 Jessica Berenice Flores-Mendoza1
Jessica Berenice Flores-Mendoza1 Rebeca Robles García2*Mirna García-Méndez1
Rebeca Robles García2*Mirna García-Méndez1 Norma Liliana Rodríguez-Argüelles3
Norma Liliana Rodríguez-Argüelles3- 1Facultad de Estudios Superiores Zaragoza, Universidad Nacional Autónoma de México, Mexico City, Mexico
- 2Centro de Investigación en Salud Mental Global, Instituto Nacional de Psiquiatría Ramón de la Fuente Muñiz, Mexico City, Mexico
- 3Sindicato Nacional de Trabajadores, Instituto de Seguridad y Servicios Sociales de los Trabajadores del Estado, Mexico City, Mexico
Introduction: Cardiovascular diseases (CVD) are the leading cause of death globally. This burden of disease is particularly high among healthcare workers (HCW). However, adherence to treatment of well-known cardiovascular risk conditions (CRC) still represents a challenge, even among healthcare workers (HCW). Since the identification of modifiable related factors is a prerequisite for developing effective public health interventions, the purpose of this study was to develop a predictive model for adherence to pharmacological treatment (APT) for CRC in HCW, using psychological variables related to CVD mortality, such as the type A behavior pattern, perceived stress, depression, anxiety and attitudes toward treatment adherence.
Methods: An anonymous online survey was completed by a non-probabilistic sample of 1,377 Mexican HCW from tertiary public hospitals, with a diagnosis of only one of the following CRC: ischemic heart disease, diabetes, high blood pressure or dyslipidemia. Sociodemographic questionnaires and self-reported measures were used to collect data: PSS-14 for perceived stress, Type A Behavior Pattern Withdrawal Scale, HADS for anxiety and depression symptoms, the Attitudes toward Medication Scale and the Therapeutics Adherence Scale for Patients with Chronic Diseases.
Results: Anxiety and depression symptoms were higher in the group with risk for non-adherence, while perceived stress and positive attitudes toward medication were higher in the group with likelihood of adherence (p ≤ 0.05). The Type A behavior pattern and sociodemographic variables did not differ between groups. In a regression model, positive attitudes toward medication and perceived stress doubled APT (OR = 2.04, CI95% = 1.39–2.97; OR = 2.02, CI95% = 1.71–2,39, respectively) whereas depression decreased its likelihood (OR = 0.61, CI95% = 0.58–0.73).
Discussion: In conclusion, psychoeducation for patients with CRC should include information on the advantages of medication for treating their condition, even if they are HCW. Promoting adaptative coping skills to handle daily stressful events, including their CRC, could reduce the level of stress that could increase their APT but also their cardiovascular risk. Moreover, our data provide evidence regarding the importance of identifying and treating depressive symptoms as part of the standard care of this population.
1 Introduction
Cardiovascular diseases (CVD), including all diseases of the heart and blood vessels (such as heart attacks and strokes, atherosclerosis, ischemic heart disease, hypertensive diseases, and cardiomyopathy) are the leading cause of death worldwide (1). Ischemic heart disease, diabetes, high blood pressure and dyslipidemia are risk conditions for premature deaths due to CVD (2), which have effective treatment. However, treatment adherence to such cardiovascular risk conditions (CRC) is low in both women and men (3), and among both general population and healthcare workers (HCW), mainly because it involves lifestyle changes, including increasing overall physical activity, reducing alcohol and tobacco use, controlling blood pressure and/or glucose, adopting a heart-healthy diet, and ensuring medication adherence (4–6).
Even HCW are considered to be well informed about etiology, risks and treatment of physical illnesses, they have higher prevalences of such CRC compared to general population (7). Several authors have proposed that this could be explained, at least in part, given the addition of HCW’s occupational exposure to high and chronic stress, which contribute to the development of CVD (8). According to the National Institude for Occupational Safety and Health (9) HCW are exposed to hazards such as working long hours and shifts, and emotional overload due to daily exposure to human suffering and death, and more attention should be pay to elucidate and warn HCW about specific modifiable risk factors that could negatively impact their cardiovascular health.
Negative psychological characteristics related directly or indirectly to CVD mortality might be related also to poor adherence of pharmacological treatment (APT) of CRC such as ischemic heart disease, diabetes, high blood pressure and dyslipidemia among HCW, mainly the so-called Type A behavior pattern (TABP) and the individual poor mental health status. TABP is characterized by a strong drive for competitiveness, achievement and recognition, accompanied by tendencies toward hostility, aggression, impatience, extreme urgency, and environmental control (10) involve a coping style that includes excessive use of active strategies and negative emotional responses that trigger and directly increase the mortality of CVD (11–14), due to the constant overload of the sympathetic nervous system (15, 16).
Regarding the poor mental health status, it is well-stablished that depression and anxiety are indirectly associated with CVD mortality (17–21), due to the related lack of adherence to pharmacological and behavioral treatments (22, 23). Unfortunately, these mental health problems are common in those with CVD (24). Indeed, current clinical recommendations emphasize routine mental health screening and treatment in patients with CVD as an integral part of standard care (25–30).
