 Saibal Das1,2†
Saibal Das1,2† Shweta Khare1,3*†
Shweta Khare1,3*† Jaran Eriksen1,4
Jaran Eriksen1,4 Vishal Diwan1,5
Vishal Diwan1,5 Cecilia Stålsby Lundborg1
Cecilia Stålsby Lundborg1 Kristina Skender1
Kristina Skender1- 1Department of Global Public Health, Karolinska Institutet, Stockholm, Sweden
- 2Indian Council of Medical Research - Centre for Ageing and Mental Health, Kolkata, India
- 3Department of Public Health Sciences and Environment, RD Gardi Medical College, Ujjain, India
- 4Department of Clinical Science and Education, Södersjukhuset, Karolinska Institutet, Stockholm, Sweden
- 5Indian Council of Medical Research - National Institute for Research in Environmental Health, Bhopal, India
Objective: Informal healthcare providers (IHCPs) play a big role in health systems in low-and middle-income countries (LMICs) and are often the first point of contact for healthcare in rural and underserved areas where formal healthcare infrastructure is insufficient or absent. This study was performed to systematically review the literature on interventions targeting IHCPs in improving the delivery of healthcare services in LMICs.
Methods: PubMed, Embase, and Cochrane CENTRAL databases were searched for studies that assessed any type of intervention among IHCPs to improve the delivery of healthcare services in any LMIC. Outcomes included changes in knowledge, attitude, and reported practice of appropriate case diagnosis and management; improved referral services; effective contraceptive use; and medication appropriateness (PROSPERO ID: CRD42024521739).
Results: A total of 7,255 studies were screened and 38 were included. Most of the studies were conducted in Africa and Asia. The IHCPs who were trained included medicine sellers, community health workers/traditional healers, and traditional birth attendants. The main intervention used was educational programs in the form of training. The other interventions were health services, policy and guidelines, and community-based interventions. Most of the interventions were multi-faceted. The disease/service areas targeted were mainly maternal and child health, sexually transmitted diseases, common infectious diseases, medicine use/dispensing practices, and contraception. The outcomes that showed improvements were knowledge, attitude, and reported practice; diagnosis and case management; improved referral services; contraceptive uses; and medication appropriateness. Around one-fourth of the studies reported negative results. The certainty of evidence generated (GRADE criteria) was very low.
Conclusion: Some multifaceted interventions coupled with training showed improvements in the delivery of healthcare services by IHCPs. However, the improvements were inconsistent. Hence, it is unclear to identify any context-specific optimum intervention to improve the delivery of healthcare services by IHCPs.
1 Introduction
Informal healthcare providers (IHCPs) play a big role in providing healthcare services in low-and middle-income countries (LMICs), especially in places like India, Bangladesh, and various parts of Africa due to their accessibility, affordability, and familiarity within the community (1–3). IHCPs practice allopathic and non-allopathic medicine with minimal or no formal training and constitute a significant portion of the private healthcare sector (1–3). IHCPs are broadly categorized based on the nature of their practice. This encompasses retail medicine sellers, traditional healers, faith healers, traditional birth attendants, untrained allopathic providers, and traditional medicine practitioners (1, 2). Additionally, IHCPs include individuals trained in one field but practicing in another, such as nurses offering medical consultations as doctors within their communities (1).
IHCPs are often the first point of contact for healthcare in rural and underserved areas where formal healthcare infrastructure is insufficient or absent. The gap in healthcare systems in LMICs is primarily due to inadequate infrastructure, a shortage of formally trained healthcare professionals, and logistical challenges in reaching remote areas. Limited resources and funding constraints often mean that formal healthcare facilities are sparse, poorly equipped, or concentrated in urban centers, leaving rural and impoverished communities underserved. IHCPs, despite their lack of formal training, attempt to fill this gap by offering various health services, often tailored to the specific needs and cultural contexts of their communities (1, 2). People seek out the services of IHCPs for a range of interventions, including preventive, curative, and restorative care.
Despite their significant role, IHCPs are often overlooked in the healthcare system, which particularly affects the poor who rely on them. Unlike formal private actors, IHCPs lack recognition within a country’s regulatory and legal framework, despite being sought after by the clients they serve. Payment is usually received directly from patients, without documentation, rather than from institutions (2). They may also belong to professional associations that lack certification or regulatory authority (2, 4). Many IHCPs may be hesitant to formalize their practice, especially if government penalties exist for those who advertise themselves illegally as legitimately trained professionals (2, 4).
Despite the renewed emphasis on primary healthcare, surprisingly few studies have explored the potential of the informal sector to extend healthcare to communities (5). Interventions recognizing IHCPs’ contribution to healthcare provision could help legitimize their profession and identify opportunities to expand essential healthcare in LMICs in alignment with public health goals of quality and affordability. Training IHCPs could potentially enhance healthcare in these communities, but implementing such an approach necessitates identifying these providers, their practice locations, and the specific training they require. Currently, there is a lack of summarized data about the types of interventions and their effectiveness in improving the quality of healthcare delivery provided by IHCPs. Conducting a systematic review of interventions targeting IHCPs is essential to consolidate existing knowledge and evaluate the effectiveness of these interventions in enhancing healthcare delivery in LMICs. Given the significant role IHCPs play in providing accessible healthcare services, especially in rural and underserved areas, a comprehensive review was aimed at identifying successful interventions.
2 Methods
2.1 Search strategy and information sources
The researchers conducted a literature search in the PubMed, Embase, and Cochrane CENTRAL electronic databases for original interventional studies published in English from LMICs between 1990 and June 2024. The search was last conducted on 30 June 2024. Systematic reviews, qualitative studies, editorials, commentaries, conference proceedings, and case series/reports were not included. Various search terms were utilized, as outlined in Supplementary Table S1. These search terms were adapted for different bibliographic databases, incorporating database-specific filters. Two independent authors identified relevant studies based on their titles and abstracts using the search strategy. They then obtained the abstracts and, if necessary, the full texts of the studies to evaluate their suitability for inclusion. The discrepancies were resolved by discussion with the arbiter.
