 Yan Zhao
Yan Zhao Bei Yang
Bei Yang Jianying Chu
Jianying Chu- 1Department of General Surgery, Qilu Hospital of Shandong University, Jinan, China
- 2Department of Plastic, Aesthetic, Reparative and Reconstructive Unit Nursing, West China Second Hospital, Sichuan University/West China School of Nursing, Sichuan University, Key Laboratory of Birth Defects and Related Diseases of Women and Children (Sichuan University), Ministry of Education, Chengdu, Sichuan, China
- 3Department of Obstetrics, Qilu Hospital of Shandong University, Jinan, Shandong, China
- 4Nursing Theory & Practice Innovation Research Center, Shandong University, Jinan, Shandong, China
Background: This study aimed to identify the types of quality of life (QoL) based on the five dimensions of the EQ-5D and predict factors affecting QoL.
Methods: A multistage stratified cluster sampling survey was conducted among the staff of 12 general hospitals, 1,965 nurses completed the survey, and the data were analyzed using SPSS 26.0 and Mplus 8.3 for latent analysis.
Results: Three latent classes of QoL were identified: low-level (2.8%), pain and discomfort (7.6%), medium-level (47.1%), and high-level (42.5%). The types and characteristics of QoL differed among these latent classes. The low-level group had the lowest EQ visual analog scale (EQ-VAS) score (F = 75.217, P < 0.001) and the highest K10 score (F = 61.90, P < 0.001). Moreover, increased age (OR = 0.819, 95% CI: 0.817–0.973), never having drunk alcohol (OR = 0.107, 95% CI: 0.023, 0.488), and increased EQ-VAS scores (OR = 0.935, 95% CI: 0.919, 0.952) were protective factors for quality of life, while working in obstetrics and gynecology (OR = 6.457, 95% CI:1.852, 22.512) and higher K10 scores (OR = 1.153, 95% CI: 1.100, 1.209) were risk factors for quality of life.
Conclusion: The results indicated significant heterogeneity in the types of QoL and identified predictors of QoL. These findings provide basic information for the development of nursing interventions to improve quality of life and identified specific characteristics that should be considered during intervention development.
1 Background
Health-related quality of life refers to the experience of individuals in different cultures and value systems regarding their goals, expectations, standards, and living conditions related to things they care about as a subjective perception and expression of health; it reflects individuals' physical, psychological, social, spiritual, and personal roles (1). The complete state of experience in aspects such as psychology, society, spirit, and personal role function is a comprehensive reflection of an individual's health status (2).
There are several factors influencing health-related quality of life, which are not only related to individual health status, health behavior, economic, and cultural factors (2–5), but also closely related to occupational characteristics (6). Nursing staff play an important functional role in medical and health services, and the health-related quality of life of clinical nurses is affected by the high risk and pressure of nursing work and the insufficiency of family and social resources (7). Studies have shown that nurses' quality of life is at the middle to lower levels (6). Nurses' quality of life is important as it is closely related to the quality of nursing work (8).
The Latent Class Model (LCM) is a statistical analysis method in which the model fit is determined by the data, which can capture the inequalities of the population, thereby objectively identifying mutually exclusive subtype categories (9). From the group heterogeneity perspective, this study explored the latent categories of nurses' quality of life based on the LCM and identified the performance characteristics of different latent categories regarding demographic sociology, physical health, mental health, etc. Through population characteristics, low-level QoL groups can quickly be identified, effective targeted intervention strategies can be formulated, and a theoretical basis for improving nurses' QoL can be provided.
2 Methods
2.1 Study population
The study sample consisted of 1,965 nurses employed at general hospitals in Shandong Province. A multi-stage stratified whole-group sampling method was applied from November 2020 to January 2021. First, all prefecture-level cities in Shandong Province were ranked according to their 2018 GDP per capita levels and were divided into three categories: good, medium, and poor. Subsequently, one prefecture-level city was selected from each category via simple random sampling (Qingdao City, Zaozhuang City, and Dezhou City). Second, a district city with only one municipal general hospital was surveyed. In cases of more than one hospital being present within a district city, one general hospital was selected via simple random sampling. Following this, three counties (districts/county-level cities) in each prefecture-level city were randomly selected. In each county (district/county-level city), one (district/county-level city) general hospital was randomly selected via the same sampling method used for city-owned hospitals. As such, this study surveyed 12 general hospitals, including three city-affiliated and nine county-affiliated hospitals. Among these, three wards were randomly selected for each discipline according to the discipline classification (all wards were surveyed in cases where fewer than three wards existed). Further, the surveyed wards' night nursing staff members were asked to complete the questionnaire.
