 Betlihem Muche Engdyhu1
Betlihem Muche Engdyhu1 Kedir Abdela Gonete
Kedir Abdela Gonete Berhanu Mengistu
Berhanu Mengistu Netsanet Worku
Netsanet Worku- 1Department of Human Nutrition, Institute of Public Health, University of Gondar, Gondar, Ethiopia
- 2Caring Futures Institute, College of Nursing and Health Sciences, Flinders University, Adelaide, SA, Australia
Background: Disordered eating attitudes are characterized by abnormal beliefs, thoughts, and feelings regarding food and weight control. Dieting, intentional weight loss, and weight control affect 41–62% of girls worldwide. However, there is limited information related to disordered eating attitudes and associated factors among late adolescent girls in Ethiopia, including in the study area. Thus, the study aimed to assess disordered eating attitudes and associated factors among late adolescent girls in Gondar city, northwest Ethiopia.
Methods: For this community-based cross-sectional study, which was conducted from 26 June to 26 July 2022, in Gondar city, Ethiopia, 1,188 adolescent girls were included. Multistage stratified sampling followed by a systematic random sampling technique was applied to recruit participants for the study. Data were collected using an interviewer-administered questionnaire containing the Eating Attitudes Test-26 (EAT-26). Anthropometric measurements were also taken. Bivariable and multivariable logistic regressions were employed to identify factors associated with disordered eating attitudes. In the final model, variables with a p-value of < 0.05 were considered statistically significant.
Results: A total of 1,158 late adolescent girls (a response rate of 97.5%) participated in the study. The prevalence of disordered eating attitudes among late adolescent girls was 9.7% [95% confidence interval (CI): 7.96, 11.4%]. Having a mother who was unable to read and write [adjusted odds ratio (AOR): 3.88 (95% CI: 1.07, 14.11)], having a mother who could read and write [AOR: 4.31: (95% CI: 1.14, 16.24)], having a father who only attended primary school [AOR: 3.78 (95% CI: 1.33, 10.78)], having severe anxiety [AOR: 3.26 (95% CI: 1.42, 7.49)], and severe usage of social media [AOR: 2.80 (95% CI: 1.22, 6.46)] were factors significantly associated with disordered eating attitudes among late adolescent girls.
Conclusion: This study revealed that disordered eating attitudes among late adolescent girls were relatively high. The educational status of parents, anxiety, and severe usage of social media were positively associated with disordered eating attitudes. Therefore, nutritional education for parents of adolescents who are vulnerable to unhealthy behavior is imperative. The finding also implied the importance of an inclusive strategy to mitigate the emerging problem of targeting vulnerable groups.
Background
The recent economic and nutrition transitions documented in developing countries have been an entry point for behavioral changes (1). These changes are common across all age groups but are more pronounced among adolescents (2). In the period of adolescence, there is accelerated growth and development (3). There are also psychological and behavioral changes at this time, and adolescents become more self-conscious and critical of their bodies (4). Consequently, a disordered eating attitude (DEA) emerges (5, 6).
Disordered eating attitudes (DEAs) refer to disordered beliefs, thoughts, and feelings regarding food and weight control, which can occur as a part of an eating disorder (7). DEAs have a substantial effect on the eating practices of individuals. For example, individuals with DEAs engage in calorie restriction, dieting, extreme exercise, self-induced vomiting, and binge eating (8–10). They also involve in restrictive dieting or unhealthy weight and shape management (9). Dieting, intentional weight loss, and weight control affect 41–62% of girls worldwide and they have grown to be a significant public health problem (11).
Even though the disorder frequently occurs in developed countries, recent epidemiological data have revealed a rapid spread of the disorder in other parts of the world (12). Regardless of cultural and religious practices, an increasing number of individuals are engaging in unhealthy eating attitudes and behaviors (13). Additionally, it has been observed that female adolescents are disproportionately engaged in unhealthy weight control behaviors compared to their male counterparts (14).
In adolescent girls, DEA is the third most common disease, next to asthma and obesity (15). The prevalence of DEAs among late adolescent girls (15–19 years) varied from 16.2 to 42.7% in high-income countries (16–18), 4 to 48.9% in middle–upper income countries (19–23), and 24.7 to 31.5% in middle–lower income countries (24, 25). A recent study in Ethiopia also highlighted the existence of DEAs among female adolescents, which is in agreement with the study, where 5.98% of adolescent girls had DEAs (26). In addition, studies have documented that the problem is more prominent among female adolescents than among their male counterparts (26, 27).
A variety of sociodemographic factors have been linked to the rising prevalence of DEAs in adolescent girls. To illustrate, age, marital status of parents (unmarried), educational status of parents (low level) (17, 25, 26), peer pressure (28–30), family pressure (28, 29), family income (17, 29), and residency (17, 30) were found to be the predictors of DEAs among adolescent girls. Moreover, anxiety (18, 21), depression (21), body weight perception (overweight) (21, 25, 30, 31), being obese or overweight (19, 25, 30, 31), social media addiction (20, 30), low self-esteem (31, 32), and limited consumption of animal source food (19) were also positively associated with DEAs among adolescent girls.
In general, adolescent girls with DEAs are more likely to become stunted, which can result in low birth weight babies and obstetric complications, thus preserving the progress of malnutrition from generation to generation (33, 34). Adolescent girls with DEAs are also more likely to manifest fatigue, high blood pressure, reduced learning capacity, delayed sexual maturity, lack of concentration, poor school performance, low self-esteem, and sluggish growth (12).
In cognizance of the dire consequences of poor dietary intake during the period of adolescence, different policies, programs, and strategies have been enacted in Ethiopia to promote optimal nutrition (35). However, decision-makers have placed little focus on behavioral factors that affect optimal nutrition during the adolescent period. In light of this, devising and placing a policy that strives to ameliorate healthy food choices is of paramount importance for the less-empowered groups of the population. Given the dearth of empirical evidence on this issue, the current study hypothesized that the magnitude of DEAs among late adolescent girls (15–19 years) is on the rise, even in resource-limited areas, which owes much to social media use, anxiety, depression, and unhealthy food choices.
Thus, the objectives of this study were 2-fold. The first objective was to estimate the prevalence of DEAs among late adolescent females in Gondar city, Ethiopia, and the second objective was to identify factors associated with DEAs.
