 Marina Rodríguez-Gómez1
Marina Rodríguez-Gómez1 Guadalupe Pastor-Moreno2,3,4*†Isabel Ruiz-Pérez2,3,4†Vicenta Escribà-Agüir5Vivian Benítez-Hidalgo2†
Guadalupe Pastor-Moreno2,3,4*†Isabel Ruiz-Pérez2,3,4†Vicenta Escribà-Agüir5Vivian Benítez-Hidalgo2†- 1Hospital Clínico Universitario de Valencia, Valencia, Spain
- 2Andalusian School of Public Health (EASP), Granada, Spain
- 3CIBER of Epidemiology and Public Health (CIBERESP), Madrid, Spain
- 4Instituto de Investigación Biosanitaria de Granada. Ibs. GRANADA, Granada, Spain
- 5Fundación para el Fomento de la Investigación Sanitaria y Biomédica de la Comunidad Valenciana (FISABIO), Valencia, Spain
Objectives: Cancer is a major public health problem worldwide, given its magnitude and growing burden, in addition to the repercussions on health and quality of life. Palliative care can play an important role improving quality of life and it is cost-effective, but some population groups may not benefit from it or benefit less based on age and gender inequalities. The aim of this systematic review was to analyze the available evidence on age- and gender-based social inequalities in access to and use of palliative care in cancer patients.
Methods: A systematic review was conducted following the PRISMA guidelines. An exhaustive literature research was performed in Pubmed, CINHAL and Embase until November 2022 and were not restricted by language or date of publication. Eligible studies were observational studies analyzing the access and use of palliative care in cancer patients.
Results: Fifty-three studies were included in the review. Forty-five analyzed age and 44 analyzed gender inequalities in relation to use of and access to palliative care. Our results show that older people receive poorer quality of care, worst symptom control and less preferences for palliative care. In relation to gender, women have a greater preference for the use of palliative care and generally have more access to basic and specialized palliative care services and palliative care facilities.
Conclusion: This review reveals difficulties for older persons and men for access to key elements of palliative care and highlights the need to tackle access barriers for the most vulnerable population groups. Innovative collaborative services based around patient, family and wider community are needed to ensure optimal care.
1 Introduction
Cancer is one of the main causes of morbidity and mortality in the world. The International Agency for Research on Cancer estimates that in 2025 there will be 21.6 million new cases and 11.3 million deaths from cancer worldwide (1).
Advances in cancer diagnosis and treatment have led to an increase in survival and quality of life of cancer patients. But despite these advances, when cancer is diagnosed in advanced stages the chances of a cure are minimal and many people die of this disease. In such cases, palliative care plays an important role, as the aim of this type of care is to improve the quality of life of patients and their families by controlling pain and other symptoms and offering psychological, social and spiritual support (2). The origin of palliative care lies in the modern hospice movement, which is considered a philosophy of care for patients with advanced and terminal diseases that seeks to ensure a “good death” for those who are at the end-of-life (3).
Palliative care is currently seen in a broader perspective that includes the concept of early intervention and ongoing care suited to the needs of the sick and their families. According to the American Society of Clinical Oncology, palliative care should be initiated as early as possible from the time of advanced-stage cancer diagnosis, during treatment and after treatment. The objective is to provide quality care focused on improving symptom control, satisfying patients and their families, reducing use of healthcare services, such as visits to emergency departments, hospitalizations, admissions to intensive care units (ICUs), etc., and performance of inappropriate or unnecessary diagnostic and therapeutic procedures (4, 5).
However, there are difficulties inherent in any effort to develop quality indicators for palliative care, especially focused on end-of-life care. There is a limited evidence base and little consensus among experts and patients as to what constitutes optimal care, and the end-of-life period is hard to identify prospectively (4). There is scientific evidence of social inequalities in relation to cancer (6) and also in relation to palliative care, and the following have been observed: (a) disparities in the various approaches, such as variation in delivery of palliative radiotherapy to persons dying of cancer (7), intensity of end-of-life care (8) and variations in the use of hospice care (9), and (b) population groups that might not benefit from palliative care or would benefit to a lesser extent (10, 11).
These inequalities may be influenced by socio-demographic, clinical or geographical factors (12).
Among the socio-demographic variables, age and gender appear as essential factors in all chronic processes (13, 14).
Age discrimination may give rise to a limitation of healthcare opportunities for a large population group, given the aging of the population (15). It is clear that there are different complexities in care needs between some age groups and others (16, 17) and palliative care should be tailored to these needs to avoid this potential discrimination.
As for gender inequalities, the differences between men and women are not limited to differences in the presentation, identification and course of cancer; the social roles attributed to men and women also influence health and disease processes (18), including palliative care (19).
The objective of this study is to analyze the available evidence on age- and gender-based social inequalities in access to and use of palliative care in cancer patients.
2 Materials and methods
This study was part of a broader systematic review aimed to identify and analyze social inequalities in the access and use of palliative care in cancer patients. This review is part of a larger doctoral thesis1 and was not registered in any database prospectively. But to increase the transparency of the process, the review and its procedures were planned, conducted, and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline (20), and sufficient details have been provided so that other researchers can reproduce the process.
2.1 Search strategy
A specific search strategy was developed for Pubmed using a combination of MeSH (Medical Subject Headings) terms and keywords from titles and abstracts, then the search was adapted for the other databases (CINAHL and Embase). The search strategy is shown in Supplementary Appendix 1. All the searches were performed up to November 2022 and were not restricted by language or date of publication. That is to say, there was no limit set on the number of years backward.
2.2 Study selection
Inclusion criteria: original studies with cross-sectional, cohort or case–control design targeting adult patients (≥18 years) with any type of cancer whose outcome variables measure access to or use of palliative care in the age and gender inequality axes.
2.3 Selection and data extraction process
The references obtained from the literature searches were loaded into the software Rayyan Qatar Computing Research Institute (Doha, Qatar), a free web application designed to facilitate the screening process for researchers working on systematic reviews, scoping reviews and other literature review projects (21). After deleting the duplicate references, we proceeded to screen the studies, first by reviewing the titles and abstracts and then by full-text review. The whole process was carried out by two reviewers (MRG and VEA) and doubts or discrepancies were discussed with a third reviewer (IRP).
Subsequently, forms were designed for data extraction from each study selected. The following information was recorded: title, author, year of publication, country of study, design, number of participants, target population, type of cancer and data collection instrument. The variables related to the inequality axes present and to the various approaches for assessing access to and use of palliative care were also recorded. Finally, the results found in the studies and the results of the risk-of-bias assessment of the studies were recorded.
2.4 Risk-of-bias assessment of the studies
An assessment of the methodological quality of each study was performed using the Newcastle-Ottawa scale (NOS) (22) adapted for case–control, cohort or cross-sectional studies.
The studies were classified into three groups according to the point score obtained in the analysis: high methodological quality (7–10 stars), moderate methodological quality (4–6 stars) and low methodological quality (<4 stars).
2.5 Data synthesis and analysis
According to a previous narrative review conducted by the authors (23), the terms and concepts used in the literature to refer to palliative care and the access and use to this type of care are very wide-ranging, since the same is true of the clinical or therapeutic measures to be adopted in patients. In this study, in order to standardize the terminology and facilitate analysis of the results, palliative care is grouped into five blocks, according to the approaches involved: (a) symptom management: pharmacological measures and/or cancer treatments for palliative purposes; (b) adequacy and quality of care: use of end-of-life healthcare services and aggressiveness end-of-life care (overuse of aggressive anticancer therapies or misuse of non-specific palliative care procedures or devices); (c) access to palliative care services: basic (supportive care) or specialized (end-of-life care [hospice care], palliative care programs, specialist palliative care units, etc.); (d) advance care planning: knowledge of palliative care, preferences and registration of these preferences (clinical history, prior instructions/advance directives) and (e) place of death: home, specialist palliative care centers, acute hospitals and nursing homes. This grouping was formulated on the basis of proposals made by other important authors and/or institutions (24–26).
The results were therefore synthesized and analyzed qualitatively, including a detailed description of the characteristics of the studies and of the inequality axes examined, a classification of the studies into the various approaches considered and an analysis of the inequalities, taking the findings of the studies into account.
