 Katarzyna Tomaszewska
Katarzyna Tomaszewska- 1Department of Nursing, Institute of Health Protection, The Bronisław Markiewicz Academy of Applied Sciences, Jarosław, Poland
- 2Department of Integrated Medical Care, Medical University of Bialystok, Białystok, Poland
- 3Department of Nursing, Institute of Health Protection, State Academy of Applied Sciences, Przemyśl, Poland
Introduction: Work in health care is classified as a difficult profession and nurses are considered among the professional group that is exposed to the permanent impact of occupational stress. Psychosocial working conditions and related hazards are defined as those aspects that have the potential to cause harm to an employee’s mental or physical health. Lack of psycho-physical health well-being reduces job satisfaction and thus job commitment.
Aim: The aim of this study was to assess the overall well-being of nurses and examine the correlation between nurses’ well-being and their assessment of psychosocial working conditions in conjunction with occupational and demographic factors.
Materials and methods: A descriptive cross-sectional survey was conducted among 526 nurses employed in a selected public clinical hospital in Poland. All nurses provided labor during the survey. A diagnostic survey method using the standardized Psychosocial Working Conditions questionnaire based on the demands-control-support stress model was used for measurement.
Results: The examined nurses rated highly job demands (mean 3.46) as well as the scale of desired changes (mean 3.44). The ability to control their work (mean 3.19) and the level of social support (mean 3.21) were rated at a slightly lower level. The scale of well-being was rated highest by respondents (mean 3.68). Several statistically significant correlations (p < 0.05) can be observed between the well-being scale and the other scales of psychosocial working conditions across age categories. The least correlated are the well-being and demands scales, although as age increases with higher levels of well-being, the demands scale scores decrease.
Conclusion: The well-being of the examined nurses was closely related to sociodemographic data and the individual scales of the Psychosocial Working Conditions questionnaire. Chronic diseases are associated with greater demands at work and reduced well-being. Respondents who receive higher levels of support at work experience higher levels of well-being.
1 Introduction
Mental well-being is considered an important indicator of health in research and policy debates because it reflects a person’s overall assessment of quality of life, happiness and satisfaction. It is an important determinant of individual productivity at both enterprise and societal level (1). Physical well-being is a basic indicator of quality of life, which characterizes the health condition of an individual or social group. It is treated as the well-being of a person who knows one’s potential and understands one’s emotions. At the same time, one is resilient to stress, takes care of one’s body, and has a sense of purpose, connectedness and belonging to the community (2). Lack of well-being in terms of not only mental health, but also physical health lowers the level of job satisfaction and thus commitment to work (1).
Work in health care is classified as a difficult profession due to its complexity, as well as multitasking. Carrying out the work of a nurse due to the specifics of the profession – constant contact with another (sick, suffering, sometimes dying) person causes nurses to be counted among the professional group that is exposed to the permanent impact of occupational stress (3, 4). An undeniable source of stress among medical personnel is the specific organization of work, which is characterized by irregularity, shift work, prolonged periods of work in constant tension or shortage of staff. All these factors consequently translate into physical and mental fatigue (5). The professional work of nurses is inextricably linked to unpredictable situations, during which often the lives of patients are decided by mere seconds. Time pressure contributes to progressive fatigue, reduced work efficiency, as well as a decline in nurses’ psychological well-being (6).
Psychosocial hazards can be defined as those aspects of the design and management of the work process, along with their socio-organizational context, that can cause psychological or physical harm (7, 8). The International Labor Organization defines psychosocial risk factors as the interaction between the content of work, the management and organization of the work process and other organizational and environmental conditions on the one hand, and the needs and competencies of workers on the other (9). Psychosocial risks can be defined more simply as those aspects of the work process with their organizational and social context that have the potential to cause psychological or physical harm and are associated with the experience of occupational stress (10, 11). Psychosocial working conditions are a key determinant of work stress, an important mediator in the path between shift work and health (12). Therefore, the work environment is very important for employee health and productivity (13). Thanks to decades of extensive research on occupational health and safety, the physical and psychosocial work conditions that pose risks and resources are now well understood (14). Psychosocial occupational hazards are not always immediately apparent and are sometimes difficult to diagnose, but like physical hazards they are controllable (e.g., through psychosocial risk management) (15).
Important factors associated with stress at work are its demands, job tension and uncertainty, and resources such as job control and social support. High job demands, low levels of job control and poor social support are associated with various outcomes of poor health, such as poor mental health and sick leave (16). In contrast, high demands combined with high levels of control lead to better well-being, learning, motivation and skill development. Various models of stress at work commonly maintain that high demands at work do not necessarily negatively affect psychological well-being when combined with sufficient resources and rewards (2). According to Siegrist’s effort-reward imbalance model, high levels of effort expended combined with low reward can lead to strong negative emotions and stress reactions. Job insecurity and employment anxiety are considered determinants of poor psychological well-being, although the mechanisms of how these problems affect employee well-being are unclear. Nevertheless, perceived job insecurity has been linked to reduced psychological well-being. The risk of losing one’s job can be just as stressful as actually losing one’s job, as the uncertainty of the situation makes it difficult to manage the situation and respond appropriately (17).
Nursing requires commitment to the work and concern for the welfare of the patient (5, 18). Two key determinants of the quality of nurses’ psychosocial work environment are workload and the quality of relationships with other health care professionals. Regarding workload, studies have shown that even when nurses manage to effectively prioritize and adjust their work practices under high time pressure, the increased risk of adverse consequences for patients remains highly unsatisfactory. In terms of social relationships in the workplace, some of the key characteristics include the ability to work with competent colleagues, supportive relationships with management, and working in cultures that promote continuous improvement and skill development (19).
The presented study can expand the knowledge of the factors on which the well-being of the studied group of nurses depends. It can also show that the provision of proper psychosocial working conditions is a very important element in the job satisfaction of the examined nurses.
