 Wei Wang1,2,3*
Wei Wang1,2,3*- 1Shanghai Engineering Research Center of Tooth Restoration and Regeneration and Tongji Research Institute of Stomatology, Shanghai, China
- 2Department of Clinical Medical Laboratory, Tongji University Stomatological Hospital, Shanghai, China
- 3Dental School, Tongji University, Shanghai, China
Background: Properly adhering to oral hygiene and medical care is an important public health issue. Several studies examined the knowledge, attitudes, and practices (KAP) toward oral care in various populations and generally reported relatively sufficient knowledge but unfavorable attitudes and poor practice. However, no previous studies have examined the KAP toward oral examinations among Chinese patients with oral diseases. This study aimed to examine the KAP toward oral examinations among patients with oral diseases in China.
Methods: This cross-sectional study was conducted in patients with oral diseases who visited The Affiliated Stomatological Hospital of Tongji University between December 2023 and February 2024. Data collection and KAP scores assessment were performed using a self-designed questionnaire.
Results: A total of 519 valid questionnaires were included, with 292 females. The mean knowledge, attitude, and practice scores were 6.42 ± 2.47 (possible range: 0–9 points), 35.04 ± 5.68 (possible range: 10–50 points), and 16.22 ± 2.05 (possible range: 4–20 points), respectively, indicating sufficient knowledge, positive attitudes, and proactive practice. Pearson’s correlation analysis showed that knowledge was positively correlated to attitude (r = 0.468, p < 0.001) and practice (OR = 0.416, p < 0.001). Attitude was positively correlated to the practice (r = 0.503, p < 0.001). Moreover, the structural equation model showed that knowledge influenced attitude (estimate = 1.010, p < 0.001) and practice (estimate = 0.169, p < 0.001). Attitude influenced practice (estimate = 0.122, p < 0.001). The frequency of oral examination per year influenced knowledge (estimate = −0.761, p < 0.001) and practice (estimate = −0.515, p < 0.001). Expenses for oral disease per year influenced attitude (estimate = 0.537, p < 0.001).
Conclusion: Patients with oral disease might have sufficient knowledge, positive attitude, and proactive practice toward oral examinations. Specific knowledge items were identified to require improvements.
Introduction
Oral diseases encompass a wide variety of diseases and conditions, including odontogenic diseases (e.g., dental caries and pulpitis) (1, 2), tooth fracture (3), crack, temporomandibular joint disease (4), tooth implantation (5), oral mucosal diseases (e.g., oral ulcers) (6), periodontal diseases (e.g., gingivitis) (7), maxillofacial deformities, and tumors (8, 9). Despite their vast differences in etiology, risk factors, incidence, prevalence, and management, most of these conditions have in common that they require an oral examination for diagnosis, examinations during management until resolution, and regular follow-up examinations to check for recurrence and allow early treatment. Gingivitis can be diagnosed by oral hygienists and can be reversed by adequate oral hygiene, but the patients might need guidance regarding oral hygiene. Maintaining good oral health is important since periodontal diseases are risk factors for non-communicable diseases like cardiovascular diseases, diabetes, cancers, and adverse pregnancy outcomes, among others (10–12).
The adequate management of these conditions first requires the patient to realize that something is wrong and seek consultation. After that, a proper understanding of the importance of adherence to oral examinations during the management and follow-up of the condition is also required. Indeed, several oral conditions have a high risk of recurrence after successful management. Repeated recurrences, especially if the recurrence is not managed early, are associated with significant morbidity and treatment costs and can increase the risk of mortality (e.g., cancer, of course, but also the risk of endocarditis in patients with untreated dental abscess) (13–15).
Hence, properly adhering to oral hygiene and medical care is an important public health issue (16). Knowledge, attitude, and practice (KAP) studies are designed to provide quantitative and qualitative information about the gaps, misunderstandings, and misconceptions that represent barriers to adequately implementing a specific subject in a specific population (17, 18). Such studies are particularly useful in identifying specific points that should be addressed in educational interventions. Several studies examined the KAP toward oral care in various populations and generally reported relatively sufficient knowledge but unfavorable attitudes and poor practice (19–24). Still, no previous studies have examined the KAP in relation to oral examinations among Chinese patients with oral diseases. Therefore, this study aimed to explore the KAP toward oral examinations among patients with oral diseases.
Materials and methods
Study design and setting
This cross-sectional study was conducted in patients with oral diseases at The Affiliated Stomatological Hospital of Tongji University between December 2023 and February 2024.
Participants
The inclusion criterion was patients with oral diseases who visited the hospital. The exclusion criteria were (1) medical professionals, (2) <18 years of age, (3) questionnaires with contradictory answers, or (4) questionnaires with all answers selected with the same option. This study was approved by the Ethics Committee of Tongji University Affiliated Stomatological Hospital ([2023]-SR-36). Written informed consent was obtained by all participants before completing the questionnaire. For the electronic survey, the informed consent statement was the first step of the questionnaire; electronic consent was necessary to access the questionnaire itself.
Variables
The basic information section included gender, age, residence, education, employment, income, marital status, smoking, oral health expenses, medical insurance, course of oral diseases, types of oral disease, tooth brushing frequency, tooth cleaning frequency, oral examination frequency, and history of head and neck electrotherapy.
Data sources and measurements
The questionnaire was designed based on “Prevention, Diagnosis, and Treatment of Oral Diseases.” The questionnaire was reviewed by experts in the field to clarify the questions (content value). A small-scale pilot study (44 participants) showed a Cronbach’s α of 0.810, indicating good internal consistency. The participants of the pilot study were invited to indicate any unclear questions (face value).
The final questionnaire was in Chinese and included information collected from four dimensions, comprising 41 items. The basic information section included 16 items. The knowledge dimension included nine items, with 1 point awarded for a correct answer and 0 points for an incorrect or unclear answer (possible range: 0–9 points). A score <5 indicated poor knowledge, and 5–9 indicated sufficient knowledge. The attitude dimension included 10 items, with options ranging from negative to positive and scored from 1 to 5 (possible range: 10–50 points), with a score of 10–20 indicating a negative attitude, 21–35 indicating a neutral attitude, and >35 indicating a positive attitude. The practice dimension included five items. Items P1–P4 were scored from negative (1 point) to positive (5 points) (possible range: 4–20 points), with a score of 4–8 indicating poor practice, 9–15 indicating average practice, and 16–20 indicating good practice. Item P5 was a multiple-choice question and was not scored but was described as a separate categorical variable.
