 Change Zhu1,2†
Change Zhu1,2† Christine A. Walsh
Christine A. Walsh- 1School of Health Economics and Management, Nanjing University of Chinese Medicine, Nanjing, China
- 2Jiangsu Research Center for Major Health Risk Management and TCM Control Policy, Nanjing University of Chinese Medicine, Nanjing, China
- 3Faculty of Social Work, University of Calgary, Calgary, AB, Canada
Background: This scoping review aims to examine the extant literature and summarize findings related to barriers to accessing health care faced by older Chinese immigrants in Canada.
Methods: We conducted a search of electronic databases for peer-reviewed articles using a comprehensive set of keywords without limiting the search to a specific time period. To be included in our review, articles had to meet the following criteria: (a) published in a peer-reviewed journal, (b) written in English, (c) provide a clear description of the methods used, and (d) respond to our research question, which focuses on identifying barriers to accessing healthcare for older Chinese immigrants living in Canada.
Results: Fifteen papers were selected based on the criteria, and five main barriers were identified, which are ranked in descending order according to the number of times they were mentioned: culture and health beliefs (N = 13), language and communication (N = 7), structural and circumstances (N = 2), health literacy and information (N = 2), and demographic, social, and economic factors (N = 2).
Conclusions: The issue of accessing healthcare for older Chinese immigrants in Canada is complex, as it involves multiple aspects that are relevant to both patients and healthcare providers. Our research findings suggest that the culturally and linguistically sensitive education programs, inter-sectoral coordination, and social support should be improved for older Chinese immigrants and those of other ethnic backgrounds.
1 Introduction
The demographic landscape across the globe has been shaped by a notable trend of international migration (1). Canada, as a popular destination for immigrants (2), has seen a substantial influx, with Statistics Canada (2021) reporting over 8.36 million immigrants by 2021, accounting for 23% of the overall population (3). This growing trend includes a significant number of immigrants primarily from Asia and the Middle East (4).
In urban centers, such as the Toronto Census Metropolitan Area, immigrants not only make up a considerable portion of the general population but are also a substantial part of the older adult demographic. For instance, while immigrants constitute 48% of Toronto's population, they represent 70% of those aged 65 and above (5). This pattern is reflected nationwide where, as of 2015, 30% of Canadians aged 65 or above were immigrants (6), highlighting the growing presence of older adult immigrants in the healthcare system.
Zooming in further, within Canada's visible minority population, Chinese residents form the second largest group, totaling 1.3 million from mainland China, Hong Kong, and Macao (5). Remarkably, 96% of older Chinese individuals (aged 60 and above) in Canada are immigrants (5), reflecting historical immigration patterns (7), family reunification (8), and economic opportunities (9). Given their significant representation, it is crucial to explore the specific healthcare access barriers faced by older Chinese immigrants, as they encounter distinct challenges not solely due to their population size but also due to cultural and linguistic differences. Unlike many other immigrant groups, older Chinese immigrants often face language barriers, unfamiliarity with Western healthcare practices, and traditional health beliefs that may conflict with mainstream medical approaches. These factors create unique barriers in accessing and utilizing healthcare services. Thus, targeted research is needed to better understand and address the specific healthcare needs of this population, ensuring more equitable access within the aging demographic.
The challenges faced by the aging immigrant population are profound and multifaceted (10). They not only grapple with the normal decline in physical functioning but also with acculturative stress, lifestyle changes, and the nuances of Western healthcare systems. These challenges are compounded for older immigrants, who experience more significant health issues compared to their non-immigrant counterparts. For example, older immigrants are more likely to report mental illnesses (11) and show a more pronounced decline in emotional functioning over time compared to non-immigrant older adults (12). This heightened emotional functioning vulnerability can be attributed to factors such as cultural adaptation stress and social isolation, which are less prevalent among non-immigrant older adults (13). As a result, immigrants may experience a sharper decline in emotional functioning over time. Furthermore, long-term immigrants (residing in Canada for over 10 years) also report deteriorating health conditions, indicating a gradual decline in immigrant health status (14, 15).
Despite Canada's publicly funded healthcare system designed to provide equitable access irrespective of age and immigration status, research indicates that older immigrants utilize healthcare services less frequently than younger ones, with data over two decades old still suggesting low utilization among this group (16).
Furthermore, existing studies have identified multiple barriers to healthcare access for older immigrants, including language and communication difficulties (17), transportation issues (18), and financial constraints (19). However, no study has specifically mapped out the barriers faced by older Chinese immigrants in accessing healthcare services in Canada. Although some of these challenges may overlap with those of other immigrant groups, the distinct cultural and linguistic barriers faced by Chinese older adults, coupled with traditional health beliefs, warrant a dedicated scoping review. Understanding these barriers is crucial for guiding future research aimed at improving healthcare access for older adults.
Hence, this scoping review aims to comprehensively examine the existing literature on the barriers older Chinese immigrants face in accessing healthcare services in Canada. Through this analysis, we seek to identify knowledge gaps and suggest directions for future research.
2 Methods
Arksey and O'Malley's five stages of scoping review framework was adopted for this review (20). The framework comprises five stages: identifying the research question, identifying the relevant studies, selecting studies, charting the data, and collating, summarizing, and reporting the results, each of which is described in the following section.
2.1 Stage 1: identifying the research question
To conduct a successful scoping review, it is essential to formulate focused research questions while keeping the investigation inclusive enough to avoid disregarding any valuable literatures (20). The review was guided by the research questions: (1) What original research has been conducted on the barriers to healthcare access faced by older Chinese immigrants in Canada? This served as the primary research question. (2) How can access to healthcare be improved for older Chinese immigrants in Canada? This functioned as the secondary research question.
2.2 Stage 2: identifying relevant studies
Firstly, expert consultation was sought to determine the most appropriate databases for the search. Following the recommendations of the expert, the following eight databases were systematically searched to identify relevant studies for review: Abstracts in Social Gerontology, PubMed, Social Services Abstracts, CINAHL, Social Work Abstracts, Sociological Abstracts, ScienceDirect, and Web of Science. Finally, the EndNote software was employed to organize the gathered literature.