Methods
Study setting and period
A community-based cross-sectional study was conducted between 26 June and 26 July 2022 in Gondar city. Gondar city is one of the few historical and ancient cities in Ethiopia. It is located ~750 km from Addis Ababa, the capital city of Ethiopia. Based on the Central Statistical Agency (CSA) 2007 report, the estimated population size of the city during the study period was 454,045; out of which, 47,276 were late adolescent girls. Administratively, there were six sub-cities and 37 lowest administrative units (kebeles) in the city. The city had one comprehensive and specialized referral hospital, two general hospitals, and eight health centers.
Participants and sampling technique
All late adolescent girls who resided in Gondar city for at least 6 months were included in the study. The sample size was estimated using a single population proportion formula by considering 5.98% (26) of the proportion of DEAs among late adolescent girls at a 95% confidence interval (CI) with a 2% margin of error. Finally, after considering 10% contingency and a design effect of 2, 1,188 late adolescent girls were recruited for this study. Adolescent girls who were unable to respond due to illness were excluded.
A multistage sampling technique was used. First, two sub-cities were selected randomly using a lottery method from the six sub-cities in the city. Then, the final sample size was proportionated to the kebeles of the selected sub-cities. Finally, using a systematic random sampling technique, every 12th (k ≈ 14,200/1,188) household was employed. When there was more than one adolescent girl in a single household, the participant was randomly selected using the lottery method.
Data collection
A pretested interviewer-administered questionnaire was used. The data were collected by six trained B.Sc. nurses, and they were supervised by a public health officer. The first section of the questionnaire comprised sociodemographic variables (age, educational status, parents' occupation, family size, living status, and wealth status). Late adolescent girls were defined as those aged between 15 and 19 years. The wealth status was computed using principal component analysis (PCA), using 20 variables that were used to assess housing quality: roofing, walls, and floor material; toilet ownership; and the ownership of durable household tools: chair, table, sofa, mattress, mobile telephone, non-mobile telephone, television, radio, refrigerator, electric stove, bicycle, horse cart, Bajaj (a three-wheel vehicle), and car. These house facilities and durable goods and items were regarded as modern goods that reflected wealth status in urban areas. The responses were dichotomized, with zero indicating non-ownership of the item and one indicating ownership. Finally, they were categorized into poor, medium, and rich.
The second section of the questionnaire contained the Eating Attitudes Test-26 (EAT-26). The EAT has 26 items, each with six responses ranging from always to never. A score of 3 was given for always, 2 for very often, 1 for often, and 0 for occasionally, sometimes, and never. The scores were computed after summing up each response, which ranged from 0 to 78. Finally, adolescent girls who scored 20 and above were considered to have DEAs (26). The reliability of the tool was assessed using a Cronbach's alpha value of 0.70.
Social media usage was measured using the Internet Addiction Test (IAT). The IAT comprised 20-item questionnaires, with each item rated on a 6-point Likert scale (ranging from 0 to 5). The total score was computed; those with a score ranging from 0 to 30 were considered normal users, those with a score between 31 and 49 were considered mild social media users, those with a score between 50 and 79 were considered moderate social media users, and those with a score between 80 and 100 were considered severe social media users (36). The internal consistency (Cronbach's alpha) of the tool (IAT) in this study was 0.96.
The nine-item Patient Health Questionnaire (PHQ-9) was used to define depression among adolescent girls. The questionnaire had nine items with four responses (“not at all-0,” “several days-1,” “more than half of the days-2,” and “nearly every day-3”) for depressive symptoms in the past 2 weeks. The scores ranged from 0 to 27. Then, the scores were categorized into no depression (0–4), mild depression (5–9), moderate depression (10–14), moderately severe depression (15–19), and severe depression (20–27) (37–39). The item showed good internal consistency (Cronbach's alpha, 0.86).
Anxiety was measured using the seven-item General Anxiety Disorder-7 (GAD-7) questionnaire for adolescents. It assessed symptoms related to anxiety in the period of 2 weeks preceding the study. The questionnaire provided the following response options: “not at all-0,” “several days-1,” “over half the days-2,” and “nearly every day-3.” The scores varied between 0 and 21, with the following categories: minimal anxiety (0–4), mild anxiety (5–9), moderate anxiety (10–14), and severe anxiety (15–21) (40). The internal consistency (Cronbach's alpha) of the questionnaire in this study was 0.81.
Body weight perception was defined as the self-evaluation of one's weight as underweight, normal weight, overweight, and obese irrespective of the actual body weight (41).
The weight and height of adolescent girls were measured in accordance with the World Health Organization (WHO) guidelines. A calibrated weight scale was used to measure the weight to the nearest 100 g, and the height was measured to the nearest centimeter with the participant standing in the Frankfurt plane using a stadiometer. During the measurements, the participants did not wear heavy garments or footwears. The weight measuring scale was calibrated to zero from time to time. The AnthroPlus software was used to compute the body mass index (BMI) for the age of adolescent girls. In accordance with the WHO 2007 growth reference, the adolescents were classified as overweight (Z-score > +1 SD), normal weight (Z-score ≥ −2 SD and +1 SD), and thin (thin < −2 SD) (42).
Analysis
The data were checked for completeness and clarity. The data were then entered into EpiData 4.6, and statistical analysis was conducted using the Statistical Package for Social Sciences (SPSS) version 25. Descriptive statistics (frequency, percentage, median, and interquartile range) were used to summarize the data, and, figuratively, the findings were presented using tables. Multicollinearity between independent variables was checked using the variance inflation factor (VIF), and multicollinearity was not found (VIF < 10). Binary logistic regression was used to identify the independent predictors of DEAs. Variables with a p-value of < 0.2 in the bivariable logistic regression were considered for the final model. The strength of the association was assessed using a crude odds ratio (COR) and adjusted odds ratio (AOR) at 95% CI in the bivariable and multivariable models, respectively. In the final model, a p-value of < 0.05 was used to declare significance. The Hosmer–Lemeshow goodness-of-fit test was conducted to check the ability of the model to fit the data (p = 0.19).