3 Results
3.1 Study selection
A total of 2,666 references were identified (Figure 1). Having excluded 58 duplicates, we proceeded to read the titles, abstracts and full texts. After reading full texts 182 studies were excluded. Finally, 53 studies that met the selection criteria and were suitable for the review were selected. Of these, 45 analyzed age (7, 8, 12, 14, 27–66) and 44 analyzed gender (7, 8, 12, 14, 27, 29–43, 45–68) in relation to use of and access to palliative care.
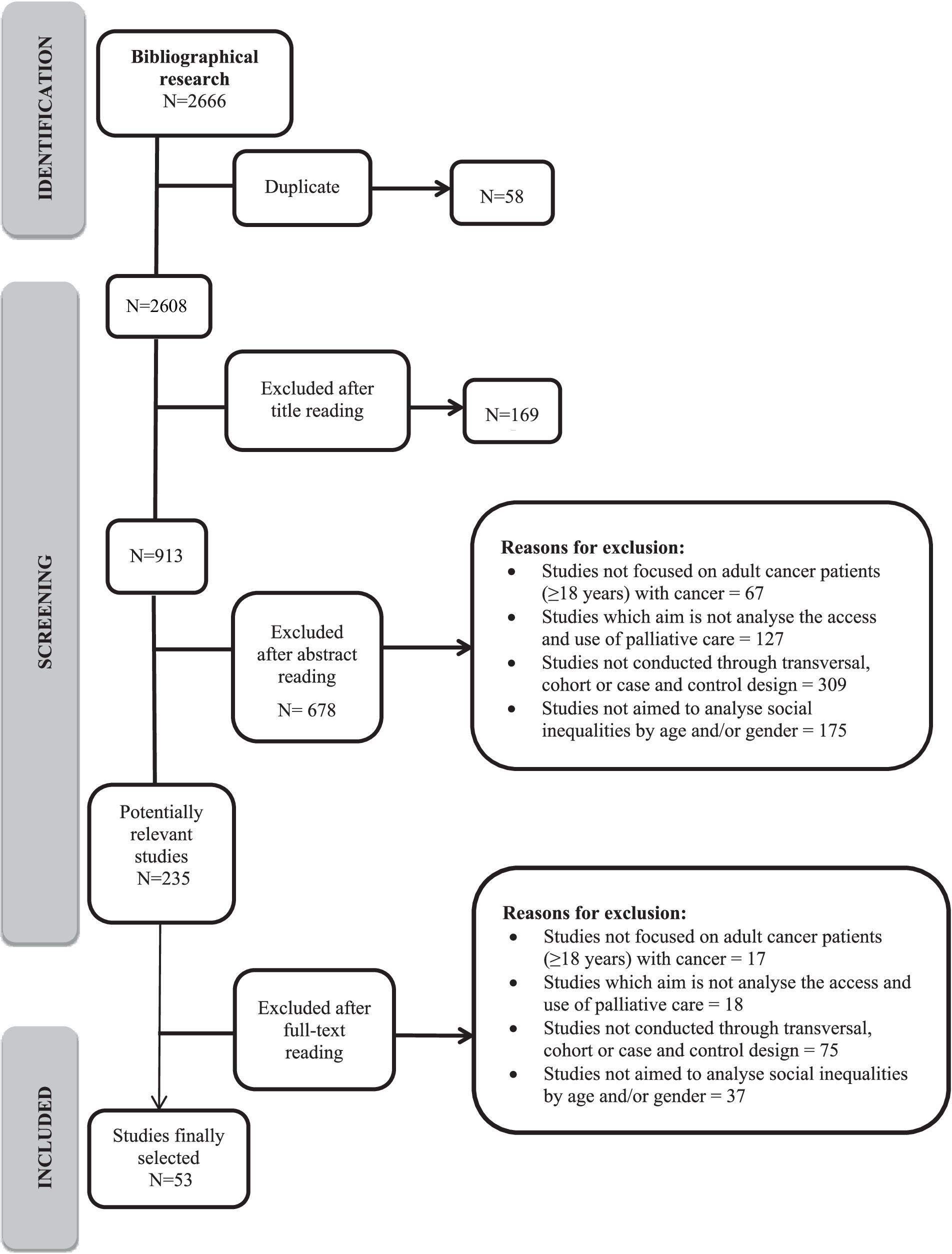
Figure 1. PRISMA flow diagram.
3.2 Study characteristics
The studies were published between 2001 and 2022. The years with the highest number of publications were 2020–2022 (20; 37.7%). The country in which the most studies were conducted was the United States (25), followed by Canada (7). Thirty-four studies analyze several types of cancer together, sometimes without identifying which. Of the remainder, 10 studies focus on gastrointestinal cancer, 2 on lung cancer, 2 on gynecological cancer, 2 on genitourinary cancer, 2 on central nervous system cancer and 1 on breast cancer.
Thirty-three of the studies follow a retrospective cohort design and the other 20 use a cross-sectional design (Table 1).
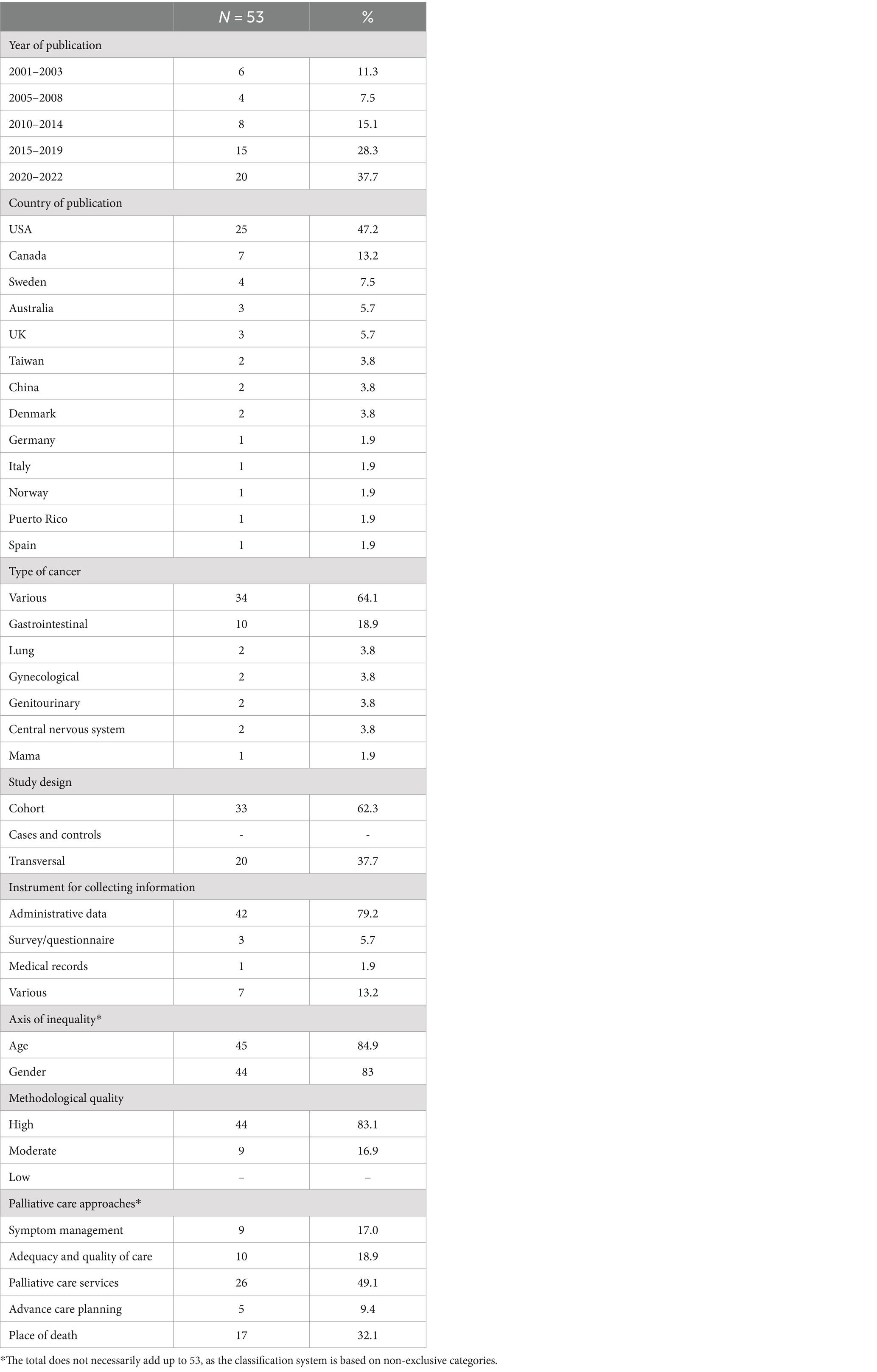
Table 1. Characteristics of the studies.