The aim of this paper was to assess the overall well-being of nurses and to investigate the correlation between nurses’ well-being and their assessment of psychosocial working conditions in relation to occupational and demographic factors. Based on the purpose of the study, the following research problems were formulated:
1. Is the assessment of well-being correlated with selected sociodemographic factors?
2. Are there correlations between well-being and individual scales of the Psychosocial Working Conditions questionnaire?
3. Are there correlations between the prevalence of chronic diseases among respondents, well-being and the individual scales of the Psychosocial Working Conditions questionnaire?
Analysis of the obtained results would allow us to understand what the respondents’ well-being depends on, whether the examined nursing staff expects changes in their work environment, and if so, what aspects they concern. At the same time, thanks to the knowledge of what factors affect their well-being, it will be possible to outline strategies for improvement at individual workplaces.
2 Materials and methods
2.1 Research design
In the present study, a survey was conducted among nurses employed at a selected clinical hospital in Poland’s public health sector. The survey was conducted in May 2023. This survey-based, descriptive cross-sectional study was carried out to assess respondents’ knowledge of psychosocial working conditions.
2.2 Research tools
Authors used the standardized Psychosocial Working Conditions questionnaire to measure psychosocial working conditions, which is based on the demands-control-support stress model. According to this model, stress at work is the resultant of three main characteristics of work: the magnitude of job demands; the possibility of control, i.e., the ability to influence the work and its conditions; and social support, i.e., the feeling of being able to receive help in everyday and difficult situations. The most unfavorable situation from the point of view of stress is one in which high demands are accompanied by low levels of control and social support.
The questionnaire consists of five theoretical scales:
1. Demands scale (W) – what demands does your job make?
2. Control scale (K) – to what extent can you influence what happens at work?
3. Social support scale (WS) – what support and help can you count on?
4. Well-being scale (D) – what is your well-being?
5. Scale of desired changes (PZ) – do you expect any changes at work?
In addition to the theoretical scales, empirical scales were developed. They consist of three scales on requirements:
1. intellectual requirements,
2. psycho-physical requirements and those arising from safety responsibilities,
3. requirements resulting from role conflict and overload.
Within the scales measuring control, there are two empirical scales:
1. behavioral control,
2. cognitive control.
The scale to assess social support includes two empirical scales:
1. support from superiors,
2. support from co-workers.
The scale for well-being distinguishes two empirical scales:
1. physical well-being,
2. psychological well-being.
The advantage of the Psychosocial Working Conditions questionnaire is the norms obtained from 8 different occupational groups, which allow the results to be compared with other occupations. A total of 3,992 people were examined from the following occupational groups: banking and insurance specialists, nurses, construction workers, salespeople, government officials, IT specialists, public transportation drivers and teachers. The norms of the questionnaire make it possible to relate the results of the examined group to all of the aforementioned occupational groups combined. The internal consistency indices (Cronbach’s alpha) of the individual theoretical scales are high. They range from 0.74 to 0.87 for the requirements scale, 0.79–0.86 for the control scale, 0.92–0.96 for the social support evaluation scale, 0.88–0.91 for the well-being scale, and 0.88–0.93 for the need for change scale in each professional group. For the purposes of this study, scores were calculated for each scale and subscale according to the coding rule and key provided by the authors. The scores for the answers to the questions included in the scale were then summed and the obtained values were compared with the norms (20).
2.3 Participants
In the present study, a survey was conducted among 526 nurses employed at a selected clinical hospital in Poland’s public health sector. The survey was conducted by a diagnostic survey method using Psychosocial Working Conditions Questionnaire. Respondents had varying levels of seniority and education. Each respondent independently and voluntarily completed the survey questionnaire and gave written consent to participate in the study, and each respondent received information about the processing of respondents’ personal data. The consents and survey questionnaires are in the possession of the author of the paper. Initially 752 questionnaires were distributed, 526 were accepted and correctly completed, which accounted for 69.95%. The criteria for inclusion in the study were current employment and consent to participate in the study. The questionnaires were left in the nursing rooms and after completion were collected by the authors of the study.
2.4 Statistical analysis
In the analysis of the collected material, descriptive statistics were used to present the most important information about the variables analyzed in the study and the group of respondents. The choice of statistical methods was determined by the nature of the characteristics under consideration. In the case of the study of the impact of a trait of a nominal nature on the evaluation of working conditions, statistical analysis was reduced to a comparison of average values in the separated groups. Correlations between ordinal or quantitative variables (during the unfulfilled conditions of using parametric tests) were made using Spearman’s rho coefficient, which indicates the intensity of the relationship and its direction – positive or negative. The resulting value ranges from −1 to 1, with (−1) indicating a perfect negative correlation and (1) a perfect positive correlation. Having previously met the assumptions provided for parametric tests, the analyses used r-Pearson correlations and stepwise linear regression. The r-Pearson correlation coefficient can take values from −1 to 1. Based on the numerical value, we can infer the strength of the relationship – the closer the value is to zero, the weaker the strength of the relationship. The analysis was performed using the IBM SPSS 29.0 package with the Exact Tests module. All relationships/correlations/differences are statistically significant when p ≤ 0.05.
2.5 Ethical procedures
The participation of nurses in the study was voluntary and anonymous. The study was conducted in accordance with the ethical standards set forth in the Declaration of Helsinki (64th WmA General Assembly, Fortaleza, Brazil, October 2013) and in accordance with Polish legal regulations. The application was favorably approved by the Bioethics Committee of the State Academy of Applied Sciences in Przemysl (KBPANS No. 06/2023).
3 Results
The characteristics of the study group are shown in Table 1.