This study was reviewed and approved by the Ethics Committee of the School of Public Health, Shandong University (approval number: 20181219). The fieldwork was initiated after approval was obtained. All participants signed an informed consent form before participating in the survey.
2.2 Quality of life
The EQ-5D-3L was used to assess QoL in this study. The scale includes two parts: the EQ-5D descriptive system and EQ-VAS (10). The health description system includes five dimensions: mobility, self-care, daily activities, pain/discomfort, and anxiety/depression, with three levels in each dimension: difficulty/problem, moderate difficulty/problem, and severe difficulty/problem; the EQ-VAS section is a vertical visual scale with 100 at the top representing “best health” and 0 at the bottom representing “worst health.” This study calculated the utility value of the EQ-5D using the Chinese version of the TTO (11).
2.3 Psychological distress
Kessler Psychological Distress Scale (K10) is a 10-item screening tool designed for non-specific psychological distress (12). In our survey, it was measured by the Chinese version of the K10 (13). Each item adopts a 5-level score of 1 (almost never) to 5 (all the time), with a total score of 50. A score of >15 indicates psychological distress, 10–15 indicates mild distress, 16–21 indicates moderate distress, 22–29 indicates severe distress, and 30–50 indicates severe psychological distress. The Cronbach's alpha coefficient in this study was 0.930.
2.4 Statistical analyses
SPSS 25.0 and Mplus 8.3 statistical software were used for data entry and statistical analysis. Enumeration data were expressed as frequency (percentage), measurement data were normally distributed, and expressed as mean ± standard deviation. Latent class analysis was used to classify participants' quality of life responses. When performing latent class analysis, the evaluation indicators of model adaptation include (1) Akaike Information Criteria (AIC), Bayesian Information Criteria (BIC), and sample size-adjusted BIC (saBIC). The smaller the value, the better the fit and the higher the performance of the model. (2) Entropy index: the higher the entropy value, the higher the accuracy of classification; when entropy = 0.6, the classification accuracy exceeds 80%, and when entropy = 0.8, the classification accuracy exceeds 90%. (3) The likelihood ratio test (Lo-Mendell-Rubin, LMR) and Bootstrap-based likelihood ratio test (BLRT). When the P value reaches a level of significance, it indicates that the model of k categories is significant due to k-1 class models (14, 15). When the models of the evaluation indicators were inconsistent, this study comprehensively considered the results of measuring each indicator and combined the “best explanation model” to determine the best model. Multivariate logistic regression was used to analyse the factors influencing each category. All statistical tests were two-sided with a test level of α = 0.05.
3 Results
3.1 The current status of the quality of life of nurses
According to the EQ-5D Effect Value Score System calculation in China, the EQ-5D and its health effect value of the nurse group was (0.9382 ± 0.1078), which was significantly lower than the QoL level of urban civilian in a certain province of China (16) (t = −7.125, P < 0.001).
3.2 Classification of nurses' quality of Life
This study begins with the initial model of the two categories and gradually increases the number of categories to determine the best model. The fitting index data are presented in Table 1. As the model category increased, the AIC, BIC, and SaBIC values of each category decreased. When the number of categories was three, the entropy value of the latent-category model was 0.804. When the number of categories was four, the entropy value was 0.784, nearly 0.8, which indicates that the classification accuracy exceeds 90%. When dividing the categories, they were distinguished in combination with practical significance and interpretability. The second category was too concise and lacked practical significance, while the fifth category was too complicated to explain. The AIC and BIC indicators of the fourth category were smaller than those of the third category, and the entropy value was close to 0.8. Comprehensively, the four-category model was the optimal model.

Table 1. Fit indices of latent class analysis and distribution rate of HRQoLs (EQ-5D).