3.3 Methodological quality
A total of 83.1% of the studies were assessed as being of high methodological quality with low risk of bias and 16.9% of moderate methodological quality (9, 14, 39, 47, 53, 57, 58, 62, 64) (Table 2).
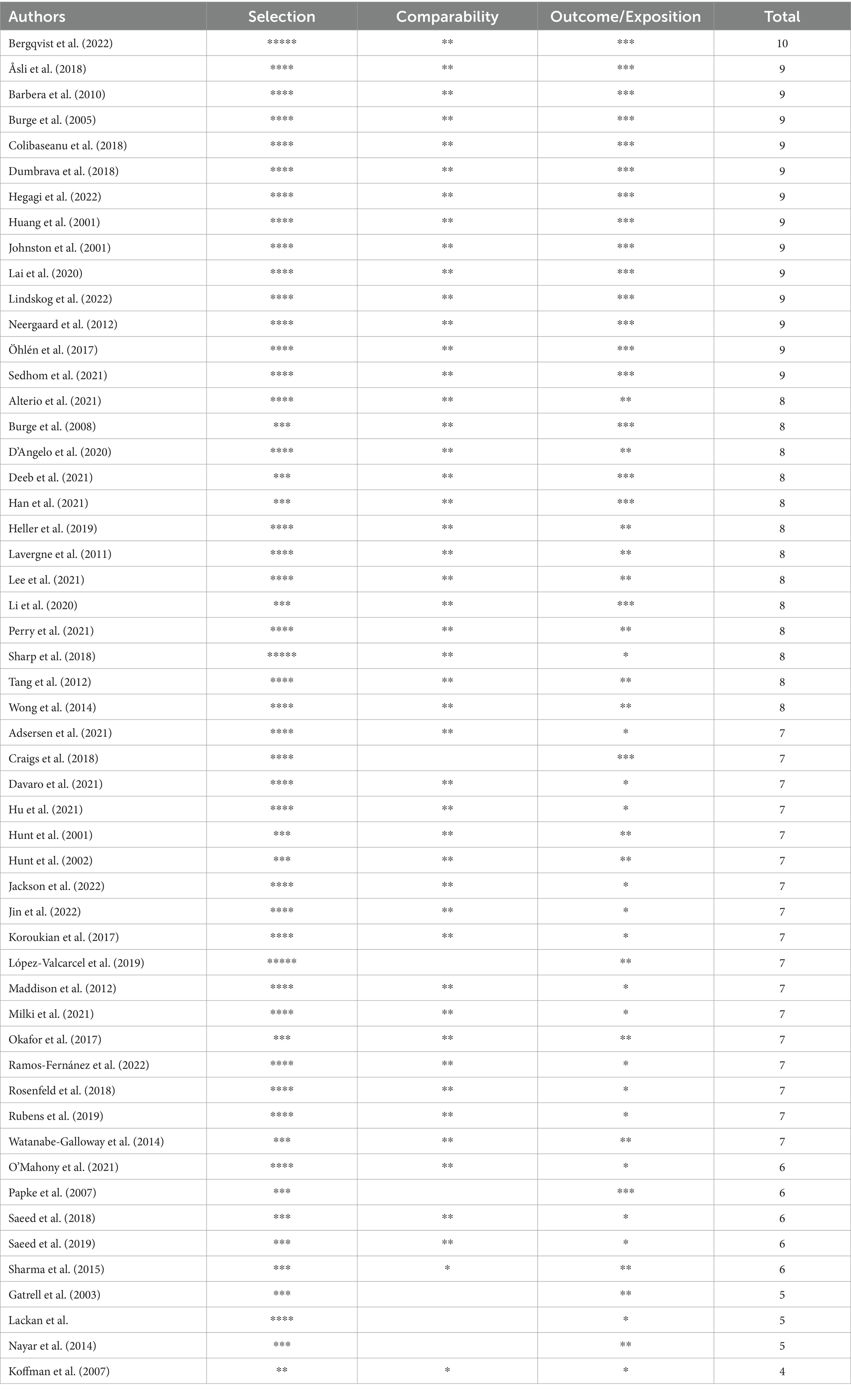
Table 2. Methodological quality evaluation.
3.4 Synthesis of results
The Tables 3–5 shows the results of the classification of the studies finally included according to the type of palliative care approach and the result variables examined and grouped by common characteristics, and in Supplementary Appendix 2 these can be seen in more detail.
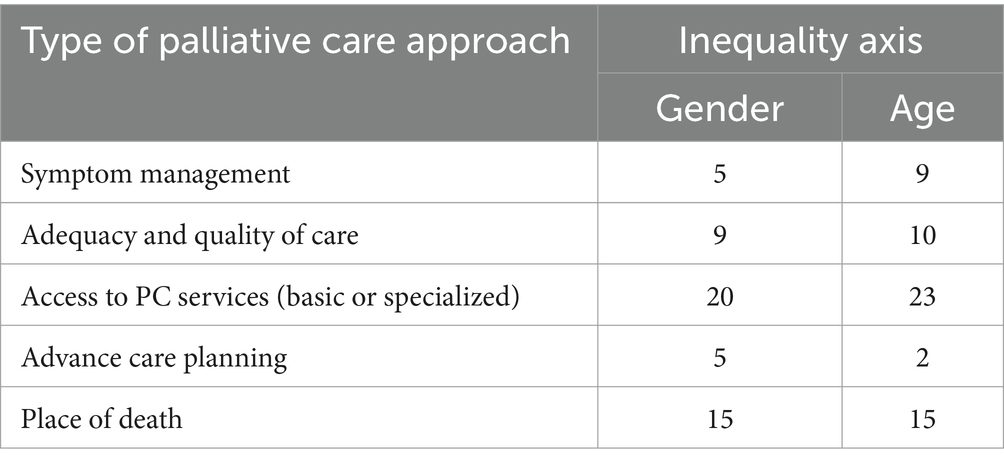
Table 3. Number of studies identified by inequality access and type of approach.

Table 4. Approaches to analyze the access and use of palliative care of included studies.