Other candidate factors to consider in order to explain poor adherence to pharmacological treatment in HCW are the lack of knowledge and more importantly the negative attitudes toward health risk conditions and their pharmacological treatment (31). According to several theoretical models of behavioral change, attitudes, as cognitive mediators of behavior change (32–34) should be evaluated and modified if they are negative, to achieve healthy practices and APT (35–41).
Given the above, the objective of the study was to develop a predictive model for APT in a sample of HCW with CRC (ischemic heart disease, diabetes, high blood pressure and dyslipidemia), through perceived stress, type A behavior pattern, depression, anxiety, and attitudes toward APT.
2 Method
2.1 Participants
This is a descriptive correlational design with a single group of 1,377 Mexican HCW at public tertiary hospitals in Mexico who completed an online survey. The sample was non-probabilistic with standard participants (42) with only one diagnosis (no comorbidity) of the CRC included in the study (ischemic heart disease, diabetes, high blood pressure or dyslipidemia), based on the New York Heart Association (NYHA) criteria (43).
2.2 Measures
Sociodemographic variables (gender, marital status, educational attainment), weight (in kg) and health (in cm) were self-reported in an ad hoc questionnaire, and body mass index (BMI) was subsequently calculated through the reported weight and height values.
The Type A Behavior Pattern was evaluated using the Spanish version of the Type A Behavior Pattern Withdrawal Scale, validated by Herrera et al. (44) in the Mexican population with CVD, demonstrating a high global Cronbach’s alpha of 0.93, and an explained variance of 67.3%. It is a self-administered tool comprising eight items with five possible answers scored from 0–4. The Type A Behavior Pattern is present if the final score is 24 or more.
Perceived stress was assessed using the Spanish version of the Perceived Stress Scale (PSS-14), validated by Brito-Ortiz et al. (45) in the Mexican population, demonstrating global Cronbach’s alpha of 0.86, and an explained variance of 47%. It is a self-administered questionnaire comprising fourteen items, with five possible answers scored from 0–4. A total score of 14 or less means absence of stress, while 15–28 points implies a perception of occasional stress, 29–42 points means often stressed, and 43 or more points is equivalent to very often stressed.
Anxiety and depressive symptoms were evaluated using the Spanish version of the Hospital Anxiety and Depression Scale (HADS) (46), a self-administered questionnaire comprising 14 items with four possible answers scored from 0–3, for a total of 0–21. In both subscales for anxiety and depression, a score of 0–7 indicated absence of symptoms, 8–10 indicated moderate presence of symptoms, and 11–21 indicated significant presence of symptoms. This version for Mexican patients with a CVD yielded a global Cronbach’s alpha of 0.90 (anxiety subscale α = 0.87, and depressive subscale α = 0.77), and an explained variance of 46.94%.
Attitudes toward pharmacological treatment were evaluated using the Attitudes toward Medication Scale (47), a scale designed in Spanish especially for Mexican patients that has an adequate overall reliability index (ω =0.907) and an explained variance of 67.5%. It comprises 21 evaluative bipolar adjectives, with seven response options scored from 1–7. Based on the cut-off points of the instrument, attitudes are considered negative if the score is 15–64, while attitudes toward adherence to pharmacological treatment are considered positive if the score is 65–147.
Finally, APT was evaluated using the Spanish version of the Therapeutic Adherence Scale for Patients with Chronic Diseases, validated by Soria, Vega and Nava (48), which has a global Cronbach’s alpha of 0.91 and an explained variance of 41.1%. This is a self-administered tool comprising 24 items, with three response options ranging from 1–3. Based on the cut-off points established in the instrument by the authors, a greater risk of non-adherence is considered if scores are between 24 and 48, while a greater possibility of adherence is reflected with scores between 49 and 72.
2.3 Procedure and data analyses
The instruments were administered through a national online cardiovascular mental health session, in which a total of 2,051 HCW were invited to participate in the study. Four hundred and eighty-nine were excluded for failing to meet the inclusion criteria, and 185 removed for having more than one CVC. Evaluation was anonymous, through Google Forms and lasted 30 min. At the beginning of the assessment, those who agreed to participate were asked to electronically sign the informed consent form and given instructions for each instrument and their respective response options. The survey remained active for a month.
Descriptive statistics were used to characterize the study sample, including mean, standard deviation, and range for continuous variables, and frequencies and percentages for categorical variables. Shapiro–Wilk test was used to confirm that data set was well-modeled by a normal distribution, as it has proven to be a powerful normality test for large samples size (49). Therefore, comparisons of age and treatment adherence by CRC were performed using one-way analyses of variance (ANOVA) with Bonferroni correction (for), as the typical method for comparing three or more groups means in clinical studies (50). Comparisons of categorical variables by CRC were warried out using Pearson’s chi-square tests, which might be used to examine this type of variables when the sample size is large (51).
Psychological variables were compared by adherence groups (1 = with higher risk of non-adherence, and 2 = with higher likelihood of adherence) using independent samples Student’s t test. Those showing a significant difference between those with higher risk of non-adherence, and higher likelihood of adherence were included as possible predictors in a logistic regression analysis, using APT as the dependent variable. The Hosmer-Lemeshow goodness-of-fit test was conducted to prove the final model. In all cases, data with p < 0.05 were considered statistically significant.