2.2 Eligibility criteria and study selection
Since the informality of care varies depending on the context, rigid criteria cannot universally define IHCPs. Therefore, a set of operational criteria was established to define IHCPs operating in LMICs: individuals lacking formal training in an institution recognized and affiliated by the regulatory authority/council of a particular country; those without registration, regulation, or oversight by any institution or governing body for their practice; and those working in a private setting whose scope of work is not recognized by the regulatory authority/council of that particular country (2). Community health workers trained and recognized by non-governmental organizations and governments, such as the Accredited Social Health Activist women workforce in India, who act as the first point of contact for any health-related issue, were excluded. Original interventional studies assessing any type of intervention (educational, behavioral, social, etc.) among IHCPs to enhance the delivery of healthcare services in any setting in any LMIC were included. The comparator was no intervention or any specific active intervention. Outcomes included changes in knowledge, attitude, and reported practice of appropriate case diagnosis and management; improved referral services; effective contraceptive use; and medication appropriateness. Specifically, studies were not included if they did not meet our predefined selection criteria, such as studies that were not quasi-experimental or randomized controlled trials (inappropriate study design) or studies that did not focus on IHCPs in LMICs based on our operational criteria (inappropriate population) (Figure 1).
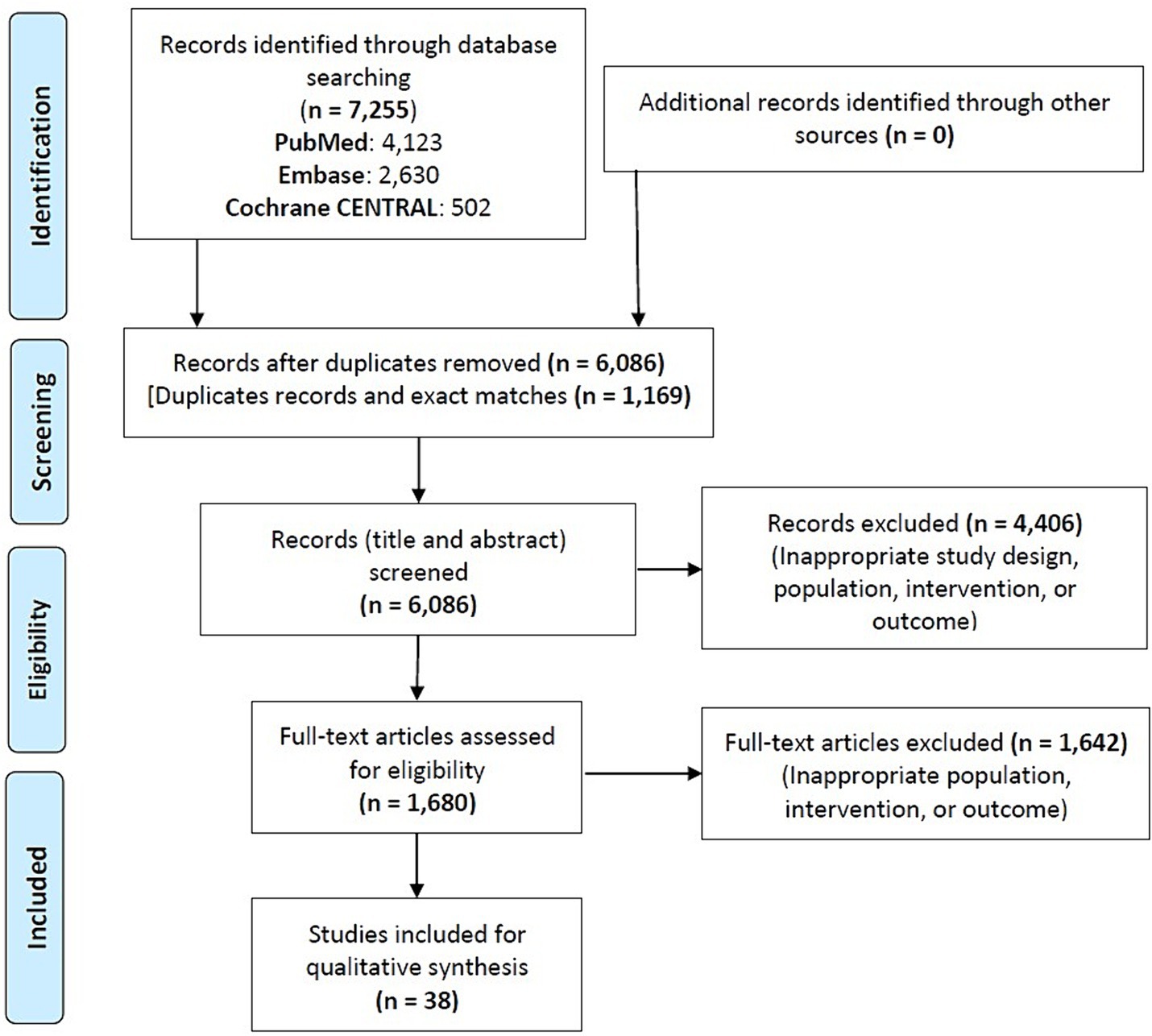
Figure 1. Study flowchart.
2.3 Data items and analysis
A standardized, pre-formatted form was used to extract data from the eligible studies. The extracted information encompassed various aspects, including the study setting, study population (type of IHCPs), participant demographics and characteristics, details of interventions and comparators, and outcomes. The data was managed using Microsoft Excel. Descriptive statistics were used to summarize the results. Additionally, The World Health Organization (WHO) Health Intervention Classification Framework categories were used to classify the interventions as follows (62):
(1) Education and training: activities aimed at improving knowledge and skills.
(2) Health services: direct healthcare services provided to individuals.
(3) Policy and guidelines: implementation of policies or guidelines to improve health outcomes.
(4) Community-based interventions: activities that engage community members in health promotion and disease prevention.
2.4 Risk of bias assessment
For the risk of bias analysis, the ROBINS-I tool (6) was used for quasi-experimental studies and the Cochrane risk of bias tool 2 (59) was used for randomized controlled trials by an independent author. The ROBINS-I tool includes the assessment of the following biases: confounding, selection of participants in the study, classification of interventions, deviations from intended interventions, missing data, measurement of outcomes, selection of the reported result, and overall. The Cochrane risk of bias tool 2 includes the assessment of the following biases: randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, selection of the reported result, and overall. Attrition rates, including dropouts, loss to follow-up, and withdrawals, were also examined. Issues of missing data and imputation methods were critically evaluated.
