
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 26 July 2024
Sec. Aging and Public Health
Volume 12 - 2024 | https://doi.org/10.3389/fpubh.2024.1429244
This article is part of the Research TopicEffects of Aging on Skeletal MuscleView all 10 articles
 Lihan Xu1
Lihan Xu1 Haojing Zhou2*
Haojing Zhou2*Background: The relationship between the weight-adjusted-waist index (WWI) and grip strength, a crucial marker in assessing sarcopenia, lacks clarity. We aimed to explore the relationship between WWI and muscle strength across genders.
Methods: The cross-sectional study involved adults with complete data on WWI and grip strength from the 2011–2014 National Health and Nutrition Examination Survey. WWI was derived by dividing waist circumference by the square root of weight. Weighted multivariable logistic regression and smooth curve fitting techniques were used to examine the independent association and potential non-linear relationship between WWI and grip strength. A two-piecewise linear regression model was utilized to determine the threshold effect. Additionally, subgroup analyses and interaction tests were conducted.
Results: The study encompassed 9,365 participants, including 4,661 males and 4,704 females. Multivariate logistic regression analysis revealed a negative correlation between WWI and grip strength among males (β = −11.49, 95% CI: −12.38, −10.60, p < 0.001) as well as females (β = −2.53, 95% CI: −2.98, −2.08, p < 0.001). Subgroup analysis showed that the negative correlation of WWI with grip strength remained consistent across various age groups and levels of obesity for both males and females.
Conclusion: An increase in WWI correlates with reduced muscle strength in both males and females. WWI was negatively associated not only with muscle mass but also with muscle strength. WWI may serve as an assessment tool for sarcopenia, but further large-scale studies are needed to clarify causality.
Sarcopenia is delineated as the gradual and progressive reduction in skeletal muscle mass and strength, often accompanied by a decline in physical function (1, 2). This condition stands as a significant aging-related syndrome, independently foretelling multiple clinically consequential adverse outcomes, encompassing an elevated susceptibility to fractures, reduced quality of life, impaired mobility, and heightened mortality rates (3–5). In Asian countries, the prevalence of sarcopenia varies between 5.5 and 25.7%, with a higher occurrence among males (5.1–21.0% in male compared to 4.1–16.3% in female), leading to significant socioeconomic implications (6, 7). Throughout the revision of sarcopenia guidelines, there is an increased emphasis on muscle strength. This shift stems from the acknowledgment that, in anticipating negative outcomes, muscle strength surpasses muscle mass in predictive accuracy (1, 8). Grip strength, acknowledged as a dependable proxy for overall muscle strength, has garnered considerable attention in numerous guidelines as a pivotal marker for assessing and diagnosing sarcopenia (1, 7, 9).
The weight-adjusted-waist index (WWI) is a recently introduced anthropometric measure derived by standardizing waist circumference (WC) to body weight, computed as the WC in centimeters divided by the square root of weight in kilograms (10). Similar to body mass index (BMI), a higher WWI score signifies increased levels of obesity. Previous studies demonstrated an independent association between WWI and sarcopenic obesity in specific populations like type 2 diabetes mellitus patients and males undergoing maintenance hemodialysis (11, 12). Notably, WWI exhibits a stronger correlation with sarcopenic obesity in older men compared to other anthropometric indices such as waist-to-height ratio, BMI, and WC (13).
Previous studies have demonstrated an inverse correlation between WWI and both appendicular lean mass and abdominal muscle mass among middle-aged and older adult populations (14–16). The association between WWI and sarcopenia has been initially explored. However, the association between WWI and grip strength, a crucial component in assessing sarcopenia, lacks clarity.
The objectives of this study are as follows: Firstly, it aims to investigate the relationship between WWI and grip strength in the adult population. Secondly, the study aims to explore the potential of WWI as a predictive indicator for sarcopenia. It is assumed that there exists a negative correlation between WWI and grip strength.
Data were sourced from National Health and Nutrition Examination Survey (NHANES), a nationally conducted cross-sectional survey aimed at gathering information on potential health risk factors and the nutritional status of non-institutionalized civilians in the United States, conducted by the National Center for Health Statistics. A complex, stratified, multistage probability cluster sampling design was employed to obtain a representative sample of the entire the United States population (17). The NHANES study protocols were sanctioned by the Research Ethics Review Board of the NCHS. Written informed consent was acquired from all survey participants or from a parent/legal guardian for those under 16 years of age. Comprehensive details regarding the NHANES study design and data can be accessed publicly at https://www.cdc.gov/nchs/nhanes/.
Our study utilized data from the NHANES survey cycles spanning 2011 to 2014, as only these cycles encompassed information on grip strength and WWI. Initially, 19,932 participants were enrolled; however, following the exclusion of those lacking grip strength data (n = 5,191), missing WWI data (n = 561), and those under 20 years of age (n = 4,815), our final analysis comprised 9,365 participants. The cohort consisted of 4,661 males and 4,704 females (Figure 1).
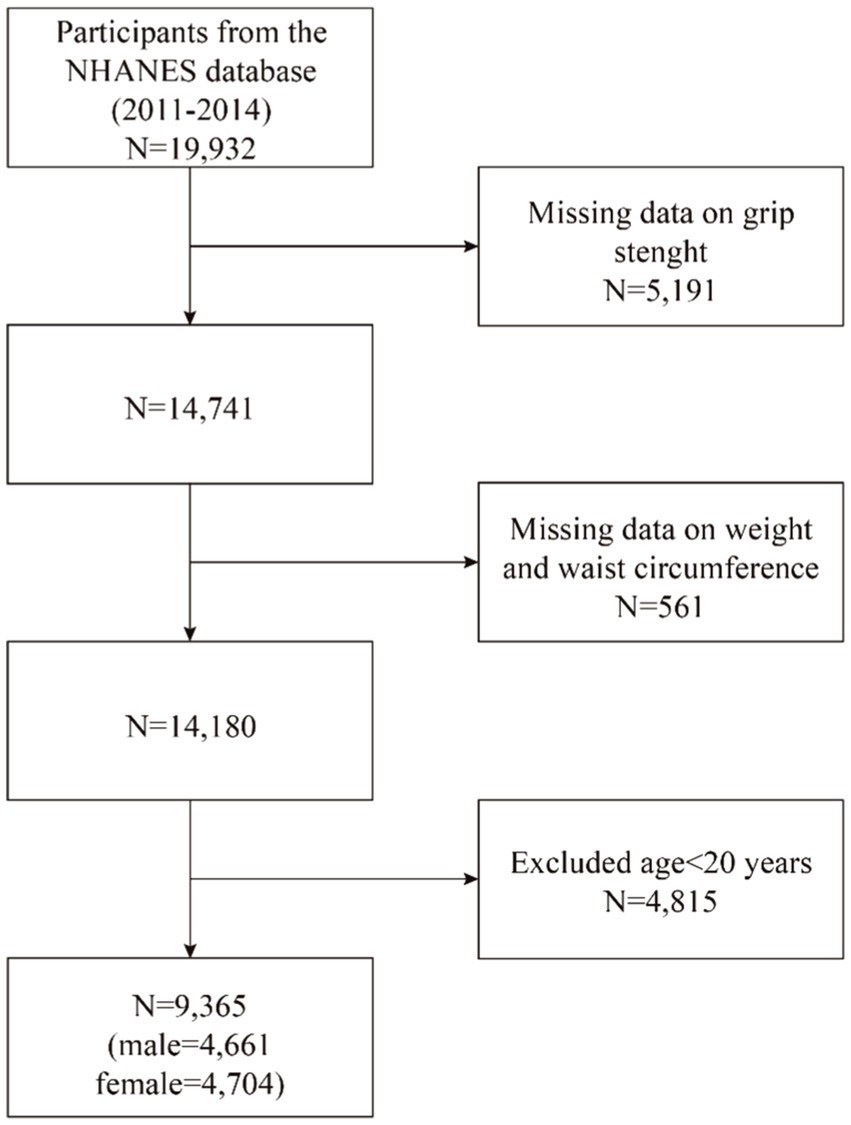
Figure 1. Flowchart of population included in our final analysis.