With our sample size, according to G*power calculation, a power of 95% was obtained (alpha = 0.05, two tails).
3 Results
The final study sample comprised 1,377 HCW with a diagnosis of either ischemic heart disease (n = 554, 40.23%), diabetes (n = 341, 24.76%), hypertension (n = 242, 17.57%) or dyslipidemia (n = 240, 17.44%). Table 1 provides a description of the sociodemographic variables, BMI and treatment adherence in the total sample and by CRC.
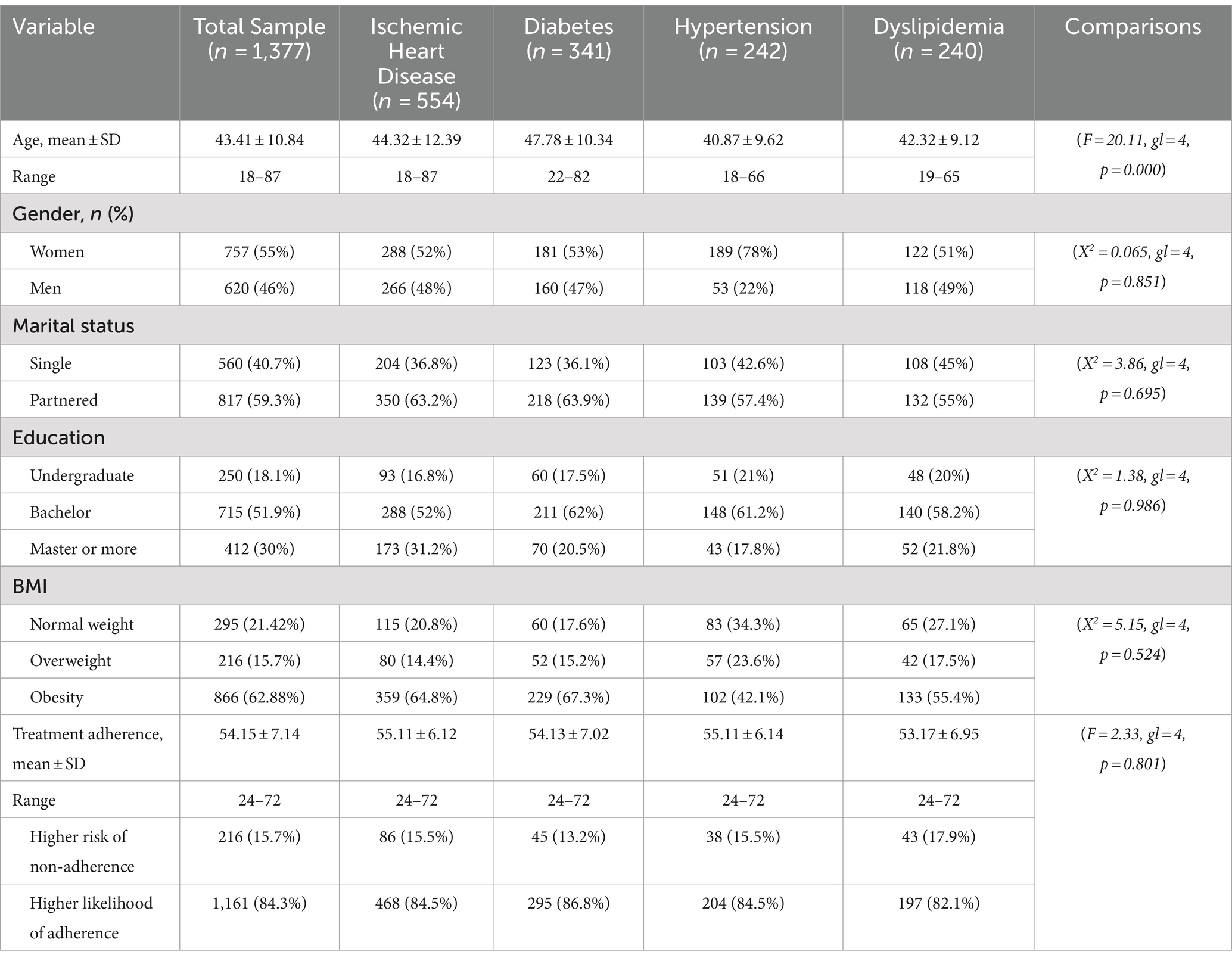
Table 1. Sociodemographic variables, BMI and pharmacological treatment adherence by CRC.
In general, approximately half of the participants was women (n = 757, 55%) and the mean age of the total sample was 43.41 ± 10.84 (range = 18–87) years old. Around 60 % had a partner, and the majority has completed the bachelor’s degree or more (master or doctorate). Only around 20 % of the participants has a Body Mass Index (BMI) indicative of normal weight. Concerning APT, 15.7% (n = 216) had higher risk of non-adherence, and 1,161 (84.3%) reported higher likelihood of adherence.
As can be seen, there were not significant differences in most of sociodemographic variables and the total score of treatment adherence (our dependent variable). Thus, further analyses were using all participant as a single group.