2.3 Stage 3: selecting studies
Our study exclusively considered research studies published in the English language. A total of 5,739 titles and abstracts from various sources, including PubMed (N = 2,958), CINAHL (N = 97), Social Work Abstracts (N = 5), Abstracts in Social Gerontology (N = 37), Social Services Abstracts (N = 1,100), Sociological Abstracts (N = 932), ScienceDirect (N = 331), and Web of Science (N = 279), were obtained during the initial literature search. The systematic identification and removal of duplicate references were conducted using EndNote software. Following the removal of duplicates (N = 518), book section (N = 76), thesis (N = 9), and conference proceedings (N = 2), a thorough review was conducted on the remaining 5,134 titles and abstracts using the established inclusion and exclusion criteria. Then, a two-step screening process was performed by two separate reviewers (ZC and PE). The initial step involved evaluating the titles and abstracts according to specified inclusion and exclusion criteria (see Table 1). To ensure a focused examination, only articles specifically studying older Chinese immigrants were selected for inclusion. Studies involving older individuals from other countries or ethnicities were excluded to maintain the specificity of the research population. This process resulted in the retrieval and evaluation of 39 full-text articles. At this step, 27 articles were excluded from the analysis as they focused on health behavior, health status, or the factors affecting health instead of the barriers to accessing health care. Also, despite the exclusion of related review papers, a manual search was conducted to identify relevant articles included within those reviews. As a result, 3 additional articles were included in the analysis. In total, 15 articles comprised the final sample for further analysis. The papers selected from the first step were then thoroughly reviewed in the second step. Any disagreements between the two reviewers were reconciled through consensus or by seeking a decision from a third reviewer (CW) to determine the final papers to be included. Since no existing guidelines exist for reporting scoping reviews, the flow of articles included in this review was documented using the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (21) (see Figure 1).
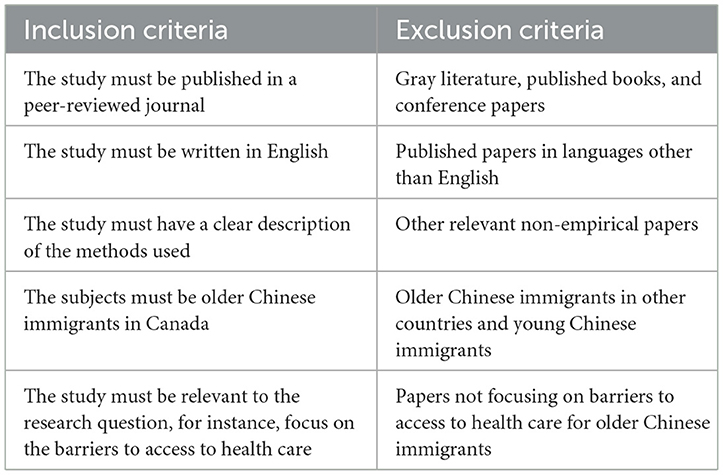
Table 1. Inclusion and exclusion criteria for study selection.
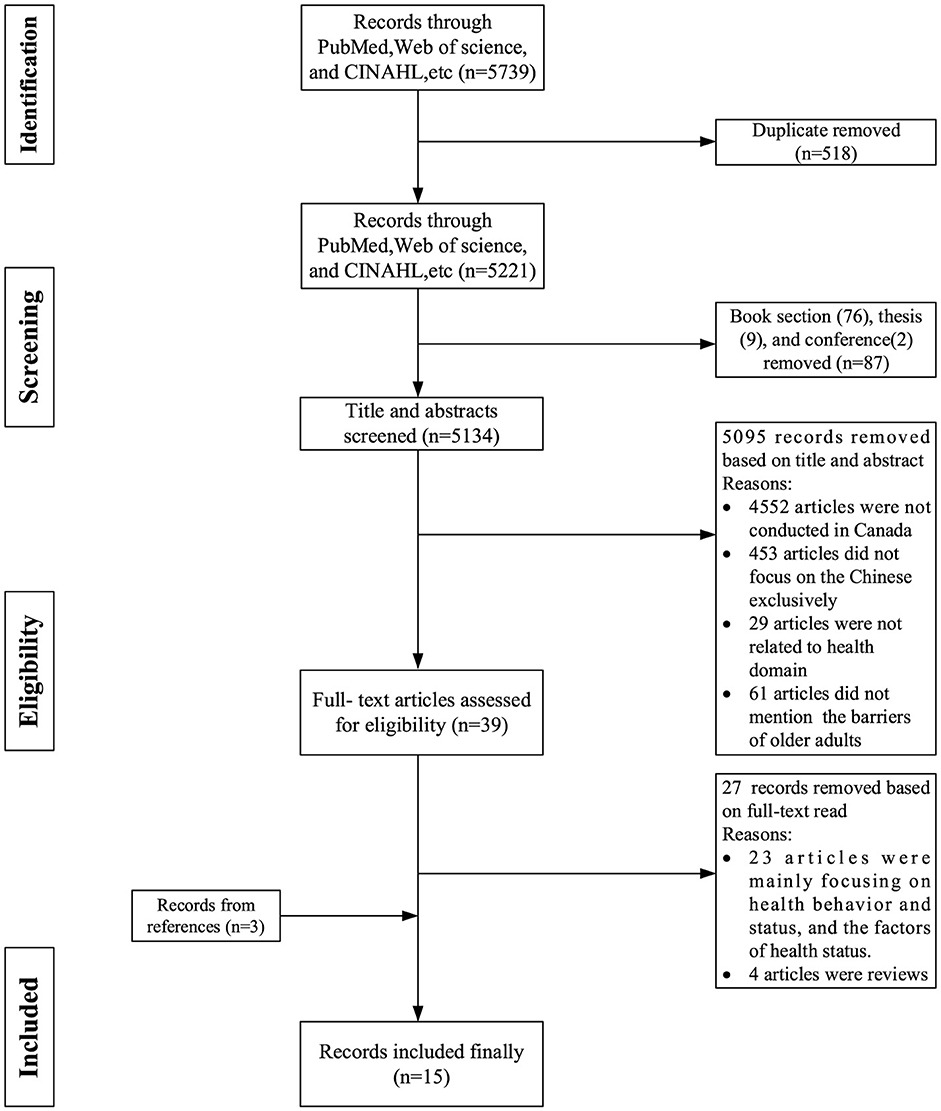
Figure 1. PRISMA flow diagram on the outcomes of the search strategies.
