
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 24 October 2024
Sec. Infectious Diseases: Epidemiology and Prevention
Volume 12 - 2024 | https://doi.org/10.3389/fpubh.2024.1454759
 Yuqing Jin1
Yuqing Jin1 Huiyao Feng2
Huiyao Feng2 Qin Xiao1
Qin Xiao1 Fenglin Tian1
Fenglin Tian1 Huan Yao1
Huan Yao1 Runquan Zhang1
Runquan Zhang1 Qiqi Wu1Haiyuan Zhu1
Qiqi Wu1Haiyuan Zhu1 Wanshan Zheng1Jin Chen1
Wanshan Zheng1Jin Chen1 Tao Liu1
Tao Liu1 Wenjun Ma1Xiongfei Chen3*
Wenjun Ma1Xiongfei Chen3* Xiaomei Dong1*
Xiaomei Dong1*Background: Primary healthcare workers in China were vital in controlling COVID-19, facing unprecedented challenges due to the pandemic’s suddenness and transmissibility. This paper analyzed their work in Guangzhou, highlighting key difficulties in past epidemic control efforts.
Methods: Semi-structured qualitative interviews were conducted with selected primary healthcare workers in Guangzhou City and audio-recorded until saturation of themes was reached. The data were analyzed independently for themes using NVivo V.12.
Results: Thematic analysis of qualitative interview data revealed that challenges and difficulties encountered in grassroots epidemic prevention and control work during the COVID-19 pandemic were primarily categorized into seven dimensions: human resource allocation, material and vehicle support, epidemic prevention subsidies and compensation, humanistic care, upper-level management, horizontal collaboration, and resident cooperation.
Conclusion: Based on the findings, the research team recommends that administrative departments and institutions related to primary healthcare should appropriately schedule personnel work and rest time, adjust work content flexibly, optimize the allocation of medical and logistical resources, and increase investment in primary healthcare work as well as staff protection.
Since the outbreak of the COVID-19 pandemic at the end of 2019, this global public health crisis had a far-reaching impact on the healthcare systems of various countries (1). Guangzhou, located in the southern part of China, is the capital city of Guangdong Province, a national central city, and a mega-city. It serves as a major transportation hub and a comprehensive transportation hub city, acting as the southern gateway for China’s connection with the world. With a high degree of urbanization, Guangzhou has a vast population of permanent and transient residents. Guangdong Province bore the greatest pressure of overseas COVID-19 importation cases during the pandemic, with nearly 30,000 people under quarantine daily. As the most important city in Guangdong Province, Guangzhou Baiyun International Airport handled a huge passenger flow. The large number of people under entry quarantine observation increased the risk of disease transmission during the pandemic. This necessitated a more proactive approach by the primary healthcare system in tracking, testing, and isolating cases (2). Primary healthcare institutions not only needed to maintain daily medical services, but also had to respond and adapt quickly to the new requirements of epidemic prevention and control (3).
In the normalization of COVID-19 prevention and control, primary healthcare institutions bore the responsibility for early detection, early treatment, and early intervention, serving as the linchpin in preventing sustained community transmission of the epidemic (4). Under government directives, primary healthcare institutions established a joint prevention and control system, horizontally coordinating with communities and street offices to provide basic medical and public health services to residents within their jurisdiction. Activities such as education and promotion, home isolation, and nucleic acid sampling constitute their pandemic prevention and control efforts. Vertically, they strengthened connections with higher-level healthcare institutions and disease control centers, strictly implementing the responsibility system for initial diagnosis. They ensured the smooth transfer of suspected fever patients and guide fever patients to seek medical treatment (5).
Primary healthcare workers played an essential role in public health crises, acting as the frontline workers of the public health system. Their responsibilities were not limited to routine diagnosis and treatment but also involved epidemic monitoring, case tracking, health education, and vaccination programs (6). In large cities like Guangzhou, they were the bridge connecting residents to higher-level medical services. Their work was related not only to individual health but also to the public health safety of the entire community and city.
Studies had shown that the rapid changes in the pandemic required primary healthcare workers to continuously update their knowledge and skills to adapt to new prevention and control guidelines and treatment methods (7). Furthermore, due to the uncertainty of the pandemic, they often had to make quick decisions under limited resources, which increased work pressure and occupational risks (8). Additionally, primary healthcare workers needed to address panic and misunderstandings from patients and the public, which demanded stronger communication skills and psychological support techniques (9). During the COVID-19 pandemic, anxiety and depression were widespread among primary healthcare workers (10). The prevalence of sleep disorders was higher among the frontline healthcare workers compared to the non-frontline and non-medical staff, while anxiety and depression were prevalent in the entire cohort (11).
This study utilized qualitative interview methods to explore the work experiences of primary healthcare workers in Guangzhou during the COVID-19 epidemic prevention and control period. The research aimed to identify the primary difficulties and challenges they faced in their professional duties, analyze the causes of these issues, and offer recommendations for improvement based on the findings of the investigation. Although the COVID-19 pandemic has ended, the weaknesses exposed in the epidemic prevention and control work during this period require our continuous reflection. The significance of this study lies not only in the difficulties encountered in grassroots epidemic prevention work during the COVID-19 period but also in gaining a better understanding of the complexity and challenges of epidemic prevention and control. It is essential to continuously summarize experiences and learn lessons to prepare for potential public health events that may arise in the future.
The study participants were selected from primary healthcare institutions in Guangzhou City, based on specific inclusion criteria: (1) They have been involved in grassroots COVID-19 epidemic prevention and control work since June 2021 or even earlier, possessing extensive on-site experience and a profound understanding of grassroots epidemic prevention work; (2) Their involvement in grassroots epidemic prevention work includes activities such as nucleic acid sampling, household management, vaccine administration, transportation of high-risk individuals, operation of epidemic prevention systems, and three-person team investigations; (3) They provided informed consent and voluntarily participated in the study.
Purposive sampling was used in this study to select eligible healthcare workers engaged in grassroots epidemic prevention from healthcare institutions. Across Tianhe, Baiyun, and Liwan districts. Tianhe, as the Central Business District (CBD) of Guangzhou City, was characterized by a high degree of urbanization and bustling commercial activities. With significant population mobility and frequent economic activities, this area faced unique challenges in epidemic prevention and control. Baiyun was one of the most populous areas in Guangzhou City. The dense population led to more complex demands for epidemic prevention and control. Liwan, an old town area of Guangzhou City, was the first area in Guangzhou to implement community-level epidemic lockdown and management measures, which provided it with unique experiences and lessons in epidemic prevention and control (12). The selected primary healthcare workers included a variety of professional types, such as general practitioners, public health physicians, nurses, and administrative personnel. The sample size was determined through information saturation (13, 14), where data collection proceeded until no new insights emerged from additional interviews.
This study utilized qualitative research methods, conducting semi-structured interviews with epidemic prevention personnel and special team members from primary-level medical and health institutions. The aim was to explore the status of grassroots epidemic prevention work, the existing problems and their impacts, the needs for protective measures for the epidemic prevention staff, and suggestions for the optimization of grassroots epidemic prevention efforts. Qualitative research data are collected through a variety of means, such as interviews, direct observations, personal narrative statements, documents, photographs, and audio or video recordings (15). Investigators have the flexibility to change the content and flow of questions when needed to explore deeper meanings (16). The use of qualitative research allowed for an understanding of new phenomena (17), which was crucial for mitigating the difficulties and challenges faced by primary healthcare workers in epidemic prevention work. The findings from the analysis called for action to be taken.