Results
Sociodemographic and economic characteristics of respondents
In this study, 1,158 adolescent girls consented to participate, making the response rate 97.5%. The median age of adolescent girls was 17 ± 3 inter quantile range (IQR), and half (50.8%) of them were in the age group between 17 and 19 years. Almost half (47.3%) of them had completed their secondary school education. The majority (84.6%) had ≥5 family members. More than one-third (35.1%) were from rich households. Regarding the maternal characteristics of the study participants, the majority of them (83.7%) were married and more than one-third (36.4%) had completed their secondary school education (Table 1).
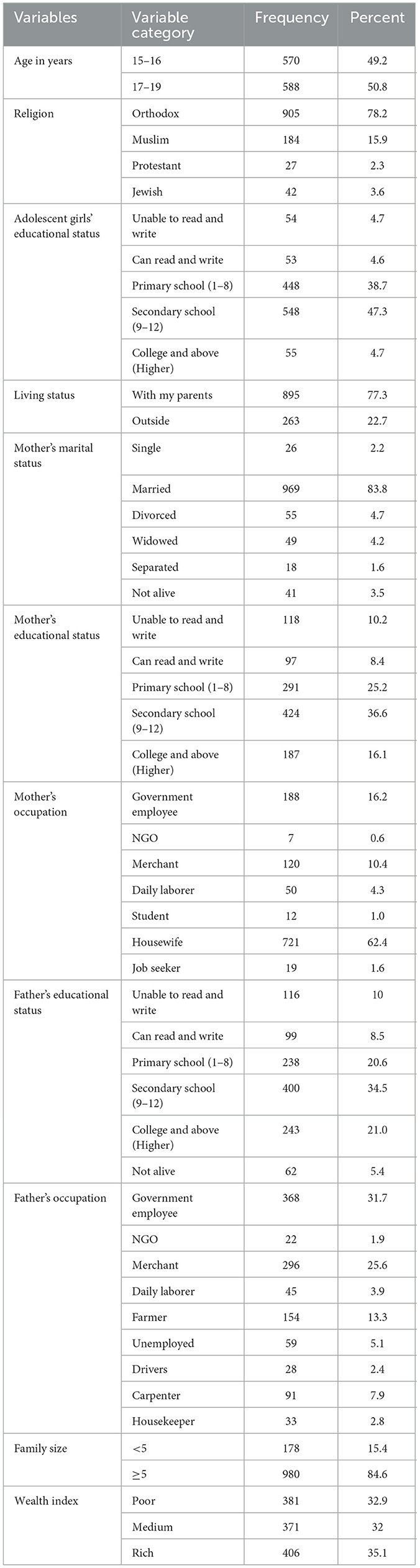
Table 1. Sociodemographic and economic characteristics of late adolescent girls in Gondar city, northwest Ethiopia, 2022 (n = 1,158).
Psychosocial and behavioral characteristics of respondents
In this study, two-fifths (41.3%) and almost two-thirds (28.2%) of adolescent girls had developed mild depression and severe anxiety, respectively. Furthermore, almost half (49%) of the girls perceived that their weight was normal (Table 2).
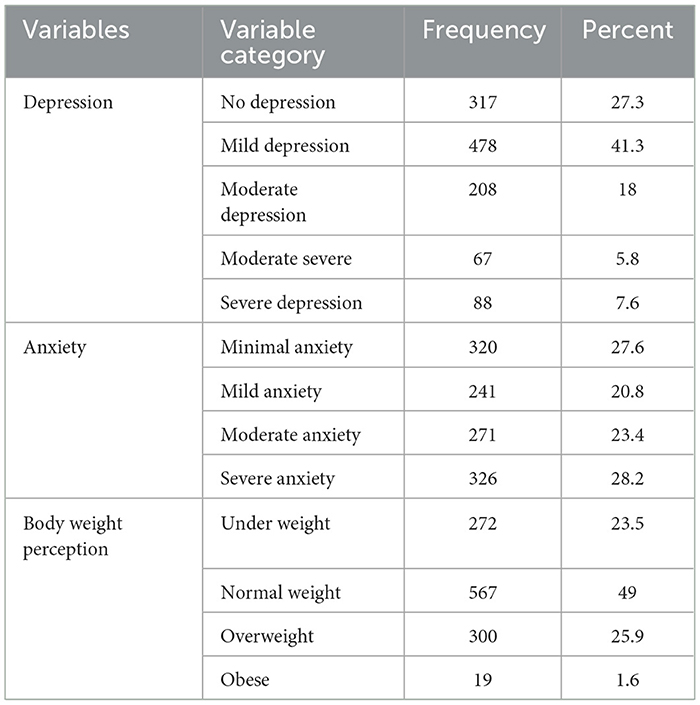
Table 2. Psychosocial and behavioral characteristics of late adolescent girls, Gondar city, northwest Ethiopia, 2022 (n = 1,158).
Social media and nutritional status
Of the total, just over half (53.9%) of adolescent girls used social media, with less than one-fifth (14.2%) being normal social media users. In addition, based on the anthropometric measurements, almost three-quarters (71.2%) were normal weight (Table 3).
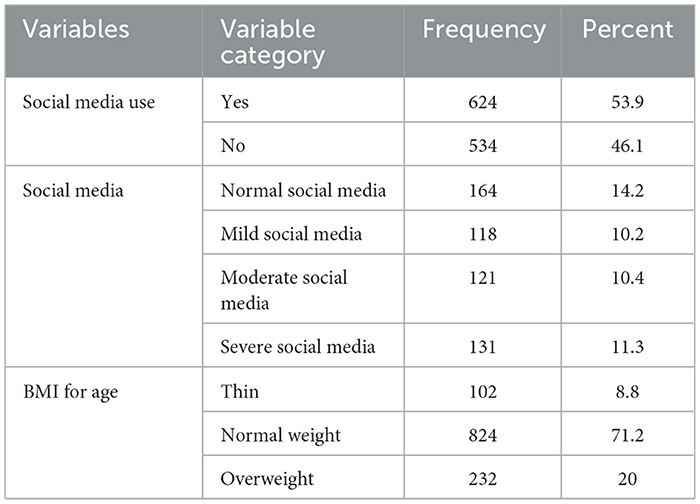
Table 3. Social media and nutritional status of late adolescent girls, Gondar city, northwest Ethiopia, 2022 (n = 1,158).