The WWI, an anthropometric index combining WC and weight, serves as an estimation tool for obesity. A higher WWI score indicates a higher level of obesity. Body measurement data pertaining to WC and weight were gathered within the mobile examination center by proficient health technicians. The WWI for each participant was computed as the WC in centimeters divided by the square root of weight in kilograms, rounded to two decimal places. In our analysis, we regarded WWI as a continuous variable, subsequently grouping participants according to WWI quartiles for further investigation. WWI was utilized as an exposure variable in our study.
Grip strength measurements were conducted during the NHANES 2011–2014 survey, following the protocol specified for that period. The assessment of grip strength adhered to the guidelines outlined in the Muscle Function Procedures Manual and utilized the Takei Digital Grip Strength Dynamometer, Model T.K.K.5401 (Takei Scientific Instruments Co., Niigata, Japan). Beforehand, the dynamometer was adjusted to fit each participant’s hand size while they stood with their arm straight down and wrist in a neutral position. Participants were instructed to exert maximum force while squeezing the dynamometer using one hand, repeating the test three times on alternate hands with a 60-s interval between measurements of the same hand. The NHANES recorded the combined handgrip strength by summing the highest readings from each hand, expressed in kilograms.
Our study incorporated covariates that might influence the relationship between WWI and grip strength. These included gender (male/female), age (year), race (non-Hispanic White/non-Hispanic Black/Mexican American/other races), education level (less than high school/high school/more than high school), height (cm), weight (kg), BMI (kg/m2), WC (cm), intake of energy (kcal/day), intake of protein (gm/day), smoking status (yes/no), alcohol status (yes/no), hypertension (yes/no), diabetes (yes/no) and hypercholesterolemia (yes/no). Energy and protein intake were calculated by averaging the intake across day 1 and day 2. Smoking status was determined based on whether one had smoked at least 100 cigarettes in life. Participants who had at least 12 alcohol drinks per year were considered drinkers. Hypertension, diabetes, and hypercholesterolemia were identified based on self-reported diagnoses of these conditions. Subgroup analysis categorized BMI as <25, 25–29.9, and ≥30 kg/m2, representing normal weight, overweight, and obese categories, respectively, for the participants. Further details were accessible at www.cdc.gov/nchs/nhanes.
The statistical analyses adhered to Centers for Disease Control and Prevention guidelines, and an adjusted NHANES sampling weight was utilized, considering the intricate multistage cluster survey design during analysis. Significant disparities in grip strength were observed between male and female (18). Consequently, this study was segregated into male and female groups to investigate the correlation between WWI and grip strength. Continuous variables were expressed as mean ± standard deviation, while categorical variables were displayed as percentages. Group differences based on WWI quartiles were assessed using either a weighted Student’s t-test (for continuous variables) or a weighted chi-square test (for categorical variables). Three models of multivariable logistic regression were employed to assess the association between WWI and grip strength. In model 1, no covariates were adjusted. In model 2, age, race, and education level were adjusted. Model 3 was adjusted for age, race, education level, BMI, intake of energy, intake of protein, smoking status, alcohol status, hypertension, diabetes, and hypercholesterolemia. Subgroup analyses examining the associations between WWI and grip strength were performed, stratified by gender (male/female), age groups (20–39/40–59/≥60 years), and BMI categories (normal weight/overweight/obesity). These stratified factors were considered as predetermined potential effect modifiers. An interaction term was introduced to assess the diversity of associations among the subgroups. Additionally, smooth curve fittings were employed to identify potential non-linear relationships between WWI and grip strength, and a two-piecewise linear regression model was employed to further explore their threshold effects. Missing values for continuous variables were imputed using the mean, and for categorical variables, the mode was used, limited to existing cases of those variables. All analyses were performed using R version 3.4.3 (http://www.R-project.org, The R Foundation) and Empower software (www.empowerstats.com; X&Y solutions, Inc., Boston, MA). Statistical significance was set at a two-sided p-value <0.05.
The demographic characteristics of the study cohort categorized by gender-specific quartiles of WWI were presented in Tables 1, 2. Among males, the mean WWI was 10.82 ± 0.81, with quartile ranges of 8.37–10.25, 10.25–10.82, 10.82–11.39, and 11.39–14.79 for Quartiles 1 through 4, respectively. Grip strength exhibited a mean of 87.23 ± 18.92 kg, with values of 95.79 ± 17.45, 90.86 ± 16.98, 85.30 ± 17.62, and 76.98 ± 18.29 kg for Quartiles 1, 2, 3, and 4, respectively. Among females, the mean WWI was 11.22 ± 0.83, with quartile ranges of 8.38–10.63, 10.63–11.20, 11.20–11.79, and 11.79–14.20 for Quartiles 1 through 4, respectively. Grip strength exhibited a mean of 55.63 ± 11.92 kg, with values of 59.52 ± 10.64, 57.33 ± 11.39, 54.85 ± 11.55, and 50.84 ± 12.27 kg for Quartiles 1, 2, 3, and 4, respectively.