Regarding psychological variables, it highlights that 15% (n = 207) of the sample reported Type A personality, more than 70 % has moderate to severe anxiety symptoms (moderate: n = 244, 17.7% and severe: n = 735, 53.4%), around 40 % reported moderate to severe depressive symptoms (moderate: n = 366, 26.6%; severe: n = 164; 11.9%), and more than 60% perceived to be frequent or very frequent stressed (frequently: n = 766; 55.6%, very frequently: n = 102; 7.4%).
The mean score in attitudes toward treatment adherence was 91.5 ± 17.7 (range = 16–134); around 10 % (n = 142; 10.3%) with a score indicative of negative attitudes toward treatment adherence, and n = 1,235 (89.7%) with positive attitudes toward treatment adherence.
Table 2 offers descriptives and the results of the comparisons of these psychological variables by groups of APT: (1) with higher risk of non-adherence, and (2) with higher likelihood of adherence. As can be seen, anxiety and depression were higher in the group with risk for non-adherence, while perceived stress and positive attitudes toward medication were higher in the group with likelihood of adherence.
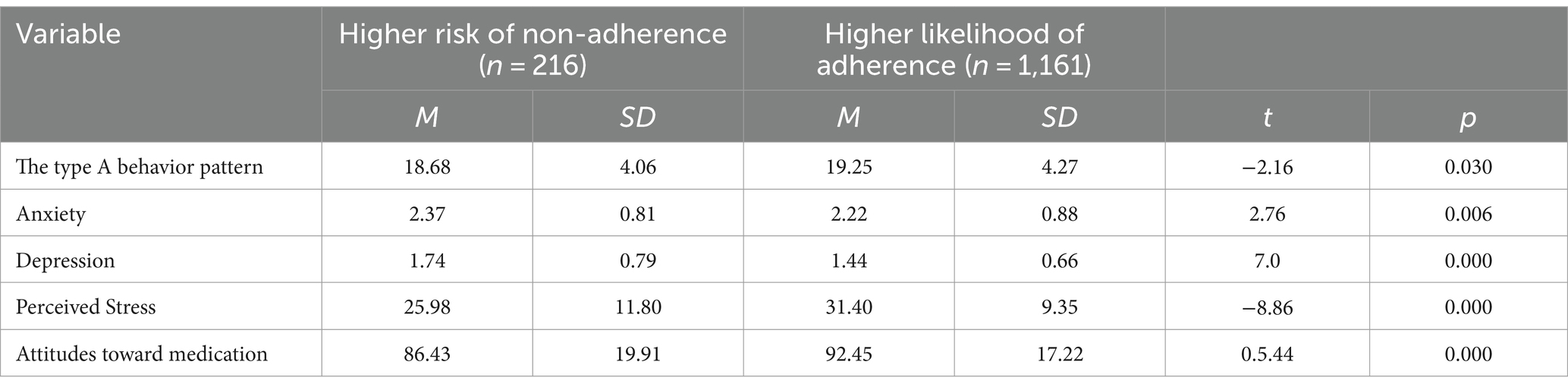
Table 2. Psychological variables and attitudes toward medication by groups of treatment adherence.
Only the Type A behavior pattern did not differ between groups; therefore, it was excluded for further regression analysis. The same happened with sociodemographic variables (age, gender, marital status, education) and BMI, which did not differ statistically between the non-adherence risk group and the group with a higher likelihood of adherence.
Table 3 shows the results of the logistic regression analysis. As can be seen, positive attitudes toward medication and perceived stress doubled APT (OR = 2.04, CI95% = 1.39–2.97; OR = 2.02, CI95% = 1.71–2.39, respectively) whereas depression decreased its likelihood (OR = 0.61, CI95% = 0.58–0.73).
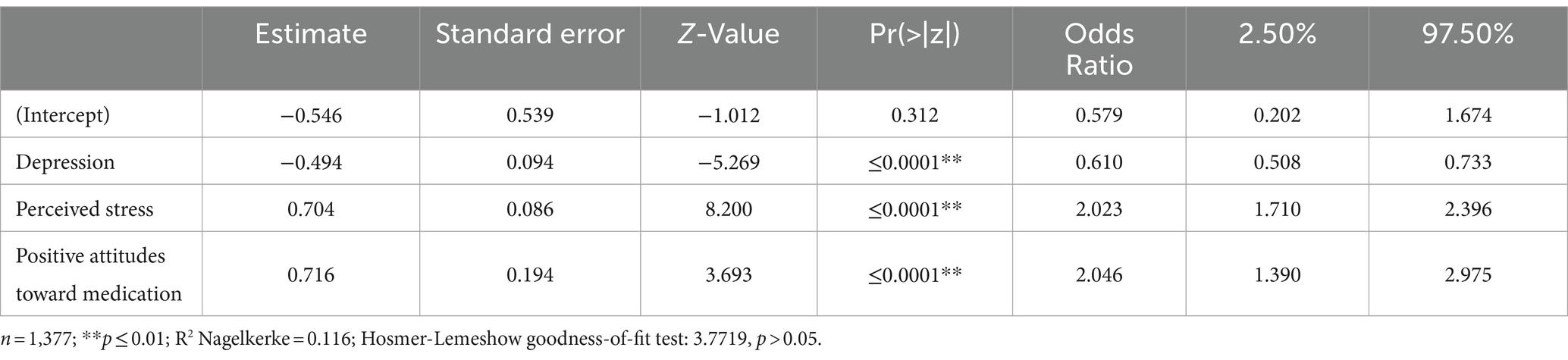
Table 3. Psychological predictors of pharmacological treatment adherence (n = 1,377).