2.5 Certainty assessment
The GRADE (Grading of Recommendations Assessment, Development and Evaluation) approach was used to assess the certainty of the generated evidence (7, 57).
2.6 Study protocol
This systematic review complies with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The study protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO ID: CRD42024521739).
3 Results
3.1 Study selection, characteristics, and results of quality assessment
A total of 7,255 studies were screened and finally, 38 were included (Figure 1). The studies were published between 1992 and 2021. The results of the risk of bias analysis are itemized in (Supplementary Tables S2, S3). Eight quasi-experimental studies had high risk of bias, while the randomized controlled trials had a moderate or low risk of bias. The summary of the study characteristics is enumerated in Table 1. The quasi-experimental study design was used in most of the cases (68%). Most of the studies were conducted in Africa (50%) and Asia (40%). The sample size ranged from 17 to 1,133.

Table 1. Summary of the study characteristics (n = 38).
3.2 Synthesis of study results
The main intervention used was educational programs in the form of training. These interventions included regular interactive educational training programs, both short-term (up to 3 months) and long-term (9 months to 2 years), aimed at improving knowledge in specified areas. Additionally, outreach education programs and interactive seminars were employed to enhance knowledge and management practices. The IHCPs who were trained included medicine sellers (34%), community health workers/traditional healers (34%), and traditional birth attendants (29%). The common disease/service areas that were targeted were maternal and child health (39%), sexually transmitted diseases/infections (STDs/STIs) (24%), and malaria (16%) (Table 2). We identified various types of interventions categorized based on their intended impact on provider behavior. Many interventions were implemented in combination with related strategies. Approximately 68% of all studies employed multiple intervention strategies, with nearly all studies measuring more than one outcome. The common strategy was management improvement, including training, provision of supplies, job aids, and financial incentives (market-based approach). However, the interventions were inconsistent and heterogeneous across studies. The comparator was no intervention in all studies except two (8, 9), where specific active interventions were used as a comparator.
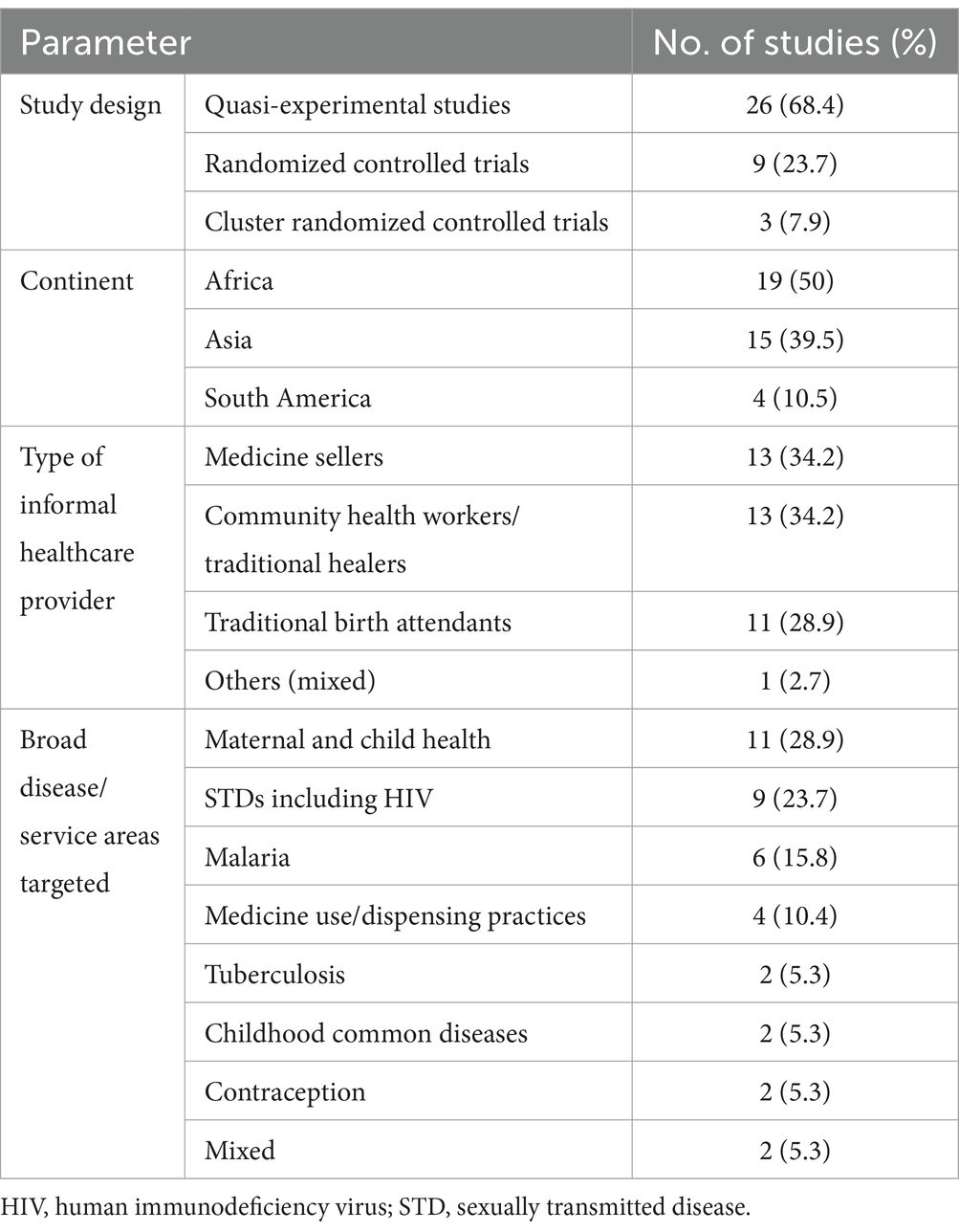
Table 2. Summary of the findings (n = 38).