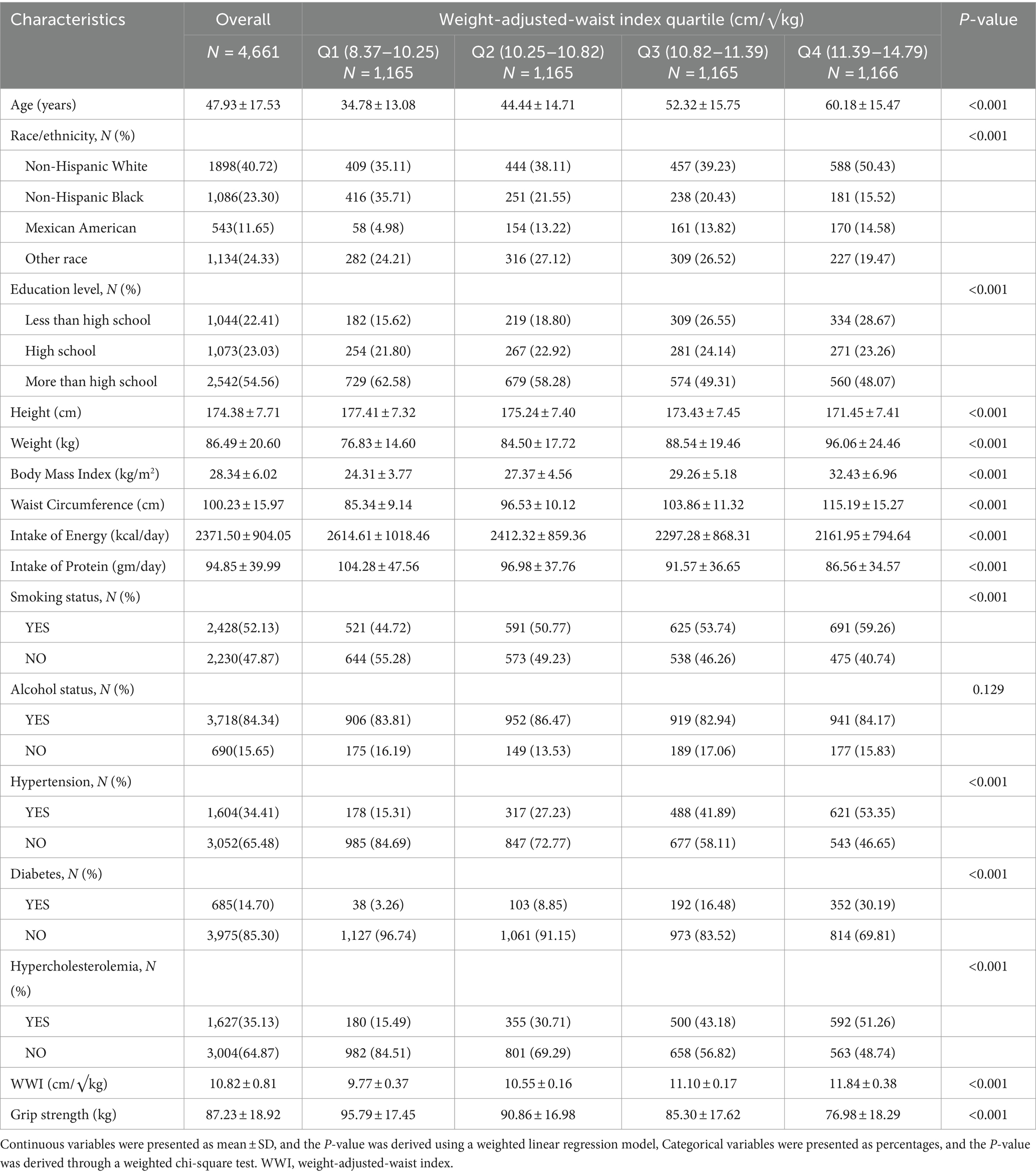
Table 1. Basic characteristics of participants by WWI quartile in male.
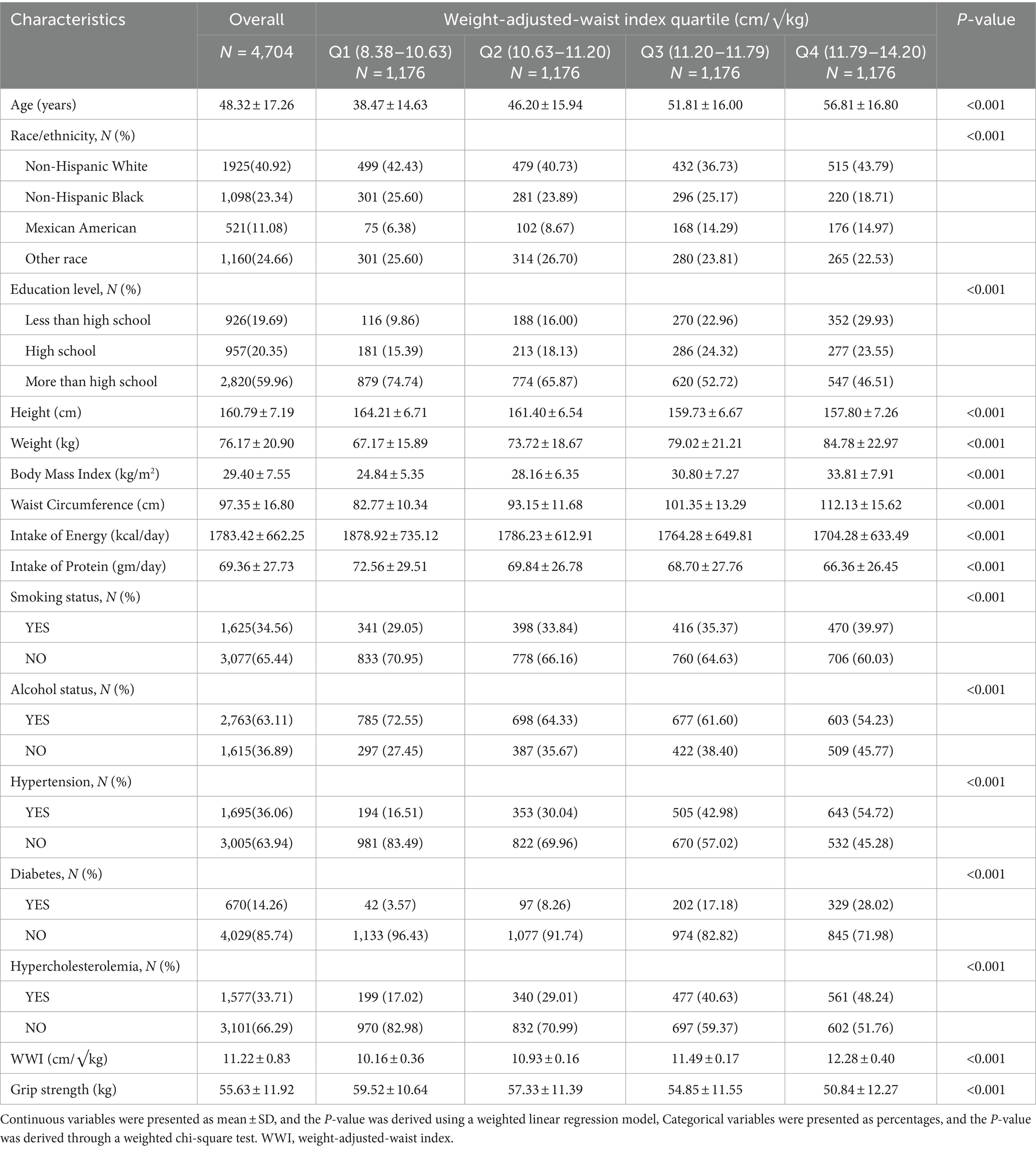
Table 2. Basic characteristics of participants by WWI quartile in female.