4 Discussion
Although effective pharmacological treatment for CRC such as ischemic heart disease, diabetes, high blood pressure and dyslipidemia is available, APT is a challenge for many patients. Given that the identification of modifiable related factors is a prerequisite for developing effective interventions to increase complex healthy behaviors such as APT, and the need for interventions including psychosocial aspects to prevent HCW’s CVD risks more effectively (52), this study sought to determine the psychological variables that predict the APT of these CRC in a sample of Mexican HCW, an specific population with increased cardiovascular risk (53).
Potential psychological predictors of APT among HCW include those systematically associated with CVD mortality according to the literature in the field: Type A behavior pattern, perceived stress, depression, anxiety, and attitudes toward medication (10, 11, 13–16, 54, 55).
According to our data, positive attitudes toward medication and perceived stress double the probability of APT, while depressive symptoms decrease its probability. In line with previous studies (32–34, 40, 46, 56), attitudes toward healthy practices and treatment play a key role in achieving and maintaining the APT of CRC in Mexican HCW. In this study, positive attitudes toward medication were found to increase APT, highlighting the importance of efforts to boost them rather than merely identifying and modifying negative attitudes (such as fear of negative side effects). Interventions to improve APT for HCW with CRC should therefore strategies to promote positive attitudes toward medication, including the analysis of the advantages of medication for treating their condition.
Interestingly, perceived stress, which is a relevant occupational issue among HCW (8, 9), increased APT for CRC in our sample. This might reflect that stress could prompt active coping with daily stressful events in this specific population, including their CRC and treatment. However, it has been clearly established that chronic high stress levels increase the probabilities of CVD mortality (26–28). Promoting more adaptative coping skills for dealing with these daily stressful events could replace the need for a stressful approach to solving problems, (including CRC though APT) while HCW could also learn evidence-based techniques for stress management (57).
The findings regarding the negative impact of depressive symptomatology on APT for CRC in our sample are in line with prior evidence on depression as a variable that increases CVD mortality due to a related lack of adherence to pharmacological and behavioral treatments (18, 22, 23, 29), and contributes evidence on the importance of identifying and treating depressive symptoms as part of the standard care of patients with CRC (19, 30), mainly in HCW, which compared with other groups of population, have a higher prevalence of depression (58).
Finally, we realize that although a large sample of HCW with CRC was recruited, our study has limitations, including that all information is based solely on self-reports. Moreover, its cross-sectional design makes it impossible to generalize or determine causal links between the variables studied. Additionally, the type of HCW (e.g., nurses, physicians, etc.) was not considered in the present study as variables that can affect directly or indirectly the APT of CRC. Future studies with more objective evaluations, a longitudinal design exploring the effectiveness of the psychological techniques proposed to modify the impact of attitudes toward medication, perceived stress and depressive symptoms on the APT of CRC, as well as comparing the results by type of HCW should be conducted to corroborate and expand our findings.
In conclusion, according to this study among Mexican HCW from tertiary public hospitals with a diagnosis of one CRC (ischemic heart disease, diabetes, high blood pressure or dyslipidemia), some psychological variables related to CVD mortality also impact on APT of CRC, mainly positive attitudes toward medication and perceived stress, which doubled APT for CRC, and depression, which decreased its likelihood.
Data availability statement
The original contributions presented in the study are publicly available. This data can be found here: https://figshare.com/s/fa462efb9684ccca3737.
Ethics statement
The studies involving humans were approved by Local Committee for Research, Ethics and Biosafety of the Hospital Centro Médico Nacional 20 de Noviembre of the ISSSTE with registration number 4632020. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
JF-M: Conceptualization, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. RR: Conceptualization, Formal analysis, Investigation, Methodology, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. MG-M: Investigation, Validation, Visualization, Writing – review & editing. NR-A: Investigation, Validation, Visualization, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This project was supported by a postdoctoral research grant from UNAM-DGAPA awarded to JF-M.
Acknowledgments
We would like to thank the Postdoctoral Scholarship Program of the General Directorate of Academic Personnel Affairs (DGAPA) of the National Autonomous University of Mexico (UNAM), as well as the Faculty of Higher Studies Zaragoza and the National Union of ISSSTE Workers (SNTISSSTE).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Dattani, S., Samborska, V., Ritchie, H., and Roser, M. (2023). Cardiovascular diseases. Our World in Data. Available online at: https://ourworldindata.org/cardiovascular-diseases. (Accessed October 2, 2024).