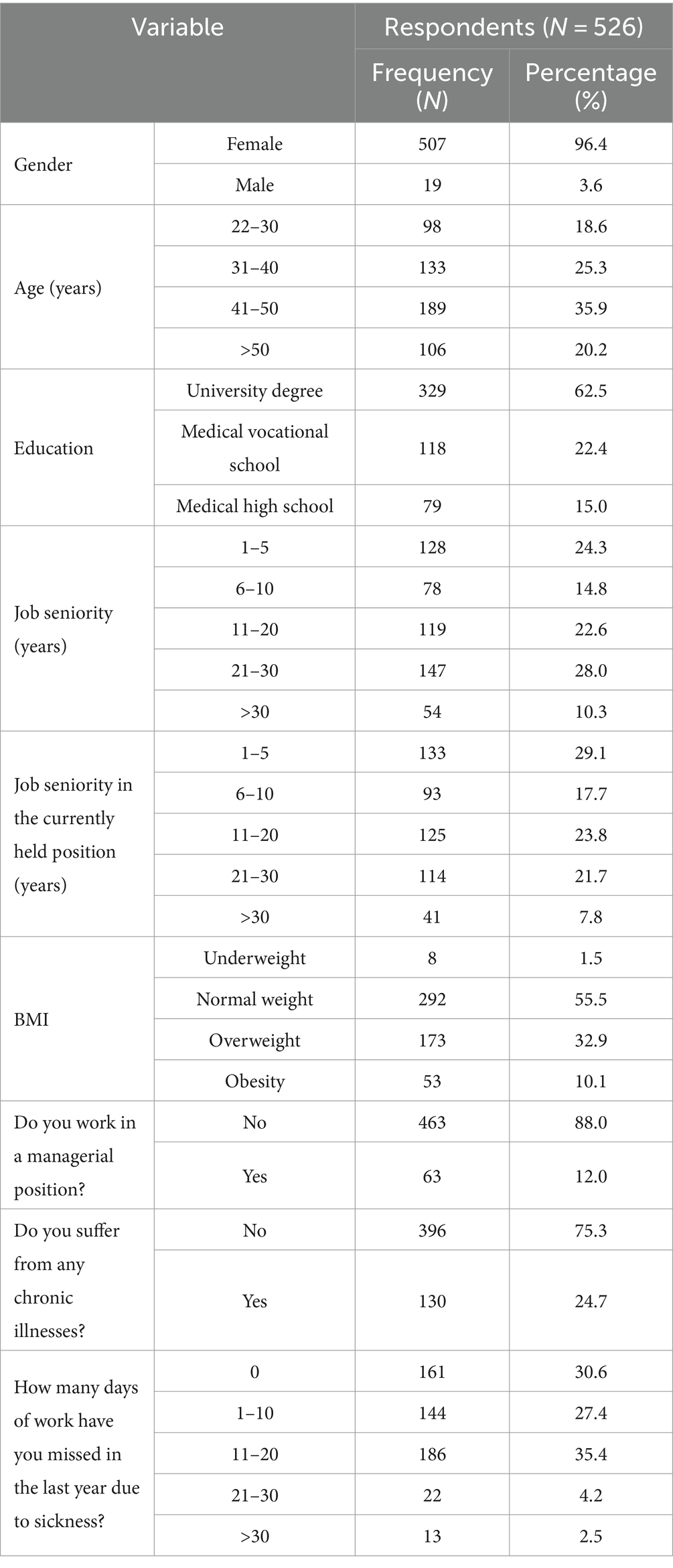
Table 1. Characteristics of the study group.
The mean age of the nurses examined was 41.82. The mean BMI score indicates that the respondents are of normal weight. During the past year, the respondents’ absenteeism from work due to sickness averaged 8.4 days.
In the results obtained, the higher the mean (range from 1 to 5), the higher the level of requirements (W), the higher the range of control (K), the higher the level of perceived social support (WS), the higher the level of well-being (D) and the higher the level of desired changes at work (PZ).
The nurses examined rated highly the demands made by the job (mean 3.46) as well as the scale of desired changes (mean 3.44). The ability to control their work (mean 3.19) and the level of social support (mean 3.21) were rated at a slightly lower level. The scale of well-being was rated highest by respondents, with a mean of 3.68. Detailed results are presented in Table 2.

Table 2. Mean scores of individual scales of the psychosocial working conditions questionnaire.
Several statistically significant correlations (p < 0.05) can be observed between the well-being scale and the other scales of psychosocial working conditions across age categories. The least correlated are the well-being and demands scales, although as age increases with higher levels of well-being, the demands scale scores decrease. In addition, the clear values of the correlation coefficients inform that the higher the well-being scores, the higher the scores of control and social support, and lower scores of the scale of desired changes are observed. Between the well-being scale and the scales of control and desired changes, a trend can be seen that there is greater strength of the relationship in older age groups (Table 3).
