 Oscar A. Martínez-Martínez
Oscar A. Martínez-Martínez Araceli Ramírez-López2
Araceli Ramírez-López2 Javier Reyes-Martínez
Javier Reyes-Martínez- 1Department of Social and Political Sciences, Universidad Iberoamericana, Ciudad de México, Mexico
- 2Colegio de Postgraduados, Montecillo, Mexico
- 3Universidad Nacional Autónoma de México, Centro Regional de Investigaciones Multidisciplinarias, Cuernavaca, Morelos, Mexico
- 4División de Administración Pública, Centro de Investigación y Docencia Económicas (CIDE), Ciudad de México, Mexico
Introduction: Poverty is one of the macro factors that has been little studied in terms of its effect on death from COVID-19 since most studies have focused only on investigating whether the pandemic increased poverty or not. With that on mind, the present study aims to analyze how the social deprivations that comprise the measurement of municipal poverty in interaction with health comorbidities and sociodemographic characteristics, increased the probability of death from COVID-19.
Methods: The study is cross-sectional and covers daily reports on the conditions of COVID-19 in the Mexican population for almost 2 years. Using data from the National Epidemiological Surveillance System and the National Council for Evaluation of the Social Development Policy (N = 5,387,981), we employ a Generalized Linear Mixed Model (GLMM), specifically a binomial generalized linear mixed model.
Results: The findings indicate that, besides comorbidities, sociodemographic traits, and clinical aspects, living in a municipality where one or more of the social deprivations exist increases the probability of death. Specifically, in those municipalities where there is deprivation in education, social security, and food, as well as deprivation due to access to health services and deprivation in household services, the probability of death was greater.
Discussion: Living in a municipality with one or more of the social deprivations that compose poverty generated a greater probability of death. Each one of them or together, shows that poverty is a substantial factor for a pandemic like COVID-19 to worsen contagion and death, becoming a circle from which it is difficult to escape.
1 Introduction
The first case of COVID-19 was recorded in December 2019 in Wuhan China, when a group of people with pneumonia of unknown origin was reported; some days later, the Chinese health authorities confirmed that it was COVID-19 or SARS-CoV2 (1). From that moment on, countries around the world began to prepare for this health emergency, implementing various measures, such as quarantines and social distancing (2) as well as prevention measures such as the use of face masks, application of antibacterial gel, and hand washing frequently, in order to prevent the countries’ health systems from collapsing (3). Despite the various actions of governments, there were 676,609,955 infected people globally and 6,881,955 deaths from this disease (4).
On May 5, 2023, the World Health Organization officially ended the COVID-19 pandemic, however, this does not mean that this virus has ceased to be a threat to global health as this same organization points out. Therefore, it is necessary to investigate which health and social factors mainly influenced people’s deaths. In this regard, different investigations found that certain comorbidities were related to this disease (5) and increased the probability of death from SARS-CoV2 (6), putting some populations at greater risk of developing complications (7). Within these comorbidities are cardiovascular diseases, diabetes, hypertension, obesity, and Chronic Obstructive Pulmonary Disease (COPD) (7, 8).
Health comorbidities had different implications in infected people. It has been found that patients with a greater number of comorbidities had less encouraging diagnoses (9), were more likely to develop severe symptoms (10), and therefore, were more likely to enter hospital intensive care (11). Likewise, other factors such as age and sex significantly changed the probability of death (8), thus older adults and men were within the group with the highest probability of death (3).
Some studies have shown that besides comorbidities and sociodemographic variables, there are social determinants of health that place certain populations at greater risk, which are determined by socioeconomic conditions that reproduce inequalities and vulnerability (12, 13), such as income, education, housing, working conditions, food insecurity, and discrimination (14, 15), which are present mainly in populations in poverty (16). In that sense, poverty and its relationship with the COVID-19 pandemic is an understudied aspect. In a few studies, evidence show that poverty was a factor that contributed to the spread of the pandemic due to inequality in access to health services and treatments of this disease (17). Similarly, they found that income was a gradient that was linked to excess mortality from COVID-19 in the poorest municipalities (18). This could be explained by the lack of income and the difficulty or impossibility of social isolation due to the dynamics and conditions of the labor market (17) of people in conditions of poverty. For these reasons, people with higher levels of poverty had lower survival rates from the virus compared to less poor people (19).
Other evidence indicates that municipalities with greater poverty had a higher density of COVID-19 cases (20). Hence, populations with better access to drinking water, sanitation, electricity, food, and private insurance, (i.e., these aspects are part of deprivation in multidimensional poverty measurements) had a greater capacity to prevent contagion (21) and death from this virus.
Poverty is one of the macro factors that has been little studied in terms of its effect on death from COVID-19 since most studies have focused on investigating whether the pandemic increased poverty (22–24) or not. Therefore, our findings cover gaps in the literature for countries that have high levels of poverty such as Mexico, where, during the first 2 years of the pandemic, 37.9% of people were in poverty and 6.7% in extreme poverty (25). Regarding the dimensions that make up this multidimensional measurement, the population presented different deprivations: 52% in social security, 28.2% in health services, 19.2% in education, 17.9% in housing services, 9.3% in quality and spaces of the housing, likewise 22.5% of the population were food insecure and 17.2% did not have enough income to buy a basic food basket for adequate nutrition (25). Although in the last poverty measurement, there was a reduction in poverty, 31.1% of the population continues in these conditions (26) in a country of more than 100 million people.