Twenty-eight studies reported changes in knowledge, attitude, and reported practice of appropriate case diagnosis and management after intervention for common conditions (respiratory infection, diarrhea, malaria, etc.), STDs/STIs, and perinatal care. Seven studies evaluated improvement in referral services post-intervention for perinatal care, STDs/STIs, and tuberculosis. Seven studies evaluated increased knowledge of contraceptive use and increased sales of condoms. Eight studies evaluated post-training improved medication appropriateness focusing on antibiotics for common diseases (respiratory infection, diarrhea, malaria, etc.). Among the studies, 26% reported positive outcomes with training alone, while 47% reported positive outcomes with training combined with other interventions. Most studies assessed provider performance as a basic measure of intervention effectiveness. Traditional healers showed the greatest improvement in provider knowledge. Post-training, improvements were observed in knowledge, attitude, and reported practice of appropriate case diagnosis and management; improved referral services; effective contraceptive use; and medication appropriateness. However, the improvements were inconsistent across studies. A high proportion (89%) of randomized controlled trials reported positive outcomes, while 26% of all studies reported one or more negative outcomes. The certainty of evidence generated (GRADE criteria) was; however, very low for all outcomes (Supplementary Tables S4–S8).
The interventions from the study primarily fall under the WHO Health Intervention Classification Framework categories of education and training, health services, policy and guidelines, and community-based interventions (Table 3; Supplementary Table S9) (World Health Organization, 2023). Education and training were the most common and reported in most of the studies, leading to improved knowledge and skills among healthcare providers, traditional healers, and community workers, often resulting in better health practices, increased treatment adherence, and reduced mortality rates. The service areas covered by education and training were common infectious diseases, STDs, malnutrition, and antenatal care. Health services interventions, such as the establishment of birthing homes in villages for perinatal care (10) or the establishment of a novel community-based delivery system for effective infectious disease management (11). Multi-component policy and guidelines intervention led to improved knowledge and reported practice of the treatment of acute respiratory infections and STDs and the sale of antibiotics (12). Lastly, community-based interventions demonstrated success in the deployment of anti-malarial medicine sellers and village health motivators for increased identification of malaria and improved correct chloroquine use (13).
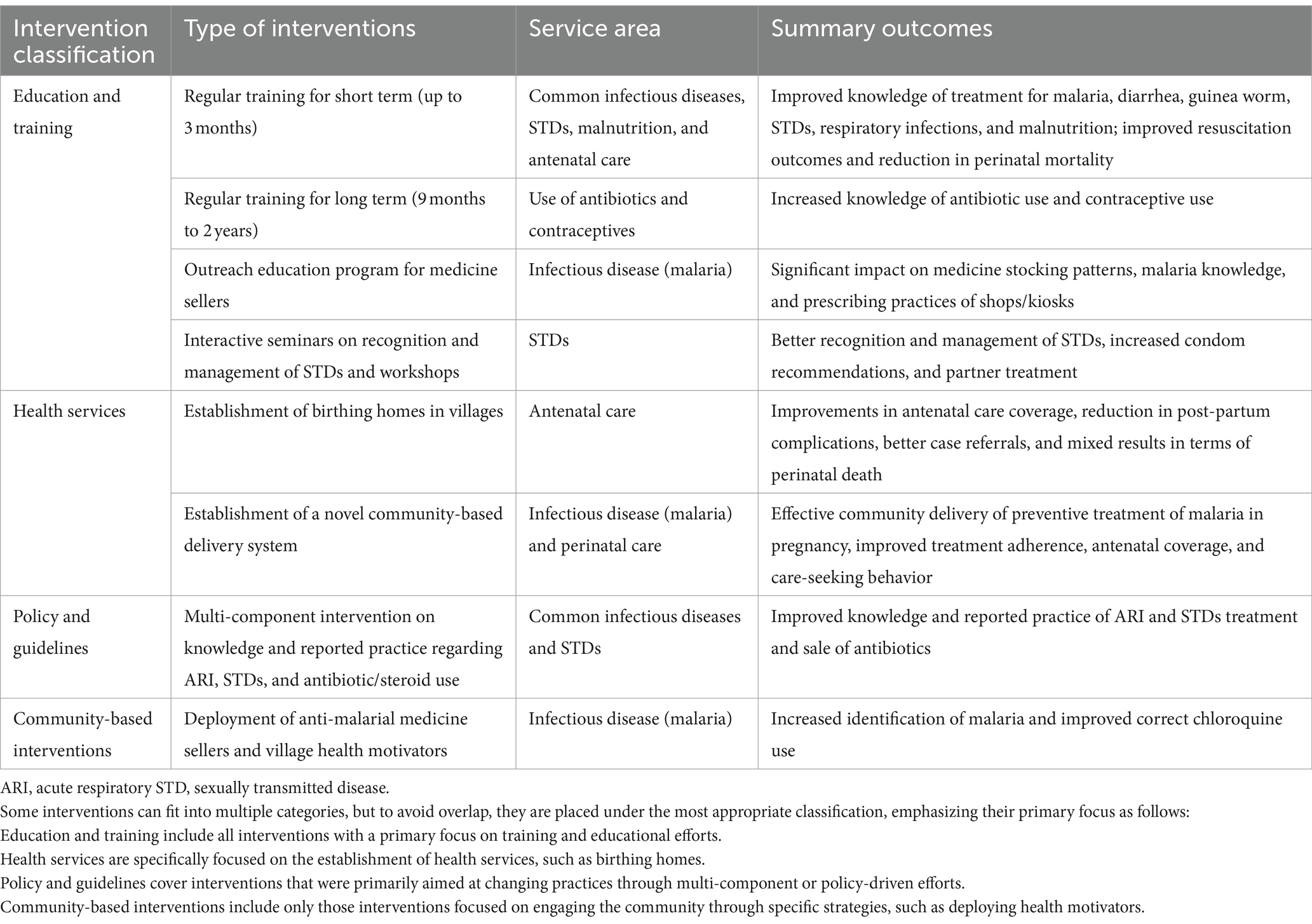
Table 3. Summary of the interventions and outcomes based on the World Health Organization (WHO) Health Intervention Classification Framework categories.
4 Discussion
This systematic review aimed to summarize the evidence on various interventions in improving the delivery of healthcare services by IHCPs in LMICs. A total of 38 studies published between 1992 and 2021 were included. The majority of these were conducted in Africa and Asia, targeting IHCPs, including medicine sellers, community health workers, and traditional birth attendants. Interventions primarily focused on maternal and child health, STDs/STIs, and malaria employing educational programs in the form of training. Training included both short-term and long-term interactive educational sessions, along with outreach education programs and interactive seminars. Post-intervention improvements were observed in areas such as knowledge, diagnosis, referral services, contraceptive use, and medication appropriateness, although some studies reported negative outcomes. A context-specific optimum intervention strategy to improve healthcare delivery by IHCPs in LMICs was not identified overall.