We applied the thematic analysis approach proposed by Braun and Clarke to identify themes from the collected data (18). Thematic Analysis is a qualitative research data analysis technique that involves searching within datasets to identify, analyze, and report recurring patterns known as themes. This method not only describes data but also performs interpretive work during the selection of codes and the construction of themes, demonstrating its flexibility and independence from specific epistemological frameworks. Braun and Clarke define a theme as a “patterned response or meaning,” distinguishing between latent and semantic themes. Semantic themes deal with explicit or surface meanings in the data, while latent themes reveal deeper implications, assumptions, or meaning formations. The six-step analysis method they propose is a nonlinear and recursive process that includes familiarizing oneself with the data, forming initial codes, searching for themes, reviewing themes, defining and naming themes, and writing the analytical report. Thematic Analysis is oriented towards addressing research questions. Although its process is similar to Grounded Theory, its core objective is not to find core concepts that reflect the essence of phenomena and construct related theories based on systematic data collection. Instead, it aims to identify and refine “themes” from raw data and use these themes to analyze research questions (19). Thematic Analysis differs from Content Analysis in methodology as well. Content Analysis systematically encodes, classifies, and semantically judges text content to analyze word frequency and relationships between terms, focusing on a more quantified approach to research questions (20). In contrast, Thematic Analysis does not solely rely on word frequency to identify “themes” but bases its analysis on the thematic relevance to the research issue, which may appear frequently or infrequently in the data.
To protect the rights and interests of interviewees, prior to conducting interviews, interviewers proactively inform participants that their contributions will remain anonymous and solely utilized for research purposes. It is ensured that the interviews do not violate any rights of the participants, who retain the right to voluntary participation, refusal, or withdrawal from the study. All interviews are conducted in familiar and quiet settings, with participants’ informed consent obtained before recording. Interviewers adhere to the original interview outline but also delve deeper into relevant topics based on participants’ responses. They promptly adjust questioning methods and sequences in response to interview data to ensure the collection of authentic and accurate information.
Prior to undertaking our research, our project team first engaged in direct participation, immersing ourselves in grassroots epidemic prevention work. This firsthand experience provided us with invaluable primary data and a profound understanding of the challenges faced at the grassroots level. Building upon this foundation, we conducted an extensive review of literature related to qualitative interviews and studied literature concerning the difficulties and challenges encountered in grassroots epidemic prevention work. Based on our practical experience and literature review, we formulated a detailed interview protocol. As detailed in Table 1.
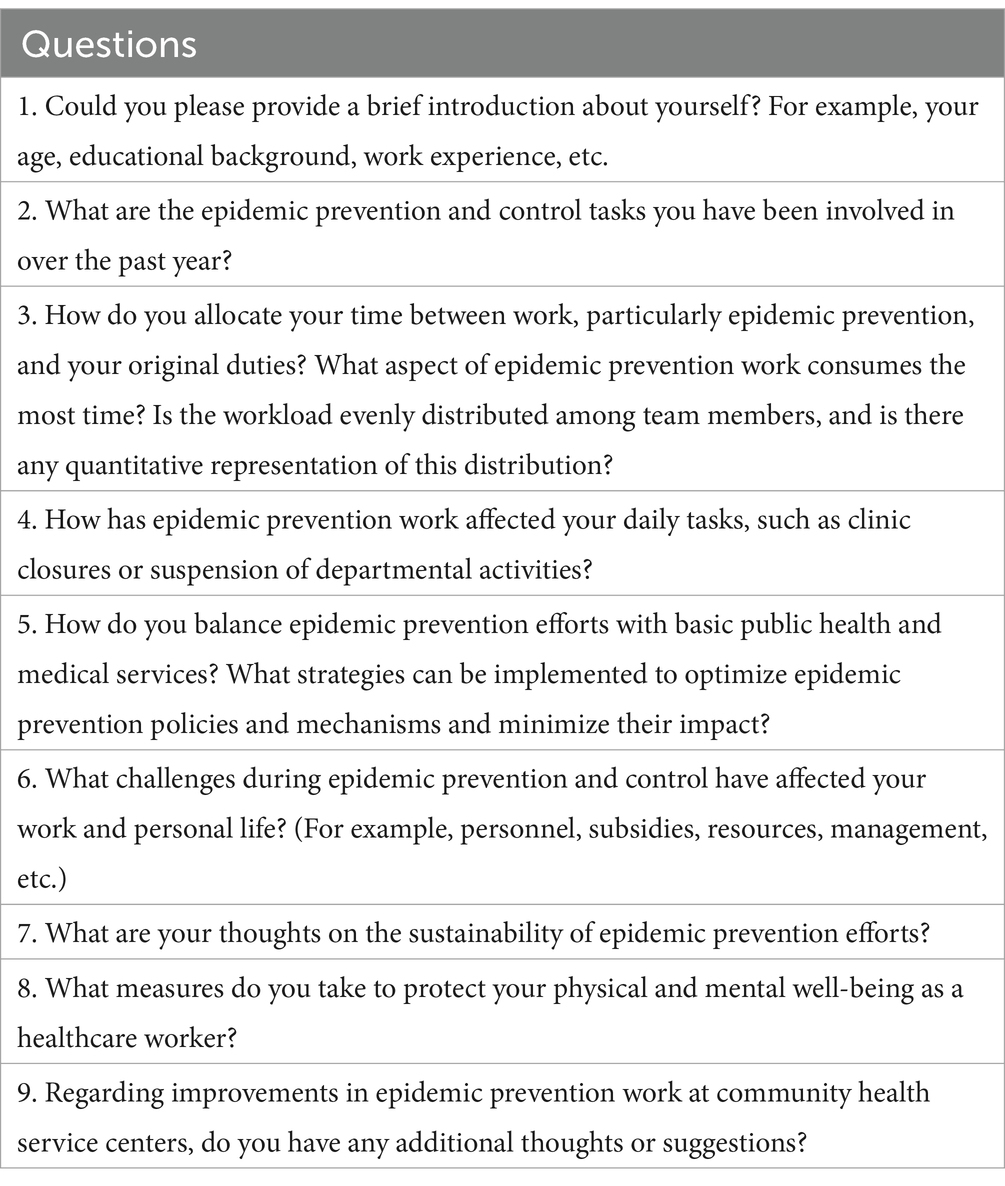
Table 1. Semi-structured interview outline.
Interviews were conducted by two researchers (JYQ and FHY) in two-person teams, with one researcher taking the lead in guiding participants through the interviews, while the second researcher was responsible for taking field notes and prompting the participants when necessary. Before commencing the interview, the interviewer explained the interview’s purpose and content to the participant, confirmed the interview details including time and location, and proceeded with complete audio recording throughout the interview. Key points were also noted down in writing. Before the formal interview, 5–10 min were spent explaining in detail the purpose, content, and methods of the study, as well as confidentiality commitments, the voluntary nature of the research, and the required informed consent. The formal interview lasted approximately 45–60 min. Throughout the interview, appropriate communication techniques were employed, with the interviewer avoiding directive statements and actively encouraging the interviewee to freely articulate their perspectives. The interview questions and sequence were flexibly adjusted based on the interviewee’s responses and interests. Each participant was interviewed only once. To ensure the completeness and accuracy of the interview materials, the written record was returned to the participant for corrections at the end of the interview. On the same day the interview was conducted, the audio recording and notes were integrated to form textual content, which was then sent to the interviewee for review and final confirmation.