A model with four potential categories was used as the optimal model to obtain the parameter estimation results. The conditional probability distributions for each category are presented in Figure 1. In this study, nurses were divided into four groups based on five factors. In category 1, the conditional probabilities of mobility, self-care, daily activities, pain, and anxiety/depression at the no difficulty level were 0.410, 0.639, 0.188, 0.054, and 0.227, respectively; in category 2, the conditional probabilities were 0.916, 0.921, 0.831, 0.382, and 0.418, respectively; in category 3, the conditional probabilities were 0.983, 0.986, 0.978, 0.782, and 0.818, respectively; in category 4, the conditional probabilities were 0.995, 0.990, 0.993, 0.945, and 0.968, respectively. The distribution trend of each factor was relatively consistent, consequently, they were named: “Low-level group (2.8%) (category 1),” “Pain and discomfort group (7.6%) (category 2),” “Medium-level group (47.1%) (category 3),” and “High-level group (42.5%) (category 4).”
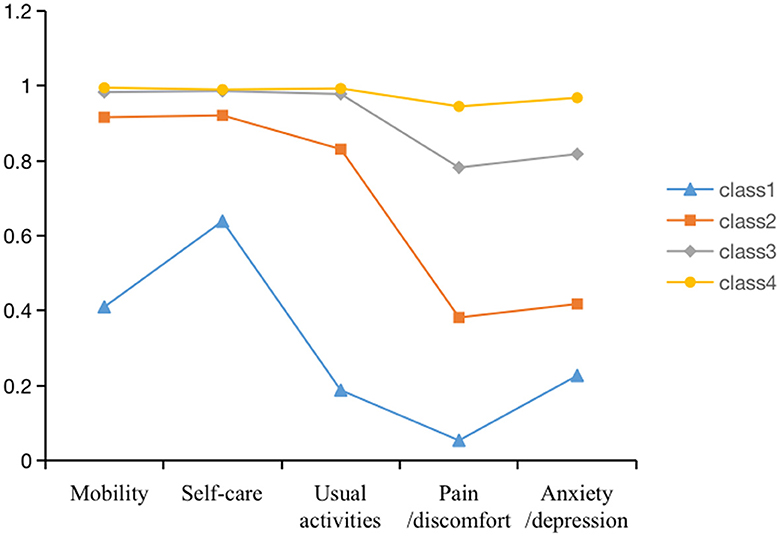
Figure 1. Types of health-related quality of life by latent classes.
3.3 Comparison of various demographic and psychological characteristics among various categories
Comparing different category characteristics, the results showed that the average age of the low-level group was (31.42 ± 5.68) years old, which was lower than other groups, and the proportion of junior professional titles and below was 79.2%, which was higher than other groups.
The proportion of obstetrics and gynecology workers was 31.3%, which was higher than other groups. In addition, a one-way analysis of variance was used to explore the differences in EQ-VAS scores and K10 scores for each category. The results showed that the low-level group had the lowest EQ-VAS score, that is, the worst health level (F = 75.217, P < 0.001), and the highest K10 score, that is, the worst psychological health level (F = 61.90, P < 0.001) (Table 2).