Under this context of social deprivation and poverty, the data on the COVID-19 pandemic show that there were 7,587,643 infections and 333,913 deaths from this virus, until May 5, 2023 (27). Therefore, the question we seek to answer is: how did the social deprivations that comprise the municipal poverty measurement affect the probability of death from COVID-19? The research is relevant because the challenge of facing a pandemic such as COVID-19 requires studying in a multidimensional way that includes both health and social vulnerabilities. Above all, different governments, especially those in the global south, are going through a series of historical problems related to poverty, marginalization, and vulnerability (28) as well as the lack of a strong public health systems, which allows us to face the epidemiological challenges of the population (29).
Bearing that on mind, the present study aims to analyze how the social deprivations that comprise the measurement of municipal poverty, in interaction with health comorbidities and sociodemographic characteristics, increased the probability of death from COVID-19.
2 Methods
2.1 Database
The information was obtained from two open-access databases, one prepared by the National Epidemiological Surveillance System published by the General Direction of Epidemiology belonging to the Ministry of Health of Mexico, the second is the 2020 municipal poverty measurement, carried out by the National Council for Evaluation of the Social Development Policy (CONEVAL, in Spanish). Regarding the first database, it is where COVID-19 cases have historically been recorded in the country since April 2020. Each state is responsible for monitoring cases and reporting to the Federal Ministry of Health. This dataset includes data from COVID-19 patients who voluntarily underwent SARS-CoV-2 testing, both in public and private hospitals and clinics, as well as in laboratories. The database records confirmed, negative, and suspected cases, from different municipalities in the country, as well as their age, sex, ethnicity, and comorbidities (27).
At the end of January 2022, 14,814,144 cases were registered in the database, of which 8,819, 422 were negative, 5,416,636 were positive and 641,078 were suspicious. We built our database with people who tested positive for COVID-19. From these, we excluded those observations that had missing values in three or more variables. The database consisted of a final sample of 5,387,981 cases confirmed with COVID-19, on which the information from the second database was imputed, which contained the percentages at the municipal level of each of the dimensions that make up the poverty measurement (30), in such a way that the seven deprivations of the multidimensional measurement of poverty were associated with the municipality of residence of each observation (see Table 1).
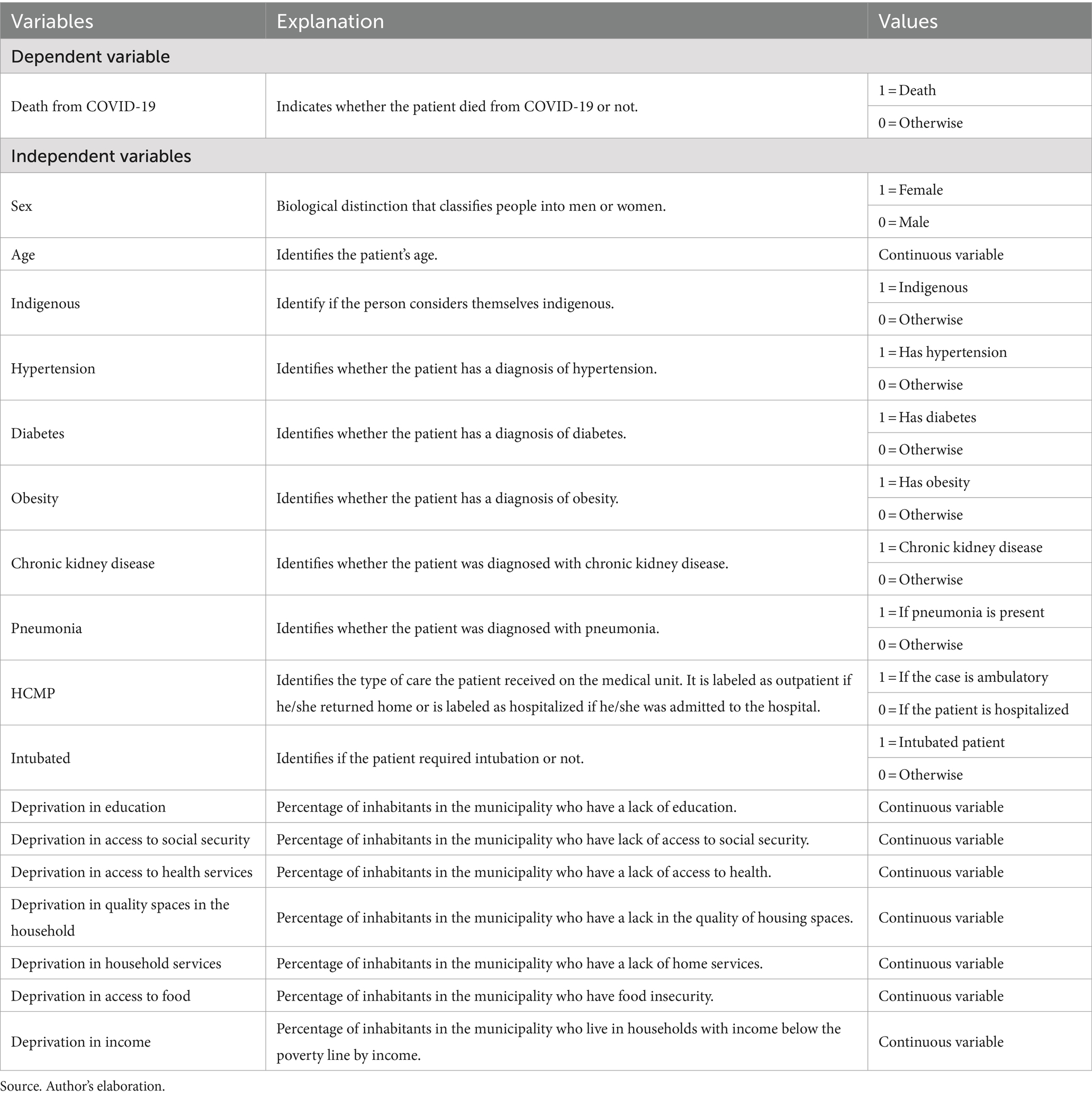
Table 1. Description of dependent and independent variables.