To ensure interviewees’ privacy, numerical codes are assigned sequentially based on interview time. Following interviews, recorded content is transcribed into text on the same day. We employed NVivo V.12 for the management, storage, and organization of all data. We scrutinized and analyzed the data using thematic analysis, identifying and extracting key themes through a rigorous structured analysis methodology that ensured a structured academic approach to thematic analysis. (1) Familiarization: The text is thoroughly reviewed multiple times to understand interviewee contributions. (2) Coding: Meaningful segments (e.g., phrases, sentences, paragraphs) relevant to research questions are identified and coded preliminarily. (3) Theme Development: Initial themes are derived from coded segments, and all relevant codes and excerpts are categorized under each theme. (4) Theme Review: Themes and corresponding excerpts are reviewed for consistency and completeness, ensuring no relevant codes are overlooked. (5) Refinement: Themes are further refined for clarity and coherence, organizing excerpts to construct cohesive narratives. (6) Reporting: Findings are summarized and documented in the final report. All interviews were transcribed verbatim by the first author (JYQ) and checked for accuracy and completeness by a second researcher (FHY). Triangulation was employed to ensure the credibility of the analysis. This involved randomly selecting 10% of the transcripts for independent analysis by researchers who were not involved in the data collection process. In cases of discrepancies, team meetings were frequently held to discuss and review until a consensus was reached. The sample became saturated after the 12th interview, and two additional interviews were conducted to ensure that no more data could be collected. No participants withdrew during the interview period.
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board of Jinan University (NO.JNUKY-2023-0037). The study team obtained informed consent from all participants. Participants were made aware that they could withdraw at any time.
In this study, a total of 14 healthcare workers from three districts of Guangzhou City, who had participated in grassroots epidemic prevention work, were interviewed. Among them, there were 7 males and 7 females, all with undergraduate degrees. Their positions included public health physicians, general practitioners, nursing management personnel, and hospital infection control department heads, among others. Please refer to Table 2.
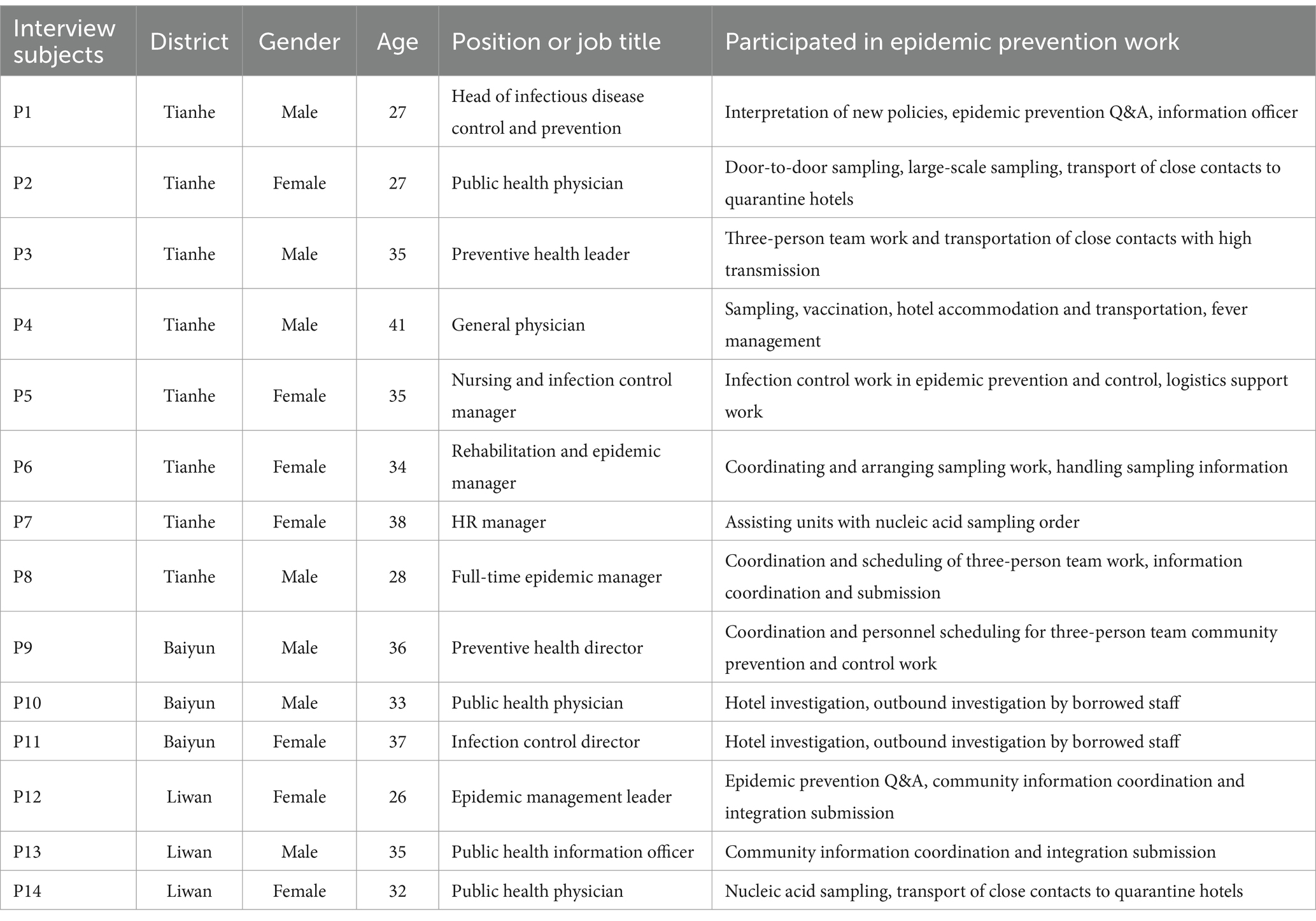
Table 2. General information of interviewees.
By organizing and summarizing the interview results, the difficulties in grassroots epidemic prevention work were primarily categorized into seven dimensions: human resource allocation, material and vehicle support, epidemic prevention subsidies and compensation, humanistic care, upper-level management, horizontal collaboration, and resident cooperation. Please refer to Table 3.