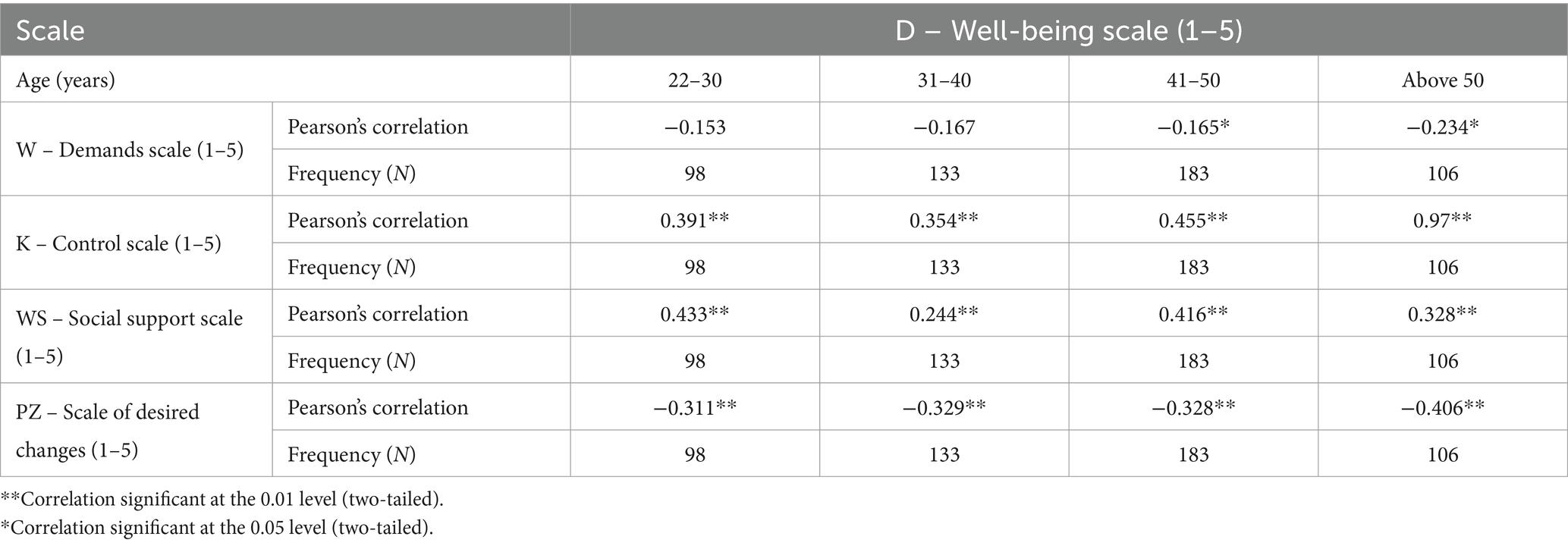
Table 3. Correlations between respondents’ age, well-being and individual scales of the psychosocial working conditions questionnaire.
Considering the two types of educational degree, similar values of correlation coefficients are observed between well-being and the scales of demands, control, social support and desired changes. The most pronounced relationship strengths that are statistically significant (p < 0.05) are between the well-being scale and the scales of control, social support and the scale of desired changes (Table 4).
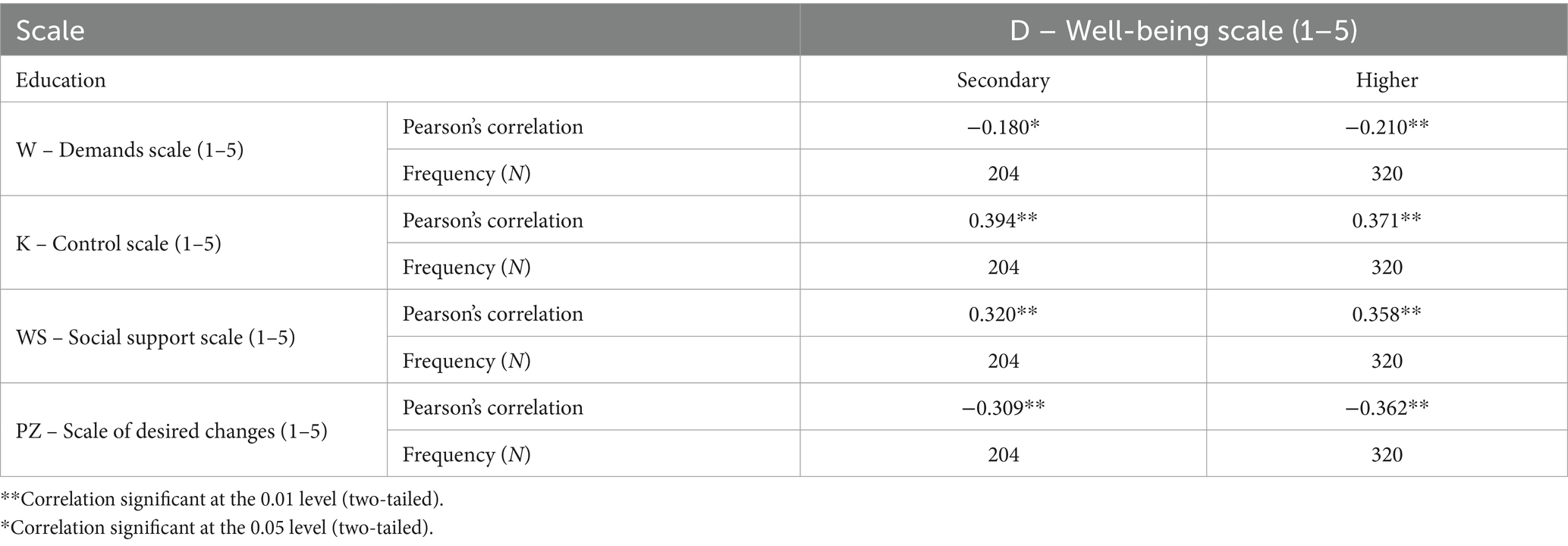
Table 4. Correlations between respondents’ education, well-being and individual scales of the psychosocial working conditions questionnaire.
Analyzing the correlations between well-being and the other scales relating to psychosocial working conditions in each category of job seniority, the strongest value of the correlation coefficient, which is statistically significant (p < 0.05), informs that in the group of those who have been working for 6–10 years, the higher the well-being scores, the higher the control scale scores. Similar correlations apply to the other seniority groups, but they are already less pronounced. In addition, higher levels of well-being are associated with higher levels of social support and lower levels of desired changes, but less clear statistically significant correlations in this regard can be seen in the group of those working from 11 to 20 years (Table 5).