Prevalence of disordered eating attitudes
In this study, the overall prevalence of DEAs among late adolescent girls was 9.7% (95% CI: 7.96, 11.4%). Moreover, the study revealed that almost one-tenth (9.6%) of adolescent girls always felt that others would prefer it if they ate more. However, only a small proportion (0.5%) of adolescent girls always had the urge to vomit after meals. A small percentage (8.1%) of the girls were always preoccupied with the thought of having fat on their bodies (Table 4).
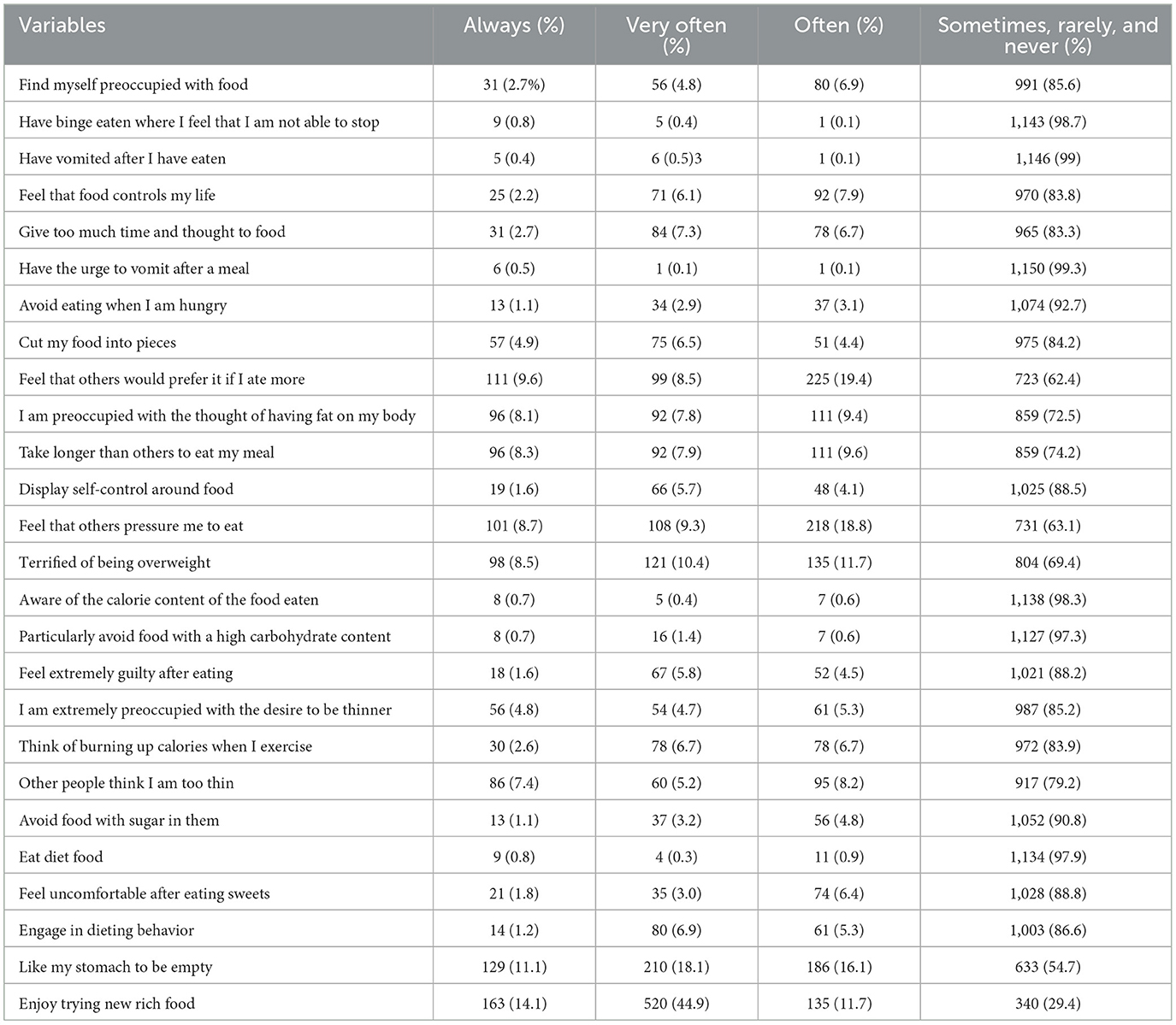
Table 4. EAT-26 score among late adolescent girls, Gondar city, northwest Ethiopia, 2022 (n = 1,158).
Factors associated with disordered eating attitudes among late adolescent girls
In the bivariable logistic regression analysis, the age of adolescent girls, the living status in the family, the mother's educational status, the father's educational status, household wealth index, anxiety, depression, social media use, family size, and nutritional status showed a significant association with DEAs at a p-value of <0.2. Subsequently, these variables were fitted to the multivariable logistic regression analysis to control for potential confounders. Accordingly, it was noted that having a mother who was unable to read and write, having a mother who could read and write, having a father who had attended primary school, having severe anxiety, and having severe social media use were independently associated with DEAs (p < 0.05 (Table 5). In addition, the fitness of the model was assured using the Hosmer–Lemeshow goodness-of-fit test (p-value = 0.19) and adjusted R square (p-value = 0.28).