2.2 Measure
The variables used in the study are found in Table 1. Death from COVID-19 is determined by the Ministry of Health as part of the death monitoring subject to epidemiological surveillance (31). The independent variables are divided into four blocks, the first included the comorbidities evidenced in different studies that have shown a strong association with the probability of death from COVID-19, such as diabetes, hypertension, obesity, pneumonia, and kidney diseases (6, 32). The second is the risk conditions, such as age, sex, and being indigenous, which are based on different previous research that points to their association with death from the virus (11, 33, 34).
The third comprised clinical variables since as documented (35) the treatment of manifestations due to the SARS-CoV-2 coronavirus is in relation to the severity of the symptoms and the possibility of access to hospitals equipped to treat the disease. In this case, the variables used were Health Care Management of Patients (HCMP) and whether the person was intubated or not. The fourth block included the seven dimensions that make up the multidimensional measurement of poverty: deprivation in social security, health services, education, housing services, quality and spaces of housing, income, and food insecurity (36).
2.3 Procedures and data analysis
The employed model is the Generalized Linear Mixed Model (GLMM), specifically a binomial generalized linear mixed model, expressed by the equation
On the left side of the equation, the link function is equal to the logit function , where represents the probability of death for individual in municipality . It’s worth noting that is known as the odds of the probability of death. On the right side of the equation, there is the linear predictor, consisting of both fixed and random effects. The first part is a linear combination of regression coefficients with and , where representing the covariate associated with individual in municipality and being the covariate associated with municipality . In other words, the fixed part captures the effect of covariates at the individual level and some variables at the municipal level. The random effects part of the model refers to the term , and its existence assumes that specific conditions in each municipality, not accounted for in the variables , may influence the variability of the probability of death. and represent the number of municipalities and the number of infected individuals per municipality, respectively.
The selection of the model employed the Bayesian Information Criterion () and the Akaike Information Criterion (AIC) , where is the number of parameters estimated, is the likelihood model, and is the number of observations. In order to evaluate the goodness of fit, the log-transformed residual goodness of fit statistic (37) was used and is defined by , where , , is the estimated residual vector and under the null hypothesis, has standard normal distribution. In this model , with critical value .
3 Results
Table 2 shows the main characteristics of the people in the study, specifically the percentages of deaths from COVID-19, sociodemographic data, hospitalizations, intubated people, health comorbidities, and the seven social deprivations that compose poverty at the municipal level.
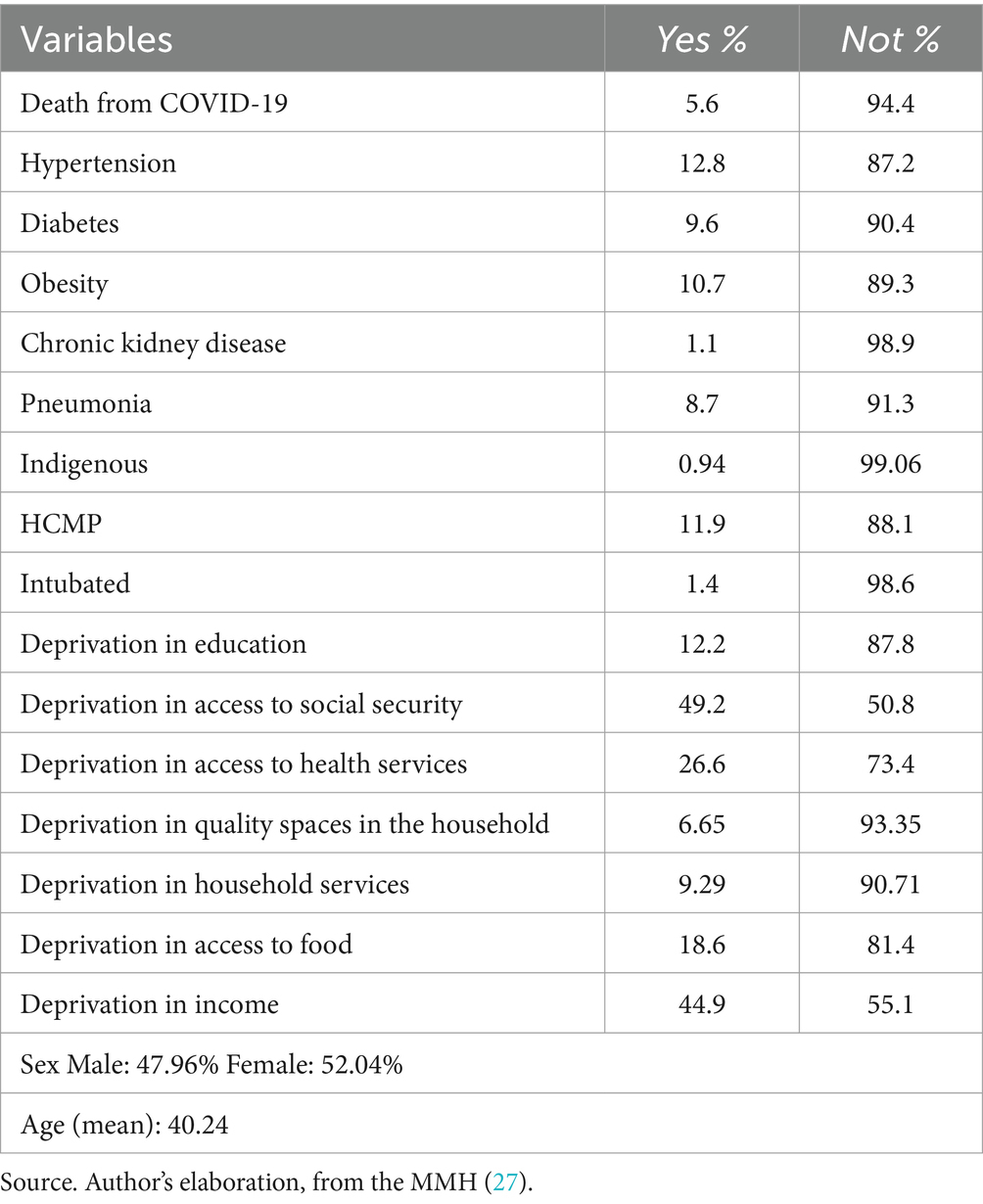
Table 2. Characteristics of the population.