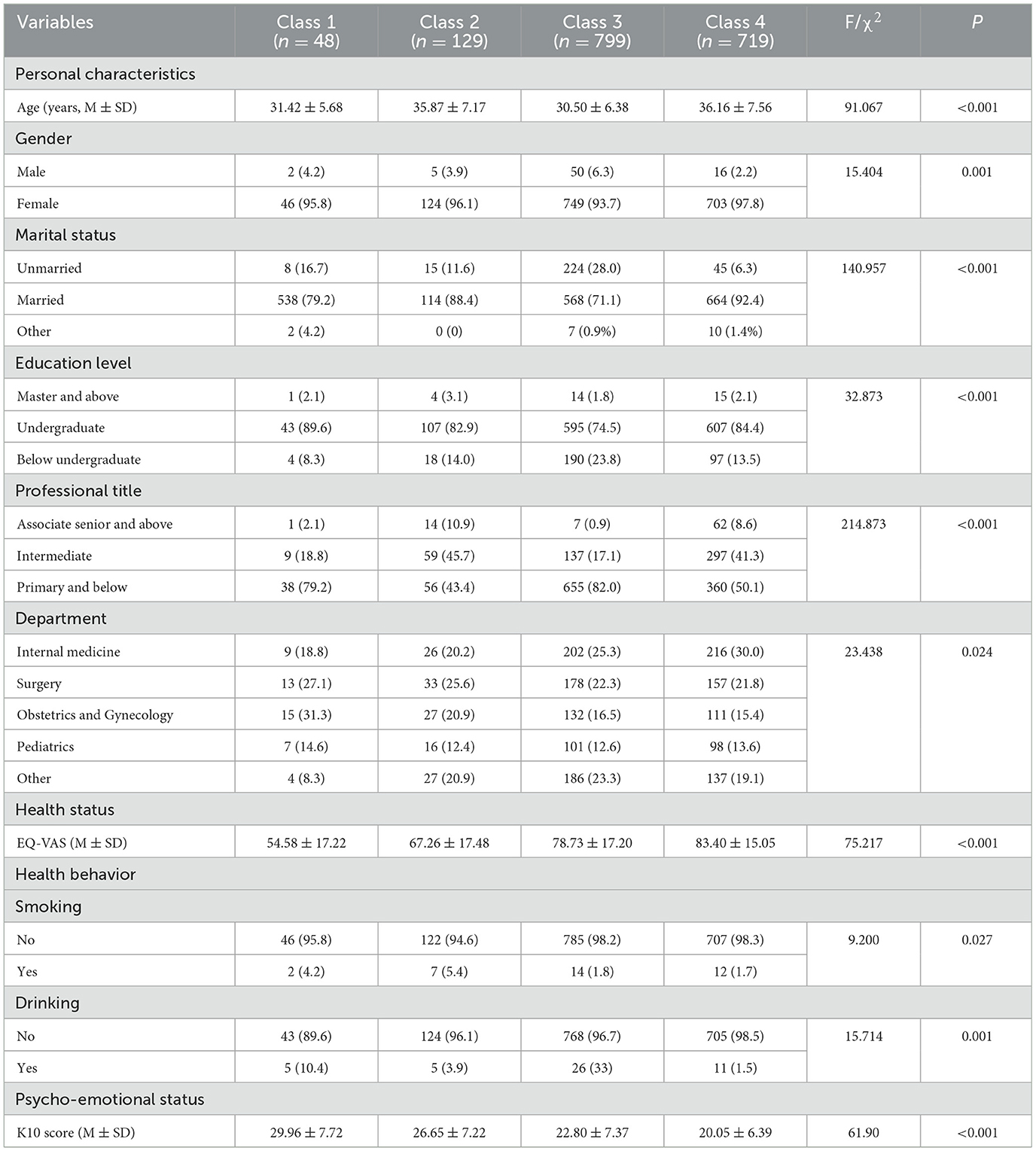
Table 2. Comparison of characteristics among latent classes in Chinese nurses n (%).
3.4 Multivariate logistic regression analysis of potential quality of life categories of nurses
Nurses' quality of life category was taken as the dependent variable (category four as the reference group), nurses' characteristics (age, sex, marital status, education level, professional title, and department), health level (EQ-VAS), health behavior (smoking, alcohol consumption), and psycho-emotional status (K10 score) were taken as independent variables, and a multivariate logistic regression model was constructed to analyse the relevant factors influencing nurses' low health levels. The results showed that increased age (OR = 0.819, 95% CI: 0.817, 0.973), never having drunk alcohol (OR = 0.107, 95% CI: 0.023, 0.488), and increased EQ-VAS scores (OR = 0.935, 95% CI: 0.919, 0.952) were quality of life protective factors, while working in obstetrics and gynecology (OR = 6.457, 95% CI: 1.852, 22.512) and higher K10 scores (OR = 1.153, 95% CI: 1.100, 1.209) were quality of life risk factors (Table 3).