2.4 Stage 4: charting the data
Essential information from the selected articles was collected and organized into a data chart format. This chart included details such as the first author, year of publication, study sites, aims, methods, mentioned barriers and interventions. Two evaluators (ZC and PE) separately evaluated the initial version of the data chart form using five randomly selected papers. Following mutual discussions and feedback, the chart form was modified. The updated chart form was then thoroughly reviewed and accepted by the team (ZC, PE, and CW) and was utilized to gather information from all the studies included in a narrative form.
2.5 Stage 5: collating, summarizing, and reporting the results
The main objective of scoping studies is not to assess the literature's quality but to create a comprehensive overview of existing research or establish a thematic framework that offers a broad understanding of the research conducted in a specific area of inquiry. The data were analyzed using a thematic approach (22). In the data synthesis phase, NVivo software was employed to facilitate the thematic analysis. The imported literature underwent an initial review, with key concepts and themes marked using the software's tagging and annotation features. A preliminary coding framework was established, creating nodes within NVivo to represent different themes or concepts identified in the literature. Systematic coding was then applied to each piece of literature, associating relevant text with the established nodes. Utilizing NVivo's analytical tools, the coded data was synthesized to identify recurring themes across multiple pieces of literature. The coding process underwent validation and cross-checking within NVivo to ensure consistency and accuracy, involving collaborative efforts and discussions among team members. To further guarantee consistency and validate the fifth stage of the process, two reviewers (ZC and PE) each conducted their own independent thematic analysis of the literature. The research team collectively approved the final results after critical evaluations and discussions.
3 Results
3.1 Study characteristics
Out of the 15 studies, most were quantitative (N = 9, 60%); the remainder were qualitative (N = 3, 20%); and mixed-methods (N = 3, 20%), as shown in Tables 2 and 3. Concerning the research location, nine studies were conducted in Ontario, primarily in Toronto; five studies were conducted in Alberta, mainly in Calgary and Edmonton and in addition, six studies were conducted in British Columbia, particularly in Vancouver and Victoria. Further, four studies were conducted throughout Canada without specifying a particular region or city. In addition, Lai, Tieu, and Todd were the primary authors dedicated to research on barriers to accessing health services for older immigrants in Canada. A total of 9 papers were completed by these authors, with Lai, the lead author contributing five papers and Tieu and Todd each leading two papers, respectively. Among the selected papers, 12 out of 15 were conducted a decade ago, while only three papers were conducted within the past 10 years, indicating a dearth of recent studies addressing this particular topic.
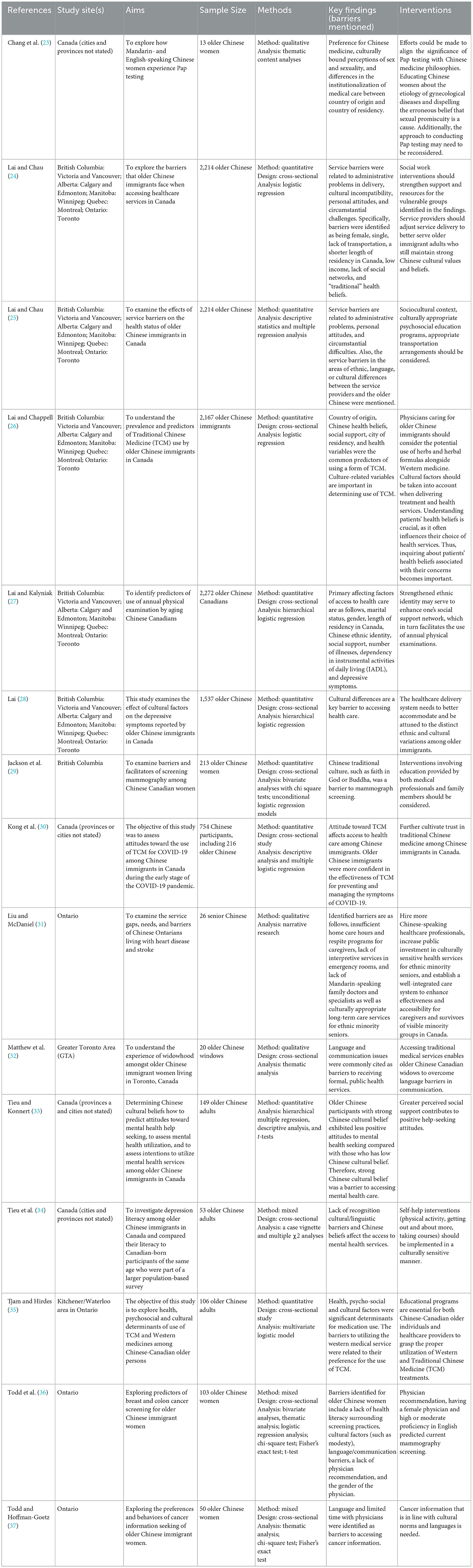
Table 2. Study description and mentioned barriers.
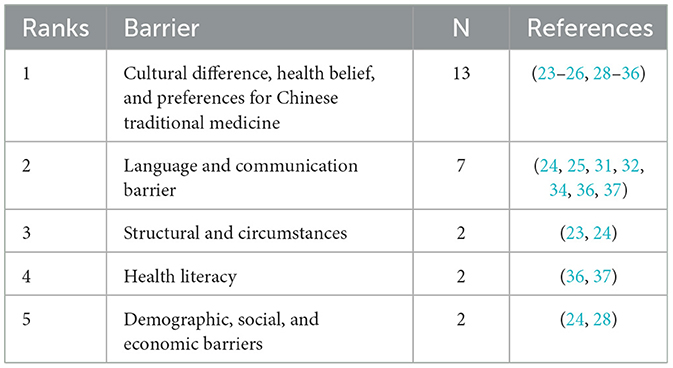
Table 3. Number of studies listing specific barriers to accessing healthcare.