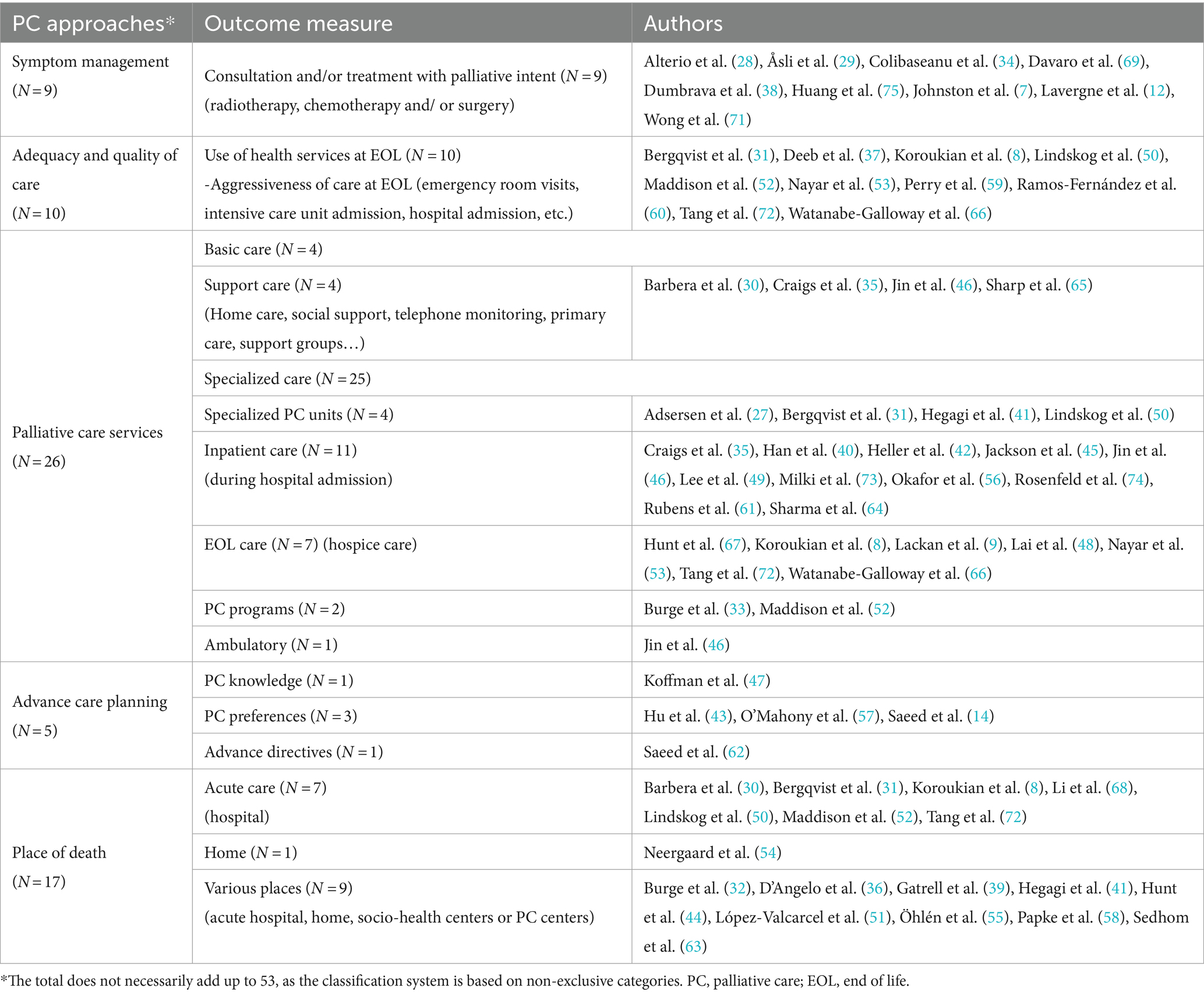
Table 5. Study classification by PC approaches.
Forty-four studies analyze how gender influences access to and use of palliative care. Five analyze access to symptom management (7, 12, 29, 34, 38), 9 adequacy and quality of care (8, 31, 37, 50, 52, 53, 59, 60, 66), 20 access to palliative care services (8, 27, 30, 33, 35, 40–42, 45, 46, 48–50, 52, 53, 56, 61, 64–66), 5 advance care planning (14, 43, 47, 57, 62) and 15 the place of death (8, 30–32, 36, 39, 44, 50–52, 54, 55, 58, 63, 68).
Of the 45 studies identified that examine the effect of age on access to and use of palliative care, 9 analyze access to care for symptom management (7, 12, 28, 29, 34, 38, 69–71), 10 adequacy and quality of care (8, 31, 37, 50, 52, 53, 59, 60, 66, 72), 23 access to palliative care services (8, 9, 27, 30–32, 35, 40–42, 45, 48–50, 52, 53, 61, 65–67, 72–74), 2 advance care planning (14, 62) and 15 the place of death (8, 30–32, 36, 39, 41, 50, 52, 54, 55, 58, 63, 67, 72).
3.5 Age and symptom management
Of the 9 studies that assess the effect of age on access to care for symptom management (access to consultation and/or cancer treatment for palliative purposes: radiotherapy, chemotherapy, palliative surgery and pain management), 7 show that access to such care is lower in older patients, especially those over the age of 80, compared to younger patients (7, 12, 29, 34, 38, 71, 75). Alterio et al. (28) and Davaro et al. (69) find no age differences in reception of palliative care in patients with metastasis and advanced cancer.
3.6 Age and adequacy and quality of care
Of the 10 studies that assess the aggressiveness of end-of-life care according to age, and therefore the adequacy and quality of care, 8 report fewer emergency department visits, hospital admissions, curative treatment with chemotherapy, etc., and therefore lesser therapeutic aggressiveness in older patients, especially those aged over 80–85 years (8, 31, 37, 53, 59, 60, 66, 72). Three studies find no differences in respect of age and emergency department visits (50, 52, 73).
Lindskog et al. find no differences in hospital admissions, but their study is restricted to the last 3 months of life (50), and Perry et al. find no differences in ICU admissions, but in relation to the last month of life (59).
3.7 Age and access to palliative care services
Twenty-three studies analyze the effect of age on access to palliative care services.
In 12 studies older patients were less likely to have access to basic palliative care (supportive care, home care, telephone follow-up, etc.) (30, 35, 65) and to specialized palliative care (specialist palliative care units, palliative care programs and hospice care) (9, 27, 31, 33, 35, 48, 50, 52, 66).
In contrast, 9 studies show more frequent use of palliative care in older patients (40–42, 49, 53, 61, 72–74) and 4 find no statistically significant differences in access to basic palliative care (35, 65) and to specialized palliative care (hospice care and palliative care during hospitalization [inpatient palliative care]) (8, 45).
3.8 Age and advance care planning
Two studies examine how age influences opinions on advance care planning. Saeed et al. conclude that completion of advance directives on care is preferred by older patients compared to younger patients (62) and that patients over 65 show less preference for palliative care compared to younger patients (14).
3.9 Age and place of death
Fifteen studies analyze the association between place of death and age and 8 show that older patients die at home less often (30, 31, 39, 44, 55, 58, 63, 72).
With regard to dying in hospital, older patients did so more often in 2 studies (39, 44) and less often in 5 (30, 31, 55, 63, 72).
Six studies find no statistically significant relationship between age and dying in acute hospital or dying out of hospital (8, 32, 41, 50, 55).
3.10 Gender and symptom management
Five studies evaluate the association between gender and access to care for symptom management (access to consultation and/or cancer treatment for palliative purposes [radiotherapy]) (7, 12, 29, 34, 38). Two of these studies show that women are less likely to receive palliative radiotherapy compared to men (12, 29). The other three studies (7, 34, 38) find no statistically significant differences in access to consultation and/or radiotherapy, chemotherapy and surgery.
3.11 Gender and adequacy and quality of care
Nine studies assess suitability of care according to gender, analyzing aggressiveness of end-of-life care (hospital admissions, ICU admissions, visits to emergency departments, systemic therapy: chemotherapy, mechanical ventilation, etc.).
Four studies show that women have better therapeutic suitability because they receive less aggressive care (50, 53, 60, 66). As for admissions, Bergqvist et al. show a higher number of hospitalizations in women with breast cancer than in men with prostate cancer (31).
Seven studies find no differences in chemotherapy treatment (8, 59), emergency department visits (8, 37, 50, 52, 53, 59), hospital admissions (59, 66), ICU admission (59) or use of invasive treatments (37, 59).
3.12 Gender and access to palliative care services
Twenty studies consider access to palliative care services according to gender. Ten of them show that being a woman increased the chances of having access to palliative care, both basic (30, 46) and specialized (27, 33, 35, 48, 49, 53, 56, 66), compared to men.
Three studies (30, 35, 46) show greater access for women to palliative care plans such as home visits, inpatient palliative care and social support. In the study by Sharp et al. (65) it was men that were more likely to have access to personalized care plans.
Thirteen studies find no gender differences in access to basic (30, 35, 46, 65) or specialized (40, 42, 45, 46, 61, 64) palliative care, specialist palliative care units (41, 50), outpatient palliative care (46), hospice care (8) and registration in a palliative care program (52).
3.13 Gender and advance care planning
Five studies analyze how gender influences preferences on care planning (14, 43, 47, 57, 62).