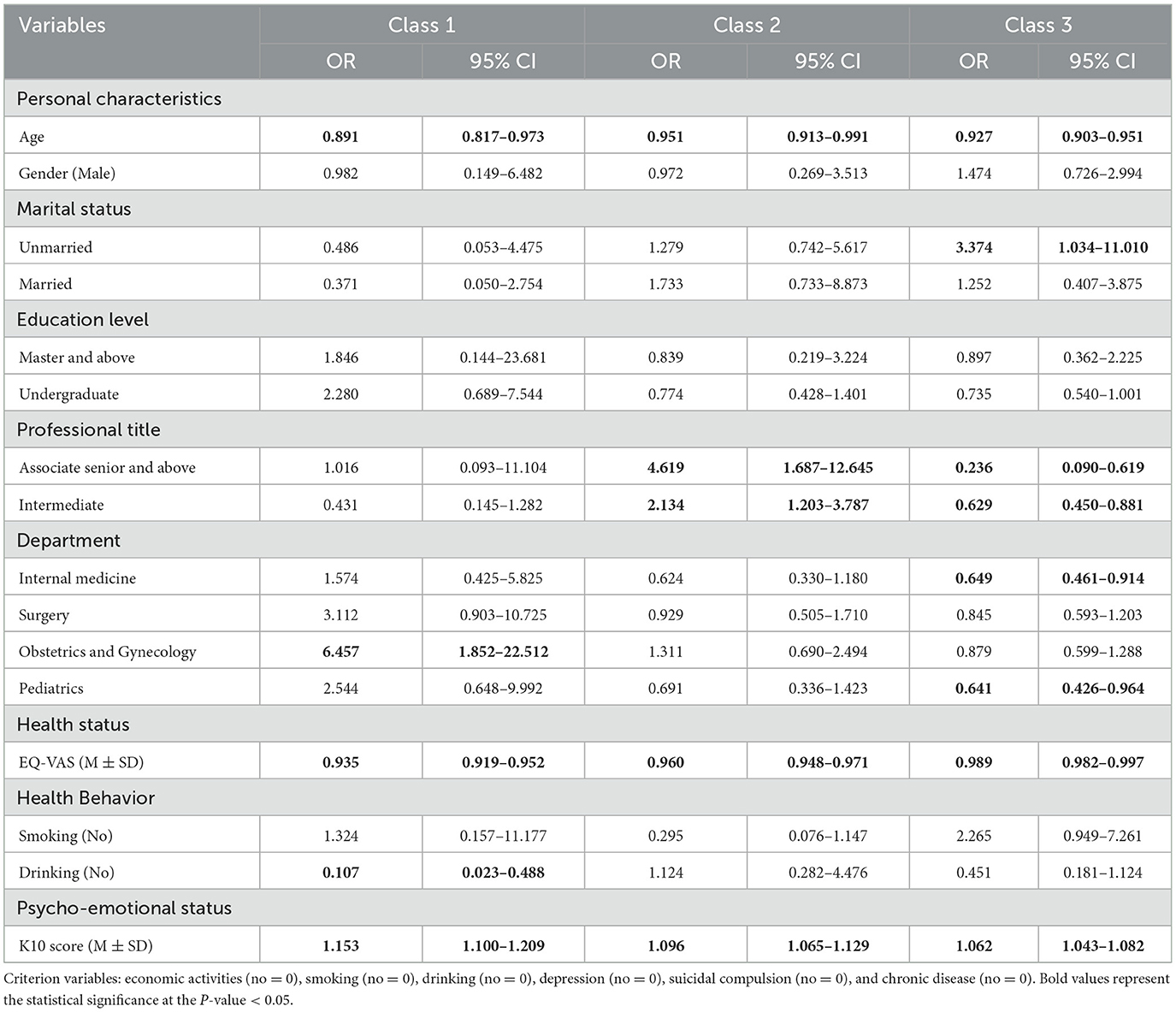
Table 3. Multinomial logistic regression models of latent class analysis of health-related quality of life.
4 Discussion
4.1 Low level of quality of life for nurses
This study found that the quality of life of nurses was lower than that of the general urban population in China (16). Nurses in the 21st century are facing increasingly difficult challenges to maintain a high quality of life (17). From long hours to inadequate pay, nurses are often overworked and underpaid (18, 19). According to the China Statistical Yearbook on Health and Family Planning, the number of registered nurses in China in 2015 was 3 million (20). Considering China's great population, China needs at least 6 million nurses (21). Due to the shortage of medical personnel, they have to work longer hours under tremendous pressure but receive very low rewards (22, 23). This leads to decreased job satisfaction and a decrease in quality of care. Therefore, there is a need to focus on the professional development of nurses at the policy level, improve the protection and training system and raise the quality of life level of the nursing community.