Two research assistants, both professional interns in the field of medical laboratory, were trained to handle recruitment and the questionnaire. The research assistants contacted the patients through the patient contact information disclosed in the hospital’s online platform or communicated with the patients in person in the office and recruited and issued questionnaires to the eligible patients. The questionnaires included paper questionnaires, electronic questionnaires, and questionnaires pushed by the hospital platform.
Bias
In order to ensure that the participants could correctly understand the questionnaire content, the writing was in the form of clear and concise questions, providing definitions and examples. In addition, the research assistants could provide supplementary explanations or answer participants’ questions during the questionnaire delivery process.
Incomplete questionnaires and those with all KAP items answered using the same option (e.g., all first options) were considered invalid. For offline questionnaires, the participants could not go home with the questionnaire and bring it back later; doing so led to questionnaire exclusion. For online questionnaires, response time <60 s or >1,800 s led to questionnaire exclusion. Only one questionnaire could be submitted from a given IP address.
Study size
The sample size was estimated based on Ni’s method for quantitative surveys, i.e., 5–10 times the number of KAP items in the survey (25). The survey included 23 items. Therefore, the minimal sample size was 115–230.
Quantitative variables
Descriptive analysis was used to describe the demographic data of the study participants and their KAP scores, using means ± standard deviations for continuous variables and n (%) for categorical data. Since the sample size of this paper was relatively large, based on the central limit theorem, it was assumed that the data in this study were normally distributed.
Statistical analysis
SPSS 22.0 (IBM Corp., Armonk, NY, USA) was used for statistical analysis. In order to compare the differences in KAP scores among study participants with different demographic characteristics, the t-test (two-group comparisons) or ANOVA (comparisons of more than two groups) were used for continuous variables that met the normality assumption, while the Wilcoxon–Mann–Whitney test (comparison of two groups) or the Kruskal–Wallis analysis of variance (multiple groups) were used. Pearson’s correlation analysis was performed to examine the correlations among KAP dimensions. Structural equation modeling (SEM) was used to explore the path relationships between KAP and basic information. The SEM was based on the hypotheses that (1) knowledge influences attitude, (2) knowledge influences practice, (3) attitude influences practice, (4) the frequency of oral examinations per year influences knowledge, attitude, and practice, (5) the course of oral diseases influences knowledge, attitude, and practice, and (6) and the expenses for oral diseases per year influences knowledge, attitude, and practice. Two-sided p-values <0.05 were considered statistically significant.
Results
This study collected 522 questionnaires, but one was excluded for missing age information, one for contradictory answers in the pitfall question, and one for the same answer being selected for all KAP questions. Finally, 519 valid questionnaires were included for analysis (Figure 1). There were 56.26% of female patients, with 18–30 years of age (35.26%). The mean knowledge, attitude, and practice scores were 6.42 ± 2.47 (possible range: 0–9 points), 35.04 ± 5.68 (possible range: 10–50 points), and 16.22 ± 2.05 (possible range: 4–20 points), respectively, indicating sufficient knowledge, positive attitudes, and good practice (Table 1). Among them, 68.98% had sufficient knowledge, 46.24% had a positive attitude, and 91.14% had a proactive practice (Figure 2).

Figure 1. Participant flowchart.

Table 1. Characteristics of the participants.
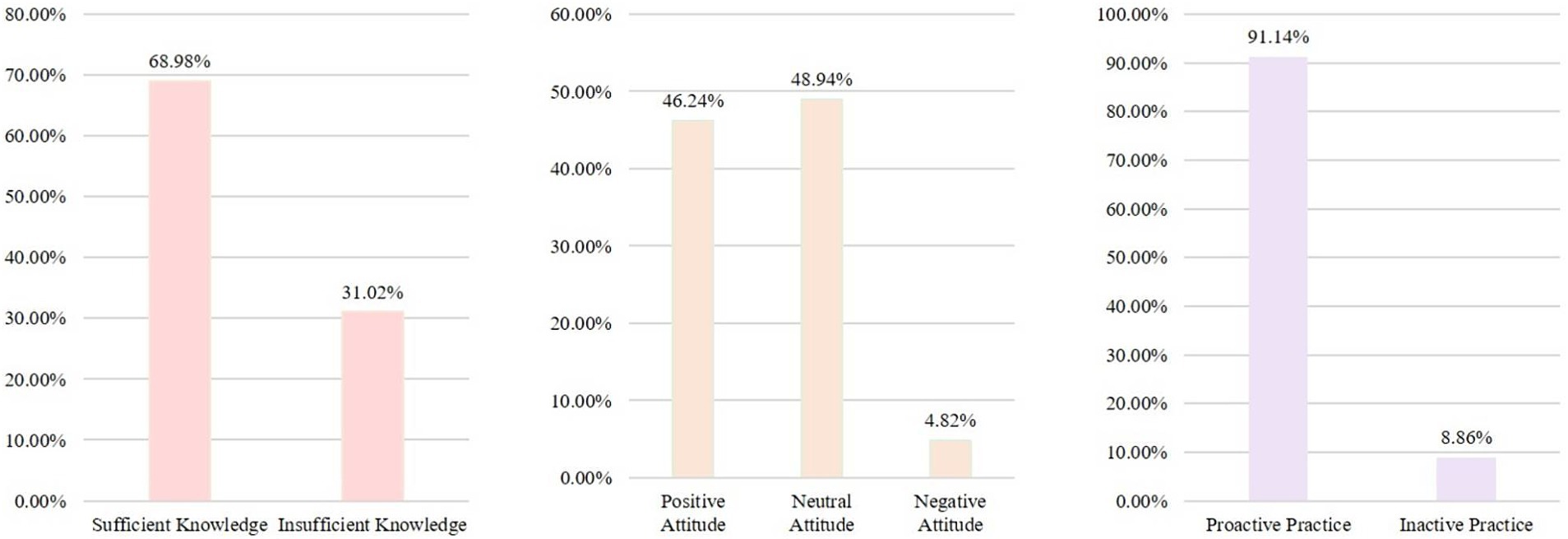
Figure 2. Histogram of the score distribution. K: There are nine questions, with scores ranging from 0 to 5 indicating insufficient knowledge and scores ranging from 6 to 9 indicating sufficient knowledge. A: There are 10 questions, with scores ranging from 10 to 26 indicating a negative attitude, scores ranging from 27 to 36 indicating a neutral attitude, and scores ranging from 37 to 50 indicating a positive attitude. P: There are four questions, with scores ranging from 4 to 13 indicating inactive practice and scores ranging from 14 to 20 indicating proactive practice.