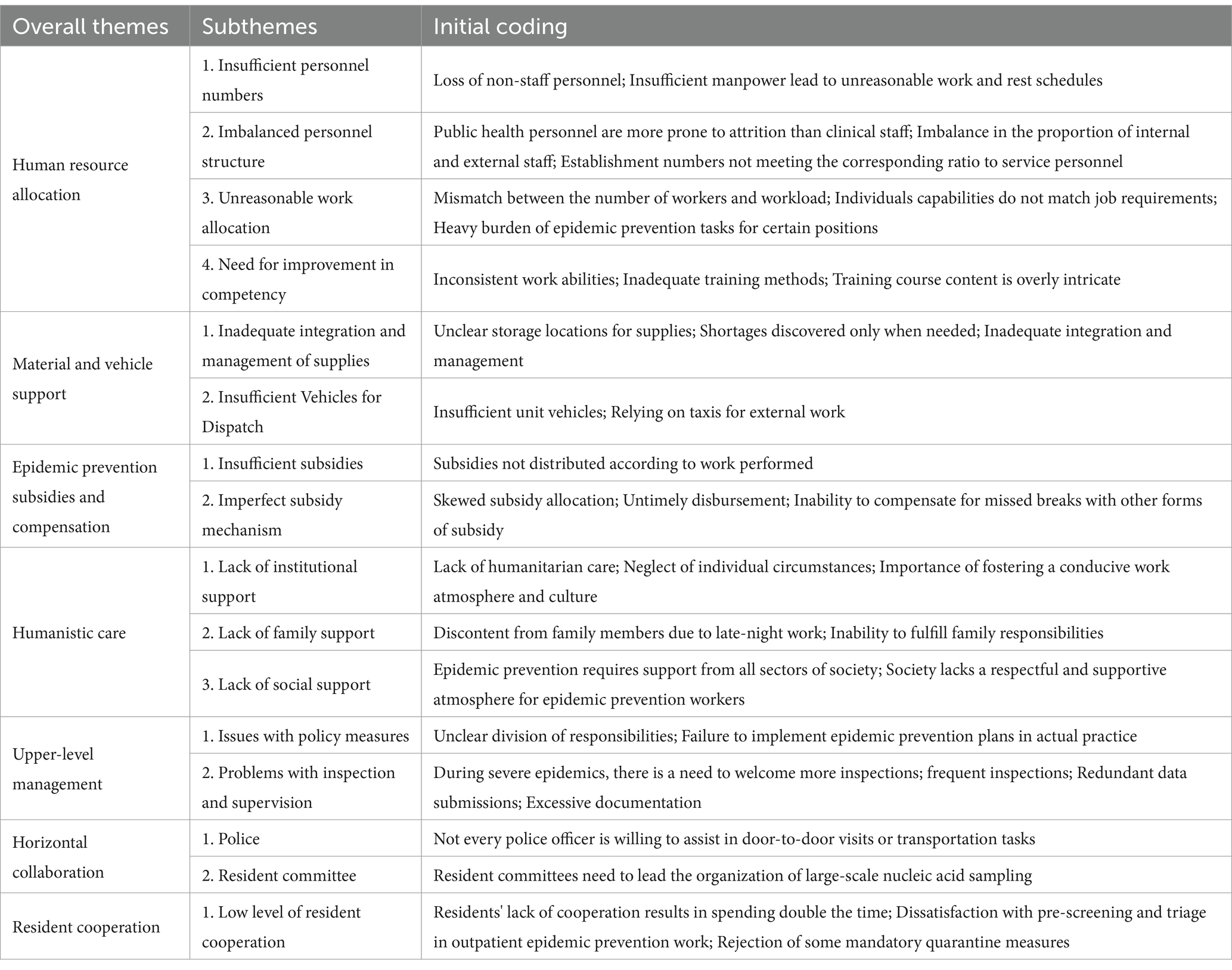
Table 3. Initial coding, key themes, and overall themes of theme analysis.
The grassroots epidemic prevention work, due to its heavy and complex nature, demands a significant amount of human resources. However, the reality faced by the majority of grassroots epidemic prevention personnel was a shortage of workers. This shortage forced the remaining workers to take on a workload beyond the ordinary, leading to a sharp increase in their work intensity and prolonged exposure to a high-pressure work environment. This state of overload not only posed a threat to the health and well-being of individuals but also severely affected work efficiency and service quality. What was even more serious was that the heavy burden of epidemic prevention caused by the personnel gap made the remaining workers more likely to choose to leave when facing sustained work pressure, thereby exacerbating the problem of personnel turnover. The departure of personnel not only weakened the strength of grassroots epidemic prevention but also further expanded the personnel gap, creating a vicious cycle.
“Staff attrition, especially non-official personnel leaving, many have departed, and even if new ones arrive, they soon leave as well” (P1).
“The most prominent issue is the shortage of manpower, which leads to unreasonable scheduling of work and rest time” (P3).
“Staff attrition can be severe, especially in public health” (P4).
“The shortage of manpower is not only a problem in our unit, but in fact, every grassroots unit lacks sufficient personnel” (P9).
Primary healthcare institutions serve as the cornerstone of the public health system, and the services they provide are directly linked to the health and well-being of community residents. If these institutions faced a shortage of healthcare personnel in specific professional fields, it would severely impact the quality and efficiency of grassroots health services, thereby affecting the overall epidemic prevention status of the community. Furthermore, when there was an insufficiency of workers in certain professional fields, healthcare workers from other fields might have had to bear additional workloads to compensate for the service gaps.
“The lack of specialized public health physicians and insufficient manpower result in a significant proportion of frontline clinical medical staff participating in epidemic control, thereby impeding the effective delivery of medical services” (P4).
“An uneven personnel structure affects the entire department, including scheduling at the center and other work arrangements” (P5).
There was a mismatch between the number of personnel and the workload, which led to a decline in work efficiency and service quality. Specifically, there was an insufficient number of workers for heavy-duty tasks, while there was an excess for simpler tasks. This imbalanced allocation severely affected the progress and effectiveness of the overall work. Additionally, the issue of personnel capabilities not aligning with the nature of the work could not be overlooked. If the professional skills and experience of the workers did not match the tasks they undertook, it would be difficult for them to perform at their best, thereby affecting the progress and outcomes of the work. The distribution of epidemic prevention tasks was overly skewed towards some primary healthcare workers, which not only subjected them to unreasonable work burdens but also hindered the effective conduct of their primary duties.
“Almost all epidemic prevention tasks require public health personnel to be dispatched because we do not need to run outpatient clinics, so there will definitely be more epidemic prevention shifts” (P2).
“The epidemic control consumes most of our time and manpower, resulting in a lag in public health work, yet the targets from higher-ups have not decreased but increased” (P3).
“Some positions require young computer-savvy individuals to work fast, but sometimes older individuals are assigned computer tasks” (P12).
“Many non-medical technical issues are handled by medical personnel, with excessive paperwork consuming manpower for management and organization” (P13).
As the frontline warriors in the fight against the pandemic, the learning ability and professional literacy of primary healthcare workers were key to ensuring the smooth progress of epidemic control work. In the ever-changing environment of the epidemic, these capabilities were particularly crucial. Only with the ability to quickly adapt to and respond to new situations, coupled with solid professional literacy, could primary healthcare workers properly handle the heavy and complex tasks of grassroots epidemic prevention. However, in the face of intense and heavy work tasks, the issues of insufficient capability and professional training among some workers gradually emerged. These issues not only affected the efficiency and quality of epidemic prevention work but also had adverse effects on the career development and mental health of the workers themselves.
“There is disparity in work capabilities. Some individuals simply do not grasp it, no matter how much you teach them, while others understand it instantly” (P1).
“These matters are specialized. They cannot be understood with just a few words” (P3).
“There are some online training sessions, but in reality, few people attend them because everyone is very busy. Many individuals initially performing nucleic acid sampling at the grassroots level do not follow standardized procedures” (P7).
To ensure the smooth progress of grassroots epidemic prevention work, it was imperative for primary-level medical and health institutions to stock up on ample epidemic prevention supplies. However, merely stockpiling supplies was not sufficient; effective integration and management of these supplies were crucial for enhancing the efficiency of usage and ensuring the efficient conduct of epidemic prevention work. At present, some units had issues with supply management that urgently needed to be addressed. During an outbreak, it was vital to quickly and accurately allocate supplies to where they were needed. If the information on supplies was unclear, the inventory data was inaccurate, or the allocation process was complex, it could delay the distribution of epidemic prevention supplies, affecting the timeliness and effectiveness of epidemic prevention work.
“Supplies are not effectively integrated, and sometimes it’s only when needed that we realize they are not available, as there is no designated personnel to organize them” (P2).
“Sometimes colleagues return from work and just randomly place supplies in the room. Despite having personnel assigned to regular cleanup, it still remains disorderly” (P10).
“Supplies are not effectively arranged. They are just categorized and placed aside. There is no dedicated public health emergency warehouse” (P11).
The epidemic prevention work of primary healthcare workers not only included door-to-door investigation and sampling for the homebound population but also involved real-time monitoring of the epidemic and rapid response. In this process, the guarantee of transportation was one of the key factors to ensure the smooth progress of epidemic prevention work. Insufficient transportation support directly affected the efficiency of epidemic prevention work. If transportation facilities were inconvenient, it would greatly increase their travel time, reduce work efficiency, and even possibly miss the best opportunity for epidemic prevention. However, this need was often overlooked in actual operations.
“We have insufficient vehicles. Often, when going out for work, we need to take taxis ourselves, which is very inconvenient” (P1).