3.2 Thematic categorization of access to healthcare barriers
Accessing healthcare services can be more challenging for older individuals who belong to ethnic minority groups due to the unique barriers they may face. Increasing globalization and migration have led to a growing number of older immigrants facing significant challenges in accessing health care, primarily due to factors such as cultural disparities, language barriers, and unfamiliarity with the local healthcare system (17). This is particularly true for older Chinese immigrants in Canada. We have classified the 15 articles into five main categories based on their focus areas and specific thematic categorization of the barriers to accessing healthcare by older Chinese immigrants in Canada as follows. To provide specific details, among the selected articles, 13 articles addressed barriers associated with cultural differences, health beliefs, and preferences for Chinese traditional medicine. Seven articles focused on language and communication barriers, while 2 articles examined barriers related to structural and circumstantial factors. Also, 2 articles discussed barriers related to health literacy. Lastly, 2 of them discussed barriers related to demographics, social and economic factors.
3.2.1 Theme- I cultural and health beliefs barriers
Culture involves the distinctive ways of thinking and acting that set individuals or groups apart from one another (38). As people participate in social groups and share experiences, culture becomes deeply embedded in their identity, shaping their attitudes and behaviors (39). Their cultural tendencies influence the way people approach their health and make decisions related to healthcare. Thus, healthcare providers must have an understanding of their patient's cultural backgrounds in order to provide optimal care.
Cultural differences have been shown to affect the healthcare access of older Chinese immigrants in Canada (24). Over half of the articles identified cultural differences as a significant factor to access to health care among older Chinese immigrants in Canada (23–26, 28–36). For example, older Chinese immigrants may hold different beliefs and attitudes toward health and health care compared to the Canadian population. Also, immigrants originating from Hong Kong may exhibit distinct cultural values that differ from those of Canadian culture, thus resulting in a higher likelihood of reporting obstacles to accessing services compared to immigrants from other regions (24). Cultural incompatibility resulting from the unique and strong cultural values held by older Chinese immigrants, which differ from the Western perspective, significantly impacts their utilization of healthcare services (24, 25). Moreover, due to the modesty culture and emphasis on privacy in China, Chinese women tend to be conservative in sexual health, such as breast examination, thus exhibiting a shorter continuance of mammography use (36). Even some older Chinese females hold traditional beliefs, such that cancer can be prevented through faith in God or Buddha, thus presenting a low frequency of
mammography (29). Chinese women in Canada generally prefer the compulsory and depersonalized manner in which Pap tests are performed in China, as this can help to reduce the embarrassment associated with undergoing the test (23). Again, Chinese health beliefs and values are associated with mental health help-seeking attitudes among older Chinese immigrants in Canada. Strong adherence to Chinese health culture predicts a lower likelihood of positive attitudes toward seeking healthcare in Canada (33, 34). Hence, it was reported that older Chinese widows in Canada show a preference for services from private TCM practitioners, acupuncturists and herbalists because it is culturally relevant and easily understood (32). In addition, a strong health belief in the effectiveness of traditional Chinese medicine, deeply rooted in the Chinese mindset, has decreased the desire to access Western healthcare services in Canada (30).
3.2.2 Theme-II language and communication barriers
The most common languages of Canadian Chinese immigrants are Mandarin and Cantonese (35). Therefore, a considerable number of Canadian Chinese immigrants may not be able to communicate effectively with doctors in Canada. To be more specific, 7 out of 15 studies mentioned language barriers to access to health care services (24, 25, 31, 32, 34, 36, 37). When seeking healthcare or accessing healthcare information, language fluency is a primary concern (37). A qualitative study by Martin-Mathews et al. reported that widows did not recognize the direction to the clinic and missed the appointment with a doctor as a result of limited English proficiency (32). Chinese older immigrants often also underutilize mental health services due to linguistic barriers (34). Furthermore, limited English proficiency resulted in underutilization of specific health services, such as colon cancer screening (36). Also, language and communication have been identified as significant barriers not only for older Chinese immigrants to access healthcare but also for healthcare providers who may be insensitive or unresponsive to their need (25). For instance, Lai and Chau found that most of the top service barriers were related to language among 2,214 older Chinese individuals, specifically manifested as the physicians not speaking their preferred language (24). Lack of Mandarin-speaking physicians and interpretive services are the main gaps in Canadian healthcare services, which have been shown to hinder older adults with heart disease and stroke access to healthcare (31).
3.2.3 Theme-III structural and circumstances barriers
Besides languages and cultural barriers, structural and circumstances barriers were also found to pose hindrances to seeking healthcare by older Chinese immigrants. Structural and circumstantial barriers are a persistent and comprehensive concept that includes health system patterns, transportation, waiting list, geographical distance, health-related information availability, institutionalization variations, and other related factors. For instance, the absence of transportation was a significant obstacle to obtaining formal health care (24). A cross-sectional study on 2,214 older Chinese immigrants by Lai and Chau study revealed that insufficient transportation was a potential barrier to access to healthcare services (24). Furthermore, they also reported that administrative issues in service delivery, such as excessively long waiting lists, inconvenient office hours, and overly complex procedures, can reduce the motivation to seek health care services (24). A study has noted that older immigrants, in particular, are unwilling to wait for extended periods to access health services (24). Finally, Institutionalization variations in health care between China and Canada were found to be related to health utilization behavior, preference for Chinese institutionalization of medical care predicting a lower prevalence of pap screening (23).
3.2.4 Theme-IV health literacy and information barriers
Health literacy and access to information play crucial roles in enabling immigrants to effectively utilize health services. Previous studies have demonstrated that the lack of health knowledge is a barrier for immigrants to access and utilize health services (40, 41). Furthermore, improved health literacy among immigrants has been shown to substantially enhance their utilization of primary healthcare services. For instance, older Chinese women in Canada with greater health literacy are more likely to participate in breast and colon cancer screenings compared to those with lesser knowledge (36). Additionally, research indicates that lower health literacy among older Chinese immigrant women, particularly those who are English as a Second Language (ESL) speakers, often results in a preference for interpersonal sources of health information, such as consultations with doctors or discussions with family members, over written materials. This reliance on interpersonal sources, while beneficial, may limit their exposure to comprehensive health information and reduce their engagement in preventive health behaviors, such as cancer screening (37). These insights emphasize the importance of targeted educational interventions to increase health literacy and facilitate better access to healthcare among immigrant populations.