For the knowledge dimension, the highest correct rate was for item K4 (81.50%; “Before root canal treatment, patients need to undergo clinical examinations to determine the size of the carious tissue and whether the dental nerve is vital, such as blood tests and imaging examinations”), while the lowest correct rate was for item K2 (48.36%; “Periodontitis does not require blood tests”) (Table 2). Among the items in the attitude dimension, the item with the highest proportion of positive responses was A1 (“You attach great importance to oral diseases, so you believe that regular oral examinations should be conducted”), while the lowest was observed for A4 (“You believe that the treatment of oral diseases will increase the risk of infectious diseases”) (Table 3). Among the items in the practice dimension, the item with the highest proportion of positive responses was P3 (“You follow the doctor’s advice on whether to undergo blood tests or other medical examinations”), while the lowest was P4 (“Even if there are no obvious oral symptoms, you regularly have your teeth cleaned and undergo blood tests or other medical examinations if necessary”) (Table 4). In addition, the main barrier to practice was the cost (Figure 3).
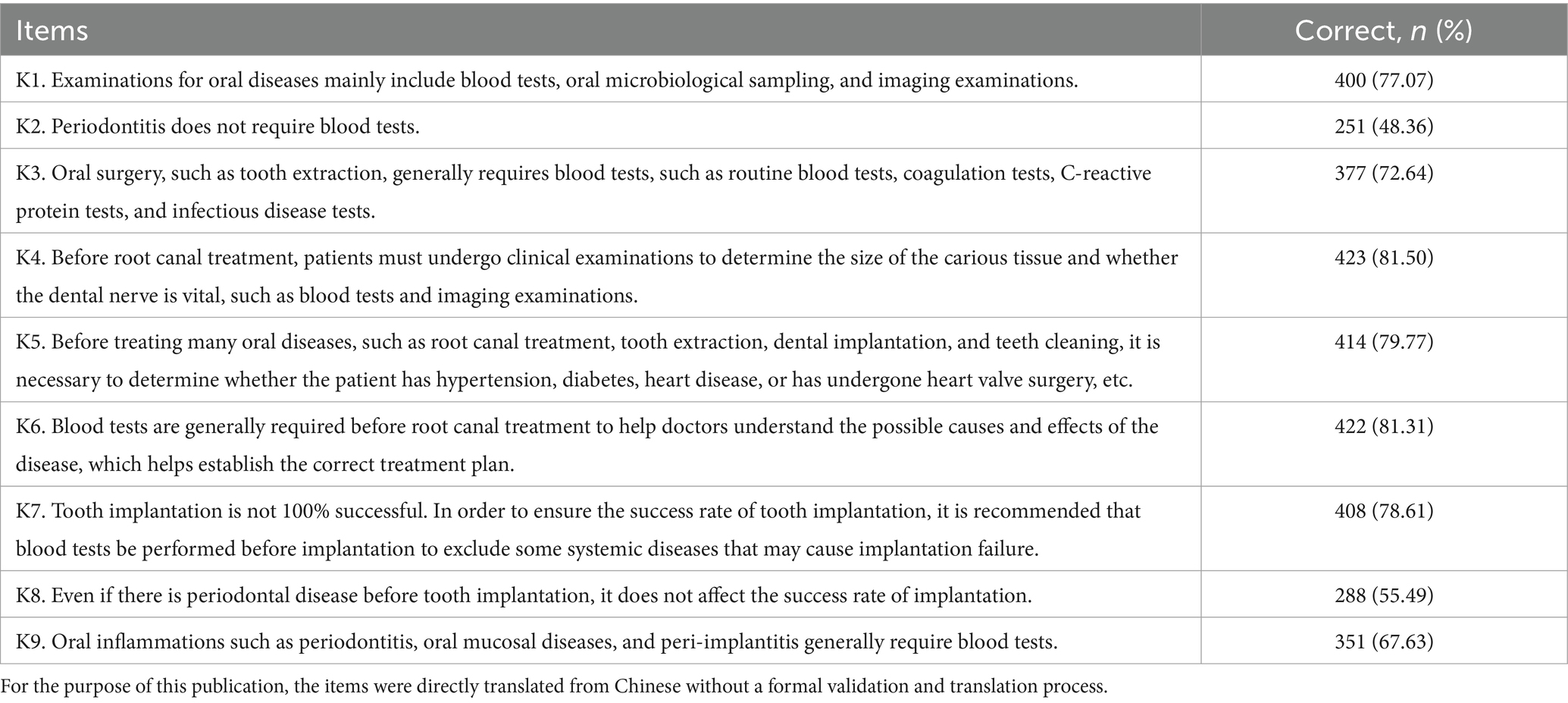
Table 2. Knowledge dimension.