“The main issue is the shortage of vehicles. Routine tasks and emergency support cannot be balanced” (P4).
“Vehicle use is indeed a problem. Sometimes, our unit’s vehicles cannot even be coordinated. Just because the unit has a car does not mean it can be used directly for you.” (P14).
Primary healthcare workers played an irreplaceable role on the frontlines of combating the epidemic, bearing immense work pressure and occupational risks. After completing a large amount of epidemic prevention work, reasonable subsidies and compensation were crucial for enhancing their work enthusiasm, safeguarding their rights and interests, and motivating their continued commitment to epidemic prevention. However, there were still issues where some workers did not receive the due subsidies or did not receive compensation according to their labor, and economic uncertainty might have made it difficult for them to fully commit to their work, affecting the quality and efficiency of their work. This not only affected their motivation but also posed a challenge to the long-term effectiveness of grassroots epidemic prevention work.
“There are no epidemic prevention allowances for those of us who are in official positions. There might be some for non-official positions, but we still cannot retain personnel, indicating that the epidemic prevention subsidy is indeed very minimal” (P1).
“We have subsidies, but I think they are not substantial” (P2).
“We are in official positions, so it’s okay, but for those who are not, the pay is not much. Indeed, because of this issue, we have had at least five or six people resign” (P11).
“The workload is high, but the subsidies are minimal” (P14).
The epidemic prevention subsidy mechanism was an essential safeguard to ensure that primary healthcare workers received necessary support and incentives when facing the challenges of the epidemic. A robust subsidy system could not only provide them with necessary financial support but also reflect recognition and respect for their hard work. However, due to the imperfections in the subsidy mechanism at the time, there were some urgent issues in the distribution and implementation of epidemic prevention subsidies, such as biased distribution of subsidies, delays in disbursement, and the inability to convert untaken leave into other forms of compensation.
“The subsidies are not distributed promptly. It’s usually delayed by half a year or even a year” (P2).
“Official personnel cannot take compensatory leave, and it cannot be exchanged for other allowances” (P4).
“For official personnel, there is basically no epidemic prevention subsidy for outbound sampling or vaccine administration, but temporary hires may receive it. The subsidy policy is also not very comprehensive, and the disbursement is not timely enough” (P10).
After engaging in long-term epidemic prevention and control work, primary healthcare workers not only faced physical fatigue but also had to cope with psychological stress. Under such circumstances, the support from their organization became a crucial factor in enabling primary healthcare workers to continue their efforts. However, numerous issues had persisted in various aspects such as work management systems, personal development opportunities, welfare benefits, and physical and mental health care.
“The arrangement of work and rest time is unreasonable because time is spent on what I personally consider meaningless tasks” (P1).
“The compensatory leave system urgently needs improvement, as it is vital for safeguarding the lives of grassroots epidemic prevention workers” (P4).
“There should be an increase in welfare subsidies and opportunities for civil service examination, especially for contractual employees” (P6).
“During maternity leave, there is no compensation, indicating inadequate humanistic care” (P14).
Primary healthcare workers not only bore the heavy burden of grassroots epidemic prevention work but also almost every individual shoulders their family responsibilities. When work responsibilities consumed most of one’s time and energy, solving family concerns became a challenge. The prolonged work and constant state of readiness made it difficult for grassroots epidemic prevention personnel to devote sufficient time and energy to their family life. This not only affected the time they spent with their family but could also lead to emotional estrangement among family members, increasing the stress on family relationships.
“Physical fitness declines, leading to anxiety, and nighttime work outings cause dissatisfaction among family members” (P1).
“There’s conflict between work and family. Even when working from home, there’s no time to take care of the children” (P3).
“There’s conflict between work and family. Since the outbreak of the epidemic, I have not been home for major holidays” (P10).
“In dual-income families, both parents are on assignment, leaving no one to care for the children” (P11).
The importance of grassroots epidemic prevention work often exceeded the general public’s understanding. This job not only required primary healthcare workers to have professional knowledge and skills, but also demanded a significant investment of energy and emotion, facing high-intensity work pressure and complex work situations. However, when this heavy responsibility and hard work did not receive widespread understanding and support from society, some primary healthcare workers might have felt even more physically and mentally exhausted. This situation reflected a deficiency in the support and encouragement of grassroots epidemic prevention personnel by current social opinion and relevant social departments.
“Epidemic prevention work is overwhelming, leading to significant psychological stress and a lack of understanding from others” (P2).
“I hope that grassroots unions can offer diverse forms of support and care” (P5).
“I hope that teachers in schools can pay attention to students’ studies. Because during the epidemic, there has not been much time to focus on children’s learning” (P7).
The continuous evolution of the epidemic posed new challenges to epidemic prevention work, requiring policy measures to be updated in a timely manner to adapt to new situations. However, primary healthcare workers sometimes encountered problems with policy measures when executing their tasks, which affected the efficiency and effectiveness of the epidemic prevention work. The ambiguity of work guidelines brought operational confusion to primary healthcare workers. Epidemic prevention measures required specific and clear guidance so that workers could execute them swiftly and accurately. The vagueness of the guidelines not only increased the difficulty of execution but could also lead to the inadequate implementation of epidemic prevention measures, affecting the effectiveness of control. Moreover, in epidemic prevention work, every link was crucial, requiring clear responsibility allocation to ensure that every worker was aware of their duties and tasks. Unclear division of responsibilities could lead to overlapping or omission of work, affecting the coordination and coherence of the overall epidemic prevention work.
“Superiors often distribute documents without thoroughly reading and understanding them” (P1).
“When problems arise in epidemic prevention work, it’s difficult to identify the responsible unit or individual because the documents lack specificity and the division of responsibilities is unclear” (P4).
“Epidemic prevention measures are continually intensified without clear benchmarks. Without clear guidance at the grassroots level, it’s challenging to implement control measures” (P8).
“While there are overarching frameworks and documents, each individual’s interpretation of the documents may vary” (P13).
Inspection and supervision were key to ensuring the efficiency and orderliness of grassroots epidemic prevention work, playing an irreplaceable role in identifying problems promptly, guiding improvement measures, and enhancing work quality. However, when inspection and supervision became too frequent or overly formal, it required primary healthcare workers to spend a significant amount of time preparing for and participating in inspections, potentially becoming a source of work burden and stress for them, thereby diverting their attention and energy from the core epidemic prevention tasks.
“Sometimes, there are overlapping inspections, with vertical supervision from superiors, as well as inspections between districts, but each expert who comes gives different opinions” (P5).
“There are many inspections. They occur frequently, every few days” (P7).
“During periods of stable epidemic conditions, inspections and supervision might decrease, but when there is a local outbreak, there are inspections every day” (P11).
“Different higher-level units require the completion of reports, but some of the content is repetitive, resulting in redundant efforts by personnel to fill out forms” (P13).
Grassroots epidemic prevention work was a systematic project, relying on the close collaboration and joint efforts of various parties such as primary-level medical institutions, community neighborhood committees, and public security departments. However, in the actual operation process, issues in horizontal collaboration, such as low levels of coordination among members, could become factors hindering the smooth progress of epidemic prevention work. In epidemic prevention, a swift and unified response was key to controlling the spread of the epidemic. If there was a lack of efficient coordination and communication among the three-person team members, it would be difficult to achieve rapid response and unified action.
“Some police officers are unwilling to cooperate in conducting door-to-door tasks. When encountering residents unwilling to cooperate with transportation, some police officers also refuse to assist” (P2).
“The responsibilities of the three-person teams are not effectively implemented. Many tasks that could be completed by community committees and police officers are instead assigned to community health workers” (P3).