3.2.5 Theme-V demographic, social, and economic barriers
When studying barriers to healthcare utilization among older Chinese immigrants in Canada, Lai identified several barriers, which are as follows: female gender, being single, being an immigrant from Hong Kong, and shorter length of residency in Canada (28). To be more specific, the studies reported that gender exerts an effect on healthcare access as being female, to some extent, is a barrier to accessing the health care (24). Also, being single decreased the probability of utilization of health care (24). Furthermore, Lai and Chau (25) mentioned that discrimination based on ethnicity and age is likely the cause of the issues faced by older Chinese immigrants when trying to access healthcare services (24).
4 Discussion
4.1 Discussion on five primary barriers
Based on the thematic analysis conducted above, five primary barriers to accessing healthcare services among older Chinese immigrants in Canada have been identified, as shown in Table 3. These barriers include cultural differences, language and communication, structural and circumstantial factors, health literacy and information, as well as demographic, social, and economic status. Consequently, it is imperative to delve deeper into these barriers and engage in further discussions.
4.1.1 Culture difference
Cultural barriers were discovered to be particularly noteworthy among the five types of barriers identified in this study. The challenge of limited cultural competency hindering access to healthcare is not unique to Canada. Other countries with high immigration rates, such as Australia and the United States, are also facing similar predicaments (42, 43). Therefore, it is imperative to pay attention to cultural variation between different ethnicities, as depicted in the Chinese and Canadian context found in this research. Given the diverse array of cultures represented in Canada, healthcare professionals must possess a decent comprehension of the subtleties associated with their patients' cultures in order to deliver culturally sensitive care. As a previous study indicated, Canadian physicians must receive culturally appropriate medical education (44). To be more specific, it would be beneficial to incorporate appropriate cultural competency training into the curricula of medical education programs (45). The training should consider the challenges immigrants face in Canada when seeking healthcare. Cultural programs should be tailored to older Chinese clients. This measure can increase physicians' understanding of this matter and improve their preparedness to deliver care.
4.1.2 Language and communication
Among all the obstacles to healthcare for this population, communication difficulties have been extensively researched (46). Language and communication have been identified as significant barriers not only for older Chinese immigrants to access healthcare but also for healthcare providers (25). It was noted that healthcare providers may experience frustration when they are unable to comprehend their patients' requirements or concerns (47). Some healthcare facilities utilize professional translators to address language barriers, but healthcare providers may feel uncomfortable communicating through an interpreter due to uncertainty about the interpreter's appropriate role and the need for confidentiality (48). As is well known, communicating through a translator or other support person, who lacks proficiency in medical terminology, can be challenging in accurately conveying a patient's feelings to a physician (49). Usually, interpreters are instructed not to express their opinions or add their personal comments, which means that they should refrain from providing extensive “cultural interpretation” and instead leave this task to the patient and physician. Physicians then face the challenge of comprehending the diverse cultures of the patients they treat in their aim to deliver “culturally competent” care (50). Additionally, most provincial health policies do not typically cover professional translator services, leading to significant variation in availability throughout Canada (51). Although governments and healthcare service providers have attempted to address barriers to immigrant healthcare by providing brochures or pamphlets printed in different languages, relying solely on printed material may not be sufficient to make a significant impact.
4.1.3 Structural and circumstances
The circumstantial obstacles were barriers associated with insufficient transportation, unfavorable weather conditions for travel, excessively lengthy waitlists, inconvenient office hours, and complex procedures. The above barriers severely hinder the desire to utilize health care for older immigrants. It is well acknowledged that many older adults are unable to navigate public transit (32). Therefore, lack of transportation will lead to less mobility (52), a commonly reported barrier to accessing service (53). Due to financial constraints, older immigrants often have to work multiple jobs, making their time particularly limited (51). Therefore, they are afraid to wait for extended periods to access healthcare services (54).
4.1.4 Health literacy
As depicted above, the low rates of healthcare utilization among older Chinese immigrants might be attributed not only to their limited awareness of healthcare coverage and service availability but also to their insufficient comprehension of the significance and advantages of receiving health examinations (27). Ballantyne et al. found that older immigrants from China often avoided discussing their self-care and alternative healthcare practices with their physicians in their research on medication usage among a diverse group of older immigrants (55). It can be inferred that older Chinese immigrants lack awareness of health promotion and have low health literacy. Also, health literacy is significant for access to healthcare services, given the complexity of the health system and information (56). Therefore, diminishing the lack of health knowledge as a crucial barrier among immigrants could be achieved by enhancing their comprehension of the Canadian healthcare system through public sensitization programs.
4.1.5 Demographic, social, and economic status
We also discovered that the socioeconomic status of older immigrants poses a hindrance to access to healthcare. Upon their arrival in Canada, older immigrants frequently encounter financial difficulties that result from limited employment prospects (57), given that they are mostly retired or generally beyond the typical age of retirement in Canada (32). Also, older immigrants with low socioeconomic status or those who have recently immigrated are especially at a disadvantage as they are frequently excluded from the Canadian pension system due to their limited duration of employment in Canada (58). The Healthcare Act of Canada, enacted in 1984, stipulates that all individuals in Canada, regardless of their immigrant status, are entitled to equal access to healthcare services (59). Although healthcare is accessible to everyone in Canada, immigrants often prioritize working multiple jobs to support their families or accept low-paying positions over seeking healthcare, even when they are unwell (51). In addition, the lack of health insurance is another significant barrier older Chinese immigrants face in accessing health care, such as optometry, dentistry, and therapies, which are considered to be extended health care and not covered by public health insurance (17).
4.2 Policy and implications
From the scoping review on barriers to healthcare access for older Chinese immigrants in Canada, five key obstacles were identified: cultural and health beliefs, language and communication, structural circumstances, health literacy and information, and demographic, social, and economic barriers. To address these challenges, recommendations for policy, practice, and research were put forward.