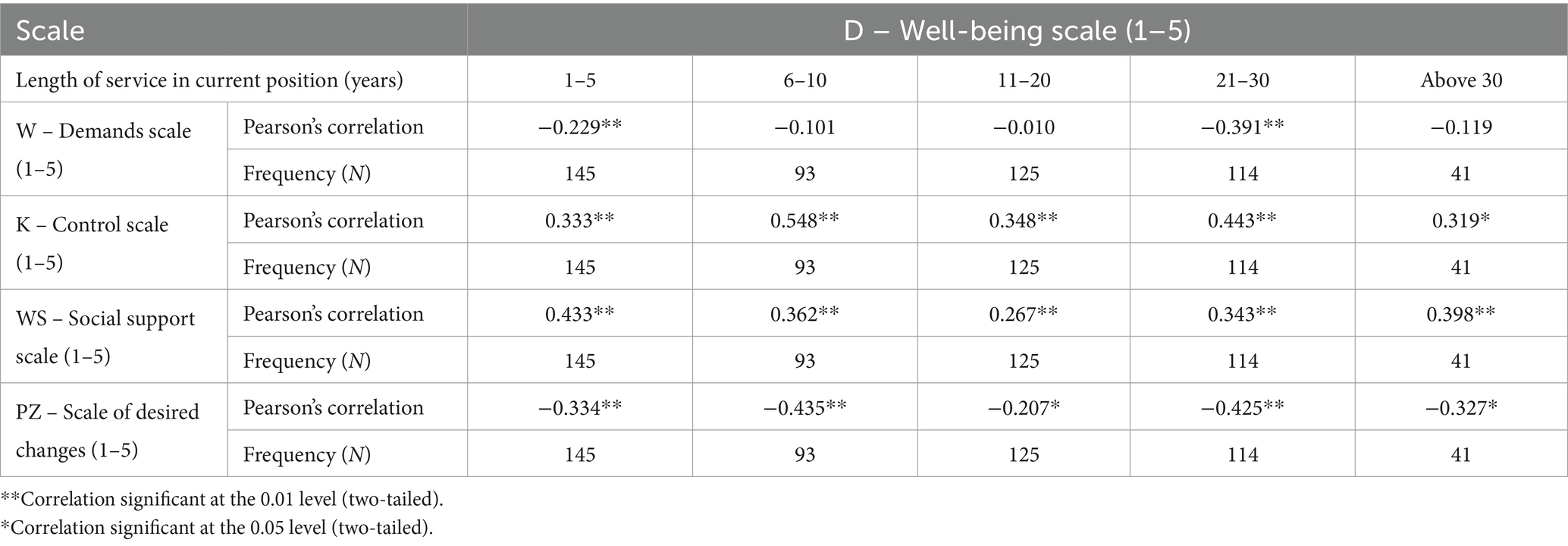
Table 5. Correlations between respondents’ job seniority, well-being and individual scales of the psychosocial working conditions questionnaire.
There is a higher strength of the relationship between well-being and the scales of control and social support among those who work in managerial positions compared to those in lower positions. Higher values of one variable are associated with higher values of the other variable. For both managerial and non-managerial positions, a clear and negative statistically significant correlation (p < 0.05) is found between the well-being scale and the scale of desired changes (Table 6).
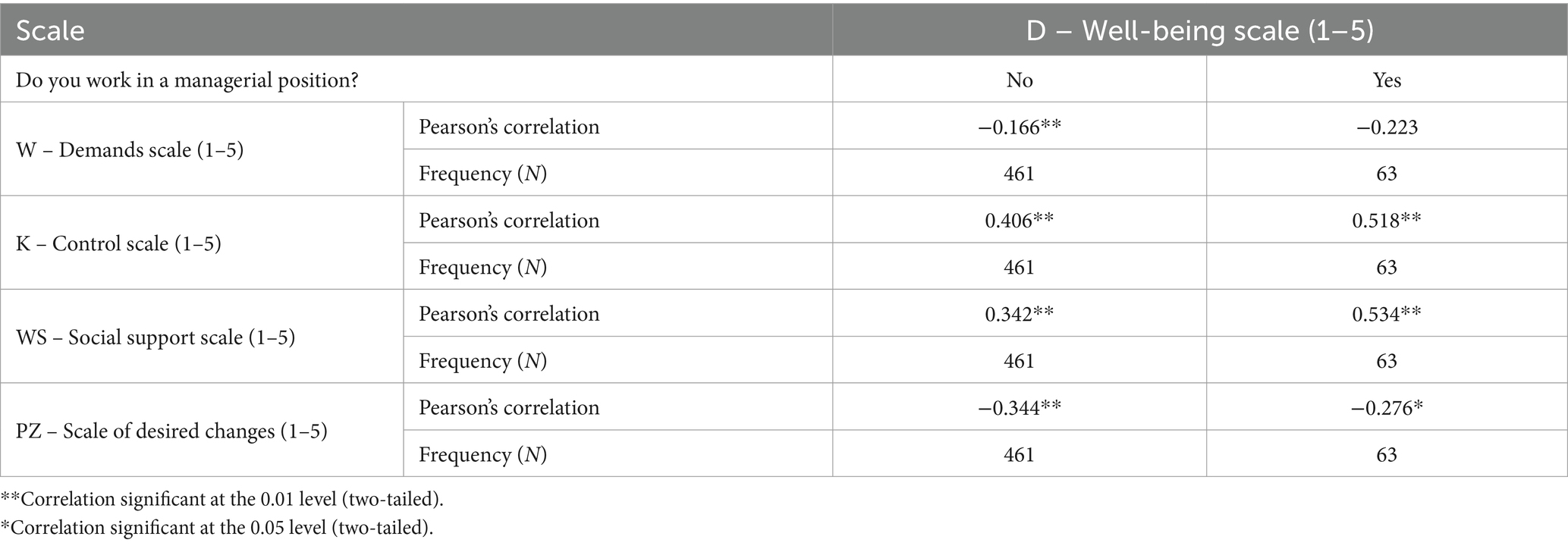
Table 6. Correlations between occupation, well-being and individual scales of the psychosocial working conditions questionnaire.