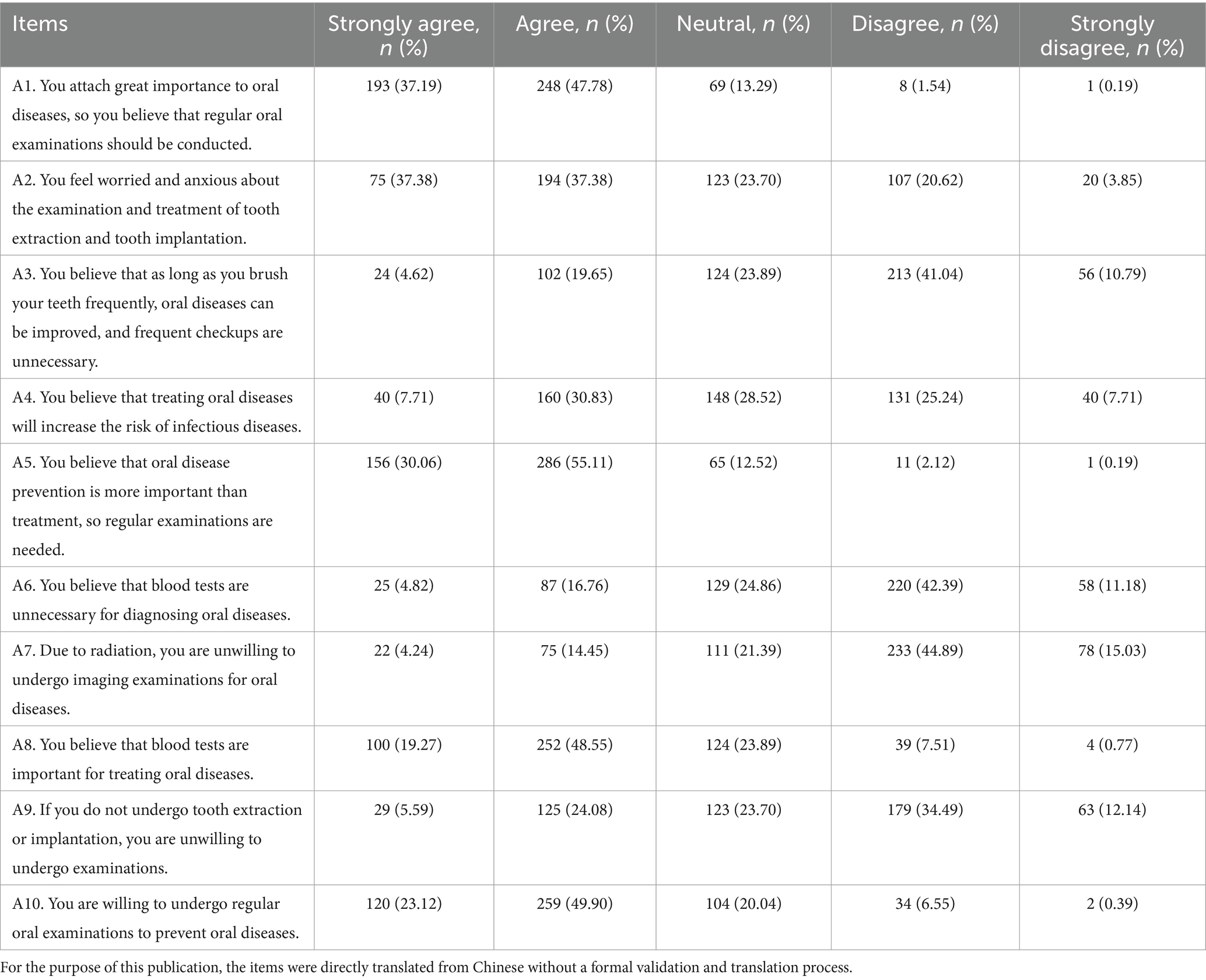
Table 3. Attitude dimension.

Table 4. Practice dimension.
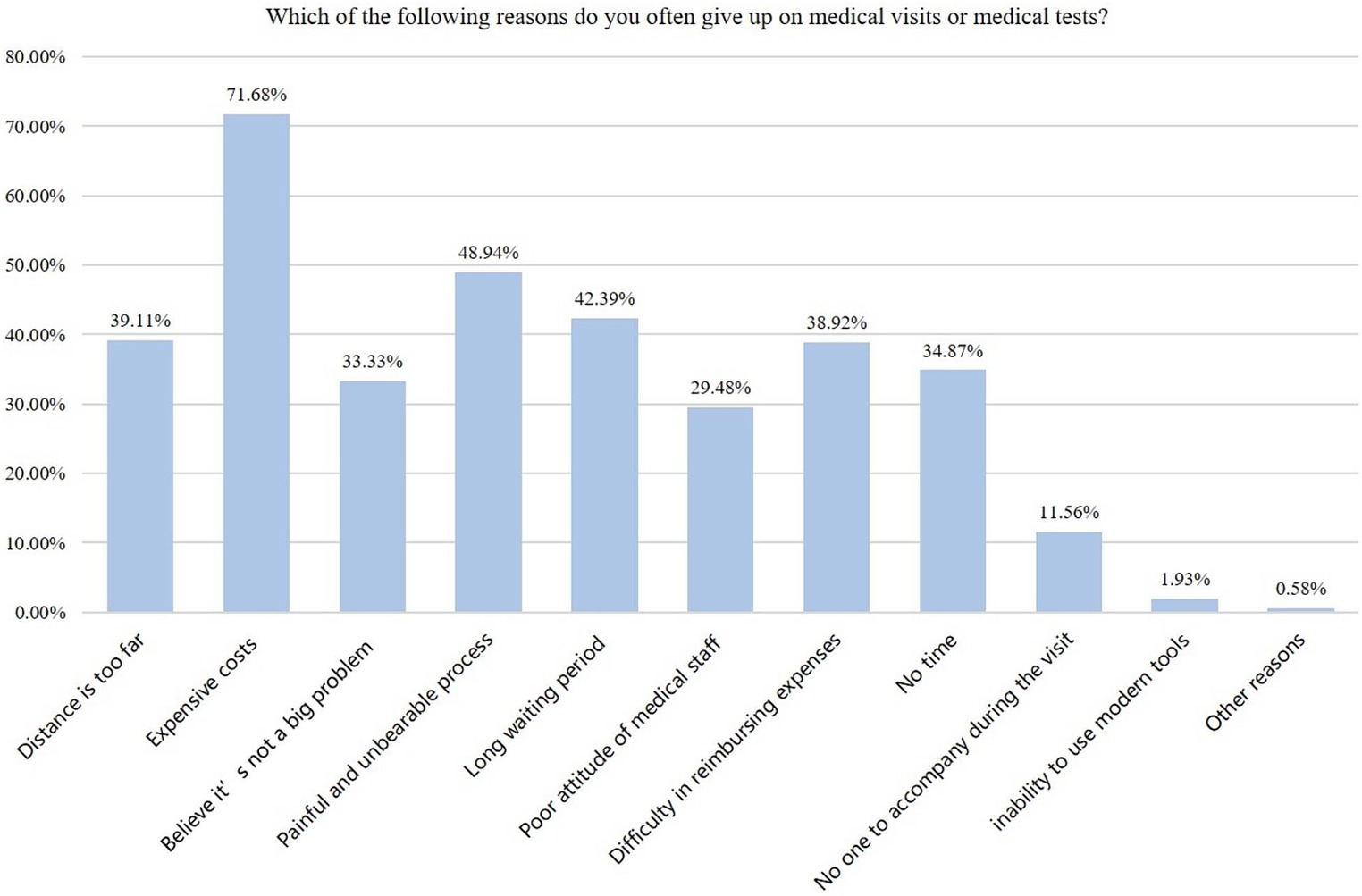
Figure 3. Barriers to medical examinations.
