension. Hypertension. (2018) 72:1037–46. doi: 10.1161/HYPERTENSIONAHA.118.11190
35. Ravichandran, S, Sukumar, S, Chandrasekaran, B, Kadavigere, R, N, SK, Palaniswamy, HP, et al. Influence of sedentary behaviour interventions on vascular functions and cognitive functions in hypertensive adults-a scoping review on potential mechanisms and recommendations. Int J Environ Res Public Health. (2022) 19:15120. doi: 10.3390/ijerph192215120
36. Lim, MS, Park, B, Kong, IG, Sim, S, Kim, SY, Kim, JH, et al. Leisure sedentary time is differentially associated with hypertension, diabetes mellitus, and hyperlipidemia depending on occupation. BMC Public Health. (2017) 17:278. doi: 10.1186/s12889-017-4192-0
37. Li, Z, Zhong, W, Gao, J, Zhang, X, Lin, G, Qi, C, et al. Association between leisure sedentary behaviors and hypertension risk: a prospective cohort study and two-sample Mendelian randomization analysis in Europeans. Prev Med. (2024) 181:107915. doi: 10.1016/j.ypmed.2024.107915
38. Gallagher, J, and Carr, LJ. Leisure but not occupational physical activity and sedentary behavior associated with better health. J Occup Environ Med. (2021) 63:e774–82. doi: 10.1097/JOM.0000000000002365
39. Hashem, R, Rey-Lόpez, JP, Hamer, M, McMunn, A, Rowlands, A, Whincup, PH, et al. Associations between objectively assessed and questionnaire-based sedentary behaviour with body mass index and systolic blood pressure in Kuwaiti adolescents. BMC Res Notes. (2019) 12:588. doi: 10.1186/s13104-019-4626-0
40. Almoosawi, S, Winter, J, Prynne, CJ, Hardy, R, and Stephen, AM. Daily profiles of energy and nutrient intakes: are eating profiles changing over time? Eur J Clin Nutr. (2012) 66:678–86. doi: 10.1038/ejcn.2011.210
41. Dunstan, DW, Kingwell, BA, Larsen, R, Healy, GN, Cerin, E, Hamilton, MT, et al. Breaking up prolonged sitting reduces postprandial glucose and insulin responses. Diabetes Care. (2012) 35:976–83. doi: 10.2337/dc11-1931
42. Carter, S, Hartman, Y, Holder, S, Thijssen, DH, and Hopkins, ND. Sedentary behavior and cardiovascular disease risk: mediating mechanisms. Exerc Sport Sci Rev. (2017) 45:80–6. doi: 10.1249/JES.0000000000000106
43. Wang, Q. Changes in blood pressure during the transition of retirement: the role of physical activity in China. J Hum Hypertens. (2020) 34:536–43. doi: 10.1038/s41371-019-0277-9
44. Sedentary Behaviour Research Network. Letter to the editor: standardized use of the terms “sedentary” and “sedentary behaviours”. Appl Physiol Nutr Metab. (2012) 37:540–2. doi: 10.1139/h2012-024
45. Tremblay, MS, Aubert, S, Barnes, JD, Saunders, TJ, Carson, V, Latimer-Cheung, AE, et al. Sedentary behavior research network (SBRN) - terminology consensus project process and outcome. Int J Behav Nutr Phys Act. (2017) 14:75. doi: 10.1186/s12966-017-0525-8
46. Adler, NE, and Newman, K. Socioeconomic disparities in health: pathways and policies. Health Aff (Millwood). (2002) 21:60–76. doi: 10.1377/hlthaff.21.2.60
47. Li, J, and Powdthavee, N. Does more education lead to better health habits? Evidence from the school reforms in Australia. Soc Sci Med. (2015) 127:83–91. doi: 10.1016/j.socscimed.2014.07.021
48. Sumimoto, Y, Yanagita, M, Miyamatsu, N, Okuda, N, Nishi, N, Nakamura, Y, et al. Association between socioeconomic status and prolonged television viewing time in a general Japanese population: NIPPON DATA2010. Environ Health Prev Med. (2021) 26:57. doi: 10.1186/s12199-021-00978-6
49. Moga Rogoz, AT, Sart, G, Bayar, Y, and Gavriletea, MD. Impact of economic freedom and educational attainment on life expectancy: evidence from the new EU member states. Front Public Health. (2022) 10:907138. doi: 10.3389/fpubh.2022.907138