2. Vaduganathan, M, Mensah, GA, Turco, JV, Fuster, V, and Roth, GA. The global burden of cardiovascular diseases and risk: a compass for future health. J Am Coll Cardiol. (2022) 80:2361–71. doi: 10.1016/j.jacc.2022.11.005
3. Gieniusz-Wojczyk, L, Dąbek, J, and Kulik, H. Type a behaviour pattern and health behaviour of polish nurses. Int J Environ Res Public Health. (2022) 19:6358. doi: 10.3390/ijerph19116358
4. Al-Arkee, S, Mason, J, Lane, DA, Fabritz, L, Chua, W, Haque, MS, et al. Mobile apps to improve medication adherence in cardiovascular disease: systematic review and Meta-analysis. J Med Internet Res. (2021) 23:e24190. doi: 10.2196/24190
5. Sánchez-de-la-Torre, M, Gracia-Lavedan, E, Benitez, ID, Sánchez-de-la-Torre, A, Moncusí-Moix, A, Torres, G, et al. Adherence to CPAP treatment and the risk of recurrent cardiovascular events: a meta-analysis. J Am Med Assoc. (2023) 330:1255–65. doi: 10.1001/jama.2023.17465
6. Simon, ST, Kini, V, Levy, AE, and Ho, PM. Medication adherence in cardiovascular medicine. Br Med J. (2021) 374:n1493. doi: 10.1136/bmj.n1493
7. Mohanty, A, Kabi, A, and Mohanty, AP. Health problems in healthcare workers: a review. J Family Med Prim Care. (2019) 8:2568–72. doi: 10.4103/jfmpc.jfmpc_431_19
8. LaDou, J, and Harrison, RJ. Current Diagnosis & Treatment: Occupational & Environmental Medicine, 6th ed. New York, NY: McGraw Hill (2021).
9. National Institude for Occupational Safety and Health. (2023). Healthcare Workers. Available online at: https://www.cdc.gov/niosh/healthcare/risk-factors/index.html (Accessed October 2, 2024).
10. Nasiłowska-Barud, A, and Barud, M. Psychological risk factors for cardiovascular diseases. Wiadomosci lekarskie. (2020) 73:1829–34. doi: 10.36740/WLek202009104
11. Chida, Y. Heart disease and type A behavior. In: Encyclopedia of behavioral medicine. Cham: Springer International Publishing 2020. 1043–1045.
12. Hamdani, A, Khawar, D, Rabia, K, and Rubab, H. Aggressive behavior and coping strategies among cardiac patients with type a and type B behavior pattern. Pakistan Heart J. (2022) 55:242–6. doi: 10.47144/phj.v55i3.2242
13. Hosseinpour, MR, Eskandari, N, Abdollahi, E, and Tork, A. Personality type a or personality type D, which is a strong predictor of coronary heart disease? Trends J Sci Res. (2021) 5:1–6. doi: 10.31586/Psychology501004
14. Liu, D, Lei, F, Yu, H, Li, L, Wei, G, Liu, Y, et al. Morphological characteristics of culprit plaques in acute myocardial infarction patients with different scores of type a personality. An intravascular optical coherence tomography study. Circ J. (2023) 87:1654–60. doi: 10.1253/circj.CJ-22-0524
15. An, S. The moderated mediation effect of age and relaxation on the relationship between the type a behavior pattern and blood pressure in South Korea. Healthcare. (2023) 11:2264. doi: 10.3390/healthcare11162264
16. Fukita, S, Kawasaki, H, and Yamasaki, S. Does behavior pattern influence blood pressure in the current cultural context of Japan? Iran J Public Health. (2021) 50:701–9. doi: 10.18502/ijph.v50i4.5994
17. Karlsen, HR, Matejschek, F, Saksvik-Lehouillier, I, and Langvik, E. Anxiety as a risk factor for cardiovascular disease independent of depression: a narrative review of current status and conflicting findings. Health Psychol Open. (2021) 8:205510292098746. doi: 10.1177/2055102920987462
18. Li, X, Zhou, J, Wang, M, Yang, C, and Sun, G. Cardiovascular disease and depression: a narrative review. Front Cardiovasc Med. (2023) 10:1274595. doi: 10.3389/fcvm.2023.1274595
19. Mina, K, and Gehendra, M. Heart diseases, anxiety disorders, and negative thoughts. Heart Mind. (2022) 6:22–5. doi: 10.4103/hm.hm_45_21
20. Peng, B, Meng, H, Guo, L, Zhu, J, Kong, B, Qu, Z, et al. Anxiety disorder and cardiovascular disease: a two-sample Mendelian randomization study. ESC Heart Failure. (2024) 11:1174–81. doi: 10.1002/ehf2.14676
21. Szczepanowski, R, Wójta-Kempa, M, Pawlak, A, Kolasa, J, Uchmanowicz, I, Czapla, M, et al. Depressive and anxiety disorders in the cardiological conditions: psychological interventions. Med Res J. (2022) 7:333–9. doi: 10.5603/MRJ.a2022.0051
22. Díaz-Piñera, A., Rodríguez-Salvá, A., León-Sánchez, M., Fernández-González, L., Seuc-Jo, A., and Álvarez-Mesa, N. (2022). Adherencia terapéutica en pacientes hipertensos del Policlínico Universitario Julio Antonio Mella de Guanabacoa. Revista Finlay, 12. Available online at: https://revfinlay.sld.cu/index.php/finlay/article/view/1086 (Accessed October 2, 2024).