Pearson’s correlation analysis showed that knowledge was positively correlated to attitude (r = 0.468, p < 0.001) and practice (OR = 0.416, p < 0.001). The attitude scores were positively correlated to the practice scores (r = 0.503, p < 0.001) (Table 5).
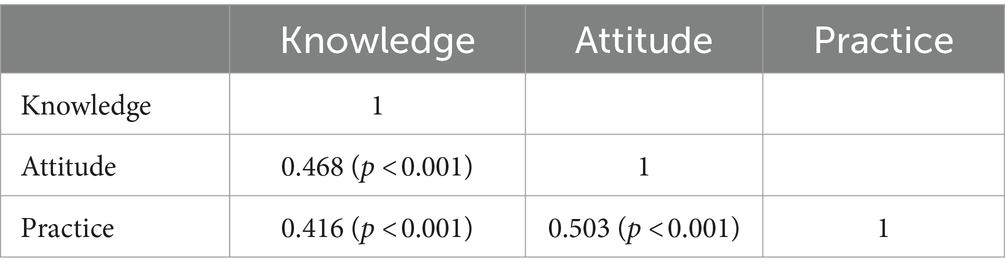
Table 5. Correlation analysis.
SEM showed that knowledge influenced attitudes (estimate = 1.010, p < 0.001) and practice (estimate = 0.169, p < 0.001). Attitude influenced practice (estimate = 0.122, p < 0.001). The frequency of oral examination influenced knowledge (estimate = −0.761, p < 0.001) and practice (estimate = −0.515, p < 0.001). Expenses for oral disease per year influenced attitude (estimate = 0.537, p < 0.001) (Table 6 and Figure 4).
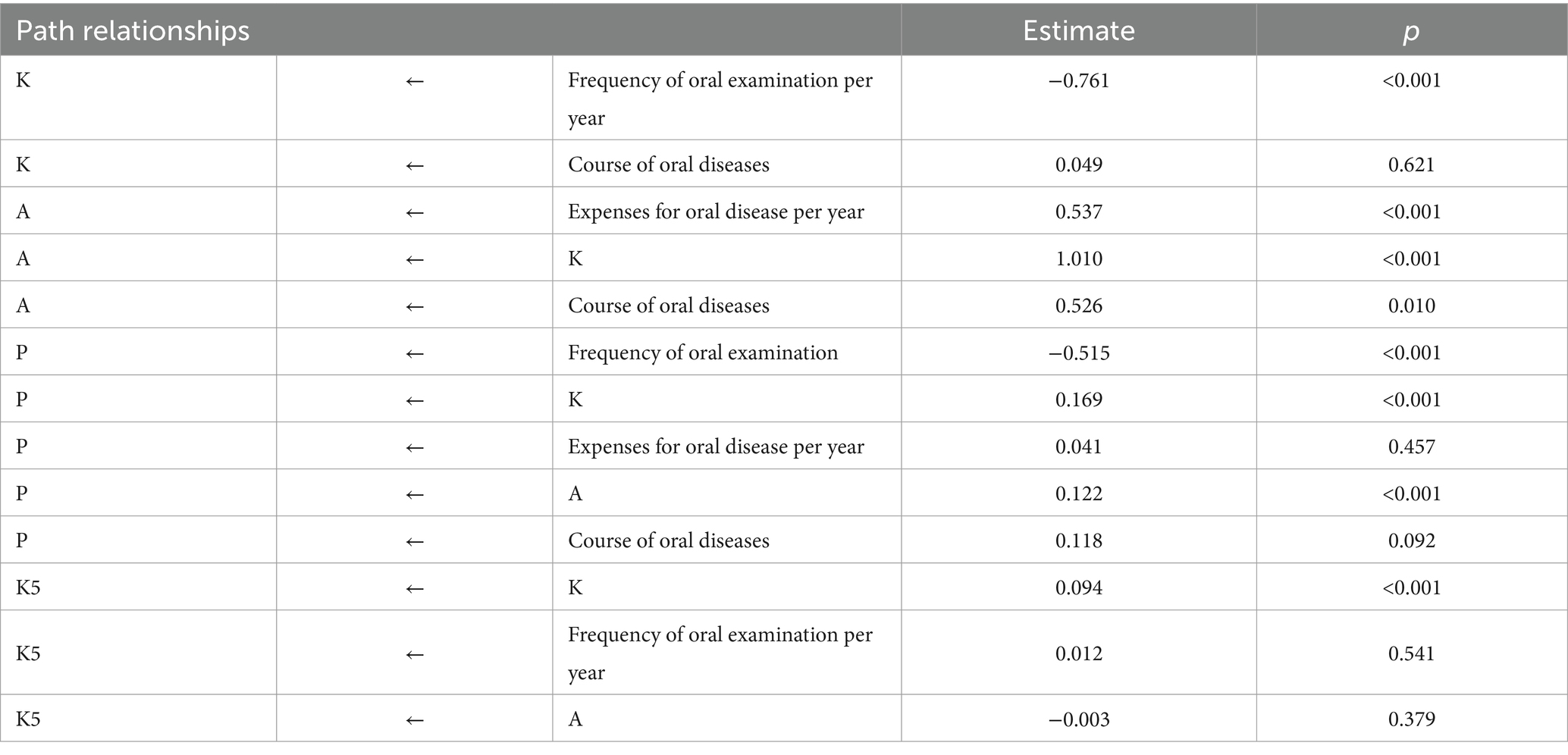
Table 6. SEM.