Our results show that the interventions to improve the IHCPs’ delivery of healthcare services were heterogeneous and while the majority reported positive outcome(s), the improvements were inconsistent. Education and training were the most common interventions, leading to improved knowledge and skills of IHCPs, often resulting in improvement in health practices. However, when considering the training of IHCPs, greater attention is required to integrate it within a broader context of factors likely to promote better practices and reinforce the training. The effectiveness of training likely requires continuous efforts rather than one-time initiatives, and its retention should be evaluated at multiple points in time (14). As IHCPs operate within the private sector, their livelihood often depends on customer satisfaction and repeat business. As a result, interventions like external quality assessments, mandatory training programs, and the distribution of printed materials, which IHCPs believe do not affect their financial outcomes, have not been well customized (15, 16). Institutional innovations, like franchising, or locally tailored regulatory approaches, such as performance reviews, could create the necessary pressure for IHCPs to adhere to norms and deliver improved care (17). Training played a supplementary, yet potentially crucial, role alongside marketing efforts that could shape public expectations and demand. In our review, we also found that financial incentives as a market-based approach that involves using economic motivations to influence behaviors were useful (52). Similarly, interventions that altered incentives and enhanced accountability for providers were more effective in changing provider behaviors.
We found that a significant factor consistently influencing the delivery of healthcare services by IHCPs was the combination of interventions that mutually reinforced each other. For example, studies combined training with organizational changes to establish referral systems, integrating strategies such as accreditation and the provision of educational materials and resources. This approach proved effective across various subject areas and settings, ranging from establishing emergency trauma systems to assisting medicine sellers in managing sexually transmitted diseases to collaborating with traditional medical practitioners on family planning services (5, 18, 19). The range of studies on interventions with IHCPs is limited, indicating insufficient data to advocate for any specific intervention. Moreover, very few studies report on the costs of interventions, despite the necessity of this data to justify public funding. The overall impression is that the long-term effects of interventions with IHCPs are uncertain, and many of the strategies would be challenging to replicate. Very few studies provided detailed information about the interventions, such as training curricula, contents of birthing kits, or frequency of supervision. However, we found evidence supporting the effectiveness of IHCPs in certain medical conditions, such as lay health volunteers in tuberculosis, fever, and malaria management, and trained birth attendants in neonatal healthcare.
The studies included in our review do not definitively identify the most impactful interventions; however, it is evident that initiatives aimed at enhancing basic health service coverage through IHCPs or improving the quality of care they provide should be accompanied by rigorous evaluation research, publication of findings, and dissemination of lessons learned to maximize benefits (20, 21). The certainty of evidence generated was very low for all outcomes. Some interventions did not yield favorable results, and while study design issues might have played a role, other non-educational factors (e.g., deployment of anti-malarial medicine sellers and village health motivators or negotiation sessions) could indirectly hinder the promotion of appropriate dispensing in private pharmacies and medicine shops.
The strength of our study is the inclusion of a fairly large number of interventional studies across various LMICs and the comprehensive summary of the findings. The included studies were published between 1992 and 2021. The decision to search for a 35-year period was made to ensure a comprehensive review of the literature, capturing the historical evolution and long-term trends of interventions targeting IHCPs. While social changes in recent years are significant, the inclusion of earlier studies allows for a broader understanding of how interventions adapted over time. This wide margin provides a more complete picture of the evidence, identifying consistent patterns and emerging strategies that can inform current and future practices, despite the potential bias from earlier data. However, there are some limitations to this study. Only studies published in the English language were included. Changes in the practice of IHCPs over time contextualizing the societal perspective were not captured. Country-or context-specific interventions were not analyzed separately. The included studies had heterogeneities in the study populations, interventions, and outcomes and this debarred us from performing a meta-analysis. All required information was not available from all studies. Further limitations include the absence of providing a direction towards generalizability, sustainability, feasibility, and scalability of the interventions used across various studies and the certainty of evidence generated was very low for all outcomes.
There is a clear demand for high-quality intervention research targeting IHCPs. Given the high level of positive provider behaviors and knowledge among traditional birth attendants, further research into sustainable interventions and population-level outcomes with these providers would be particularly valuable. To achieve the greatest benefit, interventions should target providers most frequently used by the target demographic or for the target disease, rather than implementing blanket strategies across a geographic region (17, 21). Efforts should be directed toward identifying effective approaches for collaborating with traditional healers and unqualified doctors, who are relied upon by many. Given the constraints in resources to train and retain allopathic practitioners, both public and private health financiers must acknowledge the extensive market access and population interaction available to IHCPs. They have the potential to be valuable allies in extending the right to health for all individuals (22).
The practice of IHCPs raises ethical concerns about the quality of healthcare, accountability, and patient rights (23). The findings of this systematic review highlight the importance of addressing these considerations in policy and practice to safeguard patient outcomes and uphold ethical principles in the delivery of healthcare services. IHCPs must have adequate training and competency to deliver safe and effective care, respecting patients’ autonomy and right to informed decision-making, and addressing potential conflicts of interest, such as profit motives that may influence treatment decisions. Moreover, there is a need to balance the benefits of engaging IHCPs, such as improved access to care and cultural relevance, with potential risks, such as misdiagnosis, inappropriate treatment, and delays in seeking care from qualified healthcare professionals. The local context and situation also need to be addressed; for example, IHCPs were found to be useful in certain healthcare delivery during the Coronavirus Disease 2019 pandemic in LMICs (24, 25). By promoting transparency; accountability; and collaboration between IHCPs, formal healthcare providers, and regulatory bodies, various stakeholders can work together to ensure that patient care is delivered ethically and responsibly in a quality manner, ultimately improving health outcomes for underserved populations. It is essential to address the balance between the profit motives of IHCPs and the health goals of the public system.