50. Apfel, F, and Tsouros, AD. Health literacy: the solid facts. Copenhagen: World Health Organization. (2013) 3–26.
51. Wolf, MS, Gazmararian, JA, and Baker, DW. Health literacy and health risk behaviors among older adults. Am J Prev Med. (2007) 32:19–24. doi: 10.1016/j.amepre.2006.08.024
52. McNaughton, CD, Kripalani, S, Cawthon, C, Mion, LC, Wallston, KA, and Roumie, CL. Association of health literacy with elevated blood pressure: a cohort study of hospitalized patients. Med Care. (2014) 52:346–53. doi: 10.1097/MLR.0000000000000101
53. Zhao, M, Konishi, Y, and Glewwe, P. Does information on health status lead to a healthier lifestyle? Evidence from China on the effect of hypertension diagnosis on food consumption. J Health Econ. (2013) 32:367–85. doi: 10.1016/j.jhealeco.2012.11.007
54. Ciancio, A, Kämpfen, F, Kohler, HP, and Kohler, IV. Health screening for emerging non-communicable disease burdens among the global poor: evidence from sub-Saharan Africa. J Health Econ. (2021) 75:102388. doi: 10.1016/j.jhealeco.2020.102388
55. Lubans, DR, Hesketh, K, Cliff, DP, Barnett, LM, Salmon, J, Dollman, J, et al. A systematic review of the validity and reliability of sedentary behaviour measures used with children and adolescents. Obes Rev. (2011) 12:781–99. doi: 10.1111/j.1467-789X.2011.00896.x
56. Su, Y, Li, X, Li, H, Xu, J, and Xiang, M. Association between sedentary behavior during leisure time and excessive weight in Chinese children, adolescents, and adults. Nutrients. (2023) 15:424. doi: 10.3390/nu15020424
57. Cao, B, Zhao, Y, Ren, Z, McIntyre, RS, Teopiz, KM, Gao, X, et al. Are physical activities associated with perceived stress? The evidence from the China health and nutrition survey. Front Public Health. (2021) 9:697484. doi: 10.3389/fpubh.2021.697484
58. Zhou, C, Wu, Q, Ye, Z, Liu, M, Zhang, Z, Zhang, Y, et al. Inverse association between variety of proteins with appropriate quantity from different food sources and new-onset hypertension. Hypertension. (2022) 79:1017–27. doi: 10.1161/HYPERTENSIONAHA.121.18222
59. Schaare, HL, Blöchl, M, Kumral, D, Uhlig, M, Lemcke, L, Valk, SL, et al. Associations between mental health, blood pressure and the development of hypertension. Nat Commun. (2023) 14:1953. doi: 10.1038/s41467-023-37579-6
60. Wang, Z, Yang, T, and Fu, H. Prevalence of diabetes and hypertension and their interaction effects on cardio-cerebrovascular diseases: a cross-sectional study. BMC Public Health. (2021) 21:1224. doi: 10.1186/s12889-021-11122-y
61. Chen, F, Zhang, X, and Chen, Z. Air pollution and mental health: evidence from China health and nutrition survey. J Asian Econ. (2023) 86:101611. doi: 10.1016/j.asieco.2023.101611
62. Shahab, H, Khan, HS, Almas, A, Khan, SA, Artani, A, and Khan, AH. Defining the hemodynamic response of hypertensive and normotensive subjects through serial timed blood pressure readings in the clinic. Clin Hypertens. (2019) 25:8. doi: 10.1186/s40885-019-0114-z
63. Waghorn, J, Liu, H, Yanlin, W, Rayner, SE, Kimmerly, DS, and O’Brien, MW. A single bout of prolonged sitting augments very short-term blood pressure variability. Am J Hypertens. (2024) 37:700–7. doi: 10.1093/ajh/hpae055