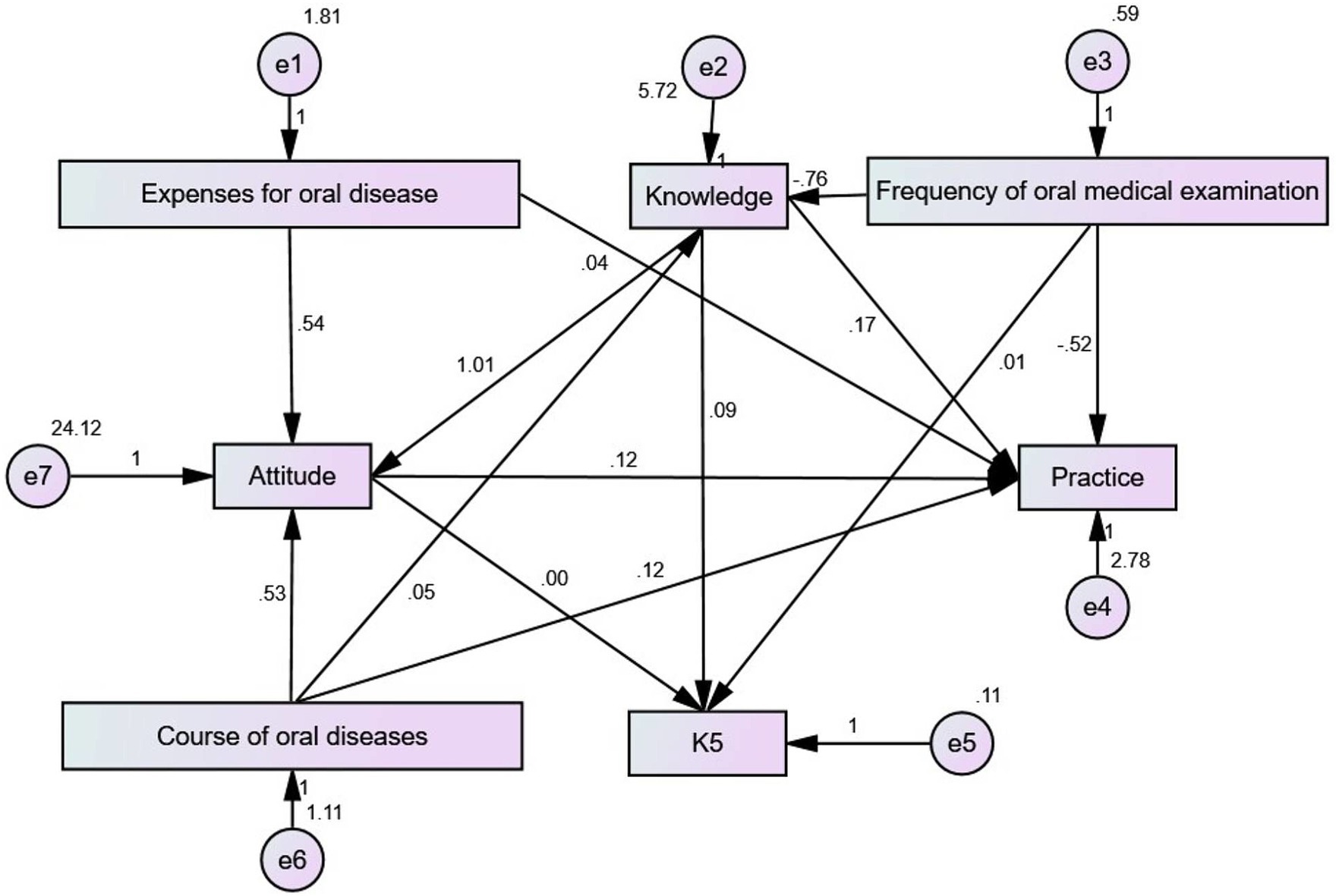
Figure 4. Structural equation model.
Discussion
This cross-sectional study examined the KAP toward oral examinations among Chinese patients with oral diseases. Chinese patients with oral disease have sufficient knowledge, positive attitudes, and good practice toward oral diseases. Knowledge influenced the attitudes, practice, and attitude influenced practice. The frequency of oral examinations per year influenced knowledge and practice. Expenses for oral disease per year influenced attitude. The findings could help design interventions to improve oral health in general. This study identified specific knowledge items that could be improved through educational interventions, especially regarding the need for blood tests in some oral diseases and the possible complications of diseases on tooth implantation. The present study showed that improvements in knowledge should also translate into improvements in attitudes and practice.
Oral health is a major public health concern because it significantly impacts healthcare expenses, quality of life, and the risk of complications and other diseases (16, 26). For example, an untreated dental abscess can cause endocarditis, or an apparently benign oral lesion can be a developing oral cancer (13–15). Therefore, oral health requires the individuals’ active participation, with proper hygiene habits (brushing teeth, flossing, and looking for potential lesions), undergoing regular teeth cleaning and dentist consultation, and consulting in the presence of a problem (16, 26). The present study revealed good knowledge, positive attitudes, and proactive practice in patients with oral diseases. It contrasts with several previous studies that reported variable knowledge but generally negative attitudes and poor practice toward oral care (19–24). Of course, adherence to oral health can vary widely among countries based on the socioeconomic status, healthcare literacy of the general population, oral health services available, etc. In addition, these previous studies (19–24) were performed in specific populations (e.g., nurses, patients with heart diseases, dental hygienists, parents, adolescents, and married couples) and conditions (oral health, oral hygiene, and oral cancer), limiting their scope and generalizability.
In China, an earlier study published in 2007 showed that 1,590 Chinese individuals aged >25 years had practically no knowledge of common periodontal prevention and treatment, with only a few undergoing more or less regular oral examinations (27). A subsequent study performed in 2012–2015 among 50,991 Chinese showed that 75% of them lacked periodontal knowledge and that 97% did not have regular scaling (28). The present study is the first to examine the KAP toward oral diseases among Chinese patients with oral diseases. The high KAP is probably because all participants had been diagnosed with oral diseases and underwent treatments for their condition, in contrast with the previous Chinese studies that were performed in the general population. Therefore, the participants in the present study are more likely to have received information about their disease and oral health in general and advice on proper oral care to prevent recurrence or the development of other diseases or sought information by themselves.
Supporting that view, the SEM analysis showed that the frequency of oral examination influenced knowledge and practice, suggesting that higher exposure to oral health professionals increased knowledge and improved practice. The participants are also likely to have sought information by themselves on the Internet or with relatives. In addition, most participants had a college/undergraduate education and a middle income. Socioeconomic factors are major determinants of KAP (29), and the present study might be biased due to the participants’ higher socioeconomic status than the general Chinese population. It is well known that socioeconomic status is a major determinant of health literacy (29). Nevertheless, the participants also represent the population of patients seeking oral care since patients with a lower socioeconomic status will often not undergo proper oral care (30, 31), as also observed in China (32, 33), Germany (34), Jordan (35), and Sweden (36). The SEM analysis also showed that expenses for oral disease per year influenced attitudes. Indeed, several studies showed that treatment costs were a barrier to proper oral health (37, 38). In the present study, two-thirds of the participants were ≤35 years old. Age is a major determinant of oral health (39), with older adults showing poor oral health. The young age of the participants in the present study could have contributed to the high KAP compared with previous studies.