23. Warriach, ZI, Patel, S, Khan, F, and Ferrer, GF. Association of Depression with Cardiovascular Diseases. Cureus. (2022) 14:e26296. doi: 10.7759/cureus.26296
24. Amadio, P, Zarà, M, Sandrini, L, Ieraci, A, and Barbieri, SS. Depression and cardiovascular disease: the viewpoint of platelets. Int J Mol Sci. (2020) 21:7560. doi: 10.3390/ijms21207560
25. Garcia, M, Moazzami, K, Almuwaqqat, Z, Young, A, Okoh, A, Shah, AJ, et al. Psychological distress and the risk of adverse cardiovascular outcomes in patients with coronary heart disease. JACC: Advances. (2024) 3:100794. doi: 10.1001/jamanetworkopen.2024.1349
26. Guo, Z, Ding, C, Gao, W, Hong, J, Tang, J, Zhang, Y, et al. Psychometric properties of the Chinese version of attitudes and beliefs about cardiovascular disease risk perception questionnaire. Sci Rep. (2022) 12:20241. doi: 10.1038/s41598-022-24620-9
27. Hendricks, B, Quinn, TD, Price, BS, Dotson, T, Claydon, EA, and Miller, R. Impact of stress and stress mindset on prevalence of cardiovascular disease risk factors among first responders. BMC Public Health. (2023) 23:1929. doi: 10.1186/s12889-023-16819-w
28. Levine, N. Psychological stress and heart disease: fact or folklore? Am J Med. (2022) 135:688–96. doi: 10.1016/j.amjmed.2022.01.053
29. Rivera, MAM, Rivera, IR, Avila, W, Marques-Santos, C, Costa, FA, Ferro, CR, et al. Depression and cardiovascular disease in women. Int J Cardiovasc Sci. (2022) 35:537–45. doi: 10.36660/ijcs.20200416
30. Shiga, T. Depression and cardiovascular diseases. J Cardiol. (2023) 81:485–90. doi: 10.1016/j.jjcc.2022.11.010
31. Hassan, D, Patel, KK, Peddemul, A, Sikandar, R, Singh Kahlon, S, Nair, S, et al. Knowledge, attitude and health practice towards cardiovascular disease in health care providers: a systematic review. Curr Probl Cardiol. (2023) 48:101206. doi: 10.1016/j.cpcardiol.2022.101206
32. Hassan, MO, Ahmed, SA, Hassan, MS, Mohamud, MA, and Abdi, AE. Exploring myocardial infarction knowledge, attitudes, and practice among Mogadishu's Somali residents. Vasc Health Risk Manag. (2024) 20:13–20. doi: 10.2147/VHRM.S448220
33. Williamson, TM, Rouleau, CR, Aggarwal, SG, Arena, R, Hauer, T, and Campbell, TS. The impact of patient education on knowledge, attitudes, and cardiac rehabilitation attendance among patients with coronary artery disease. Patient Educ Couns. (2021) 104:2969–78. doi: 10.1016/j.pec.2021.04.024
34. Yu, M, Wang, L, Guan, L, Qian, M, Lv, J, and Deng, M. Knowledge, attitudes, and barriers related to medication adherence of older patients with coronary heart disease in China. Geriatr Nurs. (2022) 43:235–41. doi: 10.1016/j.gerinurse.2021.12.001
35. Akenine, U, Barbera, M, Beishuizen, CR, Fallah Pour, M, Guillemont, J, Rosenberg, A, et al. Attitudes of at-risk older adults about prevention of cardiovascular disease and dementia using eHealth: a qualitative study in a European context. Br Med J Open. (2020) 10:e037050. doi: 10.1136/bmjopen-2020-037050
36. Akuiyibo, S, Anyanti, J, Amoo, B, Aizobu, D, and Idogho, O. Effects of behaviour change communication on hypertension and diabetes related knowledge, attitude and practices in Imo and Kaduna states: a quasi-experimental study. BMC Public Health. (2022) 22:715. doi: 10.1186/s12889-022-13139-3
37. Al-Ashwal, FY, Sulaiman, SAS, Sheikh Ghadzi, SM, Kubas, MA, and Halboup, A. Risk assessment of atherosclerotic cardiovascular diseases before statin therapy initiation: knowledge, attitude, and practice of physicians in Yemen. PLoS One. (2022) 17:e0269002. doi: 10.1371/journal.pone.0269002
38. Bakkar, A, Mujakkir, S, Hosen, S, Mamun, A, and Akter, H. Assessment of knowledge, attitudes, and practices regarding cardiovascular diseases (CVDs) among older individuals of rural Bangladesh: findings from a face-to-face interview. Front Public Health. (2024) 12:1336531. doi: 10.3389/fpubh.2024.1336531
39. Crawford, K, Jakub, K, Lockhart, JS, and Wold, JL. Knowledge, attitudes, and beliefs of cardiovascular disease prevention in young adults in the country of Georgia. J Nurs. (2023) 55:903–913. doi: 10.1111/jnu.12875
40. Meng, R, Yu, C, Liu, N, He, M, Lv, J, Guo, Y, et al. Association between depression and all-cause and cardiovascular mortality in Chinese adults. JAMA Netw Open. (2020) 3:e1921043. doi: 10.1001/jamanetworkopen.2019.21043
41. Yang, X, Qin, Q, Wang, Y, Ma, Z, Li, Q, Zhang, F, et al. Knowledge, attitudes, and practices regarding cardiovascular disease prevention among middle school students in China: a cross-sectional study. Front Public Health. (2024) 12:1301829. doi: 10.3389/fpubh.2024.1301829
42. Shaughnessy, JJ, Zechmeister, EB, and Zechmeister, JS. Research methods in psychology. 8th ed. New York, NY: McGraw-Hill (2007).