“Without support from police officers, the three-person teams often face resistance and lack of cooperation from residents during door-to-door checks and sampling” (P10).
“Community health workers are burdened with too many responsibilities within the three-person teams” (P14).
The core of grassroots epidemic prevention work lay in the extensive participation and active cooperation of residents within the jurisdiction, as their understanding and cooperation were key to implementing effective epidemic prevention measures. However, in actual work, primary healthcare workers sometimes encountered residents who did not understand or cooperate, which not only increased the difficulty of epidemic prevention work but could also have a negative impact on the effectiveness of prevention. A lack of understanding from residents could lead to the obstruction of the dissemination of epidemic prevention information. If residents lacked awareness of the necessity and urgency of epidemic prevention measures, they might not take epidemic prevention guidance and advice seriously, thereby affecting the implementation of these measures. Faced with uncooperative residents, primary healthcare workers needed to spend more time and energy explaining, persuading, and educating these residents.
“The majority of residents are cooperative, but there are still a few who are not cooperative” (P1).
“Most residents are not rejecting, but there are indeed some cases where they refuse to cooperate. Sometimes, even when we are prepared, residents refuse to come out of their homes to cooperate” (P2).
“Conducting screenings is extremely difficult. Some residents may even lodge complaints” (P10).
“There are some who are unwilling to receive vaccinations” (P12).
In this study, interviewees indicated that insufficient personnel is a critical factor affecting the implementation of epidemic prevention work and is the fundamental reason for the unreasonable scheduling of work and rest time. Furthermore, an imbalance in personnel structure, with shortages of certain specialized personnel, necessitates the substitution of other professionals, making it difficult to carry out their primary duties. Previous studies have found that some regions still face issues of imbalanced development, unreasonable allocation, and low quality of primary healthcare human resources (21, 22). Following the outbreak of the epidemic, the proportion of grassroots public health professionals in Tongzhou District, Beijing, decreased, reflecting the loss and insufficient introduction of grassroots public health talents in the region, which has been the trend in healthcare talent development in the area over the past decade (22). Whether before or after the epidemic, in urban or rural areas, the shortage of grassroots public health talent remains a prominent issue contributing to the imbalance in the structure of healthcare personnel (23–25). Additionally, epidemic prevention work required collaboration among multiple individuals, and when personnel capabilities did not align with the nature of the work, the efficiency of epidemic prevention work was significantly affected. Inadequate infectious disease prevention and control capabilities had already been present in some primary healthcare institutions, and with the increase in COVID-19 prevention and control efforts and the development and utilization of new healthcare systems, further inadequacies in the professional competence and training of primary healthcare personnel were exposed.
At the beginning of the COVID-19 pandemic, the shortage of primary healthcare supplies was the primary problem. As the problem of insufficient material allocation was gradually alleviated, the importance of material management issues gradually came to the fore. Ensuring that grassroots emergency supplies can be rapidly deployed and utilized is the key to improving the management level of public health emergency supplies stockpile, and is also an important guarantee to enhance the ability of grassroots to respond to public health emergencies (26). In the process of fighting the COVID-19 epidemic, the imperfections of the grassroots emergency material reserve system and the low level of material management informatization were exposed due to the suddenness and urgency of the task. Many primary healthcare institutions still used the traditional warehouse management method, and the inventory and registration of materials rely on manual operation, which not only consumed manpower, but also affected the accuracy and efficiency of management (27). Due to the lack of an effective monitoring mechanism, materials might not have been replenished in a timely manner when they were out of stock, or might have been requisitioned without being put into storage in a timely manner, which affected the operational efficiency of the organization and the efficiency of access to materials (28).
In the early stages of the COVID-19 outbreak, the Central Leading Group for COVID-19 Response issued the “Notice on Fully Implementing Measures to Further Protect, Care for, and Support Medical Personnel,” which explicitly outlined specific requirements such as “localities must issue temporary work subsidies to medical personnel involved in epidemic prevention and control, increase the total amount of one-time performance pay, and implement healthcare and epidemic prevention allowances for healthcare personnel” (29). Due to the delayed nature of subsidies, it was possible that certain regions faced constraints due to economic development or institutional financial conditions, resulting in the delayed distribution of subsidies. The epidemic prevention subsidy policy directly impacts the interests of each prevention and control worker and plays a significant motivating role. If compensation subsidies do not accurately reflect the labor value of individuals, it can significantly impact the job satisfaction and motivation of healthcare personnel (30).
During the COVID-19 pandemic, government departments at all levels responded swiftly, adopting a top-down task assignment model for epidemic prevention and control to ensure the mandatory distribution and implementation of epidemic prevention tasks. This model played a crucial role in rapidly mobilizing resources and manpower. However, due to the suddenness and novelty of the outbreak, even senior leaders may have faced challenges due to lack of experience, which to some extent led to deficiencies and vulnerabilities in management. Amidst the rapid development of the epidemic and the continuous changes in policies, guidance for grassroots epidemic prevention work might become unclear, and the division of responsibilities might become ambiguous, leading to inconsistencies between actual execution and higher-level policies. Primary healthcare workers sometimes did not clearly understand their specific tasks, and community residents were uncertain whom to turn to for questions about epidemic prevention measures. Moreover, due to the lack of targeted measures, the top-down task assignment sometimes tended to adopt a “one-size-fits-all” or “increasingly stringent” approach, which not only restricted the effectiveness of grassroots prevention work but also increased the burden on Primary healthcare workers and the inconvenience to the public (31). The frequency of higher-level inspections was partly due to a close watch on the implementation of prevention and control measures, as well as a high level of concern for the development of the epidemic. However, if there was a lack of effective communication between higher authorities, it might have led to repetitive or excessive inspections, which not only consumed grassroots resources and energy but might also interfere with normal epidemic prevention work. Phenomena of bureaucracy and formalism, such as turning “information reporting” into a formalized process, failed to truly serve the purpose of prevention and control, instead adding to the burden on the grassroots level (32). Under the influence of the trace management philosophy, there might have been a tendency in the epidemic prevention process to focus more on evidence than actual effectiveness. This led primary healthcare workers to spend a lot of time preparing for inspections and leaving records, which in turn affected their focus on the prevention and control work itself. Such a tendency might have caused grassroots epidemic prevention personnel to work for the sake of coping with inspections, rather than for the actual effect of prevention and control, which contradicted the original intention of the inspections and supervision (33).
From the interviews, it can be observed that there were other issues affecting the implementation of grassroots epidemic prevention work, such as inadequate coordination among the three-person teams and insufficient cooperation from residents. However, it was noted in the interviews that only a small number of police officers or community workers failed to fulfill their responsibilities, thereby reducing the effectiveness of grassroots epidemic prevention work. Additionally, the majority of residents understood and cooperated with the epidemic prevention efforts, with only a few residents showing resistance. While these situations were difficult to completely avoid, efforts can be made to enhance publicity, change perceptions, and increase cooperation.
While the occurrence of epidemics remains unpredictable, it is crucial to promptly assess current issues in epidemic prevention efforts and address them proactively to glean valuable insights for effectively managing potential future epidemics. The emergence of the COVID-19 pandemic has underscored the pivotal role of grassroots efforts in epidemic prevention and control, particularly within a well-functioning grassroots public health system. Therefore, enhancing the workforce at the grassroots level, particularly through robust training and recruitment of public health professionals, is essential. Establishing corresponding human resource allocation plans and coordinating work reasonably will ensure a more balanced distribution of talent. It is crucial to implement proper rotation management for staff, ensuring an adequate pool of backup personnel for different positions to prevent prolonged work periods for primary healthcare workers during times of heightened epidemic activity. Timely training for new recruits should focus on enhancing medical skills and standardizing learning processes, with an emphasis on emergency response and epidemic data management training for grassroots personnel, while reducing non-medical skills training that may be less relevant (34).