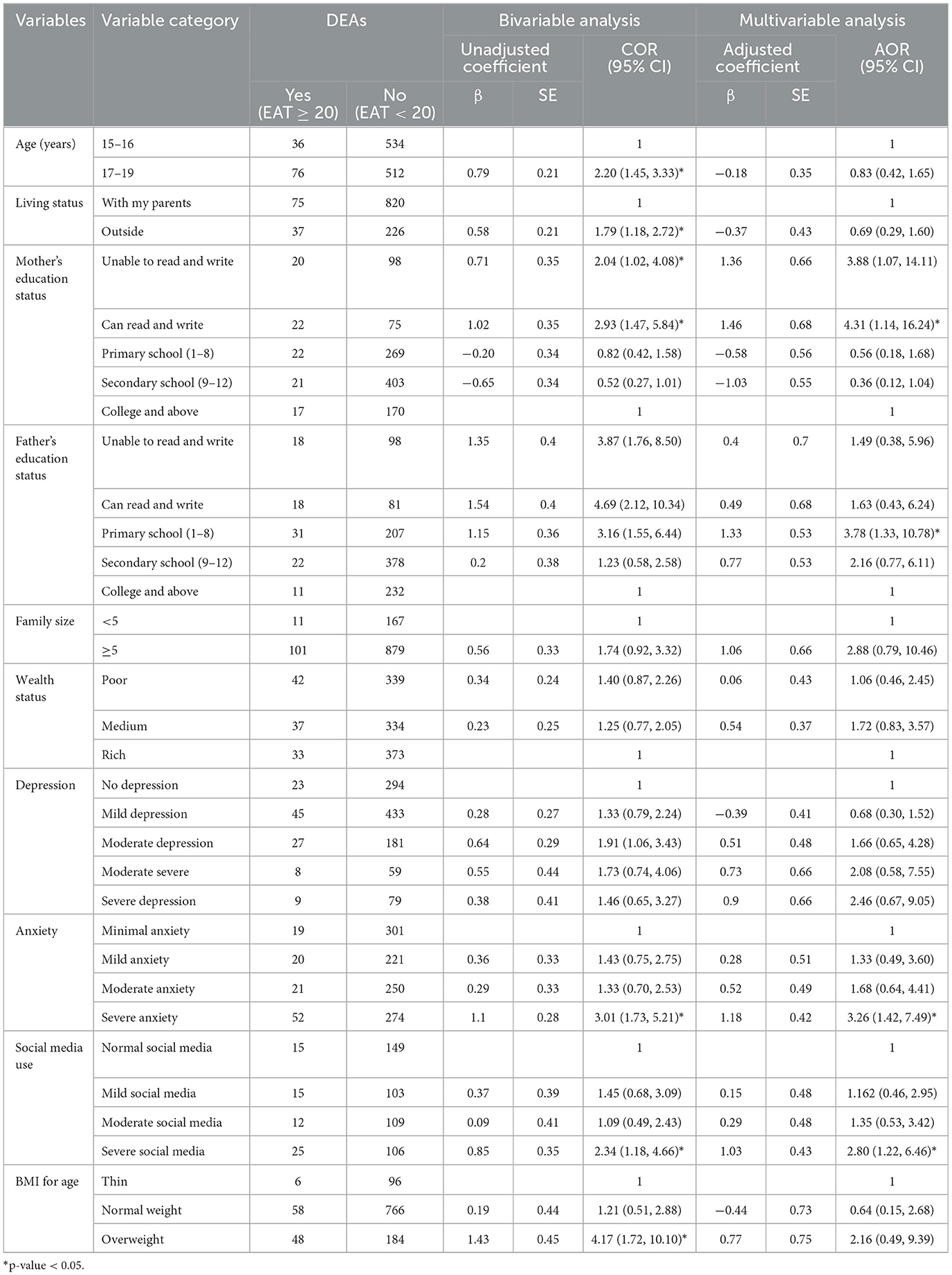
Table 5. Bivariable and multivariable logistic regression analysis of the factors associated with DEAs among late adolescent girls in Gondar city, northwest Ethiopia, 2022 (n = 1,158).
When compared to adolescent girls whose mothers had attended college and above, the odds of developing DEAs were 3.88 [AOR: 3.88 (95% CI: 1.07, 14.11)] times higher for adolescent girls whose mothers were unable to read and write and 4.31 [AOR: 4.31: (95% CI: 1.14, 16.24)] times higher for adolescent girls whose mothers could read and write. When comparing adolescent girls whose fathers had only primary school education to adolescent girls whose fathers had higher education, the odds of having DEAs was 3.78 [AOR: 3.78 (95% CI: 1.33, 10.78)] times higher for the former group.
Furthermore, adolescent girls with severe anxiety had 3.26 [AOR: 3.26 (95% CI: 1.42, 7.49)] times higher odds of developing DEAs than those with minimal anxiety. When comparing late adolescent girls with normal social media usage to those with severe social media use, the odds of having DEAs was 2.8 [AOR: 2.80 (95% CI: 1.22–6.46] times higher among the latter group (Table 5).
Discussion
This study was undertaken to estimate the prevalence and associated factors of disordered eating attitudes (DEAs) among late adolescent girls in Gondar city. The study indicated that the prevalence of DEAs among late adolescent girls was 9.7% (95% CI: 7.96, 11.4%). This finding was in line with a previous study conducted in Singapore (10.5%) (43). However, the prevalence found in this study was higher than in a study conducted in Addis Ababa, Ethiopia (5.98%) (26). The difference in the study period might explain the discrepancy. In recent years, along with the increased availability of smartphones, social media users in Ethiopia have been increasing on a daily basis, which has become an entry point to Western lifestyles (44, 45). Unregulated usage of these social media outlets in Ethiopia could lead to body dissatisfaction and anxiety, which is associated with an increased rate of DEAs (18). Moreover, this study also revealed a higher proportion of DEAs among adolescents when compared to a report from China (4%) (17). The controlled use of social media among adolescents in China might explain this decreased rate (46).
On the contrary, the prevalence of DEAs in the current study was lower than that reported in other African countries, such as Nigeria (13.1%) and Egypt (35.5%) (24, 25). The observed discrepancy could be explained by the Western culture that has been imposed upon these African countries due to the strong ties that they have established over the centuries (47, 48). Furthermore, this finding was lower than the findings from countries in the Middle East, such as Iran (24.7%) (21), Saudi Arabia (25.47%) (19), and Jordan (25.47%) (31). Rapid economic changes that resulted in sociocultural changes in Middle Eastern countries might explain the difference (49). Moreover, this finding was lower than the findings reported in European countries, such as Bulgaria (22.5%) (10), Greece (17.8%) (18), and Spain (29.87%) (16). The possible reasons for this difference could be sociocultural differences, such as considering thinness as a standard of beauty in industrial society. In addition, an increased consumption of processed foods in these countries could result in rapid weight gain and obesity, which later predisposes adolescents to depression and body image dissatisfaction (50).