Table 3 shows the results of the GLMM model. Regarding sex, when the person with COVID-19 is a woman, she is 0.7321 times less likely to die than when she is a man. In relation to age, the odds of the probability of death are 1.046 times greater for each additional year of age; in that sense, the probability of death is 1.252 times greater for each additional 5 years of age. Being indigenous increases the probability of death by 1.063 times compared to those who are not.
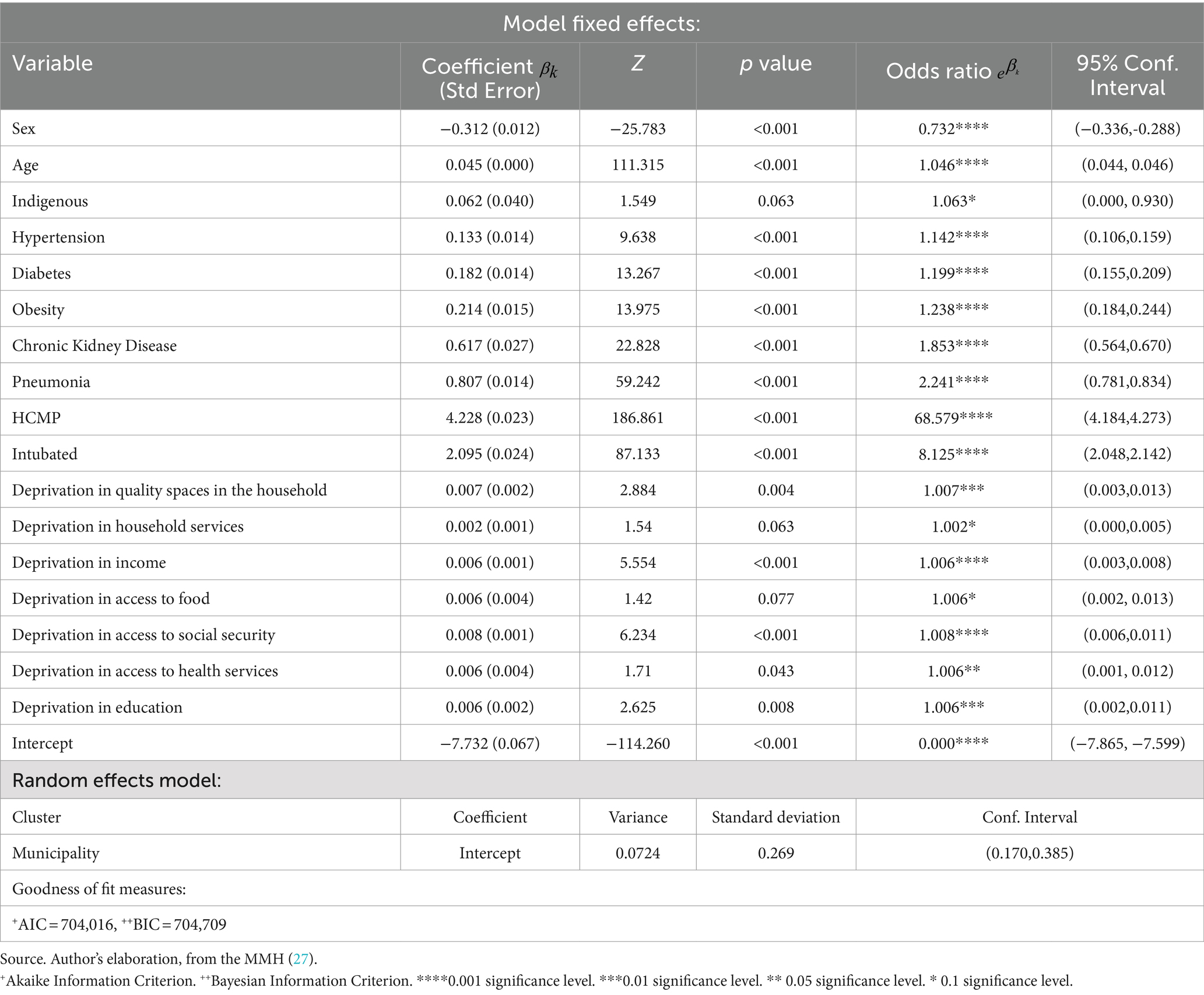
Table 3. Probabilities of death from COVID-19.
In relation to people with health comorbidities, it is found that the probability of death is 1.142 times higher for people who have hypertension compared to those who do not have it. The probability of death with diabetes is 1.199 times greater than that of a person without this disease. Likewise, the probability of death of patients who have obesity is 1.238 times greater than for those without the condition. As for people with chronic kidney disease, the odds of death are 1.853 times greater than people who do not have it. The probability of death of patients who have pneumonia is 2.241 times greater than the probability of those who do not have it. The clinical variables show that the probability of death of people who were hospitalized is 68.579 times greater than the probability of death compared to those who did not require specialized care in a hospital. The odds of death probability increased by 8.125 times when the person was intubated.