Strengthen the establishment of emergency material management systems, assign dedicated personnel to manage materials, and ensure that materials are properly categorized, accessed according to regulations, and managed effectively. Provide regular training for material management staff to enhance their operational capabilities and professional qualities, ensuring proficiency in material management knowledge and skills. Define the responsibilities of material management personnel, and intensify supervision and assessment to ensure the regulation and effectiveness of material management. Improve the informatization management of emergency prevention and control materials by establishing an inventory information system for specialized management of material reception, distribution, and storage. Establish standardized protocols for emergency vehicle support, with institutions potentially dedicating specific emergency vehicles or collaborating with local communities to provide such resources. Alternatively, explore partnerships with third-party companies capable of supplying vehicles and drivers as needed.
Establishing a dedicated fund for major epidemic prevention and control efforts can bolster emergency support capabilities. Governments at all levels may allocate a specific portion of their budget expenditures to establish an epidemic prevention special fund, managed in a fund-style manner with surplus funds reserved for future needs. This ensures a stable financial resource for responding to sudden public health emergencies and safeguarding epidemic prevention subsidies for frontline workers (35). Enhancing incentive and support policies is crucial to ensure that all personnel engaged in epidemic prevention and control receive appropriate subsidies. Comprehensive subsidy standards should be developed based on factors such as workload, working hours, job complexity, and risk level during epidemic prevention and control activities. This approach ensures that subsidies are distributed in a reasonable, equitable, and transparent manner based on justified criteria.
Facing the heavy tasks of grassroots epidemic prevention, it is particularly important to ensure that primary healthcare workers receive proper rest and support in a high-pressure working environment. Although they cannot leave their posts at will, institutions should take positive measures to reasonably arrange rest time and, where possible, establish dedicated rest areas to ensure that primary healthcare workers can get enough rest and a comfortable resting environment, thus avoiding over-fatigue caused by long working hours (36). To alleviate the pressure of primary healthcare workers’ family life, institutions can optimize and adjust the scheduling system in a timely manner according to the actual situation of the department and the age and family status of the primary healthcare workers. Such flexible arrangements can allow them to reduce worries about family while working and focus more on their work. In addition, career development is a matter of great concern to primary healthcare workers. After the epidemic, relevant departments and units should consider optimizing the promotion channels for primary healthcare workers. Targeted promotion plans can be formulated according to different professions and professional titles, and professional work knowledge and practical experience can be taken as the main content of the review. This will help to reduce the pressure of scientific research topics and papers that primary healthcare workers face in the promotion process (37). With the continuous deepening of medical system reform, the pressure faced by primary healthcare workers is also increasing. Therefore, managers should pay more attention to the humanistic care of primary healthcare workers, provide necessary support and help by listening to their needs and expectations. This kind of care can not only improve the satisfaction of primary healthcare workers with managers, but also effectively improve the overall efficiency and quality of primary healthcare work (33).
To improve this situation, higher-level authorities need to enhance internal communication to avoid unnecessary repetitive inspections while ensuring that inspections are targeted and effective. In addition, processes should be streamlined to reduce the burden of formalism, allowing primary healthcare workers to focus their energy on the implementation and effectiveness of prevention measures. Through these measures, the efficiency and effectiveness of prevention work can be improved, while also reducing the pressure on primary healthcare workers and enhancing the satisfaction and trust of the public.
Our study had several limitations. As with other qualitative studies, the perspectives and beliefs of the research subjects influenced the research process (38). However, the differing viewpoints of the researchers facilitated rigorous debate and data analysis to ensure appropriate generalization and thematic emergence. The sample size was relatively small, but the interview content reached saturation from the responses of the interviewees. This met the qualitative analysis needs of our study. The study was conducted in Guangzhou, and the difficulties in epidemic prevention work in different regions and cities may differ from those reported in Guangzhou. Therefore, caution should be exercised when applying the results of this study to other regions or countries.
Overall, this study found that during the COVID-19 pandemic prevention and control period, primary healthcare workers faced seven main challenges in carrying out epidemic prevention work, namely: manpower allocation, material and vehicle support, epidemic prevention subsidies and compensation, humanitarian care, superior management, horizontal cooperation, and resident cooperation. These issues not only affected the efficiency and quality of epidemic prevention work but also reflected the vulnerability of grassroots medical and health systems in responding to public health emergencies. The study suggests that efforts should focus on enhancing the professional competence of grassroots medical and health personnel, improving material management practices, establishing effective incentive and support mechanisms, enhancing humanitarian care, and optimizing superior management systems. These measures aim to comprehensively enhance the epidemic prevention capabilities and efficiency of grassroots medical and health institutions. They also seek to minimize obstacles and challenges faced by primary healthcare workers in conducting epidemic prevention work, alleviate their workload, and bolster their work motivation.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board of Jinan University (NO.JNUKY-2023-0037). The study team obtained informed consent from all participants. Participants were made aware that they could withdraw at any time.
YJ: Visualization, Writing – review & editing, Writing – original draft, Methodology, Formal analysis, Data curation, Conceptualization. HF: Writing – original draft, Investigation, Formal analysis, Data curation, Conceptualization. QX: Writing – original draft, Investigation, Formal analysis, Data curation, Conceptualization. FT: Writing – original draft, Investigation, Data curation, Conceptualization. HY: Writing – original draft, Investigation, Data curation, Conceptualization. RZ: Writing – original draft, Methodology, Investigation, Data curation. QW: Writing – original draft, Visualization, Investigation, Data curation. HZ: Writing – original draft, Visualization, Investigation, Data curation. WZ: Writing – original draft, Methodology, Investigation. JC: Writing – original draft, Visualization, Investigation. TL: Writing – review & editing, Supervision, Project administration. WM: Writing – review & editing, Supervision, Project administration. XC: Writing – review & editing, Supervision, Project administration. XD: Writing – review & editing, Supervision, Project administration.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Li, X, Wang, W, Zhao, X, Zai, J, Zhao, Q, Li, Y, et al. Transmission dynamics and evolutionary history of 2019-nCoV. J Med Virol. (2020) 92:501–11. doi: 10.1002/jmv.25701
2. Ruixi, S, Junjie, T, and Yuan, Y. Research on the planning of medical facilities at the sub-district level under the requirements of regular epidemic prevention and control: a case study of Guangzhou. South Architect. (2020) 4:1–5. doi: 10.3969/j.issn.1000-0232.2020.04.001
3. Yunjie, R, Ming, Z, and Hongqiong, D. Practice and thinking of operation of the up-down linkage mechanism within the medical treatment combination based on the prevention of COVID-19. Chin J Soc Med. (2021) 38:8–10. doi: 10.3969/j.issn.1673-5625.2021.01.003
4. Liang, WN, Yao, JH, Wu, J, Liu, X, Liu, J, Zhou, L, et al. Experience and thinking on the normalization stage of prevention and control of COVlD-19 in China. Chin Med J. (2021) 101:695–9. doi: 10.3760/cma.j.cn112137-20210104-00008
5. Guozhen, Y, Caiyun, Z, and Dewen, W. Measures of primary health institutions taken in regular epidemic prevention and control. Chinese Rural Health Service Administration. (2021) 41:182–6. doi: 10.3969/j.issn.1005-5916.2021.03.008
6. Xu Zhijie, L, and Yiting, FL. The roles and challenges of primary care practitioners in prevention and control of the outbreak of coronavirus disease 2019. Chin J Gen Pract. (2020) 19:273–6. doi: 10.3760/cma.j.cn114798-20200221-00149
7. Dawei, Y. Research on the construction of community health service system in the post-epidemic era. Northern Forum. (2022) 4:95–102. doi: 10.13761/j.cnki.cn23-1073/c.2022.04.011
8. Yuxuan, Y, Luning, N, Xin, Z, Hui, Y, Wenhui, Z, and Wei, L. Current situation and relationship of lifestyle, work stress and life satisfaction in medical staff under background of normalized epidemic prevention and control. Occup Health. (2023) 39:1496–501. doi: 10.13329/j.cnki.zyyjk.2023.0285
9. Hui, L, Huayi, X, and Yali, C. The ethical challenges faced by disease control and prevention personnel in response to public health emergency based on COVID-19 prevention and control. Med Philos. (2023) 44:11–5. doi: 10.12014/j.issn.1002-0772.2023.02.03
10. Shi, LS, Xu, RH, Xia, Y, Chen, DX, and Wang, D. The impact of COVID-19-related work stress on the mental health of primary healthcare workers: the mediating effects of social support and resilience. Front Psychol. (2022) 12:800183. doi: 10.3389/fpsyg.2021.800183
11. Wang, W, Song, W, Xia, Z, He, Y, Tang, L, Hou, J, et al. Sleep disturbance and psychological profiles of medical staff and non-medical staff during the early outbreak of COVID-19 in Hubei Province, China. Front Psych. (2020) 11:733. doi: 10.3389/fpsyt.2020.00733
12. Guangzhou Municipal Statistics Bureau and Guangzhou Survey Office of National Bureau of Statistics. 2022 Guangzhou statistical yearbook. Beijing: China Statistics Press (2022).