4.2 Potential categories of quality of life levels in the nurse population
This study used latent class analysis to examine the quality of life of the nurse population to reveal differences in the different quality of life categories and their distribution on demographic and sociological variables. The model fitting results of the four latent categories were found to be the best, consequently, the researchers divided quality of life into four categories according to the nurses' response probability map of each item of the EQ-5D-3L scale. These categories were named low-level groups, pain and discomfort group, medium-level group, and high-level group; each group accounted for 2.8%, 7.6%, 47.1%, and 42.5%, respectively, among which the middle- and high-level groups were the majority groups. In addition, the pain symptoms of nurses in each group were more apparent than other symptoms, which may be related to the high work intensity and heavy workload of nurses (24, 25). The results suggest that nursing managers should pay attention to the quality of life and work intensity of nurses and take appropriate timely intervention measures to improve the pain symptoms of clinical nurses.
4.3 Attention should be paid to low quality-of-life groups
Compared to the nurses in the high-level group, younger age, working in obstetrics and gynecology, and poor emotional state were quality-of-life risk factors for the nurses in the low-level group, while higher health scores and non-smoking were quality-of-life protective factors for the nurses in the low-level group.
Study have shown that an increase in years of working experience results in employees having strong professional technical abilities, rich knowledge, strong economic strength, and social status (26). Consequently, the level of supervisor happiness is high and the quality of life is better (27), which is consistent with this study's results. Compared to the high-level group, obstetrics and gynecology nurses were 6.45 times more likely to experience a lower quality of life. A possible reason is that the work of obstetrics and gynecology nurses is centered on the puerpera, and the time of puerpera's labor has no rules (28). Consequently, nurses often need to participate in emergency treatment and surgery (29). Therefore, the requirements of obstetrics and gynecology nurses are relatively high. In addition, it is common for obstetrics and gynecology nurses to work overtime. The significant amount of work consumes the obstetrics and gynecology nurses' energy, resulting in poor quality of life (30). Simultaneously, the quality of life of nurses with poor emotional states was lower, while the quality of life of nurses who did not drink alcohol and had a high level of health was higher, further verifying previous research results (27, 31). Therefore, the results suggest that clinical nursing managers should pay attention to low-level quality-of-life nurse groups, such as obstetrics and gynecology nurses with fewer working years.
4.4 Limitations
This study has some limitations. Firstly, although this study adopted a multistage stratified whole-group sampling method, the selection of primary hospitals was relatively large, and the representativeness was biased. Therefore, these conclusions should be further explored and tested continuously. Secondly, this study did not include interventional research or an assessment of the impact of psychotherapy or psychological interventions on nurses' quality of life. Considering the potential significance of these interventions, future research is needed to address this gap.
5 Conclusions
In this study, the quality of life levels of nurses in 12 hospitals in Shandong province was analyzed using latent class analysis, and the number of optimal model categories was fitted to four groups: low-level group, pain and discomfort group, medium-level group, and high-level group. The clinical characteristics of nurses in different groups were distinguished, and the probability of entering the low-level quality of life group was higher for younger nurses, who work in obstetrics and gynecology, and have poor emotional states than those entering the high-level group. This method sought to identify nursing staff with poorer quality of life in a more targeted manner and can provide an important reference basis for clinical interventions to improve nurses' quality of life.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Ethics Committee of the School of Public Health, Shandong University (approval number: 20181219).
Author contributions
YZ: Writing – original draft. BY: Data curation, Methodology, Software, Writing – original draft, Writing – review & editing. JC: Conceptualization, Formal analysis, Funding acquisition, Resources, Supervision, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was supported by Education and Teaching Reform Research Project of Shandong University, No. 2020Y236.