The studies by Saeed et al. (14), O’Mahony et al. (57) and Hu et al. (43) show that women have a greater preference for palliative care and less for the use of life-prolonging invasive treatments (mechanical ventilation) compared to men, but in some cases women prefer decisions on care to be initiated by others (healthcare professionals). Two studies find no statistically significant differences in relation to knowledge of palliative care (47) and preferences regarding care objectives or cardiopulmonary resuscitation orders (57).
3.14 Gender and place of death
Fifteen studies show results on gender and place of death.
Four show that women die less often in acute hospitals (30, 39, 51, 63). They are more likely than men to die out of hospital (32), at home (51), in a specialist palliative care center (44, 51, 63) and in nursing homes (39, 44, 58, 63).
Hunt et al. show that women, compared to men, are more likely to die in a private hospital than in a public hospital (44).
Eight studies found no relationship between gender and dying at home (36, 44, 54), in specialist palliative care centers (36), in acute hospitals (8, 50, 52, 55, 68), in nursing homes (55) or out of hospital (41).
4 Discussion
Although palliative care services have increased, it is equally important to understand whether these services are used by patients who really need them. The social determinants of health influence access to and use of palliative care (52, 76, 77), but no reviews have been published on this that allow us to assess whether or not inequalities exist. This is the first systematic literature review to analyze palliative care in respect of two axes of inequality (age, gender) and of five specific ways of addressing access to and use of this type of care in adult cancer patients. The main results to be highlighted are the following: older people receive worse care for symptom control and poorer quality of care and show less preference for palliative care; there are no conclusive results on place of death. With regard to gender, women have a greater preference for the use of palliative care, generally have more access to basic and specialized palliative care and die less often in hospitals and more in palliative care facilities.
The contradictory results found may be explained by the fact that the use of palliative care cannot be addressed without taking account of comorbidities and the presence or absence of metastasis (42, 61) and even the type of cancer. Moreover, survival time in a specialized palliative care setting is a good indicator of timely referral to the service and is often associated with less aggressive treatments (use of chemotherapy, emergency department visit, intensive care admission) (36).
On the other hand, there is literature on the need to use quality indicators to improve comparability in studies, among other things (4), but in spite of this, a large degree of variability has been observed in the time windows considered. For example, Colibaseanu et al. consider patients who survived for less than 6 months (34), Dumbrava et al. restrict their analysis to patients who did not die within 30 days of diagnosis (38), Lavergne et al. study palliative radiotherapy (PRT) treatment received in the last 9 months of life (12), Wong et al. examine the reception of chemotherapy within 14 days of death (71) and Asli et al. consider patients who had PRT at least once during the last two years before death (29). Bergqvist et al. use data on palliative care services received for the 3 months preceding the date of death (31) and Tang et al. examine underuse of hospice services as measured by lack of or very late referral to hospice (3 days before death) (72).
Most of the studies use administrative databases, and as with many studies relying on administrative sources of healthcare data, some of the services identified in the administrative data have not been validated with chart review data or individualized information.
We find that 10 studies independently looked at gastrointestinal cancers. The type of cancer studied may be determined by its magnitude and burden. Gastrointestinal cancers represent a large proportion of new cases and deaths from cancer worldwide, for example, colorectal cancer is one of the most incident and deadly cancer (78). Also, the aggressiveness and the stage of cancer can determine the study of a type of cancer, for example pancreatic cancer is usually diagnosed in advanced stages with poor prognoses and high palliative needs. Therefore, there is a greater need for evaluating the state of palliative care in these types of cancer. In addition, gastrointestinal cancer encompasses different types of cancer related to the diverse organs that are part of the gastrointestinal system.
Most of the studies were carried out in the USA. It is possible that the American health system (unlike universal coverage) could create more inequalities than other health systems, thus generating more interest among the country’s scientific community. It is also possible that the development level of low-income countries corresponds to the underdevelopment of their health systems or financial difficulties. Generally, there is limited access to palliative care due to distances, poor accessibility to healthcare in general, and cultural beliefs and attitudes toward illness (79). Peeler’s review highlights that the northern and central regions of Africa are underrepresented in the published scientific literature. They found that almost all African countries lacking published literature on primary palliative care also had no known palliative care activities or were in very early stages of capacity development (80).In this review we have seen that many studies continue to analyze the suitability of care and end-of life palliative care and that few studies have focused on studying advance planning of care, another important issue within palliative care, despite the change in the palliative care model that suggests early integration of palliative care (81).
Another essential issue within palliative care is the place of death, and especially dying at home (82).
However, this is not always possible or desirable and depends on the availability of resources (83). The best choice is one that is mutually agreed and takes account of the preferences and wishes of the patient, family members and caregivers (84) and the best place to die is the one that matches those preferences (85). In the studies reviewed here preferences are not taken into account or not mentioned and only the place where the patients die is analyzed. Moreover, the outcome measure is the actual place of death, which is not necessarily where patients spend most of their last months. Death in the hospital does not rule out the possibility that they were dying somewhere else up until their last days.
Very few of the studies reviewed were designed to examine differences between men and women and the gender variable was included as an adjustment variable. The importance of gender has recently been highlighted as a source of inequalities in palliative care (11, 86, 87).
The social roles ascribed to men and women in a given society influence attitudes and beliefs about health and disease and may guide healthcare decisions (88). It must be borne in mind that there are differences between men and women in the presentation, detection and evaluation of the disease and the related symptoms (86, 88) and that women, for cultural reasons, may prefer decisions about their health to be initiated by others (43), which could also determine access to palliative care and might explain the lower access of women to care for symptom control as well as cancer treatment for palliative purposes (14).
The limitations of this review arise from the variability of the studies analyzed, which makes it difficult, in many cases, to obtain conclusive results. On the other hand, however, it has allowed us to point out the difficulties of the study proposed and the need to explore the disparities identified here in more depth. Taking only two axes of inequality into account, our study reveals difficulties faced by structurally vulnerable population groups in gaining access to key elements of palliative care and highlight the need to tackle barriers to access.
Future interventions should promote that all cancer patients receive high-quality palliative care, regardless of their age or gender, respecting their individual needs and promoting equity in healthcare. It is necessary to ensure that professionals understand the particularities of palliative care in older patients, including polypharmacy, frailty, and comorbidities. Support services are also required to address the specific concerns of each gender, such as the caregiver role traditionally associated with women or the stigma of vulnerability in men.
This review reveals difficulties for older persons and men for access to key elements of palliative care and highlights the need to address access barriers for the most vulnerable population groups. The inequalities identified in this review are not just the responsibility of the hospice movement. Innovative collaborative services based around patient, family and wider community are needed to ensure optimal care for all. For some groups, therefore, lower use of hospice services may reflect care preferences and choices rather than inequality of provision.
Author contributions
MR-G: Data curation, Formal analysis, Investigation, Visualization, Writing – original draft, Writing – review & editing. GP-M: Supervision, Validation, Writing – original draft, Writing – review & editing. IR-P: Conceptualization, Methodology, Writing – original draft, Writing – review & editing. VE-A: Conceptualization, Methodology, Writing – original draft, Writing – review & editing. VB-H: Data curation, Software, Visualization, Writing – original draft, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research was supported by CIBERESP-Consorcio Centro de Investigación Biomédica en Red Epidemiología y Salud Pública, Instituto de Salud Carlos III, Ministerio de Ciencia e Innovación.
Acknowledgments
The authors would like to thank Camila Higueras Callejón, the documentalist responsible for designing and executing the search strategies.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2024.1421940/full#supplementary-material
Footnotes
References
1. Ervik, M, Lam, F, Laversanne, M, Ferlay, J, and Bray, F. Global Cancer observatory: Cancer over time. Lyon, France: International Agency for Research on Cancer (2021).