Regarding the social deprivations that integrate poverty at the municipal level, their effect is approximately the same magnitude. Results show that living in a municipality where one or more of the social deprivations exist increases the probability of death. Specifically, deprivation in education, income, health services and food, the probability of death for each one is 1.067 times greater for every 10 percentage points when there is any of that deficiency in the municipality. The probability of death related to access to social security is 1.08 times greater for every 10 percentage points when there is this lack in the municipality. The probability of death in patients is 1.07 times greater for every 10 percentage points when there is a deprivation in quality spaces in the household. Having deprivation in household services in the municipality increases the probability of death by 1.02 times for every 10 percentage points.
4 Discussion
Different pre-pandemic studies (38, 39) have documented that respiratory viruses are an emerging threat to global health security because they have given rise to epidemics around the world with high morbidity and considerable mortality. COVID-19 is an example of this because it had different negative effects on certain population groups related to sociodemographic conditions, pre-existing comorbidities, as well as the poverty conditions of the context.
Regarding the sociodemographic variables, our study shows that men had a higher probability of death from COVID-19, as other studies have found (40, 41). In the case of age, like other investigations (31, 42), our evidence indicates that as it increases, the probability of death also increases, which is worse in the case of older adults. Self-identify as Indigenous turned out to be a trait that generates a greater probability of death. This is probably due to all the social inequalities that this group historically has experienced (43, 44). For instance, in several studies, it has been observed the lack of access of health services of Indigenous individuals, and how it affects health outcomes (45) and perceptions of health (46).
In the case of health comorbidities, the evidence from our study shows that hypertension, diabetes, obesity, chronic kidney disease, and pneumonia generated a greater probability of death from COVID-19, in the same line as other international studies since the beginning of the pandemic (7, 9, 41, 42). Although having comorbidities was a predominant factor in developing more severe symptoms of the disease (10, 47) and mainly death, our evidence also suggests that being hospitalized for COVID-19 was one of those factors with the highest probability of death. It could be explained by the time (days or weeks) it took to go to the hospital after they had the first symptoms or tested positive, as well as by the lack of access to hospitals in their context or their saturation.
Going to the hospital in an advanced stage of COVID-19 has an aftermath death or more severe diagnoses due to the severity of the disease (35), leading on several occasions to people being intubated, which, according to our evidence, is one of those with the highest probability of death. Some scholars have found (35) that going to the hospital or medical consultation at the beginning of COVID-19 symptoms helped sick people not be hospitalized and be treated on an outpatient basis.
Living in a municipality where one or more of the social deprivations that compose poverty occur generates a greater probability of death. Each one of them or together, shows that poverty is a substantial factor for a pandemic like COVID-19 to worsen contagion and death, becoming a circle from which it is difficult to escape. For example, the probability of dying due to the deprivation of quality spaces in the household can be explained because one of the variables with which this deprivation is integrated is overcrowding; being in a home where several people live in a small space could generate greater contagion among its members. In addition to this, living in a context of deprivation in household services increased the probability of having as an outcome death because it implies not having water and/or drainage inside the home, which made several of the basic recommendations during the pandemic difficult, such as washing hands frequently or washing and disinfecting food and cloths. For this reason, in another investigation, housing conditions worsened the risk of death from coronavirus by up to 63% (48).
During the pandemic, lack of income was one of the main problems due to the loss of both formal and informal employment (49). In addition, some households experienced a temporary reduction in their income, for this reason having this deprivation increased the probability of death, because the lack of economic resources meant that people had to go out and look for work to bring income to the home. In this sense, some studies show that income was directly related to the high number of infections and deaths from COVID-19 (50) and that people in the lowest income decile had a higher probability of dying. by COVID-19 when they were infected compared to those with higher incomes (51).
Regarding food insecurity, both the scarcity of food in the context and the lack of income to buy it, caused people to have to leave their homes in search of food, increasing their probability of contagion and death. Similar studies show that having been infected with COVID-19 and having food insecurity increased the risk of death from this disease (52), which was higher in populations of less than 5,000 inhabitants (40).
In the Mexican case, by not having a formal job, you do not have access to social security and, therefore, to the benefits that it entailed in the time of the pandemic, such as guaranteed salary, teleworking, and health insurance. In this way, the deprivation of social security increased the probability of death. Likewise, having deprivation in health services means that in the context where one lives one does not have access to public or private hospitals or health clinics. Besides, even if health care facilities existed it did not mean that they were prepared to care for COVID-19 patients, given the deficiencies in quality and services in the health system that historically exist in the country (29, 53). For this reason, the lack of access to health services has been considered one of the most important factors impacts on the probability of death from COVID-19 (54), especially due to inequality in access to health services and treatments for this disease (17).
Deprivation in education had effects on death, probably due to the lack of access to information about the pandemic that could have been obtained at the highest levels of education or because of lack of knowledge of their pre-existing health problems and how to treat them, hence other studies have found that educational lag was a predictor of higher mortality from COVID-19 (55, 56).
Our findings show that the social deprivations that make up the measurement of poverty in interaction with pre-existing health comorbidities generated effects on the probability of death, showing that the COVID-19 pandemic was a syndemic—i.e., the combination of two or more simultaneous or successive epidemics in a population, with biological interactions, which worsen the prognosis, as other research has pointed out (51, 57).
5 Conclusion
The COVID-19 pandemic showed the need to change the health model focused on corrective care that prevails in the National Health System in Mexico and move to a preventive health policy. In that sense, one of the most important challenges to be considered are modifications in the demographic and epidemiological profile of the country, such as population aging and the increment in comorbidities that rise the probability of death.