64. Plotnikoff, R, and Karunamuni, N. Reducing sitting time: the new workplace health priority. Arch Environ Occup Health. (2012) 67:125–7. doi: 10.1080/19338244.2012.697407
65. Krtalic, B, Knezevic, T, Zeljkovic-Vrkic, T, Kos, J, Pecin, I, Gellineo, L, et al. Family history, blood pressure and life style. Result from EHUH study. J Hypertens. (2019) 37:e230–17. doi: 10.1097/01.hjh.0000572956.60503.d4
66. Zhao, J, Zuo, L, Sun, J, Su, C, and Wang, H. Geographic and urban–rural disparities in dietary energy and macronutrient composition among women of childbearing age: findings from the China health and nutrition survey, 1991–2015. Nutr J. (2023) 22:23. doi: 10.1186/s12937-023-00851-y
67. Burt, VL, Whelton, P, Roccella, EJ, Brown, C, Cutler, JA, Higgins, M, et al. Prevalence of hypertension in the US adult population. Results from the third national health and nutrition examination survey, 1988-1991. Hypertension. (1995) 25:305–13. doi: 10.1161/01.hyp.25.3.305
68. Zhang, Y, Salm, M, and van Soest, A. The effect of retirement on healthcare utilization: evidence from China. J Health Econ. (2018) 62:165–77. doi: 10.1016/j.jhealeco.2018.09.009
69. Hou, B, Wang, G, Wang, Y, and Zhao, Y. The health capacity to work at older ages in urban China. China Econ Rev. (2021) 66:101581. doi: 10.1016/j.chieco.2020.101581
70. Liu, DT-W. The effects of institutionalization in China: a difference-in-differences analysis of the mandatory retirement age. China Econ Rev. (2018) 52:192–203. doi: 10.1016/j.chieco.2018.07.005
71. Rosenbaum, PR, and Rubin, DB. The central role of the propensity score in observational studies for causal effects. Biometrika. (1983) 70:41–55. doi: 10.1093/biomet/70.1.41
72. Copeland, JL, Ashe, MC, Biddle, SJH, Brown, WJ, Buman, MP, Chastin, S, et al. Sedentary time in older adults: a critical review of measurement, associations with health, and interventions. Br J Sports Med. (2017) 51:1539. doi: 10.1136/bjsports-2016-097210
73. Lewbel, A. Constructing instruments for regressions with measurement error when no additional data are available, with an application to patents and R&D. Econometrica. (1997) 65:1201–13. doi: 10.2307/2171884
74. Hu, BY, Johnson, GK, and Wu, H. Screen time relationship of Chinese parents and their children. Child Youth Serv Rev. (2018) 94:659–69. doi: 10.1016/j.childyouth.2018.09.008
75. Munasib, A, and Bhattacharya, S. Is the ‘Idiot's box’ raising idiocy? Early and middle childhood television watching and child cognitive outcome. Econ Educ Rev. (2010) 29:873–83. doi: 10.1016/j.econedurev.2010.03.005
76. Caspersen, CJ, Powell, KE, and Christenson, GM. Physical activity, exercise, and physical fitness: definitions and distinctions for health-related research. Public Health Rep. (1985) 100:126–31.
77. U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Division of Nutrition and Physical Activity. Promoting physical activity: a guide for community action. Champaign: Human Kinetics (1999).