2. Bruera, E, and Yennurajalingam, S. Palliative care in advanced cancer patients: how and when? Oncologist. (2012) 17:267–73. doi: 10.1634/theoncologist.2011-0219
3. Ferrell, BR, Temel, JS, Temin, S, Alesi, ER, Balboni, TA, Basch, EM, et al. Integration of palliative care into standard oncology care: American Society of Clinical Oncology clinical practice guideline update. J Clin Oncol. (2017) 35:96–112. doi: 10.1200/JCO.2016.70.1474
4. Earle, CC, Neville, BA, Landrum, MB, Souza, JM, Weeks, JC, Block, SD, et al. Evaluating claims-based indicators of the intensity of end-of-life cancer care. Int J Qual Health Care. (2005) 17:505–9. doi: 10.1093/intqhc/mzi061
5. Hui, D, and Bruera, E. Integrating palliative care into the trajectory of cancer care. Nat Rev Clin Oncol. (2016) 13:159–71. doi: 10.1038/nrclinonc.2015.201
6. Vaccarella, S, Lortet-Tieulent, J, Saracci, R, Conway, DI, Straif, K, and Wild, CP eds. Reducing social inequalities in cancer: Evidence and priorities for research. Lyon, FR: International Agency for Research on Cancer (2019).
7. Johnston, GM, Boyd, CJ, Joseph, P, and MacIntyre, M. Variation in delivery of palliative radiotherapy to persons dying of cancer in Nova Scotia, 1994 to 1998. J Clin Oncol. (2001) 19:3323–32. doi: 10.1200/JCO.2001.19.14.3323
8. Koroukian, SM, Schiltz, NK, Warner, DF, Given, CW, Schluchter, M, Owusu, C, et al. Social determinants, multimorbidity, and patterns of end-of-life care in older adults dying from cancer. J Geriatric Oncol. (2017) 8:117–24. doi: 10.1016/j.jgo.2016.10.001
9. Lackan, NA, Freeman, JL, and Goodwin, JS. Hospice use by older women dying with breast cancer between 1991 and 1996. J Palliat Care. (2003) 19:49–53. doi: 10.1177/082585970301900109
10. Abdollah, F, Sammon, JD, Majumder, K, Reznor, G, Gandaglia, G, Sood, A, et al. Racial disparities in end-of-life care among patients with prostate Cancer: a population-based study. J Natl Compr Cancer Netw. (2015) 13:1131–8. doi: 10.6004/jnccn.2015.0138
11. Wong, AD, and Phillips, SP. Gender disparities in end of life care: a scoping review. J Palliat Care. (2023) 38:78–96. doi: 10.1177/08258597221120707
12. Lavergne, MR, Johnston, GM, Gao, J, Dummer, TJB, and Rheaume, DE. Variation in the use of palliative radiotherapy at end of life: examining demographic, clinical, health service, and geographic factors in a population-based study. Palliat Med. (2011) 25:101–10. doi: 10.1177/0269216310384900
13. MacGuire, FAS . Reducing health inequalities in aging through policy frameworks and interventions. Front Public Health. (2020) 8:315. doi: 10.3389/fpubh.2020.00315
14. Saeed, F, Hoerger, M, Norton, SA, Guancial, E, Epstein, RM, and Duberstein, PR. Preference for palliative Care in Cancer Patients: are men and women alike? J Pain Symptom Manag. (2018) 56:1–6.e1. doi: 10.1016/j.jpainsymman.2018.03.014
15. Butler, RN . Age-ism: another form of bigotry. Gerontologist. (1969) 9:243–6. doi: 10.1093/geront/9.4_part_1.243
16. Abdelaal, M, Mosher, PJ, Gupta, A, Hannon, B, Cameron, C, Berman, M, et al. Supporting the needs of adolescents and young adults: integrated palliative care and psychiatry Clinic for Adolescents and Young Adults with Cancer. Cancers (Basel). (2021) 13:770. doi: 10.3390/cancers13040770
17. Hall, S . Palliative care for older people: Better practices. Copenhagen: World Health Organization, Regional Office for Europe (2011).
18. Lee, E, and Wen, P. Gender and sex disparity in cancer trials. ESMO Open. (2020) 5:e000773. doi: 10.1136/esmoopen-2020-000773
19. Cain, JM, and Denny, L. Palliative care in women’s cancer care: global challenges and advances. Int J Gynaecol Obstet. (2018) 143:153–8. doi: 10.1002/ijgo.12624
20. Page, MJ, McKenzie, JE, Bossuyt, PM, Boutron, I, Hoffmann, TC, Mulrow, CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
21. Ouzzani, M, Hammady, H, Fedorowicz, Z, and Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Syst Rev. (2016) 5:210. doi: 10.1186/s13643-016-0384-4
22. Wells, GA, Wells, G, Shea, B, Shea, B, O’Connell, D, Peterson, J, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses (2014) Available at: https://api.semanticscholar.org/CorpusID:79550924 (Accessed May 14, 2023).
23. Rodríguez-Gómez, M, Ruiz-Pérez, I, Escribà-Agüir, V, Pastor-Moreno, G, and Henares-Montiel, J. Cuidados paliativos y desigualdades sociales en cáncer. Una revisión narrativa de la literatura. Med paliat. (2023) 30:95–101. doi: 10.20986/medpal.2022.1358/2022
24. Hasson, F, Jordan, J, McKibben, L, Graham-Wisener, L, Finucane, A, Armour, K, et al. Challenges for palliative care day services: a focus group study. BMC Palliat Care. (2021) 20:11. doi: 10.1186/s12904-020-00699-7
25. Saga, Y, Enokido, M, Iwata, Y, and Ogawa, A. Transitions in palliative care: conceptual diversification and the integration of palliative care into standard oncology care. Chin Clin Oncol. (2018) 7:32. doi: 10.21037/cco.2018.06.02
26. Types of palliative and supportive care. CancerNet (2019) https://www.cancer.net/coping-with-cancer/physical-emotional-and-social-effects-cancer/types-palliative-and-supportive-care (Accessed November 15, 2023).
27. Adsersen, M, Chen, IM, Rasmussen, LS, Johansen, JS, Nissen, M, Groenvold, M, et al. Regional and age differences in specialised palliative care for patients with pancreatic cancer. BMC Palliat Care. (2021) 20:1–9. doi: 10.1186/S12904-021-00870-8/FIGURES/1
28. Alterio, RE, Ju, MR, Wang, SC, Mansour, JC, Yopp, A, and Porembka, MR. Socioeconomic and racial/ethnic disparities in receipt of palliative care among patients with metastatic hepatocellular carcinoma. J Surg Oncol. (2021) 124:1365–72. doi: 10.1002/JSO.26672
29. Asli, LM, Myklebust, TA, Kvaloy, SO, Jetne, V, Moller, B, Levernes, SG, et al. Factors influencing access to palliative radiotherapy: a Norwegian population-based study. Acta Oncol. (2018) 57:1250–8. doi: 10.1080/0284186X.2018.1468087
30. Barbera, L, Sussman, J, Viola, R, Husain, A, Howell, D, Librach, SL, et al. Factors associated with end-of-life health service use in patients dying of Cancer. Healthcare Policy. (2010) 5:e125–43. doi: 10.12927/hcpol.2013.21644
31. Bergqvist, J, Hedman, C, Schultz, T, and Strang, P. Equal receipt of specialized palliative care in breast and prostate cancer: a register study. Supportive Care Cancer. (2022) 30:7721–30. doi: 10.1007/S00520-022-07150-Y
32. Burge, FI, Lawson, B, and Johnston, G. Where a Cancer patient dies: the effect of rural residency. J Rural Health. (2005) 21:233–8. doi: 10.1111/j.1748-0361.2005.tb00088.x
33. Burge, FI, Lawson, BJ, Johnston, GM, and Grunfeld, E. A population-based study of age inequalities in access to palliative care among cancer patients. Med Care. (2008) 46:1203–11. doi: 10.1097/MLR.0b013e31817d931d
34. Colibaseanu, DT, Osagiede, O, Spaulding, AC, Frank, RD, Merchea, A, Mathis, KL, et al. The determinants of palliative care use in patients with colorectal Cancer: a National Study. Am J Hosp Palliat Med. (2018) 35:1295–303. doi: 10.1177/1049909118765092