Acknowledgments
We would like to express our deepest gratitude to the directors of the hospital that hosted the study and to all the nursing staff who agreed to participate.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Han MA, Ryu SY, Park J, Kang MG, Park JK, Kim KS. Health-related quality of life assessment by the EuroQol-5D in some rural adults. J Prev Med Public Health. (2008) 41:173–80. doi: 10.3961/jpmph.2008.41.3.173
2. Calvert MJ, Freemantle N, Cleland JG. The impact of chronic heart failure on health-related quality of life data acquired in the baseline phase of the CARE-HF study. Eur J Heart Fail. (2005) 7:243–51. doi: 10.1016/j.ejheart.2005.01.012
3. Farhah N, Srinivasan S, Mital D, Coffman FD. The effect of socioeconomic factors on health-related quality of life among adults with depressive disorder in the USA. Int J Med Eng Inform. (2022) 14:229–239. doi: 10.1504/IJMEI.2022.122282
4. Govindaraju T, Mccaffrey TA, Mcneil JJ, Reid CM, Smith BJ, Campbell DJ, et al. Quality of life and associations with health-related behaviours among older adults with increased cardiovascular risk. Nutr Metab Cardiovasc Dis. (2022) 32:1146–53. doi: 10.1016/j.numecd.2022.01.025
5. Kagawa-Singer M, Padilla GV, Ashing-Giwa K. Health-related quality of life and culture. Semin Oncol Nurs. (2010) 26:59–67. doi: 10.1016/j.soncn.2009.11.008
6. Lebni JY, Toghroli R, Abbas J, Kianipour N, NeJhaddadgar N, Salahshoor MR, et al. Nurses' work-related quality of life and its influencing demographic factors at a public hospital in western Iran: a cross-sectional study. Int Q Community Health Educ. (2021) 42:37–45. doi: 10.1177/0272684X20972838
7. Sullivan D, White KM, Frazer C. Factors associated with burnout in the United States versus International nurses. Nurs Clin North Am. (2022) 57:29–51. doi: 10.1016/j.cnur.2021.11.003
8. Rahma M, Khu A, Girsang E, Silalahi M. Analysis of the influence of workload and the quality of the nurse with the quality of medical services in the inpatient building B general hospital Royal Prima Medan 2019. Int J Res Med Sci. (2021) 9:1. doi: 10.18203/2320-6012.ijrms20212359
9. Wang M, Hanges PJ. Latent class procedures: applications to organizational research. Organ Res Methods. (2011) 14:24–31. doi: 10.1177/1094428110383988
10. Janssen MF, Pickard AS, Golicki D, Gudex C, Niewada M, Scalone L, et al. Measurement properties of the EQ-5D-5L compared to the EQ-5D-3L across eight patient groups: a multi-country study. Qual Life Res. (2013) 22:1717–27. doi: 10.1007/s11136-012-0322-4
11. Zhuo L. A Study of modeling for European quality of life (EQ-5D-3L) value sets based on nationally representative sample of Chinese population. Nanjing Medical University. (2018).
12. Kessler RC, Andrews G, Colpe LJ, Hiripi E, Mroczek DK, Normand SL, et al. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol Med. (2002) 32:959–76. doi: 10.1017/S0033291702006074
13. Bu XQ, You LM, Li Y, Liu K, Zheng J, Yan TB, et al. Psychometric properties of the Kessler 10 scale in Chinese parents of children with cancer. Cancer Nurs. (2017) 40:297–304. doi: 10.1097/NCC.0000000000000392
14. Lin TH, Dayton CM. Model selection information criteria for non-nested latent class models. J Educ Behav Stat. (1997) 22:249–64. doi: 10.3102/10769986022003249
15. Muthén, LK, Muthén, BO. MPlus user's guide: the comprehensive modeling program for applied researchers. Muthén & Muthén. (2010) 1–758. Available at: https://www.mendeley.com/catalogue/99037498-9b82-3228-b7da-5c5cb8e05cc6/
16. Zhou ZL, Zhou ZY, Li D, Wang D, Shi C, Shen L, et al. Analyzing the health-related quality of life of urban and rural residents in Shaanxi: estimation based on the EQ-5D Value Set. Chin Health Econ. (2015) 34:13–16. doi: 10.7664/CHE20150202
17. Khatatbeh H, Pakai A, Al-Dwaikat T, Onchonga D, Amer F, Prémusz V, et al. Nurses' burnout and quality of life: a systematic review and critical analysis of measures used. Nurs Open. (2022) 9:1564–74. doi: 10.1002/nop2.936