Living in contexts of poverty increases the probability of death. Evidence here is especially relevant for countries like Mexico where the majority of its population lives with these conditions. Our finding also has implications in public policy because it shows the relevance of carrying out public policy interventions to reduce the social deprivations that detonate poverty. First, the urgent need to address social inequalities in Mexico, mostly those related to the access of healthcare systems and sanitary conditions. The COVID-19 pandemic underscores the priority of more universal healthcare access to all individuals, regardless of individual conditions or regional contexts.
Second, the central need to move from the health model system focused on corrective care that prevails in the National Health System in Mexico to a preventive health policy. The role of previous comorbidities on the outcomes of the COVID-19 pandemic highlights the importance of healthcare systems that do not ignore the proactive measures for managing chronic conditions, ensuring regular health check-ups, and promoting lifestyle changes to mitigate risks.
Data availability statement
Publicly available datasets were analyzed in this study. This data can be found here: https://www.gob.mx/salud/documentos/datos-abiertos-152127.
Ethics statement
The Mexican Ministry of Health, through the hospitals, health clinics, and laboratories that performed COVID-19 tests in the country, obtained informed consent from all study participants.
Author contributions
OM-M: Conceptualization, Investigation, Methodology, Writing – original draft, Writing – review & editing. AR-L: Data curation, Methodology, Writing – original draft, Writing – review & editing. BC: Conceptualization, Supervision, Writing – original draft, Writing – review & editing. JR-M: Conceptualization, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by the Universidad Iberoamericana Ciudad de México, Departamento de Ciencias Sociales y Políticas.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Hui, DS, Azhar, EI, Madani, TA, Ntoumi, F, Kock, R, Dar, O, et al. The continuing 2019-nCoV epidemic threat of novel coronaviruses to global health—the latest 2019 novel coronavirus outbreak in Wuhan, China. Int J Infect Dis. (2019) 91:264–6. doi: 10.1016/j.ijid.2020.01.009
2. Milani, F. COVID-19 outbreak, social response, and early economic effects: a global VAR analysis of cross-country interdependencies. J Popul Econ. (2021) 34:223–52. doi: 10.1007/s00148-020-00792-4
3. Martínez-Martínez, O.Y., and Reyes, J. (2023). “Pandemia COVID-19 y sus efectos en la informalidad laboral. Exploración por sectores económicos y géneros” in Premio Nacional de Investigación Social y de Opinión Pública (2022). Honorable Cámara de Diputados del congreso de la Unión. p.81-110
4. Johns Hopkins University and Medicine (2022). COVID-19 Dashboard. Available online at: https://coronavirus.jhu.edu/map.html. (Accessed January 11, 2022).
5. World Health Organization (WHO) (2020a). Global Surveillance for human infection with coronavirus disease (COVID-19). Available online at: https://rb.gy/erfdbj (Accessed February 18, 2022).
6. World Health Organization (WHO) (2020b). Preguntas y respuestas sobre la enfermedad por coronavirus (COVID-19). Available online at: https://www.who.int/es/emergencies/diseases/novel-coronavirus-2019/question-and-answers-hub/q-a-detail/coronavirus-disease-covid-19 (Accessed January 21, 2022).
7. Yang, J, Zheng, YA, Gou, X, Pu, K, Chen, Z, Guo, Q, et al. Prevalence of comorbidities and its effects in patients infected with SARS-CoV-2: a systematic review and meta-analysis. Int J Infect Dis. (2020) 94:91–5. doi: 10.1016/j.ijid.2020.03.017
8. Huang, C, Wang, Y, Li, X, Ren, L, Zhao, J, Hu, Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. (2019) 395:497–506. doi: 10.1016/S0140-6736(20)30183-5
9. Guan, WJ, Liang, WH, Zhao, Y, Liang, HR, Chen, ZS, Li, YM, et al. Comorbidity and its impact on 1590 patients with COVID-19 in China: a nationwide analysis. Eur Respir J. (2020) 55:5. doi: 10.1183/13993003.00547-2020
10. Bellido, V, and Pérez, A. Consecuencias de la COVID-19 sobre las personas con diabetes. Endocrinol Diabet Nutr. (2020) 67:355–6. doi: 10.1016/j.endinu.2020.04.001
11. Wang, B, Li, R, Lu, Z, and Huang, Y. Does comorbidity increase the risk of patients with COVID-19: evidence from meta-analysis. Aging. (2020) 12:6049–57. doi: 10.18632/aging.103000
12. Artiga, S, and Hinton, E (2018). Beyond Health Care: The Role of Social Determinants in Promoting Health and Health Equity. Kaiser Family Foundation. Available at: https://www.kff.org/racial-equity-and-health-policy/issue-brief/beyond-health-care-the-role-of-social-determinants-in-promoting-health-and-health-equity/ (Accessed March 27, 2024).