The findings of this research may provide practical implications for various stakeholders in the healthcare system in LMICs. It is practical to recognize the role of IHCPs as primary care providers and the trust and acceptance they receive from the community (1–3). Regulatory bodies can establish guidelines for IHCPs to ensure compliance with quality care standards for fostering a people-centered health system (26). Often initiatives are taken from different stakeholders to train and integrate IHCPs as a part of the formal healthcare system (27). The Indian Medical Association does not endorse this (28) as this is illegal as per section 15.2(b) of the Indian Medical Council Act, 1965 (29). Healthcare providers and professional associations can collaborate with IHCPs to enhance care delivery, while community organizations and non-government organizations can implement targeted interventions to improve IHCP capacity. Overall, our findings can inform policy, practice, and community engagement efforts, aiming to improve the delivery of healthcare services by IHCPs and address health disparities for underserved populations.
5 Conclusion
In many LMICs, IHCPs often serve as the initial point of care for common illnesses like diarrhea, fever, and cough in children, as well as for family planning and reproductive healthcare in adults. Several multifaceted interventions coupled with training showed improvements in the delivery of healthcare services by IHCPs. However, the improvements were inconsistent across studies and the certainty of evidence generated was very low for all outcomes. Based on the review, it is difficult to identify any context-specific optimum intervention strategy to improve the delivery of healthcare services by IHCPs in LMICs. Implementing additional strategies, such as increased regulatory oversight, or the establishment of referral systems to qualified providers, alongside training, could enhance the delivery of healthcare services by IHCPs.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
SD: Writing – review & editing, Writing – original draft, Methodology, Investigation, Formal analysis, Data curation, Conceptualization. SK: Writing – review & editing, Writing – original draft, Methodology, Investigation, Formal analysis, Conceptualization. JE: Writing – review & editing, Supervision, Resources, Conceptualization. VD: Writing – review & editing, Supervision, Project administration, Conceptualization. CS: Writing – review & editing, Writing – original draft, Supervision, Resources, Project administration, Methodology, Conceptualization. KS: Writing – review & editing, Writing – original draft, Supervision, Resources, Project administration, Methodology, Investigation, Conceptualization.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
The authors acknowledge Ingrid Andersson and Emma-Lotta Säätelä from the University Library, Karolinska Institutet, Stockholm, Sweden for their kind support with the literature search.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2024.1456868/full#supplementary-material
References
1. Kumah, E . The informal healthcare providers and universal health coverage in low and middle-income countries. Glob Health. (2022) 18:45. doi: 10.1186/s12992-022-00839-z
2. Sudhinaraset, M, Ingram, M, Lofthouse, HK, and Montagu, D. What is the role of informal healthcare providers in developing countries? A systematic review. PLoS One. (2013) 8:e54978. doi: 10.1371/journal.pone.0054978
3. World Health Organization . The world health report: 2006: working together for health. (2006). Available at:The world health report 2006: Working together for health (https://www.who.int/)
4. McPake, B, and Hanson, K. Managing the public-private mix to achieve universal health coverage. Lancet. (2016) 388:622–30. doi: 10.1016/S0140-6736(16)00344-5
5. Shah, NM, Brieger, WR, and Peters, DH. Can interventions improve health services from informal private providers in low and middle-income countries?: a comprehensive review of the literature. Health Policy Plan. (2011) 26:275–87. doi: 10.1093/heapol/czq074
6. Sterne, JA, Hernán, MA, Reeves, BC, Savović, J, Berkman, ND, Viswanathan, M, et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ. (2016) 355:i4919. doi: 10.1136/bmj.i4919
7. Andrews, J, Guyatt, G, Oxman, AD, Alderson, P, Dahm, P, Falck-Ytter, Y, et al. GRADE guidelines: 14. Going from evidence to recommendations: the significance and presentation of recommendations. J Clin Epidemiol. (2013) 66:719–25. doi: 10.1016/j.jclinepi.2012.03.013
8. Singhal, N, McMillan, DD, Cristobal, FL, Arciaga, RS, Hocson, W, Franco, J, et al. Problem-based teaching of birth attendants in the PhilIHCPines. Health Care Women Int. (2001) 22:569–83. doi: 10.1080/07399330127196
9. Talukder, S, Farhana, D, Vitta, B, and Greiner, T. In a rural area of Bangladesh, traditional birth attendant training improved early infant feeding practices: a pragmatic cluster randomized trial. Matern Child Nutr. (2017) 13:e12237. doi: 10.1111/mcn.12237
10. Alisjahbana, A, Williams, C, Dharmayanti, R, Hermawan, D, Kwast, BE, and Koblinsky, M. An integrated village maternity service to improve referral patterns in a rural area in West-Java. Int J Gynaecol Obstet. (1995) 48:S83–94. doi: 10.1016/0020-7292(95)02323-5
11. Mbonye, AK, Bygbjerg, IC, and Magnussen, P. A community-based delivery system of intermittent preventive treatment of malaria in pregnancy and its effect on use of essential maternity care at health units in Uganda. Trans R Soc Trop Med Hyg. (2007) 101:1088–95. doi: 10.1016/j.trstmh.2007.06.017
12. Nsimba, SE . Assessing the impact of educational intervention for improving management of malaria and other childhood illnesses in Kibaha District-Tanzania. East Afr J Public Health. (2007) 4:5–11.
13. Kaona, FA, and Tuba, M. Improving ability to identify malaria and correctly use chloroquine in children at household level in Nakonde District. Northern Province Zambia Malar J. (2003) 2:43. doi: 10.1186/1475-2875-2-43
14. Das, J, Chowdhury, A, Hussam, R, and Banerjee, AV. The impact of training informal health care providers in India: a randomized controlled trial. Science. (2016) 354:aaf7384. doi: 10.1126/science.aaf7384
15. Mills, A, Brugha, R, Hanson, K, and McPake, B. What can be done about the private health sector in low-income countries? Bull World Health Organ. (2002) 80:325–30.
16. Travis, P, and Cassels, A. Safe in their hands? Engaging private providers in the quest for public health goals. Bull World Health Organ. (2006) 84:427. doi: 10.2471/BLT.06.032755
17. Patouillard, E, Goodman, CA, Hanson, KG, and Mills, AJ. Can working with the private for-profit sector improve utilization of quality health services by the poor? A systematic review of the literature. Int J Equity Health. (2007) 6:17. doi: 10.1186/1475-9276-6-17
18. Garcia, P, Hughes, J, Carcamo, C, and Holmes, KK. Training pharmacy workers in recognition, management, and prevention of STDs: district-randomized controlled trial. Bull World Health Organ. (2003) 81:806–14.