18. Loisa E, Hoppu S, Hytönen SM, Tirkkonen J. Rapid response team nurses' attitudes and barriers to the rapid response system: a multicentre survey. Acta Anaesthesiol Scand. (2021) 65:695–701. doi: 10.1111/aas.13779
19. Dean E. RCN's gender report highlights reasons for poor pay - An RCN report on why nurses have been historically underpaid calls for fairer and more realistic job evaluation frameworks. Nurs Manage. (2020) 27:8. doi: 10.7748/nm.27.1.8.s7
20. Jiao M, Ning N, Li Y, Gao L, Cui Y, Sun H, et al. Workplace violence against nurses in Chinese hospitals: a cross-sectional survey. BMJ Open. (2015) 26:e006719. doi: 10.1136/bmjopen-2014-006719
21. Zeng HJ, Zhou GY, Yan HH, Yang XH, Jin HM. Chinese nurses are at high risk for suicide: a review of nurses suicide in China 2007-2016. Arch Psychiatr Nurs. (2018) 32:896–900. doi: 10.1016/j.apnu.2018.07.005
22. Hong KJ, Cho SH. Effort-reward imbalance and its effects on satisfaction with working conditions and sleep-related problems: comparison of nurses and other occupations. J Nurs Scholarsh. (2021) 53:595–603. doi: 10.1111/jnu.12666
23. Tian M, Yang H, Yin X, Wu Y, Zhang G, Lv C, et al. Evaluating effort-reward imbalance among nurses in emergency departments: a cross-sectional study in China. BMC Psychiatry. (2021) 14:353. doi: 10.1186/s12888-021-03344-6
24. Hosseini E, Daneshmandi H, Bashiri A, Sharifian R. Work-related musculoskeletal symptoms among Iranian nurses and their relationship with fatigue: a cross-sectional study. BMC Musculoskelet Disord. (2021) 22:629. doi: 10.1186/s12891-021-04510-3
25. Zuazua-Rico D, Mosteiro-Diaz MP, Maestro-Gonzalez A, Fernandez-Garrido J. Nursing workload, knowledge about pain, and their relation to pain records. Pain Manag Nurs. (2020) 21:510–5. doi: 10.1016/j.pmn.2020.03.009
26. Martinez MC, Fischer FM. Work ability and job survival: four-year follow-up. Int J Environ Res Public Health. (2019) 16:3143. doi: 10.3390/ijerph16173143
27. Dolan SL, García S, Cabezas C, Tzafrir SS. Predictors of “quality of work” and “poor health” among primary health-care personnel in Catalonia: evidence based on cross-sectional, retrospective and longitudinal design are personnel in Catalonia. Int J Health Care Qual Assur. (2008) 21:203–18. doi: 10.1108/09526860810859058
28. De la Fuente-Solana EI, Suleiman-Martos N, Velando-Soriano A, Cañadas-Dela Fuente GR, Herrera-Cabrerizo B, Albendín-García L. Predictors of burnout of health professionals in the departments of maternity and gynaecology, and its association with personality factors: a multicentre study. J Clin Nurs. (2021) 30:207–216. doi: 10.1111/jocn.15541
29. Veit-Rubin N, Brossard P, Gayet-Ageron A, Montandon CY, Simon J, Irion O, et al. Validation of an emergency triage scale for obstetrics and gynaecology: a prospective study. BJOG. (2017) 124:1867–73. doi: 10.1111/1471-0528.14535
30. Matlala MS, Lumadi TG. Perceptions of midwives on shortage and retention of staff at a public hospital in Tshwane District. Curationis. (2019) 42:e1–e10. doi: 10.4102/curationis.v42i1.1952
Keywords: nursing staff, quality of life, EQ-5D, latent class analysis, psychological distress
Citation: Zhao Y, Yang B and Chu J (2024) Latent class analysis for health-related quality of life in nurses in China. Front. Public Health 12:1433018. doi: 10.3389/fpubh.2024.1433018
Received: 15 May 2024; Accepted: 18 November 2024;
Published: 11 December 2024.
Edited by:
Marília Silva Paulo, Universidade Nova de Lisboa, PortugalReviewed by:
Yuke Tien Fong, Singapore General Hospital, SingaporeMassimo Tusconi, University of Cagliari, Italy
Copyright © 2024 Zhao, Yang and Chu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jianying Chu, MTM5NTMxMTA1NTdAMTM5LmNvbQ==
†These authors share first authorship