Table 3 illustrated the relationship between WWI and grip strength in males and females using three weighted generalized linear regression models. In the fully adjusted model (Model III), a negative correlation between WWI and grip strength was evident in males (β = −11.49, 95% CI: −12.38, −10.60, p < 0.001). Similarly, females displayed a negative correlation between WWI and grip strength (β = −2.53, 95% CI: −2.98, −2.08, p < 0.001). Regardless of gender, compared to the lowest quartile of WWI, the second, third, and fourth quartiles of WWI exhibited a statistically significant association with grip strength (Male: Q2: β = −4.24, 95% CI: −5.59, −2.89, p < 0.001; Q3: β = −9.35, 95% CI: −10.91, −7.80, p < 0.001; Q4: β = −19.84, 95% CI: −21.72, −17.96, p < 0.001; Female: Q2: β = −1.25, 95% CI: −2.06, −0.45, p = 0.002; Q3: β = −2.33, 95% CI: −3.22, −1.45, p < 0.001; Q4: β = −5.18, 95% CI: −6.18, −4.18, p < 0.001). Sensitivity analysis confirmed this trend (p for trend <0.001).
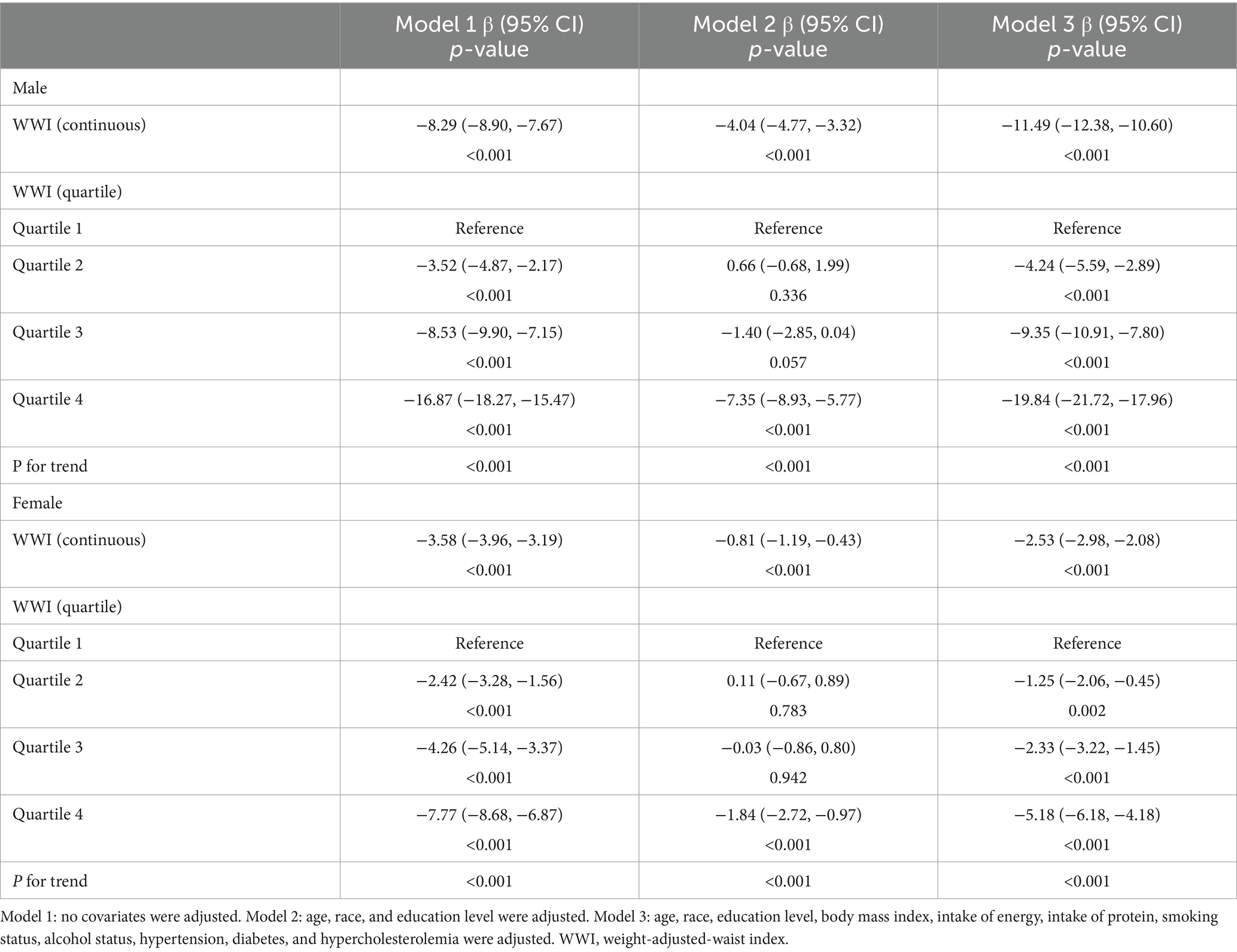
Table 3. The associations between WWI and grip strength.
To investigate the relationship between WWI and grip strength in the general population, subgroup analyses and interaction tests were conducted based on age and BMI for both males and females (Table 4). In males, the negative correlation between WWI and grip strength endured across all age groups. When stratified by BMI, the negative relationship between WWI and grip strength remained consistent across the normal weight, overweight, and obese populations. Similarly, in females, the negative correlation between WWI and grip strength was stable across different age groups and levels of obesity. Interaction analyses indicated that in females, the association between WWI and grip strength was influenced by BMI rather than age, while in males, neither age nor BMI appeared to affect this association.