This study revealed that mothers' educational status has a positive association with DEAs among late adolescent girls. The odds of having DEAs were higher among late adolescent girls whose mothers were unable to read and write and the girls whose mothers could only read and write when compared to late adolescent girls whose mothers had a higher educational status (college and above). This was comparable with a report from Addis Ababa (26). This might be due to the fact that a high level of parental education would create a healthy lifestyle. Clearly, educated mothers could provide advice to their daughters on the importance of following healthy nutritional practices (51, 52).
Similarly, the odds of developing DEAs were higher among late adolescent girls whose fathers had primary school education compared to the adolescents whose fathers had a higher educational status (college and above). This result was in line with a previous study conducted in Singapore (43). The possible reason is that increased literacy raises people's awareness regarding various preventive actions for a healthy lifestyle (52).
The odds of developing disordered eating attitudes among adolescent girls who developed severe anxiety were higher than adolescent girls who developed minimal anxiety. This was consistent with earlier findings reported in Iran and Greece (18, 21). Increased anxiety levels may lead adolescents to maladaptive ways of managing their stress and emotions, through disordered eating. When one eats more to cope with a stressful situation, then one may exercise more or eat less the next day to offset the caloric over-consumption, which in turn results in DEAs (53).
Furthermore, the odds of developing DEAs among adolescent girls with severe social media usage were higher than among adolescent girls whose social media usage was normal. This was comparable with a study from the Philippines and Turkey (54, 55). The possible reason is that repeated exposure to social media could direct individuals' perceptions and views toward body appearance in a different direction. For example, in different social media outlets, a thin woman is often portrayed as an ideal woman, which has encouraged girls to lose weight and engage in dieting (56).
There are some limitations in the present study. On assessing depression and anxiety over a period of 2 weeks, the participants may have been prone to recall bias. In addition, the cross-sectional nature of the study may have limited the establishment of causal associations between the predictors and disordered eating attitudes. Finally, as male adolescents were not included in this study, the findings of this study should be carefully interpreted for all late adolescents.
Practical implication
In developing countries, such as Ethiopia, the problem of eating disorders among adolescents is unsolicited in public health research. Due to this reason, identifying the causes of disordered eating to provide an effective solution has been a challenge in the country. In light of this, the current study attempted to provide baseline information for researchers and policymakers to design an inclusive strategy for mitigating this emerging problem.
This study also revealed that social media influence (severe social media use) is an important challenge in disordered eating attitudes. It is, therefore, noteworthy to create an awareness that the body image that is being advertised in different social media outlets is unattainable. Moreover, the findings of this study implied the importance of developing messages that can be used by educators, social media influencers, and parents in raising awareness to limit social media's influence on body image.
Conclusion
The current study revealed that the rate of disordered eating attitudes among late adolescent girls was relatively high. Having a mother who was unable to read and write, having a mother who could only read and write, having a father with a primary school education, participants with severe anxiety, and a severe social media user were significantly associated with disordered eating attitudes among late adolescent girls in Gondar city. Therefore, nutritional education for the parents of adolescents who are vulnerable to unhealthy behavior is imperative for alleviating the problem. In addition, parental control and legislation that limit social media usage among adolescent girls need to be encouraged.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by University of Gondar, Gondar, Ethiopia. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants' legal guardians/next of kin.
Author contributions
BE: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Resources, Software, Supervision, Writing – original draft, Writing – review & editing. KG: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Writing – original draft, Writing – review & editing. BM: Conceptualization, Data curation, Formal analysis, Methodology, Software, Writing – original draft, Writing – review & editing. NW: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Supervision, Validation, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
The authors would like to thank the study participants, without whom it would have not been possible. We would also like to thank Gondar city health bureau for granting us a permission letter to conduct this study. Finally, we would also like to extend our gratitude to the data collectors and supervisors.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
AOR, adjusted odds ratio; BMI, body mass index; CI, confidence interval; COR, crude odds ratio; DEA, disordered eating attitude; GAD, General Anxiety Disorder; IAT, Internet Addiction Test; IQR, inter quantile range; NGO, non-governmental organization; PHQ, Patient Health Question; SD, standard deviation; SE, standard error; SPSS, Statistical Package for the Social Sciences; VIF, variance inflation factor; WHO, World Health Organization.
References
1. Popkin BM, Adair LS, Ng SW. Global nutrition transition and the pandemic of obesity in developing countries. Nutr Rev. (2012) 70:3–21. doi: 10.1111/j.1753-4887.2011.00456.x
2. Amuna P, Zotor FB. Epidemiological and nutrition transition in developing countries: impact on human health and development: the epidemiological and nutrition transition in developing countries: evolving trends and their impact in public health and human development. Proc Nutr Soc. (2008) 67:82–90. doi: 10.1017/S0029665108006058
3. Viru A, LokoJ, Harro M, Volver A, Laaneots L, Viru M. Critical periods in the development of performance capacity during childhood and adolescence. Eur J Phys Educ. (1999) 4:75–119. doi: 10.1080/1740898990040106
4. Dumontheil I. Adolescent brain development. Curr Opin Behav Sci. (2016) 10:39–44. doi: 10.1016/j.cobeha.2016.04.012
5. Robeva R, Kumanov P. Physical changes during pubertal transition. In: Kumanov P, Agarwal A, editors. Puberty. Cham: Springer International Publishing (2016). p. 39–64.
6. Das JK, Salam RA, Thornburg KL, Prentice AM, Campisi S, Lassi ZS, et al. Nutrition in adolescents: physiology, metabolism, and nutritional needs. Ann N Y Acad Sci. (2017) 1393:21–33. doi: 10.1111/nyas.13330
7. Jones JM, Bennett S, Olmsted MP, Lawson ML, Rodin G. Disordered eating attitudes and behaviours in teenaged girls: a school-based study. CMAJ. (2001) 165:547–52.