13. Bernard, HR, and Ryan, GW. Analyzing qualitative data: Systematic approaches. Thousand Oaks, CA: Sage (2010).
14. Guest, G, Bunce, A, and Johnson, L. How many interviews are enough? An experiment with data saturation and variability. Field Methods. (2006) 18:59–82. doi: 10.1177/1525822X05279903
15. Tenny, S, Brannan, JM, and Brannan, GD (2022). Qualitative Study. In StatPearls. StatPearls Publishing.
16. Kiger, ME, and Varpio, L. Thematic analysis of qualitative data: AMEE guide no. 131. Med Teach. (2020) 42:846–54. doi: 10.1080/0142159X.2020.1755030
18. Braun, V, and Clarke, V. Using thematic analysis in psychology. Qual Res Psychol. (2006) 3:77–101. doi: 10.1191/1478088706qp063oa
21. Qian, Li. (2015). Research on the demand and distribution status of health professionals and incentives factors in Guizhou primary health system. Master's thesis, Guizhou Medical University.
22. Jiali, S, Chunxin, S, and Haiquan, M. Human resources analysis of emergency prevention and control in primary health care institutions in Tongzhou District before and after the outbreak of COVlD-19. Chin Primary Health Care. (2022) 36:23–5. doi: 10.3969/j.issn.1001-568X.2022.11.0007
23. Yaguang, Z. The construction of rural public health talent team under the perspective of epidemic prevention and control. Chin Talents. (2022) 2:33–5. doi: 10.3969/j.issn.2096-3521.2022.02.017
24. Liangyu, X, Wang Lijie, X, Mingyuan, LF, and Ji, W. Study on reconstruction strategy of primary public health service system in the post-epidemicperiod in Longgang district of Shenzhen city. Chin Commun Doctors. (2021) 37:189–90. doi: 10.3969/j.issn.1007-614x.2021.25.091
25. Kun, H, Tianxing, W, Wenyu, J, and Min, Z. Analysis on the public health human resource allocation in community health service centers of Hongkou District, Shanghai. Chin Primary Health Care. (2019) 33:17–20. doi: 10.3969/j.issn.1001-568X.2019.08.0006
26. Yan'e, Z, Xiaqin, L, and Ting, L. Research on countermeasures for the Management of Emergency Materials Reserve in primary-level public health. China Chief Financial Officer. 222:180–3. doi: 10.3969/j.issn.1672-576X.2022.01.061
27. Yanling, Y, Bing, X, Junbo, L, Genge, W, and Weibiao, H. Practice and discussion on Management of Materials for emergency public health events. Hosp Manag Forum. (2021) 38:91-92+83. doi: 10.3969/j.issn.1671-9069.2021.02.026
28. Xiuqin, L, Mingjie, Z, and Guoliang, X. Current status and optimization suggestions for the Management of non-medical Materials in hospitals. J Tradit Chin Med. (2022) 30:80–2. doi: 10.16690/j.cnki.1007-9203.2022.22.068
29. Cheng, W, Longmei, H, and Wenhua, B. Improving remuneration of medical staff in the fight against COVlD-19. China Manag Account Rev. (2021) 17:29–36.
30. Jiangmei, Q. The reform of remuneration should "Lead" the overall system construction. China Health. (2018) 3:38–9. doi: 10.15973/j.cnki.cn11-3708/d.2018.03.019
31. Pei, Zhang. (2022). Research on local government responsibility avoidance behaviorin the prevention and control of the new crown epidemic- based on multi-case analysis. Master's thesis, Northeast Normal University. doi: 10.27011/d.cnki.gdbsu.2022.000426
32. Zhang, H, Hanlei, S, and Lun, X. Construction of epidemic prevention and control capacity based on the perspective of big data. Acta Mathematic Applicatae Sinica. (2020) 43:468–81.
33. Lan, G. Nursing managers in primary-level hospitals should pay attention to the humanistic Care of Nursing Staff. China Rural Health. (2019) 11:61+63. doi: 10.3969/j.issn.1674-361X.2019.02.062
34. Qiong, W, Ping, J, Wei, P, Peiyan, Z, and Xing, Z. Practice and exploration of comprehensive ability training for primary health personnel in Changning District. Chinese Primary Health Care. (2024) 38:37–9. doi: 10.3969/j.issn.1001-568X.2001.11.023
35. Wenhao, W. Exploration on long-term mechanism of public health emergencies prevention and control in rural community-review and reflection based on COVlD-19. J Beijing Vocat College Agric. (2021) 35:68–73. doi: 10.3969/j.issn.1671-7252.2021.03.011
36. Yan, X, and Hongchun, L. Discussion on the path of humanistic Care for Medical Staff-Taking the position of infectious disease work in the post-COVID-19 era as an example. Chin Med Human. (2023) 9:15–8. doi: 10.3969/j.issn.2095-9753.2023.04.006
37. Guiqin, W, and Shaofan, F. Construction of hospital humanistic care system under normalized prevention and control of COVID-19. Modern Hospitals. (2022) 22:1188–90. doi: 10.3969/j.issn.1671-332X.2022.08.012
Keywords: COVID-19, primary healthcare workers, work challenges, qualitative survey, public health emergency management
Citation: Jin Y, Feng H, Xiao Q, Tian F, Yao H, Zhang R, Wu Q, Zhu H, Zheng W, Chen J, Liu T, Ma W, Chen X and Dong X (2024) The work challenges faced by primary healthcare workers in Guangzhou during the COVID-19 pandemic prevention and control period of 2021–2022: a qualitative study. Front. Public Health. 12:1454759. doi: 10.3389/fpubh.2024.1454759
Edited by:
Juan Gómez-Salgado, University of Huelva, SpainReviewed by:
Humaira Sharif, University of Malaya, MalaysiaCopyright © 2024 Jin, Feng, Xiao, Tian, Yao, Zhang, Wu, Zhu, Zheng, Chen, Liu, Ma, Chen and Dong. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiongfei Chen, MTE3NDI1MTNAcXEuY29t; Xiaomei Dong, bnR5ZHhtQDEyNi5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.