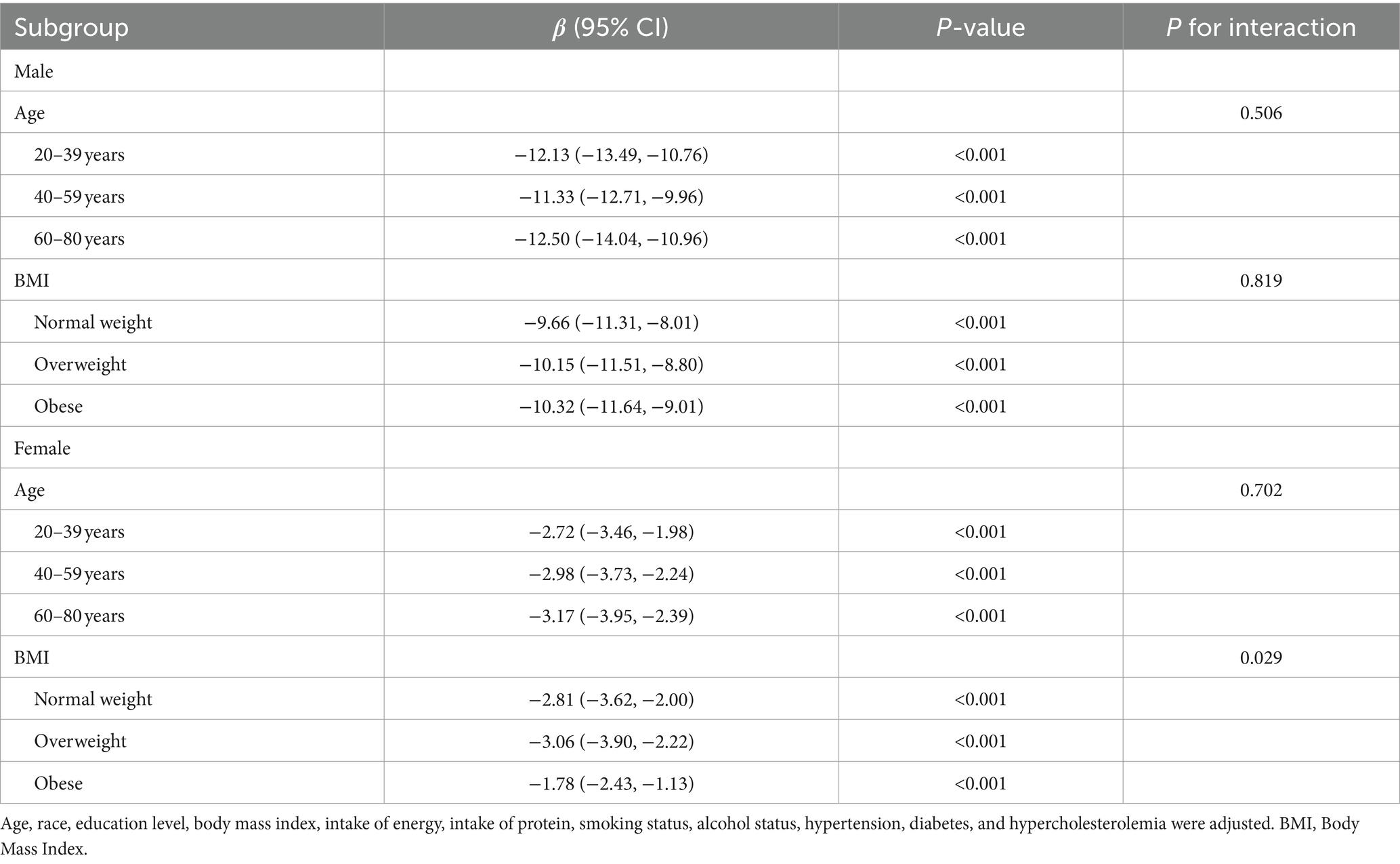
Table 4. Subgroup analysis of the association between WWI and grip strength.
As depicted in Figure 2, a non-linear inverse relationship between WWI and grip strength was observed in both males and females. Table 5 illustrated that the inflection points (K), determined through the two-piecewise linear regression model, were calculated at 10.83 for males and 11.43 for females. Both genders exhibited a significant negative correlation between WWI and grip strength on either side of the inflection point. Among males, on the left side of the inflection point, a unit increased in WWI corresponded to a reduction of grip strength by 7.59 kg, while on the right side, each unit rose in WWI resulted in a decrease of grip strength by 15.16 kg. Similarly, among females, on the left side of the inflection point, a unit increased in WWI corresponded to a reduction of grip strength by 1.45 kg, and on the right side, each unit rose in WWI led to a decrease of grip strength by 4.18 kg. Both groups exhibited logarithmic likelihood ratio test p-values <0.001.
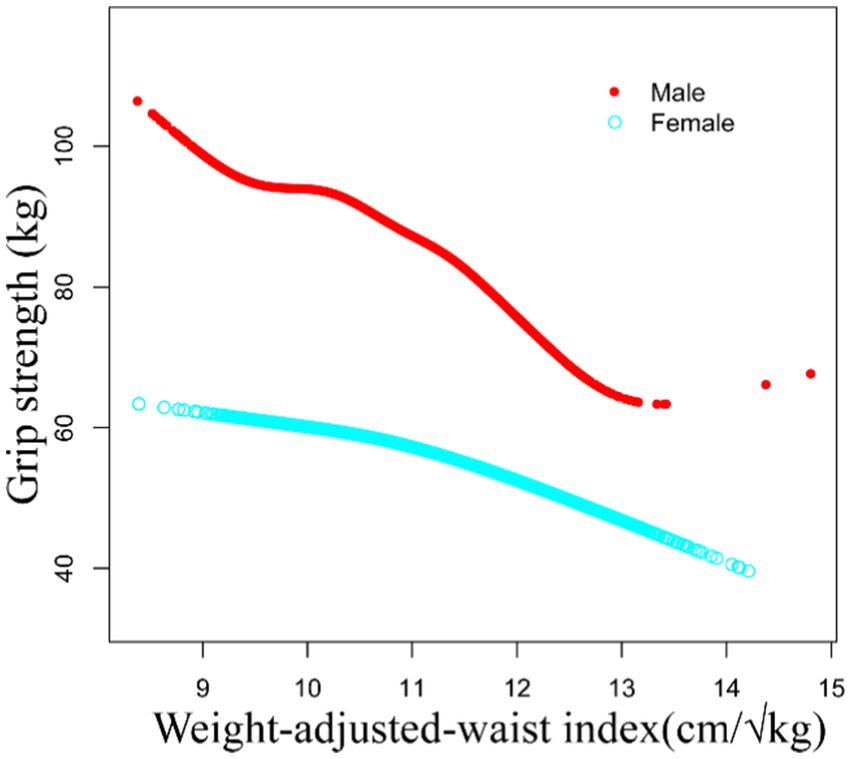
Figure 2. The non-linear associations between WWI and grip strength.