13. Castañeda, H, Holmes, SM, Madrigal, DS, Young, MEDT, Beyeler, N, and Quesada, J. Immigration as a social determinant of health. Annu Rev Public Health. (2015) 36:375–92. doi: 10.1146/annurev-publhealth-032013-182419
14. World Health Organization (WHO) (2021). Social Determinants of Health. Available online at: https://www.who.int/westernpacific/health-topics/social-determinants-of-health. [Accessed March 15, 2022]
15. Klassen, S, and Murphy, S. Equity as both a means and an end: lessons for resilient food systems from COVID-19. World Dev. (2020) 136:105104. doi: 10.1016/j.worlddev.2020.105104
16. Lopez, PJ, and Neely, AH. Fundamentally uncaring: the differential multi-scalar impacts of COVID-19 in the U.S. Soc Sci Med. (2021) 272:113707. doi: 10.1016/j.socscimed.2021.113707
17. Wachtler, B, Michalski, N, Nowossadeck, E, Diercke, M, Wahrendorf, M, Santos-Hövener, C, et al. Socioeconomic inequalities and COVID-19—a review of the current international literature. J Health Monitor. (2020) 5:3–17. doi: 10.25646/7059
18. Brandily, P, Brébion, C, Briole, S, and Khoury, L. A poorly understood disease? The unequal distribution of excess mortality due to COVID-19 across French municipalities. Eur Econ Rev. (2020) 140:103923. doi: 10.1016/j.euroecorev.2021.103923
19. Millán-Guerrero, RO, Caballero-Hoyos, R, and Monárrez-Espino, J. Poverty and survival from COVID-19 in Mexico. J Public Health. (2020) 43:437–44. doi: 10.1093/pubmed/fdaa228
20. Henao-Cespedes, V, Garcés-Gómez, YA, Ruggeri, S, and Henao-Cespedes, TM. Relationship analysis between the spread of COVID-19 and the multidimensional poverty index in the city of Manizales, Colombia. Egyptian journal of remote sensing and space. Science. (2022) 25:197–204. doi: 10.1016/j.ejrs.2021.04.002
21. Tavares, FF, and Betti, G. The pandemic of poverty, vulnerability, and COVID-19: evidence from a fuzzy multidimensional analysis of deprivations in Brazil. World Dev. (2021) 139:105307. doi: 10.1016/j.worlddev.2020.105307
22. Lustig, N, and Martínez Pabón, V. The impact of Covid-19 on inequality an poverty in Mexico. Estud Econ. (2021) 36:7–25. doi: 10.24201/ee.v36i1.416
23. Belkiss, M, Pauli, RIP, and De Oliveira, SV. Pobreza multidimensional na pandemia do covid-19: uma aplicação do método Alkire-Foster (AF) para o caso brasileiro multidimensional. Rev Ciênc Econ. (2021) 17:2. doi: 10.5902/2236117043592
24. Bonfiglio, J. I., and Robles, R. (2021). “Efectos de la pandemia COVID-19 sobre la dinámica del bienestar en la Argentina urbana. Una mirada multidimensional acerca de impacto heterogéneo de la crisis tras una década de estancamiento económico (2010–2020)” in Documento estadístico del Barómetro de la Deuda Social Argentina. 2021, 1. Encuesta de la Deuda Social Argentina Serie Agenda para la Equidad. Pontificia Universidad Católica Argentina. Observatorio de la Deuda Social Argentina. Barómetro de la Deuda Social Argentina.
25. CONEVAL (2021). Estimaciones de la pobreza multidimensional 2018 y 2020. Comunicado No. 9. 2021. Digital repository. Available online at: https://www.coneval.org.mx/Medicion/Paginas/PobrezaInicio.aspx
26. CONEVAL (2023). Estimaciones de la pobreza multidimensional 2022. Comunicado No. 7. Digital repository. Available online at: https://www.coneval.org.mx/Medicion/MP/Paginas/Pobreza_2022.aspx
27. Mexican Ministry of Health (MMH) (2021). Sistema Nacional de Vigilancia Epidemiológica, Dirección General de Epidemiología. México. Available online at: https://www.gob.mx/salud/documentos/datos-abiertos-152127
28. Martínez-Martínez, O., Zamudio-Lazarín, C., and Coutiño, B. (2021). Policy Brief. Desafíos de América Latina ante el COVID-19. Desigualdad, pobreza y vulnerabilidad social. Asociación de Universidades Confiadas a la Compañía de Jesús en América Latina.
29. Medrano, A., and Velázquez, R. (2023). “Universalismo y Reformas de pensiones y Salud en México bajo un gobierno de “izquierda” in Política Social en tiempos de la cuarta transformación. Continuidad o cambio de paradigma. Editorial comunicación científica. Ciudad de México. p. 75–98.
30. MCS (2020). Módulo de condiciones socioeconómicas. Instituto Nacional de Estadística y geografía, México.
31. Sanyaolu, A, Okorie, C, Marinkovic, A, Patidar, R, Younis, K, Desai, P, et al. Comorbidity and its impact on patients with COVID-19. Comprehens Clin Med. (2020) 2:1069–76. doi: 10.1007/s42399-020-00363-4
32. Cervera, R, Espinosa, G, Ramos, M, Hernández-Rodríguez, J, Prieto, S, Espígol-Frigolé, G, et al. (2020). Respuesta Inmunoinflamatoria en la COVID-19. 1st Edition. Editorial Médica Panamericana p.752.
33. World Health Organization (WHO) (2020c). Guidance on COVID-19 and NCDs, 2020. Available online at: https://rb.gy/8rcqsj (Accessed March 15, 2022).
34. Argoty-Pantoja, AD, Robles-Rivera, K, Rivera-Paredez, B, and Salmerón, J. COVID-19 fatality in Mexico's indigenous populations. Public Health. (2021) 193:69–75. doi: 10.1016/j.puhe.2021.01.023
35. Martínez-Martínez, OA, Valenzuela-Moreno, KA, and Coutiño, B. Effect of comorbidities and risk conditions on death from COVID-19 in migrants in Mexico. Int J Equity Health. (2022) 20:257. doi: 10.1186/s12939-021-01599-9
36. CONEVAL (2019). “Metodología para la medición multidimensional de la pobreza en México (tercera edición). CONEVAL, Ciudad de México.
37. Saaid, J. A. (2013). Goodness of fit statistics for mixed effect logistic regression models. Unco.edu. University of Northern Colorado.