A large study performed in the Chinese general population in 2012–2015 revealed that 2.6% were using floss at least once a day, 2.6% were undergoing scaling at least once a year, and 6.4% would visit a dentist in case of gingival bleeding (28). Since then, the Chinese government implemented policies to try to improve oral health in China (40), which could also have contributed to the high KAP observed here.
Nevertheless, this study has limitations. It was performed at a single hospital, leading to a small sample size and limited generalizability. The participants were enrolled through convenience sampling, which could introduce bias since only the interested individuals applied for participation. The online and offline participants were not compared. The questionnaire was designed by local investigators, and its content was probably biased by the local guidelines and policies, also limiting generalizability. In addition, the questionnaire did not undergo a formal validation process; it was not intended to be a standardized questionnaire but a survey. The study was cross-sectional, preventing the analysis of cause-to-effect relationships. Although the SEM analysis provides some information about the relationships among KAP dimensions and possible influencing factors, it is a statistical method that provides an approximation, at best. Finally, all KAP studies are at risk of the social desirability bias, which entails that some participants might answer that they do what they should do instead of what they are really doing (41, 42). Considering the high attitude and practice scores, that bias is probably active in the present study. In addition, KAP is subjective and reflects more on the intention rather than the actual execution.
In conclusion, Chinese patients with oral disease have sufficient knowledge, positive attitudes, and good practice toward oral diseases. Specific knowledge gaps and misconceptions were identified in the participants and would require improvements. Educational interventions should be designed to improve the KAP toward dental care further.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by the Ethics Committee of Tongji University Affiliated Stomatological Hospital ([2023]-SR-36). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
WW: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing.
Funding
The author declares that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Rathee, M, and Sapra, A. Dental caries. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. (2023).
2. Erazo, D, and Whetstone, DR. Dental infections. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. (2023).
3. Patnana, AK, and Kanchan, T. Tooth fracture. In:StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. (2023).
4. Maini, K, and Dua, A. Temporomandibular syndrome. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. (2023).
5. Gupta, R, Gupta, N, and Weber, DK. Dental implants. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. (2023).
6. Bell, A, and Kasi, A. Oral mucositis. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. (2023).
7. Gasner, NS, and Schure, RS. Periodontal disease. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. (2023).
8. Watters, C, Brar, S, and Pepper, T. Oral mucosa cancer. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. (2023).
9. Gonzalez, M, and Riera March, A. Tongue cancer. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. (2023).
10. Bourgeois, D, Goncalves, LS, Lima-Junior, JDC, and Carrouel, F. Editorial: the oral microbiome is a key factor in oral and systemic health. Front Microbiol. (2022) 13:855668. doi: 10.3389/fmicb.2022.855668
11. Gare, J, Kanoute, A, Meda, N, Viennot, S, Bourgeois, D, and Carrouel, F. Periodontal conditions and pathogens associated with pre-eclampsia: a scoping review. Int J Environ Res Public Health. (2021) 18:7194. doi: 10.3390/ijerph18137194
12. Maitre, Y, Mahalli, R, Micheneau, P, Delpierre, A, Amador, G, and Denis, F. Evidence and therapeutic perspectives in the relationship between the oral microbiome and Alzheimer’s disease: a systematic review. Int J Environ Res Public Health. (2021) 18:11157. doi: 10.3390/ijerph182111157
13. Warnakulasuriya, S, Kujan, O, Aguirre-Urizar, JM, Bagan, JV, Gonzalez-Moles, MA, Kerr, AR, et al. Oral potentially malignant disorders: a consensus report from an international seminar on nomenclature and classification, convened by the WHO Collaborating Centre for Oral Cancer. Oral Dis. (2021) 27:1862–80. doi: 10.1111/odi.13704
14. Maymone, MBC, Greer, RO, Burdine, LK, Dao-Cheng, A, Venkatesh, S, Sahitya, PC, et al. Benign oral mucosal lesions: clinical and pathological findings. J Am Acad Dermatol. (2019) 81:43–56. doi: 10.1016/j.jaad.2018.09.061
15. Maymone, MBC, Greer, RO, Kesecker, J, Sahitya, PC, Burdine, LK, Cheng, AD, et al. Premalignant and malignant oral mucosal lesions: clinical and pathological findings. J Am Acad Dermatol. (2019) 81:59–71. doi: 10.1016/j.jaad.2018.09.060
16. Vozza, I. Oral prevention and management of oral healthcare. Int J Environ Res Public Health. (2021) 18:1970. doi: 10.3390/ijerph18041970
17. Andrade, C, Menon, V, Ameen, S, and Kumar, PS. Designing and conducting knowledge, attitude, and practice surveys in psychiatry: practical guidance. Indian J Psychol Med. (2020) 42:478–81. doi: 10.1177/0253717620946111
18. World Health Organization. Advocacy, communication and social mobilization for TB control: a guide to developing knowledge, attitude and practice surveys. (2008). Available at: http://whqlibdoc.who.int/publications/2008/9789241596176_eng.pdf (Accessed November 22, 2022).
19. Lakshmi, KPD, Venkatalakshmi, S, Bharath, C, Saravanan, N, Reddy, LS, and Nagilla, J. Correlation of knowledge, attitude, and practice with their oral health status among young adults of nursing care: a cross-sectional survey. J Pharm Bioallied Sci. (2022) 14:S82–6. doi: 10.4103/jpbs.jpbs_555_21
20. Rasouli-Ghahroudi, AA, Khorsand, A, Yaghobee, S, Rokn, A, Jalali, M, Masudi, S, et al. Oral health status, knowledge, attitude and practice of patients with heart disease. ARYA Atheroscler. (2016) 12:1–9.