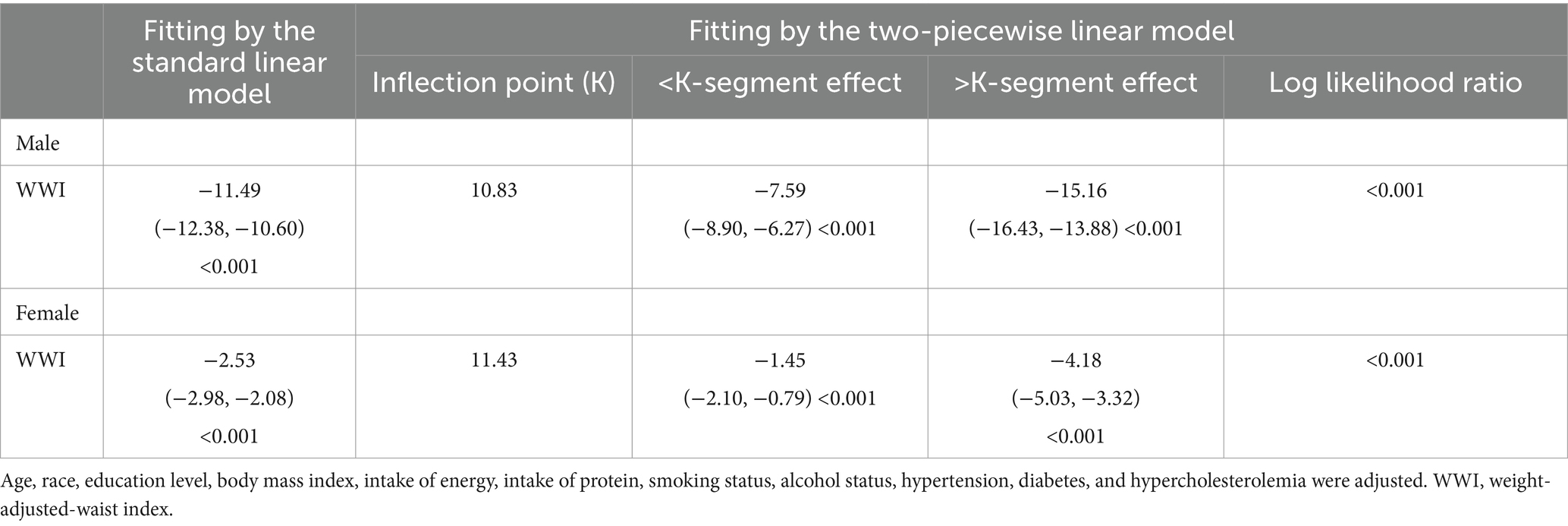
Table 5. Threshold effect analysis of WWI on grip strength using a two-piecewise linear regression model.
The objective of this study was to assess the correlation between WWI and grip strength. In our cross-sectional analysis encompassing 4,661 male and 4,704 female, a notable adverse correlation between WWI and grip strength was observed. This correlation persisted even subsequent to adjustments for all potential confounding variables. Subgroup analysis showed that the negative correlation of WWI with grip strength remained consistent across various age groups and levels of obesity for both males and females. Our findings indicated a negative association between WWI and grip strength in the adult population of the United States, which held true across various age groups and levels of obesity.
To our knowledge, this study was the inaugural exploration into the association between WWI and muscle strength. The diagnostic criteria for sarcopenia, as proposed by the European Working Group on Sarcopenia in Older People, comprise three elements: low muscle strength, low physical performance and low muscle mass (1). Prior investigations have shown an inverse relationship between WWI and both abdominal muscle mass and appendicular lean mass in middle-aged and older adult cohorts (14–16). However, no research has explicitly elucidated the correlation between WWI and muscle strength which is more associated with poor outcomes. This study filled this gap. Similar to muscle mass, our findings revealed a negative correlation between WWI and muscle strength.
The association between WWI and bone and muscle mass has been partially substantiated. Studies indicated a negative correlation between WWI and bone mineral density in the lumbar spine, pelvis, femoral neck, and total (19). And, previous research on WWI and muscle mass primarily concentrated on middle-aged and older adult individuals (14–16) and even people with characteristic diseases (11, 12), and noted gender disparities. However, through subgroup analysis, the correlation between WWI and muscle strength remained consistent across young, middle-aged, and older adults, encompassing both males and females. BMI stratification indicated that the negative correlation between WWI and grip strength applies consistently across different levels of obesity. The prevalence of obesity is rising worldwide (20). Data sourced from the World Health Organization indicates that 39% of the global adult population are overweight, of which 13% fall under the category of obesity, with a persistent increase in the count of obese individuals (21, 22). The relationship between WWI and grip strength also existed in the obese population. Given this context, WWI shows a growing potential to predict muscle strength.
The association between other obesity indices (BMI, body fat rate, waist-to-hip ratio) and muscle strength remained contentious. In several studies, conflicting results have emerged. Agtuahene et al. (23) showed a positive link between BMI and grip strength in youth, while Alahmari et al. (24) suggested no correlation between BMI and grip strength in grown men. Moreover, Siqueira revealed no substantial relationship between BMI and leg strength in active older adult individuals, except concerning grip strength (25). The sample sizes in these studies were relatively small, ranging from 64 to 304 participants. Nevertheless, a substantial cross-sectional study with a sample size exceeding 7,000 middle-aged individuals uncovered a positive association between BMI and grip strength (26). Variations in sample sizes and age group differences among the studies might explain these inconsistencies in research findings. In the context of body fat percentage, a comprehensive study revealed a positive correlation between body fat percentage and grip strength among middle-aged participants (26). Conversely, a separate study demonstrated a negative correlation between body fat percentage and abdominal strength. Notably, there was no observed correlation between waist-to-hip ratio and either grip strength or abdominal strength (26, 27).