35. Craigs, CL, West, RM, Hurlow, A, Bennett, MI, and Ziegler, LE. Access to hospital and community palliative care for patients with advanced cancer: a longitudinal population analysis. PLoS One. (2018) 13:e0200071–1. doi: 10.1371/journal.pone.0200071
36. D’Angelo, D, Di Nitto, M, Giannarelli, D, Croci, I, Latina, R, Marchetti, A, et al. Inequity in palliative care service full utilisation among patients with advanced cancer: a retrospective cohort study. Acta Oncol. (2020) 59:620–7. doi: 10.1080/0284186X.2020.1736335
37. Deeb, S, Chino, FL, Diamond, LC, Tao, A, Aragones, A, Shahrokni, A, et al. Disparities in care management during terminal hospitalization among adults with metastatic Cancer from 2010 to 2017. JAMA Netw Open. (2021) 4:e2125328–8. doi: 10.1001/JAMANETWORKOPEN.2021.25328
38. Dumbrava, MI, Burmeister, EA, Wyld, D, Goldstein, D, O’Connell, DL, Beesley, VL, et al. Chemotherapy in patients with unresected pancreatic cancer in Australia: a population-based study of uptake and survival. Asia Pac J Clin Oncol. (2018) 14:326–36. doi: 10.1111/ajco.12862
39. Gatrell, AC, Harman, JC, Francis, BJ, Thomas, C, Morris, SM, and McIllmurray, M. Place of death: analysis of cancer deaths in part of north West England. J Public Health Med. (2003) 25:53–8. doi: 10.1093/pubmed/fdg011
40. Han, H, Yu, F, Wu, C, Dai, L, Ruan, Y, Cao, Y, et al. Trends and utilization of inpatient palliative care among patients with metastatic bladder Cancer. J Palliat Care. (2021) 36:105–12. doi: 10.1177/0825859720924936
41. Hegagi, M, James, P, Hsu, A, and Tanuseputro, P. Home care use and out-of-hospital death in pancreatic Cancer patients: a retrospective cohort study. J Palliat Care. (2022) 38:175–83. doi: 10.1177/08258597221075088
42. Heller, D, Jean, R, Chiu, A, Feder, S, Kurbatov, V, Cha, C, et al. Regional differences in palliative care utilization among geriatric colorectal Cancer patients needing emergent surgery. J Gastrointest Surg. (2019) 23:153–62. doi: 10.1007/S11605-018-3929-0
43. Hu, L, Chu, Q, Fan, Z, and Chen, Y. Discussion of advance care planning on end-of-life decisions with lung cancer patients in Wuhan, China: attitude, timing and future directions. Intern Med J. (2021) 51:2111–8. doi: 10.1111/IMJ.14958
44. Hunt, RW, Fazekas, BS, Luke, CG, and Roder, DM. Where patients with cancer die in South Australia, 1990-1999: a population-based review. Med J Aust. (2001) 175:526–9. doi: 10.5694/j.1326-5377.2001.tb143710.x
45. Jackson, I, Jackson, N, and Etuk, A. Prevalence and factors associated with palliative care utilization among hospitalized patients with esophageal Cancer in the United States. J Palliat Care. (2022) 38:192–9. doi: 10.1177/08258597221113716
46. Jin, MC, Hsin, G, Ratliff, J, Thomas, R, Zygourakis, CC, Li, G, et al. Modifiers of and disparities in palliative and supportive care timing and utilization among neurosurgical patients with malignant central nervous system tumors. Cancers. (2022) 14:2567–7. doi: 10.3390/CANCERS14102567
47. Koffman, J, Burke, G, Dias, A, Raval, B, Byrne, J, Gonzales, J, et al. Demographic factors and awareness of palliative care and related services. Palliat Med. (2007) 21:145–53. doi: 10.1177/0269216306074639
48. Lai, YJ, Chen, YY, Ko, MC, Chou, YS, Huang, LY, Chen, YT, et al. Low socioeconomic status associated with lower utilization of hospice care services during end-of-life treatment in patients with Cancer: a population-based cohort study. J Pain Symptom Manag. (2020) 60:309–315.e1. doi: 10.1016/J.JPAINSYMMAN.2020.03.015
49. Lee, K, Gani, F, Canner, JK, and Johnston, FM. Racial disparities in utilization of palliative care among patients admitted with advanced solid organ malignancies. Am J Hosp Palliat Care. (2021) 38:539–46. doi: 10.1177/1049909120922779
50. Lindskog, M, Schultz, T, and Strang, P. Acute healthcare utilization in end-of-life among Swedish brain tumor patients - a population based register study. BMC Palliat Care. (2022) 21:133–3. doi: 10.1186/S12904-022-01022-2
51. López-Valcárcel, BG, Pinilla, J, and Barber, P. Dying at home for terminal cancer patients: differences by level of education and municipality of residence in Spain. Gac Sanit. (2019) 33:568–74. doi: 10.1016/j.gaceta.2018.06.011
52. Maddison, AR, Asada, Y, Burge, F, Johnston, GW, and Urquhart, R. Inequalities in end-of-life care for colorectal cancer patients in Nova Scotia, Canada. J Palliative Care. (2012) 28:90–6. doi: 10.1177/082585971202800205
53. Nayar, P, Qiu, F, Watanabe-Galloway, S, Boilesen, E, Wang, H, Lander, L, et al. Disparities in end of life Care for Elderly Lung Cancer Patients. J Community Health. (2014) 39:1012–9. doi: 10.1007/s10900-014-9850-x
54. Neergaard, MA, Jensen, AB, Sokolowski, I, Olesen, F, and Vedsted, P. Socioeconomic position and place of death of cancer patients. BMJ Support Palliat Care. (2012) 2:133–9. doi: 10.1136/bmjspcare-2011-000116
55. Ohlen, J, Cohen, J, and Hakanson, C. Determinants in the place of death for people with different cancer types: a national population-based study. Acta Oncol. (2017) 56:455–61. doi: 10.1080/0284186X.2016.1250946
56. Okafor, PN, Stobaugh, DJ, Nnadi, AK, and Talwalkar, JA. Determinants of palliative care utilization among patients hospitalized with metastatic gastrointestinal malignancies. Am J Hospice Palliat Care. (2017) 34:269–74. doi: 10.1177/1049909115624373
57. O’Mahony, S, Kittelson, S, Barker, PC, Delgado Guay, MO, Yao, Y, Handzo, GF, et al. Association of Race with end-of-life treatment preferences in older adults with Cancer receiving outpatient palliative care. J Palliat Med. (2021) 24:1174–82. doi: 10.1089/JPM.2020.0542
58. Papke, J, and Koch, R. Places of death from cancer in a rural location. Onkologie. (2007) 30:105–8. doi: 10.1159/000098705
59. Perry, LM, Walsh, LE, Horswell, R, Miele, L, Chu, S, Melancon, B, et al. Racial disparities in end-of-life care between black and white adults with metastatic Cancer. J Pain Symptom Manag. (2021) 61:342–349.e1. doi: 10.1016/J.JPAINSYMMAN.2020.09.017
60. Ramos-Fernández, MR, Ortiz-Ortiz, KJ, Torres-Cintrón, CR, and Tortolero-Luna, G. Patterns of end-of-life care as measured by emergency room visits among Cancer patients in Puerto Rico. Am J Hosp Palliat Care. (2022) 39:72–8. doi: 10.1177/10499091211025743
61. Rubens, M, Ramamoorthy, V, Saxena, A, Das, S, Appunni, S, Rana, S, et al. Palliative care consultation trends among hospitalized patients with advanced Cancer in the United States, 2005 to 2014. Am J Hospice Palliat Care. (2019) 36:294–301. doi: 10.1177/1049909118809975
62. Saeed, F, Xing, G, Tancredi, DJ, Epstein, RM, Fiscella, KA, Norton, SA, et al. Is annual income a predictor of completion of advance directives (ADs) in patients with cancer. Am J Hospice Palliat Med. (2019) 36:402–7. doi: 10.1177/1049909118813973