In terms of cultural and health beliefs barriers, healthcare providers should align their practices with traditional Chinese medicine (TCM) philosophies. For example, integrating TCM perspectives with western medical practices, such as reconsidering the approach to pap testing, can help bridge the cultural gap. Educating healthcare professionals on Chinese health beliefs and providing culturally sensitive care are essential steps. The establishment of multicultural healthcare teams that integrate TCM alongside western medicine will enhance the trust of older Chinese immigrants in the healthcare system. Physicians should also consider using TCM-based treatments alongside western interventions, especially in areas like herbal formulas, to respect patient preferences. Additionally, providing accessible cancer information in line with Chinese cultural norms will further enhance healthcare literacy and trust in preventive care services, as cancer prevention and treatment beliefs are often deeply tied to cultural perspectives. For language and communication barriers, language barriers can be mitigated by hiring more mandarin-speaking healthcare professionals and offering language training to current staff. The availability of multilingual healthcare materials is crucial for ensuring that older Chinese immigrants can understand the healthcare services available to them. Further, healthcare institutions should develop systems that enable clear communication in culturally sensitive ways, such as providing interpreter services in emergency rooms. These efforts will help overcome communication challenges and ensure that older Chinese immigrants have access to necessary healthcare services. Regarding structural and circumstances barriers (administrative and logistical), such as administrative issues and transportation challenges, they can be alleviated by improving inter-departmental coordination and developing seamless referral systems. Social work interventions should be adjusted to cater to the specific needs of older Chinese immigrants who face logistical challenges like limited access to transportation. Healthcare providers should offer transportation assistance and ensure that medical services are located in easily accessible areas. Furthermore, healthcare delivery systems must be more culturally attuned to address the administrative difficulties faced by older Chinese immigrants, especially those who have recently relocated or lack adequate social support networks. With respect to health literacy and information barriers, health literacy interventions should focus on developing culturally appropriate and easy-to-understand health information materials. Campaigns aimed at raising awareness about health literacy, especially concerning screening practices such as mammography, should be tailored to older Chinese immigrants. These campaigns should highlight the importance of preventive healthcare services and provide clear guidance on how to access them. Physician recommendations for screenings, combined with culturally relevant education programs, will help increase participation in preventive health services. Finally, to address demographic, social, and economic barriers, advocating for social justice policies that ensure equitable access to healthcare services for older Chinese immigrants is crucial. Tailored social services, such as enhancing social support networks and providing psychosocial education programs, are critical to improving access. Specific efforts should be made to support those with limited financial resources, ensuring that healthcare is affordable and accessible. Strengthening ethnic identity and community support networks can also facilitate better healthcare access by promoting annual physical exams and routine health check-ups. Lastly, research should continue to investigate the impact of social and economic inequalities on healthcare access for this vulnerable population, with the goal of informing future policy changes.
However, while some of the articles included in this review were published over 10 years ago, and 3 of them more than 20 years ago, the challenges identified—such as language barriers, cultural differences, and healthcare system navigation—are long-standing issues that may persist today. Further research is needed to assess whether these barriers continue to affect older Chinese immigrants' access to healthcare services and to determine the most appropriate interventions in the current context.
4.3 Strengths and limitations
Compared to studies focusing on the general older immigrants, this was the first scoping review to our knowledge to focus on mapping out and documenting the barriers to accessing health care for older Chinese immigrants in Canada. The identified five main barriers, such as culture and health beliefs, language and communication, health literacy and information, structural circumstances, and demographic, social, and economic, identified in the study give implications to the government to improve the health care system and provides better service to ethnic older immigrants. However, this article was restricted to several limitations. Firstly, some of the articles included in this review were published over 10 years ago, with 3 of them being more than 20 years old. Although the barriers identified remain relevant, the age of some studies may affect the direct applicability of the findings to the current context, highlighting the need for updated research in this area. In addition, our study focused exclusively on barriers to accessing healthcare for older Chinese immigrant Canadians and did not address obstacles faced by other ethnic immigrants or non-immigrants, such as refugees and temporary Chinese residents. Due to differences in the populations examined, the barriers identified in this research may not be universally applicable to all older Chinese immigrant groups.
5 Conclusions
Scoping reviews are particularly beneficial for subjects that have not been thoroughly reviewed previously (20). From the above analysis, our scoping review found that the majority of studies (N = 12) were conducted decades ago, which shows a gap in recent understanding of barriers to healthcare for older Chinese immigrants. Hence, this indicates a new for more recent studies to better understand contemporary challenges and barriers to accessing healthcare by older Chinese immigrants. A total of 15 papers were included and five primary barriers were identified, which are ranked in descending order of importance as follows: culture and health beliefs (N = 13), language and communication (N = 7), structural circumstances (N = 2), health literacy and information (N = 2), and demographic, social and economic (N = 2).
The findings highlight the urgency of addressing these barriers to improve the health and wellbeing of this population. Moving forward, it is crucial to consider the policy, practice, and research implications. Addressing the identified barriers has the potential not only to enhance the health outcomes of older Chinese immigrants but also to contribute significantly to reducing healthcare disparities and costs in the long run.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding authors.
Author contributions
CZ: Writing – original draft, Writing – review & editing. BS: Writing – review & editing. CW: Writing – review & editing. PE: Writing – review & editing. XQ: Writing – review & editing. AX: Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Donner W, Rodríguez H. Population composition, migration and inequality: the influence of demographic changes on disaster risk and vulnerability. Soc Forces. (2008) 87:1089–114. doi: 10.1353/sof.0.0141
2. Reitz JG. The distinctiveness of Canadian immigration experience. Patt Prejudice. (2012) 46:518–38. doi: 10.1080/0031322X.2012.718168
3. Canada Statistics. Immigration and ethnocultural diversity statistics. (2021). Available at: https://www.statcan.gc.ca/en/subjects-start/immigration_and_ethnocultural_diversity (accessed June 26, 2024).
4. Canada Statistics. Guide to the Census of Population. (2016). Available at: https://www150.statcan.gc.ca/n1/en/catalogue/98-304-X (accessed June 26, 2024).
5. Canada Statistics. NHS Profile. (2011). Available at: https://www12.statcan.gc.ca/nhs-enm/2011/dp-pd/prof/index.cfm?Lang=E (accessed June 26, 2024).