21. Coppola, N, Rivieccio, I, Blasi, A, Ferrigno, R, Baldares, S, Mignogna, MD, et al. Current knowledge, attitude and practice among dental hygienists in oral cancer awareness: systematic review. Int J Dent Hyg. (2022) 20:249–61. doi: 10.1111/idh.12575
22. Patil, AN, Karkare, SR, Jadhav, HS, Sirikonda, S, Suryawanshi, VB, and Patil, SN. Knowledge attitude and practices of parents towards oral health maintenance among their children and correlation with dental caries experience-a cross-sectional study. Med J Dr DY Patil Vidyapeeth. (2021) 14:40–4. doi: 10.4103/mjdrdypu.mjdrdypu_310_20
23. Lawal, FB, and Oke, GA. Clinical and sociodemographic factors associated with oral health knowledge, attitude, and practices of adolescents in Nigeria. SAGE Open Med. (2020) 8:2050312120951066. doi: 10.1177/2050312120951066
24. Zhang, Y, Wong, MC, and Lo, EC. Pathways of oral health knowledge, attitudes, practices, and status in married couples. Community Dent Oral Epidemiol. (2016) 44:400–7. doi: 10.1111/cdoe.12228
25. Ni, P, Chen, JL, and Liu, N. Sample size estimation for quantitative studies in nursing research. Chinese J Nurs. (2010) 45:378–80. doi: 10.3761/j.issn.0254-1769.2010.04.037
26. Peres, MA, Macpherson, LMD, Weyant, RJ, Daly, B, Venturelli, R, Mathur, MR, et al. Oral diseases: a global public health challenge. Lancet. (2019) 394:249–60. doi: 10.1016/S0140-6736(19)31146-8
27. Wang, QT, Wu, ZF, Wu, YF, Shu, R, Pan, YP, and Xia, JL. Epidemiology and preventive direction of periodontology in China. J Clin Periodontol. (2007) 34:946–51. doi: 10.1111/j.1600-051X.2007.01139.x
28. Zhao, Q, Wang, SB, Xu, G, Song, Y, Han, X, Liu, Z, et al. Periodontal health: a national cross-sectional study of knowledge, attitudes and practices for the public oral health strategy in China. J Clin Periodontol. (2019) 46:406–19. doi: 10.1111/jcpe.13082
29. Svendsen, MT, Bak, CK, Sorensen, K, Pelikan, J, Riddersholm, SJ, Skals, RK, et al. Associations of health literacy with socioeconomic position, health risk behavior, and health status: a large national population-based survey among Danish adults. BMC Public Health. (2020) 20:565. doi: 10.1186/s12889-020-08498-8
30. Oberoi, SS, Sharma, G, and Oberoi, A. A cross-sectional survey to assess the effect of socioeconomic status on the oral hygiene habits. J Indian Soc Periodontol. (2016) 20:531–42. doi: 10.4103/0972-124X.201629
31. Northridge, ME, Kumar, A, and Kaur, R. Disparities in access to oral health care. Annu Rev Public Health. (2020) 41:513–35. doi: 10.1146/annurev-publhealth-040119-094318
32. Lin, HC, Wong, MC, Wang, ZJ, and Lo, EC. Oral health knowledge, attitudes, and practices of Chinese adults. J Dent Res. (2001) 80:1466–70. doi: 10.1177/00220345010800051601
33. Zhu, L, Petersen, PE, Wang, HY, Bian, JY, and Zhang, BX. Oral health knowledge, attitudes and behaviour of adults in China. Int Dent J. (2005) 55:231–41. doi: 10.1111/j.1875-595x.2005.tb00321.x
34. Deinzer, R, Micheelis, W, Granrath, N, and Hoffmann, T. More to learn about: periodontitis-related knowledge and its relationship with periodontal health behaviour. J Clin Periodontol. (2009) 36:756–64. doi: 10.1111/j.1600-051X.2009.01452.x
35. El-Qaderi, SS, and Quteish, T'a D. Assessment of periodontal knowledge and periodontal status of an adult population in Jordan. Int J Dent Hyg. (2004) 2:132–6. doi: 10.1111/j.1601-5037.2004.00080.x
36. Martensson, C, Soderfeldt, B, Andersson, P, Halling, A, and Renvert, S. Factors behind change in knowledge after a mass media campaign targeting periodontitis. Int J Dent Hyg. (2006) 4:8–14. doi: 10.1111/j.1601-5037.2006.00158.x
37. Thompson, B, Cooney, P, Lawrence, H, Ravaghi, V, and Quinonez, C. The potential oral health impact of cost barriers to dental care: findings from a Canadian population-based study. BMC Oral Health. (2014) 14:78. doi: 10.1186/1472-6831-14-78
38. Levy, BB, Goodman, J, and Eskander, A. Oral healthcare disparities in Canada: filling in the gaps. Can J Public Health. (2023) 114:139–45. doi: 10.17269/s41997-022-00692-y
39. Kassebaum, NJ, Bernabe, E, Dahiya, M, Bhandari, B, Murray, CJ, and Marcenes, W. Global burden of severe periodontitis in 1990-2010: a systematic review and meta-regression. J Dent Res. (2014) 93:1045–53. doi: 10.1177/0022034514552491
40. Zhou, X, Xu, X, Li, J, Hu, D, Hu, T, Yin, W, et al. Oral health in China: from vision to action. Int J Oral Sci. (2018) 10:1. doi: 10.1038/s41368-017-0006-6
41. Bergen, N, and Labonte, R. “Everything is perfect, and we have no problems”: detecting and limiting social desirability bias in qualitative research. Qual Health Res. (2020) 30:783–92. doi: 10.1177/1049732319889354
Keywords: knowledge, attitude, practice, oral diseases, patients, cross-sectional study
Citation: Wang W (2024) Knowledge, attitude, and practice of patients with oral diseases toward oral examinations: a cross-sectional survey study. Front. Public Health. 12:1424503. doi: 10.3389/fpubh.2024.1424503
Edited by:
Ammar Ahmed Siddiqui, University of Hail, Saudi ArabiaReviewed by:
Mohammad Aljanakh, University of Hail, Saudi ArabiaFlorence Carrouel, Université Claude Bernard Lyon 1, France
Farooq Ahmad Chaudhary, Shaheed Zulfiqar Ali Bhutto Medical University (SZABMU), Pakistan
Copyright © 2024 Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wei Wang, Y2hlbmppYWx1bzIwMjMwNjA1QG91dGxvb2suY29t