Among those who have chronic diseases compared to those who do not have such diseases, there is a more pronounced strength of the relationship statistically significant (p < 0.05) between the scale of well-being and the sum of desired changes. Higher levels of well-being are associated with lower levels of desired changes. In addition, quite clear and similar values of correlation coefficients in the two analyzed groups relate to the scale of well-being and the scale of control and social support. The higher the level of well-being, the higher the scores of the scale of control and social support (Table 7).
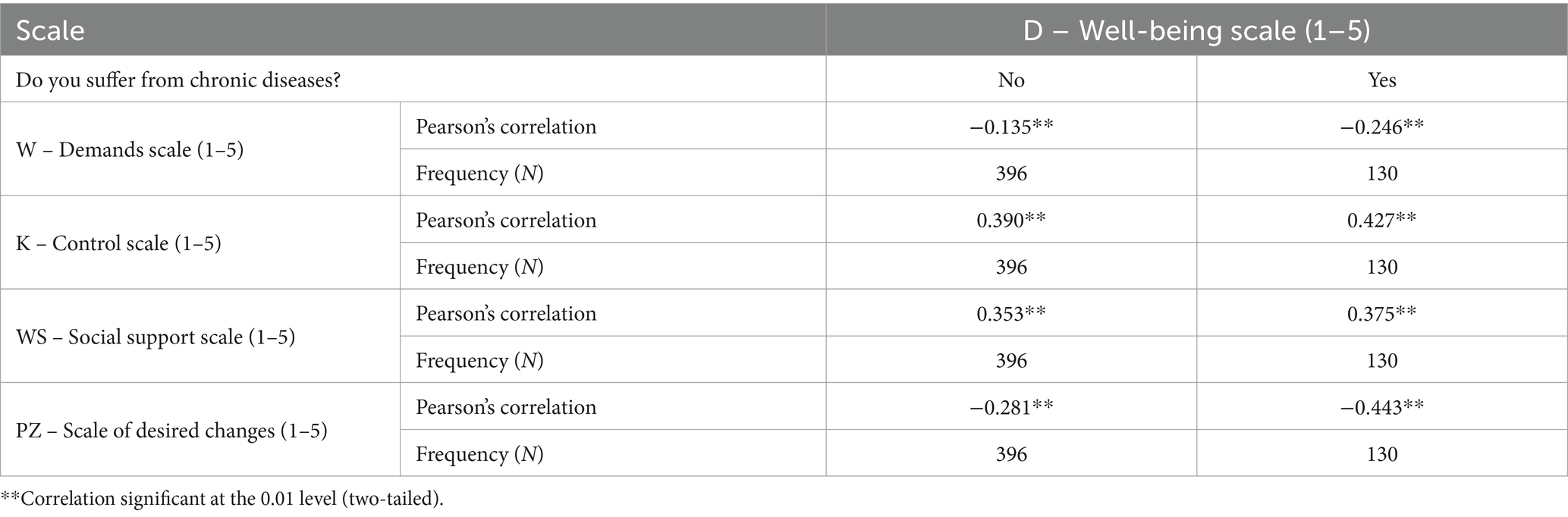
Table 7. Correlations between respondents’ prevalence of chronic diseases, well-being and individual scales of the psychosocial working conditions questionnaire.
4 Discussion
The aim of the study was to assess the overall well-being of nurses and examine the correlation between nurses’ well-being and their assessment of psychosocial working conditions in conjunction with occupational and demographic factors.
An analysis of the relationship between ratings of various aspects of nurses’ psychosocial working conditions was conducted. The respondents rated the scale of well-being highest and at a comparable high level rated the demands of their work as well as the scale of desired changes. The ability to control their work and the level of social support were rated at a slightly lower level. There are a few statistically significant correlations between the length of job tenure and the scores of the various scales, but each is characterized by negligible strength of association. It should also be noted that there are no statistically significant correlations between age and psychosocial working conditions. Older employees with a high sense of well-being showed less need for change than their younger counterparts. Almeida et al. proved that nurses’ levels of job well-being differed significantly in terms of education level, job satisfaction and life satisfaction (6). This was corroborated by Carneiro and Bastos, proving that factors related to well-being at work include sociodemographic data and interactions within the treatment team, interaction between personal and professional life, and organizational commitment (21). Self-study among people with chronic diseases showed a stronger correlation between well-being and the scale of desired changes. Other studies have found that middle-aged individuals were characterized by poorer health and greater exposure to psychosocial risks (12, 22, 23). Bujacz et al. demonstrated that mid-career nurses in work environments characterized by low autonomy and support tended to report poorer health outcomes (19), while other authors have found that nurses working in hospitals find that their jobs place high demands on them, while their sense of control over their work is reduced, which predisposes them to very high levels of stress (7) and poor quality of life (24). A study in Norway using data from the WorkSafeMed survey, statistically found only differences between the time control scale and social relationships (3).
Our own study found that lower levels of education were associated with lower scores on the control scale, the social support scale and the well-being scale, but the strengths of the association between the variables were insignificant. A study by Misiak et al. found that better-educated respondents rated the level of demands at work as higher, but they were also more satisfied in the well-being category (5). Lorber et al. proved that the level of well-being differed significantly according to the level of education, and seniority and place of work (10), which is confirmed by other studies (25).
Gustafsson et al. showed that by examining three dimensions of psychosocial working conditions: job demands, job control and job support, the problems of presenteeism and low work capacity among many health and care workers can be alleviated by reducing psychosocial demands (11).