However, as an index indicating increased obesity with higher values, BMI either lacks correlation or shows a positive one with muscle strength. Conversely, this study illustrated that WWI, also employed as an obesity indicator, displayed a negative correlation with muscle strength. The relationship between obesity and muscle is intricate. In the progression of obesity and muscle mass decline, a phenomenon of fat redistribution occurs. This presents as the transfer of fat from subcutaneous regions to the abdominal cavity (visceral fat) and its infiltration into muscles (28–30). This results in diminished muscle strength and functionality. Fat infiltration into muscles heightens the risk of advancing toward obesity, while obesity hampers muscle regeneration, initiating pre-sarcopenia. This synergistic interaction between muscle loss and fat infiltration could initiate and worsen sarcopenic obesity. While valuable for illustrating trends in obesity prevalence at a population level, BMI offers a rudimentary assessment of overall adiposity. Because BMI cannot differentiate between fat and muscle mass, the ratio of lean mass to fat mass may differ despite similar BMI values (31, 32). The reduction in muscle mass leading to weight loss is offset by an augmentation in visceral fat, leading to a circumstance wherein, despite diminished muscle strength, the BMI shows no alteration. This observation was also employed to elucidate the phenomenon of the obesity paradox (28, 31, 33). Additionally, the relocation of fat from subcutaneous to visceral areas does not necessarily imply weight gain, but it may enlarge WC (34), thus increasing WWI while BMI remains unchanged. This might be the reason behind the inconsistency in the correlation between WWI and BMI, two obesity indicators, with muscle strength.
The SARC-F scale is utilized for the identification of individuals potentially affected by sarcopenia. However, its sensitivity is limited, frequently resulting in the omission of certain patients (35). And the suggested techniques for assessing muscle strength and mass necessitate specialized tools such as computed tomography, magnetic resonance imaging, and ultrasound (1). Nevertheless, these methods entail substantial expenses and time commitments. The estimation of muscle strength and muscle mass without such specialized tools poses a challenge, and presently, no anthropometric index adequately reflects both these parameters. Previous studies and this study have demonstrated that WWI is correlated with both muscle strength and muscle mass. As a result, WWI holds promise as a simple screening tool for identifying sarcopenia or to complement the SARC-F scale for better detection of sarcopenia cases.
The study possesses several strengths. Primarily, it relied on NHANES data and conducted analyses while accounting for the appropriate NHANES sample weights. Secondly, we meticulously adjusted confounding covariates, enhancing the reliability of our results and their applicability to a broader spectrum of individuals. Nevertheless, the study also presents certain limitations. Initially, owing to the cross-sectional design, establishing a causal relationship was unattainable. Therefore, further prospective studies involving larger sample sizes remain imperative to elucidate causality. Furthermore, despite our adjustment for several potential covariates, the influence of other conceivable confounding factors could not be entirely ruled out.
Increased WWI correlated with reduced muscle strength in both male and female. As the WWI index rises, the strength of this negative correlation intensifies. The negative correlation of WWI with grip strength remained consistent across various age groups and levels of obesity. WWI may serve as an assessment tool for sarcopenia. Nonetheless, additional large-scale prospective studies are required to elucidate the precise causal link in this association.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
The studies involving humans were approved by Research Ethics Review Board of the National Center for Health Statistics. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
LX: Conceptualization, Data curation, Investigation, Methodology, Software, Supervision, Writing – original draft, Writing – review & editing. HZ: Formal analysis, Funding acquisition, Project administration, Resources, Validation, Visualization, Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
We would like to thank all participants in this study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
WWI, Weight-adjusted-waist index; WC, Waist circumference; BMI, Body mass index; NHANES, National Health and Nutrition Examination Survey.
1. Cruz-Jentoft, AJ, Bahat, G, Bauer, J, Boirie, Y, Bruyère, O, Cederholm, T, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. (2019) 48:16–31. doi: 10.1093/ageing/afy169
2. Cruz-Jentoft, AJ, and Sayer, AA. Sarcopenia. Lancet. (2019) 393:2636–46. doi: 10.1016/S0140-6736(19)31138-9
3. Zhang, Y, Hao, Q, Ge, M, and Dong, B. Association of sarcopenia and fractures in community-dwelling older adults: a systematic review and meta-analysis of cohort studies. Osteoporos Int. (2018) 29:1253–62. doi: 10.1007/s00198-018-4429-5
4. Beaudart, C, Demonceau, C, Reginster, JY, Locquet, M, Cesari, M, Cruz Jentoft, AJ, et al. Sarcopenia and health-related quality of life: a systematic review and meta-analysis. J Cachexia Sarcopenia Muscle. (2023) 14:1228–43. doi: 10.1002/jcsm.13243
5. Yuan, S, and Larsson, SC. Epidemiology of sarcopenia: prevalence, risk factors, and consequences. Metabolism. (2023) 144:155533. doi: 10.1016/j.metabol.2023.155533
6. Shafiee, G, Keshtkar, A, Soltani, A, Ahadi, Z, Larijani, B, and Heshmat, R. Prevalence of sarcopenia in the world: a systematic review and meta-analysis of general population studies. J Diabetes Metab Disord. (2017) 16:21. doi: 10.1186/s40200-017-0302-x
7. Chen, LK, Woo, J, Assantachai, P, Auyeung, TW, Chou, MY, Iijima, K, et al. Asian working Group for Sarcopenia: 2019 consensus update on sarcopenia diagnosis and treatment. J Am Med Dir Assoc. (2020) 21:300–7.e2. doi: 10.1016/j.jamda.2019.12.012
8. Cruz-Jentoft, AJ, Baeyens, JP, Bauer, JM, Boirie, Y, Cederholm, T, Landi, F, et al. Sarcopenia: European consensus on definition and diagnosis: report of the European working group on sarcopenia in older people. Age Ageing. (2010) 39:412–23. doi: 10.1093/ageing/afq034
9. Dent, E, Morley, JE, Cruz-Jentoft, AJ, Arai, H, Kritchevsky, SB, Guralnik, J, et al. International clinical practice guidelines for sarcopenia (ICFSR): screening, diagnosis and management. J Nutr Health Aging. (2018) 22:1148–61. doi: 10.1007/s12603-018-1139-9
10. Park, Y, Kim, NH, Kwon, TY, and Kim, SG. A novel adiposity index as an integrated predictor of cardiometabolic disease morbidity and mortality. Sci Rep. (2018) 8:16753. doi: 10.1038/s41598-018-35073-4
11. Park, MJ, Hwang, SY, Kim, NH, Kim, SG, Choi, KM, Baik, SH, et al. A novel anthropometric parameter, weight-adjusted waist index represents Sarcopenic obesity in newly diagnosed type 2 diabetes mellitus. J Obes Metab Syndr. (2023) 32:130–40. doi: 10.7570/jomes23005
12. Tian, M, Lan, Q, Yu, F, He, P, Hu, S, and Zha, Y. Sex differences in the Association of Weight-Adjusted-Waist Index with Sarcopenic obesity: a cross-sectional study of hemodialysis patients. Metab Syndr Relat Disord. (2023) 21:596–602. doi: 10.1089/met.2023.0149
13. Kim, JE, Choi, J, Kim, M, and Won, CW. Assessment of existing anthropometric indices for screening sarcopenic obesity in older adults. Br J Nutr. (2023) 129:875–87. doi: 10.1017/S0007114522001817
14. Kim, NH, Park, Y, Kim, NH, and Kim, SG. Weight-adjusted waist index reflects fat and muscle mass in the opposite direction in older adults. Age Ageing. (2021) 50:780–6. doi: 10.1093/ageing/afaa208
15. Kim, JY, Choi, J, Vella, CA, Criqui, MH, Allison, MA, and Kim, NH. Associations between weight-adjusted waist index and abdominal fat and muscle mass: multi-ethnic study of atherosclerosis. Diabetes Metab J. (2022) 46:747–55. doi: 10.4093/dmj.2021.0294
16. Kim, KJ, Son, S, Kim, KJ, Kim, SG, and Kim, NH. Weight-adjusted waist as an integrated index for fat, muscle and bone health in adults. J Cachexia Sarcopenia Muscle. (2023) 14:2196–203. doi: 10.1002/jcsm.13302
17. Curtin, LR, Mohadjer, LK, Dohrmann, SM, Kruszon-Moran, D, Mirel, LB, Carroll, MD, et al. National health and nutrition examination survey: sample design, 2007–2010. Vital Health Stat. (2013) 160:1–23.