78. Adler, NE, and Rehkopf, DH. U.S. disparities in health: descriptions, causes, and mechanisms. Annu Rev Public Health. (2008) 29:235–52. doi: 10.1146/annurev.publhealth.29.020907.090852
79. Lee, PH, and Wong, FK. The association between time spent in sedentary behaviors and blood pressure: a systematic review and meta-analysis. Sports Med. (2015) 45:867–80. doi: 10.1007/s40279-015-0322-y
80. Stock, JH, and Yogo, M. Testing for weak instruments in linear IV regression. NBER Tech Work Pap. (2005) 14:80–108. doi: 10.1017/CBO9780511614491.006
81. Acemoglu, D, Johnson, S, and Robinson, JA. The colonial origins of comparative development: an empirical investigation. Am Econ Rev. (2001) 91:1369–401. doi: 10.1257/aer.91.5.1369
82. Thorp, AA, Owen, N, Neuhaus, M, and Dunstan, DW. Sedentary behaviors and subsequent health outcomes in adults a systematic review of longitudinal studies, 1996-2011. Am J Prev Med. (2011) 41:207–15. doi: 10.1016/j.amepre.2011.05.004
83. Link, BG, and Phelan, J. Social conditions as fundamental causes of disease. J Health Soc Behav. (1995) 35:80. doi: 10.2307/2626958
84. Yin, M, Augustin, B, Fu, Z, Yan, M, Fu, A, and Yin, P. Geographic distributions in hypertension diagnosis, measurement, prevalence, awareness, treatment and control rates among middle-aged and older adults in China. Sci Rep. (2016) 6:37020. doi: 10.1038/srep37020
85. Zhou, B, Perel, P, Mensah, GA, and Ezzati, M. Global epidemiology, health burden and effective interventions for elevated blood pressure and hypertension. Nat Rev Cardiol. (2021) 18:785–802. doi: 10.1038/s41569-021-00559-8
86. Bull, FC, al-Ansari, SS, Biddle, S, Borodulin, K, Buman, MP, Cardon, G, et al. World Health Organization 2020 guidelines on physical activity and sedentary behavior. Br J Sports Med. (2020) 54:1451–62. doi: 10.1136/bjsports-2020-102955
87. Katzmarzyk, PT, Powell, KE, Jakicic, JM, Troiano, RP, Piercy, K, Tennant, B, et al. Sedentary behavior and health: update from the 2018 physical activity guidelines advisory committee. Med Sci Sports Exerc. (2019) 51:1227–41. doi: 10.1249/MSS.0000000000001935
88. Piercy, KL, and Troiano, RP. Physical activity guidelines for Americans from the US Department of Health and Human Services. Circ Cardiovasc Qual Outcomes. (2018) 11:e005263. doi: 10.1161/CIRCOUTCOMES.118.005263
89. Midha, T, Lalchandani, A, Nath, B, Kumari, R, and Pandey, U. Prevalence of isolated diastolic hypertension and associated risk factors among adults in Kanpur, India. Indian Heart J. (2012) 64:374–9. doi: 10.1016/j.ihj.2012.06.007
90. Saeed, AA, and Al-Hamdan, NA. Isolated diastolic hypertension among adults in Saudi Arabia: prevalence, risk factors, predictors and treatment. Results of a National Survey. Balkan Med J. (2016) 33:52–7. doi: 10.5152/balkanmedj.2015.153022
91. Mahajan, S, Zhang, D, He, S, Lu, Y, Gupta, A, Spatz, ES, et al. Prevalence, awareness, and treatment of isolated diastolic hypertension: insights from the China PEACE million persons project. J Am Heart Assoc. (2019) 8:e012954. doi: 10.1161/JAHA.119.012954
92. Sheriff, HM, Tsimploulis, A, Valentova, M, Anker, MS, Deedwania, P, Banach, M, et al. Isolated diastolic hypertension and incident heart failure in community-dwelling older adults: insights from the cardiovascular health study. Int J Cardiol. (2017) 238:140–3. doi: 10.1016/j.ijcard.2017.02.142