6. de Jong Gierveld J, Van der Pas S, Keating N. Loneliness of older immigrant groups in Canada: effects of ethnic-cultural background. J Cross Cult Gerontol. (2015) 30:251–68. doi: 10.1007/s10823-015-9265-x
7. Li P S. The rise and fall of Chinese Immigration to Canada: newcomers from Hong Kong Special Administrative Region of China1 and Mainland China, 1980–20002. Int Migr. (2005) 43:9–34. doi: 10.1111/j.1468-2435.2005.00324.x
8. Man G, Chou E. Transnational familial strategies, social reproduction, and migration: Chinese immigrant women professionals in Canada. J Family Stud. (2020) 26:345–61. doi: 10.1080/13229400.2017.1402805
9. Kobayashi A, Preston V. Transnationalism through the life course: Hong Kong immigrants in Canada. Asia Pac Viewp. (2007) 48:151–67. doi: 10.1111/j.1467-8373.2007.00338.x
10. Wu Z, Penning MJ, Schimmele CM. Immigrant status and unmet health care needs. Canadian J Public Health. (2005) 96:369–73. doi: 10.1007/BF03404035
11. Rudner A. What are the data telling us about immigrant seniors' health? In: National Metropolis Conference “Immigration: Bringing the World to Canada,” Vancouver, BC (2011).
12. De Maio FG, Kemp E. The deterioration of health status among immigrants to Canada. Glob Public Health. (2010) 5:462–78. doi: 10.1080/17441690902942480
13. Wu Z, Penning M. Immigration and loneliness in later life. Ageing Soc. (2015) 35:64–95. doi: 10.1017/S0144686X13000470
14. Dunn JR, Dyck I. Social determinants of health in Canada's immigrant population: results from the National Population Health Survey. Soc Sci Med. (2000) 51:1573–93. doi: 10.1016/S0277-9536(00)00053-8
15. Laroche M. Health status and health services utilization of Canada's immigrant and non-immigrant populations. Canadian Public Policy. (2000) 26:51–75. doi: 10.2307/3552256
16. Hislop TG, Teh C, Lai A, Labo T, Taylor VM. Cervical cancer screening in BC Chinese women. B C Med J. (2000) 42:456–60.
17. Wang L, Guruge S, Montana G. Older immigrants' access to primary health care in Canada: a scoping review. Canadian J Aging. (2019) 38:193–209. doi: 10.1017/S0714980818000648
18. MacEntee MI, Mariño R, Wong S, Kiyak A, Minichiello V, Chi I, et al. Discussions on oral health care among elderly Chinese immigrants in Melbourne and Vancouver. Gerodontology. (2012) 29:e822–32. doi: 10.1111/j.1741-2358.2011.00568.x
19. Guruge S, Birpreet B, Samuels-Dennis JA. Health status and health determinants of older immigrant women in Canada: a scoping review. J Aging Res. (2015) 2015:393761. doi: 10.1155/2015/393761
20. Arksey H, O'Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. (2005) 8:19–32. doi: 10.1080/1364557032000119616
21. Parums D V. Review articles, systematic reviews, meta-analysis, and the updated preferred reporting items for systematic reviews and meta-analyses (PRISMA) 2020 guidelines. Med Sci Monit Int Med J Exp Clin Res. (2021) 27:e934475–934471. doi: 10.12659/MSM.934475
22. Hsieh H, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. (2005) 15:1277–88. doi: 10.1177/1049732305276687
23. Chang SC, Woo JS, Yau V, Gorzalka BB, Brotto LA. Cervical cancer screening and chinese women: insights from focus groups. Front Psychol. (2013) 4:48. doi: 10.3389/fpsyg.2013.00048
24. Lai DWL, Chau SBY. Predictors of health service barriers for older Chinese immigrants in Canada. Health Soc Work. (2007) 32:57–65. doi: 10.1093/hsw/32.1.57
25. Lai DWL, Chau SBY. Effects of service barriers on health status of older Chinese immigrants in Canada. Soc Work. (2007) 52:261–9. doi: 10.1093/sw/52.3.261
26. Lai D, Chappell N. Use of traditional Chinese medicine by older Chinese immigrants in Canada. Fam Pract. (2007) 24:56–64. doi: 10.1093/fampra/cml058
27. Lai DWL, Kalyniak S. Use of annual physical examinations by aging Chinese Canadians. J Aging Health. (2005) 17:573–91. doi: 10.1177/0898264305279778
28. Lai DWL. Impact of culture on depressive symptoms of elderly Chinese immigrants. Canadian J Psychiat. (2004) 49:820–7. doi: 10.1177/070674370404901205
29. Jackson SL, Hislop TG, Teh C, Yasui Y, Tu SP, Kuniyuki A, et al. Screening mammography among Chinese Canadian women. Canadian J Public Health. (2003) 94:275–80. doi: 10.1007/BF03403605
30. Kong Y, Shaver LG, Shi F, Yang L, Zhang W, Wei X, et al. Attitudes of Chinese immigrants in Canada towards the use of Traditional Chinese Medicine for prevention and management of COVID-19: a cross-sectional survey during the early stages of the pandemic. BMJ Open. (2021) 11:e051499. doi: 10.1136/bmjopen-2021-051499
31. Liu LW, McDaniel SA. Family caregiving for immigrant seniors living with heart disease and stroke: Chinese Canadian perspective. Health Care Women Int. (2015) 36:1327–45. doi: 10.1080/07399332.2015.1038346
32. Martin-Matthews A, Tong CE, Rosenthal CJ, McDonald L. Ethno-cultural diversity in the experience of widowhood in later life: Chinese widows in Canada. J Aging Stud. (2013) 27:507–18. doi: 10.1016/j.jaging.2012.12.011
33. Tieu Y, Konnert CA. Mental health help-seeking attitudes, utilization, and intentions among older Chinese immigrants in Canada. Aging Ment Health. (2014) 18:140–7. doi: 10.1080/13607863.2013.814104
34. Tieu Y, Konnert C, Wang J. Depression literacy among older Chinese immigrants in Canada: a comparison with a population-based survey. Int Psychogeriatr. (2010) 22:1318–26. doi: 10.1017/S1041610210001511
35. Tjam EY, Hirdes JP. Health, psycho-social and cultural determinants of medication use by Chinese-Canadian older persons. Canad J Aging. (2002) 21:63–73. doi: 10.1017/S0714980800000647