18. Dodds, RM, Syddall, HE, Cooper, R, Benzeval, M, Deary, IJ, Dennison, EM, et al. Grip strength across the life course: normative data from twelve British studies. PLoS One. (2014) 9:e113637. doi: 10.1371/journal.pone.0113637
19. Zhang, Y, Wu, H, Li, C, Liu, C, Liu, M, Liu, X, et al. Associations between weight-adjusted waist index and bone mineral density: results of a nationwide survey. BMC Endocr Disord. (2023) 23:162. doi: 10.1186/s12902-023-01418-y
20. Anderson, MR, and Shashaty, MGS. Impact of obesity in critical illness. Chest. (2021) 160:2135–45. doi: 10.1016/j.chest.2021.08.001
21. Wong, MCS, Huang, J, Wang, J, Chan, PSF, Lok, V, Chen, X, et al. Global, regional and time-trend prevalence of central obesity: a systematic review and meta-analysis of 13.2 million subjects. Eur J Epidemiol. (2020) 35:673–83. doi: 10.1007/s10654-020-00650-3
22. Silva, L, Oliveira, MM, Stopa, SR, Gouvea, E, Ferreira, KRD, Santos, RO, et al. Temporal trend of overweight and obesity prevalence among Brazilian adults, according to sociodemographic characteristics, 2006-2019. Epidemiol Serv Saude. (2021) 30:e2020294. doi: 10.1590/s1679-49742021000100008
23. Agtuahene, MA, Quartey, J, and Kwakye, S. Influence of hand dominance, gender, and body mass index on hand grip strength. S Afr J Physiother. (2023) 79:1923. doi: 10.4102/sajp.v79i1.1923
24. Alahmari, KA, Silvian, SP, Reddy, RS, Kakaraparthi, VN, Ahmad, I, and Alam, MM. Hand grip strength determination for healthy males in Saudi Arabia: a study of the relationship with age, body mass index, hand length and forearm circumference using a hand-held dynamometer. J Int Med Res. (2017) 45:540–8. doi: 10.1177/0300060516688976
25. Siqueira, V, Sebastião, E, Camic, CL, and Machado, DRL. Higher body mass index values do not impact physical function and lower-extremity muscle strength performance in active older individuals. Int J Exerc Sci. (2022) 15:330–40.
26. Cooper, R, Tomlinson, D, Hamer, M, and Pinto Pereira, SM. Lifetime body mass index and grip strength at age 46 years: the 1970 British cohort study. J Cachexia Sarcopenia Muscle. (2022) 13:1995–2004. doi: 10.1002/jcsm.12992
27. Arif, M, Gaur, DK, Gemini, N, Iqbal, ZA, and Alghadir, AH. Correlation of percentage body fat, waist circumference and waist-to-hip ratio with abdominal muscle strength. Healthcare. (2022) 10:2467. doi: 10.3390/healthcare10122467
28. Li, CW, Yu, K, Shyh-Chang, N, Jiang, Z, Liu, T, Ma, S, et al. Pathogenesis of sarcopenia and the relationship with fat mass: descriptive review. J Cachexia Sarcopenia Muscle. (2022) 13:781–94. doi: 10.1002/jcsm.12901
29. Hughes, VA, Roubenoff, R, Wood, M, Frontera, WR, Evans, WJ, and Fiatarone Singh, MA. Anthropometric assessment of 10-y changes in body composition in the older adult. Am J Clin Nutr. (2004) 80:475–82. doi: 10.1093/ajcn/80.2.475
30. Song, MY, Ruts, E, Kim, J, Janumala, I, Heymsfield, S, and Gallagher, D. Sarcopenia and increased adipose tissue infiltration of muscle in older adult African American women. Am J Clin Nutr. (2004) 79:874–80. doi: 10.1093/ajcn/79.5.874
31. Després, JP . Excess visceral adipose tissue/ectopic fat the missing link in the obesity paradox? J Am Coll Cardiol. (2011) 57:1887–9. doi: 10.1016/j.jacc.2010.10.063
32. Bosello, O, and Vanzo, A. Obesity paradox and aging. Eat Weight Disord. (2021) 26:27–35. doi: 10.1007/s40519-019-00815-4
33. Kalinkovich, A, and Livshits, G. Sarcopenic obesity or obese sarcopenia: a cross talk between age-associated adipose tissue and skeletal muscle inflammation as a main mechanism of the pathogenesis. Ageing Res Rev. (2017) 35:200–21. doi: 10.1016/j.arr.2016.09.008
34. Li, X, Katashima, M, Yasumasu, T, and Li, KJ. Visceral fat area, waist circumference and metabolic risk factors in abdominally obese Chinese adults. Biomed Environ Sci. (2012) 25:141–8. doi: 10.3967/0895-3988.2012.02.003
Keywords: cross-sectional studies, muscle strength, NHANES, obesity, sarcopenia, weight-adjusted-waist index
Citation: Xu L and Zhou H (2024) The association between weight-adjusted-waist index and muscle strength in adults: a population-based study. Front. Public Health. 12:1429244. doi: 10.3389/fpubh.2024.1429244
Edited by:
Craig Willis, University of Bradford, United KingdomReviewed by:
Anna Kęska, Józef Piłsudski University of Physical Education in Warsaw, PolandCopyright © 2024 Xu and Zhou. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Haojing Zhou, aGFvamluZ3owODI2QDEyNi5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.