93. Arima, H, Anderson, C, Omae, T, Woodward, M, Hata, J, Murakami, Y, et al. Effects of blood pressure lowering on major vascular events among patients with isolated diastolic hypertension: the perindopril protection against recurrent stroke study (PROGRESS) trial. Stroke. (2011) 42:2339–41. doi: 10.1161/STROKEAHA.110.606764
94. Edwardson, CL, Henson, J, Biddle, SJH, Davies, MJ, Khunti, K, Maylor, B, et al. activPAL and ActiGraph assessed sedentary behavior and cardiometabolic health markers. Med Sci Sports Exerc. (2020) 52:391–7. doi: 10.1249/MSS.0000000000002138
95. Shen, A, Chen, C, Zhang, Z, Zhou, J, Lv, Y, Wang, J, et al. Associations between socioeconomic status and rates of blood pressure changes among Chinese older adults: a longitudinal community-based cohort study. Public Health. (2024) 232:121–7. doi: 10.1016/j.puhe.2024.04.027
96. Marmot, M, and Bell, R. Fair society, healthy lives. Public Health. (2012) 126:S4–S10. doi: 10.1016/j.puhe.2012.05.014
97. Schaan, CW, Cureau, FV, Salvo, D, Kohl, HW 3rd, and Schaan, BD. Unhealthy snack intake modifies the association between screen-based sedentary time and metabolic syndrome in Brazilian adolescents. Int J Behav Nutr Phys Act. (2019) 16:115. doi: 10.1186/s12966-019-0880-8
98. Hamilton, MT, Hamilton, DG, and Zderic, TW. Exercise physiology versus inactivity physiology: an essential concept for understanding lipoprotein lipase regulation. Exerc Sport Sci Rev. (2004) 32:161–6. doi: 10.1097/00003677-200410000-00007
99. Hamilton, MT, Hamilton, DG, and Zderic, TW. Role of low energy expenditure and sitting in obesity, metabolic syndrome, type 2 diabetes, and cardiovascular disease. Diabetes. (2007) 56:2655–67. doi: 10.2337/db07-0882
100. Brindle, RC, Ginty, AT, Phillips, AC, and Carroll, D. A tale of two mechanisms: a meta-analytic approach toward understanding the autonomic basis of cardiovascular reactivity to acute psychological stress. Psychophysiology. (2014) 51:964–76. doi: 10.1111/psyp.12248
101. Ferreira-Silva, R, Goya, TT, Barbosa, ERF, Durante, BG, Araujo, CEL, Lorenzi-Filho, G, et al. Vascular response during mental stress in sedentary and physically active patients with obstructive sleep apnea. J Clin Sleep Med. (2018) 14:1463–70. doi: 10.5664/jcsm.7314
102. Larsen, RN, Kingwell, BA, Sethi, P, Cerin, E, Owen, N, and Dunstan, DW. Breaking up prolonged sitting reduces resting blood pressure in overweight/obese adults. Nutr Metab Cardiovasc Dis. (2014) 24:976–82. doi: 10.1016/j.numecd.2014.04.011
103. Mainsbridge, C, Ahuja, K, Williams, A, Bird, ML, Cooley, D, and Pedersen, SJ. Blood pressure response to interrupting workplace sitting time with non-exercise physical activity: results of a 12-month cohort study. J Occup Environ Med. (2018) 60:769–74. doi: 10.1097/JOM.0000000000001377
104. Li, Z, Lu, Y, Xie, B, and Wu, Y. Large-scale greenway exposure reduces sedentary behavior: a natural experiment in China. Health Place. (2024) 89:103283. doi: 10.1016/j.healthplace.2024.103283
Keywords: risky health behaviors, leisure sedentary time, diastolic blood pressure, systolic blood pressure, statutory retirement policy, China
Citation: Li H and Zeng W (2024) Leisure sedentary time and elevated blood pressure: evidence from the statutory retirement policy. Front. Public Health. 12:1468221. doi: 10.3389/fpubh.2024.1468221
Edited by:
Kuai Yu, Huazhong University of Science and Technology, ChinaReviewed by:
Pinpin Long, Huazhong University of Science and Technology, ChinaHao Wang, Huazhong University of Science and Technology, China
Copyright © 2024 Li and Zeng. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Weihong Zeng, emVuZ3doQG1haWwueGp0dS5lZHUuY24=