8. Fadipe B, Oyelohunnu MA, Olagunju AT, Aina OF, Akinbode AA, Suleiman TF. Disordered eating attitudes: demographic and clinico-anthropometric correlates among a sample of Nigerian students. Afr Health Sci. (2017) 17:513–23. doi: 10.4314/ahs.v17i2.27
9. Harrison AN, Bateman CCBJ, Younger-Coleman NOM, Williams MC, Rocke KD, Scarlett SCC-D, et al. Disordered eating behaviours and attitudes among adolescents in a middle-income country. Eat Weight Disord. (2020) 25:1727–37. doi: 10.1007/s40519-019-00814-5
10. Massaldjieva R, Bakova DR, Semerdjieva MA, Tornyova B. Disordered eating attitudes and behaviors: gender differences in adolescence and young adulthood. J Womens Health Care. (2017) 6:3. doi: 10.4172/2167-0420.1000368
11. Wade KH, Kramer MS, Oken E, Timpson NJ, Skugarevsky O, Patel R, et al. Prospective associations between problematic eating attitudes in midchildhood and the future onset of adolescent obesity and high blood pressure. Am J Clin Nutr. (2017) 105:306–12. doi: 10.3945/ajcn.116.141697
12. Hoek HW. Incidence, prevalence and mortality of anorexia nervosa and other eating disorders. Curr Opin Psychiatry. (2006) 19:389–94. doi: 10.1097/01.yco.0000228759.95237.78
13. Pedro TM, Micklesfield LK, Kahn K, Tollman SM, Pettifor JM, Norris SA. Body image satisfaction, eating attitudes and perceptions of female body silhouettes in rural South African adolescents. PLoS ONE. (2016) 11:e0154784. doi: 10.1371/journal.pone.0154784
14. Mann RB, Blumberg F. Adolescents and social media: the effects of frequency of use, self-presentation, social comparison, and self esteem on possible self imagery. Acta Psychol. (2022) 228:103629. doi: 10.1016/j.actpsy.2022.103629
15. Golden NH. Eating disorders in adolescence and their sequelae. Best Pract Res Clin Obstetr Gynaecol. (2003) 17:57–73. doi: 10.1053/ybeog.2003.0344
16. Pamies-Aubalat L, Quiles Marcos Y, Torregrosa Díez MS. Psychosocial profile related to disordered eating attitudes in Spanish adolescents. Curr Psychol. (2022) 42:20193–202. doi: 10.1007/s12144-022-03164-1
17. Yu J, Lu M, Tian L, Lu W, Meng F, Chen C, et al. Prevalence of disordered eating attitudes among university students in Wuhu, China. Nutr Hosp. (2015) 32:1752–7. doi: 10.3305/nh.2015.32.4.9187
18. Bacopoulou F, Foskolos E, Stefanaki C, Tsitsami E, Vousoura E. Disordered eating attitudes and emotional/behavioral adjustment in Greek adolescents. Eat Weight Disord. (2018) 23:621–8. doi: 10.1007/s40519-017-0466-x
19. Fatima W, Ahmad LM. Prevalence of disordered eating attitudes among adolescent girls in Arar City, Kingdom of Saudi Arabia. Health Psychol Res. (2018) 6:7444. doi: 10.4081/hpr.2018.7444
20. Allihaibi MM. Disordered eating attitudes among secondary schoolgirls in Al-Iskan sector, Makkah Al-Mukarramah, Saudi Arabia. Int J Med Sci Public Health. (2015) 4:939–46. doi: 10.5455/ijmsph.2015.12032015191
21. Sanaei H, Dabiran S, Seddigh L. Eating attitudes among adolescent girls in Tehran: a schoolbased survey between 2010-2011. Soc Determin Health. (2016) 2:98–105. doi: 10.22037/sdh.v2i3.16390
22. Canan F, Yildirim O, Ustunel TY, Sinani G, Kaleli AH, Gunes C, et al. The relationship between internet addiction and body mass index in Turkish adolescents. Cyberpsychol Behav Soc Netw. (2014) 17:40–5. doi: 10.1089/cyber.2012.0733
23. Yardimci H, Hakli G, Özçelik AÖ, Çakiroglu FP. Evaluation of eating attitudes of Turkish adolescents based on certain variables. Anthropologist. (2016) 24:810–7. doi: 10.1080/09720073.2016.11892077
24. Koleoso ON, Akanni OO, James JO. Body image objectification and disordered eating attitudes among secondary school students of South-West Nigeria. Int J Sch Health. (2018) 5:1–5. doi: 10.5812/intjsh.66891
25. Abu-Elenin MM, Shalby S, Fly A. Disordered eating attitudes, weight abnormalities and body image perception among high school adolescent girls in Gharbia Governorate, Egypt disordered eating attitudes among high school adolescent girls in Egypt. Can J Clin Nutr. (2019) 8:21–35. doi: 10.14206/canad.j.clin.nutr.2020.01.03
26. Yirga B, Gelaw YA, Derso T, Wassie MM. Disordered eating attitude and associated factors among high school adolescents aged 12–19 years in Addis Ababa, Ethiopia: a cross-sectional study. BMC Res Notes. (2016) 9:1–7. doi: 10.1186/s13104-016-2318-6
27. Cohen E, Richter LM, Chidumwa G, Abdalla S, Weber AM, Darmstadt GL, et al. Relationships between maternal factors and weight loss attempts among urban male and female adolescents living in Soweto, Johannesburg, South Africa. J Adolesc Health. (2020) 66:S17–24. doi: 10.1016/j.jadohealth.2019.10.015
28. Shomaker LB, Furman W. Interpersonal influences on late adolescent girls' and boys' disordered eating. Eat Behav. (2009) 10:97–106. doi: 10.1016/j.eatbeh.2009.02.003
29. Tremblay L, Lariviere M. The influence of puberty onset, body mass index, and pressure to be thin on disordered eating behaviors in children and adolescents. Eat Behav. (2009) 10:75–83. doi: 10.1016/j.eatbeh.2008.12.001
30. Al-Kloub MI, Al-Khawaldeh OA, ALBashtawy M, Batiha AM, Al-Haliq M. Disordered eating in Jordanian adolescents. Int J Nurs Pract. (2019) 25:e12694. doi: 10.1111/ijn.12694
31. Ghraiybah T. Prevalence and correlates of disordered eating attitudes among Jordanian adolescents. Arab J Nutr Exerc. (2018) 3:35–53. doi: 10.18502/ajne.v3i2.2745
32. Shea ME, Pritchard ME. Is self-esteem the primary predictor of disordered eating? Pers Individ Dif. (2007) 42:1527–37. doi: 10.1016/j.paid.2006.10.026