In our own research, the mean period of respondents’ incapacity to work on sick leave was more than 8 days. A survey of nurses in Sweden found that the high rate of sickness absence among care workers in Sweden can be reduced if simultaneous exposure to high psychosocial and physical challenges is avoided. Management policies to reduce time pressure, improved lifting aids and measures to prevent uncomfortable working positions are recommended (26). In another study, due to the numerous stressors and psychosocial working conditions, it was claimed that employers should make an effort to modify them (27) which is supported by other studies (28). A study by Ersin et al. found a positive, weakly significant relationship between nurses’ psychological well-being and their perception of social support (29) and increasing social support from fellow nurses is an effective way to deal with the negative effects of nurses’ emotional demands. Younger nurses tended to have higher emotional demands and lower social support from colleagues (30). Social support is a key resource in the context of nursing work, with beneficial effects on well-being (e.g., reducing role stress) and job satisfaction (31). Factors of the work environment, such as adequate staffing, good cooperation with physicians, support from management, and professional autonomy, significantly affect nurses’ assessment of patient safety (32). Given the large number of published studies on the impact of psychosocial working conditions on workers’ health, it is important to consider that for outcomes such as cardiovascular disease and depression, their results show that respondents reporting excessive workloads, imbalance between commitment and reward, job insecurity and long working hours are at increased risk of psychosocial strain (33).
5 Limitations of the study
A strength of the study is the number of examined nurses participating in the survey. Limitations characteristic of cross-sectional studies apply. The survey was conducted in a single clinical hospital at a specific time. In addition, during the survey, there was a possibility of an exchange of opinions among the nurses, which may have influenced their responses.
6 Conclusion
The study has proved that the higher the well-being scores, the higher the control and social support scores, and observed lower scores on the desired change scale. Older employees with high levels of feelings of well-being showed less need for change than their younger counterparts. Education, length of service and position held did not significantly differentiate the correlation between well-being and the other scales of psychosocial working conditions. Among those with chronic diseases, there was a stronger correlation between well-being and the scale of desired changes. Nurse managers and executives should consider the above findings when developing strategies to improve the work environment, aiming to reduce workload and retain nurses in the profession. It is also worth conducting multi-center studies to generalize the findings and gain better insight into the psychosocial aspects of nurses’ work, which are the basis of job satisfaction which is inextricably linked to higher quality of services provided.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the Bioethics Committee of the State Academy of Applied Sciences in Przemysl. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
KT: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. KK: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. BM: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Supervision, Validation, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Graham, C, Laffan, K, and Pinto, S. Well-being in metrics and policy. Science. (2018) 362:287–8. doi: 10.1126/science.aau5234
2. Ni, MY, Yao, XI, Cheung, F, Wu, JT, Schooling, CM, Pang, H, et al. Determinants of physical, mental and social well-being: a longitudinal environment-wide association study. Int J Epidemiol. (2020) 49:380–9. doi: 10.1093/ije/dyz238
3. Wagner, A, Nübling, M, Hammer, A, Manser, T, and Rieger, MAon behalf of the WorkSafeMed Consortium, et al. Comparing perceived psychosocial working conditions of nurses and physicians in two university hospitals in Germany with other German professionals – feasibility of scale conversion between two versions of the German Copenhagen psychosocial questionnaire (COPSOQ). J Occup Med Toxicol. (2020) 15:26. doi: 10.1186/s12995-020-00277-w
4. Nordenmark, M, Almén, N, and Vinberg, S. Work/family conflict of more importance than psychosocial working conditions and family conditions for mental wellbeing. Societies. (2020) 10:67. doi: 10.3390/soc10030067
5. Misiak, B, Sierżantowicz, R, Krajewska-Kułak, E, Lewko, K, Chilińska, J, and Lewko, J. Psychosocial work-related hazards and their relationship to the quality of life of nurses-a cross-sectional study. Int J Environ Res Public Health. (2020) 17:755. doi: 10.3390/ijerph17030755
6. Almeida, D, Figueiredo, AR, and Lucas, P. Nurses’ well-being at work in a hospital setting: a scoping review. Healthcare. (2024) 12:173. doi: 10.3390/healthcare12020173
7. Nowacka, AL, Wolfshaut-Wolak, R, Piskorz, A, Wadas, T, and Gniadek, A. Psychosocial working conditions and the level of occupational burnout among nurses working in hospitals. Nurs Problems. (2022) 30:16–23. doi: 10.5114/ppiel.2022.119850
8. Janus, E, Téllez, RC, Filar-Mierzwa, K, Aleksander-Szymanowicz, P, and Bac, A. Psychosocial and health effects of the COVID-19 pandemic experienced by staff employed in social welfare facilities in Poland and Spain. Int J Environ Res Public Health. (2023) 20:3336. doi: 10.3390/ijerph20043336
9. Kuczynska, I, Mädler, M, Taibi, Y, and Lang, J. The assessment of psychosocial work conditions and their relationship to well-being: a multi-study report. Int J Environ Res Public Health. (2020) 17:1654. doi: 10.3390/ijerph17051654
10. Lorber, M, Treven, S, and Mumel, D. Well-being and satisfaction of nurses in Slovenian hospitals: a cross-sectional study. Zdr Varst. (2020) 59:180–8. doi: 10.2478/sjph-2020-0023
11. Gustafsson, K, Marklund, S, Leineweber, C, Bergström, G, Aboagye, E, and Helgesson, M. Presenteeism, psychosocial working conditions and work ability among care workers-a cross-sectional Swedish population-based study. Int J Environ Res Public Health. (2020) 17:2419. doi: 10.3390/ijerph17072419
12. Tucker, P, Peristera, P, Leineweber, C, and Kecklund, G. Can psychosocial working conditions help to explain the impact of shiftwork on health in male- and female-dominated occupations? A prospective cohort study. Chronobiol Int. (2020) 37:1348–56. doi: 10.1080/07420528.2020.1805458
13. Wesołowska, K, Elovainio, M, Gluschkoff, K, Hietapakka, L, Kaihlanen, AM, Lehtoaro, S, et al. Psychosocial work environment and cross-cultural competence among native and foreign-born registered nurses. Res Nurs Health. (2019) 42:349–57. doi: 10.1002/nur.21970
14. Corin, L, Pousette, A, Berglund, T, Dellve, L, Hensing, G, and Björk, L. Occupational trajectories of working conditions in Sweden: development trends in the workforce, 1997–2015. Scand J Work Environ Health. (2021) 47:335–48. doi: 10.5271/sjweh.3955
15. Najder, A, and Potocka, A. Relationships between psychosocial risks, health and occupational functioning among health professionals. Pielęgniarstwo Polskie NR. (2015) 3:313–20.