43. McMurray, J, Adamopoulos, S, Anker, S, Auricchio, A, Böhm, M, Dickstein, K, et al. ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: the task force for the diagnosis and treatment of acute and chronic heart failure 2012 of the European Society of Cardiology. Developed in collaboration with the heart. Eur Heart J. (2012) 33:1787–847. doi: 10.1093/eurheartj/ehs104
44. Herrera, C., Deissy, C. A., Muñoz, Z. D. A., Graillet, M. O., Aranda, G. E., Rojas, F., et al. (2017). Impacto del estrés psicosocial en la salud. Neurobiologia. Available online at: www.uv.mx/eneurobiologia/vols/2017/17/17.html (Accessed October 2, 2024).
45. Brito-Ortíz, J, Juárez-García, A, Nava-Gómez, M, Castillo-Pérez, J, and Brito-Nava, E. Factores psicosociales, estrés psicológico y burnout en enfermería: un modelo de trayectorias. Enfermería Universitaria. (2019) 16:138–48. doi: 10.22201/eneo.23958421e.2019.2.634
46. Galindo, O, Benjet, C, Juárez, F, Rojas, E, Riveros, A, Aguilar, PJ, et al. Propiedades psicométricas de la Escala Hospitalaria de Ansiedad y Depresión (HADS) para pacientes con cáncer en población mexicana. Salud Mental. (2015) 38:253–8. doi: 10.17711/SM.0185-3325.2015.035
47. Flores-Mendoza, JB, Villanueva Bustamante, M, Méndez-González, SM, Vázquez-Pérez, S, Tenorio-Bautista, F, Díaz-Loving, R, et al. El papel de la ansiedad y el afrontamiento en la adherencia a la alimentación cardiosaludable: una visión psicosocial en cardiopatía isquémica. Revista Electrónica De Psicología Iztacala. (2022) 25:1338–59.
48. Soria, R, Vega, C, and Nava, C. Escala de adherencia terapéutica para pacientes con enfermedades crónicas, basada en comportamientos explícitos. Alternativas en Psicología. (2009) 14:89–103.
49. Razali, N, and Wah, Y. Power comparisons of Shapiro–Wilk, Kolmogorov–Smirnov, Lilliefors and Anderson–Darling tests. J Stat Model Analyt. (2011) 2:21.33.
52. Hwang, WJ, Park, Y, and Kim, JA. A systematic review of interventions for workers with cardiovascular disease risk factors: using an ecological model. Korean J Occup Health Nurs. (2016) 25:41–54. doi: 10.5807/kjohn.2016.25.1.41
53. Juárez-Pérez, CA, Aguilar-Madrid, G, Haro-García, LC, Gopar-Nieto, R, Cabello-López, A, Jiménez-Ramírez, C, et al. Increased cardiovascular risk using atherogenic index measurement among healthcare workers. Arch Med Res. (2015) 46:233–9. doi: 10.1016/j.arcmed.2015.03.002
54. Nelson, AJ, Pagidipati, NJ, and Bosworth, HB. Improving medication adherence in cardiovascular disease. Nat Rev Cardiol. (2024) 21:417–29. doi: 10.1038/s41569-023-00972-1
55. Peter, R, Meyer, M, Mons, U, Schöttker, B, Keller, F, Schmucker, R, et al. Long-term trajectories of anxiety and depression in patients with stable coronary heart disease and risk of subsequent cardiovascular events. Depress Anxiety. (2020) 37:784–92. doi: 10.1002/da.23011
56. Raevschi, E, Grib, L, Penina, O, and Obreja, G. Relationship between cardiovascular health status and attitudes towards responsibility for health. Folia Med. (2022) 64:327–32. doi: 10.3897/folmed.64.e63538
57. Zhang, M, Murphy, B, Cabanilla, A, and Yidi, C. Physical relaxation for occupational stress in healthcare workers: a systematic review and network meta-analysis of randomized controlled trials. J Occup Health. (2021) 63:e12243. doi: 10.1002/1348-9585.12243
Keywords: treatment adherence, stress, depression, attitudes, cardiovascular diseases
Citation: Flores-Mendoza JB, Robles García R, García-Méndez M and Rodríguez-Argüelles NL (2024) Psychological barriers to adherence to pharmacological treatment of cardiovascular risk conditions in healthcare workers. Front. Public Health. 12:1462281. doi: 10.3389/fpubh.2024.1462281
Edited by:
Yibo Wu, Peking University, ChinaReviewed by:
Icaro Ribeiro, Universidade Estadual de Santa Cruz, BrazilJuana Mercedes Gutierrez-Valverde, Autonomous University of Nuevo León, Mexico
Semra Bulbuloglu, Istanbul Aydın University, Türkiye
Copyright © 2024 Flores-Mendoza, Robles García, García-Méndez and Rodríguez-Argüelles. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rebeca Robles García, cmViZXJvYmxlc0BpbnByZi5nb2IubXg=; cmViZXJvYmxlc0Bob3RtYWlsLmNvbQ==