63. Sedhom, R, Kuo, PL, Gupta, A, Smith, TJ, Chino, F, Carducci, MA, et al. Changes in the place of death for older adults with cancer: reason to celebrate or a risk for unintended disparities? J Geriatric Oncol. (2021) 12:361–7. doi: 10.1016/J.JGO.2020.10.008
64. Sharma, RK, Cameron, KA, Chmiel, JS, Von Roenn, JH, Szmuilowicz, E, Prigerson, HG, et al. Racial/ethnic differences in inpatient palliative care consultation for patients with advanced Cancer. J Clin Oncol. (2015) 33:3802–8. doi: 10.1200/JCO.2015.61.6458
65. Sharp, L, Westman, B, Olofsson, A, Leppänen, A, and Henriksson, R. Access to supportive care during and after cancer treatment and the impact of socioeconomic factors. Acta Oncol. (2018) 57:1303–10. doi: 10.1080/0284186X.2018.1484157
66. Watanabe-Galloway, S, Zhang, W, Watkins, K, Islam, K, Nayar, P, Boilesen, E, et al. Quality of end-of-life care among rural Medicare beneficiaries with colorectal Cancer. J Rural Health. (2014) 30:397–405. doi: 10.1111/jrh.12074
67. Hunt, RW, Fazekas, BS, Luke, CG, Priest, KR, and Roder, DM. The coverage of cancer patients by designated palliative services: a population-based study, South Australia, 1999. Palliat Med. (2002) 16:403–9. doi: 10.1191/0269216302pm571oa
68. Li, Z, Jiang, S, Xu, C, Lu, F, He, R, Pan, Z, et al. Determinants of place of death for end-stage cancer patients: evidence from China. Int J Qual Health Care. (2020) 32:41–7. doi: 10.1093/INTQHC/MZZ064
69. Davaro, FM, Weinstein, D, Siddiqui, SA, and Hamilton, ZA. A lack of palliative therapy use in patients with advanced penile Cancer. J Palliat Care. (2021) 36:98–104. doi: 10.1177/0825859720946887
70. Huang, CY, Hung, YT, Chang, CM, Juang, SY, and Lee, CC. The association between individual income and aggressive end-of-life treatment in older cancer decedents in Taiwan. PLoS One. (2015) 10:e0116913–3. doi: 10.1371/journal.pone.0116913
71. Wong, J, Xu, B, Yeung, HN, Roeland, EJ, Martinez, ME, Le, Q-T, et al. Age disparity in palliative radiation therapy among patients with advanced Cancer. Int J Radiaton Oncol Biol Physics. (2014) 90:224–30. doi: 10.1016/j.ijrobp.2014.03.050
72. Tang, ST, Liu, TW, Shyu, Y-IL, Huang, EW, Koong, SL, and Hsiao, SC. Impact of age on end-of-life care for adult Taiwanese cancer decedents, 2001-2006. Palliat Med. (2012) 26:80–8. doi: 10.1177/0269216311406989
73. Milki, A, Mann, AK, Gardner, A, Kapp, DS, English, D, and Chan, JK. Trends in the utilization of palliative Care in Patients with Gynecologic Cancer who Subsequently Died during Hospitalization. Am J Hosp Palliat Care. (2021) 38:138–46. doi: 10.1177/1049909120935038
74. Rosenfeld, EB, Chan, JK, Gardner, AB, Curry, N, Delic, L, and Kapp, DS. Disparities associated with inpatient palliative care utilization by patients with metastatic gynecologic cancers: a study of 3337 women. Am J Hospice Palliat Care. (2018) 35:697–703. doi: 10.1177/1049909117736750
75. Huang, J, Zhou, S, Groome, P, Tyldesley, S, Zhang-Solomans, J, and Mackillop, W. Factors affecting the use of palliative radiotherapy in Ontario. J Clin Oncol. (2001) 19:137–44. doi: 10.1200/JCO.2001.19.1.137
76. Cerni, J, Rhee, J, and Hosseinzadeh, H. End-of-life Cancer care resource utilisation in rural versus urban settings: a systematic review. Int J Environ Res Public Health. (2020) 17:4955. doi: 10.3390/ijerph17144955
77. Parajuli, J, Tark, A, Jao, Y-L, and Hupcey, J. Barriers to palliative and hospice care utilization in older adults with cancer: a systematic review. J Geriatr Oncol. (2020) 11:8–16. doi: 10.1016/j.jgo.2019.09.017
78. Bray, F, Laversanne, M, Sung, H, Ferlay, J, Siegel, RL, Soerjomataram, I, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2024) 74:229–63. doi: 10.3322/caac.21834
79. Ooko, F, Mothiba, T, Van Bogaert, P, and Wens, J. Access to palliative care in patients with advanced cancer of the uterine cervix in the low- and middle-income countries: a systematic review. BMC Palliat Care. (2023) 22:140. doi: 10.1186/s12904-023-01263-9
80. Peeler, A, Afolabi, O, Adcock, M, Evans, C, Nkhoma, K, van Breevoort, D, et al. Primary palliative care in low- and middle-income countries: a systematic review and thematic synthesis of the evidence for models and outcomes. Palliat Med. (2024):2692163241248324. doi: 10.1177/02692163241248324
81. Haun, MW, Estel, S, Rücker, G, Friederich, H-C, Villalobos, M, Thomas, M, et al. Early palliative care for adults with advanced cancer. Cochrane Database Syst Rev. (2017) 2017:CD011129. doi: 10.1002/14651858.CD011129.pub2
82. Ali, M, Capel, M, Jones, G, and Gazi, T. The importance of identifying preferred place of death. BMJ Support Palliat Care. (2019) 9:84–91. doi: 10.1136/bmjspcare-2015-000878
83. Fereidouni, A, Rassouli, M, Salesi, M, Ashrafizadeh, H, Vahedian-Azimi, A, and Barasteh, S. Preferred place of death in adult Cancer patients: a systematic review and Meta-analysis. Front Psychol. (2021) 12:704590. doi: 10.3389/fpsyg.2021.704590
84. Minamiguchi, Y . Decision-making about the place of death for Cancer patients: a concept analysis. Asia Pac J Oncol Nurs. (2020) 7:103–12. doi: 10.4103/apjon.apjon_38_19
85. García-Sanjuán, S, Fernández-Alcántara, M, Clement-Carbonell, V, Campos-Calderón, CP, Orts-Beneito, N, and Cabañero-Martínez, MJ. Levels and determinants of place-of-death congruence in palliative patients: a systematic review. Front Psychol. (2021) 12:807869. doi: 10.3389/fpsyg.2021.807869
86. Gott, M, Morgan, T, and Williams, L. Gender and palliative care: a call to arms. Palliat Care Soc Pract. (2020) 14:2632352420957997. doi: 10.1177/2632352420957997
87. MacWilliams, B, and McArthur, E. Hospice and palliative care-men and gender-specific roles. Nurs Clin North Am. (2023) 58:607–15. doi: 10.1016/j.cnur.2023.06.004
88. Ullrich, A, Grube, K, Hlawatsch, C, Bokemeyer, C, and Oechsle, K. Exploring the gender dimension of problems and needs of patients receiving specialist palliative care in a German palliative care unit - the perspectives of patients and healthcare professionals. BMC Palliat Care. (2019) 18:59. doi: 10.1186/s12904-019-0440-7
Keywords: palliative care, hospice and palliative care, gender, age, review – systematic
Citation: Rodríguez-Gómez M, Pastor-Moreno G, Ruiz-Pérez I, Escribà-Agüir V and Benítez-Hidalgo V (2024) Age- and gender-based social inequalities in palliative care for cancer patients: a systematic literature review. Front. Public Health. 12:1421940. doi: 10.3389/fpubh.2024.1421940
Edited by:
Ibou Thior, PATH, United StatesReviewed by:
Gabriel Madeira Werberich da Silva, National Cancer Institute (INCA), BrazilNicholas Matovu, Queen’s University Belfast, United Kingdom
Copyright © 2024 Rodríguez-Gómez, Pastor-Moreno, Ruiz-Pérez, Escribà-Agüir and Benítez-Hidalgo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Guadalupe Pastor-Moreno, Z3VhZGFsdXBlLnBhc3Rvci5lYXNwQGp1bnRhZGVhbmRhbHVjaWEuZXM=
†ORCID: Guadalupe Pastor-Moreno, https://orcid.org/0000-0002-8039-3427
Isabel Ruiz-Pérez, https://orcid.org/0000-0002-9565-0502
Vivian Benítez-Hidalgo, https://orcid.org/0000-0002-9879-8780