38. Ali Moni, M, and Liò, P. Network-based analysis of comorbidities risk during an infection: SARS and HIV case studies. BMC Bioinform. (2014) 2014:333. doi: 10.1186/1471-2105-15-333
39. Caughey, GE, Vitry, AI, Gilbert, AL, and Roughead, EE. Prevalence of comorbidity of chronic diseases in Australia. BMC Public Health. (2008) 8:221. doi: 10.1186/1471-2458-8-221
40. Ríos, V, Denova-Gutiérrez, E, and Barquera, S. Association between living in municipalities with high crowding conditions and poverty and mortality from COVID-19 in Mexico. PLoS One. (2022) 17:e0264137. doi: 10.1371/journal.pone.0264137
41. Coutiño, B, and Martínez-Martínez, OA. Comorbilidades en salud y sus efectos en personas con SAR-CoV-2 en México. Panor Econ. (2020) 16:183–98.
42. Atkins, J.L, Masoli, JAH, Delgado, J., Pilling, LC, Kuo, C-L, Kuchel, G.A., et al. (2020).Preexisting comorbidities predicting severe Covid-19 in older adults in the Uk biobank community cohort, United Kingdom
43. Solís, P., Güémez, B., and Lorenzo, V.. (2019). Por mi raza hablará la desigualdad: Efectos de las características étnico-raciales en la desigualdad de oportunidades en México. CDMX: OXFAM México.
44. Solís, P., and Reyes-Martínez, J. (2023). “Discriminación percibida, características étnico-raciales y género” in Interseccionalidad: Teoría antidiscriminatoria y análisis de casos, Universidad Autónoma Metropolitana.
45. Ariza-Montoya, JF, and Hernández-Álvarez, ME. Equidad de etnia en el acceso a los servicios de salud en Bogotá, Colombia, 2007. Rev Salud Públ. (2008) 10:58–71. doi: 10.1590/S0124-00642008000600006
46. Reyes-Martínez, J, Santoyo, IA, and Solís, P. Ethnoracial disparities in self-rated health: exploring the impact of skin color and other ethnoracial characteristics in Mexico. J Racial Ethn Health Disparities. (2024) 14:899–911. doi: 10.1007/s40615-024-02002-3
47. Vivanco-Hidalgo, R. (2020). Generalitat de Catalunya. Agència de Qualitat i Avaluació Sanitàries de Catalunya Edita: Agència de Qualitat i Avaluació Sanitàries de Catalunya. Primera ediciÓn: Barcelona, abril 2020.
48. Ahmad, K, Erqou, S, Shah, N, Nazir, U, Morrison, AR, Choudhary, G, et al. Association of poor housing conditions with COVID-19 incidence and mortality across US counties Khansa. PLoS One. (2020) 15:e0241327. doi: 10.1371/journal.pone.0241327
49. ENOE (2020). Encuesta Nacional de Ocupación y Empleo (ENOE). Instituto Nacional de Estadística e Informatica. Available online at: https://www.inegi.org.mx/programas/enoe/15ymas/
50. Tan, AX, Hinman, J, Magid, HAS, Nelson, L, and Odden, M. Association between income inequality and county-level COVID-19 cases and deaths in the US. Public Health. (2021) 4:1–8. doi: 10.1001/jamanetworkopen.2021.8799
51. Arceo-Gomez, E, Campos-Vazquez, R, Esquivel, G, Alcaraz, E, and Martinez, L. The income gradient in COVID-19 mortality and hospitalisation: an observational study with social security administrative records in Mexico. Lancet. (2022) 6:100115. doi: 10.1016/j.lana.2021.100115
52. Choi, SL, and Men, F. Food insecurity associated with higher COVID-19 infection in households with older adults. Public Health. (2021) 200:7–14. doi: 10.1016/j.puhe.2021.09.002
53. Valencia, E (2024). “Régimen de bienestar y modelo de seguridad social en México (1992–2020)” in Balance de la política social en tiempos del COVID-19 y retos de la postpandemia en México. Colegio de la Frontera Norte. Tijuana México.
54. Rodríguez-Izquierdo, E, Perez-Jiménez, S, Merino-Pérez, L, and Mazari-Hiriart, M (2020). Spatial analysis of COVID-19 and inequalities in Mexico City. Insights by CDP members on the COVID-19 crisis. Department of Economic and Social Affairs; 2020. Available online at: https://www.un.org/development/desa/dpad/wp-content/uploads/sites/45/COVID-19-Mexico-City.pdf
55. Zhuo, J, and Harrigan, N. Low education predicts large increase in COVID-19 mortality: the role of collective culture and individual literacy. Public Health. (2023) 221:201–7. doi: 10.1016/j.puhe.2023.06.016
56. Ortiz-Hernandez, L, and Pérez-Sastré, MA. Social inequalities in the progression of COVID-19 in the Mexican population. Rev Panam Salud Publica. (2020) 44:25e106–6. doi: 10.26633/rpsp.2020.106
Keywords: poverty, social deprivations, COVID-19, death, Mexico
Citation: Martínez-Martínez OA, Ramírez-López A, Coutiñho B and Reyes-Martínez J (2024) Death from COVID-19 in contexts of social deprivation in Mexico. Front. Public Health. 12:1463979. doi: 10.3389/fpubh.2024.1463979
Edited by:
Evasio Pasini, University of Brescia, ItalyReviewed by:
Erwin Calgua, Universidad de San Carlos de Guatemala, GuatemalaGiovanni Corsetti, University of Brescia, Italy
Copyright © 2024 Martínez-Martínez, Ramírez-López, Coutiñho and Reyes-Martínez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Oscar A. Martínez-Martínez, b3NjYXIubWFydGluZXpAaWJlcm8ubXg=