36. Todd L, Harvey E, Hoffman-Goetz L. Predicting breast and colon cancer screening among English-as-a-second-language older Chinese immigrant women to Canada. J Cancer Educ. (2011) 26:161–9. doi: 10.1007/s13187-010-0141-7
37. Todd L, Hoffman-Goetz L, A. qualitative study of cancer information seeking among English-as-a-second-Language older Chinese immigrant women to Canada: sources, barriers, and strategies. J Cancer Educ. (2011) 26:333–40. doi: 10.1007/s13187-010-0174-y
38. Hofstede G. Culture and organizations. Int Stud Manag Organiz. (1980) 10:15–41. doi: 10.1080/00208825.1980.11656300
39. Parrish P, Linder-VanBerschot J. Cultural dimensions of learning: addressing the challenges of multicultural instruction. Int Rev Res Open Distr Lear. (2010) 11:1–19. doi: 10.19173/irrodl.v11i2.809
40. Amankwah E, Ngwakongnwi E, Quan H. Why many visible minority women in Canada do not participate in cervical cancer screening. Ethn Health. (2009) 14:337–49. doi: 10.1080/13557850802699122
41. Leduc N, Proulx M. Patterns of health services utilization by recent immigrants. J Immigr Health. (2004) 6:15–27. doi: 10.1023/B:JOIH.0000014639.49245.cc
42. Derose KP, Escarce JJ, Lurie N. Immigrants and health care: sources of vulnerability. Health Aff. (2007) 26:1258–68. doi: 10.1377/hlthaff.26.5.1258
43. Murray SB, Skull SA. Hurdles to health: immigrant and refugee health care in Australia. Austr Health Rev. (2005) 29:25–9. doi: 10.1071/AH050025
44. Chugh U, Dillmann E, Kurtz SM, Lockyer J, Parboosingh J. Multicultural issues in medical curriculum: implications for Canadian physicians. Med Teach. (1993) 15:83–91. doi: 10.3109/01421599309029015
45. Eshleman J, Davidhizar RE. Strategies for developing cultural competency in an RN-BSN program. J Transc Nurs. (2006) 17:179–83. doi: 10.1177/1043659605285416
46. Fiscella K, Franks P, Doescher MP, Saver BG. Disparities in health care by race, ethnicity, and language among the insured: findings from a national sample. Med Care. (2002) 40:52–9. doi: 10.1097/00005650-200201000-00007
47. Ng C, Newbold KB. Health care providers' perspectives on the provision of prenatal care to immigrants. Cult Health Sex. (2011) 13:561–74. doi: 10.1080/13691058.2011.555927
48. Blake C. Ethical considerations in working with culturally diverse populations: the essential role of professional interpreters. Bull Can Psychiatric Assoc. (2003) 34:21–3.
49. Papic O, Malak Z, Rosenberg E. Survey of family physicians' perspectives on management of immigrant patients: attitudes, barriers, strategies, and training needs. Patient Educ Couns. (2012) 86:205–9. doi: 10.1016/j.pec.2011.05.015
50. Geiger HJ. Racial stereotyping and medicine: the need for cultural competence. CMAJ. (2001) 164:1699–700.
51. Ahmed S, Shommu NS, Rumana N, Barron GRS, Wicklum S, Turin TC. Barriers to access of primary healthcare by immigrant populations in Canada: a literature review. J Immigr Minor Health. (2016) 18:1522–40. doi: 10.1007/s10903-015-0276-z
52. Ip D, Lui CW, Chui WH. Veiled entrapment: a study of social isolation of older Chinese migrants in Brisbane, Queensland. Ageing Soc. (2007) 27:719–38. doi: 10.1017/S0144686X07006083
53. Teng L, Robertson Blackmore E, Stewart DE. Healthcare worker's perceptions of barriers to care by immigrant women with postpartum depression: an exploratory qualitative study. Arch Women's Mental Health. (2007) 10:93–101. doi: 10.1007/s00737-007-0176-x
54. Brar S, Tang S, Drummond N, Palacios-Derflingher L, Clark V, John M, et al. Perinatal care for South Asian immigrant women and women born in Canada: telephone survey of users. J Obstetr Gynaecol Canada. (2009) 31:708–16. doi: 10.1016/S1701-2163(16)34274-8
55. Ballantyne PJ, Mirza RM, Austin Z, Boon HS, Fisher JE. Becoming old as a ‘pharmaceutical person': negotiation of health and medicines among ethnoculturally diverse older adults. Canadian J Aging. (2011) 30:169–84. doi: 10.1017/S0714980811000110
56. Gulati S, Watt L, Shaw N, Sung L, Poureslami IM, Klaassen R, et al. Communication and language challenges experienced by Chinese and South Asian immigrant parents of children with cancer in Canada: implications for health services delivery. Pediatr Blood Cancer. (2012) 58:572–8. doi: 10.1002/pbc.23054
57. Newbold B. The short-term health of Canada's new immigrant arrivals: evidence from LSIC. Ethn Health. (2009) 14:315–36. doi: 10.1080/13557850802609956
58. Marier P, Skinner S. The impact of gender and immigration on pension outcomes in Canada. Canadian Public Policy. (2008) 34:S59–78. doi: 10.3138/cpp.34.4.S59
Keywords: barriers, access, health care, older Chinese immigrants, Canada, scoping review
Citation: Zhu C, Song B, Walsh CA, Ekoh PC, Qiao X and Xu A (2024) Barriers to accessing health care of older Chinese immigrants in Canada: a scoping review. Front. Public Health 12:1445964. doi: 10.3389/fpubh.2024.1445964
Received: 08 June 2024; Accepted: 21 October 2024;
Published: 05 November 2024.
Edited by:
Palmira Immordino, University of Palermo, ItalyReviewed by:
Sally Moyce, Montana State University, United StatesSilvia Candela, IRCCS Local Health Authority of Reggio Emilia, Italy
M. Alvi Syahrin, Immigration Polytechnic, Indonesia
Karen Lau, St George's, University of London, United Kingdom
Copyright © 2024 Zhu, Song, Walsh, Ekoh, Qiao and Xu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Aijun Xu, eHVhaWp1bjIwMDBAbmp1Y20uZWR1LmNu; Xuebin Qiao, cWlhb3hiQG5qbXUuZWR1LmNu
†These authors have contributed equally to this work