33. O'Hara L, Tahboub-Schulte S, Thomas J. Weight-related teasing and internalized weight stigma predict abnormal eating attitudes and behaviours in Emirati female university students. Appetite. (2016) 102:44–50. doi: 10.1016/j.appet.2016.01.019
34. Puhl RM, Wall MM, Chen C, Austin SB, Eisenberg ME, Neumark-Sztainer D. Experiences of weight teasing in adolescence and weight-related outcomes in adulthood: a 15-year longitudinal study. Prev Med. (2017) 100:173–9. doi: 10.1016/j.ypmed.2017.04.023
36. Zenebe Y, Kunno K, Mekonnen M, Bewuket A, Birkie M, Necho M, et al. Prevalence and associated factors of internet addiction among undergraduate university students in Ethiopia: a community university-based cross-sectional study. BMC Psychol. (2021) 9:1–10. doi: 10.1186/s40359-020-00508-z
37. Ganguly S, Samanta M, Roy P, Chatterjee S, Kaplan DW, Basu B. Patient health questionnaire-9 as an effective tool for screening of depression among Indian adolescents. J Adolesc Health. (2013) 52:546–51. doi: 10.1016/j.jadohealth.2012.09.012
38. Girma S, Tsehay M, Mamaru A, Abera M. Depression and its determinants among adolescents in Jimma town, Southwest Ethiopia. PLoS ONE. (2021) 16:e0250927. doi: 10.1371/journal.pone.0250927
39. Gelaye B, Williams MA, Lemma S, Deyessa N, Bahretibeb Y, Shibre T, et al. Validity of the patient health questionnaire-9 for depression screening and diagnosis in East Africa. Psychiatry Res. (2013) 210:653–61. doi: 10.1016/j.psychres.2013.07.015
40. Manzar MD, Salahuddin M, Alghadir A, Anwer S, Peter S, Bahammam AS, et al. psychometric properties of the generalized anxiety Disorder-7 Scale in Ethiopian university students. Bull Menninger Clin. (2021) 85:405–27. doi: 10.1521/bumc.2021.85.4.405
41. Tremblay L, Limbos M. Body image disturbance and psychopathology in children: research evidence and implications for prevention and treatment. Curr Psychiatry Rev. (2009) 5:62–72. doi: 10.2174/157340009787315307
42. World Health Organization. BMI-for-Age (5-19 Years). (2022). Available at: https://www.who.int/tools/growth-reference-data-for-5to19-years/indicators/bmi-for-age (accessed November 06, 2022).
43. Ho T, Tai BC, Lee EL, Cheng S, Liow PH. Prevalence and profile of females at risk of eating disorders in Singapore. Singapore Med J. (2006) 47:499.
44. World Bank Group. Individuals Using the Internet (% of Population) - Ethiopia. International Telecommunication Union (ITU) World Telecommunication/ICT Indicators Database. (2023). Available at: https://data.worldbank.org/indicator/IT.NET.USER.ZS?locations=ET (accessed April 23, 2023).
45. Bhanye J, Shayamunda R, Tavirai RC. Social media in the African context. In: The Palgrave Handbook of Global Social Problems. Cham: Springer International Publishing (2021). p. 1–32.
46. Zagidullin M, Aziz N, Kozhakhmet S. Government policies and attitudes to social media use among users in Turkey: the role of awareness of policies, political involvement, online trust, and party identification. Technol Soc. (2021) 67:101708. doi: 10.1016/j.techsoc.2021.101708
47. Ogohi DC. Impact of globalization on socio-cultural development in Nigeria. Dev Count Stud. (2014) 4:38.
48. Bier L. Revolutionary Womanhood: Feminisms, Modernity, and the State in Nasser's Egypt. California: Stanford University Press (2011).
49. Ng SW, Zaghloul S, Ali H, Harrison G, Yeatts K, El Sadig M, et al. Nutrition transition in the United Arab Emirates. Eur J Clin Nutr. (2011) 65:1328–37. doi: 10.1038/ejcn.2011.135
50. Lindberg L, Hagman E, Danielsson P, Marcus C, Persson M. Anxiety and depression in children and adolescents with obesity: a nationwide study in Sweden. BMC Med. (2020) 18:1–9. doi: 10.1186/s12916-020-1498-z
51. Yañez AM, Bennasar-Veny M, Leiva A, García-Toro M. Implications of personality and parental education on healthy lifestyles among adolescents. Sci Rep. (2020) 10:1–10. doi: 10.1038/s41598-020-64850-3
52. Haddad LG, Owies A, Mansour A. Impact of educational status of parents on nutritional status of adolescent girls-a cross sectional study. Natl J Commun Med. (2014) 5:266–9. doi: 10.1016/S0377-1237(02)80011-9
53. Fox CK, Gross AC, Rudser KD, Foy AM, Kelly AS. Depression, anxiety, and severity of obesity in adolescents: is emotional eating the link? Clin Pediatr. (2016) 55:1120–5. doi: 10.1177/0009922815615825
54. Alpaslan AH, Koçak U, Avci K, Taş HU. The association between internet addiction and disordered eating attitudes among Turkish high school students. Eat Weight Disord. (2015) 20:441–8. doi: 10.1007/s40519-015-0197-9
55. Tadena S, Kang SR, Kim S-J. The influence of social media affinity on eating attitudes and body dissatisfaction in Philippine adolescents. Child Health Nurs Res. (2020) 26:121. doi: 10.4094/chnr.2020.26.1.121
Keywords: disordered eating attitude, late adolescent girl, Gondar city, associated factors, northwest Ethiopia
Citation: Engdyhu BM, Gonete KA, Mengistu B and Worku N (2024) Disordered eating attitude and associated factors among late adolescent girls in Gondar city, northwest Ethiopia: a community-based cross-sectional study. Front. Public Health 12:1425986. doi: 10.3389/fpubh.2024.1425986
Received: 30 April 2024; Accepted: 12 August 2024;
Published: 04 September 2024.
Edited by:
Michael Leon, University of California, Irvine, United StatesReviewed by:
Ángela Hoyo, Universidad Isabel I de Castilla, SpainAncah Caesarina Novi Marchianti, University of Jember, Indonesia
Copyright © 2024 Engdyhu, Gonete, Mengistu and Worku. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Berhanu Mengistu, YmVyaGFudTVAeWFob28uY29t