19. Husum, H, Gilbert, M, Wisborg, T, van Heng, Y, and Murad, M. Rural prehospital trauma systems improve trauma outcome in low-income countries: a prospective study from North Iraq and Cambodia. J Trauma. (2003) 54:1188–96. doi: 10.1097/01.TA.0000073609.12530.19
20. Bloom, G, Standing, H, Lucas, H, Bhuiya, A, Oladepo, O, and Peters, DH. Making health markets work better for poor people: the case of informal providers. Health Policy Plan. (2011) 26:i45–52. doi: 10.1093/heapol/czr025
21. Cross, J, and MacGregor, HN. Knowledge, legitimacy and economic practice in informal markets for medicine: a critical review of research. Soc Sci Med. (2010) 71:1593–600. doi: 10.1016/j.socscimed.2010.07.040
22. McPake, B, and Mills, A. What can we learn from international comparisons of health systems and health system reform? Bull World Health Organ. (2000) 78:811–20.
23. Thapa, P, Narasimhan, P, Jayasuriya, R, Hall, JJ, Mukherjee, PS, das, DK, et al. Barriers and facilitators to informal healthcare provider engagement in the national tuberculosis elimination program of India: an exploratory study from West Bengal. PLOS Glob Public Health. (2023) 3:e0001390. doi: 10.1371/journal.pgph.0001390
24. Posada, E, Mendoza, N, Alonso-Vega, C, Billot, C, Mallén Muñoz, B, de la Torre, L, et al. Lessons from community engagement to improve COVID-19 diagnosis and treatment in Cochabamba. Bolivia Glob Health Action. (2024) 17:2358602. doi: 10.1080/16549716.2024.2358602
25. Thapa, P, Lama, S, Rai, G, Sapkota, N, Pradhan, N, Thapa, R, et al. Family caregiver experience of caring COVID-19 patients admitted in COVID-19 hospital of a tertiary care hospital in Nepal. PLoS One. (2024) 19:e0295395. doi: 10.1371/journal.pone.0295395
26. Sieverding, M, and Beyeler, N. Integrating informal providers into a people-centered health systems approach: qualitative evidence from local health systems in rural Nigeria. BMC Health Serv Res. (2016) 16:526. doi: 10.1186/s12913-016-1780-0
27. Das, S, and Barnwal, P. The need to train uncertified rural practitioners in India. J Int Med Res. (2018) 46:522–5. doi: 10.1177/0300060517724948
28. Indian Medical Association Anti-quackery . (2023). Available at:Indian Medical Association (https://www.ima-india.org/ima/)
29. The Indian medical council Act , (1956). Available at: Medical Council of India Act.pdf (https://wbconsumers.gov.in/)
30. Oshiname, FO, and Brieger, WR. Primary care training for patent medicine vendors in rural Nigeria. Soc Sci Med. (1992) 35:1477–84. doi: 10.1016/0277-9536(92)90050-Z
31. Podhipak, A, Varavithya, W, Punyaratabandhu, P, Vathanophas, K, and Sangchai, R. Impact of an educational program on the treatment practices of diarrheal diseases among pharmacists and drugsellers. Southeast Asian J Trop Med Public Health. (1993) 24:32–9.
32. Kambo, IP, Gupta, RN, Kundu, AS, Dhillon, BS, Saxena, HM, and Saxena, BN. Use of traditional medical practitioners to delivery family planning services in Uttar Pradesh. Stud Fam Plan. (1994) 25:32–40. doi: 10.2307/2137987
33. Lynch, O, and Derveeuw, M. The impact of training and supervision on traditional birth attendants. Trop Dr. (1994) 24:103–7. doi: 10.1177/004947559402400303
34. Kumar, R . Training traditional birth attendants for resuscitation of newborns. Trop Dr. (1995) 25:29–30. doi: 10.1177/004947559502500109
35. Matthews, MK, Walley, RL, Ward, A, Akpaidem, M, Williams, P, and Umoh, A. Training traditional birth attendants in Nigeria--the pictorial method. World Health Forum. (1995) 16:409–13.
36. Miller, LC, Jami-Imam, F, Timouri, M, and Wijnker, J. Trained traditional birth attendants as educators of refugee mothers. World Health Forum. (1995) 16:151–6.
37. Pick, S, Reyes, J, Alvarez, M, Cohen, S, Craige, J, and Troya, A. AIDS prevention training for pharmacy workers in Mexico City. AIDS Care. (1996) 8:55–70. doi: 10.1080/09540129650125993
38. Nations MKde Souza, MA . Umbanda healers as effective AIDS educators: case-control study in Brazilian urban slums (favelas). Trop Dr. (1997) 27:60–6. doi: 10.1177/00494755970270S118
39. Marsh, VM, Mutemi, WM, Muturi, J, Haaland, A, Watkins, WM, Otieno, G, et al. Changing home treatment of childhood fevers by training shop keepers in rural Kenya. Trop Med Int Health. (1999) 4:383–9. doi: 10.1046/j.1365-3156.1999.00403.x
40. Schaider, J, Ngonyani, S, Tomlin, S, Rydman, R, and Roberts, R. International maternal mortality reduction: outcome of traditional birth attendant education and intervention in Angola. J Med Syst. (1999) 23:99–105. doi: 10.1023/A:1020537202451
41. Adu-Sarkodie, Y, Steiner, MJ, Attafuah, J, and Tweedy, K. Syndromic management of urethral discharge in Ghanaian pharmacies. Sex Transm Infect. (2000) 76:439–42. doi: 10.1136/sti.76.6.439
42. Smith, JB, Coleman, NA, Fortney, JA, Johnson, JD, Blumhagen, DW, and Grey, TW. The impact of traditional birth attendant training on delivery complications in Ghana. Health Policy Plan. (2000) 15:326–31. doi: 10.1093/heapol/15.3.326
43. Bailey, PE, Szászdi, JA, and Glover, L. Obstetric complications: does training traditional birth attendants make a difference? Rev Panam Salud Publica. (2002) 11:15–23. doi: 10.1590/s1020-49892002000100003
44. Chalker, J, Chuc, NT, Falkenberg, T, and Tomson, G. Private pharmacies in Hanoi, Vietnam: a randomized trial of a 2-year multi-component intervention on knowledge and stated practice regarding ARI, STD and antibiotic/steroid requests. Trop Med Int Health. (2002) 7:803–10. doi: 10.1046/j.1365-3156.2002.00934.x
45. Ratanajamit, C, Chongsuvivatwong, V, and Geater, AF. A randomized controlled educational intervention on emergency contraception among drugstore personnel in southern Thailand. J am med Womens Assoc. (1972) 57:196-9
46. Poudyal, AK, Jimba, M, Murakami, I, Silwal, RC, Wakai, S, and Kuratsuji, T. A traditional healers' training model in rural Nepal: strengthening their roles in community health. Trop Med Int Health. (2003) 8:956–60. doi: 10.1046/j.1365-3156.2003.01094.x
47. Tavrow, P, Shabahang, J, and Makama, S. Vendor-to-vendor education to improve malaria treatment by private drug outlets in Bungoma District. Kenya Malar J. (2003) 2:10. doi: 10.1186/1475-2875-2-10
48. Tumwikirize, WA, Ekwaru, PJ, Mohammed, K, Ogwal-Okeng, JW, and Aupont, O. Impact of a face-to-face educational intervention on improving the management of acute respiratory infections in private pharmacies and drug shops in Uganda. East Afr Med J. (2004) Suppl:S25–32.