16. Jonsson, J, Vives, A, Benach, J, Kjellberg, K, Selander, J, Johansson, G, et al. Measuring precarious employment in Sweden: translation, adaptation and psychometric properties of the employment precariousness scale (EPRES). BMJ Open. (2019) 9:e029577. doi: 10.1136/bmjopen-2019-029577
17. De Witte, H, Pienaar, J, and De Cuyper, N. Review of 30 years of longitudinal studies on the association between job insecurity and health and well-being: is there causal evidence? Aust Psychol. (2016) 51:18–31. doi: 10.1111/ap.12176
18. Paskarini, I, Dwiyanti, E, Syaiful, DA, and Syanindita, D. Burnout among nurses: examining psychosocial work environment causes. J Public Health Res. (2023) 12:22799036221147812. doi: 10.1177/22799036221147812
19. Bujacz, A, Rudman, A, Gustavsson, P, Dahlgren, A, and Tucker, P. Psychosocial working conditions of shiftworking nurses: a long-term latent transition analysis. J Nurs Manag. (2021) 29:2603–10. doi: 10.1111/jonm.13430
20. Cieślak, R, and Widerszal-Bazyl, M. Psychospołeczne warunki pracy. Warszawa: Podręcznik do Kwestionariusza, CIOP (2000).
21. Carneiro, L, and Bastos, A. Work-related well-being: analysis of concepts and measures. Arq Bras Psicol. (2019) 72:121–40. doi: 10.36482/1809-5267.ARBP2020v72i1p.121-140
22. Moreno Martínez, M, Fernández-Cano, MI, Feijoo-Cid, M, Llorens Serrano, C, and Navarro, A. Health outcomes and psychosocial risk exposures among healthcare workers during the first wave of the COVID-19 outbreak. Saf Sci. (2022) 145:105499. doi: 10.1016/j.ssci.2021.105499
23. Januario, LB, Karstad, K, Rugulies, R, Bergström, G, Holtermann, A, and Hallman, DM. Association between psychosocial working conditions and perceived physical exertion among eldercare workers: a cross-sectional multilevel analysis of nursing homes, wards and workers. Int J Environ Res Public Health. (2019) 16:3610. doi: 10.3390/ijerph16193610
24. Teles, MA, Barbosa, MR, Vargas, AM, Gomes, VE, Ferreira, EF, Martins, AM, et al. Psychosocial work conditions and quality of life among primary health care employees: a cross sectional study. Health Qual Life Outcomes. (2014) 12:72. doi: 10.1186/1477-7525-12-72
25. Kaburi, BB, Bio, FY, Kubio, C, Ameme, DK, Kenu, E, Sackey, SO, et al. Psychological working conditions and predictors of occupational stress among nurses, Salaga government hospital, Ghana, 2016. Pan Afr Med J. (2019) 33:320. doi: 10.11604/pamj.2019.33.320.16147
26. Helgesson, M, Marklund, S, Gustafsson, K, Aronsson, G, and Leineweber, C. Interaction effects of physical and psychosocial working conditions on risk for sickness absence: a prospective study of nurses and care assistants in Sweden. Int J Environ Res Public Health. (2020) 17:7427. doi: 10.3390/ijerph17207427
27. Lisowska, A, Szwamel, K, Wilczek, A, Wolf, G, and Tomsza, K. Psycho-social working conditions of nursing, medical and paramedic staff in a hospital emergency department. Med Sci Pulse. (2022) 16:1–15. doi: 10.5604/01.3001.0016.0725
28. Kurashvili, M, Reinhold, K, and Järvis, M. Work ability and psychosocial factors in healthcare settings during COVID-19 pandemic – specific focus on ageing workers. Econ Bus. (2022) 36:164–78. doi: 10.2478/eb-2022-0011
29. Ersin, F, Havlioğlu, S, and Gür, SC. Mental well-being and social support perceptions of nurses working in a Covid-19 pandemic hospital. Perspect Psychiatr Care. (2022) 58:124–31. doi: 10.1111/ppc.12833
30. Chang, HE, and Cho, SH. The influence of social support on the relationship between emotional demands and health of hospital nurses: a cross-sectional study. Healthcare. (2021) 9:115. doi: 10.3390/healthcare9020115
31. Malinowska-Lipień, I, Micek, A, Gabryś, T, Kózka, M, Gajda, K, Gniadek, A, et al. Impact of the work environment on patients’ safety as perceived by nurses in Poland-a cross-sectional study. Int J Environ Res Public Health. (2021) 18:12057. doi: 10.3390/ijerph182212057
32. Orgambídez, A, Almeida, H, and Borrego, Y. Social support and job satisfaction in nursing staff: understanding the link through role ambiguity. J Nurs Manag. (2022) 30:2937–44. doi: 10.1111/jonm.13675
Keywords: nurse, working conditions, physical strain, mental strain, nurses
Citation: Tomaszewska K, Kowalczuk K and Majchrowicz B (2024) Correlations between well-being of nurses and psychosocial working conditions – a descriptive cross-sectional study. Front. Public Health. 12:1443015. doi: 10.3389/fpubh.2024.1443015
Edited by:
Sabina Krupa, University of Rzeszów, PolandReviewed by:
Adriano Friganovic, University of Rijeka, CroatiaPenpatra Sripaiboonkij, University College Dublin, Ireland
Copyright © 2024 Tomaszewska, Kowalczuk and Majchrowicz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Katarzyna Tomaszewska, dG9ta2E4QHdwLnBs