49. Chalker, J, Ratanawijitrasin, S, Chuc, NT, Petzold, M, and Tomson, G. Effectiveness of a multi-component intervention on dispensing practices at private pharmacies in Vietnam and Thailand—a randomized controlled trial. Soc Sci Med. (2005) 60:131–41. doi: 10.1016/j.socscimed.2004.04.019
50. Peltzer, K, Mngqundaniso, N, and Petros, G. A controlled study of an HIV/AIDS/STI/TB intervention with traditional healers in KwaZulu-Natal. South Africa AIDS Behav. (2006) 10:683–90. doi: 10.1007/s10461-006-9110-x
51. Tawfik, Y, Nsungwa-Sabitii, J, Greer, G, Owor, J, Kesande, R, and Prysor-Jones, S. Negotiating improved case management of childhood illness with formal and informal private practitioners in Uganda. Trop Med Int Health. (2006) 11:967–73. doi: 10.1111/j.1365-3156.2006.01622.x
52. Onwujekwe, O, Uzochukwu, B, Ojukwu, J, Dike, N, and Shu, E. Feasibility of a community health worker strategy for providing near and appropriate treatment of malaria in Southeast Nigeria: an analysis of activities, costs and outcomes. Acta Trop. (2007) 101:95–105. doi: 10.1016/j.actatropica.2006.07.013
53. Shah, SA, Kristensen, S, Memon, MA, White, HL, and Vermund, SH. Syndromic management training for non-formal care providers in Pakistan improves quality of care for sexually transmitted diseases STD care: a randomized clinical trial. Southeast Asian J Trop Med Public Health. (2007) 38:737–48.
54. Abuya, T, Fegan, G, Rowa, Y, Karisa, B, Ochola, S, Mutemi, W, et al. Impact of ministry of health interventions on private medicine retailer knowledge and practices on anti-malarial treatment in Kenya. Am J Trop Med Hyg. (2009) 80:905–13. doi: 10.4269/ajtmh.2009.80.905
55. Sima, BT, Belachew, T, Bjune, G, and Abebe, F. Traditional healers' role in the detection of active tuberculosis cases in a pastoralist community in Ethiopia: a pilot interventional study. BMC Public Health. (2019) 19:721. doi: 10.1186/s12889-019-7074-9
56. Sundararajan, R, Ponticiello, M, Lee, MH, Strathdee, SA, Muyindike, W, Nansera, D, et al. Traditional healer-delivered point-of-care HIV testing versus referral to clinical facilities for adults of unknown serostatus in rural Uganda: a mixed-methods, cluster-randomised trial. Lancet Glob Health. (2021) 9:e1579–88. doi: 10.1016/S2214-109X(21)00366-1
57. Andrews, JC, Schünemann, HJ, Oxman, AD, Pottie, K, Meerpohl, JJ, Coello, PA, et al. GRADE guidelines: 15. Going from evidence to recommendation-determinants of a recommendation's direction and strength. J Clin Epidemiol. (2013) 66:726–35. doi: 10.1016/j.jclinepi.2013.02.003
58. Hamid Salim, MA, Uplekar, M, Daru, P, Aung, M, Declercq, E, and Lönnroth, K. Turning liabilities into resources: informal village doctors and tuberculosis control in Bangladesh. Bull World Health Organ. (2006) 84:479–84. doi: 10.2471/BLT.05.023929
59. Higgins, JPT, Thomas, J, Chandler, J, Cumpston, M, Li, T, et al. Cochrane handbook for systematic reviews of interventions version 6.4 (updated august 2023). Cochrane, (2023). Available at:www.training.cochrane.org/handbook
60. Jokhio, AH, Winter, HR, and Cheng, KK. An intervention involving traditional birth attendants and perinatal and maternal mortality in Pakistan. N Engl J Med. (2005) 352:2091–9. doi: 10.1056/NEJMsa042830
61. Somsé, P, Chapko, MK, Wata, JB, Bondha, P, Gonda, B, Johnson, D, et al. Evaluation of an AIDS training program for traditional healers in the Central African Republic. AIDS Educ Prev. (1998) 10:558–64.
62. World Health Organization . International classification of health interventions (ICHI). (2003). Available at:International Classification of Health Interventions (ICHI) (https://www.who.int/)
Keywords: healthcare services, informal healthcare providers (IHCPs), intervention, low-and middle-income countries Normal, left
Citation: Das S, Khare S, Eriksen J, Diwan V, Stålsby Lundborg C and Skender K (2024) Interventions on informal healthcare providers to improve the delivery of healthcare services in low-and middle-income countries: a systematic review. Front. Public Health. 12:1456868. doi: 10.3389/fpubh.2024.1456868
Edited by:
Ana Pires, Universidade Atlântica, PortugalReviewed by:
Syed Mustafa Ali, The University of Manchester, United KingdomFátima Méndez-López, University of Zaragoza, Spain
Copyright © 2024 Das, Khare, Eriksen, Diwan, Stålsby Lundborg and Skender. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shweta Khare, c2h3ZXRhLmtoYXJlQGtpLnNl
†These authors share first authorship